
Abstract
Low back pain (LBP) is a leading cause of disability worldwide, and manual therapy (MT) is commonly used in its management. However, utilization patterns and perceived effectiveness vary according to training and clinical context, with limited national-level evidence describing how Saudi physical therapists apply MT in routine LBP care. To examine national patterns of MT utilization for LBP among licensed Saudi physical therapists, to identify commonly applied techniques, and to evaluate professional and educational factors associated with perceived effectiveness and frequency of use. A cross-sectional survey was conducted from January to March 2025 using a structured online questionnaire distributed nationwide via professional and social-media platforms. Eligible participants were Saudi Commission for Health Specialties (SCFHS)–licensed physical therapists actively managing LBP. The questionnaire assessed demographics, MT training exposure, frequency and type of MT use, perceived effectiveness, and outcome-measurement practices. Content validity was confirmed by six experts (S-CVI/Avg = 0.96). Data were analyzed using descriptive statistics, chi-square tests, Spearman’s rho correlation, and multivariable ordinal logistic regression (SPSS v28; α < 0.05). Of 182 responses received, 173 met the inclusion criteria. Most participants reported using MT for LBP management, with 89% employing it at least occasionally and 20% reporting routine use. MT was rated as important or very important by 87.9% of respondents, and more than half assigned a perceived usefulness score ≥ 6/10. Greater exposure to MT training was independently associated with higher MT utilization and stronger perceived effectiveness (p < 0.001; Nagelkerke R² = 0.47), whereas years of experience and clinical specialization were not significantly associated. MT is widely used and positively perceived by Saudi physical therapists managing LBP. Variability in its utilization and perceived effectiveness appears primarily related to differences in training exposure. These findings describe current practice patterns and professional perceptions and may inform future educational planning, without inferring clinical effectiveness.
Similar content being viewed by others


Background
Low back pain (LBP) is one of the most prevalent and disabling musculoskeletal conditions worldwide, imposing a substantial clinical and socioeconomic burden. It is not a disease entity but a symptom complex with multifactorial origins, including mechanical, degenerative, and psychosocial factors. Globally, LBP remains the leading cause of years lived with disability, affecting an estimated 619 million people in 2020 and projected to reach 843 million by 20501,2. Although prevalence varies across regions, rates peak among adults aged 45–55 years and are typically higher in women3,4.
Global and regional burden
According to the Global Burden of Disease 2019 report, LBP ranks among the top five causes of disability-adjusted life years (DALYs) among working-age adults5. Its recurrent nature, economic impact, and association with psychological distress have made LBP a significant public-health concern. In Saudi Arabia, the burden mirrors global trends, with prevalence among healthcare professionals and industrial workers reported between 64% and 89%5,6,7. Contributing factors include prolonged standing, heavy lifting, awkward postures, and limited ergonomic awareness5,8. Physical therapists themselves face high rates of work-related LBP due to repetitive bending, manual handling, and extended patient-contact hours5,9.
MT in the management of LBP
Evidence-based guidelines recommend a multimodal approach to LBP that integrates patient education, exercise therapy, and MT10,11,12. MT comprises skilled, hands-on techniques including joint mobilization, manipulation, and soft-tissue treatment aimed at reducing pain and restoring function13. Techniques such as Maitland, Kaltenborn, Mulligan, and Cyriax represent major schools of MT practice14,15,16,17. When combined with exercise and behavioral interventions, MT enhances outcomes across acute and chronic LBP populations18,19,20. Despite this evidence, MT utilization varies considerably among practitioners, influenced by therapists’ clinical reasoning, beliefs, and—crucially—training exposure21,22. Countries with structured postgraduate MT certification programs, such as the UK and Australia, demonstrate higher utilization and confidence compared to regions with inconsistent training opportunities23,24. Understanding these contextual variations is essential for identifying educational and systemic barriers.
Current evidence gap
Although global surveys have explored MT practice trends, studies from Saudi Arabia are scarce. Research from neighboring Middle Eastern regions highlights considerable variability in MT use linked to heterogeneous curricula and limited continuing-professional-development (CPD) options25,26,27. Preliminary Saudi data indicate that MT is taught at the undergraduate level, yet formal certification and advanced training remain inconsistent across universities28. Given the rapid expansion of the physiotherapy workforce, a national investigation is warranted to determine how Saudi physical therapists currently employ MT and how training exposure influences their clinical decision-making.
Clinical and educational relevance
Musculoskeletal disorders are among the leading causes of disability and outpatient physiotherapy visits in Saudi Arabia29. Assessing MT practice patterns can inform evidence-based updates to physiotherapy curricula and guide national CPD frameworks consistent with Vision 2030 healthcare transformation goals. Clarifying whether clinical experience or structured MT training better predicts perceived usefulness can also direct future investment toward the most impactful educational strategies.
Theoretical framework and rationale
Manual-therapy decision-making models, including the Maitland and International Federation of Orthopaedic Manipulative Physical Therapists (IFOMPT) frameworks, emphasize integration of patient assessment, therapist expertise, and current evidence30,31. Without consistent training, however, therapists may under- or overutilize specific techniques. Empirical evidence linking MT education levels to actual clinical practice remains limited in Middle Eastern contexts32,33,34. Investigating these associations can clarify whether educational investment translates into tangible practice changes—an issue central to evidence-based physiotherapy education.
Objectives and hypotheses
This study aimed to1: determine the frequency and types of MT techniques used by licensed Saudi physical therapists managing LBP2; assess their academic and professional training in MT3; evaluate perceptions of MT effectiveness; and4 identify predictors of MT utilization and perceived usefulness. It was hypothesized that therapists with greater academic and clinical exposure to MT would employ it more frequently and perceive it as more effective, whereas experience and specialization would show weaker associations.
Expected contribution
This investigation provides the first national-level data on MT utilization patterns among Saudi physical therapists treating LBP. The findings are expected to inform evidence-based educational planning, strengthen CPD policies, and highlight priorities for integrating advanced MT competencies into Saudi physiotherapy curricula.
Materials and methods
Study design
A national cross-sectional survey was conducted to investigate the utilization patterns and perceived effectiveness of MT among Saudi physical therapists treating patients with LBP. The cross-sectional design was selected because it provides a snapshot of prevailing clinical practices and professional beliefs at a single time point, enabling assessment of associations between MT exposure, experience, and utilization without manipulation of variables35. The study conformed to the ethical standards of the World Medical Association Declaration of Helsinki (2013).
Study setting and duration
Data were collected over three months (January–March 2025) across the five major Saudi regions—Central, Western, Eastern, Northern, and Southern—to ensure geographic representativeness of therapists working in governmental, semi-governmental, and private settings36. The healthcare institutions that operate under government ownership or oversight while maintaining administrative and financial autonomy (e.g., military, university, and specialized authority hospitals). The questionnaire was administered electronically via Google Forms and disseminated through professional and social-media networks (WhatsApp, LinkedIn, Telegram, Snapchat), maximizing national reach and minimizing logistical constraints37.
Participants
Eligible participants were licensed physical therapists registered with the SCFHS who were currently practicing in Saudi Arabia and actively treating patients with LBP. Participation required completion of an electronic informed-consent statement before access to the survey. Exclusion criteria included non-practicing therapists, students or interns not yet licensed by the SCFHS, and respondents providing incomplete or duplicate submissions. A convenience-sampling approach was employed to enhance national reach and feasibility while recruiting licensed physical therapists across diverse practice settings38.
Ethical considerations
Ethical approval was obtained from the Institutional Review Board (IRB) Sub-Committee of the College of Medicine, King Saud University (IRB approval reference no. 25/0010/IRB, dated: 07/01/2025). Data were collected anonymously; no personal identifiers (names, phone numbers, or IP addresses) were stored. Participants were informed about the study purpose, confidentiality, voluntary participation, and their right to withdraw at any stage. Iinformed consent was obtained electronically on the first page of the online survey, where participants were required to confirm their voluntary agreement before proceeding39.
Sample-size estimation
Sample size was estimated using the Raosoft online calculator (http://www.raosoft.com/samplesize.html)40. Assuming a total population of 11,716 licensed physical therapists41, a 95% confidence level, and a 5% margin of error, the minimum required sample was 162. To compensate for potential exclusions and incomplete responses, an additional 10–15% was targeted, yielding a final sample of 182. This sample provided > 80% power to detect moderate associations among categorical variables using chi-square (χ²) tests42.
MT utilization questionnaire (MTUQ) development
A structured questionnaire was developed after reviewing previously validated instruments exploring MT utilization and perceptions43,44,45. It comprised five sections1: participant consent2, demographic data3, education and training in MT4, clinical practice patterns for LBP, and5 perceived importance and effectiveness of MT. The survey combined multiple-choice, single-response, and short-answer items, with skip-logic to exclude ineligible participants automatically. Average completion time was approximately 10 min.
Content validity
Content validity was assessed by six independent experts in MT and rehabilitation science representing different Saudi hospital systems. Each expert rated the clarity and relevance of every item on a 4-point scale (1 = irrelevant, 4 = highly relevant)46. Ratings ≥ 3 were coded 1 (acceptable) and ≤ 2 as 0 (unacceptable). The scale-level content-validity index (S-CVI/Ave)—the mean proportion of agreement across items—was 0.96, indicating excellent content validity47. Terminology and phrasing were refined based on expert feedback. A supplemental Table S1 summarizes the Item-level content validity index (I-CVI) and scale-level content validity (S-CVI) while Table S2 presented the summary of psychometric validation results for the MTUQ (n = 6 experts). A supplemental Appendix A explains the content validity assessment scoring method and its interpretations accordingly.
Because the Universal Agreement Index (S-CVI/UA) is a highly conservative indicator that decreases with increasing numbers of experts, the Scale-level Content Validity Index (S-CVI/Ave) was considered the primary criterion for evaluating overall content validity. This is why COSMIN does not require S-CVI/UA as a pass/fail criterion.
Questionnaire content and variables
Demographic information
Participants reported age, gender, region, height, weight, body-mass index (BMI), academic qualification, years of clinical experience, work setting (private, governmental, semi-governmental, university, military, specialized, or primary-care), and clinical specialization48.
Education and training in MT
Respondents indicated whether MT was covered in undergraduate curricula, the number and duration of workshops attended, and whether they held formal MT certification49. A composite MT Exposure Level variable was derived from these responses and classified as none, minimal, moderate, high, or extensive, reflecting cumulative academic and practical exposure50.
Clinical practice patterns
Participants described the proportion of LBP patients receiving MT, average sessions per patient, predominant LBP subtypes (acute, subacute, chronic), and specific techniques used—such as Maitland, Kaltenborn, Mulligan, Cyriax, soft-tissue, and neural-mobilization methods51. They also identified primary therapeutic aims (pain relief, mobility restoration, functional improvement, or relaxation) and any adjunctive modalities routinely combined with MT52.
Outcome measures
Therapists indicated standardized instruments used for outcome evaluation, including the Visual Analogue Scale (VAS)53, Numeric Pain Rating Scale (NPRS)54, Roland–Morris Disability Questionnaire (RMDQ)55, Oswestry Disability Index (ODI)56, Quebec Back-Pain Disability Scale (QBPDS)57, and Short Form Health Survey (SF-12/SF-36)58. Functional tests such as the Timed Up-and-Go, Two-Minute Walk Test, and Berg Balance Scale were included to capture performance-based assessments59,60,61.
Perceived importance and effectiveness of MT
Therapists rated the perceived importance of MT on a five-category Likert scale (very unimportant → very important) and on a 10-point numeric scale (0 = least important, 10 = most important). Additional questions evaluated beliefs regarding MT’s efficacy and its role within multimodal rehabilitation52.
Pilot testing
A pilot study with ten physical therapists assessed clarity, sequence, and completion time45. Minor adjustments were made to terminology and item order, and pilot data were excluded from the final analysis.
Data collection procedure
After ethical approval, the survey link was disseminated nationally with an introductory statement describing objectives and inclusion criteria. Responses were stored securely on Google’s encrypted platform, accessible only to the research team. Bi-weekly reminders encouraged voluntary participation without coercion46. Google Forms’ “one response per user” restriction prevented duplication. Data collection ceased once the targeted sample size was reached21.
Data Preparation and management
Raw responses were exported to Statistical Package for the Social Sciences (SPSS) version 28 (IBM Corp., Armonk, NY, USA) for analysis. Data cleaning included checks for missing values, outliers, and logical inconsistencies. Continuous variables (e.g., age, BMI, experience) were summarized as mean ± SD, and categorical variables (e.g., gender, qualification, region, specialization) as frequencies and percentages56. Missing data < 5% were handled using pairwise deletion57.
Statistical analysis
Analyses followed a pre-specified plan consistent with established reporting standards54. Descriptive statistics were used to summarize participant characteristics, education and training levels, MT techniques, and perceived importance.
Associations between MT utilization and categorical predictors (e.g., certification, qualification, work setting, experience category) were examined using chi-square (χ²) tests29. Spearman’s rho correlation (ρ) assessed relationships among ordinal variables, including MT exposure level and perceived importance62.
Multivariable ordinal logistic regression was used to identify independent predictors of perceived MT usefulness. Variables demonstrating bivariate associations at p < 0.10 were entered simultaneously into the model, including MT exposure level, treatment aims, and MT use frequency63. Multicollinearity was assessed using variance inflation factors (VIFs) and tolerance statistics; all predictors met accepted thresholds (VIF < 5; tolerance > 0.20), indicating no problematic collinearity. Model performance was evaluated using − 2 log likelihood, Nagelkerke R², and goodness-of-fit statistics. All statistical tests were two-tailed, with p < 0.05 considered statistically significant.
Outcome variables
The primary outcome was the frequency of MT utilization for LBP, categorized as never, occasionally, frequently, or routinely. Secondary outcomes included perceived importance scores (ordinal) and MT exposure level (ordinal predictor).
Quality assurance
All statistical analyses were independently verified by a professional biostatistician to ensure accuracy and reproducibility18. Study reporting adhered to the Checklist for Reporting Results of Internet E-Surveys (CHERRIES) and the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines)42,64.
Results
Participant flow and data preparation
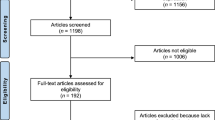
A total of 182 responses were received. Nine respondents were excluded because they were not licensed by the SCFHS or were not actively managing LBP patients, yielding a final analytical sample of 173 participants.
Data cleaning and variable recoding were completed prior to analysis. Composite variables—including MT Exposure Level and Perceived Importance—were created to capture multidimensional constructs from several questionnaire items. A schematic summary of participant assessment, inclusion, exclusion, outcomes, and analysis is presented in Fig. 1.
Demographic characteristics
Table 1 summarizes the sociodemographic and professional characteristics of the participants. The mean age was 31.3 ± 4.5 years, 64.7% were males, and the mean body-mass index was 26.3 ± 5.0 kg/m². Participants were recruited from all regions of Saudi Arabia, with the Central and Western regions contributing the largest proportions.
Most participants held a bachelor’s degree (80.3%), followed by a master’s (17.9%) and doctoral degree (1.7%). Nearly 70% reported fewer than eight years of clinical experience. The most common work settings were private hospitals (29.5%), government hospitals (22.0%), private rehabilitation centers (19.7%), and military hospitals (14.5%).
The majority of physical therapists reported involvement in general physical therapy practice (45.7%) or specialized musculoskeletal physical therapy practice (37.6%).
Education and training in MT
Training characteristics are shown in Table 2. Most respondents (79.8%) reported receiving formal MT instruction during undergraduate education. A total of 79.2% attended at least one professional MT workshop, while 20.8% reported no workshop attendance. Nearly half of the participants (49.7%) reported holding some form of MT certification, most commonly in the Maitland, Mulligan, or Kaltenborn–Evensen concepts.
Composite scoring classified therapists MT exposure level as none (7.5%), minimal (20.2%), moderate (29.5%), high (25.4%), and extensive exposure (17.3%). Workshop duration most frequently ranged from 3 to 5 days (39.9%), followed by 1–2 days (18.5%), more than 8 days (17.3%), and 6–8 days (11.6%). Short-duration workshops (< 1 day) were reported by 12.7% of participants. Workshops predominantly emphasized practical demonstration rather than competency-based assessment.
Reported motivations for persuing MT training included improving clinical competence (65.3%), staying current with evidence-based practice (47.4%), and enhancing patient satisfaction (41.0%).
Clinical practice patterns
MT use for LBP is presented in Table 3. Overall, 89.0% of participants used MT at least occasionally, and 20.2% used it routinely. Most treated both acute and chronic LBP (58.4%).
Soft-tissue mobilization and myofascial release were the most frequently used techniques (68.8%), followed by Mulligan mobilization-with-movement (54.9%), Maitland mobilization (52.0%), Kaltenborn traction (43.9%), Cyriax deep-friction massage (35.8%), and neural mobilization (32.4%).
MT was commonly combined with therapeutic exercise (78.6%), superficial heat therapy (65.9%), and electrotherapy (48.6%). Treatment aims included pain reduction (82.1%), mobility restoration (71.7%), functional improvement (57.8%), and relaxation (19.1%).
Outcome measures
Outcome-measure use is shown in Table 4. Pain intensity was frequently assessed using the VAS (72.3%) or NPRS (63.0%). Disability measures included the ODI (46.8%), RMDQ (39.3%), or QBPDS (18.5%).
Health-status and quality-of-life measures included the SF-12 (16.2%) and the SF-36 (11.0%). Performance-based tests included the TUG test (12.7%), the 2-MWT (11.0%), and the BBS (8.1%). Psychosocial assessment tools included the FABQ (4.6%) and the HADS (4.0%).
Perceived importance of MT
Perceptions are presented in Table 5. MT was rated as important or very important by 87.9% of participants. More than half (55.5%) assigned a score ≥ 6 on the 10-point scale.
MT was rated as equally effective as exercise by 64.7%, more effective by 22.5%, and less effective by 12.7%. Two-thirds (68.0%) indicated that combining MT with exercise yields better outcomes.
Inferential analyses
Training and MT utilization
A chi-square analysis demonstrated a significant association between MT certification status and frequency of MT utilization among physical therapists treating LBP (χ²(2) = 13.65, p = 0.001; Cramer’s V = 0.281) (Table 6). Certified practitioners reported routine use of MT more frequently than non-certified practitioners (24.4% vs. 16.1%). Conversely, non-certified practitioners more often reported never using MT compared with certified practitioners (19.5% vs. 2.3%).
Type of MT used and work setting
The association between type of MT used and current work setting was examined using chi-square analysis (Table 7). MT technique selection differed across work settings (Table 7). No statistically significant association was observed between MT type and work setting (χ²(282) = 288.66, p = 0.380), despite a moderate effect size suggested by Cramer’s V = 0.527.
No significant setting differences were observed for soft-tissue or neural mobilization techniques, these techniques were ubiquitous in all work setting. However, Mulligan and Maitland mobilizations were more frequently reported in private and university facilities, whereas Kaltenborn traction was more common in government hospitals.
Technique use by qualification
No associations was identified between academic qualification and MT technique selection(p > 0.05) (Table 8).
Experience and MT utilization
Experience level was not significantly associated with type or frequency of MT use (χ² = 7.32, p = 0.27) (Table 9). However, qualitative comments indicated that therapists with > 8 years’ experience relied more heavily on individualized clinical reasoning than on standardized protocols.
Correlation analysis
Spearman’s rho correlation between variables are summarized in Table 10. MT exposure level correlated with perceived importance (ρ = 0.61, p < 0.001), frequency of MT use (ρ = 0.54, p < 0.001), and with perceived effectiveness (ρ = 0.49, p = 0.002).
Multivariable ordinal logistic regression
The multivariable ordinal logistic-regression model examined predictors of perceived MT usefulness (Tables 11 and 12). Independent variables included MT exposure level, years of experience, treatment aims, and professional qualification. The model was statistically significant (χ² = 46.71, p < 0.001) with acceptable fit (− 2 Log Likelihood = 233.4; Nagelkerke R² = 0.47).
MT exposure level (B = 1.72, p < 0.001) and treatment aims (B = 0.96, p = 0.004) were significant predictors of perceived MT usefulness. However, qualification and experience were not significant (p > 0.05).
Discussion
Principal findings
This national cross-sectional study provides the first comprehensive account of MT utilization and perceived effectiveness among Saudi physical therapists managing low-back pain (LBP). The results demonstrate that MT is widely used among Saudi physical therapists treating LBP, with nearly 90% reporting some level of use and one-fifth applying it routinely. Soft-tissue, Mulligan, and Maitland techniques dominated clinical practice, and overall attitudes toward MT were strongly positive.
Training exposure emerged as the dominant determinant of both MT utilization and perceived usefulness, while years of experience and academic degree were not influential. This indicates that structured MT education, rather than professional tenure, is the primary driver of MT confidence and integration (35, 50, 71).
Comparison with international literature
The present findings align with international reports describing high MT adoption among physical therapists, though utilization rates and preferred techniques vary by country13,20,23. In Canada, almost 90% of physical therapists incorporate MT for musculoskeletal conditions, while Australian and UK studies report usage exceeding 75% in spinal-disorder cases21,22,44.
In contrast, studies from Asia and the Middle East report lower MT integration due to inconsistent training standards and limited postgraduate certification pathways25,26,27. Saudi therapists’ preference for soft-tissue methods parallels findings from Jordan and Malaysia, where comfort, accessibility, and perceived safety drive similar technique choices51. The limited use of advanced manipulative or neurodynamic techniques likely reflects insufficient postgraduate MT education and continuing-education infrastructure, as well as unclear legal boundaries for spinal manipulation28,50.
Given variations in professional scope, educational pathways, and regulatory frameworks across countries, these findings should be interpreted within the Saudi context and may not be directly generalizable to other healthcare systems.
Training exposure and professional development
Training exposure emerged as the strongest predictor of MT utilization and perceived effectiveness, suggesting that structured MT education is associated with greater professional confidence and evidence-informed practice. This observation is consistent with previous studies by Fritz et al. and Cummings et al., which reported that postgraduate MT training is linked to enhanced clinical reasoning23,30.
In the Saudi context, MT instruction within undergraduate curricula remains variable, and opportunities for structured CPD are limited28. These findings indicate that greater coordination between academic institutions and the SCFHS may support more consistent training pathways. Approaches such as standardized certification frameworks, mentorship-based learning, and modular CPD programs may contribute to more uniform professional preparation, without inferring clinical effectiveness.
Experience and qualification as Non-Significant predictors
Neither years of experience nor highest qualification predicted MT use or perceived effectiveness. This indicates that accumulated clinical exposure alone does not guarantee proficiency in manual skills. Similar patterns have been reported in Turkish and Singaporean studies, where MT utilization was independent of seniority but strongly associated with formal training certification49,55.
This distinction between experiential familiarity and structured competence underscores a paradigm shift in physiotherapy toward lifelong, evidence-based professional learning. It also suggests that postgraduate degrees may prioritize research or management competencies over advanced hands-on training unless explicitly specialized in orthopaedic MT.
Perception of effectiveness and clinical integration
More than 85% of respondents rated MT as important or very important in LBP management, reflecting a strong professional endorsement consistent with global evidence supporting MT’s role in pain reduction and mobility enhancement12,19.
Most participants considered MT equally or slightly more effective than exercise therapy, and two-thirds believed combined application achieves superior results—echoing guideline recommendations favoring multimodal rehabilitation10,11,20.
However, the predominant reliance on subjective pain scales (VAS, NPRS) to evaluate outcomes indicates a gap between clinical perception and objective measurement. Without systematic use of validated disability or function-based tools, clinicians may underestimate or overstate treatment efficacy59,60. This highlights a pressing need for training programs emphasizing standardized outcome documentation as part of evidence-based practice.
It should be noted that this study examined physical therapists’ perceptions and self-reported practice patterns; clinical effectiveness of MT interventions was not evaluated.
Outcome measurement practices
Although pain reduction was the principal therapeutic goal, fewer than half of respondents reported using validated disability indices such as the ODI or RMDQ, and less than 20% utilized performance or psychosocial measures. This selective focus on pain assessment mirrors trends in other developing physiotherapy contexts27,61 and likely reflects time constraints, absence of institutional policy, or insufficient awareness of multidimensional outcome frameworks.
Integrating training modules and electronic record systems that mandate documentation of standardized tools could strengthen clinical accountability, support quality improvement, and promote data-driven practice.
Technique preferences and clinical context
Soft-tissue and Mulligan mobilizations dominated Saudi physiotherapy practice, reflecting their accessibility, ease of instruction, and minimal equipment requirements. Maitland mobilization was also frequently applied, aligning with its global prominence14,15,16,17.
In contrast, Kaltenborn traction and neural-mobilization methods were less common, particularly in primary-care facilities, possibly due to equipment shortages or limited exposure during training. Utilization patterns varied by setting—private hospitals and rehabilitation centers showed higher MT use than government facilities, where institutional hierarchies and restricted autonomy may limit technique selection50.
These findings suggest that organizational structure and clinical governance can substantially influence the adoption of evidence-based manual interventions.
Educational and policy implications
The findings highlight the potential value of greater alignment in MT education across physiotherapy training programs in Saudi Arabia. Incorporating structured MT content—such as biomechanics, contraindications, and patient selection—may help promote more consistent baseline competencies among graduates.
At a national level, CPD frameworks aligned with the SCFHS accreditation may support skill development through tiered certification pathways and mentorship-oriented training models. Such approaches are consistent with national workforce development priorities, including those outlined in Saudi Vision 2030.
Given the observed association between MT training exposure and therapists’ utilization patterns and perceived effectiveness, strengthening educational infrastructure may contribute to more consistent professional practice, without inferring clinical effectiveness or patient outcomes.
Strengths and limitations
The study’s strengths include its national sampling across all major regions, ensuring wide representativeness, and its validated, expert-reviewed instrument (S-CVI/Avg = 0.96). The analytical approach—combining descriptive, correlational, and regression analyses—provided a multidimensional understanding of MT practice determinants.
However, limitations must be acknowledged. The cross-sectional design precludes causal inference, and self-reported data may introduce recall or desirability bias, particularly given the generally favorable perceptions reported toward MT. The convenience-sampling method might have attracted therapists with stronger interest in MT, limiting generalizability. Small subgroup sizes (e.g., doctoral-level or pediatric practitioners) restricted detailed comparison. Finally, the study did not include objective patient outcomes, limiting the ability to correlate therapist-reported perceptions with clinical effectiveness.
Future research should employ longitudinal or experimental designs to evaluate how structured MT training influences measurable patient and therapist outcomes.
Future research directions
Future research should focus on several key areas. Longitudinal and intervention-based studies are needed to evaluate how MT training influences therapists’ competencies and patient outcomes over time. Further investigations should also examine the barriers that hinder the implementation of outcome measures in clinical practice. Comparative studies exploring MT utilization among Saudi-trained and internationally trained physical therapists would provide insights into variations in practice patterns. Additionally, understanding patients’ perceptions of MT is essential to assess its cultural and psychosocial acceptability within different populations. Finally, future work should aim to validate additional psychometric properties of the MT questionnaire, including test–retest reliability and construct validity, to strengthen its utility in research and clinical applications.
Conclusion
MT is widely practiced and positively perceived by physical therapists managing low-back pain in Saudi Arabia. Greater exposure to structured manual-therapy training—rather than years of experience or academic qualification—was the strongest predictor of both utilization and perceived effectiveness, highlighting the influence of education and certification on professional confidence and practice patterns.
Although MT is broadly accepted, variability in training exposure and limited use of standardized outcome measures were observed. These findings provide descriptive insight into current practice patterns and professional perceptions and may inform future alignment of physiotherapy education and continuing professional development initiatives within national regulatory frameworks, without inferring clinical effectiveness.

STROBE (2025) flowchart of participant assessment, inclusion, and analysis. Flow diagram showing the number of responses received, screened for eligibility, excluded (with reasons), and retained for final analysis.
Data availability
The dataset supporting the findings of this study has been deposited in the Open Science Framework (OSF) repository and is openly available at https://osf.io/p2s69/overview? view_only=99d6801264334cd896e30278631f3093 under the title “MT Utilization and Perceived Effectiveness Dataset.”
Abbreviations
- LBP:
-
Low back pain
- MT:
-
Manual Therapy
- SCFHS:
-
Saudi Commission for Health Specialties
- CPD:
-
Continuing-professional-development
- IFOMPT:
-
International Federation of Orthopaedic Manipulative Physical Therapists
- S-CVI:
-
Scale-Level Content Validity Index
- VAS:
-
Visual Analog Scale
- NPRS:
-
Numeric Pain Rating Scale
- RMDQ:
-
Roland–Morris Disability Questionnaire
- QBPDS:
-
Quebec Back-Pain Disability Scale
- SF-12/SF-36:
-
Short Form Health Survey
- SPSS:
-
Statistical Package for the Social Sciences
- CHERRIES:
-
Checklist for Reporting Results of Internet E-Surveys
- STROBE:
-
Strengthening the Reporting of Observational Studies in Epidemiology
- OSF:
-
Open Science Framework
References
Vos, T. et al. Global burden of 369 diseases and injuries in 204 countries and territories, 1990–2019: a systematic analysis for the global burden of disease study 2019. Lancet 396 (10258), 1204–1222. https://doi.org/10.1016/S0140-6736(20)30925-9 (2020).
Ferreira, M. L. et al. Global, regional, and National burden of low back pain, 1990–2020, its attributable risk factors, and projections to 2050: a systematic analysis of the global burden of disease study 2021. Lancet Rheumatol. 5 (6), e316–e329. https://doi.org/10.1016/S2665-9913(23)00098-X (2023).
Hoy, D., Brooks, P., Blyth, F. & Buchbinder, R. The epidemiology of low back pain. Best Pract. Res. Clin. Rheumatol. 24 (6), 769–781. https://doi.org/10.1016/j.berh.2010.10.002 (2010).
Hartvigsen, J. et al. What low back pain is and why we need to pay attention. Lancet 391 (10137), 2356–2367. https://doi.org/10.1016/S0140-6736(18)30480-X (2018).
Yang, Y. et al. Focus on the impact of social factors and lifestyle on the disease burden of low back pain: findings from the global burden of disease study 2019. BMC Musculoskelet. Disord. 24 (1), 679 (2023).
Al Amer, H. S. Low back pain prevalence and risk factors among health workers in Saudi Arabia: a systematic review and meta-analysis. J. Occup. Health 62(1), e12155. https://doi.org/10.1002/1348-9585.12155 (2020).
Aldera, M. A., Alexander, C. M. & McGregor, A. H. Prevalence and incidence of low back pain in the Kingdom of Saudi Arabia: a systematic review. J. Epidemiol. Glob Health 10(4), 269–279. https://doi.org/10.2991/jegh.k.200417.001 (2020).
George, S. Z. et al. Interventions for the management of acute and chronic low back pain: revision 2021. J. Orthop. Sports Phys. Ther. 51 (11), CPG1–CPG60. https://doi.org/10.2519/jospt.2021.0304 (2021).
Qaseem, A., Wilt, T. J., McLean, R. M. & Forciea, M. A. Noninvasive treatments for acute, subacute, and chronic low back pain: a clinical practice guideline from the American college of physicians. Ann. Intern. Med. 166 (7), 514–530. https://doi.org/10.7326/M16-2367 (2017).
Delitto, A. et al. Low back pain. J. Orthop. Sports Phys. Ther. 42 (4), A1–A57. https://doi.org/10.2519/jospt.2012.42.4.A1 (2012).
Oliveira, C. B. et al. Clinical practice guidelines for the management of non-specific low back pain in primary care: an updated overview. Eur. Spine J. 27 (11), 2791–2803. https://doi.org/10.1007/s00586-018-5673-2 (2018).
Nicol, V. et al. Chronic low back pain: a narrative review of recent international guidelines for diagnosis and conservative treatment. J. Clin. Med. 12(4), 1685. https://doi.org/10.3390/jcm12041685 (2023).
Zhou, T., Salman, D. & McGregor, A. H. Recent clinical practice guidelines for the management of low back pain: a global comparison. BMC Musculoskelet. Disord. 25 (1), 344. https://doi.org/10.1186/s12891-024-07468-0 (2024).
Bronfort, G., Haas, M., Evans, R., Leininger, B. & Triano, J. Effectiveness of manual therapies: the UK evidence report. Chiropr. Osteopat. 18, 3. https://doi.org/10.1186/1746-1340-18-3 (2010).
Chitale, N., Patil, D. S., Phansopkar, P. & Joshi, A. A review on treatment approaches for chronic low back pain via mulligan’s movement with mobilization and physical therapy. Cureus 14 (8), e28127. https://doi.org/10.7759/cureus.28127 (2022).
Cankaya, M. S. & Pala, O. O. Outcomes of Mulligan concept applications in obese individuals with chronic mechanical low back pain: a randomized controlled trial. Life (Basel). 14 (6), 754. https://doi.org/10.3390/life14060754 (2024).
Cyriax, J. Textbook of Orthopaedic Medicine 11th edn (Baillière Tindall, 1984).
Neto, T. et al. Effects of lower body quadrant neural mobilization in healthy and low back pain populations: a systematic review and meta-analysis. Musculoskelet. Sci. Pract. 27, 14–22. https://doi.org/10.1016/j.msksp.2016.11.014 (2017).
Bailly, F. et al. Clinical guidelines and care pathway for management of low back pain with or without radicular pain. Jt. Bone Spine 88(6), 105227. https://doi.org/10.1016/j.jbspin.2021.105227 (2021).
Shipton, E. A. Physical therapy approaches in the treatment of low back pain. Pain Ther. 7 (2), 127–137. https://doi.org/10.1007/s40122-018-0105-x (2018).
Ladeira, C. E., Cheng, M. S. & Hill, C. J. Physical therapists’ treatment choices for non-specific low back pain in florida: an electronic survey. J. Man. Manip Ther. 23 (2), 109–118. https://doi.org/10.1179/2042618613Y.0000000065 (2015).
Foster, N. E., Thompson, K. A., Baxter, G. D. & Allen, J. M. Management of non-specific low back pain by physiotherapists in Britain and Ireland. Spine 24 (13), 1332–1342. https://doi.org/10.1097/00007632-199907010-00011 (1999).
Kuik, M., Calley, D., Buus, R. & Hollman, J. Beliefs and practice patterns of spinal thrust manipulation for mechanical low back pain of physical therapists in Minnesota. J. Man. Manip Ther. 32 (4), 421–428. https://doi.org/10.1080/10669817.2023.2279821 (2024).
Alghadir, A. H., Iqbal, Z. A. & Iqbal, A. Knowledge and utilization of manual therapy in the management of knee osteoarthritis by physical therapists in Saudi arabia: a cross-sectional study. BMC Public. Health. 24 (1), 3379. https://doi.org/10.1186/s12889-024-20923-w (2024).
Fairbank, J. C. T. & Pynsent, P. B. The Oswestry disability index. Spine 25 (22), 2940–2953. https://doi.org/10.1097/00007632-200011150-00017 (2000).
Roland, M. & Fairbank, J. The Roland–Morris disability questionnaire and the Oswestry disability questionnaire. Spine 25 (24), 3115–3124. https://doi.org/10.1097/00007632-200012150-00006 (2000).
Roland, M. & Morris, R. A study of the natural history of back pain. Spine 8 (2), 141–144. https://doi.org/10.1097/00007632-198303000-00004 (1983).
Kopec, J. A. et al. The Quebec back pain disability scale. Spine 20 (3), 341–352. https://doi.org/10.1097/00007632-199502000-00016 (1995).
Jenkinson, C. & Layte, R. Development and testing of the UK SF-12. J. Health Serv. Res. Policy. 2 (1), 14–18. https://doi.org/10.1177/135581969700200105 (1997).
Ware, J. E. SF-36 health survey update. Spine 25 (24), 3130–3139. https://doi.org/10.1097/00007632-200012150-00008 (2000).
Waddell, G., Newton, M., Henderson, I., Somerville, D. & Main, C. J. A Fear-Avoidance beliefs questionnaire (FABQ) and the role of fear-avoidance beliefs in chronic low back pain and disability. Pain 52 (2), 157–168. https://doi.org/10.1016/0304-3959(93)90127-B (1993).
Snaith, R. P. & Zigmond, A. S. The hospital anxiety and depression scale. BMJ 292 (6516), 344. https://doi.org/10.1136/bmj.292.6516.344 (1986).
Podsiadlo, D. & Richardson, S. The timed up and go: a test of basic functional mobility for frail elderly persons. J. Am. Geriatr. Soc. 39 (2), 142–148. https://doi.org/10.1111/j.1532-5415.1991.tb01616.x (1991).
Butland, R. J., Pang, J., Gross, E. R., Woodcock, A. A. & Geddes, D. M. Two-, six-, and 12-minute walking tests in respiratory disease. BMJ 284 (6329), 1607–1608. https://doi.org/10.1136/bmj.284.6329.1607 (1982).
Chiarotto, A. et al. Measurement properties of VAS, NRS, and the pain severity subscale of the brief pain inventory in patients with low back pain: a systematic review. J. Pain. 20 (3), 245–263. https://doi.org/10.1016/j.jpain.2018.07.009 (2019).
Alghadir, A., Anwer, S., Iqbal, A. & Iqbal, Z. Test–retest reliability, validity, and minimum detectable change of VAS, NRS and VRS for Osteoarthritic knee pain. J. Pain Res. 11, 851–856. https://doi.org/10.2147/JPR.S158847 (2018).
Yusoff, M. S. B. ABC of content validation and content validity index calculation. Educ. Med. J. 11 (2), 49–54. https://doi.org/10.21315/eimj2019.11.2.6 (2019).
World Medical Association. World medical association declaration of helsinki: ethical principles for medical research involving human subjects. JAMA 310 (20), 2191–2194. https://doi.org/10.1001/jama.2013.281053 (2013).
Algarni, A. S., Ghorbel, S., Jones, J. G. & Guermazi, M. Validation of an Arabic version of the Oswestry index in Saudi Arabia. Ann. Phys. Rehabil Med. 57 (9–10), 653–663. https://doi.org/10.1016/j.rehab.2014.06.006 (2014).
Jenks, A. et al. RMDQ, ODI, and QBPDS: which has superior measurement properties in older adults with low back pain? J. Orthop. Sports Phys. Ther. 52 (7), 457–469. https://doi.org/10.2519/jospt.2022.10802 (2022).
Nicol/Oliveira/George. (refs 7–12) — multimodal recommendation cited in Results/Discussion (already listed; no duplicate entry).
Rubinstein, S. M. et al. Benefits and harms of spinal manipulative therapy for chronic low back pain: systematic review and meta-analysis of RCTs. BMJ 364, l689. https://doi.org/10.1136/bmj.l689 (2019).
Thomas, J. S. et al. Effect of spinal manipulative and mobilization therapies in young adults with mild to moderate chronic low back pain. JAMA Netw. Open. 3 (8), e2012589. https://doi.org/10.1001/jamanetworkopen.2020.12589 (2020).
Guzmán Pavón, M. J. et al. Comparative effectiveness of manual therapy interventions on pain and pressure pain threshold in patients with myofascial trigger points. Clin. J. Pain. 38 (12), 749–760. https://doi.org/10.1097/AJP.0000000000001079 (2022).
Pensri, P., Foster, N. E., Srisuk, S., Baxter, G. D. & McDonough, S. M. Physiotherapy management of low back pain in thailand: a study of practice. Physiother Res. Int. 10 (4), 201–212. https://doi.org/10.1002/pri.16 (2005).
Poitras, S., Blais, R., Swaine, B. & Rossignol, M. Practice patterns of physiotherapists in the treatment of work-related back pain. J. Eval Clin. Pract. 13 (3), 412–421. https://doi.org/10.1111/j.1365-2753.2006.00725.x (2007).
Ladeira, C. E., Cheng, M. S. & da Silva, R. A. Clinical specialization and adherence to Evidence-Based practice guidelines for low back pain management: A survey of US physical therapists. J. Orthop. Sports Phys. Ther. 47 (5), 347–358. https://doi.org/10.2519/jospt.2017.6561 (2017).
Agnus Tom, A., Rajkumar, E., John, R. & Joshua George, A. Determinants of quality of life in individuals with chronic low back pain: a systematic review. Health Psychol. Behav. Med. 10 (1), 124–144. https://doi.org/10.1080/21642850.2021.2022487 (2022).
Maughan, E. F. & Lewis, J. S. Outcome measures in chronic low back pain. Eur. Spine J. 19 (9), 1484–1494. https://doi.org/10.1007/s00586-010-1353-6 (2010).
Hansen, A., Nim, C. G., O’Sullivan, K. & O’Neill, S. Testing walking performance in patients with low back pain: will two minutes do instead of six minutes? Disabil. Rehabil. 46 (6), 1173–1177. https://doi.org/10.1080/09638288.2023.2194683 (2024).
Alanazi, F., Gleeson, P., Olson, S. & Roddey, T. Translation and validation of the Arabic version of the Fear-Avoidance beliefs questionnaire in patients with low back pain. Spine (Phila Pa. 1976). 42 (7), E411–E416. https://doi.org/10.1097/BRS.0000000000001802 (2017).
Hallegraeff, J. M., Van Zweden, L., Oostendorp, R. A. & Van Trijffel, E. Psychological assessments by manual physiotherapists in the Netherlands in patients with nonspecific low back pain. J. Man. Manip Ther. 29 (5), 310–317. https://doi.org/10.1080/10669817.2021.1919283 (2021).
Holopainen, R., Piirainen, A., Karppinen, J., Linton, S. J. & O’Sullivan, P. Physiotherapists’ conceptions of learning and integrating cognitive functional therapy into clinical practice. Physiother Theory Pract. 38 (2), 309–326. https://doi.org/10.1080/09593985.2020.1753271 (2022).
Mourad, F. et al. Knowledge, beliefs, and attitudes of spinal manipulation: a cross-sectional survey of Italian physiotherapists. Chiropr. Man. Th. 30 (1), 33. https://doi.org/10.1186/s12998-022-00449-x (2022).
Ali, M., Uddin, Z. & Hossain, A. Clinical practice pattern of managing low back pain among physiotherapists in bangladesh: a cross-sectional study. Physiother Pract. Res. 43 (2), 93–100 (2022). (If volume/pages differ in your thesis file, keep your originals.).
Anggiat, L. & Rahmansyah, B. Trends in the use of manual therapy among physiotherapists in jakarta: a survey study. Int. J. Sport Exerc. Health Res. 6 (2), 121–125. https://doi.org/10.31254/sportmed.6205 (2022).
Chavula, G. Level of knowledge and practice of manual therapy among physiotherapy practitioners at the university teaching Hospital, Lusaka, Zambia. Int. J. Clin. Exp. Med. Res. 6 (2), 103–110. https://doi.org/10.26855/ijcemr.2022.04.001 (2022).
Hamm, L. et al. Danish physiotherapists’ management of low back pain. Adv. Physiother. 5 (3), 125–131 (2003).
Poitras, S., Blais, R., Swaine, B. & Rossignol, M. Management of work-related low back pain: a population-based survey of physical therapists. Phys. Ther. 85 (11), 1168–1181 (2005).
Rubinstein, S. M. & van Tulder, M. A best-evidence review of diagnostic procedures for neck and low-back pain. Best Pract. Res. Clin. Rheumatol. 22 (3), 471–482. https://doi.org/10.1016/j.berh.2007.12.003 (2008).
Anderson, D. B. & Shaheed, C. A. Medications for treating low back pain in adults: overview for musculoskeletal clinicians. J. Orthop. Sports Phys. Ther. 52 (7), 425–431. https://doi.org/10.2519/jospt.2022.10788 (2022).
Hiroshi, Takasaki Takahiro, Ueno Japanese Clinical Physical Therapists With the Mechanical Diagnosis and Therapy License Are More Competent and Confident in Pain Management Than Those Without It: A Cross-Sectional Study. Cureus. 16:e70652. https://doi.org/10.7759/cureus.70652 (2024).
Birgitta, Widerström Eva, Rasmussen-Barr Carina, Boström. Aspects influencing clinical reasoning and decision-making when matching treatment to patients with low back pain in primary healthcare Musculoskeletal Science and Practice 416-14. http://doi.org/10.1016/j.msksp.2019.02.003 (2019).
Ismail, Saracoglu Meltem Isintas, Arik Emrah, Afsar Hasan Huseyin, Gokpinar. The effectiveness of pain neuroscience education combined with manual therapy and home exercise for chronic low back pain: A single-blind randomized controlled trial. Physiotherapy Theory and Practice. 38(7), 868-878. 10.1080/09593985.2020.1809046 (2022).
Acknowledgements
The authors extend their appreciation to the Ongoing Research Funding program – Research Chairs (ORF-RC-2025-1000), King Saud University, Riyadh, Saudi Arabia for funding this research.
Funding
This study was funded by the Ongoing Research Funding program – Research Chairs (ORF-RC-2025-1000), King Saud University, Riyadh, Saudi Arabia. The funding body played no role in the design, execution, analysis and interpretation of data, or writing of the study.
Author information
Authors and Affiliations
Contributions
Y.M.Z. A.H.A. S.A.A. F.A.A. A.S.A. and A.I. proposed the study conception and design. Y.M.Z. A.H.A and A.I. completed the methodological work and collected data. Y.M.Z. A.H.A. S.A.A. F.A.A. A.S.A. and A.I. contributed to the data analysis and its interpretation. Y.M.Z. and A.I. prepared the manuscript’s initial draft. Y.M.Z. A.H.A. S.A.A. F.A.A. A.S.A. and A.I. critically reviewed and edited the manuscript’s intellectual content. All authors read and approved the manuscript’s final version to be submitted or published and took responsibility for the intellectual content of the same manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethics approval and consent to participate
Ethical approval for this study was conducted by the Institutional Review Board Ethics Committee of the College of Medicine at King Saud University (approval number 25/0010/IRB on 07/01/2025). The study was conducted in accordance with the ethical principles outlined in the Declaration of Helsinki (2010). All participants were informed about the purpose of the study, assured of confidentiality, and provided written consent prior to participation. Participation was voluntary, and respondents could withdraw at any time without consequence.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Zubayni, Y.M., Alhammad, S.A., Alodaibi, F.A. et al. Utilization patterns and perceived effectiveness of manual therapy for low back pain among Saudi physical therapists: a national cross-sectional study. Sci Rep 16, 8551 (2026). https://doi.org/10.1038/s41598-026-38025-5
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-026-38025-5
