
Abstract
The aim of this study is to investigate the relationship between neck circumference-to-height ratio (NHtR) and the risk of coronary heart disease (CHD) in women from Northern China. A total of 553 female patients presenting with suspected CHD due to chest pain at Chengde Central Hospital between 2021 and 2025 were included in the study. Based on coronary angiography results, the participants were categorized into the CHD group and the non-CHD group. Logistic regression analysis was performed to identify potential influencing factors. The diagnostic value of NHtR was evaluated using Receiver Operating Characteristic (ROC) curves and the Area Under the Curve (AUC). In the Northern Chinese female population, NHtR is associated with susceptibility to CHD. After adjusting for potential confounders, including age, hypertension, diabetes, smoking, and CR, multivariable regression analysis demonstrated a positive correlation between elevated NHtR levels and increased CHD risk (P < 0.05). The correlation heatmap revealed significant associations between NHtR and factors such as age, hypertension, diabetes, and CR. The model exhibited robust discriminative power, with an AUC of 0.728. This study was conducted in a single-center female population in northern China, and the results demonstrate an independent association between NHtR and coronary heart disease. This finding offers a promising biophysical metric for conducting more in-depth research on disease associations within this specific population.
Similar content being viewed by others

Introduction
Cardiovascular disease (CVD) remains the leading cause of mortality among both urban and rural populations in China.1 Among the various forms of CVD, the burden of coronary atherosclerotic heart disease (CHD) is especially pronounced. A review of global epidemiological data reveals that CHD-related deaths comprise between 30.8 and 40% of all-cause mortality among adults.2 Notably, women represent 6.2% of coronary heart disease deaths.3 A comparison of cardiovascular risk factors between men and women reveals that pregnancy-related diseases, oral contraceptive use, and polycystic ovary syndrome are more prevalent among women.4 The China Acute Myocardial Infarction (AMI) Registry Study (CAMI) further elucidates this disparity, demonstrating that the proportion of female patients undergoing percutaneous coronary intervention (PCI) is lower than that of males, while the risk of in-hospital death is 5 times higher. This figure is eight times higher than that of males of the same age group. Furthermore, among discharged patients, the two-year mortality rate of young females was significantly higher than that of males in the same age group.5 This evidence underscores the necessity for heightened awareness regarding cardiovascular health in women. Epidemiological studies have revealed a heightened burden of CVD in the northern and northeastern regions of China.6 This geographical discrepancy may be attributable to the pronounced climatic variations in the northern regions, particularly the vasoconstrictor response and substantial fluctuations in blood pressure induced by extreme cold temperatures (e.g., as low as − 30 °C) during winter months, which have been demonstrated to elevate the risk of cardiovascular events. Consequently, northern female populations encounter a notably elevated risk of CHD.
In recent years, the mechanism of adipose tissue distribution patterns in cardiovascular metabolic diseases has attracted considerable attention. Compared with visceral fat, upper body subcutaneous adipose tissue (SAT) demonstrates superior pathophysiological significance due to its distinctive lipolytic properties.7 This phenomenon is particularly pronounced in the obese population, where SAT has been demonstrated to induce systemic insulin resistance by releasing excess free fatty acids.8 Neck circumference (NC), a straightforward clinical indicator of SAT accumulation in the upper body, has been significantly associated with CVD risk factors and metabolic syndrome.9,10,11 This gender discrepancy may be associated with the disparity in height between males and females.12 To address the impact of height, scholars have proposed the standardized neck circumference-to-height ratio (NHtR) as a novel metric for evaluation. A comparison of NHtR with NC revealed that the former exhibited superior cardiovascular risk prediction efficacy through standardization of individual height differences.13,14 An Indian study demonstrated that the efficacy of the standardized NHtR in predicting metabolic syndrome was significantly higher (area under the curve [AUC] = 0.770) than that of NC (AUC = 0.753).14
The objective of this study was to examine the relationship between the standardized NHtR and the likelihood of developing CHD among women in northern China. The investigation sought to furnish a scientific foundation for the early identification and intervention of cardiovascular risk in the female demographic.
Materials and methods
Study population
This study continuously included a total of 866 female patients with suspected CHD who presented to Chengde Central Hospital with chest pain and underwent coronary angiography (CAG) between September 2021 and April 2025. This study is a single-center case-control experiment. The results of the CAG were then used to determine the presence of CHD in the patients, and those who met the established criteria were divided into two groups: CHD and Non-CHD. The distribution of these groups is illustrated in Fig. 1.

Flow-diagram illustrating patient flow in the trial.
Inclusion and exclusion criteria
The inclusion criteria for this study are as follows:
-
(1)
Female patients aged > 18 years who presented to the clinic with chest pain and chest tightness and who had feasible CAG;
-
(2)
Patients with complete general clinical data and relevant auxiliary examinations.
The following criteria were used to determine exclusion from the study:
-
(1)
History of coronary reperfusion therapy, including thrombolytic therapy, PCI, or coronary artery bypass grafting (CABG).
-
(2)
History of heart valve disease, severe heart failure (New York Heart Association [NYHA] classification ≥ grade 2).
-
(3)
History of severe renal disease or liver failure.
-
(4)
Contraindications to CAG.
-
(5)
Patients with significant goiter.
Data collection
Baseline data were collected from the patients: (1) demographic characteristics: age, height, weight, calculated body mass index (BMI) = weight kg/height m2 (kg/m2); (2) past history: smoking, drinking, hypertension, and diabetes; (3) vital signs: diastolic blood pressure (DBP); (4) first laboratory indicators after admission (venous blood drawn on an empty stomach in the morning after admission): white blood cells (WBC), red blood cells (RBC), platelets (PLT), aspartate aminotransferase (AST), potassium ions (K+), uric acid (UA), creatinine (CR), total cholesterol (TC), low-density lipoprotein (LDL-C).
Relevant definitions
CHD is hereby defined as CAG showing ≥ 50% diameter stenosis in at least 1 major coronary artery or its branches.15 The CAG procedure was conducted by an experienced cardiovascular specialist, and the findings were assessed by two independent, experienced interventional cardiologists, who had no conflicts of interest regarding this study. In case of any disagreement, a third physician was asked to negotiate a consensus.
Participants were instructed to assume an upright posture with their heads positioned on the Frankfurt horizontal plane. The upper edge of the tape measure was positioned directly below the laryngeal process and applied perpendicular to the long axis of the neck. Measurements were conducted twice by trained clinicians or medical students. The precision of the measurements was maintained at 0.1 centimeters, with the requisite that the discrepancy between the two measurements be less than 0.5 centimeters. The mean value of the two measurements was utilized for subsequent analysis.
Data quality and missing data
A systematic assessment of data completeness and consistency was implemented. All missing values were classified as missing completely at random (MCAR), with the proportion of missing data being less than 10% of the total sample size. Any inconsistent or incomplete data were corrected and completed. In cases where missing data exceeded 10% of the observations for a particular variable, direct deletion was employed. For quantitative data with complete independent variables, the regression estimation method using SPSS will be employed, whereas the mode imputation method will be utilized for categorical data with complete independent variables, the mode imputation method was utilized to replace missing values. To evaluate the potential impact of missing data handling methodologies on the results, we conducted a sensitivity analysis of the models both prior to and following imputation, utilizing the area under the curve (AUC) as a metric for assessment.
Statistical analysis
The statistical analysis of the study was carried out using SPSS 27.0 software (IBM, Corporation, Armonk, NY, USA), and the graphical representation was prepared using R 4.4.1 The normality of the measurement information was assessed through the implementation of the Shapiro-Wilk test. Conforming to the normal distribution, the measurement information was expressed as the mean ± standard deviation (\(\bar{x}\)± S) through the application of the independent samples t test. For measurement information that did not conform to a normal distribution, the expression was given as M (Q1, Q2) through the utilization of the Mann-Whitney U test. The count data were expressed as a percentage, and the chi-square (χ2) test was employed to analyze the data. Logistic regression was utilized to examine the factors that influenced the outcomes, and odds ratios (OR) and 95% confidence intervals (CI) were calculated. The multifactorial logistic regression analysis model was visually represented, and the corresponding nomogram were plotted. Correlation heatmaps were implemented to analyze the relationship between NHtR and other variables. Subgroup analyses were performed to ascertain whether the relationship between NHtR and CHD was influenced by covariates. An interaction of P < 0.05 was considered to be statistically significant. The diagnostic efficacy of the model was determined by the subject operating characteristic curve (ROC) and AUC. The variance inflation factor (VIF) was calculated to test for multicollinearity among the influencing factors. The predictive ability of NHtR for CHD was evaluated using the Hosmer-Lemeshow test and the Curve of Calibration (COC). A P value greater than 0.05 indicated a strong calibration of the model and a good goodness of fit. To ensure the reliability of the model, Decision Curve Analysis (DCA) was performed to evaluate the effectiveness of the model in facilitating clinical decision-making. This paper was analyzed using the available data, so no sample size calculation was performed. A P value less than 0.05 indicates a statistical difference.
Results
Clinical baseline data comparisons
A total of 313 patients were excluded based on the established exclusion criteria, resulting in the final inclusion of 553 cases in this study. Among these, 350 cases were designated as the case group, comprising patients with CHD, while 203 cases served as the control cohort, consisting of patients without CHD. A statistically significant difference was observed between the Non-CHD and CHD cohorts regarding age, hypertension, diabetes, smoking, CR, and NHtR (P < 0.05). Conversely, the remaining indexes did not demonstrate statistical significance (P > 0.05) (Table 1).
Association of NHtR with CHD
A logistic regression analysis was conducted, with CHD (0 = no, 1 = yes) serving as the dependent variable and age, hypertension, diabetes, smoking, CR, and NHtR as independent variables. The application of univariable logistic regression analysis yielded findings that indicated the following factors to be statistically significant for CHD: age, hypertension, diabetes, smoking, CR, and NHtR. Further, the multivariable logistic regression analysis demonstrated that these variables were independent associated factors for CHD. The visualization of the multifactorial logistic regression analysis and the plotting of the corresponding nomogram graphs yielded the predicted probability of the risk of CHD. The probability of developing CHD in the 450th patient depicted in Fig. 2a was 84.40% (Table 2; Fig. 2a)
Three models were formulated to adjust for confounders: model 1 (baseline model, unadjusted), model 2 (adjusted for age), and model 3 (adjusted for hypertension, diabetes, smoking, and CR in addition to age). The NHtR was evaluated using continuous and quartile-based NHtR indices, with trend P values for NHtR quartiles being calculated. When employed as a continuous variable, the NHtR was identified as a significant risk factor for all models: unadjusted (OR: 1.233, 95% CI 1.111, 1.368) and fully adjusted (OR: 1.132, 95% CI 1.010, 1.269). The likelihood of CHD prevalence escalated 1.134-fold with each unit increase in NHtR. When conducting data analysis stratified by quartiles, participants in the highest quartile exhibited a 2.397-fold increased risk of coronary heart disease compared to those in the lowest quartile (OR 2.397, 95% CI 1.458, 3.941) in the unadjusted model. In the fully adjusted model, although the odds ratio (OR) for Q4 did not achieve statistical significance, it demonstrated a statistically significant trend upon trend testing (P for trend < 0.05). Thus, with the ascending quartile levels of NHtR (ranging from Q1 to Q4), the risk of developing coronary heart disease continued to exhibit an upward trajectory. The application of a correlation heat map was undertaken to facilitate the analysis of the interrelationship between NHtR and other independent variables. As demonstrated in Fig. 2b, NHtR exhibited a weak correlation (P < 0.05) with CR (r = 0.2), hypertension (r = 0.2), diabetes mellitus (r = 0.1), and age (r = 0.1) (Table 3; Fig. 2).

Nomogram and Heat map of NHtR for predicting CHD. a Nomogram of NHtR for predicting CHD. b Heat map of NHtR for predicting CHD.
Subgroup analysis
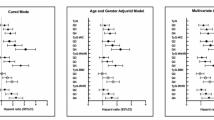
Subgroup analyses were performed for age (< 65 years or > = 65 years), hypertension, diabetes, and smoking, and interaction effects were assessed by P values. The findings indicated the absence of a statistically significant interaction effect for the aforementioned variables. This finding indicates that NHtR is independently associated with the risk of CHD in women in northern China, and this association remains consistent across various subgroups (P for interaction > 0.05) (Fig. 3).

Subgroup analysis for NHtR.
Evaluation model value
COC, DCA, and ROC curves were generated to assess the predictive value of NHtR for the development of CHD in women residing in northern China. The COC demonstrated that the Hosmer-Lemeshow test yielded a value of 0.126, and the VIF of each independent risk factor was less than 10, with no evidence of multicollinearity, suggesting a satisfactory fit and indicating a reasonable agreement between the predicted and actual probabilities. DCA was performed to assess the effectiveness of the model in facilitating clinical decision making. The model demonstrated the greatest clinical benefit across a threshold probability range of 0.11 to 0.92. The AUC for the prediction of CHD occurrence using the NHtR model was 0.728 (95% CI 0.685–0.770). The optimal cut-off value was determined to be 21.67, indicating that the risk of CHD prevalence was higher when NHtR was higher than 21.67, with a sensitivity of 74.30%. The findings indicate that the NHtR model demonstrates notable efficacy in predicting the incidence of CVD among the female population in northern China (Figs. 4, 5).

Calibration curves and decision curve for NHtR. a The calibration curve of NHtR for predicting CHD. b The decision curve for NHtR to predict CHD.

ROC analysis with respect to the detection of CHD.
Sensitivity analysis
To assess the potential impact of missing data handling strategies on the discriminative ability of the models, we compared the performance of the logistic regression models derived from the multiple imputation dataset with those obtained from the original dataset. The results indicated that the AUC of the model post-multiple imputation was 0.728 (95% CI 0.685–0.770), while the AUC of the original model, which did not undergo imputation, was 0.731 (95% CI 0.688–0.774). The difference between the two was negligible (ΔAUC = 0.003), and there was considerable overlap in the confidence intervals. This finding suggests that the principal conclusions of this study remain robust regardless of the missing data handling strategy employed. (Supplementary Material Figure S1 and Figure S2)
Discussion
The present study showed the correlation between NHtR and CHD in a cohort of women hailing from northern China. The findings of the study demonstrated that NHtR levels exhibited a substantial positive interaction with CHD risk, subsequent to adjustment for confounding variables such as age, hypertension, diabetes, smoking, and CR (P < 0.05). The quartile-corrected results revealed a gradient of CHD prevalence with increasing quartiles (Q4 vs. Q1: OR 1.572, 95% CI 0.910, 2.716, P for trend < 0.05). A correlation heatmap was employed to assess the relationship between NHtR and other independent variables. The findings indicated a modest correlation between NHtR and age, hypertension, diabetes, and CR. In the subgroup analysis, no statistically significant interaction effect was observed according to age, hypertension, diabetes, and smoking (P for interaction > 0.05). The AUC of 0.728 indicated that the model had adequate predictive value. The results of this study indicate a correlation between NHtR and the incidence of CHD in women residing in northern China. This finding offers a novel bioindicator reference point for the early detection of CHD in this demographic.
Obesity is a well-recognized risk factor for CVD.16 The BMI was previously employed as an initial indicator to assess obesity. Nonetheless, subsequent studies have demonstrated that individuals with a BMI within the normal range but with central obesity exhibit a considerably elevated risk of developing CHD.17 This finding underscores the significance of whole-body fat distribution as compared to central fat distribution (predominantly visceral fat accumulation) in disease risk assessment. Central adiposity can be further delineated into upper and lower body fat distribution. In addition to other factors, SAT accumulation may also represent a distinct fat depot, independent of systemic or central obesity per se, thus posing additional metabolic risks.18 NC has been validated as an indicator for the assessment of SAT. NC was initially investigated as an anatomical marker of the neck in the field of otorhinolaryngology, and it has been shown to be associated with Obstructive Sleep Apnea (OSA).19 Pursuing further research has revealed a correlation between NC and an elevated risk of cardiovascular disease.20 Nevertheless, the predictive value of NC for CHD and CHD events remains a subject of controversy. For instance, a secondary analysis of the Framingham Heart Study, with CVD events as the endpoint, revealed that a statistically significant association between non-cardiovascular disease (NCVD) and CVD was not observed in multivariable-adjusted models.12 Conversely, a cross-sectional study of patients undergoing CAG demonstrated that NC was a superior predictor of coronary artery disease risk compared with other anthropometric measures.21 The underlying mechanism through which NC is linked to cardiovascular risk may be connected to the metabolic activity of SAT. Adipose tissue at this site has been shown to release a greater proportion of free fatty acids (FFA) into the circulation. Elevated plasma FFA levels have been demonstrated to promote insulin resistance through multiple pathways, including the inhibition of glucose uptake and interference with insulin signaling. Furthermore, elevated FFA levels have been observed to be associated with a variety of metabolic abnormalities, including disturbed lipid metabolism, increased oxidative stress, vascular endothelial damage, and other metabolic abnormalities.22,23,24 To address the impact of height discrepancies on NC, researchers have proposed NHtR as a corrective measure. NHtR has been found to be more closely associated with CHD as a more validated assessment of SAT.25 As indicated by the extant literature, a significant correlation has been demonstrated between SAT accumulation and advanced age, hypertension, and diabetes.26 Excessive influx of free fatty acids, on one hand, can promote ectopic fat deposition in the liver and the synthesis of very low-density lipoprotein, thereby exacerbating atherogenic dyslipidemia. On the other hand, it may induce insulin resistance in peripheral tissues such as skeletal muscle, thereby activating a state of systemic low-grade inflammation. Collectively, these metabolic derangements compromise endothelial function, facilitating the onset and progression of atherosclerosis. 12,27 The findings of the correlation heat map analysis in this study corroborate these perspectives and substantiate the correlation of NHtR with age, hypertension, and diabetes mellitus. In addition, some studies have suggested that NHtR may serve as a potential marker of renal insufficiency.25 The present study found a correlation between NHtR and serum CR levels. Further exploration of the relationship between NHtR and renal disease is warranted in future studies. The results of the Framingham Heart Study suggested that NC was more strongly associated with cardiometabolic risk factors in women compared to men.12 One potential explanation for this phenomenon is that women exhibit a greater capacity to transport FFA to the liver via visceral adipose tissue compared to men.28 In accordance with the findings of this study, the AUC of NHtR for predicting CHD risk was 0.728, which was considerably higher than the predictive efficacy of NC (AUC = 0.597) in the female population from northern China included in this study. Consequently, the NHtR model demonstrates potential predictive value for CHD risk in this population.
Although there exists a statistically significant association between NHtR and coronary heart disease, independent of known risk factors, the incremental value of NHtR in clinical applications still requires further elucidation. The baseline model, which consists of age, hypertension, diabetes, smoking, and CR, yields an AUC of 0.719; incorporating NHtR, this AUC increases to 0.728. While the absolute enhancement in discriminatory power is modest, the fact that NHtR is calculated using standard health examination parameters, without incurring additional testing costs, underscores its exceptional accessibility and reproducibility. NHtR is not intended to serve as a replacement for traditional risk factors but rather functions as an informative supplementary metric. Therefore, even though its effect on the overall discriminatory capacity of the model is limited, integrating NHtR into risk screening frameworks may represent a cost-effective strategy, facilitating preliminary identification within primary care populations and subsequently guiding more targeted and precise assessments.
This study has several limitations. First, the sample population was derived from a single-center female cohort in northern China, whose specific regional, genetic, and lifestyle contexts may influence the generalizability of the findings. Furthermore, the cross-sectional case-control design inherent to this study permits only the elucidation of the association between NHtR and coronary heart disease, without establishing any causal relationships or validating its prospective predictive value. Second, the study cohort was recruited from a single center and the sample size was relatively small. Future research should involve larger, multi-center populations and include external validation. Third, direct adipose tissue quantification (e.g., via CT or MRI) is necessary to validate the accuracy of NHtR measurements.
Conclusions
The present study demonstrated that NHtR is associated with the presence of CHD risk in women in northern China. This finding provides a novel perspective for cardiovascular risk assessment in women, and prospective cohort studies are necessary to further validate the results of this study.
Data availability
The datasets generated and/or analysed during the current study are not publicly available due to patient privacy reasons but are available from the corresponding author on reasonable request.
Abbreviations
- NHtR:
-
Neck circumference to height ratio
- CHD:
-
Coronary heart disease
- PCI:
-
Percutaneous coronary intervention
- CAG:
-
Coronary angiography
- CABG:
-
Coronary artery bypass grafting
- BMI, :
-
Body mass index
- DBP, :
-
Diastolic blood pressure
- WBC, :
-
White blood cells
- Hb, :
-
Hemoglobin
- PLT, :
-
Platelets
- AST, :
-
Aspartate aminotransferase
- UA, :
-
Uric acid
- CR, :
-
Creatinine
- TC, :
-
Total cholesterol
- LDL-C:
-
Low density lipoprotein cholesterol
- ROC:
-
Receiver operating characteristic
- DCA:
-
Decision curve analysis
- AUC:
-
The area under ROC curve
- MCAR:
-
Missing completely at random
- CI:
-
Confidence interval
- OR:
-
Odds ratio
- ACS:
-
Acute coronary syndrome
- NYHA:
-
New York Heart Association
References
Center For Cardiovascular Diseases The Writing Committee Of The Report On Cardiovascular Health And Diseases. China N. Report on Cardiovascular Health and Diseases in China 2023: an updated summary. Biomed. Environ. Sci. 37, 949–992 (2024).
Yang, G. R. et al. Association between neck circumference and coronary heart disease: a meta-analysis. Asian Pac. Isl Nurs. J. 4, 34–46 (2019).
Tsao, C. W. et al. Heart disease and stroke statistics-2022 update: a report from the American Heart Association. Circulation 145, e153–e639 (2022).
Gerdts, E. & Regitz-Zagrosek, V. Sex differences in cardiometabolic disorders. Nat. Med. 25, 1657–1666 (2019).
Lv, J. et al. Clinical characteristics, prognosis, and gender disparities in young patients with acute myocardial infarction. Front. Cardiovasc. Med. 8, 720378 (2021).
Liu, S. et al. Burden of cardiovascular diseases in China, 1990–2016: findings from the 2016 global burden of disease study. JAMA Cardiol. 4 (4), 342–352 (2019).
Dai, Y., Wan, X., Li, X., Jin, E. & Li, X. Neck circumference and future cardiovascular events in a high-risk population—a prospective cohort study. Lipids Health Dis. 15, 46 (2016).
Haider, A. et al. Sex and gender in cardiovascular medicine: presentation and outcomes of acute coronary syndrome. Eur. Heart J. 41, 1328–1336 (2020).
Nielsen, S., Guo, Z., Johnson, C. M., Hensrud, D. D. & Jensen, M. D. Splanchnic lipolysis in human obesity. J. Clin. Investig. 113, 1582–1588 (2004).
Pumill, C. A. et al. Neck circumference and cardiovascular outcomes: Insights from the Jackson Heart Study. Am. Heart J. 212, 72–79 (2019).
Yang, H. H. et al. Clinical diagnostic significance of combined measurement of Lipoprotein(a) and neck circumference in patients with coronary heart disease. Int. J. Gen. Med. 17, 5015–5027 (2024).
Preis, S. R. et al. Neck circumference as a novel measure of cardiometabolic risk: the Framingham Heart study. J. Clin. Endocrinol. Metab. 95, 3701–3710 (2010).
Li, G. et al. Neck circumference as an additional predictor of cardiovascular disease mortality: a multi-center prospective population-based study in northeastern China. Prev. Med. 180, 107859 (2024).
Selvan, C. et al. Neck height ratio is an important predictor of metabolic syndrome among Asian Indians. Indian J. Endocrinol. Metab. 20, 831–837 (2016).
Xu, B. et al. Angiographic quantitative flow ratio-guided coronary intervention (FAVOR III China): a multicentre, randomised, sham-controlled trial. Lancet 398, 2149–2159 (2021).
Valenzuela, P. L. et al. Obesity and the risk of cardiometabolic diseases. Nat. Rev. Cardiol. 20, 475–494 (2023).
Yajnik, C. S. & Yudkin, J. S. The Y-Y paradox. Lancet 363, 163 (2004).
Freedman, D. S. & Rimm, A. A. The relation of body fat distribution, as assessed by six girth measurements, to diabetes mellitus in women. Am. J. Public Health. 79, 715–720 (1989).
Yang, X. et al. Neck-to-height ratio and arterial stiffness in Chinese adults: cross-sectional associations in a community-based cohort. J. Hypertens. 39, 1195–1202 (2021).
Namazi, N., Larijani, B., Surkan, P. J. & Azadbakht, L. The association of neck circumference with risk of metabolic syndrome and its components in adults: a systematic review and meta-analysis. Nutr. Metab. Cardiovasc. Dis. 28, 657–674 (2018).
Arjmand, G., Shidfar, F., Molavi Nojoomi, M. & Amirfarhangi, A. Anthropometric indices and their relationship with coronary artery diseases. Health Scope. 4 (3), e25120 (2015).
Zhang, J. et al. The association of neck circumference with incident congestive heart failure and coronary heart disease mortality in a community-based population with or without sleep-disordered breathing. BMC Cardiovasc. Disord. 18, 108 (2018).
Li, G. et al. Incremental significance and sex discrepancies of neck circumference on the odds of ischaemic stroke: a multistage, population-based, cross-sectional study from Northeast China. BMJ Open. 12, e056932 (2022).
Wu, J. et al. Association between obesity indicators and cardiometabolic disease in Chinese adults. PLoS One. 18, e0273235 (2023).
He, Z. Y. et al. Neck-to-height ratio is positively associated with diabetic kidney disease in Chinese patients with type 2 diabetes mellitus. Front. Endocrinol. (Lausanne). 13, 1100354 (2023).
Ben-Noun, L. L. & Laor, A. Relationship between changes in neck circumference and cardiovascular risk factors. Exp. Clin. Cardiol. 11, 14–20 (2006).
Kelley, D. E., Mokan, M., Simoneau, J. A. & Mandarino, L. J. Interaction between glucose and free fatty acid metabolism in human skeletal muscle. J. Clin. Investig. 92 (1), 91–98. https://doi.org/10.1172/JCI116603 (1993).
Santosa, S., Hensrud, D. D., Votruba, S. B. & Jensen, M. D. The influence of sex and obesity phenotype on meal fatty acid metabolism before and after weight loss. Am. J. Clin. Nutr. 88, 1134–1141 (2008).
Acknowledgements
The authors extend sincere thanks to the members of the Chengde Central Hospital for their contribution.
Funding
This research was funded by Medical Science Research Project of Hebei Province (No. 20200348), S&T Program of Chengde (No. 202109A019), and Project for Cultivating Innovative Ability of Postgraduates at Chengde Medical University (No. CYCXZZ202508).
Author information
Authors and Affiliations
Contributions
DL: contributed to the design and conduct of the study, led data validation, project administration, funding acquisition, review and approval of the manuscript, and decision to submit the manuscript for publication. RL and ML: contributed to the collection, analysis, and interpretation of the data, as well as preparation and editing of the manuscript. WX, CJ, HH, JD, and JG: contributed to the collection and management of the data. WW: contributed to the design and conduct of the study, review and approval of the manuscript, and decision to submit the manuscript for publication. All authors contributed to the final version of the manuscript.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Consent for publication
Not applicable.
Ethics approval and informed consent
This study was approved by the Ethics Committee of Chengde Central Hospital. (Ethics number: ChiCTR2000041499). All participating subjects were fully aware of the trial and signed informed consent. All procedures strictly adhered to the guidelines outlined in the Declaration of Helsinki.
Patient consent statement
The authors confirm that patient consent forms have been obtained for this article.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Guo, R., Sun, M., Lin, W. et al. Association between neck circumference to height ratio and coronary heart disease: a case–control study in a Northern Chinese female population. Sci Rep 16, 9762 (2026). https://doi.org/10.1038/s41598-026-40895-8
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-026-40895-8
