
Abstract
Root canal filling is a critical determinant of endodontic treatment success, yet limited evidence exists regarding the superiority of specific techniques or materials over others. This systematic review and meta-analysis compared the clinical and radiographic outcomes of different root canal obturation techniques and materials in primary treatments and retreatments. We systematically searched PubMed, Cochrane Library, and ScienceDirect up to the last week of November 2025 following PRISMA guidelines. Studies were included if they reported primary or retreatment outcomes with at least 6 months of follow-up, < 25% loss to follow-up, and explicit documentation of obturation techniques and clinical/radiographic success. Risk of bias was assessed with ROBINS-I (cohort studies) and RoB 2.0 (randomized studies), and the overall evidence certainty was rated using GRADE. Success rates were compared across techniques using mixed-effects meta-regression, estimating differences in outcomes (beta coefficients) with 95% confidence intervals and accounting for between-study heterogeneity. Eighty-four studies (11,965 samples) met all inclusion criteria. In primary treatments, overall success rates were 87.1% at 6 months and 87.2% at 12 months, without significant differences among techniques. At 24 months, success increased to 92.0%; cold lateral condensation (CLC) (difference: 5.0%, p = 0.021) and carrier-based (CB) techniques (difference: 7.5%, p = 0.011) showed higher success than single-cone (SC). Beyond 3 years, success decreased to 84.9%, with no statistically significant differences among warm vertical compaction (WVC), warm lateral compaction (WLC), CLC, SC, and CB techniques. In retreatments, success rates were 92.9% at 6 months, 77.0% at 12 months, and 83.5% at 24 months. At 12 months, SC showed a marginally higher success than CLC (p = 0.045), while at 24 months, CB significantly outperformed WVC (p = 0.004). Beyond 3 years, success decreased to 73.7%, with no significant differences between CLC and CB techniques. Overall, primary treatments presented higher success than retreatments. At 24 months, CLC and CB techniques showed modest advantages, which were not maintained at longer follow-ups. Success appears multifactorial, with operator expertise and case selection having greater impact than obturation technique. The overall certainty of evidence remained low to very low, particularly for long-term outcomes. Bioceramic sealers used with SC techniques have not demonstrated clear clinical benefits or improved retreatment outcomes. High heterogeneity and risk of bias suggest a need for well-powered, multicenter, long-term randomized trials with standardized outcome reporting to establish clinical standards (PROSPERO registration: CRD42024524608).
Similar content being viewed by others

Introduction
Root canal filling represents a critical phase in endodontic treatment, aimed at sealing the canal system, preventing reinfection, and supporting long-term success. The quality of root canal filling, including its apical sealing, homogeneity, and adaptation, has been identified as an important factor influencing the prognosis of treated teeth1,2,3. An optimal apical seal is critical to prevent microbial leakage and minimize post-treatment disease.
Historically, root canal fillings have been completed using a combination of core materials and sealers. The cold lateral condensation (CLC) technique, recognized as the classical technique, remains the most widely used due to its predictable control of filling length and cost-effectiveness4. However, its limited ability to achieve three-dimensional sealing, particularly in irregular canal spaces, led to the introduction of warm vertical compaction (WVC) technique by Schilder in 1967, which improved material adaptation to the canal system, particularly its apical and lateral irregularities5. Since then, more advanced thermoplastic techniques have evolved, such as continuous wave condensation, injection-molded gutta-percha, and carrier-based (CB) techniques, each presenting distinct advantages and limitations based on specific clinical scenario6,7.
Despite these advancements, the impact of obturation technique on treatment outcomes remains unclear. While early studies focused primarily on radiographic parameters such as the extent of the root filling relative to the apical foramen8,9,10, recent evidence has reinforced the critical role of achieving a well-sealed apical third to ensure treatment success11,12. However, most of the existing literature focused on the radiographic quality of root canal fillings, with little emphasis on direct comparisons of success rates between different techniques and materials. In recent years, bioceramic sealers have gained popularity due to their bioactivity and superior sealing potential. However, high-quality comparative studies directly evaluating their performance against traditional sealers in both primary root canal treatments (RCTs) and retreatment cases (re-RCTs) remain limited. This gap in evidence is significant, as prior filling materials can complicate retreatment procedures and influence outcomes.
With the increasing use of single-cone (SC) techniques with bioceramic sealers, alongside established methods such as CLC, WVC, and CB, there is a need for rigorous clinical comparisons. Evaluating success rates across these methods, particularly in retreatment cases, could offer clinicians evidence-based guidance for optimizing treatment protocols. Therefore, this systematic review and meta-analysis compared the clinical and radiographic success rates of root canal filling techniques and materials, aiming to support standardized and effective endodontic care.
Materials and methods
Protocol and registration
This systematic review and meta-analysis adhered to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines13 to promote comprehensive and transparent reporting, and follows the methodological approach of a recent publication14. The protocol was registered in the PROSPERO international prospective database (Registration ID: CRD42024524608), which provides a publicly accessible record of the study plan and methodology.
Focused research question
Using the PICOTSS framework, this systematic review addressed the following question: In human permanent teeth undergoing RCT or re-RCT (P), do different obturation techniques and/or materials (I), compared with alternative ones (C), influence endodontic treatment outcomes (O) at a minimum follow-up of six months (T), based on evidence from clinical studies conducted in dental or academic settings (S, S)?
Endodontic treatment outcomes were defined a priori as clinical and radiographic success. Prespecified subgroup analyses included treatment type (RCT and re-RCT), obturation technique (CLC, WVC, WLC, SC, CB), follow-up duration, and study design.
Eligibility criteria
This systematic review included randomized controlled trials and cohort studies published in any language up to November 30th, 2025. Studies were included if they involved permanent teeth, described the root canal filling technique and material, had a minimum follow-up of six months, and reported a dropout rate ≤ 25%, aligning with previous meta-analysis in Endodontology107. Outcomes had to be assessed using defined clinical and radiographic criteria.
Studies were excluded if they were case reports, case series, review articles, or animal and in vitro studies. Research involving primary teeth, studies with incomplete information on techniques or materials, or those without clear radiographic and clinical outcomes were also excluded.
Search strategy
A comprehensive electronic search was performed independently by two authors across three major databases: PubMed (National Center for Biotechnology Information), Cochrane Library (John Wiley & Sons, Ltd), and ScienceDirect (Elsevier). The search was conducted without language or publication date restrictions to ensure the inclusion of all relevant studies.
To improve the completeness of the search, grey literature was explored using the following sources: CADTH’s Grey Matters (https://greymatters.cadth.ca/), The European database on medical devices (EUDAMED) (https://ec.europa.eu/tools/eudamed/#/screen/home), and The New York Academy of Medicine Library (https://catalog.nyam.org/cgi-bin/koha/opac-search.pl). A manual search was also conducted to review relevant journals, including the International Endodontic Journal, Journal of Endodontics, Clinical Oral Investigations, European Endodontic Journal, Scientific Reports, and the Australian Endodontic Journal, bibliographies of included studies, and conference proceedings to capture any missed publications or unpublished data.
The search strategy utilized a combination of MeSH terms and relevant keywords, including “root canal treatment,” “endodontic therapy,” “prognosis,” “outcome,” “root canal obturation,” and “root canal retreatment,” combined using Boolean operators such as ‘AND’ to narrow the search and ‘OR’ to include synonymous terms. The full applied search strategy for PubMed/Medline is presented in Table 1.
Screening and study selection
Initial screening was performed from June 1 to August 14, 2023. The search was subsequently updated, and the final screening was completed on November 30, 2025, to include the most recent eligible studies. Duplicate records were removed prior to title and abstract screening. Study selection was independently performed by two reviewers (A.M. and S.A.). Any disagreements were resolved by consensus, and when necessary, a third reviewer (F.E. or K.I.A.) acted as an arbitrator.
Data extraction
After reviewing the titles and abstracts of the search results, studies that potentially met the inclusion criteria were subjected to full-text evaluation. Data extraction followed a predefined standardized collection form to ensure consistency and accuracy. Extracted information included study details such as authors, year of publication, and study design (randomized or cohort), along with sample characteristics including sample size, patient age, gender, and pulp/periapical status. Treatment-specific details were recorded, including the type of treatment (primary root canal treatment or retreatment), root canal filling techniques, materials, cement type, instrumentation technique, and irrigants used. Additional clinical variables extracted comprised tooth type, rubber dam utilization, operator skill, number of treatment sessions, and microscope use. Follow-up periods were classified into four distinct time points: 6 months, 12 months, 24 months, and more than 3 years.
Outcomes were assessed based on radiographic evaluations and resolution of clinical signs and symptoms, with data extracted for all reported follow-up periods to ensure a comprehensive analysis. Any disagreements between the two independent reviewers during the data extraction process were resolved through discussion. If consensus could not be reached, a third reviewer (F.E. or K.I.A.) served as an impartial arbitrator to finalize decisions.
Quality assessment
To evaluate the risk of bias, two independent reviewers (A.M. and S.A.) conducted quality assessments for all included studies. For randomized studies, the revised Cochrane RoB2 tool15 was employed, addressing five key domains: randomization process, deviations from intended interventions, missing outcome data, outcome measurement, and reporting bias. For non-randomized studies, the ROBINS-I tool16 was utilized, assessing bias across seven domains including selection bias, performance bias, attrition bias, and reporting bias. Disagreements were resolved by discussion; if unresolved, a third reviewer (F.E. or K.I.A.) acted as an impartial arbitrator. The assessments were performed using RevMan 5.4 software (Cochrane Collaboration) to ensure systematic organization and visualization of results.
The overall certainty of evidence was evaluated using the GRADE system, which accounts for risk of bias, inconsistency, imprecision, and overall confidence in the evidence. This systematic approach allowed for a comprehensive evaluation of study quality and evidence strength.
Statistical analysis
A comprehensive meta-analysis was conducted using a mixed-effects model, with root canal filling techniques serving as the moderator variable. To account for heterogeneity among studies, a restricted maximum likelihood estimator was applied. The overall effect size was presented using forest plots with 95% confidence intervals to illustrate the raw rate of successful outcomes across the included studies. Heterogeneity between studies was evaluated using Cochran’s Q test and quantified through the I² index, which represents the proportion of variability attributable to between-study differences. A funnel plot analysis was performed to visually inspect the potential presence of publication bias, while Egger’s test was used to statistically assess its significance. A significance level of α = 0.05 was applied to all statistical tests.
Subgroup analyses were performed to explore factors contributing to heterogeneity, including root canal filling techniques, material types, and moderating factors such as patient age, gender, tooth type, anesthetic solution, and treatment type (primary or retreatment). A meta-regression analysis was performed using a mixed-effects model to quantify the influence of these covariates on treatment outcomes. Results were reported as beta coefficients (β) with 95% confidence intervals and Z statistics, facilitating a clearer understanding of variable relationships. All statistical analyses were conducted using R software (version 4.3.1) (R Core Team, 2023), a robust statistical computing platform widely used in meta-analyses.
Results
Study selection
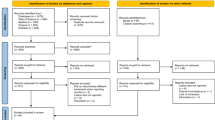
The study selection followed PRISMA guidelines (Fig. 1). From 44,602 initial records, 484 full texts were assessed after duplicate removal and title/abstract screening. Of these, 341 were excluded due to ineligible design, insufficient follow-up, or incomplete outcomes (Suppl. Table 1). A total of 84 studies met inclusion criteria and were included in qualitative and quantitative analyses (Table 2).

PRISMA flow diagram: visual representation of the study selection process.
Characteristics of included studies
The analysis incorporated 11,965 samples from 84 studies, consisting of 42 randomized controlled trials and 42 cohort studies (prospective and retrospective). These studies focused on RCT, re-RT, and apexification, categorized by different follow-up periods.
For primary root canal treatment, studies were grouped by follow-up intervals. Nine studies evaluated treatments over a 6-month period, analyzing four techniques: WVC, SC, CLC, and CB. For the 12-month period, 32 studies investigated six techniques, including WVC, SC, CLC, TH, and CB. Eighteen studies reported results for the 24-month period, covering WVC, SC, CLC, and CB techniques. Ten studies assessed outcomes at three or more years, with comparisons between WVC, WLC, CLC, SC, and CB techniques.
For retreatment procedures, two studies reported results at 6 months, evaluating SC and CLC techniques. At 12 months, ten studies examined WVC, SC, and CLC, while eight studies analyzed WVC, CLC, SC, and CB at 24 months. Results for follow-up beyond three years were reported in five studies, focusing on CLC, WVC, SC, and CB techniques. Additionally, nine articles explored the apexification technique across various follow-up durations.
Meta-analysis
The success rate for root canal filling techniques was estimated using meta-analysis, with follow-up durations serving as the moderator variable is illustrated in Fig. 2. For primary root canal treatment, the overall success rate at six months was 87.1% (95% CI: 80.2–94.0). No statistically significant differences were observed between techniques; for instance, SC showed a non-significant 3.2% lower success rate compared to CLC (p = 0.766). At 12 months, the success rate remained 87.2% (95%CI: 84.3–90.1), with no significant differences across techniques (p = 0.677). By 24 months, the success rate improved to 92.0% (95%CI: 89.9–94.1), with CLC and CB techniques demonstrating significantly better results compared to WVC (p = 0.021 and p = 0.011, respectively), Furthermore, SC exhibited significantly worse results compared to both CLC and CB (p = 0.001). The success rate beyond three years was 84.9% (95%CI: 80.8–89.0), and no significant differences between techniques were observed.
For retreatment procedures, the overall success rate at six months was 92.9% (95% CI: 88.6–97.2); however, limited data restricted further comparisons. At 12 months, the success rate was 77.0% (95%CI: 69.2–84.9), with SC demonstrating a marginally significant improvement of 16.7% over CLC (p = 0.045). The success rate at 24 months was 83.5% (95%CI: 74.7–92.2), with CB performing significantly better than WVC (p = 0.004). Beyond three years, the overall success rate dropped to 73.7% (95%CI: 67.4–80.0); although CB showed a 7.9% improvement over CLC, the difference was not statistically significant (p = 0.179). A separate analysis revealed that the apexification technique demonstrated significantly higher success rates compared to CLC at the 12-month follow-up (p = 0.019) (Suppl. Figure 1).
Meta-regression analysis
The meta-regression analysis examined the impact of various independent factors, including mean age, gender distribution, tooth position, operator expertise, and materials used (Suppl. Table 2). Tooth position significantly influenced outcomes, with maxillary teeth showing superior success rates (p = 0.006). Operator expertise also played a critical role, with specialists achieving significantly higher success rates compared to general dentists and students (p < 0.001). Material comparisons revealed marginal significance for zinc oxide eugenol compared to AH-Plus or glass ionomer cements (p = 0.091 and p = 0.080, respectively).
Qualitative assessment
Risk of bias was assessed using RoB 2.0 (randomized) and ROBINS-I (cohorts). Among RCTs, 27 had “some concerns,” others were low risk. Cohort studies mostly had serious bias, especially in outcome reporting; one study had critical participant selection bias (Fig. 3). GRADE assessment rated five outcomes as very low and three as low certainty, including 12- and 24-month RCT outcomes and 12-month re-RCT results (Table 3).

Forest plots for primary root canal treatments at different follow-up periods: (a) 6 months, (b) 12 months, (c) 24 months, and (d) 3 + years. For root canal retreatments, the outcomes are presented for (e) 6 months, (f) 12 months, (g) 24 months, and (h) 3 + years.

Summary of risk of bias assessment using (a) ROB 2.0 for randomized clinical trials and (b) ROBINS-I for non-randomized studies.
Discussion
This systematic review and meta-analysis evaluated the clinical and radiographic success rates of root canal filling techniques and materials in both primary RCTs and re-RCT across different follow-up periods. The study incorporated an extensive search strategy and included both randomized controlled trials and cohort studies to ensure robust and reliable findings.
Primary root canal treatments.
The results of the meta-analyses for primary RCTs showed consistently high overall success rates at the 6- and 12-month follow-up periods, with no statistically significant differences observed between techniques such as SC, CLC, WVC, and CB. These findings align with previous systematic reviews101,102, which similarly reported comparable outcomes among various techniques in short-term follow-ups. The SC technique, in particular, has gained clinical popularity due to its simplicity and the growing use of bioceramic sealers, which are desirable for their bioactivity and sealing properties103,104.
Within the limitations of current evidence, significant differences emerged at the 24-month follow-up period, where SC exhibited lower success rates compared to CLC and CB techniques, which showed 8.8% and 11.3% higher success, respectively. These results may reflect the better adaptation of filling materials achieved with CLC and CB, particularly in more challenging long-term scenarios. However, these differences could also be attributed to factors beyond the inherent sealing ability of the techniques. Variations in sample size and study design can significantly influence statistical outcomes, potentially exaggerating the effectiveness of one technique over another. For instance, variations in sample size and study design can introduce statistical bias, potentially exaggerating the effectiveness of one technique over another. Therefore, further high-quality randomized controlled trials are needed to confirm clinical significance.
A systematic review reported an overall success rate of 83% for core-carrier obturation but noted considerable variability among included studies, demonstrating the impact of sample size and methodology on outcomes105. Additionally, differences in case selection, such as tooth type, canal anatomy, and preoperative conditions, may have contributed to the observed success rates. Studies have shown that teeth with simpler anatomies or fewer complications are more likely to yield favorable outcomes, irrespective of the obturation technique used11.
Operator expertise includes not only technical proficiency but also case selection, complication management, and adherence to aseptic protocols. Moreover, clinicians’ familiarity with specific obturation methods can directly affect the quality of the root canal filling and treatment outcomes. These facets together are fundamental in achieving successful endodontic therapy. For instance, a study comparing CB and lateral compaction techniques concluded that both methods could achieve comparable success rates, with outcomes heavily influenced by operator skill rather than the technique itself106. These findings suggest that the apparent success observed with CLC and CB techniques at 24 months is likely multifactorial, involving variables such as case complexity, operator expertise, and study design rather than solely reflecting the sealing capabilities of the obturation materials. Despite these findings, success rates for all techniques converged beyond the 3-year follow-up period, with no statistically significant differences reported among WVC, WLC, CLC, and CB, suggesting that long-term clinical outcomes may be determined by factors unrelated to the technique itself. However, these differences were not sustained beyond 3 years, where outcomes converged across techniques. Given the low/very-low certainty of evidence and the influence of operator expertise and case selection, these intermediate differences should not be interpreted as technique-dependent superiority.
Root Canal retreatment outcomes
Retreatment analyses were limited by the scarcity of available studies, particularly for the 6-month follow-up period, where only two studies were included17,25. At the 12-month interval, analyses incorporating WVC, CLC, and SC techniques revealed no significant differences in success rates. Similarly, the 24-month follow-up data demonstrated comparable outcomes between WVC, CLC, SC, and CB techniques. Interestingly, CB showed a numerical advantage over CLC beyond the 3-year follow-up, though statistical significance was not achieved. These findings accentuate the need for additional high-quality studies investigating retreatment procedures to draw more reliable conclusions.
Influence of bioceramic sealers
The SC technique has been closely associated with bioceramic sealers, which have emerged as a promising alternative to traditional epoxy resin-based cements (e.g., AH-Plus). While bioceramic sealers have shown excellent biocompatibility, biomineralization potential, and enhanced sealing properties96,97,98,99, their long-term clinical outcomes remain inconclusive. Consistent with our findings, no long-term clinical advantage of bioceramic sealers over AH Plus has been demonstrated to date102. Most supportive evidence derives from in vitro or short-term studies, and the difficulties in retreatment removal remain unresolved. These findings are consistent with prior reviews107, which highlight the need for long-term, well-designed clinical trials to validate the clinical benefits of bioceramic materials.
Despite their advantages, bioceramic sealers pose challenges in retreatment scenarios due to the difficulty in removing them efficiently from the root canal system108. This limitation denotes the importance of careful case selection and the development of standardized protocols for their removal, particularly in cases requiring further intervention.
Clinical implications
While newer obturation techniques and materials may offer certain practical advantages, no single approach consistently outperforms others across follow-up periods. Modest 24-month (mid-term) differences observed for some techniques (slightly higher success of CLB and CB) should be interpreted with caution109, as operator expertise and case selection are likely more decisive factors. Long-term success remains multifactorial and is less dependent on technique, suggesting that operator expertise, case complexity, and patient-specific factors play a central role in treatment success. Nonetheless, given that many outcomes were rated as having low or very low certainty of evidence, these findings should be interpreted with caution, and strong clinical recommendations cannot be made at this stage.
Operator experience emerged as a critical factor influencing success rates, with specialists achieving significantly better outcomes compared to general practitioners and students. This finding supports advanced training and skill development in endodontics to optimize clinical outcomes. Additionally, anatomical factors, such as differences between maxillary and mandibular teeth, were associated with varying success rates, with maxillary teeth exhibiting higher success, possibly due to their more accessible anatomy.
Methodological amendments
This study incorporated key deviations from the initial protocol to improve clinical relevance. For instance, the inclusion criteria were adjusted to allow a dropout rate of up to 25%, as attrition rates above 20–30% are known to increase the risk of bias and compromise the validity of study outcomes. This threshold was selected to maintain methodological rigor while enabling the inclusion of a broader range of relevant endodontic clinical studies, consistent with approaches used in previous systematic reviews. Data extraction and subgroup analyses included additional factors such as tooth position, operator expertise, and material adaptation, enabling a more comprehensive assessment of treatment outcomes. To address heterogeneity, a mixed-effects meta-regression model replaced separate network meta-analyses, providing a standardized approach to outcome assessment across diverse time intervals. Quality assessment integrated ROBINS-I and the GRADE system alongside RoB 2, permitting a robust evaluation of bias and evidence certainty. Additionally, special attention was given to the impact of bioceramic sealers, particularly their influence on retreatment challenges and long-term clinical success.
Strengths and limitations
The strengths of this review include a comprehensive search strategy, adherence to PRISMA guidelines, and rigorous quality assessment using the ROB 2.0, ROBINS-I, and GRADE tools. This systematic review and meta-analysis included a wide range of studies, offering valuable insights into the performance of various obturation techniques and sealers. However, the inclusion of both RCTs and cohort studies, variation in operator expertise and case selection, and differences in follow-up durations (ranging from 6 months to over 3 years) limit direct comparability of results and contribute to heterogeneity. These factors underscore the need for cautious interpretation of pooled estimates. Nevertheless, certain limitations must be acknowledged. Given the considerable methodological heterogeneity among included studies, including the limited number of studies assessing retreatment procedures, particularly with shorter follow-up periods, differences in operator training, case selection, and follow-up intervals, our conclusions must be interpreted with caution. Although trends were identified, the low certainty of evidence as per GRADE and the limited number of studies available (particularly in re-RCTs cases), limit the formulation of strong clinical recommendations based solely on the study findings. Publication bias, though assessed, cannot be entirely ruled out. Consequently, no conclusive clinical practice guidelines can be proposed at this stage.
Further research
Future studies should prioritize well-designed, randomized controlled trials with standardized protocols for evaluating root canal filling techniques and materials to confirm clinical significance. Long-term follow-up data are essential to better understand the success and clinical impact of bioceramic sealers and other emerging materials. Additionally, further research is needed to develop efficient retreatment protocols for bioceramic-based fillings to address their limitations in re-intervention scenarios. Incorporating patient-reported outcomes (PROs) and tooth survival rates could provide a more comprehensive understanding of the effectiveness of RCTs and re-RCTs.
Conclusion
Within the limits of this secondary study, root canal filling techniques and materials demonstrated comparable clinical and radiographic success in short-term follow-ups. Some intermediate-term differences were observed, but outcomes converged beyond 3 years. Operator expertise, case selection, and patient-specific factors appear more influential than the obturation technique itself. Bioceramic sealers have not consistently demonstrated long-term clinical advantage over AH Plus, with most evidence limited to in vitro or short-term studies, and challenges in retreatment remain. Given the low to very low certainty of evidence, these findings should be interpreted with caution, understanding the need for well-designed long-term randomized controlled trials with standardized protocols to strengthen evidence-based guidance in endodontic therapy.
Data availability
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
Change history
06 April 2026
The original online version of this Article was revised: In the original version of this Article Firas Elmsmari was incorrectly affiliated with Affiliation 2. The correct affiliation is Affiliation 1: ‘Clinical Sciences Department, College of Dentistry, Ajman University, P.O. Box 346, Ajman, UAE’. The original Article has been corrected.
References
Peters, O. A. Canal preparation and obturation: An updated view of the two pillars of nonsurgical endodontics. American Association of Endodontists, 1–8 (2016). https://www.aae.org/specialty/wp-content/uploads/sites/2/2017/07/ecfefall2016canalpreparationandobturation.pdf (accessed August 2024).
Kirkevang, L. L., Vaeth, M., Hörsted-Bindslev, P., Bahrami, G. & Wenzel, A. Risk factors for developing apical periodontitis in a general population. Int. Endod J. 40, 290–299 (2007).
Sjögren, U., Figdor, D., Persson, S. & Sundqvist, G. Influence of infection at the time of root filling on the outcome of endodontic treatment of teeth with apical periodontitis. Int. Endod J. 30, 297–306 (1997).
Gilhooly, R. M., Hayes, S. J., Bryant, S. T. & Dummer, P. M. Comparison of lateral condensation and thermomechanically compacted warm alpha-phase gutta-percha with a single cone for obturating curved root canals. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 91, 89–94 (2001).
Aminsobhani, M., Ghorbanzadeh, A., Sharifian, M. R., Namjou, S. & Kharazifard, M. J. Comparison of obturation quality in modified continuous wave compaction, continuous wave compaction, lateral compaction and warm vertical compaction techniques. J. Dent. (Tehran). 12, 99–108 (2015).
Perry, C., Kulild, J. C. & Walker, M. P. Comparison of warm vertical compaction protocols to obturate artificially created defects in the apical one-third. J. Endod. 39, 1176–1178 (2013).
European Society of Endodontology. Quality guidelines for endodontic treatment: consensus report of the European society of endodontology. Int. Endod J. 39, 921–930 (2006).
Sjogren, U., Hagglund, B., Sundqvist, G. & Wing, K. Factors affecting the long-term results of endodontic treatment. J. Endod. 16, 498–504 (1990).
Hommez, G. M. G., Coppens, C. R. M. & De Moor, R. J. G. Periapical health related to the quality of coronal restorations and root fillings. Int. Endod J. 35, 680–689 (2002).
Salehrabi, R. & Rotstein, I. Endodontic treatment outcomes in a large patient population in the USA: an epidemiological study. J. Endod. 30, 846–850 (2004).
Ng, Y. L., Mann, V. & Gulabivala, K. A prospective study of the factors affecting outcomes of nonsurgical root Canal treatment: part 1: periapical health. Int. Endod J. 44, 583–609 (2011).
Gulabivala, K. & Ng, Y. L. Factors that affect the outcomes of root Canal treatment and retreatment-A reframing of the principles. Int. Endod J. 56 (Suppl 2), 82–115 (2023).
Page, M. J. et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ 372, n71 (2021).
Elmsmari, F. et al. Lasers efficacy in pain management after primary and secondary endodontic treatment: a systematic review and meta-analysis of randomized clinical trials. Sci. Rep. 14, 26028 (2024).
Sterne, J. A. C. et al. RoB 2: a revised tool for assessing risk of bias in randomised trials. BMJ 366, l4898 (2019).
Sterne, J. A. et al. ROBINS-I: a tool for assessing risk of bias in non-randomised studies of interventions. BMJ 355, i4919 (2016).
Friedman, S., Löst, C., Zarrabian, M. & Trope, M. Evaluation of success and failure after endodontic therapy using a glass ionomer cement sealer. J. Endod. 21, 384–390 (1995).
Mohan, S. M. & Kaushik, S. Root Canal treatment using thermoplasticized carrier condensation technique. Med. J. Armed Forces India. 65, 336–341 (2009).
Bezgin, T., Sönmez, H., Orhan, K. & Ozalp, N. Comparative evaluation of Ca(OH)2 plus points and Ca(OH)2 paste in apexification. Dent. Traumatol. 28, 488–495 (2012).
Martins, M. R. et al. Efficacy of Er,Cr:YSGG laser with endodontical radial firing tips on the outcome of endodontic treatment: blind randomized controlled clinical trial with six-month evaluation. Lasers Med. Sci. 28, 1049–1055 (2013).
Menakaya, I. N., Adegbulugbe, I. C., Oderinu, O. H. & Shaba, O. P. The efficacy of calcium hydroxide powder mixed with 0.2% chlorhexidine digluconate or mixed with normal saline as intracanal medicament in the treatment of apical periodontitis. J. Contemp. Dent. Pract. 16, 657–664 (2015).
Kist, S. et al. Comparison of Ozone gas and sodium hypochlorite/chlorhexidine two-visit disinfection protocols in treating apical periodontitis: a randomized controlled clinical trial. Clin. Oral Investig. 21, 995–1005 (2017).
de Figueiredo, F. E. D. et al. Effectiveness of a reciprocating single file, single cone endodontic treatment approach: a randomized controlled pragmatic clinical trial. Clin. Oral Investig. 24, 2247–2257 (2020).
Shaheed, J., Jawad, H.A., Hussain, B.M.A. & Said, A.M. Healing of apical periodontitis after minimally invasive endodontics therapy using Er,Cr:YSGG laser: a prospective clinical study. Sys. Rev. Pharm. 11, 135–140 (2020).
Kim, J. H. et al. Clinical efficacy of Sealer-based obturation using calcium silicate sealers: A randomized clinical trial. J. Endod. 48, 144–151 (2022).
da Silva, T. A. et al. Outcome of root Canal treatment of teeth with asymptomatic apical periodontitis treated with foraminal enlargement and 2% chlorhexidine gel: A retrospective cohort study. J. Endod. 49, 972–979 (2023).
Hu, J., Zhu, Y., Deng, S., Wang, Z. & He, F. Outcome of root Canal treatment using warm vertical compaction with bioceramic and resin-based sealers: A randomised clinical trial. Aust Endod J. 49 (Suppl 1), 170–178 (2023).
Danin, J., Strömberg, T., Forsgren, H., Linder, L. E. & Ramsköld, L. O. Clinical management of nonhealing periradicular pathosis. Surgery versus endodontic retreatment. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 82, 213–217 (1996).
Tani-Ishii, N. & Teranaka, T. Clinical and radiographic evaluation of root-canal obturation with obtura II. J. Endod. 29, 739–742 (2003).
Imura, N. et al. The outcome of endodontic treatment: a retrospective study of 2000 cases performed by a specialist. J. Endod. 33, 1278–1282 (2007).
Cotton, T. P., Schindler, W. G., Schwartz, S. A., Watson, W. R. & Hargreaves, K. M. A retrospective study comparing clinical outcomes after obturation with Resilon/Epiphany or Gutta-Percha/Kerr sealer. J. Endod. 34, 789–797 (2008).
Moore, A., Howley, M. F. & O’Connell, A. C. Treatment of open apex teeth using two types of white mineral trioxide aggregate after initial dressing with calcium hydroxide in children. Dent. Traumatol. 27, 166–173 (2011).
Damle, S. G., Bhattal, H. & Loomba, A. Apexification of anterior teeth: a comparative evaluation of mineral trioxide aggregate and calcium hydroxide paste. J. Clin. Pediatr. Dent. 36, 263–268 (2012).
Patel, S., Wilson, R., Dawood, A., Foschi, F. & Mannocci, F. The detection of periapical pathosis using digital periapical radiography and cone beam computed tomography - part 2: a 1-year post-treatment follow-up. Int. Endod J. 45, 711–723 (2012).
Saini, H. R., Tewari, S., Sangwan, P., Duhan, J. & Gupta, A. Effect of different apical Preparation sizes on outcome of primary endodontic treatment: a randomized controlled trial. J. Endod. 38, 1309–1315 (2012).
Mente, J. et al. Treatment outcome of mineral trioxide aggregate in open apex teeth. J. Endod. 39, 20–26 (2013).
Liang, Y. H. et al. Radiographic healing after a root Canal treatment performed in single-rooted teeth with and without ultrasonic activation of the irrigant: a randomized controlled trial. J. Endod. 39, 1218–1225 (2013).
Tang, Z., Wang, H. & Jiang, S. Clinical study of single-visit root Canal treatment with a nickel-titanium (Ni-Ti) rotary instrument combined with different ultrasonic irrigation solutions for elderly patients with chronic apical periodontitis. Biomed. Mater. Eng. 26 (Suppl 1), 311–318 (2015).
Wong, A. W. Y. et al. Treatment outcomes of single-visit versus multiple-visit non-surgical endodontic therapy: a randomised clinical trial. BMC Oral Health. 15, 162 (2015).
de Rizzi-Maia, C. Single vs Two-session root Canal treatment: A preliminary randomized clinical study using cone beam computed tomography. J. Contemp. Dent. Pract. 17, 515–521 (2016).
Sarin, A. et al. Effect of different obturation techniques on the prognosis of endodontic therapy: A retrospective comparative analysis. J. Contemp. Dent. Pract. 17, 582–586 (2016).
Sigurdsson, A., Garland, R. W., Le, K. T. & Woo, S. M. 12-month healing rates after endodontic therapy using the novel GentleWave system: A prospective multicenter clinical study. J. Endod. 42, 1040–1048 (2016).
Chen, S. J. & Chen, L. P. Radiographic outcome of necrotic immature teeth treated with two endodontic techniques: A retrospective analysis. Biomed. J. 39, 366–371 (2016).
Arya, S. et al. Healing of apical periodontitis after nonsurgical treatment in patients with type 2 diabetes. J. Endod. 43, 1623–1627 (2017).
Lin, J. et al. Regenerative endodontics versus apexification in immature permanent teeth with apical periodontitis: A prospective randomized controlled study. J. Endod. 43, 1821–1827 (2017).
Al-Nuaimi, N., Patel, S., Austin, R. S. & Mannocci, F. A prospective study assessing the effect of coronal tooth structure loss on the outcome of root Canal retreatment. Int. Endod J. 50, 1143–1157 (2017).
Galani, M. et al. Comparative evaluation of postoperative pain and success rate after pulpotomy and root Canal treatment in cariously exposed mature permanent molars: A randomized controlled trial. J. Endod. 43, 1953–1962 (2017).
Sigurdsson, A., Garland, R. W., Le, K. T. & Rassoulian, S. A. Healing of periapical lesions after endodontic treatment with the GentleWave procedure: A prospective multicenter clinical study. J. Endod. 44, 510–517 (2018).
Chybowski, E. A. et al. Clinical outcome of Non-Surgical root Canal treatment using a Single-cone technique with endosequence bioceramic sealer: A retrospective analysis. J. Endod. 44, 941–945 (2018).
Verma, N., Sangwan, P., Tewari, S. & Duhan, J. Effect of different concentrations of sodium hypochlorite on outcome of primary root Canal treatment: A randomized controlled trial. J. Endod. 45, 357–363 (2019).
Arslan, H., Doğanay Yıldız, E., Topçuoğlu, H. S., Tepecik, E. & Ayaz, N. Success of maintaining apical patency in teeth with periapical lesion: a randomized clinical study. Quintessence Int. 50, 686–693 (2019).
Kumar, G. et al. The effect of an intraorifice barrier and base under coronal restorations on the healing of apical periodontitis: a randomized controlled trial. Int. Endod J. 53, 298–307 (2020).
Best, S., Ammons, C. L., Karunanayake, G. A., Saemundsson, S. R. & Tawil, P. Z. Outcome assessment of teeth with necrotic pulps and apical periodontitis treated with Long-term calcium hydroxide. J. Endod. 47, 11–18 (2021).
Conejero, M. J., Almenar, A., Forner, L., Sanz, J. L. & Llena, C. Retrospective clinical evaluation of root Canal treatment with or without photodynamic therapy for necrotic teeth and teeth subjected to retreatment. J. Oral Sci. 63, 163–166 (2021).
Koli, B., Chawla, A., Logani, A., Kumar, V. & Sharma, S. Combination of nonsurgical endodontic and vital pulp therapy for management of mature permanent mandibular molar teeth with symptomatic irreversible pulpitis and apical periodontitis. J. Endod. 47, 374–381 (2021).
Bardini, G. et al. A 4-year follow-up of root Canal obturation using a calcium silicate-based sealer and a zinc oxide-eugenol sealer: A randomized clinical trial. Int. Endod J. https://doi.org/10.1111/iej.14167 (2024).
Fatima, S., Kumar, A., Andrabi, S. M. U. N., Mishra, S. K. & Tewari, R. K. Effect of apical third enlargement to different Preparation sizes and tapers on postoperative pain and outcome of primary endodontic treatment: A prospective randomized clinical trial. J. Endod. 47, 1345–1351 (2021).
Tosun, S., Karataslioglu, E., Tulgar, M. M. & Derindag, G. Retrospective fractal analyses of one-year follow-up data obtained after single-visit nonsurgical endodontic retreatment on periapical radiographs. Clin. Oral Investig. 25, 6465–6472 (2021).
Zahran, S., Patel, S., Koller, G. & Mannocci, F. The impact of an enhanced infection control protocol on molar root Canal treatment outcome - a randomized clinical trial. Int. Endod J. 54, 1993–2005 (2021).
Serefoglu, B., Miçooğulları Kurt, S., Kandemir Demirci, G., Kaval, M. E. & Çalışkan, M. K. A prospective cohort study evaluating the outcome of root Canal retreatment in symptomatic mandibular first molars with periapical lesions. Int. Endod J. 54, 2173–2183 (2021).
Ahmed, Y. E., Ahmed, G. M. & Ghoneim, A. G. Evaluation of postoperative pain and healing following regenerative endodontics using platelet-rich plasma versus conventional endodontic treatment in necrotic mature mandibular molars with chronic periapical periodontitis. A randomized clinical trial. Int. Endod J. 56, 404–418 (2023).
Taha, N. A., Abuzaid, A. M. & Khader, Y. S. A randomized controlled clinical trial of pulpotomy versus root Canal therapy in mature teeth with irreversible pulpitis: Outcome, quality of Life, and patients’ satisfaction. J. Endod. 49, 624–631e2 (2023).
Alzoubi, F. et al. The outcome of nonsurgical root Canal treatment using Sealer-based obturation versus warm vertical compaction: A randomized controlled trial. J. Endod. 51, 1351–1361 (2025).
Bani-Younes, H. A., Methqal, K. A., Madarati, A. A. & Daud, A. Clinical and radiographic outcome of a bioceramic sealer compared to a resin-based sealer: a retrospective study. Sci. Rep. 15, 16680 (2025).
Doğan, M. U., Arıcıoğlu, B., Köse, T. E., Çıkman, A. Ş. & Öksüzer, M. Ç. Association between the irrigation-agitation techniques and periapical healing of large periapical lesions: a randomized controlled trial. Clin. Oral Investig. 28, 376 (2024).
Field, J. W., Gutmann, J. L., Solomon, E. S. & Rakusin, H. A clinical radiographic retrospective assessment of the success rate of single-visit root Canal treatment. Int. Endod J. 37, 70–82 (2004).
Gorni, F. G. M. & Gagliani, M. M. The outcome of endodontic retreatment: a 2-yr follow-up. J. Endod. 30, 1–4 (2004).
Calişkan, M. K. Nonsurgical retreatment of teeth with periapical lesions previously managed by either endodontic or surgical intervention. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 100, 242–248 (2005).
Molander, A., Warfvinge, J., Reit, C. & Kvist, T. Clinical and radiographic evaluation of one- and two-visit endodontic treatment of asymptomatic necrotic teeth with apical periodontitis: a randomized clinical trial. J. Endod. 33, 1145–1148 (2007).
Holden, D. T., Schwartz, S. A., Kirkpatrick, T. C. & Schindler, W. G. Clinical outcomes of artificial root-end barriers with mineral trioxide aggregate in teeth with immature apices. J. Endod. 34, 812–817 (2008).
Mendoza, A. M., Reina, E. S. & García-Godoy, F. Evolution of apical formation on immature necrotic permanent teeth. Am. J. Dent. 23, 269–274 (2010).
Tootla, S. & Owen, C. P. A comparison of endodontic treatment outcomes between HIV-positive and HIV-negative patients. SADJ 67, 322–325 (2012).
Paredes-Vieyra, J. & Enriquez, F. J. J. Success rate of single- versus two-visit root Canal treatment of teeth with apical periodontitis: a randomized controlled trial. J. Endod. 38, 1164–1169 (2012).
Jordan, R. A., Holzner, A. L., Markovic, L., Brueckner, I. & Zimmer, S. Clinical effectiveness of basic root Canal treatment after 24 months: a randomized controlled trial. J. Endod. 40, 465–470 (2014).
Kandemir Demirci, G. & Çalışkan, M. K. A prospective randomized comparative study of cold lateral condensation versus Core/Gutta-percha in teeth with periapical lesions. J. Endod. 42, 206–210 (2016).
Nesković, J., Zivković, S., Medojević, M. & Maksimović, M. Outcome of orthograde endodontic retreatment–A two-year follow-up. Srp Arh Celok Lek. 144, 174–180 (2016).
Alsulaimani, R. S. Single-visit endodontic treatment of mature teeth with chronic apical abscesses using mineral trioxide aggregate cement: a randomized clinical trial. BMC Oral Health. 16, 78 (2016).
1 et al. Usage of chlorhexidine as a final irrigant in one-visit root Canal treatment in comparison with conventional two-visit root Canal treatment in mandibular molars: a randomized clinical trial. J. Evid. Based Dent. Pract. 22, 101759 (2022).
Cunha, S. A. et al. Effect of endodontic sealer in young molars treated by undergraduate Students - A randomized clinical trial. Braz Dent. J. 31, 589–597 (2020).
Gudac, J., Hellén-Halme, K. & Machiulskiene, V. Prognostic validity of the periapical and endodontic status scale for the radiographically assessed 2-year treatment outcomes in teeth with apical periodontitis: a prospective clinical study. BMC Oral Health. 21, 354 (2021).
Asgary, S. et al. Outcomes of root Canal therapy or full pulpotomy using two endodontic biomaterials in mature permanent teeth: a randomized controlled trial. Clin. Oral Investig. 26, 3287–3297 (2022).
Karaoğlan, F., Miçooğulları Kurt, S. & Çalışkan, M. K. Outcome of single- versus two-visit root Canal retreatment in teeth with periapical lesions: A randomized clinical trial. Int. Endod J. 55, 833–843 (2022).
Subbiya, A. et al. Clinical outcome of nonsurgical root Canal treatment using a matched Single-Cone obturation technique with a calcium Hydroxide-based sealer: A retrospective analysis. J. Endod. 48, 1486–1492 (2022).
Coşar, M., Kandemir Demirci, G. & Çalışkan, M. K. The effect of two different root Canal sealers on treatment outcome and post-obturation pain in single-visit root Canal treatment: A prospective randomized clinical trial. Int. Endod J. 56, 318–330 (2023).
Zamparini, F. et al. The use of premixed calcium silicate bioceramic sealer with warm Carrier-Based technique: A 2-Year study for patients treated in a master program. J. Funct. Biomater. 14, 164 (2023).
Baltieri, P. W. Q. et al. Outcome of nonsurgical root Canal retreatment of teeth with persistent apical periodontitis treated with foraminal enlargement and 2% chlorhexidine gel: A retrospective cohort study. J. Endod. 50, 1551–1559 (2024).
Ferrari Cagidiaco, E. et al. Posterior partial crowns out of lithium disilicate with or without posts: A randomized controlled study at 9 years follow up. J. Dent. 161, 106005 (2025).
Simon, S. et al. Clinical efficacy of root Canal treatment at 2 years using a new ready-to-use injectable calcium silicate-based sealer: A multicentric randomised controlled trial. Int. Endod J. 58, 1420–1432 (2025).
Sundqvist, G., Figdor, D., Persson, S. & Sjögren, U. Microbiologic analysis of teeth with failed endodontic treatment and the outcome of Conservative re-treatment. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 85, 86–93 (1998).
Weiger, R., Rosendahl, R. & Löst, C. Influence of calcium hydroxide intracanal dressings on the prognosis of teeth with endodontically induced periapical lesions. Int. Endod J. 33, 219–226 (2000).
Peters, L. B. & Wesselink, P. R. Periapical healing of endodontically treated teeth in one and two visits obturated in the presence or absence of detectable microorganisms. Int. Endod J. 35, 660–667 (2002).
Chu, C. H., Lo, E. C. M. & Cheung, G. S. P. Outcome of root Canal treatment using thermafil and cold lateral condensation filling techniques. Int. Endod J. 38, 179–185 (2005).
Aqrabawi, J. A. Outcome of endodontic treatment of teeth filled using lateral condensation versus vertical compaction (Schilder’s technique). J. Contemp. Dent. Pract. 7, 17–24 (2006).
Ozer, S. Y. & Aktener, B. O. Outcome of root Canal treatment using Soft-Core and cold lateral compaction filling techniques: a randomized clinical trial. J. Contemp. Dent. Pract. 10, 74–81 (2009).
Riccitiello, F., Stabile, P., Amato, M., Rengo, S. & D’Ambrosio, C. The treatment of the large periradicular endodontic injury. Minerva Stomatol. 60, 417–426 (2011).
Pirani, C. et al. Prognosis of root Canal treatments filled with thermafil system: a 5-year retrospective study. Giornale Italiano Di Endodonzia. 30, 46–51 (2016).
Pirani, C. et al. The fate of root canals obturated with thermafil: 10-year data for patients treated in a master’s program. Clin. Oral Investig. 23, 3367–3377 (2019).
Zandi, H. et al. Outcome of endodontic retreatment using 2 root Canal irrigants and influence of infection on healing as determined by a molecular method: A randomized clinical trial. J. Endod. 45, 1089–1098e5 (2019).
Kurt, S. M., Demirci, G. K., Serefoglu, B., Kaval, M. E. & Çalışkan, M. K. usage of chlorhexidine as a final irrigant in one-visit root Canal treatment in comparison with conventional two-visit root Canal treatment in mandibular molars: a randomized clinical trial. J. Evid. Based Dent. Pract. 22, 101759 (2022).
Bardini, G. et al. A 4-year follow-up of root Canal obturation using a calcium silicate-based sealer and a zinc oxide-eugenol sealer: A randomized clinical trial. Int. Endod J. 58, 193–208 (2025).
Marconi, D. F. et al. Influence of the root Canal filling technique on the success rate of primary endodontic treatments: a systematic review. Restor. Dent. Endod. 47, e40 (2022).
Sabeti, M. A., Karimpourtalebi, N., Shahravan, A. & Dianat, O. Clinical and radiographic failure of nonsurgical endodontic treatment and retreatment using Single-cone technique with calcium Silicate-based sealers: A systematic review and Meta-analysis. J. Endod. 50, 735–746e1 (2024).
Cardinali, F. & Camilleri, J. A critical review of the material properties guiding the clinician’s choice of root Canal sealers. Clin. Oral Investig. 27, 4147–4155 (2023).
Donnermeyer, D., Bürklein, S., Dammaschke, T. & Schäfer, E. Endodontic sealers based on calcium silicates: a systematic review. Odontology 107, 421–436 (2019).
Al-Haddad, A., Ab Aziz, C., Yusoff, M. S. B. & Z., & The impact of core-carrier obturation technique on endodontic treatment success rates: A systematic review and meta-analysis. BMC Oral Health. 17 (1), 159 (2017).
Bansal, R., Bansal, P. & Khuller, N. Comparative evaluation of sealing ability and obturation quality of three different root Canal obturation techniques using micro-CT: an in vitro study. World J. Dentistry. 11 (3), 172–177 (2020).
Zamparini, F. et al. The efficacy of premixed bioceramic sealers versus standard sealers on root Canal treatment outcome, extrusion rate and post-obturation pain: A systematic review and meta-analysis. Int. Endod J. 57, 1021–1042 (2024).
Zhekov, K. I. & Stefanova, V. P. Retreatability of bioceramic endodontic sealers: a review. Folia Med. (Plovdiv). 62, 258–264 (2020).
Gandolfi, M. G., Parrilli, A. P., Fini, M., Prati, C. & Dummer, P. M. H. 3D micro-CT analysis of the interface voids associated with thermafil root fillings used with AH plus or a flowable MTA sealer. Int. Endod J. 46, 253–263 (2013).
Acknowledgements
Open access funding partially provided by Ajman University.
Funding
This research project received no external funding. The authors conducted the study independently, with no financial or non-financial support influencing its design, analysis, or reporting.
Author information
Authors and Affiliations
Contributions
Conceptualization, F.E. and K.I.A.; methodology, F.E. and J.A.G.; software, A.M. and S.A.; validation, M.G.F., F.A.S., K.I.A., and P.V.A.; formal analysis, F.E. and J.A.G.; investigation, A.M., S.A., and M.G.F.; resources, F.E., K.I.A., and P.V.A.; data curation, J.A.G., M.G.F., and F.A.S.; writing—original draft preparation, F.E., A.M., and S.A.; writing—review and editing, F.E., J.A.G., F.A.S., K.I.A., and P.V.A.; visualization, M.G.F. and J.A.G.; supervision, F.E. and P.V.A.; project administration, F.E.; funding acquisition, F.E. and K.I.A. All authors have read and agreed to the published version of the manuscript.
Corresponding authors
Ethics declarations
Conflict of interest
The authors declare no conflict of interest.
Institutional review board statement
Not applicable.
Informed consent
Not applicable.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Mushtaq, A., Alsanafi, S., Elmsmari, F. et al. Effect of root canal filling techniques and materials on endodontic treatment outcomes: a systematic review and meta-analysis. Sci Rep 16, 9552 (2026). https://doi.org/10.1038/s41598-026-37936-7
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-026-37936-7
Keywords
- Apical periodontitis
- Bioceramics
- Carrier-based techniques
- Clinical outcomes
- Cold lateral condensation
- Dental materials
- Dental restoration failure
- Endodontic retreatment
- Endodontics
- Evidence-based dentistry
- Follow-up studies
- Gutta-percha
- Longitudinal studies
- Meta-analysis
- Prognosis
- Radiographic image interpretation, dental
- Root canal filling materials
- Root canal filling techniques
- Root canal therapy
- Systematic review
- Success rate
- Thermoplastic techniques
- Tooth pulp pathology
- Treatment outcome
