
Abstract
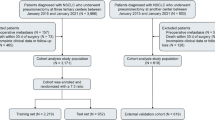
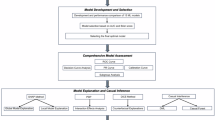
Brain and central nervous system (CNS) malignancies represent a substantial burden on healthcare systems worldwide, and unplanned reoperations following initial surgery are critical events influencing clinical prognosis. Current predictive tools for such reoperations remain limited in their ability to synthesize multifaceted clinical data into accurate risk assessments. This study sought to develop and validate interpretable machine learning algorithms designed to predict the likelihood of unplanned reoperations in patients underwent intracranial tumor surgery. We collected data on patients underwent intracranial tumor surgery who were admitted the First Affiliated Hospital of Xi’an Jiaotong University between January 2023 and January 2024. Patients were additionally partitioned into a training cohort and a validation cohort at a 7:3 proportion. We used least absolute shrinkage and selection operator regression to efficiently screen feature variables associated with CNS cancers postoperative unplanned reoperation. Five machine learning models were employed to predict postoperative unplanned reoperation. The predictive performance of these models was compared by utilizing evaluation metrics, including the area under the receiver operating characteristic curve (AUC). Moreover, the SHapley Additive exPlanation (SHAP) approach was adopted to rank the feature importance and interpret the final model. 11 independent key variables were ultimately chosen to build the model. Among these five machine learning models, the logistic regression (LR) model demonstrated the highest performance. The LR model effectively predicted the risk of unplanned reoperation in patients who underwent intracranial tumor surgery, achieving strong results in both the training set (AUC: 0.836, 95% CI 0.806–0.863) and the internal test set (AUC: 0.769, 95% CI 0.652–0.814). The calibration curve and brier score indicated a close alignment between the predicted and the actual observed risks in the internal test set. Analysis using SHAP identified the duration of surgery, tumor location, modified Frailty Index-5, and tumor type as the most significant predictive factors. To support the practical application of this ML model in a clinical environment, a web-based application was developed for easy access (https://unplanned-reoperation-risk-predicting.streamlit.app/). We developed and internally validated an explainable ML model for predicting the risk of unplanned reoperation in patients underwent intracranial tumor surgery. In this single-center cohort, this model shows promise for assisting healthcare professionals in the early identification of patients at elevated risk, thereby providing a potential basis for exploring personalized treatment strategies tailored to each patient’s specific needs.
Similar content being viewed by others

Data availability
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
References
GBD 2021 Nervous System Disorders Collaborators. Global, regional, and national burden of disorders affecting the nervous system, 1990–2021: A systematic analysis for the global burden of disease study 2021. Lancet Neurol. 23(4), 344–381 (2024).
GBD 2016 Brain and Other CNS Cancer Collaborators. Global, regional, and national burden of brain and other CNS cancer, 1990–2016: A systematic analysis for the global burden of disease study 2016. Lancet Neurol. 18(4), 376–393 (2019).
Leece, R. et al. Global incidence of malignant brain and other central nervous system tumors by histology, 2003–2007. Neuro Oncol. 19(11), 1553–1564 (2017).
Stupp, R. et al. Radiotherapy plus concomitant and adjuvant temozolomide for glioblastoma. N. Engl. J. Med. 352(10), 987–996 (2005).
Park, K. B., Johnson, W. D. & Dempsey, R. J. Global neurosurgery: The unmet need. World Neurosurg. 88, 32–35 (2016).
Bergen, D. C. & Silberberg, D. Nervous system disorders: A global epidemic. Arch. Neurol. 59(7), 1194–1196 (2002).
Gritsch, S., Batchelor, T. T. & Gonzalez Castro, L. N. Diagnostic, therapeutic, and prognostic implications of the 2021 World Health Organization classification of tumors of the central nervous system. Cancer 128(1), 47–58 (2022).
Huntington, C. R. et al. The Centers for Medicare and Medicaid Services (CMS) two midnight rule: Policy at odds with reality. Surg. Endosc. 30(2), 751–755 (2016).
McLaughlin, N., Jin, P. & Martin, N. A. Assessing early unplanned reoperations in neurosurgery: Opportunities for quality improvement. J. Neurosurg. 123(1), 198–205 (2015).
Dasenbrock, H. H. et al. Unplanned reoperation after craniotomy for tumor: A National Surgical Quality Improvement Program analysis. Neurosurgery 81(5), 761–771 (2017).
Algattas, H., Kimmell, K. T. & Vates, G. E. Risk of reoperation for hemorrhage in patients after craniotomy. World Neurosurg. 87, 531–539 (2016).
Mukerji, N., Jenkins, A., Nicholson, C. & Mitchell, P. Unplanned reoperation rates in pediatric neurosurgery: A single center experience and proposed use as a quality indicator. J. Neurosurg. Pediatr. 9(6), 665–669 (2012).
Zohdy, Y. M. et al. Causes and predictors of unplanned readmission in patients undergoing intracranial tumor resection: A multicenter analysis of 31,776 patients. World Neurosurg. 178, e869–e878 (2023).
Silva Santana, L. et al. Application of machine learning for classification of brain tumors: A systematic review and meta-analysis. World Neurosurg. 186, 204-218.e202 (2024).
International conference on harmonisation. Guidance on statistical principles for clinical trials; Availability—FDA. Notice. Fed. Regist. 63(179), 49583–49598 (1998).
Jia, B. & Lynn, H. S. A sample size planning approach that considers both statistical significance and clinical significance. Trials 16, 213 (2015).
Henry, R. K. et al. Frailty as a predictor of postoperative complications following skull base surgery. Laryngoscope 131(9), 1977–1984 (2021).
Wilson, J. R. F. et al. Frailty is a better predictor than age of mortality and perioperative complications after surgery for degenerative cervical myelopathy: An analysis of 41,369 patients from the NSQIP database 2010-2018. J. Clin. Med. https://doi.org/10.3390/jcm9113491 (2020).
Subramaniam, S., Aalberg, J. J., Soriano, R. P. & Divino, C. M. New 5-factor modified frailty index using American College of Surgeons NSQIP data. J. Am. Coll. Surg. 226(2), 173-181.e178 (2018).
Zhai, T. et al. Lipid metabolism-related miRNAs with potential diagnostic roles in prostate cancer. Lipids Health Dis. 22(1), 39 (2023).
Lundberg, S. M. & Lee, S.-I. A unified approach to interpreting model predictions. In Proceedings of the 31st conference on neural information processing systems (NIPS 2017) (Long Beach. 2017).
Lohmann, S. et al. Development and validation of prediction scores for nosocomial infections, reoperations, and adverse events in the daily clinical setting of neurosurgical patients with cerebral and spinal tumors. J. Neurosurg. 134(3), 1226–1236 (2021).
Raghib, M. F. et al. Risk factors and outcomes of redo craniotomy: A tertiary care center analysis. Cureus 14(1), e21440 (2022).
Colasacco, C. J. et al. Association of baseline frailty and age with postoperative outcomes in metastatic brain tumor patients. J. Neurosurg. Sci. 68(5), 526–532 (2024).
Sletvold, T. P., Boland, S., Schipmann, S. & Mahesparan, R. Quality indicators for evaluating the 30-day postoperative outcome in pediatric brain tumor surgery: A 10-year single-center study and systematic review of the literature. J. Neurosurg. Pediatr. 31(2), 109–123 (2023).
Karabacak, M., Jagtiani, P., Shrivastava, R. K. & Margetis, K. Personalized prognosis with machine learning models for predicting in-hospital outcomes following intracranial meningioma resections. World Neurosurg. 182, e210–e230 (2024).
Dichter, A. et al. Post-operative outcome predictions in vestibular schwannoma using machine learning algorithms. J. Pers. Med. https://doi.org/10.3390/jpm14121170 (2024).
Goecks, J., Jalili, V., Heiser, L. M. & Gray, J. W. How machine learning will transform biomedicine. Cell 181(1), 92–101 (2020).
Cai, L. Q., Yang, D. Q., Wang, R. J., Huang, H. & Shi, Y. X. Establishing and clinically validating a machine learning model for predicting unplanned reoperation risk in colorectal cancer. World J. Gastroenterol. 30(23), 2991–3004 (2024).
Chen, H. et al. Incidences, causes and risk factors of unplanned reoperation within 30 days of craniovertebral junction surgery: A single-center experience. Eur. Spine J. 32(6), 2157–2163 (2023).
Michaels, A. D. et al. Unplanned reoperation following colorectal surgery: Indications and operations. J. Gastrointest. Surg. 21(9), 1480–1485 (2017).
Dasenbrock, H. H. et al. Reoperation and readmission after clipping of an unruptured intracranial aneurysm: A National Surgical Quality Improvement Program analysis. J. Neurosurg. 128(3), 756–767 (2018).
Zhang, J. et al. Sepsis and septic shock after craniotomy: Predicting a significant patient safety and quality outcome measure. PLoS ONE 15(9), e0235273 (2020).
Rahmani, R. et al. Risk factors associated with early adverse outcomes following craniotomy for malignant glioma in older adults. J. Geriatr. Oncol. 11(4), 694–700 (2020).
Cole, K. L. et al. Association of baseline frailty status and age with outcomes in patients undergoing intracranial meningioma surgery: Results of a nationwide analysis of 5818 patients from the National Surgical Quality Improvement Program (NSQIP) 2015-2019. Eur. J. Surg. Oncol. 48(7), 1671–1677 (2022).
Dicpinigaitis, A. J. et al. Association of baseline frailty status and age with postoperative morbidity and mortality following intracranial meningioma resection. J. Neurooncol. 155(1), 45–52 (2021).
Schwartz, C. et al. Frailty indices predict mortality, complications and functional improvements in supratentorial meningioma patients over 80 years of age. J. Neurooncol. 170(1), 89–100 (2024).
Thommen, R. et al. Preoperative frailty measured by risk analysis index predicts complications and poor discharge outcomes after brain tumor resection in a large multi-center analysis. J. Neurooncol. 160(2), 285–297 (2022).
Sastry, R. A. et al. Frailty and outcomes after craniotomy for brain tumor. J. Clin. Neurosci. 81, 95–100 (2020).
Bonney, P. A. et al. Frailty is associated with in-hospital morbidity and nonroutine disposition in brain tumor patients undergoing craniotomy. World Neurosurg. 146, e1045–e1053 (2021).
Casazza, G. C. et al. Increasing frailty, not increasing age, results in increased length of stay following vestibular schwannoma surgery. Otol. Neurotol. 41(10), e1243–e1249 (2020).
Dicpinigaitis, A. J. et al. Associations of baseline frailty status and age with outcomes in patients undergoing vestibular schwannoma resection. JAMA Otolaryngol. Head Neck Surg. 147(7), 608–614 (2021).
Schipmann, S. et al. Adverse events in brain tumor surgery: Incidence, type, and impact on current quality metrics. Acta Neurochir. (Wien) 161(2), 287–306 (2019).
Farooqi, A. et al. The impact of gender on long-term outcomes following supratentorial brain tumor resection. Br. J. Neurosurg. 36(2), 228–235 (2022).
Farooqi, A., Dimentberg, R., Shultz, K., McClintock, S. D. & Malhotra, N. R. Absence of gender disparity in thirty-day morbidity and mortality after supratentorial brain tumor resection. World Neurosurg. 144, e361–e367 (2020).
Aziz, N. et al. Blood transfusions in craniotomy for tumor resection: Incidence, risk factors, and outcomes. J. Clin. Neurosci. 132, 111009 (2025).
Nia, A. M. et al. Metabolic syndrome associated with increased rates of medical complications after intracranial tumor resection. World Neurosurg. 126, e1055–e1062 (2019).
Davis, M. C., Ziewacz, J. E., Sullivan, S. E. & El-Sayed, A. M. Preoperative hyperglycemia and complication risk following neurosurgical intervention: A study of 918 consecutive cases. Surg. Neurol. Int. 3, 49 (2012).
The Lancet Respiratory Medicine. Opening the black box of machine learning. Lancet Respir. Med. 6(11), 801 (2018).
Acknowledgements
We thank the patients underwent intracranial tumor surgery, and the proxies taking good care of them.
Funding
This work was supported by the National Natural Science Foundation of China (Program No. 82371459) and the Innovation Capability Support Program of Shaanxi (Program No. 2024SF-YBXM-216).
Author information
Authors and Affiliations
Contributions
Study concept and design: Xiaobo Ye, Qiang Meng, Hua Zhang; data analysis and interpretation: Xiaobo Ye, Hui Li; drafting of the manuscript: Xiaobo Ye; supervision: Qiang Meng, Hua Zhang; reviewing and editing: Xi Zhang, Jiahao Lian, Yicong Dong, Yutao Ren, Huanfa Li, Yong Liu, Changwang Du, Hao Wu. All authors critically revised and approved the ffnal version of the manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethics approval and consent to participate
This study protocol complies with the guidelines of the Declaration of Helsinki and was approved by the Clinical Research Ethics Committee of the First Affiliated Hospital of Xi’an Jiaotong University (KYLLSL-2024-480-02). The need for informed consent was waived by the Institutional Review Board of the First Affiliated Hospital of Xi’an Jiaotong University because this study involved the analysis of existing, anonymized data. This waiver is in accordance with the institution’s guidelines on minimal-risk research.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Ye, X., Li, H., Zhang, X. et al. Development and validation of an interpretable prediction model for the risk of unplanned reoperation in patients underwent intracranial tumor surgery. Sci Rep (2026). https://doi.org/10.1038/s41598-026-43594-6
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-026-43594-6
