
Abstract
MET exon 14 skipping mutations (METex14) or amplification drives a subset of non-small cell lung cancer (NSCLC). Tepotinib, a selective MET tyrosine kinase inhibitor (TKI), has shown promise in early trials; however, comparative efficacy and safety data across MET-altered subpopulations remain limited. This systematic review of six studies (546 patients) assessed the clinical outcomes of Tepotinib in METex14 or MET-amplified NSCLC. The primary endpoint was objective response rate (ORR); secondary endpoints included disease control rate (DCR), progression-free survival (PFS), overall survival (OS), and safety. The pooled objective response rate (ORR) was 52% (95% CI: 48–56%) and a disease control rate (DCR) of 76% (95% CI: 72–80%). Median PFS was 10.16 months, and median OS was 14.67 months. Subgroup analyses revealed no significant differences in ORR between METex14 (52%) and MET amplification (53%, p = 0.905) or between monotherapy (51%) and combination therapy (56%, p = 0.242). Common treatment-related adverse events (TRAEs) were grade 1–2 peripheral edema (50%) and diarrhea (36%); grade ≥ 3 TRAEs were infrequent (8% for edema). In conclusion, Tepotinib demonstrated comparable efficacy in METex14 and MET-amplified NSCLC with a manageable safety profile. The PFS benefit of combination therapy warrants further randomized trials. These findings support Tepotinib as a valuable therapeutic option for MET-altered NSCLC.
Similar content being viewed by others

Introduction
Worldwide, approximately 1.8 million deaths annually are attributed to lung cancer, which remains the leading cause of cancer-related mortality1,2. NSCLC accounts for approximately 85% of all lung cancer cases, and its global incidence continues to rise3,4. Treatment outcomes for NSCLC remain poor, with five-year survival rates declining sharply from 68% in stage IB to just 21% in stage IIIC. Moreover, most advanced-stage NSCLC cases acquire resistance to existing therapies, leading to disease progression5,6.
NSCLC comprises a genetically heterogeneous group of malignancies driven by various oncogenic alterations7. Several recurrent and potentially targetable oncogenes have been identified in NSCLC, including mutations in epidermal growth factor receptor (EGFR) and v-raf murine sarcoma viral oncogene homolog B1 (BRAF), as well as chromosomal rearrangements involving ROS proto-oncogene 1 receptor tyrosine kinase (ROS1) and anaplastic lymphoma kinase (ALK)8,9.
The c-MET protein, encoded by the MET proto-oncogene, is a receptor tyrosine kinase expressed on cell membranes10. Constitutively altered MET pathway activation strongly propels malignant transformation, stimulates tumor cell progression as well as angiogenesis, increases tumor invasiveness as well as metastatic potential, and mediates resistance to MET tyrosine kinase inhibitors (TKIs)10,11. MET signaling dysregulation typically arises through three distinct mechanisms: protein overexpression, MET gene amplification, and exon 14 skipping mutations (METex14)11. In NSCLC, MET exon 14 skipping mutations are established oncogenic drivers, whereas MET amplification and protein overexpression are generally associated with poorer prognosis12,13,14,15,16,17. It should be noted that MET gene fusions, though rare and actionable, were not included in the present analysis due to insufficient data in the identified studies.
Given the extensive involvement of aberrant MET signaling in NSCLC pathogenesis and therapeutic resistance, MET has emerged as a promising therapeutic target. Over the past decade, several MET-targeted therapies—including TKIs and antibody-drug conjugates (ADCs)—have entered clinical evaluation18,19,20,21,22,23,24. MET-targeting TKIs are classified into two major categories: Type I inhibitors primarily engage the ATP-binding site of the c-MET kinase domain in a characteristic “U-shaped” binding orientation and are particularly active against METex14 mutations25. Type II inhibitors adopt an “extended” binding conformation, interacting with both the ATP pocket and an adjacent hydrophobic pocket. Although they may retain activity against certain resistance mutations that render Type I inhibitors ineffective, Type II inhibitors often exhibit reduced selectivity and increased off-target effects26.
Tepotinib, a highly selective and potent Type Ib MET inhibitor, has received first-line approval for the treatment of NSCLC patients harboring METex14 skipping mutations27,28. Long-term follow-up data from the VISION trial recently demonstrated an ORR of 57.3% and a median PFS of 12.6 months in treatment-naïve patients29.
Nevertheless, the existing evidence for Tepotinib has important limitations. Most available data derive from single-arm Phase II studies, such as VISION, and small-scale trials. These studies inherently lack control arms and include limited patient numbers19,29,30.
This systematic review evaluates the clinical efficacy and safety of Tepotinib in NSCLC patients harboring MET amplification or METex14 skipping mutations. This work aims to delineate the therapeutic benefit across these distinct molecular subgroups and thereby provide robust evidence to inform clinical decision-making.
Results
Literature screening results
The study selection process is illustrated in Fig. 1. A total of 739 potentially eligible studies were identified using predefined search strategies. After removing 240 duplicates, we performed title and abstract screening, which excluded a further 462 records for irrelevance, non-English articles, or wrong formats. Full-text scrutiny then excluded a further 30 studies for incomplete outcomes, continuing trials, lack of relevant outcomes, or low patient numbers. Six studies, after meeting inclusion criteria, were included in the meta-analysis.

PRISMA flow chart of study selection process.
Basic characteristics
Table 1 provides an overview of characteristics derived from the selected studies. These studies, appearing between 2022 and 2025, collectively encompassed a total of 546 patients. Most studies were Phase II clinical trials29,33,34,36,39, accompanied by one retrospective study40. All patients had metastatic or advanced NSCLC with MET alterations, including amplification and/or exon 14 skipping mutations. All patients enrolled presented with metastatic or advanced-stage NSCLC. Female patient representation ranged significantly from 12.5% to 75.0%, with average patient age varying from 59.3 to 74.0 years. The majority demonstrated an Eastern Cooperative Oncology Group (ECOG PS) performance status of 0 or 1. Smoking history varied, including current, former, and never-smokers. Tepotinib monotherapy (500 mg once daily) was used in most studies. One study investigated Tepotinib combined with gefitinib36, and another examined Tepotinib combined with osimertinib34.
Quality assessment
Assessment of non-randomized studies’ methodological rigor was conducted using the Methodological Index for Non-randomized Studies (MINORS) scale35, and detailed findings are summarized in Supplementary Table S2. The MINORS scale was selected because it is specifically validated for assessing the methodological quality of non‑comparative (single‑arm) interventional studies, which constituted the majority of our included trials. While ROBINS‑E is designed for exposure studies, MINORS better aligns with the interventional nature of our meta‑analysis. The lone randomized controlled trial included underwent evaluation through the Cochrane Risk of Bias Tool (RoB 2)36,37, revealing a high overall bias risk; detailed results for this assessment are provided in Supplementary Table S3.
Analysis of efficacy
The primary endpoint was the ORR, with secondary outcomes including DCR, DOR, PFS, and OS. Random-effects modeling was applied under conditions of notable heterogeneity; otherwise, fixed-effects modeling was utilized. The pooled analysis showed an ORR of 52% (95% CI: 48%–56%; I2 = 34.4%), a DCR of 76% (95% CI: 72%–80%; I2 = 37.6%), a mean DOR of 12.62 months (95% CI: 8.73–18.24 months; I² = 91.1%), a mean PFS of 10.16 months (95% CI: 7.60–13.58 months; I2 = 72.8%), and a mean OS of 14.67 months (95% CI: 9.60–22.43 months; I2 = 93.5%). It should be noted that this pooled ORR includes both treatment‑naive and previously treated patients, as the included studies did not consistently stratify outcomes by line of therapy. Significant heterogeneity was observed for DOR, PFS, and OS, while ORR and DCR exhibited low to moderate heterogeneity. The efficacy analysis results are shown in Figs. 2, 3, 4 and 5, and 6.

Forest plot of ORR.

Forest plot of DCR.

Forest plot of mDOR.

Forest plot of mOS.

Forest plot of mPFS.
Subgroup analysis
Subgroup analysis by MET dysregulation type revealed an ORR of 53% (95% CI: 45%–60%) for MET amplification and 52% (95% CI: 47%–57%) for MET exon 14 skipping, without significant differences between subgroups (χ² = 0.01, p = 0.9054) (Fig. 7). Subgroup analysis by therapy type showed an ORR of 51% (95% CI: 46%–56%) for monotherapy and 56% (95% CI: 48%–64%) for combination therapy (i.e., Tepotinib plus an EGFR‑TKI such as gefitinib or osimertinib), also without significant differences (χ² = 1.37, p = 0.2421) (Fig. 8).

Forest plot of ORR in subgroup analysis on MET dysregulation.

Forest plot of ORR in subgroup analysis on therapy type.
AEs
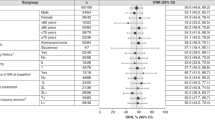
Safety evaluations of AEs were performed for all patients who received Tepotinib, but as a result of incomplete response, certain patients were excluded from the efficacy analyses. Amongst six studies that were included, there were five studies involving 511 patients with 449 treatment-related adverse event (TRAE) reports, with most TRAE being mild in nature. One study36 failed to report relevant TRAE data. Adverse events that were attributed to Tepotinib were graded by criteria established by the National Cancer Institute (National Toxicity Criteria for Adverse Events), with a detailed description given in Table 2. Pooled incidence rates for TRAEs are summarized in Table 3, indicating that most TRAEs were categorized as Grade 1–2. The most frequently reported any-grade TRAEs included peripheral edema (50%, 95% CI: 34%–65%), diarrhea (36%, 95% CI: 18%–54%), hypoalbuminemia (22%, 95% CI: 18%–25%), nausea (22%, 95% CI: 18%–26%), and elevated blood creatinine levels (18%, 95% CI: 10%–25%). Increases in alanine aminotransferase and aspartate aminotransferase were each reported in 13% of patients. Severe (Grade ≥ 3) TRAEs were uncommon, with peripheral edema (8%, 95% CI: 6%–11%) being the most frequent. Grade ≥ 3 events were uncommon (2% for hypoalbuminemia and ALT elevation) and were not reported for diarrhea, creatinine increase, or AST elevation. Estimates of other TRAEs showed low to moderate heterogeneity.
Sensitivity analysis
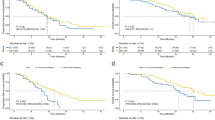
Sensitivity analysis using the leave-one-out method assessed the robustness of study findings. Each study was sequentially removed, and pooled estimates were recalculated to verify stability. Removing individual studies did not significantly alter the overall results, confirming the reliability of findings. Results of sensitivity analyses for ORR, DCR, DOR, PFS, and OS are presented in Figures S2, S3, S4, and S5, respectively.
Discussion
This systematic review and meta-analysis comprehensively evaluated the efficacy of Tepotinib in 546 patients with MET-altered advanced NSCLC. The analysis confirmed prominent clinical efficacy, yielding a pooled ORR of 52% and a DCR of 76%. The pooled efficacy estimates encompass both treatment‑naive and pretreated populations, as the included studies did not consistently stratify outcomes by line of therapy, which is an important consideration when interpreting these results. Additionally, median DOR reached 12.62 months, PFS averaged 10.16 months, and OS was 14.67 months. Analysis of time-to-event metrics revealed notable heterogeneity.
These findings closely parallel results from significant clinical trials. Notably, the VISION trial, a pivotal Phase II study investigating Tepotinib in METex14-altered NSCLC patients, demonstrated an ORR of 57.3% and median PFS of 12.6 months in treatment-naïve subjects, aligning with our current analysis29. This consistency underscores Tepotinib’s effectiveness in clinical practice. Tepotinib exhibited comparable efficacy when contrasted with other selective MET inhibitors. For instance, the GEOMETRY mono-1 trial examined capmatinib—another selective type Ib MET inhibitor—reporting an ORR of 68% (95% CI: 55.0–79.7%) in 60 previously untreated patients and 44% (95% CI: 34.1–54.3%) in 100 pretreated cases. However, cross-trial comparisons are limited by differences in patient populations and study designs41,42. The present meta-analysis contributes by quantitatively synthesizing multiple studies, providing more precise efficacy estimates and confirming reproducible Tepotinib activity.
Subgroup analyses yielded clinically relevant insights. Comparable efficacy was noted between METex14 skipping (ORR: 52%) and MET amplification (ORR: 53%) subgroups. While METex14 skipping mutations are established oncogenic drivers sensitive to MET inhibition, the notable activity in MET-amplified tumors highlights the broader therapeutic potential of Tepotinib. This finding challenges earlier assumptions regarding the limited responsiveness of MET amplification and indicates that high-level MET amplification may represent a potent, targetable driver, particularly with highly selective inhibitors such as Tepotinib.
Analysis by treatment regimen showed similar ORR for monotherapy (51%) and combination therapy (56%). However, a significant advantage emerged for combination therapy in PFS (16.60 months versus 9.35 months for monotherapy, p = 0.034). This discrepancy suggests that combination therapy, while not substantially increasing response rates, may enhance response durability. A numerical but non-significant improvement in OS for combination therapy (25.14 months versus 11.84 months, p = 0.078) further supports this notion. These findings align with preclinical evidence demonstrating synergistic effects when MET inhibitors combine with EGFR-targeted agents in MET- and EGFR-activated tumor models43,44,45.
Substantial heterogeneity observed in time-to-event outcomes (I2 > 70% for PFS, OS, and DOR) warrants attention. Potential causes include differences in patient characteristics (e.g., prior treatments, ECOG performance status, metastatic burden), methodological diversity (single-arm trials versus observational studies), and variations in defining MET amplification (especially gene copy-number thresholds). Furthermore, methodological differences in detecting MET amplification—such as variations in assay platforms and gene-copy-number thresholds—likely contributed to the observed heterogeneity. High heterogeneity in the amplification subgroup (I2 up to 94.7% for OS) reflects diverse responses, possibly due to the continuous nature of amplification compared to the binary presence of METex14 mutations.
Despite this heterogeneity, sensitivity analyses using leave-one-out methods confirmed the robustness of pooled estimates. Removing individual studies did not substantially affect conclusions, suggesting consistent central effects rather than contradictory findings. Prediction intervals for key outcomes offer clinically realistic expectations, aiding clinical decision-making.
Collectively, the findings solidify Tepotinib as a crucial therapeutic option for MET-altered NSCLC. Consistent efficacy across METex14 and amplification subgroups supports comprehensive MET testing, including both mutation and amplification analyses. The promising results of combination therapy, particularly significant PFS improvement, highlight the need for randomized trials evaluating combination approaches, especially in patients with concurrent EGFR mutations or EGFR-TKI resistance. To our knowledge, this is the first meta-analysis that quantitatively synthesizes and directly compares the efficacy of Tepotinib between MET exon 14 skipping and MET amplification subgroups, while also evaluating the differential outcomes of monotherapy versus combination regimens. Our findings provide the most robust evidence to date on this topic, addressing a critical gap in the existing literature, which primarily consists of single-arm trials.
Future research should address several knowledge gaps. Firstly, optimal patient selection criteria within the MET-altered population require refinement, especially regarding MET amplification levels. Secondly, acquired resistance mechanisms to Tepotinib need systematic investigation to inform sequential therapy strategies. Thirdly, integrating Tepotinib into earlier therapy lines and combinations with emerging modalities, such as immunotherapy, warrants exploration. Lastly, comparative studies with other MET inhibitors would further contextualize Tepotinib’s position among MET-targeted therapies.
Several limitations must be acknowledged. Firstly, the predominance of single-arm studies and the absence of randomized controlled trials prevent direct efficacy comparisons and may introduce confounding biases. Secondly, the inclusion of both prospective and retrospective study designs, while intended to synthesize all available evidence, may introduce additional confounding. However, sensitivity analyses excluding the retrospective study demonstrated robustness of the pooled estimates. Thirdly, the included studies did not systematically report coexisting genetic alterations, particularly whether patients with METex14 mutations also harbored concurrent MET amplification. Consequently, we were unable to perform subgroup analyses to evaluate the potential prognostic and predictive impact of such co‑alterations. Fourthly, limited subgroup sizes, particularly for combination therapy and MET amplification cohorts, restrict statistical power. Fifthly, variations in MET amplification testing methods and thresholds across studies may introduce misclassification bias. Finally, limited patient-level data reporting precluded deeper analyses of potential effect modifiers.
In conclusion, this meta-analysis consolidates Tepotinib as a cornerstone therapy for MET-altered NSCLC, demonstrating consistent efficacy regardless of the alteration type. The significant progression-free survival benefit observed with combination therapy highlights its potential to enhance response durability, warranting validation in prospective randomized controlled trials. These results should inform clinical guidelines to promote comprehensive MET testing and position Tepotinib as a key therapeutic option, both as monotherapy and in rational combinations.
Materials and methods
This study was prospectively registered in the PROSPERO database (CRD420251013134), and strict adherence was made to PRISMA criteria during planning of studies, execution, and preparation of manuscript31.
Literature retrieval
A comprehensive literature search was performed using electronic databases and manual screening. Two independent reviewers (JYX and QYC) thoroughly searched the PubMed, EMBASE, Web of Science, and Cochrane Library libraries. Searches were conducted with combinations of “non-small-cell lung cancer” and “MET dysregulation”, as well as “Tepotinib”. This literature search was finalized on March 20, 2025, and further information on the exact search methodology may be obtained from Supplementary Table S1.
Eligibility criteria
Inclusion criteria for studies were clinical studies reported in English that met the following explicit requirements: (1) patients with histologically proven locally advanced or metastatic NSCLC with dysregulation of the MET signaling pathway; (2) treatment with Tepotinib; (3) objective response rate (ORR) expressed, with specific definition as the proportion of patients with complete or partial responses by RECIST criteria version 1.132; and (4) AEs graded according to investigator recording with the National Cancer Institute’s Common Terminology Criteria for Adverse Events. Abstract-only articles were excluded from this systematic review.
Study selection and data extraction
Two independent reviewers (QYC and JYX) conducted literature searching, initial screening, and subsequent data extraction. Disputes during the course were addressed by discussion and agreement. Initial screening of studies was conducted by scanning titles and abstracts of articles with predefined criteria, with subsequent detailed assessments of full text conducted to validate eligibility. Data extracted from studies were (1) first author surname; (2) year of publication; (3) study design; (4) baseline patient characteristics such as number of participants, MET dysregulation categories, gender distribution, and age; (5) treatment received details (dosage, administration schedule, and regimen detail); (6) Eastern Cooperative Oncology Group performance status (ECOG PS); (7) clinical effectiveness outcomes; and (8) occurring AEs. Some studies29,32,33,34 reported results separately for two genetically different patient groups, allowing for subgroup analyses; as such, each group was independently analyzed. All other studies that were included were portrayed as a single dataset.
Quality assessment
Quality appraisal for non-randomized studies was performed using the Methodological Index for Non-randomized Studies (MINORS) scale35. The single included randomized controlled trial underwent bias evaluation employing the Cochrane Risk of Bias Tool (RoB 2)36,37.
Statistical analysis
Patient demographics, efficacy outcomes, and adverse event data extracted from selected studies underwent comprehensive statistical evaluation. Weighted mean proportions (e.g., for ORR and DCR) were calculated using inverse-variance weighting within random- or fixed-effects meta-analysis models in NSCLC patients with MET pathway dysregulation and presented with corresponding 95% confidence intervals (95% CI). Study heterogeneity was assessed statistically using the chi-square test (Q statistic) and quantified through the I² statistic, interpreted as follows: minimal (≤ 25%), mild (26–50%), moderate (51–75%), or substantial (> 75%). In cases where significant heterogeneity (p < 0.1 or I2 > 50%) was observed, random-effects models were utilized; otherwise, fixed-effects models were applied38. Subgroup analyses were further performed based on the type of MET alteration and the therapeutic approach (monotherapy vs. combination therapy). Sensitivity analyses involved the sequential exclusion of studies contributing notably to heterogeneity. The overall safety profile was evaluated by synthesizing reported AEs across studies. Meta-analytic calculation of raw proportions employed logit transformations, with an added continuity correction (0.5) applied to studies reporting zero events. All statistical computations were executed using R statistical software (version 4.5.0, R Foundation for Statistical Computing, Vienna, Austria; https://www.R-project.org/), specifically the meta package (version 4.5.0).
Data availability
All data supporting the findings are included in the manuscript and supplementary files. Extracted data for the meta-analysis are available from the corresponding author upon reasonable request.
References
Bray, F. et al. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 74, 229–263. https://doi.org/10.3322/caac.21834 (2024).
WHO Lung cancer. World Health Organization. (2023).
Imyanitov, E. N., Iyevleva, A. G. & Levchenko, E. V. Molecular testing and targeted therapy for non-small cell lung cancer: Current status and perspectives. Crit. Rev. Oncol. Hematol. 157, 103194. https://doi.org/10.1016/j.critrevonc.2020.103194 (2021).
Duma, N., Santana-Davila, R. & Molina, J. R. Non-small cell lung cancer: epidemiology, screening, diagnosis, and treatment. Mayo. Clin. Proc. 94, 1623–1640. https://doi.org/10.1016/j.mayocp.2019.01.013 (2019).
Hendriks, L. E. et al. Oncogene-addicted metastatic non-small-cell lung cancer: ESMO Clinical Practice Guideline for diagnosis, treatment and follow-up. Ann. Oncol. 34, 339–357. https://doi.org/10.1016/j.annonc.2022.12.009 (2023).
Rami-Porta, R. et al. Members of the IASLC Staging and Prognostic Factors Committee and of the Advisory Boards, and Participating Institutions. The International Association for the Study of Lung Cancer Lung Cancer Staging Project: Proposals for Revision of the TNM Stage Groups in the Forthcoming (Ninth) Edition of the TNM Classification for Lung Cancer. J. Thorac. Oncol. 19, 1007–1027. https://doi.org/10.1016/j.jtho.2024.02.011 (2024).
Chen, Z., Fillmore, C. M., Hammerman, P. S., Kim, C. F. & Wong, K. K. Non-small-cell lung cancers: a heterogeneous set of diseases. Nat. Rev. Cancer. 14, 535–546. https://doi.org/10.1038/nrc3775 (2014).
Cardarella, S. et al. The introduction of systematic genomic testing for patients with non-small-cell lung cancer. J. Thorac. Oncol. 7, 1767–1774. https://doi.org/10.1097/JTO.0b013e3182745bcb (2012).
Pao, W. & Girard, N. New driver mutations in non-small-cell lung cancer. Lancet Oncol. 12, 175–180. https://doi.org/10.1016/S1470-2045(10)70087-5 (2011).
Chagas, G. C. L., Rangel, A. R. & El Osta, B. MET alterations in advanced non-small cell lung cancer. Curr. Probl. Cancer. 49, 101075. https://doi.org/10.1016/j.currproblcancer.2024.101075 (2024).
Frampton, G. M. et al. Activation of MET via diverse exon 14 splicing alterations occurs in multiple tumor types and confers clinical sensitivity to MET inhibitors. Cancer Discov. 5, 850–859. https://doi.org/10.1158/2159-8290.CD-15-0285 (2015).
Awad, M. M. et al. MET Exon 14 Mutations in Non-Small-Cell Lung Cancer Are Associated With Advanced Age and Stage-Dependent MET Genomic Amplification and c-Met Overexpression. J. Clin. Oncol. 34, 721–730. https://doi.org/10.1200/JCO.2015.63.4600 (2016).
Engelman, J. A. & Jänne, P. A. Mechanisms of acquired resistance to epidermal growth factor receptor tyrosine kinase inhibitors in non-small cell lung cancer. Clin. Cancer Res. 14, 2895–2899. https://doi.org/10.1158/1078-0432.CCR-07-2248 (2008).
Peters, S. & Adjei, A. A. MET: a promising anticancer therapeutic target. Nat. Rev. Clin. Oncol. 9, 314-326. https://doi.org/10.1038/nrclinonc.2012.71 (2012).
Remon, J. et al. MET alterations in NSCLC-Current Perspectives and Future Challenges. J. Thorac. Oncol. 18, 419–435. https://doi.org/10.1016/j.jtho.2022.10.015 (2023).
Schrock, A. B. et al. Characterization of 298 Patients with Lung Cancer Harboring MET Exon 14 Skipping Alterations. J. Thorac. Oncol. 11, 1493–1502. https://doi.org/10.1016/j.jtho.2016.06.004 (2016).
Turke, A. B. et al. Preexistence and clonal selection of MET amplification in EGFR mutant NSCLC. Cancer Cell. 17, 77–88. https://doi.org/10.1016/j.ccr.2009.11.022 (2010).
Yang, J. J. et al. A phase Ib study of the highly selective MET-TKI savolitinib plus gefitinib in patients with EGFR-mutated, MET-amplified advanced non-small-cell lung cancer. Invest. New. Drugs. 39, 477–487. https://doi.org/10.1007/s10637-020-01010-4 (2021).
Wu, Y. L. et al. Tepotinib plus gefitinib in patients with EGFR-mutant non-small-cell lung cancer with MET overexpression or MET amplification and acquired resistance to previous EGFR inhibitor (INSIGHT study): an open-label, phase 1b/2, multicentre, randomised trial. Lancet Respir Med. 8, 1132–1143. https://doi.org/10.1016/S2213-2600(20)30154-5 (2020).
Spigel, D. R. et al. Randomized phase II trial of Onartuzumab in combination with erlotinib in patients with advanced non-small-cell lung cancer. J. Clin. Oncol. 31, 4105–4114. https://doi.org/10.1200/JCO.2012.47.4189 (2013).
Passaro, A. et al. Amivantamab plus chemotherapy with and without lazertinib in EGFR-mutant advanced NSCLC after disease progression on osimertinib: primary results from the phase III MARIPOSA-2 study. Ann. Oncol. 35, 77–90. https://doi.org/10.1016/j.annonc.2023.10.117 (2024).
Horinouchi, H. et al. Results from a phase Ib study of telisotuzumab vedotin in combination with osimertinib in patients with c-Met protein-overexpressing, EGFR-mutated locally advanced/metastatic non-small-cell lung cancer (NSCLC) after progression on prior osimertinib. Ann. Oncol. 36, 583–591. https://doi.org/10.1016/j.annonc.2025.01.001 (2025).
Drilon, A. et al. Antitumor activity of crizotinib in lung cancers harboring a MET exon 14 alteration. Nat. Med. 26, 47–51. https://doi.org/10.1038/s41591-019-0716-8 (2020).
Angevin, E. et al. A first-in-human phase I study of SAR125844, a selective MET tyrosine kinase inhibitor, in patients with advanced solid tumours with MET amplification. Eur. J. Cancer. 87, 131–139. https://doi.org/10.1016/j.ejca.2017.10.016 (2017).
Fujino, T. et al. Sensitivity and Resistance of MET Exon 14 Mutations in Lung Cancer to Eight MET Tyrosine Kinase Inhibitors In Vitro. J. Thorac. Oncol. 14, 1753–1765. https://doi.org/10.1016/j.jtho.2019.06.023 (2019).
Mo, H. N. & Liu, P. Targeting MET in cancer therapy. Chronic Dis. Transl Med. 3, 148–153. https://doi.org/10.1016/j.cdtm.2017.06.002 (2017).
Bazhenova, L. et al. Therapy for Stage IV Non-Small Cell Lung Cancer With Driver Alterations: ASCO Living Guideline, Version 2024.2. J. Clin. Oncol. 42, e72–e86. https://doi.org/10.1200/JCO-24-02133 (2024).
Markham, A. & Tepotinib First Approval Drugs 80, 829–833. https://doi.org/10.1007/s40265-020-01317-9 (2020).
Mazieres, J. et al. Tepotinib Treatment in Patients With MET Exon 14-Skipping Non-Small Cell Lung Cancer: Long-term Follow-up of the VISION Phase 2 Nonrandomized Clinical Trial. JAMA Oncol. 9, 1260–1266. https://doi.org/10.1001/jamaoncol.2023.1962 (2023).
Park, K. et al. 62O - Tepotinib in NSCLC patients harboring METex14 skipping: Cohort A of phase II VISION study. Ann. Oncol. 30, ix22–ix23. https://doi.org/10.1093/annonc/mdz420.001 (2019).
Page, M. J. et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ 372, n71. https://doi.org/10.1136/bmj.n71 (2021).
Eisenhauer, E. A. et al. New response evaluation criteria in solid tumours: revised RECIST guideline (version 1.1). Eur. J. Cancer. 45, 228–247. https://doi.org/10.1016/j.ejca.2008.10.026 (2009).
Kang, E. J. et al. A phase II study of Tepotinib in patients with advanced solid cancers harboring MET exon 14 skipping mutations or amplification (KCSG AL19-17). ESMO Open. 9, 103668. https://doi.org/10.1016/j.esmoop.2024.103668 (2024).
Wu, Y. L. et al. Tepotinib plus osimertinib in patients with EGFR-mutated non-small-cell lung cancer with MET amplification following progression on first-line osimertinib (INSIGHT 2): a multicentre, open-label, phase 2 trial. Lancet Oncol. 25, 989–1002. https://doi.org/10.1016/S1470-2045(24)00270-5 (2024).
Slim, K. et al. Methodological index for non-randomized studies (minors): development and validation of a new instrument. ANZ J. Surg. 73, 712–716. https://doi.org/10.1046/j.1445-2197.2003.02748.x (2003).
Liam, C. K. et al. Randomized Trial of Tepotinib Plus Gefitinib versus Chemotherapy in EGFR-Mutant NSCLC with EGFR Inhibitor Resistance Due to MET Amplification: INSIGHT Final Analysis. Clin. Cancer Res. 29, 1879–1886. https://doi.org/10.1158/1078-0432.CCR-22-3318 (2023).
Sterne, J. A. C. et al. RoB 2: a revised tool for assessing risk of bias in randomised trials. BMJ 366, l4898. https://doi.org/10.1136/bmj.l4898 (2019).
Higgins, J. P., Thompson, S. G., Deeks, J. J. & Altman, D. G. Measuring inconsistency in meta-analyses. BMJ 327, 557–560. https://doi.org/10.1136/bmj.327.7414.557 (2003).
Le, X. et al. Tepotinib in patients with non-small cell lung cancer with high-level MET amplification detected by liquid biopsy: VISION Cohort B. Cell. Rep. Med. 4, 101280. https://doi.org/10.1016/j.xcrm.2023.101280 (2023).
Reale, M. L. et al. MET exon 14 skipping mutations in non-small-cell lung cancer: real-world data from the Italian biomarker ATLAS database. ESMO Open. 9, 103680. https://doi.org/10.1016/j.esmoop.2024.103680 (2024).
Wolf, J. et al. Capmatinib in MET exon 14-mutated non-small-cell lung cancer: final results from the open-label, phase 2 GEOMETRY mono-1 trial. Lancet Oncol. 25, 1357–1370. https://doi.org/10.1016/S1470-2045(24)00441-8 (2024).
Wolf, J. et al. Capmatinib in MET Exon 14-Mutated or MET-Amplified Non-Small-Cell Lung Cancer. N Engl. J. Med. 383, 944–957. https://doi.org/10.1056/NEJMoa2002787 (2020).
Eser, P. Ö. et al. Oncogenic switch and single-agent MET inhibitor sensitivity in a subset of EGFR-mutant lung cancer. Sci. Transl Med. 13, eabb3738. https://doi.org/10.1126/scitranslmed.abb3738 (2021).
Morgillo, F., Della Corte, C. M., Fasano, M. & Ciardiello, F. Mechanisms of resistance to EGFR-targeted drugs: lung cancer. ESMO Open. 1, e000060. https://doi.org/10.1136/esmoopen-2016-000060 (2016).
Salgia, R., Sattler, M., Scheele, J., Stroh, C. & Felip, E. The promise of selective MET inhibitors in non-small cell lung cancer with MET exon 14 skipping. Cancer Treat. Rev. 87, 102022. https://doi.org/10.1016/j.ctrv.2020.102022 (2020).
Funding
The work was supported by the Natural Science Foundation of Gansu Province [grant number 25JRRA588]; the Gansu Health Industry Scientific Research Program [grant number GSWSKY2021-061]; and Lanzhou University Second Hospital’s Cuiying Scientific Training Program for Undergraduates [grant numbers CYXZ2022-35 and CYXZ2023-23].
Author information
Authors and Affiliations
Contributions
Conception and design: JYX and QYC. Acquisition of data: JYX and XYL. Critical revision of the manuscript for important intellectual content: JYX, DGZ, and QYC. Statistical analysis: JYX and QYC. Obtain funding: DGZ. All authors contributed to the article and approved the submitted version.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Xiao, J., Cai, Q., Li, X. et al. Efficacy and safety of tepotinib in MET‑altered non‑small cell lung cancer: a meta-analysis. Sci Rep 16, 11256 (2026). https://doi.org/10.1038/s41598-026-41989-z
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-026-41989-z
