
Abstract
The present study is the first quantitative ethnobotanical report on the traditional and new uses of medicinal plants by the inhabitants of a remote and unexplored area in Tehsil Abbaspur, District Poonch, Azad Jammu and Kashmir, Pakistan. The area is disputed territory on the edge of the Line of Control between India and Pakistan and is rich in plant diversity and socio-economic culture. During the field studies, data was collected from 62 informants using structured and semi-structured questionnaires. It was found that women knew more about the therapeutic uses of plants and herbal recipes (average 5.20 known species; 8.39 mentioned uses) than men (average 3.95 known species; 7.31 mentioned uses). A total of 125 medicinal plants from 70 genera and 61 families were documented, with Asteraceae being the most commonly used family in the area. The leaves were the most commonly used plant parts, and the extract was the most common method of preparing herbal recipes. The highest informant consensus factor (0.83) was found for indigestion and liver disorders. Mentha longifolia had the highest use value (0.96) and the highest relative frequency of citations (0.88). High relative importance values (100) were found for Berberis lycium and Mentha longifolia. Four species, namely Fragaria vesca, Berberis lycium, Mentha arvensis and Malus domestica had a fidelity value of 100. The highest similarity in the use of plants was found in studies conducted in related areas of Kotli and Toli Peer districts, indicating similar flora and strong cross-cultural exchange of ethnomedicinal knowledge between the communities. Seven plant species, namely Asplenium dalhousiae (snake bite), Cynoglossum lanceolatum (kidney disease), Sunhangia elegans(hypertension), Glycine max (liver inflammation), Impatiens edgeworthii (urinary tract infection). Plumbago zeylanica (appetite) and Swertia cordata (diabetes) were reported for the first time with new uses. The new claims about the therapeutic use of these species show that medicinal flora research still has much to offer. Mentha longifolia, Mentha. arvensis, Berberis lycium, Fragaria vesca, and Malus domestica received the most citations for their use. These highly cited plant species indicate the presence of valuable phytochemical compounds and are suggested for further pharmacological investigations to introduce new drugs. In the younger generations, botanical customs and resources are rapidly declining due to the pursuit of modernization, cultural homogeneity and overexploitation. Strict conservation measures must be taken immediately to protect traditional knowledge and ensure sustainable utilisation of plant resources. The highly important medicnal plants species including Ajuga bracteosa, Achillea millefolium, Angelica glauca, Myrsine Africana, Elsholtzia ciliate, Melia azedarach and Rhododendron arboretum, Viola odorata and Zanthoxylum armatum become endangered in the area due to overexplotition by local people, therefore need immediate conservation strategies to optimize their sustainable utilization and long term survival.
Similar content being viewed by others
Introduction
Ethnobotanical studies provide critical insight into how communities interact with and utilize their regional plant resources1,2,3,4. By integrating local and scientific knowledge, ethnobotany contributes to the broader goals of biocultural conservation5,6,7,8. These studies are central to identifying culturally and economically important plants, particularly those relevant to the discovery of crude drugs and natural therapeutic compounds9,10,11,12. In addition, ethnobotanical research plays a key role in safeguarding traditional cultural practices and conserving the biodiversity of medicinal plants13,14,15,16.
Quantitative ethnobotany applies statistical and analytical techniques to systematically documented plant-use data17,18. Such quantitative approaches, including hypothesis testing, strengthen the reliability of ethnobotanical information and support informed strategies for the conservation and sustainable use of natural resources7. The use of quantitative indices also improves sampling methods and enhances the quality of ethnobotanical data collection8. This methodological focus contributes to the advancement of ethnobotany as a scientific discipline and promotes its global recognition15,19,20.
Wild plant resources have supported human societies since prehistoric times. Although approximately 391,000 plant species are currently described worldwide, only about 5% are used for therapeutic purposes. It is estimated that 60–80% of the population in developing countries relies on herbal remedies to treat various ailments21,22. This widespread use is often attributed to accessibility, affordability, perceived efficacy, strong cultural traditions, and limited availability of modern healthcare facilities15,22,23,24,25. The use of herbal medicines is also increasing in developed countries such as China, where they account for 30–50% of total drug consumption26,27,28. In several African countries, including Zambia, Ghana, Mali, and Nigeria, herbal preparations are the first choice for approximately 60% of children suffering from malaria, while in Ethiopia nearly 80% of the population depends on herbal medicines for primary healthcare needs29,30.
Some remote areas, characterized by difficult mountainous terrain and religious and cultural constraints, have remained undocumented, making such documentation enormously important. By integrating ethnomedicinal knowledge with quantitative analyses of plant occurrence, this study further explores patterns that may reflect both the cultural significance and ecological availability of key species.
Due to the different climatic conditions, habitats and soil types, Pakistan has a rich plant diversity that is home to 6000 species of higher plants. Of these, 400–600 species are used by the rural communities to cure various diseases31. Previous ethnobotanical studies document the traditional knowledge of medicinal plants from different remote areas of the country32,33,34,35,36,37,38,39. Indigenous knowledge of medicinal plants and traditional recipes is passed down orally from generation to generation. The risk of extinction of traditional knowledge is associated with vertical transmission40,41. This knowledge is therefore highly endangered and urgently needs to be preserved. In recent decades, commercial and scientific interest in herbal medicines has increased across the country as they are economically effective and culturally acceptable42. The rural and remote areas of the country are home to a rich diversity of cultures and languages. However, the inhabitants of these areas have little access to modern healthcare facilities, leading to an overuse of herbal medicines in these cultures43.
Azad Jammu & Kashmir has a rich variety of medicinal plants due to the different habitats and climatic conditions41. Traditional healing practices have been significantly affected by changing lifestyles and access to modern healthcare systems. The indigenous knowledge of medicinal plants is threatened with extinction as this knowledge is mainly preserved by the elderly and hakims and the younger generation has little interest in traditional healing practices44. Traditional health practitioners (THPs) have a wealth of traditional knowledge, but they do not share it with other people41.
Although ethnomedical research has been conducted on a large scale in different areas of Azad Jammu & Kashmir25,39,41,45,46,47,48. However, Abbaspur remained ethnobotanically unexplored due to its remoteness, difficult mountainous terrain and religious and cultural restrictions. The current study was designed with the following objectives: (1) to document the indigenous use of medicinal plants with emphasis on the method of preparation and administration of herbal remedies, (2) to determine the association of plant occurrences with ethnomedicinal data through various quantitative approaches, (3) to compare the data documented in the current study with the published literature from neighboring areas and other parts of the world to identify new ethnomedicinal uses that may merit further pharmacological investigation.
Materials and methods
Study area
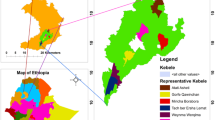
The Tehsil Abbaspur (Fig. 1) is a varied mountainous area in the district of Poonch, Azad Kashmir, Pakistan. It lies in the coordinate range of 33°46′ 34″ N to 33° 55′ 16″ N latitude and 73° 54′ 58″ E to 74° 02′ 50″ N longitude. The elevation is about 3947–9268 feet above sea level. Abasppure has a population of about 62,156 and an area of 136 square kilometres (Census 2017). It is located 167 km from Islamabad and 75 km from Muzaffarabad. There are meadows, forests and plains here. Climatically, the area varies between suptropical and temperate type at different altitudes with the highest rainfall in March (96 mm) and April (80 mm). The weather in summer is pleasant due to the high altitude of the area. June and July are the warmest months with a minimum temperature of 20.9 °C and 21.5 °C and a maximum temperature of 33.8 °C and 31.4 °C. December and January are the coldest months with a minimum temperature of 3.1 °C and 2.5 °C respectively and a maximum temperature of 15.2 °C and 12.3 °C (https://en.climate-data.org). The vegetation is dominated by oaks (Quercus incana), conifers (Pinus roxburghaii and Pinus wallichiana) and various angiosperms including Aesculus indica, Pyrus pashia, Diospyrus lotus, Berberis lycium, Punica granatum, Viburnum grandiflorum and Ziziphus nummularia occurring across different altitudinal ranges. The ground flora mainly consists of Micromeria biflora, Medicago polymorpha, Potentilla indica, Taraxacum officinale, Trifolium repens, Rumex dentatus Geranium wallichianum, Hedera nepalensis, Cynodon dactylon, Onychium japonicum and Dryopteris stewartii. The cultural composition of this region is quite diverse and is mainly inhabited by Khawaja, Gujar, Kayani, Sardar and Syed. The Khawaja, who are spread all over the region, are considered to be influential tribal groups in Abbaspur, Azad Kashmir. The vast majority of the people live in rural areas and are under the strong influence of religion. As a result, gender inequalities persist in the areas of health, education and traditional knowledge. The socio-economic conditions of the people in this area are very diverse and they are not particularly wealthy. The main sources of income are agriculture, farming and some small businesses. Some people work for the government, while others work as day labourers. To improve their socio-economic situation, residents are increasingly breeding pets in their own homes. Modern health facilities are inadequate for the population. There is no hospital nearby, but only a few outpatient clinics offering medical services. Therefore, the inhabitants of the remote and higher areas of Abbaspur rely mainly on medicinal plants and old recipes for the treatment of various diseases.

Map of the study area showing locations of sampling sites (developed by using Arc GIS 10.8; https://www.esri.com/).
Plant sampling and data collection
The field studies were conducted at different times of the year from March 2021 to February 2023. Data were collected through semi-structured interviews with 62 participants (40 men and 22 women). The participants were asked about the medicinal use of the plant species, in particular the preparation methods and the method of administration of the traditional remedies. Participants were selected randomly or partially using the snowball technique49. Ethical approval to conduct the study was obtained from the ethics committee of Women University of Azad Jammu & Kashmir Bagh (Ref. No.: WUAJ&K/IEC/05) before the commencement of the surveys. Legal permission was also obtained from the community committee members to conduct the interviews. Written Prior Informed consent (PIC) was obtained from all informants and/or their legal guardians after they had been informed of the purpose and implications of the study. The ethical guidelines of the International Society for Ethnobiology (http://www.ethnobiology.net/) were strictly followed. The interviews with the participants were conducted in the local language “Pahari”. Participants were always asked to show the specified plants during the interview.
The collection of plant specimens comply with relevant institutional, national, and international guidelines and legislation. The study of the plants and their harvesting in the wild forest areas of Abbaspur for experimental purposes and for the preparation of herbarium specimens was authorised by the responsible head of the forest department (Ref. No.: DFO/278/2020). The medicinal plant species were collected in triplicate during the survey. The specimens were carefully dried, processed and preserved using standard herbarium techniques38,50. The plant specimens were identified by taxonomist (Dr. Muhammad shoaib Amjad) using the Flora of Pakistan (https://www.efloras.org) 51 at the department of Botany, Women University of Azad Jammu and Kashmir (Supplementary Table 1). The family and botanical nomenclature were assigned according to angiosperm phylogeny group III and world flora online (https://www.worldfloraonline.org/) database respectively. The identified species were further confirmed in the Herbarium of Aromatic and Poisonous Plants of Pakistan Agriculture and Research Council (PARC). The voucher specimens were deposited in the herbarium of the Botany Department of the Women University of Azad Jammu and Kashmir Bagh.
Data analysis
The primary data collected during the survey was analyzed quantitatively by using the indices listed below to determine the homogeneity and validity of the data.
Informant consensus factor (ICF)
The informant consensus factor (ICF) was applied to check the agreement between the participants and the plant used for a specific disease group. The ICF was determined using the following formula according to Trotter and Logan52 & Vitalini et al.53.
where Nur stands for usage reports for a specific disease group, and Nt for the total species used for this disease group. The value is between 0–1. A high value (close to 1) means that the plant species are selected according to certain criteria and that there is a lively exchange of information between the participants. A low value (close to 0) means that the plants are selected at random and there is no exchange of information between the participants.
Relative frequency of citation (RFC)
It shows the native importance of the plant species and was determined according to the following formula by Vitalini et al.53 & Jabeen et al.41,
where “FC” is the number of particioants who indicated specific uses of a plant species and N are the total participants.
Use value (UV)
It is a the quantitative measure of the relative importance of locally known plant species and was calculated according to the formula of Savikin et al.54 & Jabeen et al.41:
where Ui is the total number of uses mentioned by each participant for a given species and N are is the total number of participants.
Relative importance (RI)
It was calculated according to the formula of Ali et al.55 & Jabeen et al.41 :
where “PH” is the pharmacological attribute of the selected plant and “Rel PH” are the relative pharmacological attributes associated with that plant.
where “BS” is the total number of body systems cured by the selected species and “Rel BS” is the relative number of body systems healed by that species
Fidelity level (FL)
Shows the preferred species for the treatment of a particular disease. It was calculated using the following formula according to Alexiades and Sheldon56 & Jabeen et al.41:
where “Np” is the number of participant who indicates the use of plants for the treatment of a particular disease and “N” is the total number of participants who indicated plant species for a disease.
Jaccard index (JI)
It was determined by comparing the documented data with previously published research from neighbouring areas on a regional and global scale to determine the novelty of the work. It was determined using the formula given in Gonza et al.57 & Jabeen et al.41,
where “a” are the species of the study area, “b” are the species of the neighbouring area and "c" are the common plant species in both areas.
Conservation status
The conservation status of medicinal plants in the study area was evaluated using the IUCN Red List Criteria (version 3.1). Systematic transect walks were conducted across the region during multiple seasons to capture temporal variation in species occurrence. Information on species distribution, abundance, and availability was obtained through interviews with knowledgeable local respondents, primarily plant collectors, and subsequently validated through direct field observations.
During field assessments, a suite of ecological and anthropogenic parameters was recorded, including area of occupancy, occurrence status (rare, moderate, or abundant), extent of range, trends in plant availability (stable, declining, or increasing), evidence of conservation measures, habitat modification, plant parts harvested, collection practices, and major threat factors (e.g., overharvesting, deforestation, overgrazing, fire, and pollution). Based on the combined qualitative and quantitative evidence, each medicinal plant species was assigned to the appropriate IUCN threat category.
Results
Ethnographic composition
A total of 62 participants, including 40 men and 22 women, were interviewed according to gender, age and occupation (Table 1). The ethnomedical information was mainly collected from the men, as women are very poorly represented in the region due to the prevalence of gender discrimination, the concept of honor and shame, hospitality, and veiling. However, women in the region knew more about the ethnomedicinal uses of plants (mean known species = 5.2; mean reported use = 8.19) than men (mean known species = 3.95; mean reported use = 7.31). Participants were divided into three groups according to age: under 40, between 40 and 60, and over 60. The elderly (over 60 years) had considerable knowledge of medicinal plants (mean known species = 12.75; mean reported use = 10.90), followed by middle-aged people (mean known species = 8.98; mean reported use = 5.35) and young people (mean known species = 3.80; mean reported use = 3.12).
Among the different occupational groups, traditional healers (Hakeems) showed high competence in the medicinal use of plant species (mean known species = 25.42; mean reported use = 14.80), followed by midwives (mean known species = 14.60; mean reported use = 8.01). There is a great need for traditional healers and midwives in the local health system. They still play an important role in the local health system today. Their functions change according to time and culture. Most of the doctors were men who had extensive knowledge of herbal medicines, which they prepared for the treatment of various diseases using natural methods based on medicinal plants. Midwives also recognize the problems that women have during pregnancy and treat them with various herbal remedies.
Diversity of ethnomedicinal flora
A total of 125 plant species from 61 families and 77 genera were documented in the study area. The detailed ethnomedicinal information is given in Table 2, which includes the scientific name, local name, family, habit, part used, method of preparation and mode of administration of the herbal prescriptions, disease cured and previous use reports. Asteraceae was the most commonly used family (19 species) in the study area, followed by Lamiaceae (10 species) and Rosaceae (9 species) (Fig. 2). Most of the species used were herbaceous (72%), followed by shrubs (29%), trees (20%) and climbers (4%) (Fig. 3).

Family contribution of ethnomedicinal flora.

Life form contribution of ethnomedicinal flora.
Plant parts used, method of preparation and utilization of herbal remedies
In the current study, leaves were the most commonly used plant parts (39%), followed by the whole plant (27%) and the root (23%) (Fig. 4). Local people use different methods for preparing herbs. The most common method of preparaing herbal remedies was as extracts (40%), followed by powders (21%), decoctionS (17%), juices (17%), pastes (14%), infusions (12%), herbal teas (6%), oral consumption (5%), topical (external) application (5%), poultices (4%), chewed (3%), oils (3%), vegetables (3%) and latex (2%) (Fig. 5). Of all recorded prescriptions, 65% were administered internally, whereas 35% were applied externally.

Plant parts used in herbal recipes.

Methods of preparing herbal remedies.
Informant consensus factor (ICF)
The ICF score ranges from 0.51 to 0.83. The ICF score in our study is high, suggesting that participants tend to agree on a few plant species used to cure specific ailments (Heinrich et al., 2006). The highest ICF value (0.83) was calculated for diseases of the digestive system and liver. This was followed by digestive disorders (0.83) (Fig. 6; Supplementary Table 2). This could be due to the unavailability of clean drinking water and hygienic food. The most commonly used plants for this category are Allium sativum, Verbena officinalis, Swertia cordata, Mentha longifolia, Euphorbia prostrata, Ajuga bracteosa, Berberis lycium, Zanthoxylum armatum, Salix nigra, Pyrus pashia, Prunus persica, Mentha arvensis, and Viola odorata.

Different disease treated by the plants. MJD Muscular and joint diseases, CSD Circulatory system diseases, SD Skin diseases, MTD Mouth Throat Diseases, D Diabetes, EED Eye and Ear diseases, RST Respiratory system diseases, DSLD Digestive system and Liver Diseases, URSD Urinary and Reproductive system diseases, F Fever, C Cancer, HP Hair Problems, BLSD Blood and lymphatic system diseases, A Antidote, NSD Nervous system diseases, O Others.
Relative frequency of citation and use value
The value of RFC ranged from 0.1 to 0.89. The highest relative frequency of citation was calculated for Mentha longifolia (0.89). Other plant species with a high RFC are Berberis lycium (0.85), Mentha arvensis (0.82), Malus domestica(0.79), Prunus persica (0.77) and Zanthoxylum armatum (0.62) (Table 3). Use value ranges from 0.03 to 0.96. The highest UV was documented for Mentha longifolia (0.96). It was followed by Berberis lycium (0.95), Malus domestica (0.88), Prunus persica (0.87), Allium cepa (0.83), Amaranthus viridis (0.83), Ficus palmata (0.74) and Zanthoxylum armatum (0.72) (Table 3).
Relative importance (RI) and fidelity level (FL)
Relative importance values range from 15 to100. In the study area, high relative importance values (100) were recorded for Berberis lycium and Mentha longifolia. Other species with high relative importance is Zanthoxylum armatum (91.5) (Table 3).
In the current study, FL of 50 plant species was reported. The FL value ranges from 18.7 to 100%. Highest FL (100%) was recorded for four plants used to cure some major ailments. These plants were Berberis lycium (hepatitis), Fragaria vesca (kidney diseases) and Malus domestica (body weaknesses) (Fig. 7; Supplementary Table 3). Other species with high fidelity value are Mentha arvensis (stomach pain), Pyrus pashia (liver tonic), Melia azedarach (jaundice), Glycine max (stimulate the apetite), Sarcococca saligna (blood purification), Ficus carica (diabetes), Rumex dentatus (body pain), Morus alba (body weaknesses), Allium sativum (joint pain).

Top ranked plant species with above 80% fidelity.
Jaccard index (JI)
The ethnomedical data collected in the present study were compared with 22 previously published papers from neighbouring areas of Pakistan and from other countries to verify the global perspective. The data showed that the percentage similarity of applications ranged from 0.07 to 34.4% and the percentage dissimilarity of applications ranged from 7.6 to 38.8%. The JI value ranged from 2.87 to 41.02. The highest degree of similarity was found in studies conducted in related areas of Kotli and Toli Peer districts with similarity value of 34.4% and 32.2%, respectively (Table 4). A low similarity value was found in the studies conducted in Hingol National Park with a similarity value of 0.07%.
Novelty assessment
The main objective of the present study was to compare the results of the data with previously published studies from neighboring areas and to highlight some new uses not previously reported from this region (Table 5). The comparative assessment of the data identified seven plant species with specific uses reported for the first time. An extract from the leaves of Asplenium dalhousiae was reported for the treatment of snakebite. Powder from the leaves of Cynoglossum lanceolatum was used for the treatment of kidney diseases. Herbal tea from the root of Sunhangia eleganshas been used to treat hypertension. The fruit extract of Glycine max was used to treat liver inflammation. The extract from the whole plant of Impatiens edgeworthii was used to treat urinary tract infections. The root extract of Plumbago zeylanica is said to stimulate the appetite and the extract from the aerial parts of Swertia cordata is used to treat diabetes.
Conservation status
The conservation status of medicinal plants was assesed using the IUCN criteria. Among the recorded species, 36.8% species were considered Least concern, 27.2% rare, 24.8% vulnerable, 8% endangered, and 3.2% near threatened in the study area (Fig. 8, Table 6).

Conservation status of medicinal plants of Abbaspur, AJ&K.
Discussion
Ethnobotanical information was obtained from 62 informants, including 40 men and 22 women. The interviews revealed that the older female informants from the region knew significantly more about the ethnomedicinal use of plants than the male and young respondents. This is due to the fact that housewives and older people have more experience in the use of medicinal herbs and are still closely associated with the traditional way of life. On the other hand, younger people are distancing themselves from traditional herbal practice due to changing lifestyles and modernization. These findings are in strong agreement with other studies from Azad Kashmir14,25,39,41,46,48 and Pakistan12,32,33.
Illiterate informants had a greater understanding of ethnomedical knowledge than educated informants. This is due to the fact that educated people tend to use allopathic medicine and show little interest in using traditional herbal remedies. Moreover, uneducated people come in direct contact with medicinal plants and are familiar with the usage patterns of plants. Knowledge of medicinal plants decreases with increasing levels of education as they have more access to modern education41,48,58,59. These findings are strongly supported by many other studies in Pakistan8,18,33,36,47,58,60 and abroad61,62,63.
The study area has a diverse vegetation, with 61 plant families representing a field collection of 125 plants and 77 genera. This shows that the area has a great diversity of medicinal plants used for therapeutic purposes, as well as a rich traditional knowledge. One reason for the great plant diversity is the fact that the study area is close to the Line of Control (LOC) between Pakistan and India. Plant collectors and nomads, who pose a serious threat to local biodiversity through the overexploitation of medicinal plants, are less present here. Previous reports have also reported the high plant diversity in the neighboring areas with similar climatic conditions32,41,46,48,64. The area has a subtropical to alpine climate where altitude, mean annual temperature and mean annual precipitation are the driving factors that determine the local plant richness in this area. The large number of Asteraceae and Lamiaceae in the area indicates that these families are abundant and easily accessible in the area and have cultural significance to the local people. Moreover, the members of these families are enriched with a large number of metabolites responsible for their bioactivity, organoleptic and pharmacological properties14,38,58,65,66. The same results are found in other studies from Pakistan and around the world14,36,44,48,58. The dominance of herbaceous life forms in the area indicates that the local climatic conditions are favorable for the growth of small plants. Along the altitudinal gradient, climatic conditions become less favorable for the growth of large plants and soil properties, such as soil binding capacity, do not favor the growth of woody species in high alpine areas. In addition, the high moisture content in mountain areas leads to the dominance of herbaceous species, which is a common ecological phenomenon worldwide. Moreover, herbaceous species are easily used for the preparation of herbs. These results are consistent with other studies31,36,38,41,48,67.
In ethnobotanical research, the socioeconomic conditions and demographic characteristics of informants play an important role in the assessment and interpretation of ethnomedicinal data collected from respondents46,48,68,69. The remoteness of the area, the poor road infrastructure and the poor health system in Abbaspur have limited the influx of people from different cultural backgrounds, so a preserving effect on conventional knowledge can be observed due to this lack of communication. The women of the region had a greater knowledge of the ethnomedicinal use of plants than the men. This could be due to the fact that women are generally involved in household management, which is highly associated with the preparation and administration of herbal remedies to keep the family healthy. Some other studies reported similar findings from Chail valley70, Abbottabad12, Neelum valley58, Mohmand Agency23 and Dhirkot14, Sudhanoti71 district, Poonch District48.
In the present study, leaves were identified as the most commonly used plant parts for therapeutic purposes. Our study is largely in agreement with other reports conducted in related areas14,41,58. Leaves are abundant and readily available in nature. Moreover, leaves contain a large amount of easily extractable bioactive constituents which are very effective in phytotherapy. The root is the second most commonly used plant in herbal preparations as it also contains a large amount of pharmacologically active constituents compared to other parts. The frequent use of whole plants reflects the high use of herbs in the manufacture of preparations. These findings were supported by previous studies38,41,54,58. The use of roots and whole plants could impair the regeneration potential of species and lead to species extinction14,48,72,73.
Here, we found that the preparation of herbal remedies in the form of extracts and powders is the most common form. The reason for this could be the ease of preparation by mixing certain plant parts with honey, soup, milk, tea, butter and water12,38,41. Another reason could be the amount of metabolically active components, which is increased by heating as it accelerates the biological reactions38,48,74,75. In addition to the extract, the dried powder is also preferred in high altitude areas in winter, possibly due to the cold and dry season14,41,70,76. Depending on the disease to be treated and its condition, locals use both the extract and the powder.
Herbal preparations were applied externally to the affected areas in the form of pastes, embrocations, poultices, oils and washes. Our results are confirmed by previous studies12,14,41,77. The dosage of herbal medicine varies depending on the severity of the disease, the appearance and the age of the patient. For example, the fruit of Ficus carica is used to cure constipation in the region, but 2 to 3 fruits are effective in children, while 4 to 5 fruits are used in adults.
The indigenous people of the region used plants to treat various diseases, which were classified into 16 groups based on the international categorization of diseases78, with some modifications made to reach a consensus between the informants and the medicinal plants used to cure specific groups of diseases. The ICF score ranges from 0.51 to 0.83. The ICF score in our study is high, indicating that participants generally agree on a few plant species used to cure specific diseases27. The highest ICF value (0.83) was calculated for diseases of the digestive system and liver. The devastating earthquake of 2005 made the situation even worse, as many water supply systems were destroyed and drinking water is contaminated. The most commonly used plants for this category are Allium sativum, Verbena officinalis, Swertia cordata, Mentha longifolia, Euphorbia prostrate, Ajuga bracteosa, Berberis lyceum, Zanthoxylum armatum, Salix nigra, Pyrus pashia, Prunus persica, Mentha arvensis, Viola odorata. These plants are well known among the locals and contain many active compounds that are effective in curing various diseases14,58,79. Many other studies have also found the highest ICF for digestive problems41,60,77,80. For several decades, ethnobotanical expeditions around the world have reported extensively on the use of medicinal herbs for gastrointestinal complaints81,82,83. In mountainous regions, where poor sanitation is more common, gastrointestinal complaints are reported more frequently41,84,85. Short-term dyspepsia or bloating to long-term structural abnormalities and chronic diseases are common and have a significant impact on mortality and morbidity85.
The relative frequency of mentions reflects the local importance of plant species with relevance for the participant who indicated the use of these plant species53. The maximum relative frequency of mentions and the maximum use value were calculated for Mentha longifolia, M. arvensis and Berberis lyceum. These plant species are generally known and are predominantly used by the local population. The maximum relative frequency of mentions could be due to the easy availability, wide distribution and traditional practices for curing various diseases with these plants. These species should be subjected to further phytochemical and pharmacological studies to validate this information. Conservation strategies should also be implemented immediately to preserve these species. Use value is a quantitative measure of the relative importance of a species as reported by natives and ranges from 0.03 to 0.96. The highest UV value was found for Mentha longifolia, Berberis lycium and Malus domestica. The species with the most usage reports have a high use value and vice versa. The species with a high use value are well known by local people. There is a greater likelihood that the high UV plant species found in the study area are entrenched in the local culture as the locals are most likely familiar with them and have frequently used them in home treatments58. These species are used repeatedly and are pharmacologically active12. Moreover, although the plant species with lower use value are not biologically inactive, they are no longer properly recognized by the local informants39. The constant use of a plant for the same purpose indicates that it has active components that support its use and may provide a clue for future pharmacological research46,48. Similarly, plants with low use value are not less important per se, but their low value may indicate that informants know less about how they can be used to treat common diseases. Another argument is that geographical barriers have eroded cultural knowledge86.
Relative importance reflects the diversity of specific species used to treat different diseases. In the study area, high relative importance values were found for Berberis lyceum, Mentha longifolia and Zanthoxylum armatum. The species with the highest RI values show that they are the most commonly used plants for curing various diseases25. The inhabitants of the area are well familiar with these plants and have significant ethnic medicinal knowledge about these plants. Similar findings have also been reported by other studies14,41,77. The level of fidelity is used to identify the preferred species mentioned by the locals for curing certain ailments. The high FL values of Berberis lyceum (hepatitis), Fragaria vesca (kidney diseases) and Malus domestica (body weakness) show that these plants are extensively used in the area to cure various ailments compared to those with lower FL values41,60. These plants are used either alone or in combination with other plants. The plants with high FL value are considered as model plants and these plants should be subjected to further ethnopharmacological studies to confirm the claims made by humans41,87. Cichorium intybus with low FL has been used to treat gallstones. Low FL plants are not biologically inactive, but they are not well recognized by the inhabitants of the region12,38.
The highest degree of similarity in Jaccard index was found in studies conducted in related areas of Kotli district88 and Toli Peer25, with a similarity value of 34.4% and 32.2%, respectively. The differences and similarities in ethnomedicinal studies emphasise the importance of traditional knowledge in different areas where historical89, ecological90, organoleptic and phytochemical factors91 play a role in selection. The short distance between the study area and the adjacent area may contribute to the high similarity. Other factors include similar flora and maximum exchange of cross-cultural ethnomedical knowledge. In studies conducted in Hingol National Park, a low similarity score was found92. These differences suggest that there are some ecological barriers between the two areas leading to geographical separation of species and changes in habitat and vegetation. In addition to cultural differences due to minimal cross-cultural exchange, these areas are separated by the mountain range, and the location of the study area near the LoC may also contribute to a low similarity score. The plants with new medicinal applications could be subjected to further pharmacological and phytochemical studies to develop new drugs41,46,48,58.
The conservation of medicinal plants is essential for maintaining biodiversity and ensuring their sustainable use. During the study, it was observed that local communities collect medicinal plants in large quantities for commercial purposes from remote areas of Abbaspur, leading to rapid depletion of these resources. In addition to overexploitation, other anthropogenic and ecological factors threatening the medicinal flora in the area include deforestation, overgrazing and browsing, lack of awareness, forest fires, military installations, and timber smuggling. Several plant species with high medicinal value such as Ajuga bracteosa, Achillea millefolium, Angelica glauca, Myrsine africana, Elsholtzia ciliata, Melia azedarach, Rhododendron arboreum, Viola odorata, and Zanthoxylum armatum have become endangered in the area, highlighting the urgent need for conservation strategies to prevent their local extinction. Among these, Ajuga bracteosa and Zanthoxylum armatum are not only threatened locally but also across the broader region. Similar patterns of overexploitation of medicinal plants have been reported in other areas of Pakistan and Azad Kashmir93 including Nikyal valley94, Daral valley95, Neelum valley96,97, Poonch valley98.
Conclusion
This is the first quantitative ethnobotanical report on the plant diversity of medicinal plants in unexplored Abbaspur (AJK), Pakistan. A total of 125 medicinal plants were used in ethnomedicinal applications. This shows the crucial role of medicinal plants in primary health care of the local communities where modern health facilities are not available due to the remoteness and difficult mountainous terrain of the region. The study reports a high prevalence of digestive disorders in the local population, indicating poor sanitation in the region, and further suggests the use of plant formulations as modulators of the brain-gut microbiota axis to understand the effects of gut microbiota on the human brain and behaviour. In addition, several plant species were found to have novel uses not reported elsewhere, namely Asplenium dalhousiae (leaf extract, snake bite), Cynoglossum lanceolatum (leaf powder, kidney disease), Desmodium elegans (herbal tea, hypertension), Glycine max (fruit extract, liver inflammation), Impatiens edgeworthii (whole plant extract, urinary tract infection). Plumbago zeylanica (root extract, appetite) and Swertia cordata (extract from the above-ground leaves, diabetes). New claims about the therapeutic use of these species make it clear that research into medicinal plant flora still has much to learn. Mentha longifolia, M. arvensis Berberis lycium, Fragaria vesca, and Malus domestica received the most citations. These highly cited plant species with high use value indicate the presence of valuable phytochemical compounds and are suggested for further pharmacological investigations to introduce new drugs. Some of important medicnal plants species become endangered in the area due to overexplotition by local communities and therefore require immediate conservation measures to prevent their extinction. Finally, this study has raised the concern that despite the importance of plants, botanical traditions are declining worldwide at community and individual levels, especially among younger generations due to the desire for modernization, cultural homogeneity and the loss of botanical resources through deforestation, overgrazing and overexploitation.
Data availability
All data are included in the manuscript.
References
Pirintsos, S. et al. From traditional ethnopharmacology to modern natural drug discovery: A methodology discussion and specific examples. Molecules 27, 4060 (2022).
Hani, N., Baydoun, S., Nasser, H., Ulian, T. & Arnold-Apostolides, N. Ethnobotanical survey of medicinal wild plants in the Shouf Biosphere Reserve, Lebanon. J. Ethnobiol. Ethnomed. 18, 73 (2022).
Palchetti, M. V. et al. Large-scale patterns of useful native plants based on a systematic review of ethnobotanical studies in Argentina. Persp. Ecol. Conserv. 21, 93–100 (2023).
Pieroni, A., Nebel, S., Santoro, R. F. & Heinrich, M. Food for two seasons: Culinary uses of non-cultivated local vegetables and mushrooms in a south Italian village. Int. J. Food Sci. Nutr. 56, 245–272 (2005).
Gaoue, O. G. et al. Theories and major hypotheses in ethnobotany. Econ. Bot. 71, 269–287 (2017).
Iqbal, M. S. et al. An ethnobotanical study of wetland flora of Head Maralla Punjab Pakistan. PLoS ONE 16, e0258167 (2021).
Awoke, A., Siyum, Y., Awoke, D., Gebremedhin, H. & Tadesse, A. Ethnobotanical study of medicinal plants and their threats in Yeki district, Southwestern Ethiopia. J. Ethnobiol. Ethnomed. 20, 107 (2024).
Ralte, L., Sailo, H. & Singh, Y. T. Ethnobotanical study of medicinal plants used by the indigenous community of the western region of Mizoram, India. J. Ethnobiol. Ethnomed. 20, 2 (2024).
Leonti, M., Casu, L., Sanna, F. & Bonsignore, L. A comparison of medicinal plant use in Sardinia and Sicily—De Materia Medica revisited?. J. Ethnopharmacol. 121, 255–267 (2009).
Cox, P. A. Will tribal knowledge survive the millennium?. Science 287, 44–45 (2000).
Emade Nkwelle, C. et al. Croton oligandrus pierre & hutch (Euphorbiaceae) extracts and isolated compounds reverse HIV-1 latency. J. Exp. Pharmacol. 413–425 (2024).
Kayani, S. et al. Ethnobotanical uses of medicinal plants for respiratory disorders among the inhabitants of Gallies-Abbottabad, Northern Pakistan. J. Ethnopharmacol. 156, 47–60 (2014).
Leonti, M. The future is written: Impact of scripts on the cognition, selection, knowledge and transmission of medicinal plant use and its implications for ethnobotany and ethnopharmacology. J. Ethnopharmacol. 134, 542–555 (2011).
Farooq, A. et al. Ethnomedicinal knowledge of the rural communities of Dhirkot, Azad Jammu and Kashmir, Pakistan. J. Ethnobiol. Ethnomed. 15, 45 (2019).
Cordero, C. S., Meve, U. & Alejandro, G. J. D. Ethnobotany and diversity of medicinal plants used among rural communities in Mina, Iloilo, Philippines: A quantitative study. J. Asia-Pacific Biodivers. 16, 96–117 (2023).
Yahaya, T. O. et al. Toxicological evaluation of phytochemicals and heavy metals in Ficus exasperata Vahl (Sandpaper) leaves obtained in Birnin Kebbi, Nigeria. arXiv preprint arXiv:2501.11037 (2025).
Majeed, M. et al. Ethno-veterinary uses of Poaceae in Punjab, Pakistan. PLoS ONE 15, e0241705 (2020).
Sharma, A., Adhikari, D. & Wagh, V. V. An ethnobotanical investigation of medicinal plants used among rural communities in Northeastern Madhya Pradesh, India: A quantitative study. Plant Biosyst.-An Int. J. Dealing Aspects Plant Biol. 158, 1160–1181 (2024).
Phillips, O. & Gentry, A. H. The useful plants of Tambopata, Peru: I: Statistical hypotheses tests with a new quantitative technique. Econ. Bot. 47, 15–32 (1993).
Shaheen, S. et al. Knowledge of medicinal plants for children diseases in the environs of district Bannu, Khyber Pakhtoonkhwa (KPK). Front. Pharmacol. 8, 430 (2017).
Shinwari, Z. K. Medicinal plants research in Pakistan. J. Med. Plants Res 4, 161–176 (2010).
Organization, W. H. Traditional and complementary medicine in primary health care. (2018).
Aziz, M. A. et al. Traditional uses of medicinal plants practiced by the indigenous communities at Mohmand Agency, FATA, Pakistan. J. Ethnobiol. Ethnomed. 14, 2 (2018).
Organization, W. H. WHO global report on traditional and complementary medicine 2019. (World Health Organization, 2019).
Amjad, M. S. et al. Descriptive study of plant resources in the context of the ethnomedicinal relevance of indigenous flora: A case study from Toli Peer National Park, Azad Jammu and Kashmir, Pakistan. PLoS ONE 12, e0171896 (2017).
Heinrich, M., Chan, J., Wanke, S., Neinhuis, C. & Simmonds, M. S. Local uses of Aristolochia species and content of nephrotoxic aristolochic acid 1 and 2—A global assessment based on bibliographic sources. J. Ethnopharmacol. 125, 108–144 (2009).
Heinrich, M., Kufer, J., Leonti, M. & Pardo-de-Santayana, M. Ethnobotany and ethnopharmacology—Interdisciplinary links with the historical sciences. J. Ethnopharmacol. 107, 157–160 (2006).
Wang, W.-Y., Zhou, H., Wang, Y.-F., Sang, B.-S. & Liu, L. Current policies and measures on the development of traditional Chinese medicine in China. Pharmacol. Res. 163, 105187 (2021).
Wubetu, M., Abula, T. & Dejenu, G. Ethnopharmacologic survey of medicinal plants used to treat human diseases by traditional medical practitioners in Dega Damot district, Amhara, Northwestern Ethiopia. BMC Res. Not. 10, 157 (2017).
Kassaye, K. D., Amberbir, A., Getachew, B. & Mussema, Y. A historical overview of traditional medicine practices and policy in Ethiopia. Ethiopian J. Health Dev. 20, 127–134 (2006).
Ali, S., Munazir, M., Sher, H., Qureshi, R. & Akram, M. An ethnobotanical study of aromatic medicinal plants of Swat Valley, Pakistan. Asian J. Ethnobiol. 6 (2023).
Ullah, I. et al. Ethnobotanical knowledge and ethnomedicinal uses of plant resources by urban communities of Khyber Pakhtunkhwa, Pakistan: A novel urban ethnobotanical approach. J. Ethnobiol. Ethnomed. 21, 13 (2025).
Ullah, H. & Badshah, L. The ethnobotanical heritage of Lotkuh, a high-altitude tribal haven of Chitral, the Eastern Hindu Kush, Pakistan. J. Ethnobiol. Ethnomed. 20, 54 (2024).
Elahi, R. et al. Ethno-medicinal knowledge and geo-referenced profiling of medicinal plants in Amazi Valley, Buner, Pakistan. Genetic Resources and Crop Evolution, 1–33 (2025).
Hussain, S. T., Muhammad, S., Khan, S., Hussain, W. & Pieroni, A. Ethnobotany for food security and ecological transition: Wild food plant gathering and consumption among four cultural groups in Kurram District, NW Pakistan. J. Ethnobiol. Ethnomed. 19, 35 (2023).
Bibi, F., Abbas, Z., Harun, N., Perveen, B. & Bussmann, R. W. Indigenous knowledge and quantitative ethnobotany of the Tanawal area, Lesser Western Himalayas, Pakistan. PLoS ONE 17, e0263604 (2022).
Majeed, S. et al. Opuntia spp.: Chemistry, Bioactivity and Industrial Applications 49–80 (Springer, 2021).
Amjad, M. S. et al. Ethnobotanical survey of the medicinal flora of Harighal, Azad Jammu & Kashmir, Pakistan. J. Ethnobiol. Ethnomed. 16, 65 (2020).
Qaseem, M. et al. Ethno-botanical evaluation of indigenous flora from the communities of rajh mehal and goi union councils of district Kotli, Azad Jammu Kashmir Pakistan. Appl. Ecol. Environ. Res. 17, 2799–2829 (2019).
Tahir Hameed, I. A., Ullah, S. & Hussain, W. Ethnobotanical study and conservation status of medicinal plants used by traditional healers in Toormang Valley, Northern Pakistan.
Jabeen, T. et al. Ethnomedicinal plants and herbal preparations used by rural communities in tehsil hajira (poonch district of azad kashmir, Pakistan). Plants 13, 1379 (2024).
Razzaq, A., Ameen, H. & Aziz, R. An ethnobotanical servey of Pakistani medicinal plants and their future in pharmaceuticals development. Adv. Herb. Res. 7, 1–12 (2024).
Siddique, Z. et al. Exploration of ethnomedicinal plants and their practices in human and livestock healthcare in Haripur District, Khyber Pakhtunkhwa, Pakistan. J. Ethnobiol. Ethnomed. 17, 55 (2021).
Din, S. U. et al. Exploring conservation status and ethnoveterinary uses of medicinal plants in Upper-Haramosh, Gilgit-Baltistan, Pakistan. Ethnobot. Res. Appl. 29, 1–14 (2024).
Maqsood, T. et al. Study of plant resources with ethnomedicinal relevance from district Bagh, Azad Jammu and Kashmir, Pakistan. Open Chem. 20, 146–162 (2022).
Habib, T. et al. Quantitative ethnobotanical investigation in northern district of lesser himalayas of azad jammu and kashmir, pakistan. J. Ecol. Environ. 48 (2024).
Liaqat, I. et al. An ethnobotanical survey of medicinal plants used for primary health care from Patan Sher Khan and surrounding areas of district Sudhnoti, Azad Jammu and Kashmir, Pakistan. J. Appl. Res. Plant Sci. 4, 518–528 (2023).
Mustafa, A. et al. Exploring the diversity and ethnomedicinal uses of wild edible plants in District Poonch, Azad Jammu and Kashmir. Genet. Resources Crop Evol. 1–25 (2025).
Aziz, M. A. et al. On the trail of an ancient Middle Eastern ethnobotany: Traditional wild food plants gathered by Ormuri speakers in Kaniguram, NW Pakistan. Biology 10, 302 (2021).
Jain, S. K. & Rao, R. R. A handbook of field and herbarium methods. (1977).
Nasir, E. & Ali, S. Flora of west Pakistan. (1972).
Trotter, R. T., Logan, M. H. & Etkin, N. L. Plants in indigenous medicine and diet. New York: Redgrave, 91–112 (1986).
Vitalini, S. et al. Traditional knowledge on medicinal and food plants used in Val San Giacomo (Sondrio, Italy)—An alpine ethnobotanical study. J. Ethnopharmacol. 145, 517–529 (2013).
Šavikin, K. et al. Ethnobotanical study on traditional use of medicinal plants in South-Western Serbia, Zlatibor district. J. Ethnopharmacol. 146, 803–810 (2013).
Ali, K. et al. The ethnobotanical domain of the Swat Valley, Pakistan. J. Ethnobiol. Ethnomed. 14, 39 (2018).
Alexiades, M. N. & Sheldon, J. W. Selected guidelines for ethnobotanical research: a field manual. (1996).
González-Tejero, M. R. et al. Medicinal plants in the Mediterranean area: Synthesis of the results of the project Rubia. J. Ethnopharmacol. 116, 341–357 (2008).
Ahmad, K. S. et al. Ethnopharmacological studies of indigenous plants in Kel village, Neelum valley, Azad Kashmir, Pakistan. J. Ethnobiol. Ethnomed. 13, 68 (2017).
Saynes-Vásquez, A., Vergara-Silva, F. & Caballero, J. Ethnobotany of Mexico: Interactions of People and Plants in Mesoamerica 457–473 (Springer, 2016).
Bibi, T. et al. Ethnobotany of medicinal plants in district Mastung of Balochistan province-Pakistan. J. Ethnopharmacol. 157, 79–89 (2014).
Giday, M., Asfaw, Z., Elmqvist, T. & Woldu, Z. An ethnobotanical study of medicinal plants used by the Zay people in Ethiopia. J. Ethnopharmacol. 85, 43–52 (2003).
Woldeamanuel, M. M. et al. Ethnobotanical study of endemic and non-endemic medicinal plants used by indigenous people in environs of Gullele botanical garden Addis Ababa, central Ethiopia: A major focus on Asteraceae family. Front. Pharmacol. 13, 1020097 (2022).
Nyakoojo, C. & Tugume, P. Traditional use of wild edible plants in the communities adjacent Mabira Central Forest Reserve, Uganda. Ethnobot. Res. Appl. 20, 1–14 (2020).
Naz, A., Amjad, M. S., Umair, M., Altaf, M. & Ni, J. Medicinal plants used as therapeutic medicine in the Himalayan region of Azad Jammu and Kashmir. S. Afr. J. Bot. 150, 194–216 (2022).
Guzo, S., Lulekal, E. & Nemomissa, S. Ethnobotanical study of underutilized wild edible plants and threats to their long-term existence in Midakegn District, West Shewa Zone, Central Ethiopia. J. Ethnobiol. Ethnomed. 19, 30 (2023).
Lulekal, E., Asfaw, Z., Kelbessa, E. & Van Damme, P. Ethnomedicinal study of plants used for human ailments in Ankober District, North Shewa Zone, Amhara region, Ethiopia. J. Ethnobiol. Ethnomed. 9, 63 (2013).
Mahmood, A., Mahmood, A. & Malik, R. N. Indigenous knowledge of medicinal plants from Leepa valley, Azad Jammu and Kashmir, Pakistan. J. Ethnopharmacol. 143, 338–346 (2012).
Gillani, S. W. et al. An insight into indigenous ethnobotanical knowledge of medicinal and aromatic plants from Kashmir Himalayan region. Ethnobot. Res. Appl. 28, 1–21 (2024).
Waheed, M., Haq, S. M., Jameel, M. A., Arshad, F. & Bussmann, R. W. Documentation of ethnomedicinal plants used by the people living in reserved forests of semi-arid region Punjab Pakistan. Ethnobot. Res. Appl. 26, 1–17 (2023).
Ahmad, M. et al. An ethnobotanical study of medicinal plants in high mountainous region of Chail valley (District Swat-Pakistan). J. Ethnobiol. Ethnomed. 10, 36 (2014).
Khan, M. F. et al. An ethnopharmacological survey and comparative analysis of plants from the Sudhnoti District, Azad Jammu and Kashmir, Pakistan. J. Ethnobiol. Ethnomed. 17, 14 (2021).
Giday, K. et al. Ethnobotanical study of medicinal plants from degraded dry afromontane forest in northern Ethiopia: Species, uses and conservation challenges. J. Herb. Med. 6, 96–104 (2016).
Ghimire, S. K. Medicinal plants in the Nepal Himalaya: Current issues, sustainable harvesting, knowledge gaps and research priorities. Med. Plants Nepal Anthol. Contemp. Res. 25–42 (2008).
Nondo, R. S. et al. Ethnobotanical survey and in vitro antiplasmodial activity of medicinal plants used to treat malaria in Kagera and Lindi regions, Tanzania. J. Med. Plants Res. 9, 179–192 (2015).
Siew, Y.-Y. et al. Ethnobotanical survey of usage of fresh medicinal plants in Singapore. J. Ethnopharmacol. 155, 1450–1466 (2014).
Bano, A. et al. Quantitative ethnomedicinal study of plants used in the skardu valley at high altitude of Karakoram-Himalayan range, Pakistan. J. Ethnobiol. Ethnomed. 10, 43 (2014).
Shaheen, H., Qaseem, M. F., Amjad, M. S. & Bruschi, P. Exploration of ethno-medicinal knowledge among rural communities of Pearl Valley; Rawalakot, District Poonch Azad Jammu and Kashmir. PLoS ONE 12, e0183956 (2017).
Staub, P. O., Geck, M. S., Weckerle, C. S., Casu, L. & Leonti, M. Classifying diseases and remedies in ethnomedicine and ethnopharmacology. J. Ethnopharmacol. 174, 514–519 (2015).
Umair, M., Altaf, M., Bussmann, R. W. & Abbasi, A. M. Ethnomedicinal uses of the local flora in Chenab riverine area, Punjab province Pakistan. J. Ethnobiol. Ethnomed. 15, 7 (2019).
Aziz, M. A. et al. Ethno-medicinal survey of important plants practiced by indigenous community at Ladha subdivision, South Waziristan agency, Pakistan. J. Ethnobiol. Ethnomed. 12, 53 (2016).
Madikizela, B., Kambizi, L. & McGaw, L. J. An ethnobotanical survey of plants used traditionally to treat tuberculosis in the eastern region of OR Tambo district, South Africa. S. Afr. J. Bot. 109, 231–236 (2017).
Doğan, Ş. & Doğan, A. The ethnobotanical study of traditional medicinal plants in Orhangazi (Bursa–Türkiye). Genet. Resources Crop Evol. 1–29 (2025).
Shawarb, N., Qaoud, H. A. & Hussein, F. Ethnopharmacological survey of medicinal plants used by patients with gastrointestinal tract disorders in the northern region of Palestine. Pal. Med. Pharm. J. 7, 97–116 (2021).
Rokaya, M. B. et al. Traditional uses of medicinal plants in gastrointestinal disorders in Nepal. J. Ethnopharmacol. 158, 221–229 (2014).
Wali, R. et al. Ethnomedicinal appraisal of plants used for the treatment of gastrointestinal complaints by tribal communities living in Diamir district, Western Himalayas, Pakistan. PLoS ONE 17, e0269445 (2022).
Hussain, S. et al. Quantitative ethnomedicinal study of indigenous knowledge on medicinal plants used by the tribal communities of Central Kurram, Khyber Pakhtunkhwa, Pakistan. Ethnobot. Res. Appl. 23, 1–31 (2022).
Hussain, A. et al. Biosynthesized silver nanoparticle (AgNP) from Pandanus odorifer leaf extract exhibits anti-metastasis and anti-biofilm potentials. Front. Microbiol. 10, 8 (2019).
Ajaib, M., Khan, Z. & Zikrea, A. Ethnobotanical survey of some important herbaceous plants of District Kotli, Azad Jammu & Kashmir. Biologia (Pakistan) 60, 11–22 (2014).
Moerman, D. E. Native American Medicinal Plants: An Ethnobotanical Dictionary (Timber Press Portland, 2009).
Ladio, A., Lozada, M. & Weigandt, M. Comparison of traditional wild plant knowledge between aboriginal communities inhabiting arid and forest environments in Patagonia, Argentina. J. Arid Environ. 69, 695–715 (2007).
Leonti, M., Sticher, O. & Heinrich, M. Antiquity of medicinal plant usage in two Macro-Mayan ethnic groups (Mexico). J. Ethnopharmacol. 88, 119–124 (2003).
Qureshi, R. Medicinal flora of hingol national park, Baluchistan, Pakistan. Pak. J. Bot. 44, 725–732 (2012).
Bano, A., Ayub, M., Rashid, S., Sultana, S. & Sadia, H. Ethnobotany and conservation status of floral diversity of Himalayan range of Azad Jammu and Kashmir Pakistan. Pak. J. Bot. 45, 243–251 (2013).
Amjad, M. S., Arshad, M., Sadaf, H. M., Akrim, F. & Arshad, A. Floristic composition, biological spectrum and conservation status of the vegetation in Nikyal valley, Azad Jammu and Kashmir. Asian Pacific J. Trop. Dis. 6, 63–69 (2016).
Shah, M., Hassan Sher, H. A., Allkin, B. & Cossu, T. A. Floristic and quantitative ethnobotanical exploration of Daral valley. Swat. Pak. J. Bot 57, 617–638 (2025).
Ahmad, K. S., Rahmatullah Qureshi, R. Q., Mansoor Hameed, M. H., Farooq Ahmad, F. A. & Tahira Nawaz, T. N. Conservation assessment and medicinal importance of some plants resources from Sharda, Neelum Valley, Azad Jammu and Kashmir, Pakistan. (2012).
Ijaz, S., Perveen, A. & Ashraf, S. Anthropogenic threats and their impact assessment on medicinal flora of western Himalaya-Neelum Valley (Azad Jammu & Kashmir). Pak. J. Bot 54, 1827–1839 (2022).
Khan, M. A., Khan, M. A., Hussain, M. & Ghulam, G. M. An ethnobotanical inventory of himalayan region poonch valley azad kashmir (Pakistan). Ethnobot. Res. Appl. 8, 107–123 (2010).
Acknowledgements
Authors are thankful to the local people of Abbaspur for giving time and information during data collection.
Funding
NA.
Author information
Authors and Affiliations
Contributions
A.A., S.K. and M.S.A designed project, involve in data collection and prepared final draft of manuscript. A.A., S.K., M.S.A and Z.B invole in data analsis and interpretation. M.S.A., S.K, and I.V.-K. revised and commented the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Competing interests
Authors indicate no potential conflict of interest.
Ethics approval and consent to participate
The present research is purely based on field surveys. The ethical approval to conduct the study was given by the Ethics Committee of the Women University of Azad Jammu & Kashmir Bagh (Ref No.: WUAJ&K/IEC/05) before initiating the surveys. In addition to this, legal permission to conduct interviews was given by members of municipality committee. A written Prior Informed Consent (PIC) was obtained from all the informants and/or their legal guardians after explaining the objective and consequence of study. The ethical guidelines provided by the International Society of Ethnobiology (http://www.ethnobiology.net/) were strictly followed.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Ayoub, A., Kanwal, S., Binish, Z. et al. Ethnobotanical heritage and conservation priorities of medicinal flora in a remote Himalayan border region of Azad Kashmir, Pakistan. Sci Rep 16, 9063 (2026). https://doi.org/10.1038/s41598-026-39964-9
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-026-39964-9
