
Abstract
High-risk non-muscle invasive bladder cancer (HR-NMIBC) presents a significant therapeutic challenge due to its high recurrence and progression rates, particularly in patients with human epidermal growth factor receptor 2 (HER2) expression who are unresponsive to or ineligible for Bacillus Calmette–Guérin (BCG) therapy. This study aimed to evaluate the efficacy and safety of the HER2-targeted antibody-drug conjugate (ADC), Disitamab Vedotin (RC48), alone or in combination with PD-1 inhibitors, as a systemic bladder-sparing approach in a real-world HR-NMIBC cohort. We conducted a multicenter, retrospective, real-world study involving 32 patients with HR-NMIBC who received RC48 alone (n = 3) or in combination with PD-1 inhibitors (n = 29) between June 2022 and December 2024. Eligibility criteria included BCG-unresponsive (n = 7) or BCG-ineligible (n = 25). Data were collected on demographics, clinical characteristics, treatment responses, and adverse events. The primary endpoint was complete response rate (CRR). Secondary endpoints included event-free survival (EFS), duration of complete response (DoCR), 6-month bladder preservation rate, and safety. At a median follow-up of 13.3 months, the overall CRR was 71.9% (23/32; 95% CI: 53.3%–86.3%). In the BCG-unresponsive and BCG-ineligible subgroups, CRRs were 85.7% (6/7) and 68.0% (17/25), respectively. The median EFS for the overall cohort was 22.1 months (95% CI: 16.7–27.4), with no significant difference between the BCG subgroups (P = 0.98). Among the 23 responders, the median DoCR was 16.9 months (95% CI: 13.1–20.7). Treatment-related adverse events (TRAEs) occurred in 53.1% of patients, primarily Grade 1–2 peripheral neuropathy (21.9%) and rash (21.9%). Grade ≥ 3 TRAEs were rare (6.3%). In this real-world study, RC48-based systemic therapy, particularly in combination with PD-1 inhibitors, demonstrates promising preliminary activity and a manageable safety profile in BCG-unresponsive or BCG-ineligible HR-NMIBC. Large prospective trials are required to confirm long-term durability and the optimal role of this systemic approach.
Similar content being viewed by others

Introduction
Bladder cancer is a significant global health concern, with non-muscle invasive bladder cancer (NMIBC) accounting for 75%-80% of newly diagnosed cases, among which high-risk NMIBC (HR-NMIBC) represents a significant clinical challenge due to its high recurrence and progression rates1. Bacillus Calmette-Guérin (BCG) intravesical therapy following transurethral resection of bladder tumors (TURBT) remains the standard of care (SOC) for HR-NMIBC. However, many patients either fail to respond to BCG or experience recurrence after initial treatment, especially in patients with human epidermal growth factor receptor 2 (HER2) overexpression, where the efficacy of BCG is significantly reduced, leaving radical cystectomy (RC) as the next line of treatment2,3. This highlights the urgency of developing effective and well-tolerated alternative bladder-sparing therapies for patients with HER2-expression HR-NMIBC.
Immunotherapy has emerged as a pivotal strategy in this paradigm, with PD-1/PD-L1 inhibitors demonstrating durable responses in HR-NMIBC patients. The phase II KEYNOTE-057 trial evaluated pembrolizumab monotherapy in patients with HR-NMIBC and reported a complete response rate of 41% at 3 months4. These findings led to FDA approval of pembrolizumab for BCG-unresponsive NMIBC with carcinoma in situ (CIS) in patients ineligible for or refusing cystectomy, representing a landmark shift toward systemic immunotherapy in early-stage bladder cancer. Additional trials, such as SWOG S1605 (atezolizumab) and NCT03528694 (durvalumab), have further supported the feasibility of immune checkpoint blockade in this context5,6. However, monotherapy yields limited complete response (CR) rates, and durability of response remains suboptimal in a significant subset. Therefore, combinatorial strategies are being actively explored to enhance treatment efficacy.
Disitamab Vedotin (RC48), a novel HER2-targeting ADC, induces tumor cell cycle arrest and apoptosis by delivering monomethyl auristatin E (MMAE) intracellularly, and additionally exerts a bystander effect through MMAE diffusion into the tumor microenvironment, affecting adjacent cells, even with low or heterogeneous HER2 expression7. Clinical trials have demonstrated the promising efficacy and manageable toxicity of RC48 alone or combined with PD-1 inhibitors in HER2-overexpressing advanced urothelial carcinoma (UC)8,9. However, despite these encouraging results in advanced disease, evidence supporting the use of RC48 alone or in combination with PD-1 inhibitors for HR-NMIBC is still lacking, and existing trials evaluating systemic therapies in this setting are limited by strict eligibility criteria, relatively small sample sizes, and artificial trial conditions10. In this context, we conducted a multicenter, real-world study to assess the efficacy and safety of RC48, alone or in combination with PD-1 inhibitors, in patients with HR-NMIBC, aiming to provide practical evidence supporting systemic, bladder-sparing strategies for this underserved patient group.
Methods
Study design and patients
This is a multicenter, retrospective, real-world study conducted across Peking University First Hospital and Peking University First Hospital Daxing District, Beijing, China. We included patients diagnosed with HR-NMIBC who received RC48 monotherapy or RC48 in combination with PD-1 inhibitors as bladder-sparing therapy between June 2022 and December 2024. HR-NMIBC was defined according to the European Association of Urology (EAU) 2024 guidelines11, including any of the following: high-grade Ta, T1, or CIS; multifocal tumors; or presence of lymphovascular invasion or variant histology.
Eligible patients were aged ≥ 18 years, histologically diagnosed with urothelial carcinoma, had HER2-positive expression (defined as Immunohistochemical [IHC] 1+, 2 + or 3+), and refused or were ineligible for radical cystectomy. Patients were classified as either BCG-unresponsive or BCG-ineligible according to the prior BCG treatment. Patients classified as BCG-unresponsive had received adequate BCG induction and maintenance therapy according to the EAU and International Bladder Cancer Group (IBCG) guidelines and no further BCG retreatment was administered after confirmation of BCG-unresponsive. Prior to initiation of RC48-based therapy, all patients underwent repeated TURBTs to reassess disease status, and persistent high-grade non–muscle-invasive disease was confirmed histologically. RC48, with or without PD-1 inhibitors, was subsequently administered after confirmation of ongoing high-risk disease. No other intravesical or systemic antitumor therapies were administered between BCG failure and the initiation of RC48-based treatment12,13. And BCG-ineligible patients were defined as those who were unable to receive intravesical BCG due to clinical contraindications, refusal of BCG therapy because of significant comorbidities or poor tolerance, or regional shortages of BCG14.
All patients received systemic RC48 ± PD-1 inhibitor as part of bladder-sparing therapy after maximal TURBT. RC48 was administered intravenously at a dose of 2.0 mg/kg every 2 or 3 weeks (Q2W and Q3W), and PD-1 inhibitors (pembrolizumab, toripalimab, tislelizumab) were given per standard dosing schedules. The choice of treatment (monotherapy or combination) was based on physician judgment and patient preference. In the combination group, patients received combination therapy for four to six cycles followed by PD-1 inhibitor monotherapy as maintenance. As for the monotherapy group, patients received RC48 alone for a total of six cycles. Patients with muscle-invasive disease, metastatic UC, or other concurrent malignancies were excluded.
The study protocol was approved by the Ethics Committee of Peking University First Hospital (Approval No.: 2025R0556) and conducted in accordance with the Declaration of Helsinki. The requirement for informed consent was waived by the ethics committee given the participants could not be contacted due to the retrospective design.
Data collection and effectiveness evaluation
Clinical data were retrospectively collected, including patient demographics, tumor stage and grade, HER2 status (IHC), prior therapy, details of RC48-based treatment regimens, disease progression, and treatment-related adverse events. HER2 expression was assessed by immunohistochemistry in local certified pathology laboratories. Expression levels were classified into 0, 1+, 2+, or 3+, with 2+/3 + considered HER2-positive, and 1 + considered HER2-low, following previous RC48 trials8.
The primary endpoint was the complete response rate (CRR), which was the proportion of patients achieving a complete response (CR), defined as negative cystoscopy, urine cytology, and imaging (CT or MRI) as assessed by the treating physician, within 12 months after the first dose of treatment. Secondary endpoints included event-free survival (EFS), durability of complete response (DoCR), 6-month bladder preservation rate, and safety. EFS was defined as the time from treatment initiation to the first occurrence of high-grade recurrence, progression to muscle-invasive disease, cystectomy, or death from any cause. For the assessment of disease course, progressive disease (PD) was defined as the development of muscle-invasive disease, an increase in T-stage, or the occurrence of nodal/distant metastasis or upper tract disease according to the IBCG criteria15. DoCR was defined as the time from first observed complete response to documented high-grade recurrence, progression, or death in HR-NMIBC patients who achieved CR. Safety was assessed by the incidence and severity of adverse events according to Common Terminology Criteria for Adverse Events (CTCAE) version 5.0.
Statistical analysis
Descriptive statistics were used to summarize baseline characteristics, treatment details and safety outcomes. CRR was calculated with 95% confidence intervals. EFS were estimated using the Kaplan-Meier method, and differences between treatment groups were assessed using the log-rank test. Cox proportional hazards regression was used to identify factors associated with EFS. Among patients who achieved CR, DoCR was also estimated using the Kaplan–Meier method. All statistical analyses were performed using R (version 4.3.2) or SPSS (version 26.0). A two-sided p-value of < 0.05 was considered statistically significant.
Results
Baseline patient characteristics
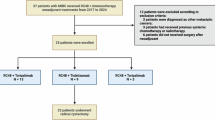
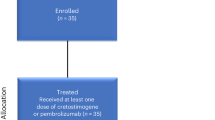
A total of 32 patients with HR-NMIBC from 2 centers were included, with 3 patients receiving RC48 monotherapy and 29 patients receiving RC48 + PD-1 inhibitor combination therapy, including toripalimab (n = 19), tislelizumab (n = 7) and pembrolizumab (n = 3). Of the three patients who received RC48 monotherapy, two were treated without PD-1 inhibitors because of contraindications to immunotherapy, and one due to a history of immune-related adverse events. The median age was 66 years (range: 37–89), with 56.3% of patients aged ≥ 65 years. The majority of patients were male (81.3%) and had an ECOG performance status of 0 (81.3%). A history of smoking was reported in 28.1% of cases. Regarding prior treatment, 7 patients (21.9%) were classified as BCG-unresponsive, while the other 25 patients (78.1%) were BCG-ineligible. Among the 25 patients classified as BCG-ineligible, five were unable to receive intravesical BCG because of clinical contraindications, four declined BCG therapy after adequate counseling due to concerns regarding tolerance or comorbidities, and the remaining sixteen did not receive BCG due to regional shortages of BCG during the study period.
For tumor characteristics, the majority were diagnosed with T1 stage tumors (87.5%), followed by Ta (6.3%) and CIS (6.3%). Histologically, 100% were high-grade urothelial carcinoma, while others included sarcomatoid differentiation (3.1%) and lymphovascular invasion (3.1%). With respect to HER2 expression levels, two patients (6.3%) had HER2 1 + status, 11 patients (34.4%) had HER2 2 + status, and 19 patient (59.4%) had HER2 3 + status. Detailed patient characteristics were shown in Table 1.
Efficacy outcomes
With a median follow-up time of 13.3 months, the CRR was 71.9% in the overall cohort, with 23 patients achieving CR. Subgroup analyses by prior BCG status were conducted to evaluate the efficacy across different clinical groups. Among patients in the BCG-unresponsive subgroup (n = 7), the CRR reached 85.7% (6/7). In the BCG-ineligible subgroup (n = 25), the CRR was 68.0% (17/25). When stratified by treatment regimens, the CRR was 100% (3/3) in patients receiving RC48 monotherapy and 69.0% (20/29) in patients receiving RC48 combined with PD-1 inhibitors as shown in Table 2. Among patients receiving different RC48 dosing schedules, the CRR in the Q2W group was 66.7% (10/15) versus 76.5% (13/17) in the Q3W group. Regarding immune checkpoint inhibitors, the CRRs were 73.7% (14/19), 57.1% (4/7), and 66.7% (2/3) in patients treated with toripalimab, tislelizumab, and pembrolizumab, respectively.
Regarding survival outcomes, the median EFS (mEFS) in the overall population was 22.1 months (95% confidence interval [CI]: 16.7–27.4) as shown in Fig. 1. The mEFS was 10.86 months for the BCG-unresponsive group and 22.0 months for the BCG-ineligible group (HR = 0.98, 95% CI 0.21–4.63, P = 0.98). Patients treated with RC48 plus PD-1 inhibitors exhibited a mEFS of 21.3 months (95%CI: 15.7–26.8), and no events were observed during the follow-up period in the RC48 monotherapy, with the mEFS not reached. Stratified by dosing regimen, mEFS in the RC48 Q2W group was 12.8 months versus 22.7 months in the Q3W group (HR = 0.92, 95% CI 0.27–3.20, P = 0.89). Among different immune checkpoint inhibitors, mEFS was the longest in the tislelizumab group (20.3 months), followed by the toripalimab group (19.2 months) and the pembrolizumab group (10.3 months). The swimming plot for all patients was depicted in Fig. 2.

Event-free survival (EFS) of all patients (A). EFS of patients regarding prior BCG treatment (B). EFS of patients receiving alone or combined with PD-1 inhibitors (C). EFS of patients receiving RC48 every 2 weeks versus every 3 weeks (D).

Swimmer plot for patients who have different treatment regimens.
Among the 23 patients who achieved complete response at 3 months, duration of complete response was evaluable in all patients. At the time of data cutoff, the median DoCR was 16.90 months (95%CI: 13.07–20.73), with 7.50 months (95%CI: 3.53–11.47) in the BCG-unresponsive group and 17.55 months (13.36–21.74) in the BCG-ineligible group (Table 2). The estimated 6-month CR durability rate was 50.0%, and 9 patients remained in complete response at 12 months. The bladder preservation rate at 6 months was 71.9% (23/32), with most responders maintaining durable responses without requiring radical cystectomy. Among the 9 patients who eventually underwent radical cystectomy due to local progression or patient preference, pathological downstaging was observed in 7 (77.8%) patients, including 6 patients with pathological CR (pCR, ypT0), and 3 patients with non–muscle-invasive disease (≤ ypT1). Specially, one patient (3.1%) experienced PD, who was initially diagnosed with T1 stage high-grade disease and experienced progression to muscle-invasive bladder cancer (T2) at the 10-month follow-up.
Safety profiles
The safety profile of RC48-based treatment is summarized in Table 3. Treatment-related adverse events (TRAEs) occurred in 53.1% (17/32) of patients (any grade), with grade ≥ 3 TRAEs in 6.3% (2/32). The most common TRAEs were peripheral neuropathy (21.9%, all grade 1–2), rash (21.9%, 1 patient grade ≥ 3), and elevated transaminases (12.5%). Patients in the combination group reported two cases of immune-related pneumonitis, with 1 patient experienced grade ≥ 3 AEs. Most AEs were manageable with supportive care or dose adjustment, and no new safety signals were identified compared to previous RC48 trials8,9. No treatment-related deaths were reported.
Exploratory biomarker analysis
To explore potential predictive biomarkers for response to RC48-based therapy, we conducted subgroup analyses according to HER2 expression levels. Patients with HER2-positive (IHC 3 + or IHC 2+) demonstrated a higher CRR compared to patients with low HER2 expression (IHC 1+), while patients with HER2 3 + demonstrated the highest CRR, reaching 84.2% (16/19), compared to 54.5% (6/11) in HER2 2 + and 50% (1/2) in HER2 1 + groups. In addition, we investigated the dynamic change of HER2 status before and after RC48 combination therapy in patients receiving radical cystectomy with paired tumor tissue samples available. IHC analyses revealed that HER2 expression was heterogeneous and subject to alteration after systemic treatment. In a patient undergoing TURBT, HER2 expression was detected as 3 + on pathological examination. After 4 cycles of RC48 combined with ICIs, subsequent IHC staining of cystectomy pathological specimens revealed HER2 1 + and this patient achieved pPR (Fig. 3).

Radiographic imaging and HER2 immunohistochemical (IHC) staining of Patient 20. The left panel shows the bladder tumor and HER2 expressing before treatment. The right panel shows the bladder tumor after 4 cycles of RC48 combined with PD-1 inhibitors and the status of HER2 expressing after radical cystectomy.
Discussion
This multicenter real-world study demonstrates that systemic therapy of RC48, alone or combined with PD-1 inhibitors, achieves compelling efficacy in HER2-expressing HR-NMIBC, with an CRR of 71.9% and a mEFS of 22.1 months. Meanwhile, the incidence of TRAEs was observed to be manageable and within an acceptable safety profile.
RC48 has demonstrated promising antitumor efficacy both as monotherapy and in combination with PD‑1 inhibitors across clinical settings of urothelial carcinoma. In the RC48‑C005 and RC48‑C009 phase II trials involving patients with HER2-positive locally advanced or metastatic urothelial carcinoma (la/mUC) refractory to prior therapies, RC48 monotherapy achieved an objective response rate (ORR) of approximately 50.5%, with a median progression-free survival (PFS) of 5.9 months and a median overall survival (OS) of 14.2 months, while maintaining a manageable toxicity profile8. Building on that, the RC48‑C014 phase Ib/II study combined RC48 with toripalimab in la/mUC, yielding an ORR of 73.2% and demonstrating a favorable safety profile suggestive of synergistic activity between the ADC and PD‑1 inhibitors9. More recently, RC48 has also shown potential in HR-NMIBC; early data from intravesical instillation in patients with HER-2 expressing HR-NMIBC reported encouraging response rates and acceptable tolerability16,17. These findings collectively validate the therapeutic value of RC48-based treatment in various stages of bladder cancer.
Bladder-sparing strategies for HR-NMIBC have long focused on BCG therapy as the SOC. However, a considerable proportion of patients are either unresponsive to or intolerant of BCG, together with the internationally known shortage of BCG, prompting exploration of alternative approaches18. Recent studies have investigated immune checkpoint inhibitors such as pembrolizumab and novel intravesical agents including nadofaragene firadenovec (NFF), yet their response durability and toxicity profiles remain areas of concern19,20. In this context, the IBCG has recommended gemcitabine/docetaxel (GEM/DOCE), nadofaragene firadenovec (NFF), and nogapendekin alfa inbakicept-pmln (NAI) + BCG for BCG-Unresponsive NMIBC patients13. While the KEYNOTE-057 trial demonstrated the potential of pembrolizumab monotherapy in BCG-unresponsive NMIBC, response rates remain modest and many patients eventually require cystectomy4. Due to its systemic toxicity, IBCG suggested that pembrolizumab should only be offered after other options failed13. In this study, RC48 alone or in combination with PD-1 inhibitors showed favorable antitumor activity in patients with HR-NMIBC, with a CRR of 71.9% (23/32) in the overall cohort. These findings align with the mechanistic rationale that RC48-mediated immunogenic cell death may enhance antigen presentation and potentiate T cell–mediated responses when combined with PD-1/PD-L1 inhibitors21,22. Subgroup analyses stratified by prior BCG status demonstrated a CRR of 85.7% (6/7) in the BCG-unresponsive subgroup (n = 7) and 68.0% in the BCG-ineligible subgroup, with a median EFS of 10.86 months and 22.0 months, respectively. Importantly, patients with BCG-unresponsive disease and those who are BCG-ineligible represent clinically distinct populations with substantially different baseline characteristics, treatment histories, and expected outcomes. In our cohort, BCG-unresponsive patients had previously received adequate BCG therapy and exhibited biological resistance, which is typically associated with an increased risk of early recurrence and disease progression. In contrast, BCG-ineligible patients were unable to undergo BCG treatment due to clinical contraindications, patient refusal, or regional BCG shortages. Consequently, this group should not be regarded as truly BCG-naïve in a trial-based sense, but rather reflects a real-world population for whom standard intravesical therapy was not feasible. Besides, although RC48-based regimens demonstrated encouraging antitumor activity in this real-world cohort, these findings should be interpreted with caution. Notably, only three patients received RC48 monotherapy, which substantially limits the interpretability of outcomes in this subgroup. Therefore, the response rates observed in patients treated with RC48 in combination with PD-1 inhibitors should not be extrapolated to RC48 monotherapy, as any potential efficacy signal may be obscured by the very small sample size.
An important aspect of our study is the exploratory evaluation of HER2 status in the context of RC48-based therapy. We observed an association between HER2 expression levels and short-term treatment response, with higher response rates in patients with IHC 3 + tumors. However, meaningful responses were also observed in patients with lower HER2 expression, which may be related to the bystander effect of RC48 or treatment-related immune activation23. In addition, we explored changes in HER2 expression in a small subset of patients with paired tissue samples before and after treatment. A decrease in HER2 expression was observed in some cases; however, due to the limited sample size and short follow-up duration, no conclusions can be drawn regarding the longitudinal stability of HER2 expression or its role in treatment resistance in NMIBC24,25. Given the retrospective design and limited follow-up, these findings should be interpreted cautiously and primarily reflect short-term clinical activity rather than durable outcomes.
In terms of safety, the most frequently reported adverse events were peripheral neuropathy, rash, and elevated transaminases, which are consistent with the known toxicity profile of antibody–drug conjugates26,27. Peripheral neuropathy occurred in 21.9% of patients; however, all events were limited to grade 1–2 severity and were generally reversible with dose modification or supportive care. Grade ≥ 3 adverse events were observed in two patients, both of whom recovered following appropriate management. The occurrence of systemic toxicities in a localized disease setting highlights an important clinical trade-off between potential bladder preservation and the risk of cumulative or chronic adverse events. Unlike intravesical therapies, which are primarily associated with localized toxicity, systemic RC48-based regimens inherently carry a risk of systemic exposure. Therefore, RC48-based systemic therapy should be reserved for carefully selected HR-NMIBC patients who are unresponsive to or ineligible for BCG therapy, rather than being considered a substitute for standard intravesical therapy in the broader NMIBC population. In addition, immune-related pneumonitis was observed in a small proportion of patients receiving combination therapy, underscoring the need for vigilant monitoring during RC48-based immunotherapy28,29.
Several limitations of this study should be acknowledged. First, the overall sample size was relatively small, particularly in subgroup analyses, and the follow-up duration was limited, which may restrict the robustness of efficacy and durability estimates. Second, the relatively large proportion of BCG-ineligible patients reflects real-world clinical practice, where standard intravesical BCG therapy is frequently precluded by contraindications, patient refusal, or regional BCG shortages. While this enhances the real-world relevance of our findings, it also introduces clinical heterogeneity and limits direct comparisons with trials focusing exclusively on BCG-unresponsive populations. Third, only a small number of patients received RC48 monotherapy, precluding definitive conclusions regarding its standalone efficacy compared with combination therapy. Finally, a substantial proportion of patients underwent radical cystectomy during follow-up, which may have influenced event-free survival outcomes and limited the assessment of long-term bladder preservation. These limitations highlight the need for larger, prospective studies with longer follow-up to further validate the role of RC48-based regimens in distinct NMIBC populations.
Conclusions
In this preliminary real-world study, RC48-based regimens, particularly in combination with PD-1 inhibitors, showed promising clinical activity and acceptable safety in patients with high-risk NMIBC. However, given the limited sample size, the small number of patients receiving RC48 monotherapy, and the relatively short follow-up, these findings should be interpreted with caution. Larger prospective studies are needed to validate these results and to clarify the optimal role of RC48 monotherapy versus combination strategies.
Data availability
The data are available upon request from the corresponding author.
References
Bray, F. et al. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 74 (3), 229–263. https://doi.org/10.3322/caac.21834 (2022).
LenisAT, LecPM, Chamie, K. & MshsMD Bladder Cancer: A Review. Jama 324 (19), 1980–1991. https://doi.org/10.1001/jama.2020.17598 (2020).
Tan, X. et al. Prognostic Significance of HER2 Expression in Patients with Bacillus Calmette-Guérin-exposed Non-muscle-invasive Bladder Cancer. Eur Urol Oncol. ;7(4):760 – 9.10.1016/j.euo.2023.10.003 (2024).
Balar, A. V. et al. Pembrolizumab monotherapy for the treatment of high-risk non-muscle-invasive bladder cancer unresponsive to BCG (KEYNOTE-057): an open-label, single-arm, multicentre, phase 2 study. Lancet Oncol. ;22(7):919 – 30.10.1016/s1470-2045(21)00147-9 (2021).
Black, P. C. et al. Phase 2 Trial of Atezolizumab in Bacillus Calmette-Guérin-unresponsive High-risk Non-muscle-invasive Bladder Cancer: SWOG S1605. Eur Urol. ;84(6):536 – 44.10.1016/j.eururo.2023.08.004 (2023).
Hahn, N. M. et al. A Phase 1 Trial of Durvalumab in Combination with Bacillus Calmette-Guerin (BCG) or External Beam Radiation Therapy in Patients with BCG-unresponsive Non-muscle-Invasive Bladder Cancer: The Hoosier Cancer Research Network GU16-243 ADAPT-BLADDER Study. European Urology. ;83(6):486 – 94.10.1016/j.eururo.2023.01.017 (2023).
Wei, Y. et al. Disitamab vedotin in combination with immune checkpoint inhibitors for locally and locally advanced bladder urothelial carcinoma: a two-center’s real-world study. Front. Pharmacol. 14 https://doi.org/10.3389/fphar.2023.1230395 (2023).
Sheng, X. et al. Efficacy and Safety of Disitamab Vedotin in Patients With Human Epidermal Growth Factor Receptor 2-Positive Locally Advanced or Metastatic Urothelial Carcinoma: A Combined Analysis of Two Phase II Clinical Trials. J Clin Oncol. ;42(12):1391 – 402.10.1200/jco.22.02912 (2024).
Zhou, L. et al. Disitamab vedotin plus toripalimab in patients with locally advanced or metastatic urothelial carcinoma (RC48-C014): a phase Ib/II dose-escalation and dose-expansion study. Ann Oncol. ;36(3):331 – 9.10.1016/j.annonc.2024.12.002 (2025).
Chen, J. et al. Adjuvant or rescue disitamab vedotin (RC48-ADC) for high-risk non-muscle invasive bladder cancer with HER2 overexpression: A phase II multi-center study. Journal of Clinical Oncology. ;42.10.1200/jco.2024.42.16_suppl.tps4625 (2024).
Gontero, P. et al. European Association of Urology Guidelines on Non-muscle-invasive Bladder Cancer (TaT1 and Carcinoma In Situ)-A Summary of the 2024 Guidelines Update. Eur. Urol. 86 (6), 531–549. https://doi.org/10.1016/j.eururo.2024.07.027 (2024).
Gontero, P. et al. European Association of Urology Guidelines on Non–muscle-invasive Bladder Cancer (TaT1 and Carcinoma In Situ)—A Summary of the 2024 Guidelines Update. Eur. Urol. 86 (6), 531–549. https://doi.org/10.1016/j.eururo.2024.07.027 (2024).
Li, R. et al. Bladder-sparing Therapy for Bacillus Calmette-Guérin-unresponsive Non-muscle-invasive Bladder Cancer: International Bladder Cancer Group Recommendations for Optimal Sequencing and Patient Selection. Eur Urol. ;86(6):516 – 27.10.1016/j.eururo.2024.08.001 (2024).
U.S. Food and Drug Administration. Bacillus Calmette-Guérin-Unresponsive Nonmuscle Invasive Bladder Cancer: Developing Drugs and Biological Products for Treatment. (2018).
Lamm, D. et al. Defining progression in nonmuscle invasive bladder cancer: it is time for a new, standard definition. J Urol. ;191(1):20 – 7.10.1016/j.juro.2013.07.102 (2014).
Hong, X. et al. A HER2-targeted Antibody‐Drug Conjugate, RC48‐ADC, Exerted Promising Antitumor Efficacy and Safety with Intravesical Instillation in Preclinical Models of Bladder Cancer. Advanced Science. ;10(32).10.1002/advs.202302377 (2023).
Chen, X. et al. Intravesical Disitamab Vedotin (RC48) for HER2-Expressing High‐Risk Non‐Muscle‐Invasive Bladder Cancer: A Single‐Arm, Dose–Escalation Phase I Trial Study. MedComm 6 (7). https://doi.org/10.1002/mco2.70288 (2025).
Giannarini, G. et al. Urologists, You’ll Never Walk Alone! How Novel Immunotherapy and Modern Imaging May Change the Management of Non-muscle-invasive Bladder Cancer. Eur Urol Oncol. ;5(3):268 – 72.10.1016/j.euo.2021.05.008 (2022).
Li, R. et al. Systematic Review of the Therapeutic Efficacy of Bladder-preserving Treatments for Non-muscle-invasive Bladder Cancer Following Intravesical Bacillus Calmette-Guérin. Eur. Urol. 78 (3), 387–399. https://doi.org/10.1016/j.eururo.2020.02.012 (2020).
Kamat, A. M. et al. Evidence-based Assessment of Current and Emerging Bladder-sparing Therapies for Non-muscle-invasive Bladder Cancer After Bacillus Calmette-Guerin Therapy: A Systematic Review and Meta-analysis. Eur Urol Oncol. ;3(3):318 – 40.10.1016/j.euo.2020.02.006 (2020).
Wu, X. et al. A HER2-targeting antibody-MMAE conjugate RC48 sensitizes immunotherapy in HER2-positive colon cancer by triggering the cGAS-STING pathway. Cell. Death Dis. 14 (8), 550. https://doi.org/10.1038/s41419-023-06073-8 (2023).
Galluzzi, L., Buqué, A., Kepp, O., Zitvogel, L. & Kroemer, G. Immunogenic cell death in cancer and infectious disease. Nat. Rev. Immunol. 17 (2), 97–111. https://doi.org/10.1038/nri.2016.107 (2017).
Wei, Q. et al. Spatiotemporal Quantification of HER2-targeting Antibody-Drug Conjugate Bystander Activity and Enhancement of Solid Tumor Penetration. Clin. Cancer Res. 30 (5), 984– (2024). – 97.10.1158/1078 – 0432.Ccr-23-1725.
Ocaña, A., Amir, E. & Pandiella, A. HER2 heterogeneity and resistance to anti-HER2 antibody-drug conjugates. Breast Cancer Res. 22 (1), 15–101186s13058 (2020).
Lei, H. et al. Assessment of the expression pattern of HER2 and its correlation with HER2-targeting antibody-drug conjugate therapy in urothelial cancer. J Natl Cancer Cent. ;3(2):121 – 8.10.1016/j.jncc.2023.02.003 (2023).
Ge, H. et al. The effectiveness and safety of RC48 alone or in combination with PD-1 inhibitors for locally advanced or metastatic urothelial carcinoma: a multicenter, real-world study. J Transl Med. ;23(1):243.10.1186/s12967-025-06237-4 (2025).
Khongorzul, P., Ling, C. J., Khan, F. U., Ihsan, A. U. & Zhang, J. Antibody–Drug Conjugates: A Comprehensive Review. Molecular Cancer Research. ;18(1):3-19.10.1158/1541–7786.MCR-19-0582 (2020).
Postow, P. MA, Sidlow, R. & HellmannMD Immune-Related Adverse Events Associated with Immune Checkpoint Blockade. N Engl. J. Med. 378 (2), 158–168. https://doi.org/10.1056/NEJMra1703481 (2018).
Zhu, Z. et al. Incidence of antibody-drug conjugates-related pneumonitis in patients with solid tumors: A systematic review and meta-analysis. Crit. Rev. Oncol. Hematol. 184, 103960. https://doi.org/10.1016/j.critrevonc.2023.103960 (2023).
Funding
This study was supported by the National Natural Science Foundation of China (Grant No. 82273347) and the Clinical Research Foundation of Central High-level Hospital (Peking University First Hospital Research Fund Program) (Grant No. 2023HQ6).
Author information
Authors and Affiliations
Contributions
Cuijian Zhang had full access to all the data in the study and take responsibility for the integrity of the data and the accuracy of the data analysis.Concept and design: X.G, Y.G, Z.H, C.Z.Acquisition of data: X.G, S.W, Y.M, Y.C, Y.D, Q.W.Analysis and interpretation of data: X.G, Y.C, K.Y, Q.T, Y.F, H.H, W.Y.Drafting of the manuscript: X.G, Y.G.Critical revision of the manuscript for important intellectual content: X.G, Y.G, Z.H, C.Z.Statistical analysis: X.G, Y.C, Y.D.Administrative, technical, or material support: None.Supervision: Z.H, C.Z.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethical approval
The study protocol was approved by the Ethics Committee of Peking University First Hospital (Approval No.: 2025R0556). The requirement for informed consent was waived by the ethics committee given the participants could not be contacted due to the retrospective nature of the research.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Guo, X., Wang, S., Ma, Y. et al. Efficacy and safety of RC48 alone or combined with PD-1 inhibitors in high-risk non-muscle invasive bladder cancer. Sci Rep 16, 15796 (2026). https://doi.org/10.1038/s41598-026-43393-z
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-026-43393-z
