
Abstract
Mac-2-binding protein glycosylation isomer (M2BPGi), a promising biomarker for predicting hepatocellular carcinoma (HCC), was evaluated in predicting HCC occurrence after hepatitis C virus (HCV) cure with direct-acting antivirals (DAAs). 704 eligible patients underwent biannual surveillance, including alpha-fetoprotein (AFP) and liver imaging studies, to detect HCC occurrence. Serum M2BPGi levels were measured at both pretreatment and sustained virologic response (SVR12). The cumulative HCC incidence was estimated by Kaplan-Meier analysis, and risk factors by Cox proportional hazards models. During a median follow-up of 4.5 years, 50 patients (7.1%) developed HCC, with cumulative incidence rates of 7.8% and 12.8% at 5 and 10 years. HCC incidence was higher in patients with pretreatment M2BPGi ≥ 4.0 and SVR12 ≥ 2.0 (p < 0.001). Multivariable analysis identified that M2BPGi levels ≥ 4.0 COI at pretreatment (adjusted hazard ratio [aHR]: 3.33; 95% confidence interval [CI]: 1.54–7.23, p = 0.002) and ≥ 2.0 COI at SVR12 (aHR: 2.60; 95% CI: 1.16–5.79, p = 0.020) were significantly associated with HCC occurrence in addition to age, sex, liver stiffness measurement (LSM), alanine transaminase (ALT) quotient, and AFP. In conclusion, serum M2BPGi may serve as a valuable biomarker for HCC risk after HCV cure with DAAs.
Similar content being viewed by others
Introduction
Hepatitis C virus (HCV) affects an estimated 50 million people globally1. Although the prevalence of HCV has declined in the era of direct-acting antivirals (DAAs), with the sustained virologic response at off-treatment week 12 (SVR12) exceeding 95%, its complications – such as cirrhosis, hepatic decompensation, and hepatocellular carcinoma (HCC) - continue to pose significant global health and economic burdens2. Currently, primary liver cancer ranks as the sixth most commonly diagnosed cancer and the third leading cause of cancer-related deaths worldwide3. Screening tools, such as ultrasonography alone or in combination with alpha-fetoprotein (AFP), offer a sensitivity of approximately 43% and 65% for early-stage HCC, respectively4. Consequently, the development of effective risk stratification tools and the identification of early predictive biomarkers for accurate HCC screening are crucial areas of ongoing research5.
Mac-2-binding protein glycosylation isomer (M2BPGi) is considered a noninvasive biomarker for predicting fibrosis stage and HCC6,7,8,9,10,11,12,13,14,15,16,17,18. Beyond these applications, recent research has expanded its role in predicting gastroesophageal varices (GOVs) and post-hepatectomy liver failure (PHLF) in chronic liver diseases19,20. However, M2BPGi levels vary depending on the underlying diseases and presence or absence of SVR12, making it challenging to establish a definite cutoff value for predicting HCC development. For instance, patients with pretreatment M2BPGi levels of ≥ 4.0 showed an increased risk of HCC development compared to those with lower levels, regardless of fibrosis stage10. Additionally, the cutoff value was adjusted to 1.75-2.0 for predicting HCC occurrence or recurrence after achieving SVR1213,15,18. While M2BPGi has been shown to correlate with HCC development in the literature, nearly all studies were conducted in Japan, highlighting the need for external validation of M2BPGi in predicting HCC risk among patients with HCV. To address this unmet medical need, we conducted an independent cohort study to validate the clinical utility of M2BPGi in predicting HCC occurrence among patients who achieved HCV cure with DAAs.
Materials and methods
Patients
From January 2014 to February 2025, we conducted a retrospective review of a prospective cohort, recruiting patients aged ≥ 18 years who had been previously diagnosed with chronic HCV infection. Chronic HCV infection was defined as the presence of detectable HCV antibody (anti-HCV) (Abbott HCV EIA 2.0®, Abbott Laboratories, Abbott Park, Illinois, USA) and quantifiable serum HCV ribonucleic acid (RNA) (Cobas TaqMan HCV Test v2.0®, Roche Diagnostics, Mannheim, Germany, lower limit of quantification (LLOQ): 15 IU/mL) for ≥ 6 months at the National Taiwan University Hospital (NTUH), NTUH Yun-Lin Branch and NTUH Hsin-Chu Branch.
Patients were excluded from the study if they had hepatitis B virus (HBV) coinfection, identified by the presence of HBV surface antigen (HBsAg) using the Abbott Architect HBsAg qualitative assay (Abbott Laboratories, Abbott Park, Illinois, USA) or human immunodeficiency virus (HIV) coinfection, identified by the presence of anti-HIV using the Abbott Architect HIV Ag/Ab Combo (Abbott Laboratories, Abbott Park, Illinois, USA); increased alcohol consumption (≥ 140 g/week for females and ≥ 210 g/week for males); decompensated cirrhosis (Child–Pugh B or C); a history of HCC; had undergone organ transplantation; failed to achieve SVR12 following DAA therapy; or declined or were unable to provide written informed consent. Additionally, patients who lacked paired serum samples for M2BPGi assessment or had a post-SVR12 follow-up period of < 6 months were also excluded.
The study received approval from the Research Ethics Committee of NTUH, and was conducted in accordance with the ethical principles and guidelines outlined in the Declaration of Helsinki21. Informed consent was obtained from all subjects and/or their legal guardians.
Study design
Patients’ demographic and clinical characteristics were recorded at baseline and at the SVR12 time point, including age, sex, platelet count, serum albumin, total bilirubin, alanine transaminase (ALT), AFP, serum HCV RNA level, and HCV genotype (Roche Cobas HCV GT®, Roche Diagnostics, Mannheim, Germany or Abbott RealTime HCV GT II®, Abbott Laboratories, Abbott Park, Illinois, USA)22. The upper limits of normal (ULNs) for ALT levels were 30 for men and 19 for women, respectively23. Liver stiffness measurement (LSM) was assessed using vibration-controlled transient elastography (VCTE) (FibroScan®, Echosens, Paris, France) equipped with an M or XL probe. A pretreatment LSM cutoff value of ≥ 9.5 kPa was used to define advanced hepatic fibrosis (≥ F3)24. Serum M2BPGi levels were semi-quantified by a Wisteria floribunda agglutinin (WFA)-antibody sandwich immunoassay on an automated HISCL-800 immunoanalyzer (Sysmex Co., Kobe, Japan). Results were expressed as a cutoff index (COI) using the following formula: ([M2BPGi]sample- [M2BPGi]NC)/ ([M2BPGi]PC - [M2BPGi]NC), where NC and PC represent the negative and positive controls8.
All patients underwent ultrasonography and serum AFP testing for HCC surveillance at semiannual intervals from the SVR12 time point to the last visit. The diagnosis of HCC was confirmed using various diagnostic methods such as contrast-enhanced computed tomography (CT), magnetic resonance imaging (MRI), hepatic angiography, or histology when appropriate. All diagnostic procedures adhered to standardized criteria recommended by the American Association for the Study of Liver Diseases (AASLD) Practice Guidance. 3
Statistical analysis
Statistical analyses were performed using RStudio (version 2024.09.0 + 375). Patient characteristics at pretreatment and the SVR12 time point were presented as median (interquartile range [IQR]) for continuous variables and as counts (percentages) for categorical variables. Comparison of the characteristics before and after antiviral treatment were conducted using the Wilcoxon signed rank test for continuous variables and Pearson’s chi-squared test for categorical variables, as appropriate.
We reported the prevalence rate, which was shown as percentage, as well as the incidence rate, which was shown as per 100 person-years of follow-up (PYFU) with 95% confidence interval (CI), for the entire population. The cumulative incidence rates of HCC occurrence were reported using the Kaplan-Meier method for patients with M2BPGi cutoff levels of 4.0 COI at pretreatment and 2.0 COI at the SVR12, respectively. In addition to analyzing the entire population, we stratified the comparison of the cumulative HCC incidence rate based on patients with LSM of ≥ 9.5 kPa and < 9.5 kPa at pretreatment and SVR12, respectively. Finally, we calculated the cumulative HCC incidence by categorizing patients into three groups based on the dynamic changes in M2BPGi levels at both pretreatment and SVR12. Category 1 consisted patients with M2BPGi < 4.0 COI at pretreatment and < 2.0 COI at SVR12; Category 2 consisted those with M2BPGi < 4.0 COI at pretreatment but ≥ 2.0 COI at SVR12; Category 3 consisted those with M2BPGi ≥ 4.0 COI at pretreatment but < 2.0 COI at SVR12; Category 4 consisted those with M2BPGi ≥ 4.0 at pretreatment and ≥ 2.0 COI at SVR12. All comparisons were performed using the long-rank test. Univariable Cox proportional hazards models were used to evaluate the association between HCC occurrence and potential risk factors at pretreatment and SVR12 for the entire cohort. Results were reported as crude hazard ratios (cHRs) with 95% CIs. Multivariable Cox proportional hazards models were conducted to identify independent predictors of HCC occurrence, with results reported as adjusted hazard ratios (aHRs) with 95% CI. We built two multivariable hazards models: a full model, in which all factors of interest - regardless of their p values in the univariable hazards model - were included to assess the relationship between potential confounders and outcomes, and a backward stepwise Akaike information criterion (AIC) model, which was used to identify the most optimal subset of predictors by balancing model complexity and goodness-of-fit25.
All statistical analyses were two-tailed, with statistical significance defined as a p-value < 0.05.
Results
Patient characteristics
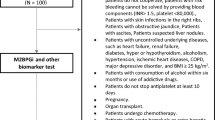
Of the 1165 patients receiving DAAs for chronic HCV infection, 357 were excluded from the study due to HBV coinfection (n = 47), HIV coinfection (n = 129), increased alcohol intake (n = 15), decompensated cirrhosis (n = 20), a history of HCC (n = 62), organ transplantation (n = 31), failure to achieve SVR12 (n = 32), or decline/unable to provide informed consent (n = 21). Among the remaining 888 patients, 104 were also excluded due to unavailable paired serum M2BPGi samples (n = 36) and a post-SVR12 follow up < 6 months (n = 68). Ultimately, 704 eligible patients were included in the study (Fig. 1).

Study flow. HCV, hepatitis C virus; DAA, direct-acting antivirals; HBV, hepatitis B virus; HIV, human immunodeficiency virus; HCC, hepatocellular carcinoma; SVR12, sustained virologic response at off-treatment week 12; M2BPGi, Mac-2 binding protein glycosylation isomer.
Table 1 presents patients characteristics at both the pretreatment and SVR12 time point. Compared to pretreatment status, patients at the SVR12 time point were older and exhibited significantly lower levels of liver stiffness measurement (LSM), M2BPGi, total bilirubin, ALT quotient, and AFP, while showing higher platelet counts and albumin levels (p < 0.001). Furthermore, the proportions of patients with LSM ≥ 9.5 kPa, M2BPGi ≥ 4.0 or ≥ 2.0 COI, ALT ≥ 2 or ≥ 1 ULN, and AFP ≥ 10 or ≥ 6 ng/mL were significantly lower at SVR12 compared to pretreatment (p < 0.001). In contrast, the proportions of patients with platelet counts < 100 × 10⁹/L or < 150 × 10⁹/L were significantly higher at pretreatment than at the SVR12 time point (p < 0.001). The median (IQR) duration of post-SVR12 follow-up was 4.5 (2.0–6.0) years.
Risk of HCC occurrence following the attainment of HCV cure
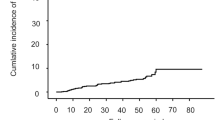
During a total of 3214.25 PYFU, 50 of the 704 patients (7.1%) in the entire population developed de novo HCC. The incidence rate of HCC was 1.56 (95% CI: 1.17–2.07) per 100 PYFU. Additionally, the cumulative incidence rates at 5 and 10 years post-SVR12 were 7.8% (95% CI: 5.5%-10.1%) and 12.8% (95% CI: 9.2%-17.1%), respectively.
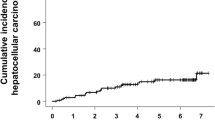
The incidence rates of HCC were 7.83 (5.57–10.90) per 100 PYFU among patients with a pretreatment M2BPGi level ≥ 4.0 COI and 0.67 (0.43–1.05) per 100 PYFU among those with a pretreatment M2BPGi level of < 4.0 COI. The cumulative HCC incidence rate was significantly higher among patients with a pretreatment M2BPGi level ≥ 4.0 COI compared to those with a pretreatment M2BPGi level of < 4.0 COI (p < 0.001) (Fig. 2A). For patients with a pretreatment M2BPGi level ≥ 4.0 COI, the cumulative incidence rates were 31.7% (95% CI: 20.6%-41.3%) at 5 years and 52.8% (95% CI: 31.0%-67.7%) at 10 years post-SVR12. Moreover, significant differences in cumulative HCC incidence were observed at the M2BPGi cutoff of 4.0 COI in subgroups based on pretreatment LSM: patients with LSM < 9.5 kPa (p = 0.0017) and those with LSM ≥ 9.5 kPa (p = 0.00044) (Fig. 2B and C).


Cumulative incidence rates of HCC with 95% CI according to the pretreatment M2BPGi cutoff level of 4.0 COI. The p values of the log-rank test were < 0.001 in the entire population (A); = 0.0017 in patients with pretreatment LSMs < 9.5 kPa (B); = 0.00044 in patients with pretreatment LSMs ≥ 9.5 kPa (C).
At SVR12, the incidence rates of HCC were 6.28 (4.55–8.61) per 100 PYFU among patients with an M2BPGi level ≥ 2.0 COI and 0.56 (0.34–0.92) per 100 PYFU among those with an M2BPGi level of < 2.0 COI. The cumulative incidence rate of HCC was significantly higher among patients with an M2BPGi level ≥ 2.0 COI compared to those with an M2BPGi level of < 2.0 COI (p < 0.001) (Fig. 3A). Among patients with an M2BPGi level ≥ 2.0 COI at SVR12, the cumulative incidence rates were 28.5% (95% CI: 19.1%-36.9%) at 5 years and 42.9% (95% CI: 27.3%-55.2%) at 10 years post-SVR12. Additionally, significant differences in cumulative HCC incidence at the M2BPGi cutoff of 2.0 COI at SVR12 were observed in subgroups based on LSM: patients with LSM < 9.5 kPa (p = 0.0097) and those with LSM ≥ 9.5 kPa (p = 0.00061) (Fig. 3B and C).


Cumulative incidence rates of HCC with 95% CI according to the M2BPGi cutoff level of 2.0 COI at the time point of SVR12. The p values of the log-rank test were < 0.001 in the entire population (A); = 0.0097 in patients with pretreatment LSMs < 9.5 kPa (B); = 0.00061 in patients with pretreatment LSMs ≥ 9.5 kPa (C).
When the dynamic changes in M2BPGi levels were taken into consideration, patients in Category 4 patients carried the highest HCC risk, distinct from the intermediate risk observed in Categories 2 and 3, while Category 1 patients had the lowest HCC risk. (p < 0.001; Fig. 4).

Cumulative incidence rates of HCC with 95% CI according to the dynamic changes of M2BPGi levels of 4.0 at pretreatment and 2.0 COI at the time point of SVR12. The p values of the log-rank test were < 0.001 in patients with Categories 1 to 4.
Pretreatment factors associated with HCC occurrence
A pretreatment M2BPGi level ≥ 4.0 COI (cHR: 11.25 [95% CI: 6.36–19.92], p < 0.001), LSM ≥ 9.5 kPa (cHR: 9.68 [95% CI: 5.05–18.56], p < 0.001), age ≥ 60 years (cHR: 4.17 [95% CI: 2.21–7.84], p < 0.001), platelet count < 100 × 10⁹/L (cHR: 4.62 [95% CI: 2.55–8.37], p < 0.001), ALT ≥ 2-fold ULN (cHR: 8.18 [95% CI: 2.94–12.75], p < 0.001), and AFP ≥ 10 ng/mL (cHR: 7.68 [95% CI: 4.38–13.47], p < 0.001) were all significantly associated with HCC in the univariable Cox proportional hazards model. In contrast, male sex (cHR: 0.97 [95% CI: 0.55–1.70], p = 0.97), HCV genotype 1 (cHR: 1.67 [95% CI: 0.90–3.09], p = 0.11), and HCV RNA level > 2,000,000 IU/mL (cHR: 0.99 [95% CI: 0.57–1.73], p = 0.99) were not significantly associated with HCC (Table 2).
In the full multivariable Cox proportional hazards model, M2BPGi ≥ 4.0 COI (aHR: 2.70 [95% CI: 1.15–6.35], p = 0.022), LSM ≥ 9.5 kPa (aHR: 2.64 [95% CI: 1.07–6.51], p = 0.035), male sex (aHR: 1.99 [95% CI: 1.08–3.66], p = 0.027), age ≥ 60 years (aHR: 2.78 [95% CI: 1.38–5.64], p = 0.004), and ALT ≥ 2 folds ULN (aHR: 5.21 [95% CI: 1.80-15.15], p = 0.002) with an AIC value of 515.85 were independently associated with HCC. Using a backward stepwise AIC selection model, M2BPGi ≥ 4.0 COI (aHR: 3.33 [95% CI: 1.54–7.23], p = 0.002), LSM ≥ 9.5 kPa (aHR: 3.00 [95% CI: 1.26–7.17], p = 0.013), male sex (aHR: 1.97 [95% CI: 1.09–3.57], p = 0.026), age ≥ 60 years (aHR: 2.88 [95% CI: 1.43–5.78], p = 0.003), and ALT ≥ 2-fold ULN (aHR: 5.60 [95% CI: 1.98–15.89], p = 0.001) with an improved AIC value of 509.82 were independently associated with HCC (Table 2).
Factors at the SVR12 time point associated with HCC occurrence
M2BPGi ≥ 2.0 COI (cHR: 10.83 [95% CI: 5.91–19.84], p < 0.001), LSM ≥ 9.5 kPa (cHR: 8.29 [95% CI: 4.63–14.82], p < 0.001), age ≥ 60 years (cHR: 3.77 [95% CI: 1.99–7.04], p < 0.001), platelet count < 150 × 109/L (cHR: 5.47 [95% CI: 3.07–9.74], p < 0.001), ALT ≥ ULN (cHR: 3.22 [95% CI: 1.85–5.60], p < 0.001), and AFP ≥ 6 ng/mL (cHR: 8.12 [95% CI: 4.66–14.17], p < 0.001) were significantly associated with HCC in the univariable Cox proportional hazards model. Additionally, male sex (cHR: 0.97 [95% CI: 0.55–1.70], p = 0.91) was not associated with HCC (Table 3).
In the full multivariable Cox proportional hazards model, M2BPGi ≥ 2.0 COI (aHR: 2.56 [95% CI: 1.14–5.76], p = 0.023), LSM ≥ 9.5 kPa (aHR: 2.56 [95% CI: 1.09–6.03], p = 0.031), age ≥ 60 years (aHR: 2.53 [95% CI: 1.29–4.97], p = 0.007), and AFP ≥ 6 ng/mL (aHR: 3.55 [95% CI: 1.89–6.70], p < 0.001) with an AIC value of 511.21 were independently associated with HCC. Using a backward stepwise AIC selection model, M2BPGi ≥ 2.0 COI (aHR: 2.60 [95% CI: 1.16–5.79], p = 0.020), LSM ≥ 9.5 kPa (aHR: 2.58 [95% CI: 1.10–6.06], p = 0.029), age ≥ 60 years (aHR: 2.52 [95% CI: 1.28–4.94], p = 0.007), and AFP ≥ 6 ng/mL (aHR: 3.63 [95% CI: 1.99–6.62], p < 0.001) with an improved AIC value of 509.25 were independently associated with HCC (Table 3).
Association of pretreatment factors and dynamic M2BPGi levels with HCC occurrence
In the univariable Cox proportional hazards model, Category 4 (cHR: 16.34 [95% CI: 8.49–31.45], p < 0.001), Category 3 (cHR: 7.60 [95% CI: 1.71–33.72], p = 0.008), and Category 2 (cHR: 5.55 [95% CI: 2.11–14.60)], p < 0.001) were significantly associated with HCC, along with other factors detailed in Table 2.
In the full multivariable Cox proportional hazards model, M2BPGi Category 4 (aHR: 4.60 [95% CI: 1.65–12.82], p = 0.004), male sex (aHR: 2.24 [95% CI: 1.19–4.19], p = 0.012), age ≥ 60 years (aHR: 2.66 [95% CI: 1.31–5.40], p = 0.007), and ALT ≥ 2-fold ULN (aHR: 5.33 [95% CI: 1.82–15.56], p = 0.002) remained independently associated with HCC, with an AIC value of 514.68. Using a backward stepwise AIC selection model, M2BPGi Category 4 (aHR: 5.60 [95% CI: 2.14–14.62], p < 0.001) remained significant, while Category 3 (aHR: 2.05 [95% CI: 0.39–10.70], p = 0.40), and Category 2 (aHR: 2.54 [95% CI: 0.86–7.53], p = 0.09) showed borderline significance. Male sex (aHR: 2.14 [95% CI: 1.17–3.90], p = 0.013), age ≥ 60 years (aHR: 2.70 [95% CI: 1.34–5.43], p = 0.006), and ALT ≥ 2-fold ULN (aHR: 5.62 [95% CI: 1.98–15.98], p = 0.001) were independently associated with HCC, with an improved AIC value of 508.76 (Table 4). LSM ≥ 9.5 kPa (aHR: 2.27 [95% CI: 0.89–5.81], p = 0.09) showed borderline significance in the backward selection model.
Association of factors at SVR12 and dynamic M2BPGi levels with HCC occurrence
In the univariable Cox proportional hazards model, Category 4 (cHR: 16.34 [95% CI: 8.49–31.45], p < 0.001), Category 3 (cHR: 7.60 [95% CI: 1.71–33.72], p = 0.008), and Category 2 (cHR: 5.55 [95% CI: 2.11–14.60)], p < 0.001) were significantly associated with HCC, along with other factors detailed in Table 3.
In the full multivariable model, M2BPGi Category 4 remained significant (aHR: 4.08 [95% CI: 1.42–11.69], p = 0.009), while M2BPGi Category 3 (aHR: 2.62 [95% CI: 0.48–14.25], p = 0.27), and M2BPGi Category 2 (aHR: 2.82 [95% CI: 0.96–8.33], p = 0.06) showed borderline significance. Male sex (aHR: 1.86 [95% CI: 1.02–3.39], p = 0.042), age ≥ 60 years (aHR: 2.91 [95% CI: 1.44–5.87], p = 0.003) and AFP ≥ 6 ng/mL (aHR: 3.07 [95% CI: 1.58–5.94], p = 0.001) persisted as independent predictors, while LSM ≥ 9.5 kPa, platelet count < 150 109/L, and ALT ≥ ULN were no longer significant in this model. Using a backward stepwise AIC selection model, M2BPGi Category 4 (aHR: 5.30 [95% CI: 2.29–12.26], p < 0.001) and Category 2 (aHR: 3.29 [95% CI: 1.17–9.22], p = 0.023) remained significant, while Category 3 (aHR: 2.93 [95% CI: 0.60-14.28], p = 0.18) showed borderline significance. Age ≥ 60 years (aHR: 2.62 [95% CI: 1.33–5.15], p = 0.005), and AFP ≥ 6 ng/mL (aHR: 3.45 [95% CI: 1.84–6.45], p < 0.001) were significantly associated with HCC, while male sex (aHR: 1.71 [95% CI: 0.96–3.05], p = 0.07) and platelet count < 150 × 10⁹/L (cHR: 1.71 [95% CI: 0.87–3.38], p = 0.12) showed borderline significance (Table 5).
Discussion
Compared to interferon (IFN)-based treatment, which is limited by suboptimal antiviral responses and tolerability, the introduction of safe and potent DAAs has significantly advanced HCV management. This pharmacological breakthrough has led the World Health Organization (WHO) to set ambitious targets for HCV elimination by 2030, including 90% of cases diagnosed, 80% of eligible individuals treated, and a 65% reduction in HCV-related mortality26. While universal screening and efficient linkage to care are essential for reducing HCV prevalence and incidence, continued vigilance following the HCV cure - particularly the early detection of HCC among high-risk individuals - remains critical for achieving the goal of HCV elimination.
Our study confirmed and validated the clinical utility of serum M2BPGi levels - measured either at pretreatment or at the SVR12 time point - in predicting HCC occurrence following HCV cure27. Consistent with findings from two independent cohorts in Japan, which reported that a pretreatment M2BPGi level ≥ 4.0-4.2 COI was associated with increased HCC risk, we demonstrated that the risk of HCC occurrence significantly increased when the pretreatment M2BPGi cutoff was set at 4.0 COI. This association remained significant after adjusting for various known risk factors, including LSM, sex, age, platelet count, ALT quotient, and AFP10,11. Importantly, the predictive role of M2BPGi for HCC remained robust even when the pretreatment severity of hepatic fibrosis was accounted for, as shown in our cumulative incidence and Cox proportional hazards model analyses10. Additionally, we showed that an M2BPGi level ≥ 2.0 COI at the SVR12 time point was predictive of HCC occurrence, aligning with prior studies that identified M2BPGi cutoff values between 1.75 and 2.0 COI as significant predictors of HCC risk13,14,15,16.
To date, numerous studies have demonstrated that mean or median levels of serum M2BPGi levels around 4.0 COI correlate with a hepatic fibrosis stage of ≥ F3 in patients with HCV6,7,8,10,11,20,28. Because M2BPGi levels reflect both hepatic inflammation and fibrosis, they tend to decrease significantly shortly after DAA treatment - primarily due to the rapid resolution of hepatic inflammation rather than fibrosis8,28,29. This dynamic is supported by a recent study showing a decrease in the median serum M2BPGi level from 3.93 COI before antiviral treatment to 1.93 COI after HCV cure among individuals with a pretreatment fibrosis stage of ≥ F38. Although the risk of HCC decreases after DAA-induced viral cure, patients with a pretreatment fibrosis stage of ≥ F3 continue to have a substantial residual risk. This may be attributed to incomplete fibrosis regression, presence of monoclonal micronodules, or underlying genetic and epigenetic alterations associated with carcinogenesis30,31,32. A cost-effectiveness analysis has shown that the quality-adjusted life year (QALY) decreases substantially when the annual HCC incidence exceeds 1.32% among patients who achieved SVR12, highlighting the need for indefinite HCC surveillance - using ultrasonography alone or in combination with AFP33. In our study, the annual incidence rates of HCC were 7.83% and 6.28% among patients with an M2BPGi level ≥ 4.0 COI at pretreatment and ≥ 2.0 COI at the SVR12 time point, respectively. To date, the clinical utility of dynamic changes of noninvasive indices - such as LSM, the fibrosis index based on four parameters (FIB-4), and the aspartate transaminase-to-platelet count index (APRI)- for predicting long-term liver-related complications, particularly HCC, remains disputed34,35,36. We further explored the role of dynamic changes in serum M2BPGi at pretreatment and SVR12 in predicting HCC occurrence in our cohort. In addition to the established risk factors for HCC, we found that patterns of serum M2BPGi changes were strongly associated with long-term HCC risk, Specifically, patients with persistently elevated M2BPGi (Category 4) carried the highest risk of HCC, whereas those with consistently low levels (Category 1) had the lowest risk. The discordant groups (Categories 2 and 3) exhibited an intermediate risk profile. These findings highlight that post-treatment M2BPGi levels and their dynamic evolution are crucial for optimizing surveillance strategies.
In addition to conventional demographics and biomarkers that can predict the risk of HCC, such as age, sex, LSM, ALT quotient, and AFP, the levels of M2BPGi at both the pretreatment and SVR12 time points were associated with HCC occurrence in our cohort. This highlights the complex interactions among hepatic stellate cell (HSC) transformation or activation, in addition to hepatic fibrosis and inflammation, in regulating the secretion of M2BPGi and hepatic carcinogenesis29. Although our study focused exclusively on M2BPGi dynamics, future studies with larger sample sizes will be valuable to determine whether integrating dynamic changes across multiple biomarkers such as ALT, LSM, and FIB-4 can further enhance HCC risk stratification following HCV cure.
This study has several strengths that can aid clinicians in managing HCC risk estimation following DAA-induced HCV cure using M2BPGi-based models. First, we validated the value of serum M2BPGi levels at both the pretreatment and SVR12 time points in predicting HCC occurrence by recruiting a substantial number of patients from a different ancestry, who underwent a median post-SVR12 follow-up of up to 4.5 years. Second, we employed standardized care, encompassing consistent intervals and tools for HCC detection and data collection, to minimize bias in HCC risk estimation. Third, HCC risk stratification based on dynamic changes in M2BPGi was first introduced in our cohort, enabling physicians to optimize clinical decision-making during post-SVR12 follow-up. While our study has notable strengths, it is important to acknowledge its limitations. First, the number of patients with HCC occurrence was relatively small, making the confidence intervals for factors of interest in risk estimate models less precise. However, we adopted models with AIC selection to maintain goodness-of-fit and avoid overinterpretation. Second, our study used a semi-quantitative evaluation of M2BPGi levels. The clinical utility of the recently introduced quantitative M2BPGi assessment in predicting HCC risk following HCV cure warrants further investigation9. Third, in addition to M2BPGi levels, the role of glycan signatures of M2BP in detecting differences in lectin components for discriminating HCC risk also requires in-depth investigation37. Fourth, our cutoff values were derived using the same WFA–antibody HISCL platform employed in earlier Japanese studies. Variations in assay calibration, analytical performance, and population characteristics may limit the direct transferability of these cutoffs to other M2BPGi measurement systems or non-Asian populations; therefore, future studies are needed to externally recalibrate these thresholds in different clinical and ethnic settings10. Fifth, the overlapping survival curves between Categories 2 and 3 may be attributed to the relatively small sample sizes in both groups, which limits the statistical power to distinguish between these intermediate groups. Furthermore, lifestyle factors that may influence M2BPGi dynamics, such as alcohol consumption or weight changes, were not systematically collected. Future prospective studies with larger discordant subgroups and comprehensive lifestyle assessments will be needed to clarify these associations.
In conclusion, our study confirmed the important role of serum M2BPGi levels in predicting HCC occurrence among patients who achieved HCV cure with DAAs, independent of age, sex, LSM, ALT quotient, and AFP. The cutoff level of serum M2BPGi at pretreatment was 4.0 COI, which should be lowered to 2.0 COI at viral cure due to the regression of hepatic inflammation and HSC activation. Patients with M2BPGi levels higher than the selected cutoff values, particularly when persistently elevated, should undergo regular and intensive monitoring to detect HCC occurrence early and mitigate HCC-related morbidity and mortality during the post-HCV cure follow-up.
Data availability
Data for this study, though not available in a public repository, can be made available upon reasonable request.
References
Liu, C. H., Chang, Y. P. & Kao, J. H. Cutting-edge pharmacotherapy for hepatitis C virus infection: a comprehensive review. Expert Opin. Pharmacother. 25, 1691–1706. https://doi.org/10.1080/14656566.2024.2396024 (2024).
Martinello, M., Solomon, S. S., Terrault, N. A., Dore, G. J. & Hepatitis, C. Lancet 402, 1085–1096 https://doi.org/10.1016/s0140-6736(23)01320-x (2023).
Singal, A. G. et al. AASLD practice guidance on prevention, diagnosis, and treatment of hepatocellular carcinoma. Hepatology 78, 1922–1965. https://doi.org/10.1097/hep.0000000000000466 (2023).
Tzartzeva, K. et al. Surveillance imaging and alpha fetoprotein for early detection of hepatocellular carcinoma in patients with cirrhosis: a meta-analysis. Gastroenterology 154, 1706–1718.e1701. https://doi.org/10.1053/j.gastro.2018.01.064 (2018).
Lee, Y. T., Fujiwara, N., Yang, J. D. & Hoshida, Y. Risk stratification and early detection biomarkers for precision HCC screening. Hepatology 78, 319–362. https://doi.org/10.1002/hep.32779 (2023).
Kuno, A. et al. A serum sweet-doughnut protein facilitates fibrosis evaluation and therapy assessment in patients with viral hepatitis. Sci. Rep. 3, 1065. https://doi.org/10.1038/srep01065 (2013).
Liu, C. H. et al. Serum Mac-2 binding protein glycosylation isomer to predict the severity of hepatic fibrosis in patients with hepatitis C virus infection. Diagnostics (Basel). 12, 2650. https://doi.org/10.3390/diagnostics12112650 (2022).
Chang, Y. P. et al. Serum Mac-2 binding protein glycosylation isomer dynamics in patients achieving sustained virologic response for hepatitis C virus. J. Gastroenterol. Hepatol. 39, 2439–2446. https://doi.org/10.1111/jgh.16680 (2024).
Uojima, H. et al. Quantitative measurements of M2BPGi depend on liver fibrosis and inflammation. J. Gastroenterol. 59, 598–608. https://doi.org/10.1007/s00535-024-02100-3 (2024).
Yamasaki, K. et al. Elevated serum levels of wisteria floribunda agglutinin-positive human Mac-2 binding protein predict the development of hepatocellular carcinoma in hepatitis C patients. Hepatology 60, 1563–1570. https://doi.org/10.1002/hep.27305 (2014).
Tamaki, N. et al. Wisteria floribunda agglutinin positive human Mac-2-binding protein as a predictor of hepatocellular carcinoma development in chronic hepatitis C patients. Hepatol. Res. 45, E82–88. https://doi.org/10.1111/hepr.12466 (2015).
Takemura, K. et al. Post-Treatment M2BPGi level and the rate of autotaxin reduction are predictive of hepatocellular carcinoma development after antiviral therapy in patients with chronic hepatitis C. Int. J. Mol. Sci. 21, 4517. https://doi.org/10.3390/ijms21124517 (2020).
Sasaki, R. et al. Serum wisteria floribunda Agglutinin-Positive Mac-2 binding protein values predict the development of hepatocellular carcinoma among patients with chronic hepatitis C after sustained virological response. PLoS One. 10, e0129053. https://doi.org/10.1371/journal.pone.0129053 (2015).
Nagata, H. et al. Effect of interferon-based and -free therapy on early occurrence and recurrence of hepatocellular carcinoma in chronic hepatitis C. J. Hepatol. 67, 933–939. https://doi.org/10.1016/j.jhep.2017.05.028 (2017).
Yasui, Y. et al. Wisteria floribunda agglutinin-positive Mac-2 binding protein predicts early occurrence of hepatocellular carcinoma after sustained virologic response by direct-acting antivirals for hepatitis C virus. Hepatol. Res. 48, 1131–1139. https://doi.org/10.1111/hepr.13233 (2018).
Osawa, L. et al. Wisteria floribunda Agglutinin-Positive Mac-2 binding protein but not α-fetoprotein as a Long-Term hepatocellular carcinoma predictor. Int. J. Mol. Sci. 21, 3640. https://doi.org/10.3390/ijms21103640 (2020).
Nakagawa, M. et al. Mac-2 binding protein glycosylation isomer as a novel predictive biomarker for patient survival after hepatitis C virus eradication by DAAs. J. Gastroenterol. 55, 990–999. https://doi.org/10.1007/s00535-020-01715-6 (2020).
Yugawa, K. et al. Mac-2-Binding protein glycosylation isomer as a novel predictor of hepatocellular carcinoma recurrence in patients with hepatitis C virus eradication. Ann. Surg. Oncol. 29, 2711–2719. https://doi.org/10.1245/s10434-021-11011-z (2022).
Hayashi, T. et al. Use of the serum wisteria floribunda Agglutinin-Positive Mac2 binding protein as a marker of gastroesophageal varices and Liver-Related events in chronic hepatitis C patients. Diagnostics (Basel). 10, 173. https://doi.org/10.3390/diagnostics10030173 (2020).
Okuda, Y. et al. Usefulness of Mac-2 binding protein glycosylation isomer for prediction of posthepatectomy liver failure in patients with hepatocellular carcinoma. Ann. Surg. 265, 1201–1208. https://doi.org/10.1097/sla.0000000000001836 (2017).
World Medical Association Declaration of Helsinki. Ethical principles for medical research involving human participants. Jama 333, 71–74. https://doi.org/10.1001/jama.2024.21972 (2025).
Chang, Y. P. et al. Comparison of diagnostic performance among Abbott realtime HCV genotyping II, Abbott HCV genotype plus RUO, and Roche Cobas HCV genotyping assays for hepatitis C virus genotyping. J. Med. Virol. 96, e29686. https://doi.org/10.1002/jmv.29686 (2024).
Prati, D. et al. Updated definitions of healthy ranges for serum Alanine aminotransferase levels. Ann. Intern. Med. 137, 1–10. https://doi.org/10.7326/0003-4819-137-1-200207020-00006 (2002).
Castera, L., Forns, X. & Alberti, A. Non-invasive evaluation of liver fibrosis using transient elastography. J. Hepatol. 48, 835–847. https://doi.org/10.1016/j.jhep.2008.02.008 (2008).
Chang, Y. P. et al. Risk of incident type 2 diabetes and prediabetes in patients with direct acting Antiviral-Induced cure of hepatitis C virus infection. Aliment. Pharmacol. Ther. 61, 1508–1518. https://doi.org/10.1111/apt.70029 (2025).
Liu, C. H., Lin, H. C. & Kao, J. H. Toward the hepatitis C virus elimination in asia: the policy forum from the 2023 Asian Pacific association of the study of the liver (APASL). J. Formos. Med. Assoc. 122, 1234–1237. https://doi.org/10.1016/j.jfma.2023.10.005 (2023).
Asahina, Y. JSH guidelines for the management of hepatitis C virus Infection, 2019 Update; protective effect of antiviral therapy against hepatocarcinogenesis. Hepatol. Res. 50, 775–790. https://doi.org/10.1111/hepr.13501 (2020).
Fujita, K. et al. Fibrosis staging using direct serum biomarkers is influenced by hepatitis activity grading in hepatitis C virus infection. J. Clin. Med. 7 https://doi.org/10.3390/jcm7090267 (2018).
Shirabe, K. et al. Mac-2 binding protein glycan isomer (M2BPGi) is a new serum biomarker for assessing liver fibrosis: more than a biomarker of liver fibrosis. J. Gastroenterol. 53, 819–826. https://doi.org/10.1007/s00535-017-1425-z (2018).
Ioannou, G. N. HCC surveillance after SVR in patients with F3/F4 fibrosis. J. Hepatol. 74, 458–465. https://doi.org/10.1016/j.jhep.2020.10.016 (2021).
Negro, F. Residual risk of liver disease after hepatitis C virus eradication. J. Hepatol. 74, 952–963. https://doi.org/10.1016/j.jhep.2020.11.040 (2021).
Paradis, V. et al. Clonal analysis of micronodules in virus C-induced liver cirrhosis using laser capture microdissection (LCM) and HUMARA assay. Lab. Invest. 80, 1553–1559. https://doi.org/10.1038/labinvest.3780165 (2000).
Farhang Zangneh, H. et al. Cost effectiveness of hepatocellular carcinoma surveillance after a sustained virologic response to therapy in patients with hepatitis C virus infection and advanced fibrosis. Clin. Gastroenterol. Hepatol. 17, 1840–1849e1816. https://doi.org/10.1016/j.cgh.2018.12.018 (2019).
Nicoletti, A. et al. Dynamics of liver stiffness predicts complications in patients with HCV related cirrhosis treated with direct-acting antivirals. Dig. Liver Dis. 55, 1472–1479. https://doi.org/10.1016/j.dld.2023.04.018 (2023).
Nahon, P. et al. Value of non-invasive test dynamics in guiding HCC surveillance decisions after HCV cure in patients with cirrhosis. J. Hepatol. https://doi.org/10.1016/j.jhep.2025.02.008 (2025).
Moreau, C. et al. Dynamic personalized prediction of the individual liver-related risk after sustained viral response in HCV patients. J. Viral Hepat. 30, 567–577. https://doi.org/10.1111/jvh.13830 (2023).
Shimazaki, H. et al. M2BPgs-HCC: an automated multilectin bead array indicating aberrant glycosylation signatures toward hepatitis C Virus-Associated hepatocellular carcinoma prognosis. Molecules 29, 5640. https://doi.org/10.3390/molecules29235640 (2024).
Acknowledgements
The authors thank Hui-Ju Lin and Pin-Chin Huang for clinical data management; the 7th Core Lab of the National Taiwan University Hospital, and the 1st Common Laboratory of the National Taiwan University Hospital, Yun-Lin Branch, for the instrumental and technical support.
Funding
National Taiwan University Hospital (NTUH-113-S0040).
Author information
Authors and Affiliations
Contributions
Conceptualization: Chen-Hua Liu. Data curation: Chen-Hua Liu. Formal analysis: Yu-Ping Chang, Yu-Chu Chen, Chen-Hua Liu. Investigation: Yu-Ping Chang, Yu-Chu Chen, Tung-Hung Su, Shang-Chin Huang, Tai-Chung Tseng, Pei-Jer Chen, Chun-Jen Liu, Jia-Horng Kao, Chen-Hua Liu. Methodology: Yu-Ping Chang, Yu-Chu Chen, Chen-Hua Liu. Project administration: Yu-Ping Chang, Yu-Chu Chen, Chen-Hua Liu. Resources: Yu-Ping Chang, Yu-Chu Chen, Tung-Hung Su, Shang-Chin Huang, Tai-Chung Tseng, Pei-Jer Chen, Chun-Jen Liu, Jia-Horng Kao, Chen-Hua Liu. Software: Yu-Ping Chang, Yu-Chu Chen, Chen-Hua Liu. Supervision: Chen-Hua Liu. Validation: Yu-Ping Chang, Yu-Chu Chen, Chen-Hua Liu. Visualization: Yu-Ping Chang, Yu-Chu Chen, Chen-Hua Liu. Writing—original draft: Yu-Ping Chang, Yu-Chu Chen, Chen-Hua Liu. Writing—review & editing: Yu-Ping Chang, Yu-Chu Chen, Tung-Hung Su, Shang-Chin Huang, Tai-Chung Tseng, Pei-Jer Chen, Chun-Jen Liu, Jia-Horng Kao, Chen-Hua Liu.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Chang, YP., Chen, YC., Su, TH. et al. Serum Mac-2 binding protein glycosylation isomer in predicting hepatocellular carcinoma occurrence among patients with direct-acting antiviral-induced HCV cure. Sci Rep 16, 5757 (2026). https://doi.org/10.1038/s41598-026-36809-3
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-026-36809-3
