
Abstract
The aim of this experiment is to compare the biomechanical strength of six distinct internal fixation techniques for Mayo type IIA olecranon fractures using biomechanical analysis. This study utilized tensile tests on artificial, shape-mimicking olecranon bones to assess their biomechanical properties. A tensile test was performed on the artificial, shape-mimicking olecranon bone at a 90° angle, with the tensile load applied at a rate of 2 mm/min until the test displacement reached 2 mm, at which point the test was halted. Throughout the test, the testing system was able to collect load and displacement data in real-time and simultaneously monitor the changes in the load-displacement relationship. The maximum loads for groups A-F were (75.34 ± 2.54), (85.53 ± 2.45), (106.57 ± 3.57), (115.21 ± 11.96), (92.76 ± 3.22), and (147.19 ± 4.29) N, respectively, and the stiffnesses were (33.46 ± 2.96), (39.29 ± 1.12), (51.07 ± 3.22), (53.76 ± 5.26), (40.99 ± 1.34), and (71.66 ± 1.77) N/mm, respectively. When the implantation depth of the Kirschner wires reached four times the standard deviation depth, its maximum load and stiffness performance were superior to those of the double cortical Kirschner wire tension band fixation.
Similar content being viewed by others


Intruduction
Olecranon fractures account for 8 to 10% of all elbow fractures, exhibiting a bimodal distribution1. The Mayo classification is widely used in clinical practice, categorizing fractures into: Type I (non-displaced), Type II (stable, displaced), and Type III (unstable, displaced).At present, the common internal fixation methods for the treatment of the Olecranon fracture include tension band fixation, K-wire/screw tension band fixation, intramedullary nail fixation, and plate fixation2,3,4, tension band wiring remains the gold standard for the management of displaced, non-comminuted fractures2,5.However, recent studies6 have demonstrated that the failure rate associated with the standard Kirschner wire tension band technique for internal fixation can reach 39.6%.When the Kirschner wire is implanted too deeply through the anterior cortex of the coronoid process, it can limit forearm rotation and increase the risk of neurovascular injury7,8.Huang et al.9 compared three tension band wiring techniques for olecranon fractures. They found that placing Kirschner wires in the distal ulnar canal minimized proximal pin migration and reduced elbow irritation, making it the preferred configuration for stability and fewer complications.Therefore, to identify the optimal tension band wiring (TBW) configuration and construct, this study analyzed the biomechanical stability of intramedullary Kirschner wire (K‑wire) fixation using four different insertion depths—specifically 2, 3, 4, and 5 times a defined anatomical reference distance (D), where D represents the vertical span along the ulnar axis between the tip of the olecranon and the tip of the coronoid process. These intramedullary constructs were compared with bicortical K‑wire tension band fixation and olecranon locking plate fixation. The results establish the minimal required intramedullary K‑wire insertion depth, offering a biomechanically informed reference for clinical decision‑making.
Materials and methods
Specimen preparation and study design
This biomechanical study utilized eighteen synthetic ulnar bone models (Model 3426 C01371, Sawbones, USA). A standardized transverse olecranon fracture pattern (Mayo Type IIA)10 was simulated in each specimen. Using an oscillating saw, an intra-articular osteotomy was performed at the center of the semilunar notch, corresponding precisely to the depth of the trochlear notch, to replicate the clinical fracture morphology (Fig. 1).

Diagram of the Mayo Type IIA fracture of the olecranon process of the ulna. Line C is the vertical line from the apex of the coronal process to the ulnar axis.Line A is parallel to Line C and passes through the tip of the olecranon. Line B bisects Line A and Line C and serves as the fracture line for Mayo IIA type in this experiment. The vertical distance between line A and line C is the standard deviation depth of the Kirschner wire placement in this experiment. Point C is the installation position of the tensile cable in this experiment.
The specimens were subsequently randomized into six experimental groups (n = 3 per group) for evaluation of different fixation constructs. The primary intervention involved intramedullary Kirschner wire (K-wire) tension band fixation, tested at four defined insertion depths. Insertion depth was standardized using an anatomical reference measurement (D), defined as the vertical distance measured along the ulnar axis from the tip of the olecranon to the tip of the coronoid process. The tested depths were 2D, 3D, 4D, and 5D. These experimental constructs were compared against two control fixation methods: conventional bicortical K-wire tension band fixation and fixation with an olecranon locking plate system.
Surgical techniques
Groups A-D (intramedullary K-wire fixation)
For Groups A through D, fixation was performed using an intramedullary K-wire tension band technique. Two 2.0-mm K-wires were inserted in parallel from the olecranon tip into the medullary cavity to the specified depth (2D, 3D, 4D, or 5D for Groups A, B, C, and D, respectively). Subsequently, a 2.0-mm transverse drill hole was created through the dorsal ulnar cortex approximately 4 cm distal to the tip of the olecranon. A 1.3-mm stainless steel cerclage wire(Guangci Medical, China) was passed through this hole, crossed over the exposed K-wire ends, and routed beneath the triceps tendon in a figure-of-eight configuration. The wire was tightened and secured with a single knot to generate interfragmentary compression.
Group E (bicortical K-wire fixation)
In Group E, two 2.0-mm K-wires were inserted in parallel from the olecranon to engage the anterior cortex, achieving bicortical purchase. The subsequent tension band wiring procedure (drill hole, cerclage wire placement, and knot fixation) was identical to that described for Groups A-D.
Group F (locking plate fixation)
Specimens in Group F were fixed using an olecranon locking plate system(Dabo Medical, China). The plate was contoured and applied to the dorsal surface of the ulna.After tapping, the screws were measured by the tap length after ulna fixation.The osteotomy was fixed with 4 3.5 mm locking cancellous screws proximally and 3 3.5 mm locking bicortical screws distally11.
Verification and quality control
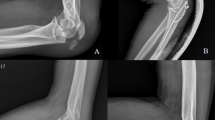
K-wire insertion depth was verified intraoperatively using a digital vernier caliper. Following construct completion, each bone-implant assembly was assessed with a high-frequency mobile C-arm X-ray system (BG9000-1) to confirm appropriate implant positioning, absence of iatrogenic fracture, and overall structural integrity prior to mechanical testing (Fig. 2).

Different internal fixation methods (A–F) for Mayo IIA fracture models and lateral views and X-ray of each group. Standard deviation depth: The standard deviation is the vertical distance along the ulnar axis from the tip of the olecranon to the tip of the coronoid process.
Biomechanical testing
Testing apparatus
Biomechanical testing was performed using an MTS Bionix858 servo-hydraulic testing system capable of applying tensile, compressive, and torsional loads(Fig. 3). The system has a static load capacity of 0–25 kN and a static torque range of 0–250 N·m. The experimental setup was designed to evaluate the fixation stability of each construct under tensile loading, a method previously validated for assessing olecranon fracture fixation12.

MTS 858 BionixHydraulic testing system.
Testing protocol
Following specimen preparation, each bone-implant construct was mounted onto the testing frame. The ulnar axis and its articular surface were aligned perpendicular to the loading axis of the machine. A horizontal cylindrical steel bar was positioned within the ulnar joint cavity to simulate the humeral trochlea and to standardize the joint articulation. To apply a tensile load simulating triceps tendon pull, a 2.0-mm transverse drill hole was created through the tip of the olecranon. A 1.3-mm metal cable was passed through this hole in a U-shaped configuration, with both free ends attached to the moving crosshead of the testing machine. This arrangement replicated the articulation between the ulna and humerus at 90° of elbow flexion, consistent with previously published methodologies12(Fig. 4).

Biomechanical test setup simulating the humeroulnar joint at 90°of flexion. The MTS Bionix858 hydraulic testing system was used to evaluate the stability and strength of the fixation under axial tensile load. In this test, the axes of the ulna and that of the articulating surface were set perpendicular to the loading axis of the machine.The distal ulna was embedded and fixed with denture base resin, and a custom fixture was fixed to the testing equipment(as indicated by the blue arrow )to simulate the elbow flexion at 90°(as indicated by the red arrow ). A horizontal, cylindrical steel bar was inserted into the ulnar joint cavity to mimic the humeral trochlea.The olecranon was vertically pulled by a cable to simulate the natural extension pulling force of the triceps tendon on the olecranon (as indicated by the yellow arrow ). Stiffness was quantified by measuring the slope of the load-displacement curve using a load sensor as an alternative indicator of the stability of fracture fixation. The ultimate strength of fracture fixation was defined as the load size at the failure point. Therefore, the test results were characterized by stiffness and maximum load in this experiment.
All tests were conducted under displacement control at a constant rate of 2 mm/min until a total displacement of 2 mm was achieved13,14. Load and displacement data were recorded in real-time throughout the test, allowing for continuous monitoring of the load-displacement behavior and determination of structural stiffness .
Statistical analysis
Analyses were performed using the SPSS software (SPSS Version 20; SPSS Inc., Chicago, IL, United States). Differences in stiffness and strength among the six fracture fixation groups were evaluated using one-way ANOVA, with significance set at P < 0.05.
Results
The maximum load and stiffness values for groups A-F are summarized in Fig. 5. Group F (ulnar olecranon locking plate) demonstrated significantly greater maximum load and stiffness than all other groups. This was followed by groups C, D, and E, while groups A and B exhibited the lowest mechanical properties (Figs. 6 and 7). Specific values were as follows: maximum loads (N): A = 75.34 ± 2.54, B = 85.53 ± 2.45, C = 106.57 ± 3.57, D = 115.21 ± 11.96, E = 92.76 ± 3.22, F = 147.19 ± 4.29; stiffnesses (N/mm): A = 33.46 ± 2.96, B = 39.29 ± 1.12, C = 51.07 ± 3.22, D = 53.76 ± 5.26, E = 40.99 ± 1.34, F = 71.66 ± 1.77.

Bar chart comparison of tensile tests on ulna fracture models.

Difference in the mean strength and stiffness between the six types of fracture fixation. ∗, statistical significance. *→****, significant enhancement.

Tensile test curve diagram of ulna fracture model. Each line shows the average data of each group of samples.
Although Group E demonstrated higher maximum load and stiffness than Group B, the differences were not statistically significant (P > 0.05). In contrast, Groups C and D exhibited significantly superior mechanical properties when compared to Group E (P < 0.05; Table 1).As shown in Table 2, the maximum load and stiffness of groups A to D demonstrate a progressive increase. This trend indicates a positive correlation between the implantation depth of the Kirschner wires and the enhancement of these biomechanical properties.
Discussion
Advantages of ulnar tension band fixation
-
The primary objective in the surgical treatment of olecranon fractures is to restore anatomical structure and provide sufficient absolute stability15. The tension band wiring (TBW) technique is considered the gold standard for non-comminuted olecranon fractures, typically involving two intramedullary Kirschner wires and a figure-of-eight cerclage wire16. This method offers several advantages, including technical simplicity, reliable fixation, the possibility of early postoperative mobilization, and excellent cost-effectiveness.
-
Historically, the tension band principle for transverse olecranon fractures was described as converting distraction forces on the dorsal ulnar cortex into compressive forces at the articular surface during elbow flexion17. However, recent biomechanical studies have demonstrated that this conversion does not occur throughout the full range of movement18. Despite this biomechanical clarification, the technique continues to yield excellent healing and functional outcomes in patients with good bone quality.
Refinements in the Tension Band Wiring (TBW) technique have progressively improved fixation outcomes for olecranon fractures and lowered the incidence of postoperative complications, notably reducing the risk of fixation failure19,20. In a comparative study by Yu et al.21, the clinical performance of a perforated Kirschner wire (K-wire) tension band was evaluated against olecranon anatomical plating and conventional TBW in Mayo IIA fractures. The perforated K-wire method was associated with shorter operative time, less blood loss, fewer intraoperative fluoroscopies, and a lower rate of skin irritation. It also resulted in accelerated fracture healing, establishing it as a favorable surgical option that promotes recovery while minimizing adverse events.
Kuwahara et al.22 proposed a modified approach termed Locked Tension Band Wiring (LTBW), which involves coiling and securing the proximal K-wire ends and tension band with a flexible wire to prevent wire migration. This technique markedly reduced complication rates (10.3% vs. 37.9%), implant removal rates (41.4% vs. 72.4%), and K-wire migration (3.79 mm vs. 8.97 mm) compared to conventional TBW. Although LTBW required longer operative time, functional outcomes were comparable between the groups.
A prospective randomized trial23 (n = 200) comparing TBW and precontoured plate fixation (PF) for isolated, displaced olecranon fractures (Mayo IIA and IIB) found TBW to be non-inferior to PF in functional outcomes at 12 months, as measured by QuickDASH scores. While TBW was associated with significantly shorter operative time (median 64 vs. 88 min), it led to a higher frequency of secondary surgeries, mainly due to hardware irritation. Other complications were similar, and both methods showed comparable clinical results at two-year follow-up.
In a biomechanical study by Zhao et al.24, three fixation methods—traditional TBW, intramedullary screw with TBW (IM-TBW), and Ding’s screw TBW (DSTBW)—were tested on Synbone models of Mayo IIA olecranon fractures. DSTBW demonstrated superior stability, evidenced by smaller fracture gaps at 60° and 90° flexion, higher maximum failure load (1229.1 ± 110.0 N), and greater pullout strength (1324.0 ± 43.8 N) relative to IM-TBW and TBW. The study supports DSTBW as a biomechanically advantageous technique with the potential to mitigate common complications such as implant migration and soft tissue irritation.
Based on a retrospective cohort study of 97 patients with Mayo IIA olecranon fractures, Steadman et al.25 reported that tension band wiring (TBW) was associated with significantly lower total direct costs during index surgery compared to plate fixation (PF), with plating costing 2.6 times more than TBW in a multivariable model. This cost advantage for TBW remained evident even under a hypothetical scenario in which all TBW hardware required removal and no plates were removed, highlighting TBW as a more cost-effective option without compromising clinical outcomes such as union and complication rates, which were comparable between groups. Similarly, a study by Tan et al.26 comparing TBW and PF for Mayo IIA fractures found no significant difference in functional outcomes at one year. TBW was associated with a significantly lower overall cost despite a higher rate of implant failure, whereas PF was linked to higher rates of wound complications and infection. The authors concluded that TBW is a cost-effective and clinically non-inferior alternative for managing these fractures.
Biomechanical analysis
-
The experimental results indicate that the maximum load and stiffness of Group F (ulnar olecranon locking plate) significantly outperform those of the other groups.
-
The maximum load and stiffness of Groups A (intramedullary Kirschner wire tension band fixation (at 2 times the standard deviation depth) to Group D (intramedullary Kirschner wire tension band fixation (at 5 times the standard deviation depth) improve with the increasing depth of Kirschner wire implantation into the bone marrow.
-
Group A exhibited the lowest maximum load and stiffness. Although Group E showed higher values than Group B, the difference was not statistically significant (P > 0.05). Notably, Groups C (intramedullary Kirschner wire tension band fixation at 4 times the standard deviation depth) and D (intramedullary fixation at 5 times the standard deviation depth) demonstrated superior maximum load and stiffness compared to Group E (bicondylar fixation). These results suggest that an intramedullary implantation depth of at least 4 times the standard deviation achieves greater biomechanical strength than the bicondylar Kirschner wire tension band fixation.
Points to note for tension band fixation
When employing the traditional Kirschner wire technique that passes through the double cortex, the tip of the Kirschner wire must not penetrate excessively into the anterior cortex of the ulna to prevent impairment of the patient’s rotational function and nerve injury7,8. These modifications to the Tension Band Wiring (TBW) technique have reduced the volume of internal fixation and the risk of K-wire pull-out, while maintaining the TBW technique as the most cost-effective treatment option19,27 .The primary challenge of intramedullary K-wire placement is the instability of the construct. This instability may lead to complications, including proximal migration of the pins, displacement of the fracture line, and an unstable construct, potentially causing osteoarthritis in long-term follow-up28.Nevertheless, intramedullary fixation using Kirschner wires can effectively avert such complications. The steel wires on either side should be tightened concurrently to avoid any imbalance that could result from one side being overly taut. The tail of the Kirschner wire should be left with adequate length—approximately 5 to 10 mm—to allow for bending and embedding. Additionally, after bending the tail of the wire 180°, it should be driven into the bone to minimize skin irritation.
The shortcomings of this study
This study has several limitations. Firstly, the small sample size of the fracture models and the single testing session may affect the findings. Secondly, the elbow is a complex joint, containing synovial fluid, multiple muscles, and ligaments. However, the biomechanical effects of soft tissues and other bony structures, such as the humerus and radius, were not included in our study. To study the biomechanics of elbow trauma, it is often challenging to establish a model that is both practically and ethically acceptable and also provides reliable results. Synbone models are frequently used in biomechanical experiments. Their advantages include uniform geometry and material properties, which eliminate sample variability due to factors such as age, sex, anatomy, demographics, and bone quality. Additionally, Synbone models are easier to obtain than cadaveric models.
Conclusions
Our biomechanical analyses indicate that the maximum load and stiffness of Group C (intramedullary Kirschner wire tension band fixation at 4 times the standard deviation depth) and Group D (intramedullary Kirschner wire tension band fixation at 5 times the standard deviation depth) surpass those of Group E (bicondylar Kirschner wire tension band fixation). This suggests that implanting the Kirschner wire at a depth of 4 times the standard deviation results in superior maximum load and stiffness performance compared to bicondylar Kirschner wire tension band fixation.
Data availability
The datasets generated and analysed during the current study are not publicly available due to the research project is still being further developed and deepened but are available from the corresponding author on reasonable request.
References
Cantore, M., Candela, V., Sessa, P., Giannicola, G. & Gumina, S. Epidemiology of isolated olecranon fractures: a detailed survey on a large sample of patients in a suburban area. JSES Int. 6, 309–314. https://doi.org/10.1016/j.jseint.2021.11.015 (2022).
den Hamer, A. et al. Current techniques for management of transverse displaced olecranon fractures. Muscles Ligaments Tendons J. 5, 129–140 (2015).
Baecher, N. & Edwards, S. Olecranon fractures. J. Hand Surg. Am. 38, 593–604. https://doi.org/10.1016/j.jhsa.2012.12.036 (2013).
Veillette, C. J. H. & Steinmann, S. P. Olecranon fractures. Orthop. Clin. North. Am. https://doi.org/10.1016/j.ocl.2008.01.002 (2008).
Chalidis, B. E., Sachinis, N. C., Samoladas, E. P., Dimitriou, C. G. & Pournaras, J. D. Is tension band wiring technique the gold standard for the treatment of olecranon fractures? A long term functional outcome study. J. Orthop. Surg, Res. 3, 9. https://doi.org/10.1186/1749-799X-3-9 (2008).
Powell, A. J., Farhan-Alanie, O. M. & McGraw, I. W. W. Tension band wiring versus locking plate fixation for simple, two-part Mayo 2A olecranon fractures: a comparison of post-operative outcomes, complications, reoperations and economics. Musculoskelet. Surg. 103, 155–160. https://doi.org/10.1007/s12306-018-0556-6 (2018).
Parker, J. R., Conroy, J. & Campbell, D. A. Anterior interosseus nerve injury following tension band wiring of the olecranon. Injury 36, 1252–1253 (2005).
Candal-Couto, J. J., Williams, J. R. & Sanderson, P. L. Impaired forearm rotation after tension-band-wiring fixation of olecranon fractures: evaluation of the transcortical K-wire technique. J. Orthop. Trauma. 19, 480–482 (2005).
Huang, T. W. et al. Tension band wiring for olecranon fractures: relative stability of Kirschner wires in various configurations. J. Trauma. 68, 173–176. https://doi.org/10.1097/TA.0b013e3181ad554c (2010).
Siebenlist, S., Buchholz, A. & Braun, K. F. Fractures of the proximal ulna: current concepts in surgical management. EFORT Open. Rev. 4, 1–9. https://doi.org/10.1302/2058-5241.4.180022 (2019).
Hewins, E. A. et al. Plate fixation of olecranon osteotomies. J. Orthop. Trauma. 21, 58–62 (2007).
Batihan, A. O., Maden, M., Ozdemir, M. & Kazimoglu, C. Is headless screw a valid alternative for the fixation of chevron olecranon osteotomy? A Biomechanical comparison of 4 fixation methods. J. Shoulder Elbow Surg. 34, 680–687. https://doi.org/10.1016/j.jse.2024.06.019 (2025).
Wang, K. Y. et al. Where should the pins be placed to decrease the failure rate after fixation of a Mayo IIA olecranon fracture? A Biomechanical analysis. Injury-International J. Care Injured 51, 1522–1526. https://doi.org/10.1016/j.injury.2020.04.018 (2020).
Lee, S. H. & Lee, Y. H. Ideal pin length and interval in tension band wiring using ring pins for transverse olecranon fractures: a biomechanical study. BMC Musculoskelet. Disord. https://doi.org/10.1186/s12891-025-08828-0 (2025).
Wilson, J., Bajwa, A., Kamath, V. & Rangan, A. Biomechanical comparison of interfragmentary compression in transverse fractures of the olecranon. J. Bone Joint Surg. Br. 93, 245–250. https://doi.org/10.1302/0301-620X.93B2.24613 (2011).
Di Francia, R. et al. Advantages of expulsion-proof pins in the treatment of olecranon fractures with tension band wiring: comparison with a control group. Orthop. Traumatol. Surg. Res. 105, 1593–1599. https://doi.org/10.1016/j.otsr.2019.08.020 (2019).
Gierer, P., Wichelhaus, A. & Rotter, R. [Fractures of the olecranon]. Oper. Orthop. Traumatol. 29, 107–114. https://doi.org/10.1007/s00064-017-0490-z (2017).
Brink, P. R. G. et al. Tension band wiring of the olecranon: is it really a dynamic principle of osteosynthesis? Injury 44, 518–522. https://doi.org/10.1016/j.injury.2012.08.052 (2012).
Villanueva, P., Osorio, F., Commessatti, M. & Sanchez-Sotelo, J. Tension-band wiring for olecranon fractures: analysis of risk factors for failure. J. Shoulder Elb. Surg. 15, 351–356 (2006).
Chan, K. W. & Donnelly, K. J. Does K-wire position in tension band wiring of olecranon fractures affect its complications and removal of metal rate? J. Orthop. 12, 111–117. https://doi.org/10.1016/j.jor.2014.04.018 (2014).
Yu, X. et al. Perforated Kirschner wire tension band in the treatment of Mayo IIA olecranon fractures. Front. Surg. https://doi.org/10.3389/fsurg.2024.1500317 (2024).
Kuwahara, Y. et al. Locked tension band wiring: A modified technique for olecranon Fractures-A multicenter study comparing clinical outcomes and complications with conventional methods. INDIAN J. Orthop. 57, 2024–2030. https://doi.org/10.1007/s43465-023-01017-y (2023).
Midtgaard, K. S. et al. Tension band wiring versus precontoured plate fixation for 2-Part and multifragmented olecranon fractures: A prospective randomized trial. J. Bone Joint Surg. Am. 107, 1907–1917. https://doi.org/10.2106/JBJS.24.01461 (2025).
Zhao, Y. et al. The effect of ding’s screws and tension band wiring for treatment of olecranon fractures: a Biomechanical study. Sci. Rep. 14, 9999. https://doi.org/10.1038/s41598-024-60264-7 (2024).
Steadman, J. N., Stephens, A. R., Zhang, C., Presson, A. P. & Kazmers, N. H. Cost assessment of plating versus tension band wiring constructs for treating Mayo type 2A olecranon fractures. J. Hand Surg. Am. 47, 311–319. https://doi.org/10.1016/j.jhsa.2021.12.009 (2022).
Tan, B. Y. J., Pereira, M. J., Ng, J. W. & Kwek, E. B. K. The ideal implant for Mayo 2A olecranon fractures? An economic evaluation. J. Shoulder Elb. Surg. 29, 2347–2352. https://doi.org/10.1016/j.jse.2020.05.035 (2020).
DelSole, E. M., Pean, C. A., Tejwani, N. C. & Egol, K. A. Outcome after olecranon fracture repair: does construct type matter? Eur. J. Orthop. Surg. Traumatol. 26, 153–159. https://doi.org/10.1007/s00590-015-1724-0 (2015).
van der Linden, S. C., van Kampen, A. & Jaarsma, R. L. K-wire position in tension-band wiring technique affects stability of wires and long-term outcome in surgical treatment of olecranon fractures. J. Shoulder Elb. Surg. 21, 405–411. https://doi.org/10.1016/j.jse.2011.07.022 (2011).
Funding
This work was supported by the following funding sources: Science and Technology Project of Yinzhou District (Project No: 2022AS062); Medical and Health Science and Technology Project of Zhejiang Province (Project No: 2020KY892); Ningbo Public Welfare Science and Technology Program Project (Project No: 2024S173); Ningbo Clinical Research Center for Orthopedics, Sports Medicine & Rehabilitation (Project No:2024L004). The funders had no role in study design, data collection/analysis, decision to publish, or preparation of the manuscript.
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Zhang, J., Fang, Y., Zhuang, Y. et al. Biomechanical study on different internal fixation methods for treating Mayo type IIA olecranon fractures of the ulna. Sci Rep 16, 4947 (2026). https://doi.org/10.1038/s41598-026-35057-9
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-026-35057-9
