
Abstract
This study compares the clinical efficacy of total thoracoscopic surgery (TTS) and thoracoscopy-assisted small-incision surgery (TASIS) in treating multiple rib fractures. A total of 95 patients were included, and propensity score matching (1:1) yielded 70 matched patients (35 per group) for primary comparison. Key perioperative parameters, including operation time, intraoperative blood loss, incision length, chest tube drainage volume, chest tube duration, hospital stay, and postoperative complications, were analyzed. Postoperative pain was assessed using the Visual Analogue Scale (VAS) on days 3 and 7, and clinical efficacy was evaluated at 3 months. No significant differences were observed in chest tube drainage volume, removal time, hospital stay, or complication rates (p > 0.05). However, TTS resulted in significantly shorter incisions but longer operation times (p < 0.05). VAS scores on postoperative days 3 and 7 were lower in the TTS group (p < 0.05), and clinical outcomes at 3 months were superior (p < 0.05). Both TTS and TASIS are effective for multiple rib fractures, but TTS offers less trauma, reduced postoperative pain, and better mid-term clinical outcomes, supporting its use as a minimally invasive approach.
Similar content being viewed by others

Introduction
Multiple rib fractures are a common and severe form of chest trauma, typically caused by high-energy impacts such as traffic accidents, falls, or direct blunt force1. These injuries often result in chest wall instability, leading to significant respiratory distress, pain, and potential pulmonary complications, such as pneumothorax, pleural effusion, and pulmonary infection2,3. Timely and effective treatment is crucial for preventing complications, restoring chest wall stability, and improving patient outcomes4. Traditionally, treatment options for rib fractures have included conservative therapy and open surgery. Conservative management typically relies on chest wall support and respiratory assistance5,6; however, it may inadequately stabilize severely displaced rib fractures, leading to slower recovery and reduced quality of life. While open surgery offers more reliable fracture reduction and fixation7, it is associated with significant trauma, higher rates of postoperative complications, and longer recovery times. Consequently, there has been a growing preference for minimally invasive surgical approaches, which result in less trauma and faster recovery8,9.
In recent years, advancements in minimally invasive techniques have revolutionized the treatment of multiple rib fractures. Compared to traditional open surgery, minimally invasive procedures involve smaller incisions10, reducing surgical trauma9, intraoperative blood loss, and postoperative complications7 while shortening postoperative recovery time. Total thoracoscopic surgery (TTS) and thoracoscopy-assisted small-incision surgery (TASIS) are currently the most widely used minimally invasive techniques11. TTS provides a clear surgical field via thoracoscopy12, allowing for precise fracture reduction and internal fixation9,11, particularly in severe displacement or multiple fractures. TASIS, on the other hand, combines the visual advantages of thoracoscopy with the flexibility of traditional open surgery13, achieving effective fixation through small incisions7. While both techniques have distinct advantages and limitations, determining the most appropriate approach for individual patients remains a critical focus of clinical research.
As a purely minimally invasive procedure, TTS offers several advantages, including minimal trauma, a clear surgical field, and faster postoperative recovery7, making it particularly suitable for precise internal fixation of rib fractures. Studies have shown that TTS significantly reduces postoperative pain, shortens hospital stays, and lowers the incidence of postoperative pulmonary complications9. However, this technique requires a high level of surgical expertise, involves longer operation times11, and demands specialized equipment, limiting its use in resource-limited healthcare settings. In contrast, TASIS combines the benefits of both minimally invasive and traditional surgery with shorter operation times and simpler procedures and is less dependent on advanced equipment, making it more accessible in various medical environments14. However, because TASIS requires a small incision, patients tend to experience more postoperative pain and longer recovery periods15. Further research is needed to assess its efficacy across different patient populations.
The objective of this case-control study is to systematically compare the efficacy of TTS and TASIS in the treatment of multiple rib fractures. The study evaluates the differences between these two surgical approaches in terms of operation time, intraoperative blood loss, postoperative complications, pain management, hospital stay, and long-term outcomes, aiming to clarify the advantages and limitations of each. The results will provide physicians with evidence-based guidance to optimize treatment decisions and enhance postoperative recovery quality. By assessing TTS’s benefits in reducing postoperative pain, lowering complication risks, and improving quality of life, as well as TASIS’s advantages in operational convenience and broader applicability, we aim to offer more precise surgical options for diverse patient groups. Additionally, this study will serve as a valuable reference for the future adoption of minimally invasive techniques, providing improved clinical strategies for treating multiple rib fractures.
Materials and methods
Clinical data
A retrospective analysis was conducted on 120 patients with multiple rib fractures who underwent surgical treatment in the Department of Cardiothoracic Surgery, Jiangyin Clinical College of Xuzhou Medical University, between January 2022 and January 2024. The inclusion criteria were: (1) rib fractures confirmed by chest Computed Tomography (CT) and 3D reconstruction; (2) significant rib displacement involving more than three ribs; (3) stable vital signs; and (4) complete clinical data.
Exclusion criteria included: (1) patients with severe heart disease, liver or kidney dysfunction, or coagulation disorders; (2) those with severe infections, particularly pulmonary infections; and (3) patients with severe concomitant injuries to the head, abdomen, spine, or limbs.
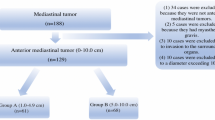
According to the inclusion and exclusion criteria, 25 cases were excluded. Specifically, 10 patients were excluded due to severe heart disease, liver or kidney dysfunction, or coagulation disorders; 5 due to severe infections, particularly pulmonary infections; and 10 due to severe concomitant injuries to the head, abdomen, spine, or limbs. Ultimately, 95 patients were included in the study: 65 males and 30 females, aged 28 to 77 years, with an average age of 54.54 ± 10.16 years.
Selection bias was minimized and group comparability enhanced via propensity score matching (PSM) on age, sex, fracture site (unilateral/bilateral), rib fracture count, and injury cause, using 1:1 nearest-neighbor matching (caliper = 0.2), yielding 70 matched patients (35 per group). According to surgical approach, patients were divided into the totally thoracoscopic group (observation, n = 35) and the thoracoscopic-assisted mini-incision group (control, n = 35) for primary efficacy comparison (Fig. 1). This study was conducted in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. The research protocol was reviewed and approved by the Clinical Ethics Committee of Jiangyin People’s Hospital (Approval number: 2024ER(057)). This statement ensures compliance with ethical standards and confirms that informed consent was obtained from all participants or their legal guardians.

Flow chart of experimental research design.
Surgical methods
All patients underwent surgery within two weeks post-injury under general anesthesia with single-lung ventilation. Preoperative CT with 3D reconstruction and ultrasound was used to locate rib fractures, which were marked on the body surface (Fig. 2A-E).

Preoperative Rib Fracture Localization with 3D CT Reconstruction and Ultrasound. Note: (A) Body surface marking of rib fracture sites prior to CT scan, with “+” marks on the skin to identify the location of surgical incisions. (B) Cross-sectional CT image displaying the transverse structure at the site of the rib fracture for further preoperative localization. (C) Patient positioning in the CT scanner to determine and record the 3D coordinates of the body surface markings, ensuring surgical precision. (D) Ultrasound image showing the fractured rib ends, verifying the fracture condition as an intraoperative reference. (E) Ultrasound used for body surface localization of the rib fracture, marking the fracture site to assist in surgical precision.
In the control group, patients were positioned on the healthy side. A 1.0 cm incision was made at the 7th intercostal space along the mid-axillary line on the affected side, or the chest drainage port was used as the observation port. Using thoracoscopic assistance, the intrathoracic fractures were examined. Based on the preoperative surface markings, incisions were made near the midpoints of the rib fractures, following the rib’s orientation. An arc-shaped incision was made along the scapular margin for fractures near the scapula. The incision length and number varied depending on the number and location of fractures, typically ranging from 8 to 15 cm. Care was taken to carefully separate the chest wall muscles, minimizing unnecessary muscle cutting. The fracture ends were exposed, and bone fragments were removed with minimal periosteal stripping. Displaced ribs were realigned and fixed using TiNi memory alloy embracing devices (Lanzhou Seemine Co., Ltd., Model: 4HL II (10–16)-45 H) (Fig. 3A). Additional 1–2 cm incisions were made in the intercostal spaces above and below the primary incision to further explore the thoracic cavity, control bleeding, debride wounds, and repair diaphragmatic or lung injuries. At the end of the procedure, a chest drainage tube was placed through the observation port (Fig. 3B).

Typical Views of TTS and TASIS. Note: (A) Intraoperative view of TASIS; (B) Postoperative incision view of TASIS; (C) Postoperative incision view of VATS; (D) Complete set of specialized thoracoscopic equipment and TiNi memory alloy fixation devices; (E) Placement of the fixation device on the target rib using a specialized thoracoscopic rib fixator; (F) Fixation device contracting and deforming to stabilize the fractured rib.
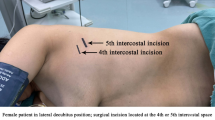
In the observation group, based on the position of the rib fractures, a 4 cm incision was made at the operation site, typically located in the 5th intercostal space near the parasternal line. The incision was placed at an appropriate distance from the fracture site to facilitate surgical access. A second 1.0 cm incision was made in the 7th or 8th intercostal space along the mid-axillary line to serve as the observation port (Fig. 3C). Under thoracoscopic guidance, the thoracic cavity was explored, and procedures such as hemostasis, debridement, and the repair of the diaphragm or lungs were performed. Based on preoperative imaging and thoracoscopic exploration, an electrocautery hook separated the muscles, intercostal tissues, and periosteum around the fracture site, exposing the fracture ends. Heart-shaped reduction forceps were used to realign the fracture, and TiNi memory alloy embracing devices (Lanzhou Seemine Co., Ltd., Model: 6Z (12–24)-(80–120)) were applied for fixation (Fig. 3D). A specialized thoracoscopic rib plate inserter (Fig. 3E) delivered the memory alloy device to the targeted rib. The device was positioned at the superior and inferior edges of the fractured rib and was restored to its original shape by flushing it with sterile warm saline at 45–50 °C, effectively stabilizing the fracture (Fig. 3F). A simplified schematic of the device operation is shown in Fig. 4. The thoracic cavity was then irrigated, incisions were sutured, and a chest drainage tube was placed through the observation port to complete the procedure.

Schematic of the simplified device operation.
Clinical indicators
Surgical indicators
The surgical indicators for both groups included operation time, incision length, intraoperative blood loss, number of fixed fractured ribs, total chest tube drainage volume within the first 3 postoperative days, duration of chest tube placement, postoperative hospital stay, and postoperative complications (such as pulmonary infection, atelectasis, pleural effusion, and incision infection).
Pain assessment
Pain levels were assessed preoperatively and on postoperative days 3 and 7 using the Visual Analogue Scale (VAS)16. The VAS (as shown in Fig. 5) ranges from 0 to 10, with 0 indicating no pain and 10 representing unbearable pain. A higher score indicates more severe pain.

VAS.
Clinical efficacy
Clinical efficacy at 3 months post-surgery was evaluated for both groups based on the following criteria: “Cured” was defined as the absence of chest wall pain, sensory abnormalities, and respiratory dysfunction. “Markedly effective” referred to occasional mild chest wall pain or sensory abnormalities without respiratory dysfunction. “Improved” indicated intermittent mild chest wall pain, occasional sensory abnormalities, mild respiratory dysfunction, and unsatisfactory chest wall appearance. “Ineffective” was characterized by persistent chest wall pain and sensory abnormalities, respiratory dysfunction affecting daily life and work, and dissatisfaction with chest wall appearance.
Postoperative analgesia management
A standardized multimodal analgesia protocol was implemented to minimize the influence of regimen differences on pain assessment: (1) Basic analgesia: continuous intravenous infusion of sufentanil (0.02 µg/kg/h) combined with flurbiprofen axetil (50 mg q12h) for the first 24 h postoperatively; (2) Rescue analgesia: intravenous parecoxib sodium 40 mg administered when VAS ≥ 4; (3) Non-pharmacological interventions: incision ice application beginning 6 h after surgery, three times daily, along with breathing exercises. The protocol was standardized by the Department of Anesthesiology and Pain Medicine, and the nursing team documented drug dosages and rescue analgesia frequency.
Statistical analysis
In multivariable analyses, potential confounders were controlled using multiple linear regression for continuous outcomes and logistic regression for categorical outcomes. Time-related repeated measures were analysed with repeated-measures analysis of variance (ANOVA) or, when model assumptions were not met, generalized estimating equation (GEE) models to assess time effects and between-group differences. Baseline imbalances between groups were addressed using propensity score matching (PSM); after matching, primary continuous and categorical outcomes were compared with paired t-tests and McNemar’s tests, respectively. As a sensitivity analysis, we re-fitted multiple linear regression models in the unmatched cohort to verify the robustness of the PSM-based findings. For key continuous outcomes (e.g., operative time, VAS pain scores, length of hospital stay), we report between-group mean differences (MDs) with 95% confidence intervals (CIs), whereas for categorical outcomes (e.g., complication rates, ordinal response categories) we report odds ratios (ORs) with 95% CIs. For the multivariable analysis of VAS pain scores, we specified a multiple linear regression model including surgical approach, age, sex, number of fractured ribs, number of fixed ribs and analgesic consumption, and present standardized regression coefficients (β), 95% CIs and P values to quantify the independent effect of surgical approach. Correlations between incision length and length of stay were examined using Pearson’s correlation, and correlations between intraoperative blood loss and complications using Spearman’s rank correlation. All statistical tests were two-sided, with p < 0.05 considered statistically significant. Statistical analyses were performed with R version 4.0.3 (MatchIt package) and SPSS version 26.0, and data were visualized using box plots, scatter plots or Kaplan-Meier curves, as appropriate.
Results
Analysis of baseline data and surgical indicators
Table 1 presents the baseline characteristics of the two groups after PSM. No statistically significant differences were observed in sex, age, cause of injury, fracture site (unilateral/bilateral), or number of rib fractures (p > 0.05), indicating effective matching and balanced baseline characteristics between groups.
After propensity score matching, comparisons of operative parameters between the two groups are summarized in Table 2. Operative time was significantly longer in the TTS group than in the TASIS group (128.4 vs. 98.7 min, p < 0.001), with an estimated mean increase of 29.7 min (MD = 29.7, 95% CI: 17.8–41.6). In contrast, incision length was markedly shorter in the TTS group (3.2 vs. 10.3 cm, p < 0.001), corresponding to a mean reduction of 7.1 cm (MD = − 7.1, 95% CI: −8.0 to − 6.2), highlighting a clear minimally invasive advantage.
For other operative variables, including intraoperative blood loss (MD = 4.4, 95% CI: −15.8 to 24.6, p = 0.661), number of ribs fixed (MD = 0.1, 95% CI: −0.5 to 0.7, p = 0.749), chest drainage volume within 3 days postoperatively (MD = 16.5, 95% CI: −72.9 to 105.9, p = 0.704), chest tube duration (MD = − 0.3, 95% CI: −1.2 to 0.6, p = 0.510), and postoperative length of stay (MD = − 0.5, 95% CI: −1.7 to 0.7, p = 0.352), no statistically significant differences were observed between the two groups.
The overall incidence of postoperative complications was also comparable between TTS and TASIS (8.6% vs. 14.3%, p = 0.450), and effect-size analysis showed no clear difference in complication risk (OR = 0.56, 95% CI: 0.14–2.28).
Taken together, TTS and TASIS demonstrated similar performance in most operative and safety endpoints. Although TTS was associated with a longer operative time, it achieved a substantially shorter incision, while other intraoperative and postoperative recovery parameters remained essentially comparable.
Analysis of the impact of Age, Comorbidities, and surgical trauma on postoperative recovery
.
This study evaluated the associations of age, comorbidities, and markers of surgical trauma with postoperative recovery in the PSM-matched cohort (n = 70; Table S1). Subgroup comparisons showed that patients aged >60 years had a longer postoperative length of stay than those aged ≤60 years (9.7 ± 2.4 vs 7.1 ± 1.8 days; p = 0.038), corresponding to a 36.6% relative increase, and had higher odds of postoperative complications, although this did not reach statistical significance (OR = 2.47, 95% CI: 0.86–7.11; p = 0.092) (Table S2). Patients with comorbidities stayed in hospital longer than those without comorbidities (11.2 ± 2.1 vs 7.6 ± 1.7 days; p (Table S1,S2).Shorter incisions were associated with lower postoperative pain scores (5.2 ± 1.2 vs 8.4 ± 0.8); the relative reduction was 38% based on group means (Tables S1, S2).
Correlation analyses further supported the association between surgical trauma markers and recovery: incision length was positively correlated with postoperative length of stay (Pearson r = 0.45, p < 0.01), and intraoperative blood loss was positively correlated with postoperative complications (Spearman r = 0.38, p < 0.05) (Table S1). In an adjusted model for postoperative pain score, surgical approach remained independently associated with pain score, whereas age was not statistically significant (Table S3)..
Taken together, advanced age, the presence of comorbidities, and greater surgical trauma were associated with delayed postoperative recovery; incision length correlated with postoperative length of stay, and intraoperative blood loss correlated with postoperative complications.
Comparison of preoperative and postoperative VAS scores on days 3 and 7 between the two groups
Preoperative VAS scores were comparable between groups (p = 0.497). As shown in Table 3, after PSM, postoperative pain scores were significantly lower in the TTS group compared with the TASIS group (day 3: 3.45 vs. 4.22, p < 0.001; day 7: 2.12 vs. 2.91, p < 0.001). In both groups, postoperative scores decreased significantly from baseline (all p < 0.001), with a greater reduction in the TTS group (day 7 vs. day 3: -38.6% vs. -31.0%). These findings indicate superior postoperative pain relief in the observation group, particularly in early postoperative pain management.
Effect-size analysis showed that the TTS group had a 0.77-point lower VAS score than the TASIS group on postoperative day 3 (MD = − 0.77, 95% CI: −1.05 to − 0.49, p < 0.001) and a 0.79-point lower score on day 7 (MD = − 0.79, 95% CI: −1.18 to − 0.40, p < 0.001). In repeated-measures ANOVA, both the main effect of time and the time-by-group interaction were statistically significant (F = 12.63, p < 0.001), confirming a differential temporal pattern of pain relief between the two approaches.
Postoperative analgesic consumption did not differ significantly between the groups (48.3 ± 6.2 µg vs. 50.1 ± 7.1 µg, p = 0.214). In a multiple linear regression model including surgical approach, age, sex, number of fractured ribs, number of fixed ribs and analgesic use, surgical approach remained independently associated with postoperative VAS scores (β = −0.86, 95% CI: −1.21 to − 0.52, p < 0.001), whereas the other covariates were not significant (all p > 0.05; Table S3).
Analysis of patient satisfaction and clinical efficacy
All patients completed a standardized questionnaire (Supplementary Materials) assessing postoperative satisfaction in terms of pain relief, incision cosmesis, and functional recovery, scored from 0 (extremely dissatisfied) to 10 (extremely satisfied). Patients were categorized into high (≥ 8) and low (< 8) satisfaction groups (Table 4). After PSM, the TTS group showed significantly higher satisfaction (91.4% vs. 71.4%, p = 0.008) and a higher 3-month cure rate (71.4% vs. 51.4%, p = 0.021) than the TASIS group. Effect-size analysis showed that patients in the TTS group were approximately 4.7 times more likely to report high satisfaction compared with those in the TASIS group (OR = 4.67, 95% CI: 1.20-18.13, p = 0.008), and the 3-month clinical cure rate was about 2.9 times higher in the TTS group (OR = 2.85, 95% CI: 1.12–7.23, p = 0.021). All patients were followed up for three months, and no rib fixation plates were found to be dislodged. The clinical efficacy at three months post-surgery in the observation group was significantly better than that in the control group, with a statistically significant difference (Fig. 6, p < 0.05). Overall, the observation group showed significantly better postoperative clinical efficacy and patient satisfaction than the control group.

Postoperative satisfaction stacked chart.
Discussion
This study compared the clinical outcomes of TTS and TASIS in the treatment of multiple rib fractures. PSM was used to balance potential confounders such as age, sex, and fracture severity, thereby enhancing comparability between groups and minimizing selection bias, which increased the credibility of differences in outcomes such as postoperative pain relief and long-term efficacy. The results demonstrated that TTS offered advantages in reducing surgical trauma, alleviating postoperative pain, and improving long-term outcomes, whereas TASIS showed benefits in operative time and procedural convenience. The following discussion integrates these findings with existing literature, focusing on operative time, complications, pain management, length of hospital stay, and long-term clinical outcomes.
Operation time and degree of trauma
In the present study, the operative time of TTS was significantly longer than that of TASIS (128.4 vs. 98.7 min after PSM), which is consistent with previous reports that total thoracoscopic procedures are technically demanding and associated with prolonged operating times30,31. A more detailed analysis of our intraoperative workflow suggests that several specific steps contribute to this difference. First, complete thoracoscopic exploration and adhesiolysis must be performed under a limited field of view, and reduction of displaced rib fragments is achieved entirely with endoscopic instruments. This requires repeated fine adjustment of the heart-shaped reduction forceps and TiNi embracing devices to obtain a satisfactory three-dimensional alignment, whereas in TASIS, fracture reduction can be performed more directly under open vision through a small incision. Second, intrathoracic delivery, positioning, and deployment of the memory alloy devices through narrow intercostal ports is time-consuming. Similar to the experience of Pieracci with completely thoracoscopic SSRF, the need for angled drills and screwdrivers, meticulous plate orientation, and confirmation of fixation under endoscopic visualization inevitably prolongs the procedure11.
The learning curve also plays an important role. Early attempts at completely thoracoscopic SSRF have been reported in only a small number of cases and were explicitly limited by surgeon inexperience and immature instrumentation11. Our findings are in line with this: in the subgroup of fractures located near the medial scapular border and paraspinal region, the time difference between TTS and TASIS gradually narrowed as the operating team accumulated experience with port placement, thoracoscopic exposure, and device manipulation. In these anatomically challenging areas, TASIS often requires a longer skin incision and extensive muscle dissection to obtain an adequate operative window, whereas thoracoscopy provides wide intrathoracic visualization of subscapular and very posterior ribs through small ports, thereby partially offsetting the time spent on thoracoscopic reduction and fixation11.
Despite the longer operative time, TTS clearly reduces the degree of soft-tissue trauma. In our cohort, the mean incision length in the TTS group was approximately one-third of that in the TASIS group, and subgroup analysis showed that longer incisions were independently associated with poorer pain relief and longer hospital stay, underscoring the clinical impact of surgical trauma.
Previous experimental and clinical studies have demonstrated that smaller surgical wounds are associated with attenuated systemic inflammatory responses and faster recovery32,33. Our results support this concept: although TTS required a longer procedure, it was associated with less postoperative pain and better 3-month functional outcomes, suggesting that minimizing tissue disruption may compensate for the additional operating time and ultimately benefit mid-term recovery.
Intraoperative blood loss and postoperative complications
This study found no significant differences between the two groups in terms of intraoperative blood loss and postoperative complications, such as pulmonary infection, atelectasis, pleural effusion, and incision infection. Previous studies have shown that both surgical approaches are equally effective in controlling intraoperative blood loss and preventing postoperative complications34. Although TTS is a minimally invasive technique, it did not show a significant advantage in reducing the incidence of postoperative complications, which may be attributed to patient variability, procedural complexity, and postoperative management34. In contrast, with its shorter operation time, TASIS may offer advantages in reducing intraoperative stress and associated surgical risks.
Postoperative pain management
VATS was associated with significantly lower VAS pain scores on postoperative days 3 and 7 compared with the thoracoscopy-assisted small-incision approach. Consistent with these results, Miyazaki et al. demonstrated that the smaller incision and minimally invasive nature of VATS reduce intercostal nerve injury, particularly to Aβ and Aδ fibers, thereby alleviating postoperative pain. CPT testing confirmed preserved postoperative nerve function and a lower incidence of persistent pain compared with thoracotomy and minithoracotomy (p < 0.05)18. This study supports this finding, further emphasizing the significant advantage of TTS in managing postoperative pain. Additionally, TTS reduced the need for postoperative analgesics, enhancing patient comfort and overall quality of life.
Postoperative hospital stay and recovery
This study found no significant difference in postoperative hospital stay between the two groups. Although TTS is theoretically expected to accelerate recovery due to its minimally invasive nature, consistent with previous research, no significant reduction in hospital stay was observed in this study34. This result may be attributed to the small sample size, patient variability, and differences in postoperative care. However, the advantages of TTS in pain management may offer the potential for faster functional recovery. Future research with larger sample sizes is needed to further assess the long-term impact of different surgical approaches on recovery speed.
Comparison of Long-Term clinical efficacy
At the 3-month follow-up, the TTS group’s long-term clinical efficacy was significantly better than that of the TASIS group. Previous studies comparing complete VATS with traditional open surgery in patients with multiple rib fractures have shown that the two approaches achieve similar radiographic outcomes in fracture fixation. However, VATS, through precise localization and minimally invasive techniques, may help reduce postoperative scar formation and is theoretically more conducive to fracture healing and functional recovery10. Our study further supports these findings, indicating that despite TTS’s complexity and longer operation time, its potential for improved long-term functional recovery and quality of life makes it a preferred option for treating multiple rib fractures.
Review of relevant literature
We conducted a comprehensive review of articles published between 2010 and 2024 using the PubMed database, with search terms including “Total thoracoscopic surgery,” “Thoracoscopic-assisted small-incision surgery,” “Multiple rib fractures,” “Memory alloy hugging device,” and “TiNi memory alloy hugging device.” Eighteen articles most relevant to the topic were selected, summarizing the clinical presentation, diagnostic methods, treatment, and prognosis of patients. A detailed discussion of these findings is provided in several key areas (Table 5).
Case characteristics
The reviewed literature primarily involves cases of multiple rib fractures with associated complex injuries, such as diaphragmatic injury, acute respiratory failure (ARF), and pulmonary contusion. Powell L and colleagues reported cases of traumatic diaphragmatic injury combined with multiple rib fractures, emphasizing the commonality and diagnostic challenges of diaphragmatic injury in rib fractures19. Wu TH’s research team described cases of severe blunt chest trauma leading to ARF and ventilator dependence, highlighting how complex injuries like pulmonary contusion can exacerbate patient outcomes20.
The studies also indicate that treating elderly and critically ill patients poses additional challenges. Zhang G’s team, in their research on rib fixation in highly elderly patients, found that despite their frail condition, these patients demonstrated good tolerance and recovery following video-assisted thoracoscopic surgery (VATS), with a significant reduction in complication rates21.
Advances in diagnostic techniques
The traditional diagnosis of chest trauma has primarily relied on X-rays and CT scans; however, the literature shows that thoracoscopy has significantly improved diagnostic accuracy in complex cases. Powell’s research team reported that thoracoscopy significantly increased the detection rate of diaphragmatic injuries in patients with multiple rib fractures19. Wemeijer TM and colleagues explored the use of diagnostic thoracoscopy during rib fixation procedures to identify overlooked injuries, demonstrating its effectiveness in detecting additional complications22.
Furthermore, emerging imaging technologies are increasingly being applied in chest trauma diagnosis. Wang YJ’s study introduced the use of electrical impedance tomography (EIT) in severe chest trauma cases, highlighting its significant role in postoperative monitoring and enhancing lung function recovery23.
Therapeutic applications
Several studies have demonstrated the effectiveness of VATS and other minimally invasive techniques in treating multiple rib fractures, diaphragmatic injuries, and pulmonary contusions. Tarng YW and colleagues showed that the use of thoracoscopy and titanium elastic nails in blunt chest trauma effectively reduced ventilator dependency and shortened intensive care unit (ICU) stays24. Similarly, a 2020 study by Wu et al. found that rib fixation significantly decreased postoperative pneumonia incidence and ventilator duration in patients with severe blunt chest trauma20.
VATS has also shown distinct advantages in addressing complex injuries. For instance, Murfee JR et al. reported in 2022 a case of rib fractures accompanied by a diaphragmatic hernia, successfully repaired via thoracoscopy, with excellent postoperative recovery25. Lee J and colleagues, in a 2017 study, highlighted the superiority of thoracoscopy in treating delayed-onset chylothorax26.
With advancing technology, 3D printing-assisted rib fixation is also gaining clinical application. In 2023, Zhou X’s team demonstrated that 3D printing significantly reduced surgical complications and improved fixation outcomes27.
Clinical outcomes
Most studies indicate that patients undergoing thoracoscopic rib fixation typically experience favorable postoperative recovery. In a 2020 study, Xia H et al. examined thoracoscopic rib fixation in patients with flail chest and pulmonary contusions, showing significant improvements in lung function and shortened recovery times14. Shi J et al., in a 2024 study, further highlighted that rib fixation improved lung function and significantly reduced hospital stays28.
Beshay M’s team emphasized the critical role of a multidisciplinary approach in managing patients with severe pulmonary contusions. Their findings indicated that multidisciplinary collaboration can significantly reduce mortality and yield positive treatment outcomes. Rib fixation has also proven safe and effective in elderly patients29. Zhang G et al. demonstrated in a 2022 study that even in very elderly patients, VATS resulted in good prognoses with high surgical tolerance and low complication rates21.
Limitations of the study
This study has several limitations. First, the small sample size and single-center design may limit the external validity of the results, thereby reducing the generalizability of the findings to a broader population. Secondly, although PSM was applied to reduce confounding bias, matching was based on measurable variables and could not fully account for the influence of unmeasured confounders. Third, differences in surgeons’ skill levels may have influenced surgical outcomes. Future research should standardize surgical procedures to minimize the impact of technical variability. Additionally, the short follow-up period in this study did not allow for a comprehensive assessment of long-term functional recovery. Moreover, some efficacy indicators used in this study include subjective components, which may introduce assessment bias due to the non-blinded nature of surgical interventions. To enhance methodological rigor, future research should integrate objective outcome measures, such as pulmonary function tests, blinded radiologic assessments, and validated patient-reported outcome instruments, and adopt multicenter, large-sample prospective designs with extended follow-up periods to more comprehensively assess the long-term effectiveness and safety of TTS.
Clinical application prospects
Using a rigorous PSM design under balanced baseline conditions, this study further demonstrated that: (1) TTS provides a consistent advantage in alleviating early postoperative pain (VAS score), which is critical for rapid recovery; (2) TTS yields superior 3-month postoperative outcomes and patient satisfaction; and (3) in complex fractures located at challenging sites such as the medial scapular border and paraspinal region, TTS offers unique benefits through enhanced visualization and precise manipulation, albeit with longer operative time. These findings provide robust evidence supporting the role of TTS in improving postoperative quality of life.
Overall, both TTS and TASIS are effective surgical options for multiple rib fractures. TTS, with its minimally invasive nature, superior pain control, and better long-term outcomes, is well-suited for patients with high demands for postoperative pain management and functional recovery, though it requires advanced surgical expertise and involves longer operative time. TASIS, with simpler techniques and shorter operative duration, is suitable for less severe injuries and remains a practical choice in resource-limited settings. Surgical approach should be tailored to patient condition, surgical team expertise, and institutional resources to optimize outcomes and enhance recovery. Further multicenter, large-scale studies are warranted to validate the long-term efficacy of both techniques.
Conclusion
Both TTS and TASIS are effective for the treatment of multiple rib fractures (Fig. 7). In the PSM-matched cohort, TTS required a longer operative time but achieved a markedly shorter incision and better early postoperative pain control (VAS on postoperative days 3 and 7). Clinical efficacy at 3 months was also superior in the TTS group, whereas intraoperative blood loss, chest tube drainage volume within the first 3 postoperative days, chest tube duration, length of hospital stay, and postoperative complication rates were comparable between groups. Therefore, when appropriate expertise and equipment are available, TTS may be considered a preferred minimally invasive option to reduce incision-related trauma and postoperative pain. Larger multicenter studies with longer follow-up are warranted to confirm long-term outcomes.

Comparison of clinical efficacy between TTS and TASIS in treating multiple rib fractures.
Data availability
The datasets generated and/or analyzed during the current study are not publicly available due to privacy and confidentiality agreements with the participants but are available from the corresponding author on reasonable request.
Abbreviations
- ANOVA:
-
Analysis of variance
- ARF:
-
Acute respiratory failure
- CT:
-
Computed tomography
- EIT:
-
Electrical impedance tomography
- GEE:
-
Generalized estimation equation
- ICU:
-
Intensive care unit
- PSM:
-
Propensity score matching
- TASIS:
-
Thoracoscopy-assisted small-incision surgery
- TTS:
-
Total thoracoscopic surgery
- VAS:
-
Visual analogue scale
- VATS:
-
Video-assisted thoracoscopic surgery
References
Pines, G., Gotler, Y., Lazar, L. O. & Lin, G. Clinical significance of rib fractures’ anatomical patterns. Injury 51, 1812–1816 (2020).
Thomas, C. N., Lindquist, T. J., Schroder, L. K. & Cole, P. A. Rib fracture map in High-Energy injuries. J. Orthop. Trauma. 37, e165–e169 (2023).
Kim, M. & Moore, J. E. Chest trauma: current recommendations for rib Fractures, Pneumothorax, and other injuries. Curr. Anesthesiology Rep. 10, 61–68 (2020).
Jiang, Y. et al. Comparison of the effectiveness of surgical versus nonsurgical treatment for multiple rib fractures accompanied with pulmonary contusion. Annals Thorac. Cardiovasc. Surg. 25, 185–191 (2019).
Liu, Y. et al. Surgical versus Conservative therapy for multiple rib fractures: a retrospective analysis. Annals Translational Med. 6, 439–439 (2018).
He, Z. et al. The ideal methods for the management of rib fractures. J. Thorac. Disease. 11, 1078–S1089 (2019).
Bae, C. M., Son, S. A., Lee, Y. J. & Lee, S. C. Clinical outcomes of minimally invasive surgical stabilization of rib fractures using Video-Assisted thoracoscopic surgery. J. Chest Surg. 56, 120–125 (2023).
Ferreira, R. O. M. et al. Surgical versus non-surgical treatment of flail chest: a meta-analysis of randomized controlled trials. Eur. J. Trauma Emerg. Surg. 49, 2531–2541 (2023).
Bauman, Z. M., Beard, R. & Cemaj, S. When less is more: A minimally invasive, intrathoracic approach to surgical stabilization of rib fractures. Trauma. Case Rep. 32, 100452 (2021).
Merchant, N. N. & Onugha, O. Novel extra-thoracic VATS minimally invasive technique for management of multiple rib fractures. J. Visualized Surg. 4, 103–103 (2018).
Pieracci, F. M. Completely thoracoscopic surgical stabilization of rib fractures: can it be done and is it worth it? J. Thorac. Disease. 11, 1061–S1069 (2019).
Franssen, A. J. P. M. et al. Treatment of traumatic rib fractures: an overview of current evidence and future perspectives. J. Thorac. Disease. 16, 5399–5408 (2024).
Kim, S. H., I, H. & Commentary Thoracoscopic-Assisted rib plating: where we are and what we have learned. J. Chest Surg. 56, 126–127 (2023).
Xia, H. et al. Current status and research progress of minimally invasive surgery for flail chest (Review). Experimental Therapeutic Med. https://doi.org/10.3892/etm.2019.8264 (2019).
Zhao, W., Chen, Y., He, W., Zhao, Y. & Yang, Y. Nonintubated minimally invasive chest wall stabilization for multiple rib fractures: a prospective, single-arm study. World J. Emerg. Surgery 2020;15(1):53..
Boonstra, A. M., Preuper, S., Balk, H. R., Stewart, R. E. & G. A. & Cut-off points for mild, moderate, and severe pain on the visual analogue scale for pain in patients with chronic musculoskeletal pain. Pain 155, 2545–2550 (2014).
Guven, H. et al. Moderate hypothermia prevents brain stem oxidative stress injury after hemorrhagic shock. J. Trauma: Injury Infect. Crit. Care. 53, 66–72 (2002).
Miyazaki, T. et al. Assessment and follow-up of intercostal nerve damage after video-assisted thoracic surgery. Eur. J. Cardiothorac. Surg. 39, 1033–1039 (2011).
Powell, L., Chai, J., Shaikh, A. & Shaikh, A. Experience with acute diaphragmatic trauma and multiple rib fractures using routine thoracoscopy. J. Thorac. Disease. 11, 1024–S1024 (2019).
Wu, T. H. et al. Facilitating ventilator weaning through rib fixation combined with video-assisted thoracoscopic surgery in severe blunt chest injury with acute respiratory failure. Critical Care 2020;24(1):49..
Zhang, G. et al. Thoracoscopic-assisted rib plating (TARP): initial single-center case series, including TARP in the super elderly, technical lessons learned, and proposed expanded indications. Trauma Surgery & Acute Care Open vol. 7 e000943 (2022).
Wemeijer, T. M., Hogeboom, W., Steenvoorde, P., Withaar, D. S. & de Groot, R. Missed injuries in trauma patients: the value of a diagnostic thoracotomy or thoracoscopy during surgical stabilisation of rib fractures. Ir. J. Med. Sci. (1971 -). 191, 1285–1289 (2021).
Wang, Y. J. et al. The application of electrical impedance tomography and surgical outcomes of thoracoscope-assisted surgical stabilization of rib fractures in severe chest trauma. Scientific Reports 2024;14(1):9669.
Tarng, Y. W. et al. The surgical stabilization of multiple rib fractures using titanium elastic nail in blunt chest trauma with acute respiratory failure. Surg. Endosc. 30, 388–395 (2015).
Murfee, J. R. et al. Unexpected diaphragmatic hernia among patients undergoing Video-Assisted thoracic surgery for internal fixation of rib fractures. Am. Surgeon™. 88, 618–622 (2021).
Lee, J., Cho, J. S., I, H. & Kim, Y. D. Delayed right chylothorax after left blunt chest trauma: a case report. Journal Med. Case Reports 2017;11(1):98.
Zhou, X. et al. Application of preoperative 3D printing in the internal fixation of posterior rib fractures with embracing device: a cohort study. BMC Surgery 2023;23(1):237.
Shi, J. & Liu, J. Retrospective cohort study of video-assisted thoracoscopic precise positioning reduction and internal fixation and thoracotomy reduction and internal fixation in treating multiple rib fractures. Pakistan J. Med. Sciences 2024;40(8):1632-1637.
Beshay, M. et al. Analysis of risk factors in thoracic trauma patients with a comparison of a modern trauma centre: a mono-centre study. World J. Emerg. Surgery 2020;15(1):45.
Hiroyuki, Kayata Akihiro, Usui Koki, Terakawa Koichi, Inukai Yu, Hashimoto Koji, Amano Fumitaka, Kato Naoki, Shinyama Nobutaka, Mukai Yoko, Yamamoto Naoki, Ikeda Masanori, Morita (2025) Feasibility and efficacy of video-assisted thoracoscopic surgery for the surgical stabilization of rib fractures: a single-center retrospective cohort study European Journal of Trauma and Emergency Surgery 51(1) 10.1007/s00068-025-02955-y
Fredric M., Pieracci (2019) (2019) Completely thoracoscopic surgical stabilization of rib fractures: can it be done and is it worth it? Journal of Thoracic Disease 11(S8) S1061-S1069 10.21037/jtd 10.21037/jtd.2019.01.70
Matthias W., Wichmann (2005) Immunological Effects of Laparoscopic vs Open Colorectal Surgery Archives of Surgery 140(7) 692-10.1001/archsurg.140.7.692
Frank J., Vittimberga David P., Foley William C., Meyers Mark P., Callery (1998) Laparoscopic Surgery and the Systemic Immune Response Annals of Surgery 227(3) 326-334 10.1097/00000658-199803000-00003
Gang, Qian Yefei, Mao Jun, He Lei, Gao (2025) Outcomes of internal rib fixation through complete video-assisted thoracoscopic surgery for multiple rib fractures and flail chest in severe chest trauma European Journal of Trauma and Emergency Surgery 51(1) 10.1007/s00068-024-02720-7
Reference 35 and reference 34 are the same document, please delete reference 35.
Funding
This study was supported by Scientific Research Project of Jiangyin Municipal Health Commission (M202316).
Author information
Authors and Affiliations
Contributions
Xiaofeng Huang and Dengshu Wang contributed equally to the conception and design of the study, data collection, and manuscript drafting. Xuewei Jiang, Song Wu, and Guiping Yu participated in patient enrollment, perioperative management, and data acquisition. Yunqiang Zhang and Ning Sheng provided technical guidance and assisted in surgical procedures. Fei Shen and Yedong Mi supervised the project, contributed to study design, data interpretation, and critical revision of the manuscript. All authors reviewed and approved the final version of the manuscript.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethics approval and consent to participate
This study was conducted in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. The research protocol was reviewed and approved by the Clinical Ethics Committee of Jiangyin People’s Hospital (Approval number: 2024ER(057)). This statement ensures compliance with ethical standards and confirms that informed consent was obtained from all participants or their legal guardians.
Consent for publication
Consent to publish statement was obtained from the participant.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Huang, X., Wang, D., Jiang, X. et al. Comparative clinical study of total thoracoscopic surgery and thoracoscopy-assisted small-incision surgery for multiple rib fractures. Sci Rep 16, 14559 (2026). https://doi.org/10.1038/s41598-026-37976-z
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-026-37976-z
