
Abstract
Magnetic resonance imaging (MRI) has become an important tool for recommending prostate biopsy (PB) in prostate cancer (PCa) detection. However, the routine use of MRI in patients with previous negative PB remains debatable. This study aimed to evaluate the utility of prostate-specific antigen (PSA) derivatives to guide MRI use and reduce unnecessary scans in such cases. Receiver operating characteristic analysis identified a Prostate Imaging Reporting and Data System score ≥ 4 as the optimal threshold for predicting clinically significant PCa (Gleason score ≥ 7). A cohort of 251 patients with at least one prior negative PB who underwent serum PSA testing, free PSA, and MRI between October 2015 and June 2024 were analyzed. The optimal cutoff values for PSA, PSA density (PSAD), and free-to-total PSA ratio (%fPSA) were 11.87 ng/mL, 0.19 ng/mL2, and 18.76%, respectively (all p < 0.001). Restricting MRI to patients with PSA < 11.87 ng/mL, PSAD < 0.19 ng/mL2, or %fPSA > 18.76% could induce MRI use by 22.7% while missing only 9.1% of significant PCa cases on MRI-targeted PB.
Similar content being viewed by others


Introduction
Prostate cancer (PCa) is the most common malignancy and the second leading cause of cancer-related deaths among men worldwide1. Over the past few decades, serum prostate-specific antigen (PSA)–based screening and subsequent prostate biopsy (PB) have become standard diagnostic practices, despite challenges such as overdiagnosis and overtreatment2,3.
Although transrectal ultrasonography (TRUS)–guided PB (TRUS-PB) has been in use since 19894, its false-negative rate ranges from 20 to 40%5. Consequently, managing patients with prior negative PB remains a significant challenge.
Magnetic resonance imaging (MRI) has emerged as a powerful tool to enhance diagnostic accuracy, particularly in patients with previous negative PB, by reducing unnecessary biopsies6,7,8. Combining MRI-targeted PB with systematic TRUS-PB has been shown to improve cancer detection9.
There is a consensus to perform MRI and subsequent MRI-targeted PB in patients with prior negative PB but persistent clinical suspicion of PCa. The decision to perform an MRI on these patients should consider the results of other biomarkers and the financial burden of the examination 10. Routine use of MRI could impose significant costs on patients and healthcare systems 7,11. Furthermore, the recommendation to conduct MRI-targeted PB after initial negative TRUS-guided PB remains questionable, particularly for patients with PSA < 10 ng/mL, due to low cancer-specific mortality12.
Detection rates for significant PCa on repeat PB following initial negative systematic and MRI-targeted PB range from 10 to 20%13,14,15,16. Therefore, determining appropriate MRI indications in patients with previous negative PB is essential. Although PSA and its derivatives, such as PSA density (PSAD) and the free-to-total PSA ratio (%fPSA), have been suggested as indicators for recommending PB17,18, studies evaluating their utility in minimizing unnecessary MRI remain limited. This study aims to assess the effectiveness of PSA and its derivatives in reducing MRI usage without comprising the detection of PCa in patients with prior negative biopsies.
Materials and methods
Data collection
This single-institution retrospective study was approved by the Institutional Review Board (IRB No. B-2410-f933-105), with a waiver of informed consent. At our institution, all male patients presenting with lower urinary tract symptoms undergo serum PSA testing and TRUS as part of their initial diagnostic workup. An additional serum-free PSA test is reimbursed by Korea’s national insurance when serum PSA levels exceed 2 ng/mL or PCa is suspected based on digital rectal examination or TRUS findings. Further MRI is performed following shared decision-making with the patient.
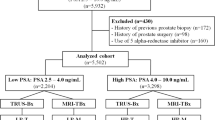
Between October 2015 and June 2024, 1,189 patients underwent repeated PB after serum PSA, free PSA testing, and MRI. Patients with a history of PCa, prostate surgery, prior PB, or use of medications affecting PSA levels (e.g., 5-α reductase inhibitors) were excluded. Ultimately, 251 patients with at least one previous negative PB were included in the study. A Gleason score ≥ 7 was classified as significant PCa.
A visible lesion on MRI was defined as one with a Prostate Imaging Reporting and Data System version 2 (PI-RADSv2) score of ≥ 3, which served as the target for MRI-targeted biopsy. Patients with MRI-visible lesions underwent MRI-targeted transrectal (TR) PB in addition to a systematic 12-core TRUS-PB. Each targeted biopsy included a minimum of two cores per lesion. Patients without visible MRI lesions underwent only systematic 12-core TRUS-PB.
The MRI/TRUS fusion-guided PB protocol used in this study has been described previously19. All patients’ prostate volumes were evaluated based on TRUS. All PB slides were reviewed by genitourinary pathologists with more than 10 yr of experience. The primary outcome was the predictive value of the Prostate Health Index (PHI) for PI-RADSv2 ≥ 3 lesions. Secondary outcomes included the diagnostic accuracy of PHI for overall PCa and significant PCa.
Statistical analysis
All statistical analyses were performed using the R statistical package (version 3.5.1; R Core Team, Vienna, Austria). Receiver operating characteristic (ROC) curves and areas under the curve (AUCs) were used to determine cutoff values for PI-RADSv2 in predicting overall and significant PCa. Cutoff values were defined using sensitivity analysis with the Youden index (sensitivity + specificity − 1). ROC curve analysis also determined optimal cutoff values for PSA and its derivatives in predicting MRI lesions. The DeLong test was used to assess statistical differences in AUCs. Multivariate logistic regression analyses were used to identify predictors for MRI lesions, overall PCa, and significant PCa on MRI-targeted PB cores. All p values were two-sided, with statistical significance set at p < 0.05.
Results
Table 1 presents the baseline demographic and clinicopathological characteristics of the patients. Among 251 patients, 127 (50.6%) patients had visible MRI lesions (PI-RADSv2 ≥ 3). Of these, 125 patients underwent MRI/TRUS fusion PB, while two patients with PI-RADSv2 ≥ 3 lesions and 124 patients without visible lesions underwent only systematic 12-core TRUS-PB. Patients with PI-RADSv2 < 3 lesions were older than those with PI-RADSv2 ≥ 3 (66.4 vs. 62.9 yr; p = 0.001). Higher PSA level (10.02 ± 9.31 ng/mL vs. 6.82 ± 5.39 ng/mL; p = 0.001) and PSAD level (0.26 ± 0.28 ng/mL2 vs. 0.15 ± 0.11 ng/mL2; p < 0.001) were observed in patients with PI-RADSv2 ≥ 3 (Table 1).
ROC curve analysis identified PI-RADSv2 ≥ 4 as the optimal cutoff value for predicting overall PCa (AUC = 0.73, p < 0.001) and significant PCa (AUC = 0.81, p < 0.001; Fig. 1). The optimal cutoff values for predicting PI-RADSv2 ≥ 4 lesions were 11.87 ng/mL for PSA (AUC = 0.63, p < 0.001), 0.19 ng/mL2 for PSAD (AUC = 0.69, p < 0.001), and 18.76% for %fPSA (AUC = 0.63, p < 0.001; Fig. 2).

Receiver operating characteristic curves of prostate-specific antigen (PSA) derivatives, including PSA density (PSAD) and the free-to-total PSA ratio (%fPSA), along with Prostate Imaging Reporting and Data System version 2 (PI-RADSv2) scores on multiparametric magnetic resonance imaging for predicting the presence of (A) overall prostate cancer and (B) clinically significant prostate cancer.

Receiver operating characteristic curve of age, prostate-specific antigen (PSA), prostate volume, PSA density (PSAD), and the free-to-total PSA ratio (%fPSA) for predicting the presence of lesions on multiparametric magnetic resonance imaging with a Prostate Imaging Reporting and Data System version 2 (PI-RADSv2) score ≥ 4.
Multivariable regression analysis showed that older age (odds ratio [OR] = 1.04; 95% confidence interval [95% CI], 1.01–1.08; p = 0.016) and higher PSAD (OR = 154.44; 95% CI, 18.54–1,286.36; p < 0.001) were significantly associated with PI-RADSv2 ≥ 4 lesions (Table 2).
Among 125 patients who underwent combined MRI-targeted PB and systematic 12-core TRUS-PB, PSAD ≥ 0.19 ng/mL and PI-RADSv2 ≥ 4 were independent risk factors for overall PCa (OR = 2.90; 95% CI, 1.24–6.80; p = 0.014, and OR = 10.97; 95% CI, 3.08–39.09; p < 0.001, respectively) and significant PCa (OR = 3.27; 95% CI, 1.28–8.35; p = 0.013, and OR = 11.10; 95% CI, 2.44–50.46; p = 0.002, respectively; Table 3).
Table 4 shows the predictive values of PSA and PSA derivatives for PI-RADSv2 ≥ 3 lesions. Although PSA < 11.87 ng/mL had the highest AUC, significant differences were observed between PSA < 11.87 and PSAD < 0.19 ng/mL2 (p = 0.612) or %fPSA > 18.76% (p = 0.062). Avoiding MRI when PSA < 11.87 ng/mL would reduce MRI use by 45.8%, but 57.6% (19/33) of significant PCa cases could be missed. Using PSAD < 0.19 ng/mL2 and %fPSA > 18.76% as criteria to omit MRI would reduce MRI use by 38.6% and 25.1%, respectively, with a risk of missing 29.5% and 22.7% of significant PCa cases. When combining each cutoff value of PSA and its derivatives, there were no significant differences in the AUC compared with PSA < 11.87 ng/mL alone. However, recommending MRI only for patients with PSA < 11.87 ng/mL, PSAD < 0.19 ng/mL2, and %fPSA > 18.76% could reduce MRI utilization by 22.7%, with a minimal risk (9.1% or 3/33 cases) of missing significant PCa by omitting MRI-targeted PB.
Discussion
Current guidelines recommend prostate MRI for patients with previous negative PB and ongoing suspicion of PCa20. A prior meta-analysis reported that the negative predictive value of MRI for detecting Gleason score ≥ 7 PCa was 90.8% when MRI-negative cases were defined as PI-RADSv2 < 321. The current guideline20 suggested that the cutoff value of Likert/PI-RADS ≥ 3 to recommend PB could reduce 30% of unnecessary PB while missing 11% of clinically significant PCa. For patients with previous negative PB, the incidences of clinically significant PCa were 5.6%, 13.6%, 33.6% and 70.3% in those with PI-RADS < 3, 3, 4, and 5 lesions22.
In this study, ROC curve analysis determined that the optimal PI-RADSv2 cutoff value for predicting both overall and significant PCa was 4, aligning with prior research findings22. Thus, we aimed to assess optimal PSA and PSA derivative cutoff values for identifying PI-RADSv2 ≥ 4 lesions on MRI. The cutoff values for predicting PI-RADSv2 ≥ 4 lesions were 11.87 ng/mL for PSA, 0.19 ng/mL2 for PSAD, and 18.76% for %fPSA. Among these markers, PSAD demonstrated the highest AUC.
Multivariate logistic regression analysis indicated that PSAD and older age were associated with the presence of PI-RADSv2 ≥ 4 lesions. After adjusting for other clinicopathologic factors, PSAD ≥ 0.19 ng/mL and PI-RADSv2 ≥ 4 lesions were identified as independent risk factors for overall and significant PCa on MRI-targeted biopsy. These results are consistent with prior studies highlighting PSAD and MRI suspicion scores as significant predictors of cancer detection23.
Although PSAD < 0.19 ng/mL2 had the highest AUC for predicting PI-RADSv2 ≥ 4 lesions, using this criterion to omit MRI could reduce MRI use by 38.6% but carried a 30.3% risk of missing significant PCa. Including %fPSA > 18.76% alongside PSAD < 0.19 ng/mL2 as a triage tool showed no significant change in AUC for predicting PI-RADSv2 ≥ 4 but reduced the risk of missing significant PCa to 9.1% while decreasing MRI use by 23.1%. Recommending MRI for patients with PSA ≥ 11.87 ng/mL, PSAD ≥ 0.19 ng/mL2, or %fPSA ≤ 18.76% resulted in a 22.7% reduction in MRI use, with a 9.1% risk of missing significant PCa.
The result of our study is comparable to those of previous studies. For overall population, the triage strategy utilizing PSA and its derivatives to recommend MRI could reduce 24.6–33.9% of MRI, with the risk of missing 4.2–9.5% of clinically significant PCa24. In addition, a recent study based on the Prostate Cancer Disease Observation (PRECISION) cohort25 reported that utilizing Rotterdam Prostate Cancer Risk Calculator (RPCRC) could reduce 34.9% of unnecessary MRI at the cost of missing 15.7% of clinically significant PCa. For patients with previous negative PB, utilizing RPCRC could reduce 51% of MRI at the cost of missing 10% of high-grade PCa24.
Although the risk of PCa in patients with previously negative PB is relatively lower than PB-naive men22, MRI and subsequent targeted PB should be determined based on patient shared decision making, considering the risk of missing clinically significant PCa.
The findings of this study should be interpreted cautiously due to several limitations, including the retrospective, single-institution design. Interobserver variability in MRI interpretation using PI-RADS remains a concern, recommending the agreement among well-experienced radiologists26. Although the radiologists in our institution are well-experienced over 20 years, the possibility of interobserver discrepancy highlights the need for multicenter studies with centralized MRI interpretation review system to validate our results. Additionally, novel biomarkers such as the PHI, PHI density27, and PCa antigen 3 gene28 were not evaluated. Considering that those novel biomarkers showed superiority to conventional PSA derivatives in prediction of PCa, the combination of such biomarkers into criteria might enhance the negative predictive value, minimizing the potential risk to miss clinically significant PCa. Further study including such novel biomarkers should be performed. Meanwhile, all biopsies in this study were performed via the TR route, which may have influenced the detection accuracy. Previous research suggests that transperineal (TP) biopsy offers equal or superior detection rates compared with TR biopsy and TP biopsy could potentially reduce unnecessary MRIs29,30. Furthermore, given the low cancer-specific mortality in patients with prior negative biopsies12, longer followup studies are needed to evaluate ultimate cost-effectiveness and survival analysis of clinical progression. Despite these limitations, this study is, to the best of our knowledge, the first to evaluate the use of PSA and PSA derivatives as a triage tool to reduce unnecessary MRI in patients with prior negative biopsy.
Conclusions
In patients with prior negative prostate biopsy, limiting MRI to cases with PSA < 11.87 ng/mL, PSAD < 0.19 ng/mL, and %fPSA > 18.76% can reduce MRI use by 22.7%, with a 9.1% risk of missing significant PCa. However, those criteria for MRI recommendation should be adjusted based on the other novel biomarkers or individual patient characteristics and preferences.
Data availability
The materials datasets used and/or analyzed during this study are available from the corresponding author upon reasonable request.
References
Bray, F. et al. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 74, 229–263 (2024).
Welch, H. G. et al. Reconsidering prostate cancer mortality—The future of PSA screening. N. Engl. J. Med. 382, 1557–1563 (2020).
Van Poppel, H. et al. Serum PSA-based early detection of prostate cancer in Europe and globally: Past, present and future. Nat. Rev. Urol. 19, 562–572 (2022).
Hodge, K. K. et al. Random systematic versus directed ultrasound guided transrectal core biopsies of the prostate. J. Urol. 142, 71–74 (1989).
Perera, M. et al. Management of men with previous negative prostate biopsy. Curr. Opin. Urol. 26, 481–487 (2016).
Abd-Alazeez, et al. The accuracy of multiparametric MRI in men with negative biopsy and elevated PSA level—can it rule out clinically significant prostate cancer?. Urol. Oncol. 32(45), e17-22 (2014).
Hutchinson, R. C. et al. The economic effect of using magnetic resonance imaging and magnetic resonance ultrasound fusion biopsy for prostate cancer diagnosis. Urol. Oncol. 34, 296–302 (2016).
Kim, E. H. et al. Should men undergo MRI before prostate biopsy—CON. Urol. Oncol. 41, 92–95 (2023).
Ahdoot, M. et al. MRI-targeted, systematic, and combined biopsy for prostate cancer diagnosis. N Engl. J. Med. 382, 917–928 (2020).
Rosenkrantz, A. B. et al. Prostate magnetic resonance imaging and magnetic resonance imaging targeted biopsy in patients with a prior negative biopsy: A consensus statement by AUA and SAR. J. Urol. 196, 1613–1618 (2016).
Kim, S. J. et al. Challenges in adopting level 1 evidence for multiparametric magnetic resonance imaging as a biomarker for prostate cancer screening. JAMA Oncol. 4, 1663–1664 (2018).
Kawa, S. M. et al. A Nationwide analysis of risk of prostate cancer diagnosis and mortality following an initial negative transrectal ultrasound biopsy with long-term follow-up. J. Urol. 208, 100–108 (2022).
Venderink, W. et al. Yield of repeat targeted direct in-bore magnetic resonance-guided prostate biopsy (MRGB) of the same lesions in men having a prior negative targeted MRGB. Korean J. Radiol. 19, 733–741 (2018).
Pepe, P. et al. Early second round targeted biopsy of PI-RADS score 3 or 4 in 256 men with persistent suspicion of prostate cancer. In Vivo 33, 897–901 (2019).
Wallstrom, J. et al. Prostate cancer screening with magnetic resonance imaging: Results from the second round of the Goteborg prostate cancer screening 2 trial. Eur. Urol. Oncol. 5, 54–60 (2022).
Barletta, F. et al. How to optimize follow-up in patients with a suspicious multiparametric MRI and a subsequent negative targeted prostate biopsy. Results from a large, single-institution series. Urol. Oncol. 40, 103 (2022).
Djavan, B. et al. Optimal predictors of prostate cancer on repeat prostate biopsy: A prospective study of 1051 men. J. Urol. 163, 1144–1148 (2000) (discussion 1148–1149).
Ploussard, G. et al. Risk of repeat biopsy and prostate cancer detection after an initial extended negative biopsy: Longitudinal follow-up from a prospective trial. BJU Int. 111, 988–996 (2013).
Hwang, S. I. et al. Value of MR-US fusion in guidance of repeated prostate biopsy in men with PSA < 10 ng/mL. Clin. Imaging. 53, 1–5 (2019).
Mottet, N. et al. EAU-EANM-ESTRO-ESUR-SIOG Guidelines on prostate cancer-2020 update. Part 1: screening, diagnosis, and local treatment with curative intent. Eur. Urol. 79, 243–262 (2021).
Sathianathen, N. J. et al. Negative predictive value of multiparametric magnetic resonance imaging in the detection of clinically significant prostate cancer in the prostate imaging reporting and data system era: A systematic review and meta-analysis. Eur. Urol. 78, 402–414 (2020).
Patel, H. D. et al. Risk of prostate cancer for men with prior negative biopsies undergoing magnetic resonance imaging compared with biopsy-naive men: A prospective evaluation of the PLUM cohort. Cancer 128, 75–84 (2022).
Vourganti, S. et al. Multiparametric magnetic resonance imaging and ultrasound fusion biopsy detect prostate cancer in patients with prior negative transrectal ultrasound biopsies. J. Urol. 188, 2152–2157 (2012).
Soeterik, T. F. W. et al. Personalised prostate cancer diagnosis: Evaluating biomarker-based approaches to reduce unnecessary magnetic resonance imaging and biopsy procedures. Eur. Urol. Open Sci. 75, 106–119 (2025).
Remmers, S. et al. Reducing biopsies and magnetic resonance imaging scans during the diagnostic pathway of prostate cancer: Applying the Rotterdam prostate cancer risk calculator to the PRECISION trial data. Eur. Urol. Open Sci. 36, 1–8 (2021).
Rosenkrantz, A. B. et al. Interobserver reproducibility of the PI-RADS version 2 Lexicon: A multicenter study of six experienced prostate radiologists. Radiology 280, 793–804 (2016).
Liu, A. Q. et al. Initial prostate health index (PHI) and PHI density predicts future risk of clinically significant prostate cancer in men with initial negative prostate biopsy: A 6-year follow-up study. Prostate Cancer Prostatic. Dis. 25, 684–689 (2022).
Pagniez, M. A. et al. Predictive factors of missed clinically significant prostate cancers in men with negative magnetic resonance imaging: A systematic review and meta-analysis. J. Urol. 204, 24–32 (2020).
Kaneko, M. et al. Transperineal vs transrectal magnetic resonance and ultrasound image fusion prostate biopsy: A pair-matched comparison. Sci. Rep. 13, 13457 (2023).
Oderda, M. et al. Transrectal versus transperineal prostate fusion biopsy: A pair-matched analysis to evaluate accuracy and complications. World J. Urol. 42, 535 (2024).
Acknowledgements
This work was supported by the research fund of Hanyang University (HY-202500000003683)
Author information
Authors and Affiliations
Contributions
S.L. and B.S. contributed to project development. S.L and B.S. conducted data analysis. S.L., H.R., and B.S. were responsible for manuscript writing and editing. S.H.S., S.I.H., and H.J.L. managed data collection and analysis. S.K.H., and S.S.B. performed the critical review. B.S. supervised the study.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Research involving human participants and/or animals
This study was approved by the Seoul National University Bundang Hospital Institutional Review Board (IRB No. B-2410-933-105). It did not involve animal subjects. All procedures followed the ethical standards of the institutional and national research committees and the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Informed consent
Due to the retrospective nature of the study, Seoul National University Bundang Hospital Institutional Review Board waived the need of obtaining informed consent.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Lee, S., Ryu, H., Song, S.H. et al. Utility of prostate-specific antigen derivatives to minimize unnecessary magnetic resonance imaging in patients with prior negative prostate biopsy. Sci Rep 16, 5202 (2026). https://doi.org/10.1038/s41598-026-36242-6
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-026-36242-6
