
Abstract
This study aimed to clarify the real world evaluation of multiparametric MRI with diffusion-weighted imaging and magnetic resonance cholangiopancreatography for surveillance of patients affected by pancreatic cancer. Findings for 169 high-risk patients who underwent surveillance from June 2017 to February 2023 were analyzed for this multicenter retrospective observational study analyzed. Those included patients who had high risk findings such as cystic lesions identified during screening or incidental imaging examinations, but not findings suggestive of malignancy shown by either EUS or multiparametric MRI. Surveillance was performed every six months using multiparametric MRI and tumor marker assessments. A variant was defined as either main pancreatic duct stenosis with tail-side dilatation, or an area with high signal intensity in diffusion-weighted images and low signal intensity in the apparent diffusion coefficient map. The primary outcome was variant incidence within a six-month period and secondary outcome was positive predictive value for variants. The median follow-up period was 30 months (range 6–78 months). The incidence of variants over six months ranged from 1.8% to 13%, with a median of 2.8%. A total of 414 person-years of follow-up were accrued, during which 19 variants were identified. The event rate for variants, calculated using person-years, was 0.046. Of the 19 variants, two were confirmed as cancer, for a positive predictive value of 11%. Multiparametric MRI-based surveillance was shown to be minimally invasive and enabled detection of pancreatic cancer at a curable stage, suggesting its potential as a standard method for detecting high-risk pancreatic cancer.
Similar content being viewed by others

Introduction
Given the extremely poor prognosis of patients with pancreatic cancer, it is crucial to develop effective surveillance methods for those with high-risk factors. The Fukuoka Guidelines recommend regular screening for intraductal papillary mucinous neoplasms (IPMNs), a risk factor for pancreatic cancer, and that has also been included in the 2024 Kyoto Guidelines1,2. However, no methods for comprehensive risk assessment or surveillance that include other risk factors have been established. We previously reported the effectiveness of the combination of MR diffusion-weighted imaging (DWI) and magnetic resonance cholangiopancreatography (MRCP) for pancreatic tumor diagnosis3. This multiple imaging technique is referred to as multiparametric MRI (mpMRI) and has been gaining attention for use in prostate, breast, and rectal cancer examinations4,5,6. Furthermore, in 2022 the PRECEDE Consortium published a consensus statement regarding standardization of MRI screening and reporting for individuals at high risk for pancreatic cancer, and recommended diagnosis multiple MRI examinations for use in diagnosis7. On the other hand, the positive predictive value of DWI for diagnosing a pancreatic tumor is relatively low at 63%, with false positive results not uncommon3. Currently, the utility of mpMRI for surveillance of high-risk patients with pancreatic cancer is not well defined, particularly regarding its real world evaluation7. The present study aimed to clarify long-term outcomes of patients who underwent pancreatic cancer surveillance using mpMRI with DWI and MRCP.
Materials and methods
Study design
This study was conducted as a multicenter retrospective observational study and received approval from the Medical Research Ethics Committee of Shimane University Faculty of Medicine (Approval No.: KS20230714-1). The Medical Research Ethics Committee of Shimane University Faculty of Medicine explicitly approved the waiver of informed consent due to the retrospective nature of the study and the use of anonymized data, in accordance with institutional guidelines and the Declaration of Helsinki. Instead, an opt-out policy was implemented through a publicly accessible institutional website, allowing participants to decline the use of their data.
Population
Eligibility criteria
We retrospectively screened consecutive asymptomatic individuals who underwent pancreatic MRI at the participating institutions between June 2017 and February 2023 because of suspected pancreatic or biliary abnormalities identified on screening ultrasonography, medical checkup, or incidental imaging. Patients were eligible for the surveillance cohort if they (i) had pancreatic cystic lesions (including branch-duct IPMN or unclassified cystic lesions) and/or pancreatic duct abnormalities, and (ii) had no findings suggestive of malignancy on baseline endoscopic ultrasound and multiparametric MRI including MRCP and DWI/ADC.
Exclusion criteria were: (i) evidence of pancreatic malignancy at baseline evaluation; (ii) absence of pancreatic cystic lesions or pancreatic duct abnormalities; (iii) inability to undergo MRI surveillance or lack of follow-up MRI (follow-up < 6 months); (iv) insufficient image quality for assessing DWI/ADC or MRCP; and (v) carriers of germline pathogenic variants associated with hereditary pancreatic cancer syndromes.
EUS was performed using SU-1 and 580UT (Fujifilm, Tokyo, Japan), or EU-ME2 and GF-UCT 260 (Olympus, Tokyo, Japan) devices.
Sample size consideration
Because this was a retrospective observational study, the sample size was determined by the number of eligible patients during the study period. We primarily aimed to estimate the incidence rate of “variants” during surveillance with adequate precision. With 414 person-years of observation and 19 variant events, the expected 95% confidence interval (CI) for the incidence rate was considered sufficiently narrow for descriptive inference. Secondary analyses, including the positive predictive value of variants for pancreatic cancer, were regarded as exploratory because of the limited number of cancer events.
Protocol
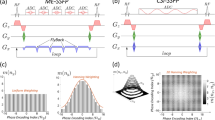
The enrolled patients had pancreatic abnormalities identified during screening or incidental imaging studies, but did not have findings suggestive of malignancy shown by EUS or mpMRI including DWI, an apparent diffusion coefficient [ADC] map, or MRCP. The surveillance protocol included mpMRI and blood testing [amylase, CEA, CA19-9, HbA1c] conducted every six months. After the initial three years, discussion with each patient regarding whether to continue biannual surveillance examinations, extend the interval to once every 12 months, or stop surveillance was conducted, and repeated annually. A variant was defined as appearance of main pancreatic duct stenosis with tail-side dilatation or an area showing high signal intensity in diffusion-weighted images with low signal intensity in an ADC map in mpMRI findings (Table 1). When a variant was detected, contrast-enhanced CT and/or EUS examinations were performed, and/or the surveillance interval was shortened, and when pancreatic cancer was suspected, further examinations and treatment were conducted. For analysis, the primary outcome was incidence of variants within a six-month period and the secondary outcome was positive predictive value for variants. At the time this study was conducted, the Fukuoka Guidelines recommended surveillance methods solely for IPMN1. Nevertheless, surveillance methodologies for cases exhibiting additional pancreatic cancer risks remain to be delineated. Consequently, the necessity for a simplified protocol to extend the scope beyond IPMN to other diseases was identified and the present method was consequently developed. mpMRI was performed using a MAGNETOM ESSENZA 1.5T (Siemens Healthineers, Erlangen, Germany) or MR Ingenia Elition 3.0T (Koninklijke Philips, The Netherlands) device. T2-weighted image acquisitions for MRCP were acquired in the coronal plane and diffusion-weighted imaging was performed with a b value of 800. The surveillance protocol is shown in Fig. 1.

The surveillance protocol for pancreatic cancer consisted of endoscopic ultrasound, multiparametric MRI including MRCP and DWI, and blood (amylase, CEA, CA19-9, HbA1c) examinations at the time of the initial diagnosis. When there were no findings suggestive of malignancy, multiparametric MRI and blood tests alone were performed every six months.
Rationale for no control group
This retrospective study aimed to describe the real world evaluation of an mpMRI-based surveillance strategy implemented in routine care after a malignancy-negative baseline evaluation. A contemporaneous control group (no-surveillance or alternative-modality surveillance) was not available with a standardized protocol across institutions and was not feasible to construct retrospectively. The lack of a control group limits comparative and causal inference regarding the superiority of mpMRI over other modalities. To mitigate this limitation, we used prespecified, objective criteria for “variants,” applied a consistent surveillance interval, and followed a uniform escalation pathway (additional EUS and/or contrast-enhanced CT when variants were detected), reporting event rates based on person-years and downstream diagnostic outcomes.
Results
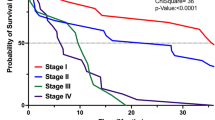
Surveillance using MRI was conducted for 169 patients with an average age of 67 years and females comprising 56.2%. High-risk factors noted were cystic lesions including branch-type IPMN in 164, chronic pancreatitis in 25, and pancreatic duct abnormalities in two (overlapping cases included) (Table 2). The median observation period was 30 months (range 6–78 months) (Fig. 2). A total of 414 person-years of follow-up were calculated using the person-years method, during which 19 variants were identified, for a variant event rate of 0.046, calculated based on person-years with a 95% CI of approximately 0.028–0.072 per person-year. The rate of incidence for variants at each interval was 1.8% at six, 2.4% at 12, 3.0% at 18, 2.6% at 24, 3.8% at 42, and 13% at 60 months, while the median variant incidence rate per interval was 2.8% (Fig. 3a). The three-year event-free survival rate was 89.7% (Fig. 3b) .

Histogram showing number of cases for each interval. The median follow-up period was 30 months (range 6–78 months), with 67% of all patients followed for at least 24 months. M, months.

(a) Bar graph showing numbers of mpMRI cases and variants for each interval, while table below shows ratio of variants for each interval. (b) Kaplan-Meier curve illustrating event-free survival for high-risk individuals enrolled in this study. Cases exhibiting new or progressive MRI findings, defined as "variants”, were considered as events. The three-year event-free survival rate was 89.7%.
A total of 19 cases with variants were noted during the study period, of which two were cancer, resulting in a positive predictive value for variants of 11%. Variants included cyst enlargement in 11, appearance of a restricted diffusion area in six, and dilation of the main pancreatic duct in two. Among those, three patients [two with restricted diffusion areas, one with main pancreatic duct dilation] underwent surgical resection due to suspected pancreatic cancer, with that found in two and an intraductal papillary mucinous adenoma in one. None of those three cases showed positive tumor markers, including CA19-9 (Table 3). As for the 16 patients who continued surveillance without findings indicating malignancy, all remained under surveillance at the time of writing, with no findings indicating malignancy obtained.
Findings for one of the surgical cases are presented in Fig. 4. That patient, a female in her 50s, was diagnosed with branch-type IPMN based on abdominal MRI and EUS findings. Six months later, a high signal area was indicated by diffusion-weighted imaging and further examinations confirmed IPMN-derived invasive cancer, which led to surgery.

A woman in her 50s was diagnosed with branch-type IPMN based on abdominal MRI and EUS findings, and surveillance (left half) was started. Six months later, MRI showed no change in the cystic lesion, though a high signal area was indicated by diffusion-weighted imaging (white arrow). Further examination results confirmed IPMN-derived invasive cancer, leading to surgery.
Discussion
In this multicenter real world cohort, we evaluated a pragmatic surveillance strategy in clinically defined high-risk individuals after a malignancy-negative baseline assessment. Our key contribution is the proposal of a reproducible imaging-based trigger (“variant”), defined by MRCP- and DWI/ADC-derived findings, and a step-up algorithm in which mpMRI is used as the primary surveillance modality and additional EUS and/or contrast-enhanced CT (or short-interval follow-up) is selectively performed only when a newly emerging variant is detected. This framework is intended to balance feasibility for repeated surveillance with diagnostic confirmation for equivocal MRI findings, thereby clarifying both the practical yield and the major limitation—false-positive triggers—of mpMRI surveillance in routine clinical practice.
Risk factors for pancreatic cancer include chronic pancreatitis, obesity, smoking, diabetes, and branch-type IPMN. Canto et al. followed 354 high-risk individuals with genetic factors for a median 5.6 years, of whom 14 (4%) developed pancreatic ductal adenocarcinoma8. In another study, Klein presented findings suggesting that pancreatic cancer screening should not be performed for the general population, but rather should target high-risk individuals, such as those with a family history of pancreatic cancer or an associated genetic syndrome9. Of particular interest, that study noted newly diagnosed diabetic patients over 50 years old as an important group for incidental pancreatic cancer screening. The IPMN guidelines propose different surveillance methods based on the size of a branch-type IPMN without high-risk stigmata or worrisome features1,2. For those smaller than 2 cm, CT or MRI is recommended, while for IPMNs sized 2 cm or larger, alternating EUS and MRI examinations are recommended. However, there is no established protocol for pancreatic cancer screening for patients with conditions other than IPMN, such as chronic pancreatitis10,11,12. A repeated surveillance protocol requires tests that are simple and minimally invasive. Sedation is needed for EUS and contrast-enhanced CT involves radiation exposure, in contrast to the low invasiveness of MRI, which is considered to be an advantage for repeated surveillance.
Established methods for pancreatic cancer screening include EUS, contrast-enhanced CT, and MRI13. In our protocol, mpMRI served as the primary modality for subsequent surveillance after the baseline evaluation. Primarily developed for prostate cancer diagnosis, Kurhanewicz et al. in 2008 reported mpMRI, which combines T2-weighted imaging for anatomical evaluation and diffusion-weighted imaging for functional assessment14. Since our study of the diagnostic potential of DWI for pancreatic tumors3, various other methods with combinations of multiple sequences have also been reported15,16,17. In 2022, the PRECEDE Consortium recommended use of T2-weighted half-Fourier acquisition single-shot turbo spin echo (HASTE), 2D and 3D MRCP, T1-weighted gradient echo (GRE), 3D spoiled gradient-echo (SPGR), and DWI/ADC7. MRCP is known to be excellent for depicting the shape of the pancreatic duct, and allows the examiner to detect stenosis of the main pancreatic duct or branch pancreatic ducts accompanied by dilation of the peripheral pancreatic duct, which are very important indirect signs of pancreatic cancer occurring in the main or nearby branch ducts. Such indirect signs can be depicted even at an early stage, such as pancreatic carcinoma in situ, even though the lesion itself cannot be detected in obtained images. Hanada et al. reported that this type of presentation, showing stenosis of the main and nearby branch ducts, is more common in histologically low papillary type tumors18. Furthermore, MRCP can easily capture changes in pancreatic duct shape and is considered effective for early diagnosis. Conversely, that report presented by Hanada et al.18 noted that flat-type tumors are less likely to spread within the pancreatic duct and tend to be more invasive. For cases in which it is difficult to detect indirect signs with MRCP alone, such as those without tail-side pancreatic duct dilation due to pancreatic duct stenosis, DWI is considered to be effective, as it has been shown to have a sensitivity of 94.4% and specificity of 94.5% for pancreatic cancer3. Also, DWI can reveal tumors even when they do not cause pancreatic duct stenosis, and is known to be effective for viewing cancer in the pancreatic uncinate or tail regions away from the main pancreatic duct, regardless of tumor type. The findings of MRCP and DWI are complementary, and inclusion of both in mpMRI is considered to provide the most suitable imaging results for surveillance of pancreatic cancer.
In our previous report, we noted concerns about false positive findings obtained with DWI3. In the present cohort, six cases were shown positive by DWI, though only one was affected by pancreatic cancer. False positive cases were mainly confirmed by use of contrast-enhanced CT and EUS, which revealed no abnormalities. Interestingly, though details are not included in the present data, the most common causes of false positive DWI findings in cases with no abnormalities actually found were lymph nodes, chronic pancreatitis, and intrapancreatic accessory spleens. For this analysis, cystic lesion T2 shine-through effect was not considered as a false positive result because an ADC map was used for confirmation. While an ADC map is always produced with DWI, any T2 shine-through effect should be evaluated by comparing it with DWI results. Although the positive predictive value of mpMRI surveillance in the present study was low at 11%, the median variant incidence per interval was 2.8%. Variants were further examined using contrast-enhanced CT, EUS, or short-interval re-examinations, resulting in confirmation of no pancreatic cancer in 17 of the 19 cases (89%). The principal disadvantage of mpMRI is possibility of false positive findings, which can be fully resolved by conducting an invasive examination, such as EUS or contrast-enhanced CT, as a subsequent step upon receiving approval. In the present study, there were two cases of operable pancreatic cancer. It is important to note that use of EUS or contrast-enhanced CT at the initial examination does not have a negative impact. However, if the initial EUS or mpMRI findings do not reveal malignancy, mpMRI then becomes the optimal primary surveillance modality, with EUS or contrast-enhanced CT employed as a secondary step only when variant findings are identified by mpMRI. Because of the need for sedation and also radiation exposure associated with EUS or contrast-enhanced CT, utilisation of those as the primary surveillance approach for pancreatic cancer is likely to impose an undue level of invasiveness on the patient.
While the Kyoto guidelines do not specify the surveillance term, the interval for IPMN is 6–18 months, depending on size of the lesion. However, other risk factors for pancreatic cancer, such as chronic pancreatitis, diabetes mellitus, certain genetic abnormalities, and family history of pancreatic cancer, are not included for determining surveillance interval. A previous report recommended cessation of surveillance for patients over 75 years old and with cysts smaller than 30 mm, or those older than 65 with cysts smaller than 15 mm19. The risk of pancreatic cancer in such patients is similar to that in the general population and unnecessary medical intervention should be avoided20. On the other hand, for younger patients or those with increased risk because of a genetic factor, extension of the surveillance period should be considered based on type and number of risk factors2. As for the case presented in Fig. 4, surveillance was started with mpMRI and EUS with no evidence of a tumor noted, then cancer diagnosis was determined six months later. Although no findings indicating pancreatic cancer were detected in the initial surveillance examinations, it is possible that microscopic evidence was present at that time. Given the limitations of EUS and mpMRI for diagnosis, a surveillance interval of six months is preferable. In Japan, cost and insurance coverage limit MRI scans for surveillance purposes to six-month intervals, and none of the cases in the present real world study were found to be in a seriously advanced state. Furthermore, maintaining a supine position for 30–45 min during an mpMRI examination can be difficult or painful, especially for elderly individuals, thus when considering extension of the surveillance interval, transitioning to an alternative method such as CT or ultrasound, or even stopping surveillance should be contemplated along with advanced care planning. Nevertheless, advanced age alone should not be the deciding factor to stop surveillance, as an individualized plan developed in consultation with the patient is a better option.
Conclusion
Surveillance using DWI and MRCP was shown to enable detection of pancreatic cancer at a curable stage. mpMRI does not expose the patient to radiation, is minimally invasive, and can be repeatedly performed. Furthermore, it is useful for evaluations of not only morphological changes in the pancreatic duct, but also lesions present in areas distant from the pancreatic duct, thus indicating its potential as a standard method for surveillance of patients at high risk of pancreatic cancer development.
Data availability
The datasets generated or analyzed for this study are available from the corresponding author upon reasonable request.
References
Tanaka, M. et al. Revisions of international consensus Fukuoka guidelines for the management of IPMN of the pancreas. Pancreatology 17, 738–753 (2017).
Ohtsuka, T. et al. International evidence-based Kyoto guidelines for the management of intraductal papillary mucinous neoplasm of the pancreas. Pancreatology 24, 255–270 (2024).
Fukuba, N. et al. Real-world evidence of Diffusion-weighted imaging combined with magnetic resonance cholangiopancreatography for pancreatic tumor screening: A cross-sectional diagnostic accuracy study. Pancreas 49 (2020).
O’Shea, A. & Harisinghani, M. PI-RADS: multiparametric MRI in prostate cancer. Magn. Reson. Mater. Phys., Biol. Med. 35, 523–532 (2022).
Marino, M. A., Helbich, T., Baltzer, P. & Pinker-Domenig, K. Multiparametric MRI of the breast: A review. J. Magn. Reson. Imaging. 47, 301–315 (2018).
Sun, Y. et al. Multiparametric MRI and radiomics in prostate cancer: a review. Australas Phys. Eng. Sci. Med. 42, 3–25 (2019).
Huang, C. et al. Standardization of MRI screening and reporting in individuals with elevated risk of pancreatic ductal adenocarcinoma: consensus statement of the PRECEDE consortium. AJR Am. J. Roentgenol. 219, 903–914 (2022).
Canto, M. I. et al. Risk of neoplastic progression in individuals at high risk for pancreatic cancer undergoing Long-term surveillance. Gastroenterology 155 740 –51.e2. (2018).
Klein, A. P. Pancreatic cancer epidemiology: Understanding the role of lifestyle and inherited risk factors. Nat. Reviews Gastroenterol. Hepatol. 18, 493–502 (2021).
Konings, I. et al. Evolution of features of chronic pancreatitis during endoscopic ultrasound-based surveillance of individuals at high risk for pancreatic cancer. Endoscopy Int. Open. 06, E541–E8 (2018).
Kim, H. S. et al. Incidence and risk of pancreatic cancer in patients with chronic pancreatitis: defining the optimal subgroup for surveillance. Sci. Rep. 13 (2023).
Greenhalf, W. et al. International consensus guidelines on surveillance for pancreatic cancer in chronic pancreatitis. Recommendations from the working group for the international consensus guidelines for chronic pancreatitis in collaboration with the international association of Pancreatology, the American pancreatic association, the Japan pancreas Society, and European pancreatic club. Pancreatology 20, 910–918 (2020).
Stoffel, E. M., Brand, R. E. & Goggins, M. Pancreatic cancer: changing epidemiology and new approaches to risk Assessment, early Detection, and prevention. Gastroenterology 164, 752–765 (2023).
Kurhanewicz, J., Vigneron, D., Carroll, P. & Coakley, F. Multiparametric magnetic resonance imaging in prostate cancer: present and future. Curr. Opin. Urol. 18, 71–77 (2008).
D’Onofrio, M. et al. Magnetic resonance imaging short protocols for intraductal papillary mucinous neoplasm [IPMN] surveillance: The time has come. Digest. Liver Dis. (2024).
Ansari, G. et al. Utilization of texture features of volumetric ADC maps in differentiating between serous cystadenoma and intraductal papillary neoplasms. Abdom. Radiol. 49, 1175–1184 (2024).
Tanabe, M. et al. Impact on the image quality of modified reduced field-of-view diffusion-weighted magnetic resonance imaging of pancreatic adenocarcinoma using spatially tailored two-dimensional radiofrequency pulses with a Tilted excitation plane: A comparison with conventional field-of-view imaging. Eur. J. Radiol. 168, 111138 (2023).
Hanada, K. et al. Pathological features and imaging findings in pancreatic carcinoma in situ. Pancreas 50, 399–404 (2021).
Han, Y. et al. Optimal surveillance interval of branch duct intraductal papillary mucinous neoplasm of the pancreas. JAMA Surg. 159, 389–396 (2024).
Marchegiani, G. et al. Surveillance for presumed BD-IPMN of the pancreas: Stability, Size, and age identify targets for discontinuation. Gastroenterology 165, 1016–24e5 (2023).
Acknowledgements
The authors wish to thank the radiology technicians at Izumo City General Medical Center and Shimane University Hospital for their excellent work in obtaining high-quality MRI findings.
Author information
Authors and Affiliations
Contributions
Each of the authors contributed significantly to the study, as noted following. Nobuhiko Fukuba was responsible for the study concept and design, as well as data analysis and interpretation; Yoshiko Takahashi, Masaki Onoe, and Yasuhide Kodama contributed to data acquisition; Hiroyuki Fukuhara and Shuichi Sato provided administrative support; Youji Tsuchie provided data analysis and interpretation; Rika Yoshida, Megumi Nakamura, and Yasushi Kaji offered technical support; and Shunji Ishihara supervised the study. All authors have reviewed and approved the final version of manuscript for submission.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Fukuba, N., Takahashi, Y., Onoe, M. et al. Real world evaluation of multiparametric MRI using diffusion weighted imaging and MRCP for pancreatic cancer surveillance. Sci Rep 16, 8856 (2026). https://doi.org/10.1038/s41598-026-38357-2
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-026-38357-2
