
Abstract
Cardiovascular disease (CVD) remains a leading global health burden, particularly in low- and middle-income countries. Tai Chi is a mind-body exercise with reported cardiovascular benefits, but its mechanistic pathways and comparative effects versus aerobic exercise are not well defined. To synthesize evidence on the effects and proposed mechanisms of Tai Chi on CVD risk factors and related biomarkers, compared with aerobic exercise or standard care. We conducted a systematic review and meta-analysis in accordance with PRISMA. We searched Google Scholar, PubMed, EBSCOhost MEDLINE, Scopus, ScienceDirect, and Web of Science from inception to October 2025. We included studies comparing Tai Chi with aerobic exercise and/or standard care and reporting outcomes related to CVD risk factors, functional capacity, mental health, or mechanistic biomarkers. Random-effects meta-analyses and subgroup analyses were performed where appropriate. Sixty studies were included (39 randomized controlled trials and 21 reviews). Tai Chi significantly reduced systolic blood pressure (MD -6.14 mmHg, 95% CI -8.44 to -3.84) and diastolic blood pressure (MD -3.45 mmHg, 95% CI -4.50 to -2.40). Improvements were also observed in HDL-C (SMD 0.43, 95% CI 0.16 to 0.69) and functional capacity (6-minute walk test, SMD 0.78, 95% CI 0.51 to 1.05). Reported psychosocial outcomes included reductions in fatigue and depression. Evidence mapping suggests Tai Chi may influence autonomic regulation and inflammatory/stress-related pathways (e.g., heart rate variability, IL-6, CRP), alongside improvements in lipid profile and functional performance. Tai Chi may offer clinically meaningful improvements in blood pressure, lipid-related outcomes, functional capacity, and psychosocial health. Mechanistic findings suggest potential effects on autonomic and inflammatory pathways, but comparative advantages over aerobic exercise and biomarker outcomes are supported largely by low- to moderate-certainty evidence and should be interpreted cautiously.
Similar content being viewed by others

Introduction
Cardiovascular diseases (CVD) remain the leading cause of mortality worldwide, responsible for nearly one-third of all deaths globally, with an estimated 17.8 million deaths attributed to CVD in 20171,2. The burden is disproportionately high in low- and middle-income countries, which account for 80% of CVD-related deaths, primarily due to limited access to preventive healthcare and effective treatment options3. Advancing age significantly elevates the risk of developing CVD, with projections suggesting that around 40.5% of the U.S. population will have some form of CVD by 2030, with those aged 65 and above being disproportionately affected4. Additionally, age-related increases in risk factors such as hypertension, high cholesterol, and diabetes further heighten the likelihood of cardiovascular events over a lifetime5. These trends underscore the urgent need for accessible, effective, and scalable interventions that address modifiable risk factors such as hypertension, physical inactivity, and dyslipidemia3,6,7,8. Therefore, addressing these modifiable risk factors is essential to reduce the growing prevalence of CVD worldwide.
To address these risk factors, several interventions are commonly recommended, including lifestyle modifications, aerobic exercise, isomeric exercise, and other physical activity-based approaches5,9,10,11. Among these, Tai Chi, which originated from traditional Chinese martial arts during the Ming and Qing dynasties, has garnered attention for its potential benefits to cardiovascular health12,13. Given that Tai Chi is a low-cost, easily accessible form of exercise, it holds particular promise for low- and middle-income countries, where healthcare resources are limited and more expensive interventions may not be feasible. The easy-to-perform and low-impact nature of Tai Chi makes it an affordable option for individuals in these regions to manage cardiovascular health without the need for expensive equipment or specialized training14. While initially developed as a form of self-defense, Tai Chi has evolved into a widely practiced mind-body exercise that integrates physical movement with mental focus15,16. Characterized by its slow, fluid movements, controlled breathing, and muscle relaxation, Tai Chi is often referred to as “moving meditation,” encapsulating its dual nature as both a physical and meditative practice17. This unique combination of attributes not only promotes cardiovascular fitness, balance, flexibility, and strength but also contributes to stress reduction, mental relaxation, and emotional regulation18,19,20. Mounting evidence supports Tai Chi’s positive impact on cardiovascular health. Research has demonstrated its ability to lower blood pressure, improve lipid profiles, and enhance overall cardiovascular function, particularly in middle-aged and elderly populations21. For instance, Tai Chi exercise training has been associated with improvements in glycemic control, aerobic capacity, and key biomarkers of heart function, making it an effective intervention for reducing the risk of hypertension, ischemic heart disease, and stroke22. Furthermore, its low-impact nature makes it suitable for individuals of all ages, particularly those who may be unable to engage in more strenuous forms of exercise, further enhancing its appeal as a cardiovascular intervention13,23.
Aerobic exercise, on the other hand, is widely recognized for its robust benefits in reducing CVD risk24. Aerobic exercise increases metabolic demand and enhances oxygen consumption in skeletal muscle. Activities such as cycling and swimming have been shown to improve cardiovascular health by lowering blood pressure, improving lipid profiles, enhancing microvascular function, and reducing oxidative stress25,26. Aerobic exercise is also closely linked to enhanced cardiovascular function, including increased VO2max, reduced body fat, and improved heart rate variability (HRV), which collectively contribute to a lower risk of sudden cardiac events4. However, aerobic exercise typically involves moderate to high-intensity activity, which demands significant cardiovascular effort and leads to elevated heart rates, distinguishing it from Tai Chi in terms of physiological effects and suitability for different populations27.
While both Tai Chi and aerobic exercise contribute to improved cardiovascular health, the mechanisms through which they reduce CVD risk may be quite different. This presents a critical question: What are the distinct and overlapping physiological and psychosocial pathways through which Tai Chi and aerobic exercise impact cardiovascular health, and how do these mechanisms compare in reducing CVD risk? Understanding the distinct mechanisms is essential for several reasons (Fig. 1). First, although both Tai Chi and aerobic exercise show general benefits in cardiovascular health, their effects may not be comparable across all CVD risk factors. For example, aerobic exercise is widely recognized for improving cardiovascular endurance and influencing traditional risk factors like lipid profiles and VO2max28,29,30. However, Tai Chi, with its mind-body integration, may offer additional benefits, such as enhancing parasympathetic activation, reducing systemic inflammation, and promoting stress reduction, which may not be fully captured by conventional measures of aerobic exercise31,32. This difference highlights the need to investigate the unique mechanisms of Tai Chi, especially in populations who cannot tolerate high-intensity exercise, or who may benefit from Tai Chi’s mind-body approach.
Existing reviews have primarily focused on the overall health benefits of Tai Chi without deeply exploring how the mechanisms of action between Tai Chi and aerobic exercise differ or overlap33,34,35. Understanding these mechanisms is critical for optimizing cardiovascular interventions for specific populations. For instance, while aerobic exercise directly enhances VO2max and lipid profiles, Tai Chi uniquely modulates biomarkers such as HRV and inflammatory markers like IL-6 and CRP through its integration of physical and mental exercises36,37,38. This review aims to fill this gap by providing a detailed, mechanism-focused comparison of Tai Chi and aerobic exercise, emphasizing key mediating biomarkers like HRV, inflammatory markers (e.g., TNF-α, IL-6, CRP), and lipid profiles (e.g., LDL-C, HDL-C), while also considering psychosocial factors such as stress reduction. By systematically analyzing these distinct physiological and psychosocial pathways, this review aims to offer a more nuanced understanding of how Tai Chi could complement or serve as an alternative to aerobic exercise for CVD prevention and management. Ultimately, we aim to provide evidence-based insights to support the clinical application of Tai Chi. Because it is scalable and holistic, Tai Chi may be particularly suitable for people with limited mobility or other barriers to traditional aerobic exercise.

Conceptual diagram of mechanisms of Tai Chi vs. Aerobic exercise in cardiovascular health.
Methods
This systematic review and meta-analysis was conducted and reported in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) and the Cochrane Handbook for Systematic Reviews of Interventions39,40. This protocol was registered at the International Prospective Register of Systematic Reviews (PROSPERO) as CRD42024620776. This study is a systematic review and meta-analysis to synthesize evidence from the literature and no patients were involved in the data collection.
Eligibility criteria (PICOS framework: population, intervention, comparison, outcome, study design)
-
1.
Population: Individuals of all ages, including adolescents, adults, and older adults, with or at risk for CVD, without restriction on gender or ethnicity.
-
2.
Intervention: Tai Chi interventions aimed at influencing cardiovascular risk factors, including those with varying durations and intensities focused on mind-body exercise.
-
3.
Comparison: Aerobic exercise interventions, placebo control, blank control, or no intervention.
-
4.
Outcomes: (1) Primary outcomes include changes in cardiovascular risk markers such as blood pressure, lipid profiles (e.g., LDL, HDL), inflammatory markers (e.g., IL-6, CRP), and HRV. (2) Secondary outcomes include improvements in physical fitness (e.g., VO2max), quality of life (QoL), mental health (e.g., reductions in stress, anxiety, or depression), and any adverse effects of the interventions.
-
5.
Study Design: (1) Primary controlled studies include randomized controlled trials (RCTs) were used for meta-analysis. Nonrandomized studies (NRSs) like cohort and case-control studies were included in descriptive synthesis. (2) Secondary studies included systematic reviews and meta-analyses. (3) Tertiary studies included umbrella reviews and evidence mapping reviews.
To ensure a comprehensive analysis, we included both primary experimental studies (RCTs and NRSs) and secondary/tertiary reviews (systematic reviews, meta-analyses, umbrella reviews, and evidence mapping). Primary studies were used to provide direct evidence on the effects of Tai Chi and aerobic exercise on cardiovascular outcomes, while secondary and tertiary reviews were incorporated to offer a broader synthesis of the available evidence, highlighting key mechanisms and contextualizing the effects observed in primary studies. This multi-tiered approach allowed for a richer understanding of the evidence base, capturing both specific study results and higher-level patterns across multiple studies.
Exclusion criteria
(1) Non-controlled studies, including case reports, case series, cross-sectional studies, and single-arm cohort studies. (2) Publications without eligible outcomes, such as abstracts or protocols without full study data. (3) Ongoing studies that have not yet provided results. (4) Studies focusing on clinical questions outside the scope of Tai Chi and cardiovascular disease. (5) Nonclinical research, such as in vitro or animal studies.
Search strategy
Search methods involved a comprehensive review of five databases—Google Scholar, PubMed, EBSCOhost MEDLINE, Scopus, ScienceDirect and Web of Science—up to October 2025. The search strategy used the following terms: (Tai Chi[Title/Abstract]) OR Tai Ji[Title/Abstract]) OR Taiji[Title/Abstract]) OR Taijiquan[Title/Abstract]) OR Tai Chi Chuan[Title/Abstract]) AND (Cardiovascular[Title/Abstract] OR CVD[Title/Abstract] OR Coronary Artery Disease[Title/Abstract] OR CAD[Title/Abstract] OR Heart Failure[Title/Abstract] OR Stroke[Title/Abstract] OR Myocardial Infarction[Title/Abstract] OR Peripheral Artery Disease[Title/Abstract] OR PAD[Title/Abstract] OR Hypertension[Title/Abstract] OR Arrhythmia[Title/Abstract] OR Atherosclerosis[Title/Abstract] OR Congestive Heart Failure[Title/Abstract] OR Blood Pressure[Title/Abstract] OR BP[Title/Abstract] OR Cholesterol[Title/Abstract] OR Low-Density Lipoprotein[Title/Abstract] OR LDL[Title/Abstract] OR High-Density Lipoprotein[Title/Abstract] OR HDL[Title/Abstract] OR Triglycerides[Title/Abstract] OR Blood Glucose[Title/Abstract] OR Body Mass Index[Title/Abstract] OR BMI[Title/Abstract] OR Waist Circumference[Title/Abstract] OR Heart Rate[Title/Abstract] OR HR[Title/Abstract] OR Heart Rate Variability[Title/Abstract] OR HRV[Title/Abstract] OR Ejection Fraction[Title/Abstract] OR Physical Activity Level[Title/Abstract] OR Cardiorespiratory Fitness[Title/Abstract] OR C-reactive Protein[Title/Abstract] OR CRP[Title/Abstract] OR Interleukin-6[Title/Abstract] OR IL-6[Title/Abstract] OR Endothelial Function[Title/8Abstract] OR Flow-Mediated Dilation[Title/Abstract] OR FMD[Title/Abstract] OR Vascular Function[Title/Abstract] OR Inflammatory[Title/Abstract] OR Lipid Profile[Title/Abstract]). The search was limited to articles published in English and Chinese. Cited reference search or trial registry search was performed.
Study selection and data extraction
Following the review procedures, two reviewers independently screened the titles and abstracts of all records retrieved via EndNote Desktop. Full-text reports were obtained for studies that seemed to meet the inclusion criteria. These reports were then independently evaluated by the two reviewers to determine their eligibility for inclusion or exclusion. Any disagreements were resolved through discussion, or by bringing in a third reviewer as an arbitrator if necessary. Data extraction from the included studies was also conducted independently by the two reviewers, with any discrepancies settled through discussion or by involving a third reviewer for arbitration. NRSs were excluded from the quantitative meta-analysis because they do not provide the necessary data to perform the calculations required for the meta-analysis. However, these studies were included in the qualitative synthesis to provide a broader understanding of the evidence base, especially since they offer valuable insights into mechanisms and outcomes that may not be fully addressed by RCTs. This approach allowed us to maintain the methodological rigor of the quantitative analysis while still considering a wider range of evidence for a more comprehensive interpretation.
Assessment of risk of bias
The risk of bias in the included studies was independently evaluated by two reviewers, with any disagreements addressed through discussion or by consulting a third reviewer for arbitration. For RCTs, the risk of bias was assessed using the RoB2 tool (Revised Tool for Risk of Bias in Randomized Trials)41. Since NRSs were not part of this review, the assessment focused solely on the RCTs. In addition to evaluating primary studies, the methodological quality of the systematic reviews included in the evidence map was critically appraised using the AMSTAR 2 (A Measurement Tool to Assess Systematic Reviews) tool42. AMSTAR 2 evaluates critical domains, including protocol registration, comprehensiveness of the search strategy, and assessment of risk of bias in individual studies, ensuring a robust evaluation of the reliability and rigor of the included reviews. This dual approach allowed for a comprehensive risk of bias assessment at both the study and review levels, ensuring that all sources of bias were accounted for.
Data synthesis methods
Data synthesis was performed using random-effects models in Review Manager (RevMan; Cochrane Collaboration) and R (R Foundation for Statistical Computing, Vienna, Austria), ensuring a more conservative interpretation of the results when studies with comparable interventions reported consistent outcomes. For continuous outcomes, mean differences (MD) or standardized mean differences (SMD) with 95% confidence intervals (CI) were calculated, depending on whether the same or different scales were used across studies43. Clinical heterogeneity was assessed based on differences in study design, intervention types, and participant characteristics, while statistical heterogeneity was evaluated using the chi-squared test (with a significance threshold of 0.05) and the I² statistic, ranging from 0% to 100%44. When sufficient studies were available and heterogeneity was observed, subgroup analyses were performed, considering factors such as intervention types, study design (RCTs only), follow-up durations, or diagnostic criteria of outcomes. Sensitivity analyses were also carried out to assess the robustness of the findings45. To explore potential sources of statistical heterogeneity, predefined subgroup analyses were conducted for key clinical and methodological factors, including (1) intervention duration, (2) frequency, (3) session length, (4) Tai Chi style (e.g., Yang style vs. other styles), and (5) baseline participant health status (e.g., healthy participants vs. those with hypertension, coronary artery disease, diabetes or other cardiometabolic conditions). Where sufficient studies were available, additional subgroups were examined according to follow-up duration and diagnostic criteria of the outcomes. Sensitivity analyses were carried out to assess the robustness of the pooled estimates by (1) omitting one study at a time (leave-one-out analysis), (2) excluding studies at high risk of bias, and (3) excluding studies with extremely short intervention duration or outlying effect sizes identified by influence diagnostics. All subgroup and sensitivity analyses were conducted in R, and results are reported in the main text and Supplementary Material.
Both intention-to-treat (ITT) and modified intention-to-treat (mITT) approaches were considered to ensure robust analysis and reduce the risk of bias. ITT ensured that all participants were analyzed based on their initial group assignments, regardless of completion, maintaining randomization benefits. mITT, applied in studies where participants received at least one session of the intervention, allowed a more focused assessment of intervention effects46. To prevent double-counting of data, primary studies included in the meta-analysis were not double-counted from secondary or tertiary reviews. Data from secondary reviews (systematic reviews and meta-analyses) were synthesized qualitatively to provide a broad overview of mechanisms and outcomes. When studies from secondary reviews overlapped with primary studies in our meta-analysis, we ensured that these studies were only counted once in the statistical analysis. The evidence from systematic reviews and meta-analyses was used to map broader mechanistic pathways and guide further interpretation, while the quantitative meta-analysis relied solely on data from primary studies.
Assessment of publication bias
Potential publication bias (small-study effects) was examined for outcomes that included 10 or more studies in the meta-analysis47. For each eligible outcome, we constructed funnel plots of the study-specific effect size against its standard error and visually inspected them for asymmetry. Visual assessment was complemented by formal statistical tests using Egger’s regression test and Begg’s rank correlation test to quantify small-study effects48. The corresponding test statistics (Egger’s z and p value; Begg’s τ and p value) are presented on the funnel plots in Supplementary Figs. 1–25. Where evidence of asymmetry was observed, we considered potential explanations such as publication bias, selective reporting, or genuine heterogeneity related to study size when interpreting the results.
Assessment of certainty
The certainty of evidence was evaluated using the GRADE approach (Grading of Recommendations, Assessment, Development, and Evaluation)49. Two reviewers independently assessed the quality of the evidence across several domains, including study design, risk of bias, consistency of results, directness of the evidence, and precision of the estimates. The certainty of the evidence was categorized as high, moderate, low, or very low. Any disagreements between the reviewers were resolved through discussion or by consulting a third reviewer.
Results
Study selection
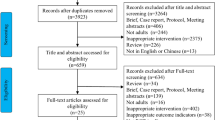
A total of 3,411 records were identified through searches in PubMed, Web of Science, and EBSCOhost MEDLINE, along with 58 records from citation searching (Fig. 2). After removing 1,455 duplicate entries, 1956 records underwent title and abstract screening. Of these, 1362 records were excluded for being irrelevant (n = 472), involving inapplicable interventions (n = 395), or lacking cardiovascular outcomes (n = 495). Subsequently, 594 full-text reports were assessed for eligibility, with 501 being excluded due to incomplete data (n = 149), methodological limitations (n = 96), or insufficient follow-up duration (n = 201). Ultimately, 60 studies met the inclusion criteria and were incorporated into the systematic review and meta-analysis.

PRISMA Flow Diagram of Study Selection (39 RCTs contributed data to the quantitative meta-analyses of clinical outcomes, 60 studies (39 RCTs and 21 mechanistic articles) contributed to the qualitative synthesis of mechanistic pathways and biomarkers).
Study characteristics
The systematic review included a total of 60 studies, comprising 39 experimental studies and 21 review articles (Table 1 and Table2). The experimental studies were predominantly RCTs, designed to evaluate the effects of Tai Chi on cardiovascular health and related outcomes. These interventions incorporated diverse forms of Tai Chi, including Yang style, Sun style, 24-form, and 32-form Tai Chi. Control groups were typically assigned to no intervention, usual activities, aerobic exercises, or standard care, enabling comparative evaluations. Sample sizes varied substantially, ranging from small-scale studies with fewer than 30 participants to larger trials exceeding 200 participants. The included studies targeted diverse populations, such as individuals with primary hypertension, type 2 diabetes, coronary artery disease, or stroke recovery, as well as other cardiovascular or metabolic conditions. Participants were primarily older adults, with mean ages spanning from early adulthood to elderly populations. Geographically, the studies were conducted across multiple countries, including China, the United States, and other regions, reflecting the global interest in Tai Chi research. The primary outcomes assessed across the studies included blood pressure (SBP and DBP), blood lipids, blood glucose, cardiovascular fitness, and psychological measures such as stress and depression. Secondary outcomes encompassed functional metrics such as walking distance, balance, and exercise adherence. The included review articles further provided comprehensive insights into Tai Chi’s mechanisms and its clinical applications. This diversity in study design, populations, and outcome measures establishes a robust foundation for the subsequent meta-analysis and evidence mapping.
Risk of bias assessment
The risk of bias was systematically assessed for both the experimental studies and the systematic reviews included in this analysis, using the ROB2 tool41 and AMSTAR42, respectively. Among the 39 experimental studies, the majority demonstrated a low risk of bias in key domains such as randomization processes and outcome measurement12,50,51,52,53,54,55. However, certain studies exhibited methodological limitations, particularly in allocation concealment and blinding of assessors, leading to a moderate risk of bias in these areas14,16,34,35,56,57,58,59,60,61,62,63,64,65,66,67,68,69,70,71,72,73,74,75,76,77,78,79,80,81,82,83. Overall, the experimental studies were predominantly rated as having low to moderate risk of bias (Fig. 3). For the 21 systematic reviews, AMSTAR assessments indicated moderate methodological quality overall, with strengths including comprehensive literature searches, dual data extraction, and consideration of publication bias (Fig. 4). Common limitations involved incomplete assessment of funding sources and insufficient reporting of conflicts of interest. While most reviews were rated as moderate in quality84,85,86,87,88,89,90,91,92,93,94,95,96,97,98,99,100,101, one achieved a high methodological rating102. Graphical summaries further illustrate the distribution of risk across key domains for both the experimental studies and systematic reviews, highlighting the robustness of the included evidence. These findings underscore the methodological rigor of the included studies and reviews, providing a strong foundation for the subsequent meta-analysis and evidence mapping (Fig. 4).

Risk of bias assessment. Note: D1: Randomization process D2: Deviations from the intended interventions D3: Missing outcome data D4: Measurement of the outcome D5: Selection of the reported result.

Heatmap of methodological quality assessment using the AMSTAR 2 Tool. Note: This figure evaluates systematic reviews using the AMSTAR 2 tool. Columns 1–16 correspond to criteria: (1) Inclusion of PICO components. (2) Predefined methods and protocol deviations. (3) Justification for study designs. (4) Comprehensive literature search. (5) Duplicate study selection. (6) Duplicate data extraction. (7) List and reasons for excluded studies. (8) Description of included studies. (9) Risk of bias assessment. (10) Reporting of funding sources. 11. Statistical methods for meta-analysis. 12. Impact of bias on meta-analysis. 13. Bias consideration in interpretation. 14. Heterogeneity discussion. 15. Publication bias investigation. 16. Conflicts of interest and funding. Reviews were rated as “Yes,” “Partial Yes,” or “No,” with overall confidence graded to ensure methodological rigor.
Meta-analysis results
Quantitative results
Effects of Tai Chi on SBP and DBP
The meta-analysis demonstrates that Tai Chi is associated with statistically significant, but heterogeneous, reductions in both SBP (Supplementary Fig. 1) and DBP (Supplementary Fig. 1). For SBP, 33 studies involving 1,560 participants in the experimental group and 1,509 in the control group revealed a pooled mean difference of −6.14 mmHg (95% CI: −8.44 to −3.84, p < 0.001), with high heterogeneity (I²= 94%). However, the very high between-study heterogeneity, much of which remained unexplained after subgroup analyses, indicates that this pooled effect should be interpreted with caution. For DBP, 32 studies with 1,591 and 1,555 participants in the experimental and control groups, respectively, showed a pooled mean difference of −3.45 mmHg (95% CI: −4.50 to −2.40, p < 0.001), also with high heterogeneity (I²= 89%). Similarly, the high residual heterogeneity limits the certainty of this pooled estimate, despite the statistically significant reduction. Taken together, these findings suggest that Tai Chi may be an effective intervention for blood pressure reduction, but the magnitude and consistency of the effect are uncertain and should be interpreted cautiously in light of the substantial residual heterogeneity, which also highlights the need for more standardized protocols and better-reported trials in future research. Subgroup analyses were further conducted (SBP: Supplementary Figs. 52a-f; DBP: Supplementary Figs. 53a-f) to explore potential sources of the substantial heterogeneity observed across outcomes. Although these subgroup analyses helped to explore potential sources of heterogeneity, they did not fully account for it. As the number of studies within several subgroups was small and reporting of intervention characteristics was inconsistent, these subgroup findings should be interpreted cautiously and considered exploratory rather than definitive.
Effects of Tai Chi on 6MWT
The meta-analysis evaluates the effects of Tai Chi on the 6-minute walk test (6MWT), reflecting physical endurance (Supplementary Fig. 3). Across 31 studies with 984 participants in the experimental group and 1,008 in the control group, Tai Chi significantly improved 6MWT performance with a SMD of 0.78 (95% CI: 0.51 to 1.05, p < 0.001). High heterogeneity was observed (I²= 86%, Tau² = 0.45), indicating variability in study characteristics and interventions. Most studies reported moderate to large improvements, with several showing statistically significant gains. These findings suggest Tai Chi enhances physical endurance, as measured by 6MWT, but the heterogeneity highlights the need for consistent methodology in future studies.
Effects of Tai Chi on RHR
The meta-analysis evaluates the effects of Tai Chi on RHR (Supplementary Fig. 4). Based on 15 studies involving 542 participants in the experimental group and 559 in the control group, Tai Chi significantly reduced RHR, with a SMD of −0.57 (95% CI: −0.93 to −0.21, p < 0.05). High heterogeneity was observed (I² = 86%, Tau² = 0.42), indicating variability in study designs, participant populations, or intervention durations. While most studies reported reductions in RHR, the effect size varied, with several showing statistically significant decreases. These findings suggest that Tai Chi effectively lowers RHR, indicating improved autonomic and cardiovascular function.
Effects of Tai Chi on HDL-C
The meta-analysis evaluated the effects of Tai Chi on HDL-C (Supplementary Fig. 5). Across 18 studies including 842 participants in the experimental group and 835 in the control group, Tai Chi was associated with a statistically significant improvement in HDL-C, with a pooled standardized mean difference (SMD) of 0.43 (95% CI: 0.16 to 0.69, p = 0.002). Using the average SD for HDL-C reported in the included trials (approximately 10–12 mg/dL), this SMD corresponds to an absolute increase of roughly 4–5 mg/dL, representing a small-to-moderate but potentially clinically relevant improvement in HDL-C levels. Heterogeneity was moderate to high (I² = 84%, τ² = 0.25), indicating considerable variability in effect sizes across studies, likely reflecting differences in study design, participant characteristics, and Tai Chi protocols. While most individual trials showed favorable effects. Overall, these findings suggest that Tai Chi may beneficially modify HDL-C, although the magnitude and consistency of the effect should be interpreted with caution in light of the substantial between-study heterogeneity.
Effects of Tai Chi on LDL-C
The meta-analysis evaluates the effects of Tai Chi on LDL-C (Supplementary Fig. 6). Based on 16 studies with 725 participants in the experimental group and 718 in the control group, Tai Chi significantly reduced LDL-C levels, with a SMD of −0.28 (95% CI: −0.52 to −0.04, p < 0.05). Moderate heterogeneity was observed (I²= 77%, Tau²= 0.17), reflecting variability in study populations, intervention protocols, and duration. While most studies reported reductions in LDL-C, the effect sizes varied, with some studies showing minimal or no effects. These findings suggest that Tai Chi has a modest but significant impact on lowering LDL-C, contributing to its potential role in cardiovascular risk reduction.
Effects of Tai Chi on FBG
The forest plot illustrates the meta-analysis results evaluating the effect of Tai Chi on FBG levels (Supplementary Fig. 7). Across 22 studies, the pooled MD in FBG between experimental and control groups was − 0.41 mmol/L (95% CI: −0.76 to −0.05, p < 0.05) under a random-effects model. The findings suggest a statistically significant reduction in FBG favoring the Tai Chi intervention. However, substantial heterogeneity was observed (I² = 94%, p < 0.00001), indicating variability among studies. Despite this, the overall effect supports the beneficial role of Tai Chi in lowering FBG levels compared to controls.
Effects of Tai Chi on TC
The forest plot evaluates the impact of Tai Chi on TC levels (Supplementary Fig. 8). Based on the meta-analysis of 19 studies, the pooled SMD was − 0.28 (95% CI: −0.52 to −0.04, p < 0.05), suggesting a statistically significant reduction in TC levels in favor of the Tai Chi intervention. Despite this favorable outcome, substantial heterogeneity was observed (I²= 77%, p < 0.00001), indicating variability across studies. These findings suggest that Tai Chi may have a beneficial effect on TC regulation.
Effects of Tai Chi on HbA1c
The forest plot examines the effects of Tai Chi on HbA1c levels (Supplementary Fig. 9). The meta-analysis of 18 studies reveals a pooled MD of −0.84% (95% CI: −1.66 to −0.02, p = 0.05), indicating a statistically significant reduction in HbA1c favoring Tai Chi interventions. However, the heterogeneity among studies is extremely high (I² = 99%, p < 0.00001), suggesting substantial variability in the intervention effects across studies. These results support the potential of Tai Chi in improving glycemic control as reflected by HbA1c.
Effects of Tai Chi on WC
The forest plot illustrates the effects of Tai Chi on WC across six studies included in the meta-analysis (Supplementary Fig. 10). The pooled results, calculated using a random-effects model, show a MD of −1.15 cm (95% CI: −2.32 to 0.03, p < 0.1), favoring the experimental group but without reaching statistical significance. The heterogeneity among studies was moderate (I² = 52%), indicating variability in study outcomes. Individual studies revealed mixed results, with some showing reductions in WC in the experimental group, while others showed minimal or no differences. Overall, the findings suggest a potential trend toward Tai Chi’s effectiveness in reducing WC, though further studies are warranted to confirm these effects.
Effects of Tai Chi on fat-free mass
The forest plot presents the effects of Tai Chi on fat-free mass based on nine studies analyzed using a random-effects model (Supplementary Fig. 11). The pooled SMD is 0.18 (95% CI: −0.03 to 0.40, p = 0.10), suggesting a slight improvement in fat-free mass in the experimental group, though the result is not statistically significant. Heterogeneity among the studies was low (I²= 23%), indicating relatively consistent findings across studies. While several individual studies show positive effects of Tai Chi on fat-free mass, others report minimal or no differences between groups. Overall, the analysis indicates a trend toward a beneficial impact of Tai Chi on fat-free mass.
Effects of Tai Chi on IL-6
The forest plot summarizes the effects of Tai Chi on IL-6 levels across 11 studies using a random-effects model (Supplementary Fig. 12). The pooled standardized mean difference was − 0.28 (95% CI: −0.81 to 0.25, p > 0.10), indicating no statistically significant difference in IL-6 between Tai Chi and control groups. Heterogeneity was high (I² = 87%), reflecting substantial variability in effect estimates across studies, likely related to differences in populations, baseline inflammatory status, and intervention protocols. Although some individual trials reported reductions in IL-6 with Tai Chi, others showed minimal or opposite changes. Taken together, these results are inconclusive and do not allow firm conclusions about the impact of Tai Chi on IL-6, underscoring the need for larger, better-standardized trials focused on inflammatory outcomes.
Effects of Tai Chi on BMI
The forest plot depicts the effects of Tai Chi on BMI across 15 studies analyzed using a random-effects model (Supplementary Fig. 13). The pooled mean difference was − 0.22 (95% CI: −0.70 to 0.26, p > 0.10), indicating no statistically significant difference in BMI between Tai Chi and control groups. Heterogeneity was very high (I² = 95%), reflecting substantial variability in effect estimates across studies, likely due to differences in populations, baseline weight status, and intervention characteristics. Although some individual trials reported modest reductions in BMI in favor of Tai Chi, others showed minimal or opposite effects. Overall, the current evidence does not support a consistent or conclusive effect of Tai Chi on BMI, and larger, well-designed trials are needed to clarify its impact on body weight and adiposity.
Effects of Tai Chi on weight
The forest plot summarizes the effects of Tai Chi on body weight across seven studies analyzed using a random-effects model (Supplementary Fig. 14). The pooled MD is −0.21 (95% CI: −1.21 to 0.79, p>0.1), indicating no statistically significant reduction in body weight in the experimental group compared to the control group. Heterogeneity was negligible (I² = 0%), suggesting consistent results across the studies. While individual studies demonstrated varying results, most showed little to no impact of Tai Chi on body weight. These findings suggest that Tai Chi does not significantly influence body weight, highlighting the need for further research to explore its potential effects in different populations.
Effects of Tai Chi on VO2max
The forest plot summarizes the effects of Tai Chi on VO2max across 13 studies using a random-effects model (Supplementary Fig. 15). The pooled standardized mean difference was 0.04 (95% CI: −0.48 to 0.57, p > 0.10), indicating no statistically significant difference in VO₂max between Tai Chi and control groups. Heterogeneity was high (I² = 88%), reflecting substantial variability in effect estimates across studies, likely related to differences in participant characteristics, baseline fitness levels, and intervention intensity or duration. Although some individual trials reported improvements in VO2max with Tai Chi, others showed minimal or opposite effects. Overall, the available evidence does not demonstrate a consistent or conclusive impact of Tai Chi on VO2max, and further rigorously designed studies are needed to clarify its effects on cardiorespiratory fitness.
Effects of Tai Chi on fatigue
The forest plot summarizes the effects of Tai Chi on fatigue across eight studies (Supplementary Fig. 16). The pooled standardized mean difference was − 1.46 (95% CI: −2.13 to −0.79, p < 0.001), indicating a large and statistically significant reduction in fatigue in the Tai Chi groups compared with controls. An SMD of this magnitude corresponds to an improvement of more than one standard deviation on commonly used fatigue scales, suggesting a substantial, clinically important decrease in perceived fatigue. Heterogeneity was high (I² = 92%, τ² = 0.88), reflecting considerable variability in effect sizes across studies, likely due to differences in patient populations, baseline fatigue severity, and intervention protocols. Nevertheless, most individual trials favored Tai Chi, with several showing particularly pronounced benefits. Overall, these findings suggest that Tai Chi may produce marked improvements in fatigue, although the variability between studies warrants cautious interpretation.
Effects of Tai Chi on depression
The forest plot illustrates the impact of Tai Chi on depressive symptoms across 22 studies (Supplementary Fig. 17). The pooled standardized mean difference was − 0.46 (95% CI: −0.81 to −0.12, p = 0.008), indicating a small-to-moderate but statistically significant reduction in depression among participants practicing Tai Chi compared with controls. Using the typical standard deviations reported across the included trials (≈ 7–8 points on commonly used depression scales), this effect size corresponds roughly to a 3–4 point reduction in depressive symptom scores, which is likely to be clinically noticeable for many patients. Heterogeneity was substantial (I² = 88%, τ² = 0.56), reflecting considerable variability in effect sizes that may be related to differences in populations, outcome measures, and intervention protocols. While several studies reported pronounced benefits, others showed smaller or negligible effects, and a few favored the control condition. Overall, despite this variability, the aggregated evidence suggests that Tai Chi may meaningfully alleviate depressive symptoms, though the magnitude and consistency of benefit should be interpreted cautiously.
Effects of Tai Chi on pain
The forest plot evaluates the effect of Tai Chi on pain across 28 studies (Supplementary Fig. 18). The pooled standardized mean difference was − 0.48 (95% CI: −0.84 to −0.12, p = 0.009), indicating a small-to-moderate but statistically significant reduction in pain in the Tai Chi groups compared with controls. Assuming a typical standard deviation of about 2 points on commonly used 0–10 pain scales in the included trials, this effect size corresponds roughly to a 1-point decrease in pain intensity, which is likely to be clinically noticeable for many patients. Heterogeneity was high (I² = 93%, τ² = 0.85), reflecting substantial variability in effect sizes across studies, probably related to differences in patient populations, pain conditions, and Tai Chi protocols. Several trials showed particularly large improvements35,96, whereas other reported more modest effects52. Overall, despite the heterogeneity, the aggregated evidence suggests that Tai Chi can meaningfully alleviate pain, although the magnitude and consistency of benefit should be interpreted with caution.
Effects of Tai Chi on mental health
The forest plot analyzes the effects of Tai Chi on mental health, summarizing data from six studies (Supplementary Fig. 19). The pooled SMD = 0.88 (95% CI: 0.12 to 1.64, p < 0.05) suggests a significant positive impact of Tai Chi on mental health, with a moderate effect size favoring the experimental group. High heterogeneity (I² = 89%) indicates substantial variability across studies. Individual results vary widely, with a study showing a pronounced benefit (SMD = 3.22), while others report negligible effects51. These findings provide evidence supporting Tai Chi as a beneficial intervention for improving mental health outcomes.
Effects of Tai Chi on anxiety
The forest plot evaluates the effects of Tai Chi on anxiety across 11 studies, comparing experimental and control groups (Supplementary Fig. 20). The pooled SMD = −0.57 (95% CI: −1.25 to 0.11, p = 0.10) suggests a trend toward reduced anxiety in the Tai Chi group, although the result is not statistically significant. Substantial heterogeneity (I² = 95%) indicates considerable variability among the studies. Some studies report significant reductions in anxiety levels, while others show limited or no effects. Overall, while the data suggest potential benefits, further research is needed to confirm Tai Chi’s efficacy in reducing anxiety.
Effects of Tai Chi on sleep quality
The forest plot presents the effects of Tai Chi on sleep quality across nine studies (Supplementary Fig. 21). The pooled SMD = −0.30 (95% CI: −0.66 to 0.06, p>0.05) indicates a trend toward improved sleep quality in the Tai Chi group, though the result is not statistically significant. Moderate heterogeneity (I²= 77%) suggests variation among the studies. Some studies report significant improvements in sleep quality.
Effects of Tai Chi on stress
The forest plot examines the effects of Tai Chi on stress levels across five studies (Supplementary Fig. 22). The pooled SMD = −0.57 (95% CI: −1.34 to 0.19, p>0.05) suggests a trend toward stress reduction in the Tai Chi group, though the results are not statistically significant. High heterogeneity (I² = 88%) reflects considerable variability among the included studies. Individual results vary, with Jo Lynne Robins (2016)68demonstrating a significant reduction in stress, while others, such as Shuting Wang (2022), report negligible effects34. These findings imply that the impact of Tai Chi on stress may depend on specific study conditions or participant characteristics.
Effects of Tai Chi on general health
The forest plot evaluates the effects of Tai Chi on general health across nine studies (Supplementary Fig. 23). The pooled SMD = −0.25 (95% CI: −0.61 to 0.11, p>0.05) indicates a slight trend toward improvement in general health within the Tai Chi group, though this result is not statistically significant. Moderate heterogeneity (I² = 66%) suggests variation among the studies. Individual outcomes range from substantial benefits79, to negligible or no effect103.
Effects of Tai Chi on physical functioning
The forest plot summarizes the effects of Tai Chi on physical functioning across eight studies (Supplementary Fig. 24). The pooled SMD = 0.23 (95% CI: −0.22 to 0.68, p>0.05) suggests a small and statistically non-significant improvement in physical functioning in the Tai Chi group compared to the control group. Moderate heterogeneity (I² = 75%) indicates variability across studies. While some studies report notable improvements, others, including Campo (2013) and Leona Yuen-ling Leung (2019), show negligible or no effects52,103. These findings suggest that Tai Chi may benefit physical functioning under specific conditions, though the overall evidence remains inconclusive.
Effects of Tai Chi on vitality
The forest plot examines the effects of Tai Chi on vitality across seven studies (Supplementary Fig. 25). The pooled SMD = 0.28 (95% CI: −0.25 to 0.81, p>0.05) indicates a small, statistically non-significant improvement in vitality in the Tai Chi group compared to controls. Substantial heterogeneity (I² = 80%) highlights variability among the included studies. Individual results are mixed, with studies showing a notable positive effect, while others, such as Campo (2013) and Lam (2004), report negligible changes51,103. These findings suggest that while Tai Chi may have some potential to enhance vitality, the evidence is not yet definitive.
Publication bias and sensitivity analyses and
Based on the assessment of publication bias using funnel plots and formal tests (Supplementary Figs. 26–50), the robustness of the evidence varied across outcomes. For well-studied endpoints such as SBP and DBP, the funnel plots were largely symmetrical, suggesting reasonably consistent reporting and a low likelihood of substantial publication bias. In contrast, for outcomes with fewer contributing studies-such as BMI, VO2max, and inflammatory markers (e.g., IL-6)-funnel plot asymmetry and indications of small-study effects suggested possible publication or selective reporting bias, with smaller trials tending to report larger effect sizes. These patterns imply that, while the evidence base for some outcomes is relatively stable, estimates for others should be interpreted with greater caution due to potential bias and methodological variability.
Leave-one-out sensitivity analyses were conducted for meta-analyses with a sufficient number of trials to examine the influence of each individual study on the pooled estimates (Supplementary Fig. 51). Sequential exclusion of single studies resulted in only minimal changes in the magnitude and direction of the pooled standardized mean differences, and all re-estimated effects remained close to the overall summary estimates with overlapping 95% confidence intervals. No individual trial meaningfully altered the statistical significance of the pooled effects or markedly reduced heterogeneity, indicating that the meta-analytic conclusions are robust and not driven by any single study. Taken together, the sensitivity analyses and publication-bias assessments suggest that the primary findings are generally stable and are unlikely to be substantially influenced by either individual studies or selective publication.
Qualitative results
Aerobic exercise pathway
Tai Chi, as a low-to-moderate-intensity aerobic exercise, offers significant cardiovascular benefits through multiple physiological and biochemical pathways. One of its primary mechanisms lies in the improvement of lipid metabolism80,81,101. Tai Chi has been shown to reduce TG and LDL-C while increasing HDL-C74. These changes extend to advanced lipid markers, including apolipoprotein B (apo B) and LDL particle size, shifting the lipid profile towards less atherogenic forms34. Such modifications play a critical role in reducing the risk of atherosclerosis and coronary artery disease.
Another key benefit of Tai Chi is its ability to enhance cardiovascular fitness. Regular practice improves parameters such as VO2max, stroke volume, and cardiac output, which collectively enhance myocardial oxygen supply and overall cardiac function54,78,79. Functional capacity also sees substantial improvement, as evidenced by increased walking distances in the 6MWT, reflecting better aerobic endurance and cardiorespiratory efficiency76. This is further supported by the improvement in peripheral blood flow and vascular elasticity, which Tai Chi achieves through rhythmic, low-impact movements that promote circulation and reduce systemic vascular resistance.
Tai Chi also demonstrates anti-inflammatory effects that significantly contribute to cardiovascular health. The practice reduces systemic inflammation by lowering markers such as C-reactive protein, IL-6, and tumor necrosis factor-alpha (TNF-α)75. These anti-inflammatory changes are comparable to those observed in traditional aerobic exercises and are instrumental in mitigating cardiovascular disease progression74. Additionally, Tai Chi effectively lowers both systolic and diastolic blood pressure, primarily through enhanced vascular endothelial function and arterial compliance70. Improvements in baroreflex sensitivity (BRS) and autonomic regulation further contribute to stable blood pressure control, highlighting Tai Chi’s impact on reducing hypertension-related risks69.
Metabolic health also benefits significantly from Tai Chi. Regular practice promotes reductions in visceral fat, body weight, and waist circumference, addressing key markers of metabolic syndrome68. Enhanced fat oxidation and glycemic control, indicated by reduced FBG and HbA1c levels, further alleviate cardiovascular risk factors67. This metabolic regulation is complemented by Tai Chi’s impact on the autonomic nervous system. By improving HRV, Tai Chi enhances parasympathetic activity and reduces sympathetic dominance, creating a balanced autonomic response that lowers cardiovascular strain and prevents arrhythmias66.
Functional and aerobic capacity are likewise improved through Tai Chi. Participants often experience higher VO2max levels, increased performance in the two-minute step test, and enhanced lower-body strength and balance13. These outcomes not only support cardiovascular health but also reduce the risks associated with physical inactivity and sedentary behavior65. Moreover, Tai Chi improves microvascular reactivity, leading to better oxygen and nutrient delivery to peripheral tissues. This improvement in microvascular function decreases peripheral resistance and supports vascular compliance, which are vital for managing hypertension and reducing cardiovascular strain64.
Tai Chi’s low-impact nature minimizes stress on the cardiovascular system while enhancing oxygen consumption efficiency16. Its slow, deliberate movements, combined with rhythmic breathing, improve thoracic expansion, respiratory function, and systemic circulation63. These benefits reduce myocardial oxygen demand and improve coronary perfusion, contributing to overall cardiac efficiency104. Tai Chi’s unique integration of aerobic, resistance, and balance training components makes it an effective intervention for preventing and managing CVD61. It addresses systemic inflammation, lipid metabolism, functional capacity, and autonomic regulation, presenting a holistic approach to cardiovascular health.
Mind-body exercise pathway
Tai Chi, as a mind-body exercise, provides a holistic mechanism of action in the prevention and management of CVD by integrating physical movement, mindfulness, and controlled breathing60. Central to its benefits is the regulation of the autonomic nervous system, where Tai Chi enhances parasympathetic activity and suppresses sympathetic overdrive52. This leads to improved HRV, reduced systemic inflammation, and lower stress-induced hormonal activity, such as cortisol secretion51. These changes collectively support cardiovascular health by mitigating stress-related risk factors like hypertension, tachycardia, and endothelial dysfunction59. Furthermore, the meditative aspects of Tai Chi reduce psychological stress and anxiety, enhancing emotional well-being and QoL58. This alleviation of stress-induced physiological responses is critical in lowering inflammatory markers such as IL-6 and TNF-α, which are implicated in the pathophysiology of atherosclerosis and other cardiovascular conditions14.
The practice of Tai Chi also fosters improvements in sleep quality, as demonstrated by significant reductions in PSQI scores57. Enhanced sleep contributes to cardiovascular repair and regulation by promoting parasympathetic dominance and reducing nocturnal sympathetic activity56. Moreover, Tai Chi’s impact on psychological health extends to alleviating symptoms of depression and anxiety, which are known contributors to CVD risk50. Through mechanisms linked to neuro-hormonal balance and mindfulness, participants experience significant emotional stabilization, improved self-efficacy, and adherence to lifestyle modifications, which are essential for long-term cardiovascular benefits50. Enhanced QoL scores across multiple domains, such as physical, social, and emotional well-being, underscore Tai Chi’s ability to address the multifaceted challenges of chronic disease management56.
Tai Chi also demonstrates significant cognitive and neural benefits, as evidenced by improved performance in tests of executive function and working memory, alongside increased P300 wave amplitudes57. These cognitive gains enhance autonomic regulation, supporting vascular and metabolic health. Tai Chi’s slow, deliberate movements also improve balance, neuromotor coordination, and postural stability, reducing fall risks and the secondary stress associated with injury58. This physical engagement, coupled with mindfulness, further amplifies cardiovascular resilience by improving blood flow regulation and functional capacity59. Additionally, Tai Chi promotes endocrine regulation, reducing fasting blood glucose levels and balancing the hypothalamic-pituitary-adrenal axis, which mitigates metabolic syndrome risks and supports vascular function51.
Overall, Tai Chi’s integration of controlled breathing, meditative focus, and physical movement supports a synergistic pathway for cardiovascular health. By reducing systemic stress, inflammation, and metabolic strain while enhancing psychological and physical resilience, Tai Chi offers an accessible and comprehensive intervention52. Its ability to improve emotional stability, sleep quality, autonomic balance, and overall QoL demonstrates its unique role as a mind-body exercise in reducing cardiovascular disease risk and promoting holistic health.
Dual pathways synergy
Tai Chi uniquely integrates aerobic exercise and mindfulness, creating a synergistic mechanism that enhances cardiovascular health through interconnected physical and psychological pathways. This dual action offers comprehensive benefits for CVD prevention and management by addressing molecular, physiological, and behavioral dimensions105. On a molecular level, Tai Chi regulates lipid metabolism, improving both the quantity and quality of lipoproteins, such as increasing large, buoyant LDL particles, which are less atherogenic106. Furthermore, it modulates inflammatory pathways by reducing serum miR-126 levels and inactivating the MAPK/ERK signaling cascade, which mitigates atherogenesis and inflammation60. These molecular adaptations are complemented by a reduction in epicardial adipose tissue volume (EATV) and enhanced nitric oxide bioavailability, contributing to improved vascular health and endothelial function107.
Physiologically, Tai Chi strengthens peripheral muscles, enhancing both isometric and isokinetic strength, while optimizing central cardiovascular markers such as blood pressure, heart rate, and NT-proBNP levels108. This dual impact is reflected in improved aerobic capacity, balance, and coordination, reducing fall risks and promoting sustained physical activity in aging populations61. Moreover, Tai Chi fosters autonomic balance, as evidenced by enhanced HRV parameters and improved baroreflex sensitivity86. These adaptations indicate a shift toward greater vagal tone and reduced sympathetic dominance, which are crucial for cardiovascular resilience104. The mindfulness component of Tai Chi amplifies these effects by reducing oxidative stress and systemic inflammation while promoting emotional stability and neurovascular regulation, creating a robust foundation for long-term cardiovascular health109.
Behaviorally, Tai Chi encourages adherence to healthier lifestyles through its low-intensity, accessible, and adaptable nature. High adherence rates among elderly and chronically ill patients highlight its practicality as a sustainable exercise63. Tai Chi not only supports regular physical activity but also facilitates behavioral changes, such as improved dietary patterns and stress management52. This holistic approach amplifies its cardiovascular benefits by promoting long-term lifestyle modifications and reducing psychological stressors that contribute to cardiovascular strain110. These benefits extend to improved emotional well-being, as Tai Chi alleviates symptoms of depression and anxiety, enhancing overall quality of life and resilience against chronic stress110.
Tai Chi’s comprehensive impact on cardiometabolic health is evident in its ability to reduce systolic and diastolic blood pressure, improve glucose metabolism, and lower inflammatory markers65. The integration of physical and mental components leads to improved cognitive function, enhanced sleep quality, and reduced fatigue, creating a virtuous cycle of health benefits16. Additionally, its ability to improve baroreflex-mediated heart rate control and vascular elasticity positions it as an effective adjunct to traditional cardiac rehabilitation programs64. The low-impact nature of Tai Chi ensures its feasibility and safety, even for populations with limited exercise tolerance or multiple comorbidities, making it a practical intervention for long-term cardiovascular health maintenance13.
Overall, the synergistic interplay between Tai Chi’s aerobic and mindfulness elements creates a uniquely effective approach to cardiovascular health66. This dual mechanism enhances both physiological and psychological resilience, reduces systemic inflammation, and promotes sustained functional improvements67. The sustained benefits of Tai Chi, such as improved cytokine profiles, reduced oxidative stress, and greater adherence to healthy behaviors, position it as a valuable non-pharmacological strategy for preventing and managing cardiovascular diseases68. With its accessibility, adaptability, and evidence-backed effectiveness, Tai Chi provides a holistic, sustainable framework for improving cardiovascular and overall health.
Evidence mapping
Distribution of evidence across outcomes
The evidence mapping reveals a heterogeneous distribution of studies across cardiovascular and related health outcomes (Fig. 5). Key outcomes such as SBP (34 studies), DBP (33 studies), and functional capacity measured by the 6MWT (31 studies) are supported by a substantial body of literature. These outcomes represent areas of concentrated research attention, providing a robust foundation for evaluating the effectiveness of Tai Chi in improving cardiovascular health. In contrast, outcomes such as BMI, VO2max, and inflammation markers like IL-6 are supported by a considerably smaller number of studies, indicating limited research focus in these areas.
Categorization of effectiveness
The bubble chart categorizes the effectiveness of Tai Chi interventions into three distinct levels: “Effective,” “Potentially Effective,” and “Unclear,” reflecting the robustness and consistency of the evidence for each outcome.
Outcomes in the Effective category, such as SBP, DBP and functional capacity (6MWT), are supported by both a substantial volume of studies and consistent findings. These results highlight Tai Chi’s significant role in improving key cardiovascular health markers, likely attributable to its combined physical and mind-body effects. The robustness of these outcomes can be attributed to the physiological mechanisms underlying Tai Chi, such as enhanced vascular function, improved physical fitness, and reduced sympathetic nervous system activation. The large literature size for these outcomes further strengthens the reliability of the findings and underscores their clinical relevance.
In the Potentially Effective category, outcomes like anxiety, sleep quality, and stress demonstrate moderate evidence suggesting beneficial effects, but the findings are not as consistent or conclusive as those in the “Effective” category. The variability in these outcomes may stem from differences in study design, intervention duration, or the heterogeneity of participant characteristics. For example, psychological outcomes such as anxiety and stress are inherently influenced by subjective reporting, which can introduce variability. Despite these limitations, the trends indicate that Tai Chi holds promise as a complementary intervention for improving mental health and stress regulation.
Outcomes in the Unclear category, such as BMI, VO2max, and inflammatory markers like IL-6, are characterized by inconsistent or insufficient evidence. These outcomes are typically supported by a smaller number of studies, limiting the statistical power and generalizability of findings. The lack of clear effectiveness may also result from challenges in achieving measurable changes in these outcomes within the relatively short timeframes of many Tai Chi interventions. Additionally, the complexity of mechanisms influencing these outcomes, such as inflammation or aerobic capacity, may require longer-term or more targeted interventions to reveal significant effects.
The categorization of effectiveness highlights clear trends: outcomes closely aligned with Tai Chi’s known mechanisms of action, such as blood pressure regulation and functional capacity, are well-supported, while outcomes requiring longer-term physiological adaptation or more precise measurement remain underexplored. This underscores the importance of targeted research to address gaps in the evidence and to clarify Tai Chi’s potential benefits for a wider range of health outcomes.
Mechanistic pathways
The observed outcomes from the evidence mapping suggest that Tai Chi’s health benefits are mediated through two primary mechanisms: aerobic pathways and mind-body integrative mechanisms, each contributing to its effects on cardiovascular health and related outcomes.
Aerobic mechanisms
Improvements in key cardiovascular outcomes, such as systolic blood pressure, diastolic blood pressure, and functional capacity measured by the 6MWT, point to the role of Tai Chi in enhancing cardiovascular efficiency and physical endurance. Tai Chi involves continuous, low-to-moderate intensity movements that mimic the effects of aerobic exercise, promoting improved blood circulation, vascular flexibility, and overall cardiorespiratory fitness. For instance, reductions in blood pressure could be attributed to improved endothelial function and decreased vascular resistance, both commonly linked to regular physical activity. Similarly, the significant enhancements in 6MWT performance indicate better oxygen utilization and increased physical capacity, reinforcing the idea that Tai Chi engages aerobic pathways to improve overall cardiovascular health.
Mind-body mechanisms
Tai Chi also exerts notable effects on psychological outcomes, including reductions in stress, anxiety, and improvements in sleep quality. These findings highlight Tai Chi’s unique role as a mind-body exercise that integrates controlled breathing, focused attention, and gentle movements, which collectively help regulate the autonomic nervous system and reduce physiological stress responses. For example, Tai Chi may lower cortisol levels, decrease sympathetic over-activation, and improve parasympathetic activity, thereby enhancing psychological well-being. These mechanisms may explain why Tai Chi appears effective in addressing mental health issues, such as anxiety and poor sleep quality, which are often interrelated with cardiovascular risk factors.
Linking mechanisms to outcomes
The dual mechanisms of aerobic and mind-body pathways provide complementary effects, with each addressing distinct yet interconnected dimensions of cardiovascular health. For instance, the blood pressure-lowering effects of Tai Chi likely arise from both improved cardiovascular fitness (via aerobic pathways) and stress reduction (via mind-body mechanisms). Similarly, better functional capacity (e.g., 6MWT) reflects physical endurance improvements, while reductions in anxiety and stress indirectly support cardiovascular health by mitigating chronic inflammation and autonomic dysregulation. Outcomes such as sleep quality and mental health, closely tied to Tai Chi’s mind-body elements, also contribute to a holistic improvement in health and wellness.
The integration of these mechanisms underscores Tai Chi’s unique position as both a physical and psychological intervention, capable of addressing multiple facets of cardiovascular health. This highlights its potential as a comprehensive, low-risk, and accessible approach for improving outcomes in populations at risk for cardiovascular diseases. Future studies should aim to delineate the relative contributions of these pathways to further refine Tai Chi as a therapeutic modality.

Evidence map of Tai Chi’s effectiveness on cardiovascular health.
Discussion
Tai Chi vs. general aerobic exercise: mechanisms of action for cardiovascular health
Both this review and prior evidence syntheses highlight the shared cardiovascular benefits of Tai Chi and general aerobic exercise, including improvements in cardiorespiratory fitness, reductions in blood pressure, and favorable modulation of blood lipid profiles84. Consistent with the broader exercise literature, both modalities are associated with higher VO₂max, lower systolic and diastolic blood pressure, and reductions in LDL-C with concomitant increases in HDL-C, changes that are central to lowering cardiovascular event risk and improving long-term cardiac outcomes85. In addition, both Tai Chi and aerobic exercise demonstrate anti-inflammatory effects, including reductions in circulating biomarkers such as IL-6 and C-reactive protein (CRP), which are key indicators of chronic low-grade inflammation and atherosclerotic risk71. In aerobic exercise, these anti-inflammatory effects are thought to arise predominantly from increased skeletal-muscle IL-6 release during activity, improved insulin sensitivity, and reductions in visceral adiposity and oxidative stress, which together down-regulate hepatic CRP production and pro-inflammatory cytokine signaling85.
Within this overall overlap, the present review delineates more clearly the distinct mechanisms through which Tai Chi and general aerobic exercise exert their effects. A growing body of randomized controlled trials and meta-analyses shows that Tai Chi significantly improves multiple indices of heart rate variability (HRV)-including time-domain (e.g., SDNN, RMSSD) and frequency-domain parameters-indicating enhanced parasympathetic (vagal) modulation and reduced sympathetic dominance87,100. Higher HRV is mechanistically linked to better baroreflex sensitivity, more stable blood pressure control, and lower risks of arrhythmia and sudden cardiac events88. Tai Chi also appears to modulate inflammatory pathways directly: meta-analytic data show that Tai Chi can reduce CRP, IL-6, and TNF-α94, and RCTs in older adults report down-regulation of pro-inflammatory gene expression and cellular inflammatory signaling following Tai Chi-based interventions75. These effects are plausibly mediated via regulation of the hypothalamic–pituitary–adrenal (HPA) axis, improved sleep, and reductions in perceived stress and depressive symptoms, which together dampen sympathetic outflow and glucocorticoid-driven inflammatory activity. In contrast, the literature on conventional aerobic exercise emphasizes its relatively stronger impact on central cardiovascular conditioning—including larger gains in VO₂max, stroke volume, and cardiac output—and on metabolic efficiency, weight management, and reduction of central adiposity, which secondarily reduce inflammatory burden and improve vascular function89,90. Taken together, these data suggest that Tai Chi and general aerobic exercise share an overlapping anti-inflammatory and cardioprotective profile (e.g., lower IL-6 and CRP, improved HRV), but achieve these changes through partially distinct physiological routes. Aerobic exercise typically relies on higher metabolic loads and improvements in fitness and body composition to reduce inflammatory markers and enhance HRV. Tai Chi, by contrast, appears to produce meaningful improvements in HRV and inflammatory biomarkers at relatively low to moderate intensity, primarily through autonomic rebalancing, stress reduction, and neuroendocrine regulation. This dual pattern is consistent with our evidence map, in which blood-pressure and functional outcomes align with classic aerobic pathways, whereas HRV, IL-6/CRP, and psychosocial outcomes cluster more closely with Tai Chi’s mind–body mechanisms.
In interpreting these findings, it is important to consider the certainty of evidence as assessed using the GRADE approach. Overall, the certainty of evidence was moderate for key hemodynamic outcomes (particularly SBP, DBP, and resting heart rate), where multiple randomized trials showed generally consistent benefit despite heterogeneity and some risk-of-bias concerns. By contrast, the certainty of evidence for cardiorespiratory fitness and metabolic outcomes (e.g., VO₂max, lipid profiles, and other cardiometabolic markers) was predominantly low, due to small sample sizes, variability in intervention protocols, and wide confidence intervals102,111. For inflammatory biomarkers (such as IL-6 and CRP), HRV, and psychosocial outcomes (including stress, mood, sleep, and quality of life), the evidence was rated as low to very low certainty, reflecting the limited number of trials, inconsistent results, and imprecision. These GRADE ratings indicate that our conclusions are most robust for blood-pressure-related outcomes, whereas mechanistic and psychosocial effects—although biologically plausible and supported by emerging biomarker data—should be interpreted more cautiously and confirmed in future high-quality trials.
Another key distinction lies in the application of these exercise modalities to specific populations. Prior reviews have emphasized Tai Chi’s suitability for older adults and individuals with limited mobility or chronic conditions, which is consistent with our findings. Tai Chi’s low-impact, slow, and adaptable movements, combined with its beneficial effects on balance, HRV, and inflammatory profiles, make it particularly attractive for populations in whom autonomic dysfunction, sleep disturbance, and chronic systemic inflammation are common92. Similarly, while aerobic exercise is effective and often preferred for general cardiovascular conditioning, our synthesis suggests that it may be especially appropriate for younger or more physically capable individuals seeking greater improvements in VO2max, weight reduction, and high-level endurance or performance goals. In such groups, the capacity to sustain higher training intensities allows aerobic exercise to exert maximal effects on metabolic and hemodynamic parameters.
While previous reviews have noted the complementary roles of Tai Chi and general aerobic exercise, our integrated framework further clarifies how these modalities can be combined in practice. Tai Chi primarily targets systemic and autonomic regulation-through parasympathetic activation, improved HRV, reductions in IL-6 and CRP, and mitigation of stress-related neuroendocrine dysregulation—whereas aerobic exercise provides direct cardiovascular conditioning via sustained elevations in cardiac output, oxygen utilization, and energy expenditure. Structuring interventions that sequence or blend these approaches (for example, incorporating Tai Chi on low-intensity days within an aerobic training program, or adding moderate aerobic sessions to Tai Chi-based rehabilitation) may optimize both biomarker profiles and functional outcomes across diverse clinical populations35. This review therefore advances the existing literature by providing a more detailed and explicitly comparative account of the molecular, physiological, and psychosocial mechanisms underlying the cardiovascular benefits of Tai Chi and general aerobic exercise93. It supports a tailored approach in which intervention choice and combination are guided by patient characteristics (e.g., age, comorbidities, baseline fitness, psychological distress) and mechanistic targets (e.g., autonomic imbalance, chronic inflammation, obesity, low cardiorespiratory fitness). By situating HRV, IL-6, and CRP within this mechanistic framework, the review contributes to the development of more personalized exercise prescriptions that go beyond single-modality interventions94.
Finally, while prior reviews have called for further research into the molecular and systemic pathways of different exercise modalities, our synthesis identifies specific priorities: (i) adequately powered trials that directly compare Tai Chi with standardized aerobic exercise on HRV, IL-6, CRP, and related biomarkers; (ii) longitudinal studies that evaluate whether biomarker changes mediate long-term reductions in clinical cardiovascular events; and (iii) pragmatic trials that test combined Tai Chi–aerobic programs in high-risk groups. Addressing these gaps will strengthen the mechanistic evidence base and inform how best to integrate Tai Chi and aerobic exercise within cardiovascular prevention and rehabilitation strategies.
Implications for cardiovascular disease management
A closer examination of the perspectives on Tai Chi’s role in CVD management reveals both areas of alignment and critical advancements unique to the current synthesis. Previous studies emphasize the suitability of Tai Chi as a low-impact exercise for populations with physical limitations, such as elderly individuals or patients recovering from surgery101. Building on this foundation, my synthesis highlights the importance of tailoring Tai Chi programs to individual needs, incorporating progressive intensity levels to ensure accessibility while maintaining effectiveness82,83. This targeted approach provides a practical pathway for integrating Tai Chi into clinical and community care settings, addressing challenges that previous discussions have not fully explored81.
In addition to its accessibility, Tai Chi’s mind-body integration has been recognized for its psychological benefits, including stress reduction and emotional resilience. However, my analysis expands this understanding by emphasizing the direct relevance of these benefits to comprehensive CVD management80. For example, I highlight its role in reducing stress-related biomarkers and alleviating depressive symptoms, which are critical factors in managing chronic diseases74. By linking these psychological improvements with physical outcomes, such as better autonomic balance and reduced inflammation, my synthesis presents a more holistic framework for understanding Tai Chi’s therapeutic value55.
While earlier research acknowledges Tai Chi’s cardiovascular benefits, including improved blood pressure and cardiorespiratory fitness, my synthesis delves deeper into its mechanisms of action100. I emphasize its impact on specific risk factors, such as heart rate variability and lipid profile regulation, which are crucial for preventing and managing cardiovascular complications79. Moreover, my perspective positions Tai Chi as a viable alternative for patients unable to engage in high-intensity aerobic exercises, broadening its relevance to a wider range of clinical scenarios78.
Practical implementation strategies also receive a more detailed exploration in my synthesis. While previous studies suggest community-based initiatives and professional training, I propose a comprehensive framework that includes the development of condition-specific programs, integration into rehabilitation plans, and systematic outcome monitoring79. These recommendations ensure that Tai Chi interventions align with therapeutic goals and address both the physical and logistical challenges of real-world healthcare delivery77.
In addition to clinical effectiveness, Tai Chi has favorable implications for accessibility and potential cost-effectiveness. Tai Chi typically requires minimal equipment and can be delivered in community or group settings, which may lower implementation costs compared with supervised facility-based aerobic training. Its low-impact nature and adaptability for older adults or those with comorbidities also enhance accessibility, suggesting that Tai Chi could be a scalable, resource-efficient option for cardiovascular risk reduction, particularly in low-resource or community settings.
In summary, the current analysis not only reaffirms the established benefits of Tai Chi but also introduces actionable insights into its integration within cardiovascular care. By addressing both physical and psychological dimensions, advocating for tailored program designs, and emphasizing practical implementation strategies, this perspective underscores Tai Chi’s potential as a scientifically validated, holistic, and scalable intervention for managing cardiovascular diseases54. These advancements highlight its unique capacity to meet the needs of diverse populations, particularly those facing mobility constraints or other exercise barriers.
Clinical and practical recommendations
This review provides a comprehensive exploration of the clinical and practical recommendations for Tai Chi, emphasizing its role as a versatile and holistic health intervention. The primary focus lies on its structured application, adaptability for diverse populations, and potential for integration into broader health management strategies112. Specifically, this review recommends practicing Tai Chi 3–5 times per week for sessions lasting 30–60 min, structured into warm-up, active practice, and cool-down phases56,87. This approach is designed to gradually build endurance, improve mastery, and ensure safe engagement for participants across different fitness levels and health conditions57. Moreover, the adaptability of Tai Chi is highlighted through the inclusion of simplified forms, such as the 8-form and 24-form Yang-style, which are particularly suitable for beginners, older adults, and individuals with limited mobility113. These simplified forms prioritize safety while maintaining therapeutic efficacy, ensuring accessibility for a wide range of participants58.
An essential feature of this review is its emphasis on personalization and dynamic feedback. Unlike traditional exercise recommendations, this review advocates tailoring Tai Chi programs based on individual health conditions, fitness levels, and psychological states51. By monitoring progress through measurable health indicators, such as balance, cardiovascular metrics, and sleep quality, practitioners can adjust the intensity, duration, and complexity of Tai Chi sessions to match individual needs52. This evidence-based approach enhances safety, engagement, and the likelihood of sustained benefits, presenting Tai Chi as a scientifically grounded and adaptable health intervention.
In addition to its physical health benefits, Tai Chi’s psychological and social dimensions are extensively explored in this review. The meditative aspects of Tai Chi foster relaxation and stress reduction, contributing to improved emotional well-being105. Moreover, group classes provide opportunities for social interaction and motivation, creating a supportive environment that promotes long-term adherence60. These multifaceted benefits not only enhance physical health outcomes but also address mental and social well-being, making Tai Chi a holistic practice for comprehensive health improvement.
This review also emphasizes the integration of Tai Chi into broader health management strategies. By combining Tai Chi with complementary activities, such as walking or resistance training, and lifestyle modifications like dietary adjustments, its benefits can be amplified88. These integrative strategies extend Tai Chi’ s therapeutic potential beyond isolated practice, positioning it as an integral component of modern health management programs104. This forward-looking perspective aligns Tai Chi with the principles of preventive and rehabilitative healthcare, broadening its applicability and relevance63.
While this review builds upon existing literature, it makes unique contributions by providing actionable and structured recommendations for practice, exploring the multidimensional benefits of Tai Chi, and addressing previously unarticulated gaps between theoretical mechanisms and clinical applications76. Specifically, this review highlights Tai Chi’s dual pathways—integrating aerobic and mind-body mechanisms—as a holistic intervention for cardiovascular health. By examining its impact on autonomic regulation, neurohormonal balance, and molecular mechanisms (e.g., lipid metabolism and inflammation), this review expands theoretical understanding, bridging gaps between molecular insights and practical implementation (e.g., reducing TNF-αand enhancing HRV)78. A significant gap addressed by this review lies in the lack of tailored frameworks for implementing Tai Chi in diverse populations. While previous studies emphasize Tai Chi’ s suitability for elderly individuals, this review further identifies its relevance for patients with specific conditions, such as hypertension, anxiety, and limited mobility34,35,55. This nuanced perspective ensures broader applicability across age groups and health conditions, underscoring Tai Chi’ s potential as a low-risk, cost-effective intervention.
Furthermore, this review identifies gaps in existing practice guidelines, such as the absence of standardized Tai Chi protocols for specific health outcomes. It offers detailed suggestions for frequency, duration, and adaptation, such as integrating Tai Chi into multidisciplinary health programs combining dietary adjustments and resistance training. These insights not only enrich theoretical models but also offer a practical roadmap for clinical and public health applications. Future research should focus on optimizing protocols for diverse populations and exploring synergistic effects with other interventions to maximize Tai Chi’s benefits.
Limitations
The study has several limitations. High heterogeneity in key outcomes (e.g., SBP and DBP, I2 > 80%) reflects variability in protocols, designs, and populations, affecting result precision. Certain outcomes, like IL-6 and VO2max, are supported by fewer studies, limiting robustness. Most interventions are short-term, hindering assessment of long-term effects. Variability in Tai Chi styles and reliance on subjective measures, such as stress and sleep quality, further reduce comparability and reliability. Addressing these issues through standardized protocols, long-term studies, and diverse populations will strengthen the evidence base.
Future research directions
Future studies should evaluate the long-term effects of Tai Chi, focusing on how its mind-body mechanisms, such as autonomic regulation and stress reduction, differ from the physiological benefits of aerobic exercise. Key unresolved questions include whether Tai Chi’s modulation of inflammatory biomarkers (e.g., TNF-α, CRP, IL-6) and psychological outcomes (e.g., stress and anxiety reduction) provides distinct advantages over aerobic exercise, and how these effects manifest across different populations.
Standardizing protocols for Tai Chi style, intensity, duration, and frequency is critical to improving comparability across studies. Correlating these parameters with those of aerobic exercise will clarify the unique and overlapping benefits of each modality. For example, future research could determine whether equivalent session durations yield similar cardiovascular or psychosocial outcomes. Expanding research to include younger and more diverse populations will enhance generalizability, while integrating objective measures such as inflammatory biomarkers and heart rate variability will complement subjective outcomes like stress relief and quality of life improvement. Comparative studies that explore the integration of Tai Chi with other therapies, including resistance training or dietary interventions, could uncover synergistic effects and refine intervention strategies.
These efforts will help address gaps in the literature, further differentiate Tai Chi from traditional aerobic exercise, and establish it as a scalable, cost-effective, and evidence-based approach for cardiovascular health management.
Conclusion
This systematic review and meta-analysis highlights Tai Chi as a unique intervention for cardiovascular health, integrating benefits from aerobic and mind-body mechanisms. Beyond traditional aerobic exercises, Tai Chi provides additional advantages in autonomic regulation, stress reduction, and modulation of inflammatory markers such as CRP and TNF-α, offering a holistic approach for managing cardiovascular diseases, especially in populations with limited mobility or chronic conditions. Tai Chi’s adaptability and low-impact nature make it accessible to diverse populations, addressing both physiological and psychosocial dimensions. Its unique integration of aerobic and meditative components ensures suitability across varying physical capacities.
Future research should prioritize long-term randomized trials to directly compare Tai Chi and aerobic exercise, focusing on mechanisms like heart rate variability and inflammation. Standardizing protocols for intensity, duration, and frequency will improve study comparability, while expanding research to younger and more diverse populations will enhance generalizability. Exploring its integration with other therapeutic modalities could further optimize its application.
This review establishes Tai Chi as a cost-effective, scalable, and scientifically validated intervention, bridging gaps between traditional exercise and holistic health approaches, and advancing its role in cardiovascular disease prevention and management.
Data availability
All data synthesized from this study are presented in the manuscript and supplementary materials.
References
Wald, N. J. & Law, M. R. A strategy to reduce cardiovascular disease by more than 80%. Bmj 326, 1419 (2003).
Schwalm, J. D., McKee, M., Huffman, M. D. & Yusuf, S. Resource effective strategies to prevent and treat cardiovascular disease. Circulation 133, 742–755 (2016).
Rose, G. Strategy of prevention: lessons from cardiovascular disease. Br. Med. J. (Clinical Res. ed). 282, 1847 (1981).
Hayes, S. M., Alosco, M. L. & Forman, D. E. The effects of aerobic exercise on cognitive and neural decline in aging and cardiovascular disease. Curr. Geriatr. Rep. 3, 282–290 (2014).
Berry, J. D. et al. Lifetime risks of cardiovascular disease. N. Engl. J. Med. 366, 321–329 (2012).
Golia, E. et al. Inflammation and cardiovascular disease: from pathogenesis to therapeutic target. Curr. Atheroscler. Rep. 16, 1–7 (2014).
Francula-Zaninovic, S. & Nola, I. A. Management of measurable variable cardiovascular disease’risk factors. Curr. Cardiol. Rev. 14, 153–163 (2018).
Jan, Y. K. et al. Diagnosis, pathophysiology and management of microvascular dysfunction in diabetes mellitus. Diagnostics 14, 2830. https://doi.org/10.3390/diagnostics14242830 (2024).
Anderson, K. M., Odell, P. M., Wilson, P. W. & Kannel, W. B. Cardiovascular disease risk profiles. Am. Heart J. 121, 293–298 (1991).
Lin, S. et al. Effects of the intensity, duration and muscle mass factors of isometric exercise on acute local muscle hemodynamic responses and systematic blood pressure regulation. Front. Bioeng. Biotech. 12, 1444598. https://doi.org/10.3389/fbioe.2024.1444598 (2024).
Jan, Y. K. & Cheung, W. C. Muscle oxygenation regulation in physical therapy and rehabilitation. Med. Gas Res. 16, 66–75. https://doi.org/10.4103/mgr.MEDGASRES-D-24-00149 (2026).
Hagglund, L., Boman, K. & Brannstrom, M. A mixed methods study of Tai Chi exercise for patients with chronic heart failure aged 70 years and older. Nurs. Open. 5, 176–185. https://doi.org/10.1002/nop2.127 (2018).
Niu, Y., Buranarugsa, R. & Kuhirunyaratn, P. Comparing the effects of Bafa Wubu Tai Chi and traditional He-Style Tai Chi exercises on physical health risk factors in overweight male college students: A randomized controlled trial. Int. J. Environ. Res. Public Health. 20 https://doi.org/10.3390/ijerph20146323 (2023).
Hu, Q. H., Qian, Y. L., Liu, X. L., Zhu, H. & Xiao, J. W. Effects of 12-week Tai Chi exercise on the microvascular reactivity of the middle-aged and elderly patients with mild hypertension and its mechanism. Chin. J. Appl. Physiol. 37, 683–687. https://doi.org/10.12047/j.cjap.6164.2021.080 (2021).
Liu, X., Miller, Y. D., Burton, N. W. & Brown, W. J. RETRACTED: A preliminary study of the effects of Tai Chi and qigong medical exercise on indicators of metabolic syndrome, glycaemic control, health-related quality of life, and psychological health in adults with elevated blood glucose (Retracted Article). Br. J. Sports Med. 44, 704–709. https://doi.org/10.1136/bjsm.2008.051144 (2010).
Manh Hung, N. & Kruse, A. A randomized controlled trial of Tai Chi for balance, sleep quality and cognitive performance in elderly Vietnamese. Clin. Interv. Aging. 7, 185–189. https://doi.org/10.2147/cia.S32600 (2012).
Geib, R. W. et al. Using computerized posturography to explore the connection between Bmi and postural stability in long-term Tai Chi practitioners - biomed 2011. Biomed. Sci. Instrum. 47, 288–293 (2011).
Wen, J. & Su, M. A. Randomized trial of Tai Chi on preventing hypertension and hyperlipidemia in Middle-Aged and elderly patients. Int. J. Environ. Res. Public Health. 18 https://doi.org/10.3390/ijerph18105480 (2021).
Oliveira Dantas, F. F. et al. Acute effects of Tai Chi Chuan Exercise on blood pressure and heart rate in peripheral artery disease patients. J. Altern. Complement. Med. 22, 375–379. https://doi.org/10.1089/acm.2015.0230 (2016).
Wang, C. et al. Tai Chi on psychological well-being: systematic review and meta-analysis. BMC Complement. Altern. Med. 10, 1–16 (2010).
Lin, C. Y. et al. Acute physiological and psychological effects of qigong exercise in older practitioners. Evid. Based Complement. Alternat. Med. 2018, 4960978 (2018).
Huang, Y. T., Wang, C. H. & Wu, Y. F. Adhering to a Tai Chi Chuan exercise program improves vascular resistance and cardiac function. Int. J. Gerontol. 5, 150–154. https://doi.org/10.1016/j.ijge.2011.09.037 (2011).
Chang, M. Y., Yeh, S. C. J., Chu, M. C., Wu, T. M. & Huang, T. H. Associations between Tai Chi Chung Program, Anxiety, and cardiovascular risk factors. Am. J. Health Promotion. 28, 16–22. https://doi.org/10.4278/ajhp.120720-QUAN-356 (2013).
Keltz, R. R. et al. A standardized approach to evaluate effectiveness of aerobic exercise training interventions in cardiovascular disease at the individual level. Int. J. Cardiol. 412, 132335 (2024).
Liao, F. & Jan, Y. K. Assessing skin blood flow function in people with spinal cord injury using the time domain, time–frequency domain and deep learning approaches. Biomed. Signal Process. Control. 84, 104790 (2023).
Kelley, G. A., Kelley, K. S. & Franklin, B. Aerobic exercise and lipids and lipoproteins in patients with cardiovascular disease: a meta-analysis of randomized controlled trials. J. Cardiopulm. Rehabil. Prev. 26, 131–139 (2006).
Rognmo, Ø. et al. Cardiovascular risk of high-versus moderate-intensity aerobic exercise in coronary heart disease patients. Circulation 126, 1436–1440 (2012).
Ades, P. A. & Wu, G. Benefits of Tai Chi in chronic heart failure: body or mind? Am. J. Med. 117, 611–612. https://doi.org/10.1016/j.amjmed.2004.08.001 (2004).
Liao, F. et al. Using wavelet phase coherence of heart rate variability and blood flow oscillations to compare mechanisms of action between Tai Chi mind-body exercise and brisk walking aerobic exercise. Biomed. Signal Process. Control. 95, 106385 (2024).
Hong, Y. L., Li, J. X. & Robinson, P. D. Balance control, flexibility, and cardiorespiratory fitness among older Tai Chi practitioners. Br. J. Sports Med. 34, 29–34. https://doi.org/10.1136/bjsm.34.1.29 (2000).
Channer, K. S., Barrow, D., Barrow, R., Osborne, M. & Ives, G. Changes in haemodynamic parameters following Tai Chi Chuan and aerobic exercise in patients recovering from acute myocardial infarction. Postgrad. Med. J. 72, 349–351. https://doi.org/10.1136/pgmj.72.848.349 (1996).
Fong, S. S. et al. Changes in heart-rate variability of survivors of nasopharyngeal cancer during Tai Chi qigong practice. J. Phys. Therapy Sci. 27, 1577–1579 (2015).
Jones, A. Y., Dean, E. & Scudds, R. J. Effectiveness of a community-based Tai Chi program and implications for public health initiatives. Arch. Phys. Med. Rehabil. 86, 619–625 (2005).
Wang, S. et al. Effectiveness of Tai Chi on blood Pressure, Stress, Fatigue, and sleep quality among Chinese women with episodic migraine: A randomised controlled trial. Evidence-Based Complement. Altern. Med. 2022 https://doi.org/10.1155/2022/2089139 (2022).
Wong, A. et al. Effectiveness of Tai Chi on cardiac autonomic function and symptomatology in women with fibromyalgia: A randomized controlled trial. J. Aging Phys. Act. 26, 214–221. https://doi.org/10.1123/japa.2017-0038 (2018).
Alsubiheen, A., Petrofsky, J., Yu, W. & Lee, H. Effect of Tai Chi combined with mental imagery on cutaneous microcirculatory function and blood pressure in a diabetic and elderly population. Healthcare 8 https://doi.org/10.3390/healthcare8030342 (2020).
Irwin, M. R. et al. Cognitive behavioral therapy and Tai Chi reverse cellular and genomic markers of inflammation in late-life insomnia: a randomized controlled trial. Biol. Psychiatry. 78, 721–729 (2015).
Maris, S. A., Winter, C. R., Paolone, V. J. & Headley, S. A. E. Comparing the changes in blood pressure after acute exposure to Tai Chi and walking. Int. J. Exerc. Sci. 12, 77–87 (2019).
Page, M. J. et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. Bmj., 372, (2021).
Higgins, J. Cochrane handbook for systematic reviews of interventions. Cochrane Collab. John Wiley & Sons Ltd (2008).
Sterne, J. A. et al. RoB 2: a revised tool for assessing risk of bias in randomised trials. BMJ. 366, (2019).
Shea, B. J. et al. AMSTAR 2: a critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ. 358, (2017).
Andrade, C. Mean difference, standardized mean difference (SMD), and their use in meta-analysis: as simple as it gets. J. Clin. Psychiatry. 81, 11349 (2020).
Greenwood, P. E. & Nikulin, M. S. A Guide To chi-squared Testing Vol. 280 (Wiley, 1996).
Christopher Frey, H. & Patil, S. R. Identification and review of sensitivity analysis methods. Risk Anal. 22, 553–578 (2002).
Gupta, S. K. Intention-to-treat concept: a review. Perspect. Clin. Res. 2, 109–112 (2011).
Sterne, J. A. & Harbord, R. M. Funnel plots in meta-analysis. Stata J. 4, 127–141 (2004).
Egger, M., Smith, G. D., Schneider, M. & Minder, C. Bias in meta-analysis detected by a simple, graphical test. BMJ. 315, 629–634 (1997).
Brożek, J. et al. Grading quality of evidence and strength of recommendations in clinical practice guidelines: part 1 of 3. An overview of the GRADE approach and grading quality of evidence about interventions. Allergy 64, 669–677 (2009).
Beebe, N. et al. Effects of the addition of t’ai Chi to a dietary weight loss program on lipoprotein atherogenicity in obese older women. J. Altern. Complement. Med. 19, 759–766 (2013).
Lam, P., Dennis, S. M., Diamond, T. H. & Zwar, N. Improving glycaemic and BP control in type 2 diabetes the effectiveness of Tai Chi. Aus. Fam. Physician. 37, 884–887 (2008).
Leung, L. Y., Chan, A. W., Sit, J. W., Liu, T. & Taylor-Piliae, R. E. Tai Chi in Chinese adults with metabolic syndrome: A pilot randomized controlled trial. Complement. Ther. Med. 46, 54–61. https://doi.org/10.1016/j.ctim.2019.07.008 (2019).
Wei, G. X. et al. Tai Chi Chuan modulates heart rate variability during abdominal breathing in elderly adults. Psych J. 5, 69–77. https://doi.org/10.1002/pchj.105 (2016).
Joseph, L. & Ramakrishnan, T. V. Tai Chi therapy attenuates biophysiological status, pain and depression in elderly subjects. J. Evol. Med. Dent. Sci. 10, 102–106 (2021).
Logghe, I. H. et al. Lack of effect of Tai Chi Chuan in preventing falls in elderly people living at home: a randomized clinical trial. J. Am. Geriatr. Soc. 57, 70–75 (2009).
Caminiti, G. et al. Tai Chi enhances the effects of endurance training in the rehabilitation of elderly patients with chronic heart failure. Rehabilitation Res. Pract. 2011, 761958–761958. https://doi.org/10.1155/2011/761958 (2011).
Guo, L. Effects of 24-Form Tai Chi on Cardio-Pulmonary functions, exercise Performances, and cognitive functions of the aged. Iran. J. Public. Health. 51, 2253–2261 (2022).
Hui, S. S. C., Xie, Y. J., Woo, J. & Kwok, T. C. Y. Effects of Tai Chi and Walking Exercises on Weight Loss, Metabolic Syndrome Parameters, and Bone Mineral Density: A Cluster Randomized Controlled Trial. Evid. Based Complement. Alternat. Med. 2015, https://doi.org/10.1155/2015/976123 (2015).
Sato, S., Makita, S., Uchida, R., Ishihara, S. & Masuda, M. Effect of Tai Chi training on baroreflex sensitivity and heart rate variability in patients with coronary heart disease. Int. Heart J. 51, 238–241. https://doi.org/10.1536/ihj.51.238 (2010).
Li, X. et al. Effect of Tai Chi vs aerobic exercise on blood pressure in patients with prehypertension: A randomized clinical trial. Jama Netw. Open. 7 https://doi.org/10.1001/jamanetworkopen.2023.54937 (2024).
Li, Y., Zhang, H. & Wang, Y. Tai Chi ameliorates coronary heart disease by affecting serum levels of miR-24 and miR-155. Front. Physiol. 10 https://doi.org/10.3389/fphys.2019.00587 (2019).
Liu, T. Effects of a Group- plus Home-based Tai Chi Program on Physical Function and Psychosocial Well-being in Chinese Patients with Coronary Heart Disease, (2020).
Liu, T., Chan, A. W. K. & Chair, S. Y. Group- plus home-based Tai Chi program improves functional Heath among patients with coronary heart disease: a randomized controlled trial. Eur. J. Cardiovasc. Nurs. 21, 597–611. https://doi.org/10.1093/eurjcn/zvab126 (2022).
Nery, R. M. et al. Tai Chi Chuan improves functional capacity after myocardial infarction: A randomized clinical trial. Am. Heart J. 169, 854–860. https://doi.org/10.1016/j.ahj.2015.01.017 (2015).
Nguyen, M. H. & Kruse, A. The effects of Tai Chi training on physical fitness, perceived health, and blood pressure in elderly Vietnamese. Open. access. J. Sports Med. 3, 7–16. https://doi.org/10.2147/oajsm.S27329 (2012).
Nosrat-abad, T. H., Bayrami, M., Namdar, H., Esmaeilpour, K. & Ezzati, D. Effects of Tai Chi on cardiovascular responses and stress reduction in prehypertensive subjects: A randomized clinical trial. Eur. J. Hum. Mov. 46, 85–94. https://doi.org/10.21134/eurjhm.2021.46.3 (2021).
Redwine, L. S. et al. An exploratory randomized sub-study of light-to-moderate intensity exercise on cognitive function, depression symptoms and inflammation in older adults with heart failure. J. Psychosom. Res. 128 https://doi.org/10.1016/j.jpsychores.2019.109883 (2020).
Robins, J. L., Elswick, R. K. Jr., Sturgill, J. & McCain, N. L. The effects of Tai Chi on cardiovascular risk in women. Am. J. Health Promotion. 30, 613–622. https://doi.org/10.4278/ajhp.140618-QUAN-287 (2016).
Wang, W. et al. Tai Chi exercise versus rehabilitation for the elderly with cerebral vascular disorder: a single-blinded randomized controlled trial. Psychogeriatrics 10, 160–166. https://doi.org/10.1111/j.1479-8301.2010.00334.x (2010).
Wang, Y., Guo, X., Liu, L., Xie, M. & Lam, W. K. Effects of Tai-Chi and running exercises on cardiorespiratory fitness and biomarkers in sedentary Middle-Aged males: A 24-Week supervised training study. Biology-Basel 11 https://doi.org/10.3390/biology11030375 (2022).
Wang, Y., Luo, B., Wu, X., Li, X. & Liao, S. Comparison of the effects of Tai Chi and general aerobic exercise on weight, blood pressure and glycemic control among older persons with depressive symptoms: a randomized trial. BMC Geriatr. 22 https://doi.org/10.1186/s12877-022-03084-6 (2022).
Yeh, G. Y. et al. Effects of Tai Chi mind-body movement therapy on functional status and exercise capacity in patients with chronic heart failure: A randomized controlled trial. Am. J. Med. 117, 541–548. https://doi.org/10.1016/j.amjmed.2004.04.016 (2004).
Yeh, G. Y. et al. Tai Chi in patients with heart failure with preserved ejection fraction. Congestive Heart Fail. (Greenwich Conn). 19, 77–84. https://doi.org/10.1111/chf.12005 (2013).
Zhang, G. et al. Tai Chi Improves Coronary Heart Disease Risk by Inactivating MAPK/ERK Pathway through Serum miR-126. Evid. Based Complement. Alternat. Med. 2020, https://doi.org/10.1155/2020/4565438 (2020).
Irwin, M. R. & Olmstead, R. Mitigating cellular inflammation in older adults: a randomized controlled trial of Tai Chi Chih. Am. J. Geriatric Psychiatry. 20, 764–772 (2012).
Janelsins, M. C. et al. Effects of Tai Chi Chuan on insulin and cytokine levels in a randomized controlled pilot study on breast cancer survivors. Clin. Breast. Cancer. 11, 161–170 (2011).
Ma, Y. et al. Complexity-based measures of heart rate dynamics in older adults following long-and short-term Tai Chi training: cross-sectional and randomized trial studies. Sci. Rep. 9, 7500 (2019).
You, T. et al. Effects of Tai Chi on beta endorphin and inflammatory markers in older adults with chronic pain: an exploratory study. Aging Clin. Exp. Res. 32, 1389–1392 (2020).
Zheng, S. et al. The effects of twelve weeks of Tai Chi practice on anxiety in stressed but healthy people compared to exercise and wait-list groups–A randomized controlled trial. J. Clin. Psychol. 74, 83–92 (2018).
Hosseini, H., Esfirizi, M. F., Marandi, S. M. & Rezaei, A. The effect of Ti Chi exercise on the sleep quality of the elderly residents in Isfahan, Sadeghieh elderly home. Iran. J. Nurs. Midwifery Res. 16, 55 (2011).
Choi, H. J. Effects of therapeutic Tai Chi on functional fitness and activities of daily living in patients with Parkinson disease. J. Exerc. Rehabilitation. 12, 499 (2016).
Hackney, M. E. & Earhart, G. M. Tai Chi improves balance and mobility in people with Parkinson disease. Gait Posture. 28, 456–460 (2008).
Kurlan, R. et al. Tai Chi in parkinson’s disease: a preliminary randomized, controlled, and rater-blinded study. Adv. Parkinson’s Disease. 4, 9 (2015).
Xinzheng, W., Fanyuan, J. & Xiaodong, W. The effects of Tai Chi on glucose and lipid metabolism in patients with diabetes mellitus: A meta-analysis. Complement. Ther. Med. 71, 102871 (2022).
Raman, G., Zhang, Y., Minichiello, V. J., D’Ambrosio, C. M. & Wang, C. Tai Chi improves sleep quality in healthy adults and patients with chronic conditions: a systematic review and meta-analysis. J. sleep. Disorders & Therapy, 2 (2013).
Wang, J. et al. Tai Chi for essential hypertension. Evidence-Based Complement. Altern. Med. https://doi.org/10.1155/2013/215254 (2013). (2013).
Lauche, R. et al. Efficacy of Tai Chi and qigong for the prevention of stroke and stroke risk factors: a systematic review with meta-analysis. Medicine 96, e8517 (2017).
Qin, J. et al. Effect of Tai Chi alone or as additional therapy on low back pain: systematic review and meta-analysis of randomized controlled trials. Medicine 98, e17099 (2019).
Song, R. et al. The impact of Tai Chi and qigong mind-body exercises on motor and non-motor function and quality of life in parkinson’s disease: a systematic review and meta-analysis. Parkinsonism Relat. Disord. 41, 3–13 (2017).
Guo, C. et al. Effects of Tai Chi training on the physical and mental health status in patients with chronic obstructive pulmonary disease: a systematic review and meta-analysis. J. Thorac. Disease. 12, 504 (2020).
Li, H. Impact of the newly compiled Tai Chi (BaFa WuBu) on vascular health in middle-aged and older postmenopausal women: an analysis of the long-term intervention effect of a 24-week RCT. Figshare, Dataset. https://doi.org/10.6084/M9.FIGSHARE.25508686.V1 (2024).
Ren, X. et al. The effects of Tai Chi training in patients with heart failure: a systematic review and meta-analysis. Front. Physiol. 8, 989 (2017).
Chen, Y. W., Hunt, M. A., Campbell, K. L., Peill, K. & Reid, W. D. The effect of Tai Chi on four chronic conditions—cancer, osteoarthritis, heart failure and chronic obstructive pulmonary disease: a systematic review and meta-analyses. Br. J. Sports Med. 50, 397–407 (2016).
Shu, C., Feng, S., Cui, Q., Cheng, S. & Wang, Y. Impact of Tai Chi on CRP, TNF-alpha and IL-6 in inflammation: a systematic review and meta-analysis. Annals Palliat. Med. 10, 7468478–7467478 (2021).
Luo, X. C. et al. Effect of Tai Chi Chuan in breast cancer patients: a systematic review and meta-analysis. Front. Oncol. 10, 607 (2020).
Hall, A. et al. Effectiveness of Tai Chi for chronic musculoskeletal pain conditions: updated systematic review and meta-analysis. Phys. Ther. 97, 227–238 (2017).
Yan, J. H. et al. Efficacy of Tai Chi on pain, stiffness and function in patients with osteoarthritis: a meta-analysis. PloS One. 8, e61672 (2013).
Zeng, Y., Luo, T., Xie, H., Huang, M. & Cheng, A. S. Health benefits of qigong or Tai Chi for cancer patients: a systematic review and meta-analyses. Complement. Ther. Med. 22, 173–186 (2014).
Yan, J. H., Pan, L., Zhang, X. M., Sun, C. X. & Cui, G. H. Lack of efficacy of Tai Chi in improving quality of life in breast cancer survivors: a systematic review and meta-analysis. Asian Pac. J. Cancer Prev. 15, 3715–3720 (2014).
Liu, L., Tan, H., Yu, S., Yin, H. & Baxter, G. D. The effectiveness of Tai Chi in breast cancer patients: A systematic review and meta-analysis. Complement. Ther. Clin. Pract. 38, 101078 (2020).
Ni, X. et al. The effects of Tai Chi on quality of life of cancer survivors: a systematic review and meta-analysis. Support. Care Cancer. 27, 3701–3716 (2019).
Huang, C. Y. et al. The effect of Tai Chi in elderly individuals with sarcopenia and frailty: A systematic review and meta-analysis of randomized controlled trials. Ageing Res. Rev. 82, 101747 (2022).
Campo, R. A. et al. Blood pressure, salivary cortisol, and inflammatory cytokine outcomes in senior female cancer survivors enrolled in a Tai Chi Chih randomized controlled trial. J. Cancer Surviv. 9, 115–125. https://doi.org/10.1007/s11764-014-0395-x (2015).
Liu, J. et al. The effects of Tai Chi on heart rate variability in older Chinese individuals with depression. Int. J. Environ. Res. Public Health. 15 https://doi.org/10.3390/ijerph15122771 (2018).
Li, X. et al. Effect of Tai Chi versus aerobic exercise on blood pressure in prehypertension patients (TCOBPP): a study protocol for a 12-month randomized controlled trial. Trials 23 https://doi.org/10.1186/s13063-022-06840-6 (2022).
Tsai, J. C. et al. The beneficial effects of Tai Chi Chuan on blood pressure and lipid profile and anxiety status in a randomized controlled trial. J. Altern. Complement. Med. 9, 747–754. https://doi.org/10.1089/107555303322524599 (2003).
Zhou, S. et al. The effects of Tai Chi on markers of Atherosclerosis, Lower-limb physical Function, and cognitive ability in adults aged over 60: A randomized controlled trial. Int. J. Environ. Res. Public Health. 16 https://doi.org/10.3390/ijerph16050753 (2019).
Xie, G. et al. Effects of Tai Chi Yunshou exercise on community-based stroke patients: a cluster randomized controlled trial. Eur. Rev. Aging Phys. Activity. 15 https://doi.org/10.1186/s11556-018-0206-x (2018).
Zaki, S., Moiz, J., Bhati, P. & Menon, G. Efficacy of high-intensity interval training on cardiac autonomic modulation in cardiovascular diseases and lifestyle disorders: a systematic review and meta-analysis. Comp. Exerc. Physiol. 18, 37–52 (2022).
Zhao, J. et al. Tailored sitting Tai Chi program for subacute stroke survivors: A randomized controlled trial. Stroke 53, 2192–2203. https://doi.org/10.1161/strokeaha.121.036578 (2022).
Tan, T. et al. The novel effectiveness of Tai Chi on cardiopulmonary fitness among stroke patients in the recovery phase: a study protocol for a randomized controlled trial. Trials 22 https://doi.org/10.1186/s13063-021-05565-2 (2021).
Huang J., Wang D. & Wang J. Clinical evidence of Tai Chi exercise prescriptions: a systematic review. Evid. Based Complement Alternat. Med. 2021, 5558805. https://doi.org/10.1155/2021/5558805 (2021).
Lu, X., Hui-Chan, C. W. & Tsang, W. W. Tai Chi, arterial compliance, and muscle strength in older adults. Eur. J. Prev. Cardiol. 20, 613–619 (2013).
Funding
This work was partly supported by Tsinghua University Initiative Scientific Research Program (20235080035 and H20240590) to HY.
Author information
Authors and Affiliations
Contributions
J.L., H.Y., and Y.J. were responsible for the literature research and screening process, data extraction and statistical analysis. J.L. draft the manuscript. H.Y. and Y.J. edited the manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Liu, J., Yu, H. & Jan, YK. A systematic review and meta-analysis of the mechanism of action of Tai Chi on cardiovascular disease: evidence map of aerobic and mind-body exercise pathways. Sci Rep 16, 6708 (2026). https://doi.org/10.1038/s41598-026-35996-3
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-026-35996-3
