
Abstract
Heatstroke has high mortality, requiring early risk stratification. This study aimed to compare the predictive value of the reverse shock index multiplied by Glasgow Coma Scale score (rSIG) with shock index (SI), GCS, and qSOFA score for mortality in ICU heatstroke patients. The reverse shock index multiplied by Glasgow Coma Scale score (rSIG), calculated as GCS × (SBP / HR) using the first recorded values at ICU admission. This multicenter retrospective study included 671 heatstroke patients from 83 ICUs. Predictive performance was compared using receiver operating characteristic (ROC) curves. Independent risk factors were identified via logistic regression, and a nomogram was developed. Subgroup analysis was conducted to assess the consistency of the predictive value of rSIG. The mortality rate was 17.88%. rSIG demonstrated the highest predictive ability (AUC = 0.739), outperforming SI, GCS, and qSOFA. Prothrombin time, creatinine, lactate, and rSIG were independent predictors. The nomogram integrating these factors achieved an AUC of 0.80. Subgroup analysis confirmed the consistent predictive value of rSIG across various patient subgroups. The rSIG is a simple and effective early screening tool for rapid risk stratification in ICU patients with heatstroke. The predictive model combining rSIG with PT, Cr, and Lac further enhances prognostic accuracy, offering significant clinical utility.
Similar content being viewed by others
Introduction
Heatstroke is a life-threatening condition caused by dysregulation of core body temperature, characterized by core temperature exceeding 40 °C and accompanied by central nervous system dysfunction such as delirium, seizures, or coma1. With increasing challenges including global warming and inadequate power supply, the incidence of heatstroke has risen significantly2. Our previous observational study indicated an overall mortality rate as high as 32.4% among heatstroke patients3. Despite advances in modern critical care, such as targeted temperature management and organ support, mortality remains high, particularly in elderly individuals and those with comorbidities4,5,6. Therefore, early identification of high-risk patients and prompt intervention are crucial for improving outcomes7.
In emergency department and intensive care unit (ICU) settings, rapid and parsimonious scoring systems—including the Shock Index (SI)8,9, Glasgow Coma Scale (GCS)10,11, and quick Sequential Organ Failure Assessment (qSOFA)12—are widely employed for risk stratification in critically ill patients. However, the predictive performance of these scoring tools has not been adequately validated specifically in patients with heatstroke. Moreover, as each score predominantly focuses on a single physiological dimension—either circulatory or neurological status—they may fail to comprehensively capture the complex multiorgan injury pathophysiology that characterizes heatstroke1,5.
The reverse shock index multiplied by Glasgow Coma Scale score (rSIG), calculated as (GCS score × systolic blood pressure) / heart rate, is a composite metric that integrates hemodynamic stability (reflected by the reverse shock index, i.e., systolic blood pressure divided by heart rate) and neurological status. Although a universally accepted normal range for rSIG has not been established, previous studies in trauma patients have demonstrated that higher rSIG values are associated with better survival13.In recent years, rSIG has demonstrated strong prognostic value for predicting outcomes in patients with trauma and sepsis9,14,15. We hypothesized that rSIG, by combining both circulatory and neurological functions, may more effectively predict mortality risk in heatstroke patients compared to single‑dimensional indicators.
This study aimed to systematically evaluate and compare the predictive capabilities of rSIG, SI, GCS, and qSOFA for short-term mortality in ICU patients with heatstroke, using a large-scale, multicenter retrospective cohort. Based on this comparison, we sought to develop and validate an individualized prediction model that integrates key prognostic indicators to aid clinical decision-making.
Methods
Study design and population
This multicenter retrospective observational study screened adult patients (age ≥ 18 years) admitted to intensive care units (ICUs) across 83 hospitals in southwestern China between June 2022 and October 2022, who met the diagnostic criteria for heatstroke. The diagnosis of heatstroke was initially made by the treating physician at the point of care, typically in the Emergency Department (ED) prior to ICU admission, based on the standard clinical criteria. Diagnosis was based on standard definitions for classic or exertional heatstroke, including core body temperature > 40 ℃(measured by rectal, esophageal, or bladder probe, as per local ICU standard practice) following exposure to a hot environment or strenuous exercise, accompanied by central nervous system dysfunction. Exclusion criteria were: missing key data (e.g., vital signs at admission, GCS score, or essential laboratory results) or hospital stay < 24 h. A total of 671 patients were ultimately included (Figure S1). This study was reported in accordance with the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines. Considering the retrospective design of this study, an informed consent exemption was obtained from the Ethics Committee on Biomedical Research, West China Hospital of Sichuan University, and no human intervention was involved in the data collection process. The Biomedical Ethics Committee of West China Hospital, Sichuan University, approved the study protocol (approval number: 2022 − 1542, clinical trial registration number: ChiCTR2200066314; Date of registration: December 1, 2022).
Data collection and quality control
Data were retrospectively extracted from the electronic medical records of all participating centers following a standardized protocol. Trained clinical staff at each site manually collected the required variables using a unified electronic case report form (eCRF). To ensure accuracy, a rigorous quality control process was implemented, which included verification by site investigators, double data entry with consistency checks using EpiData software (version 3.1), and centralized logic validation with query resolution. The final database was locked after comprehensive review and approval for analysis.
The following data were extracted from electronic medical records: (1) Demographic and baseline characteristics: age, sex, heatstroke type (classic or exertional), comorbidities (diabetes mellitus, hypertension). Heatstroke type was classified as “classic,” “exertional,” or “unknown” based on the documented history in the medical record regarding antecedent exposure (high environmental temperature without exertion) or activity (strenuous exercise). The “unknown” category was assigned when the medical record explicitly indicated unclear etiology or contained insufficient information to reliably distinguish between the two types. (2) Vital signs at admission: first-recorded body temperature, systolic blood pressure (SBP), diastolic blood pressure (DBP), heart rate (HR), and respiratory rate (RR). (3) Disease severity scores: GCS score, qSOFA score. The shock index (SI = HR/SBP) and the reverse shock index multiplied by GCS (rSIG = GCS × SBP / HR) were calculated based on these first-recorded values. (4) Laboratory parameters: initial laboratory results within 24 h of ICU admission, including white blood cell count, platelet count, total bilirubin, serum creatinine, albumin, prothrombin time (PT), procalcitonin, glucose, lactate, sodium, potassium, and calcium. (5) Treatment and complications: initiation of cooling measures, presence of infection, and in-hospital complications including respiratory failure, central nervous system impairment, hepatic dysfunction, and renal dysfunction. Complications occurring during hospitalization, including respiratory failure (requiring mechanical ventilation), hepatic dysfunction (serum bilirubin > 50 µmol/L or ALT > 100 U/L), renal dysfunction (serum creatinine > 150 µmol/L or need for renal replacement therapy), and central nervous system impairment (new focal deficit or persistent coma), were recorded. (6)Outcome measures: The primary outcome was all-cause ICU mortality. This endpoint was chosen to evaluate predictors of early death during the most critical phase of care. We acknowledge that deaths occurring after ICU discharge but during the same hospitalization were not captured as events in this analysis. Secondary outcomes included ICU length of stay and total hospital length of stay.
Statistical analysis
Missing data were handled using multiple imputation by chained equations (MICE) under the assumption of missing at random, generating five imputed datasets for analysis. Continuous variables were expressed as mean ± standard deviation or median (interquartile range) based on their distribution and compared using Student’s t-test or Mann–Whitney U test, as appropriate. Categorical variables were summarized as frequency (percentage) and compared using the chi-square test or Fisher’s exact test. Receiver operating characteristic (ROC) curves were plotted for rSIG, SI, GCS, and qSOFA in predicting mortality. The area under the curve (AUC) was calculated for each indicator, and differences in AUC were compared using DeLong’s test. Univariate logistic regression was performed first, and variables with P < 0.05 were included in a multivariate logistic regression model (forward selection) to identify independent predictors of mortality. Results were reported as odds ratios (OR) with 95% confidence intervals (CI). Based on the independent predictors identified in the multivariate analysis, an individualized nomogram prediction model was developed using R software. Internal validation of the nomogram was performed, the entire cohort was randomly divided into a training set (70%) and an internal validation set (30%), and its performance was assessed using receiver operating characteristic (ROC) curves. Subgroup analyses were conducted according to sex, use of cooling measures, presence of diabetes mellitus, hypertension, heatstroke type, and presence of infection to evaluate the consistency of the predictive value of rSIG. Interaction P-values were calculated to test for effect modification.
All statistical analyses were performed using R software (version 4.2.1) and SPSS (version 26.0). A two-sided P-value < 0.05 was considered statistically significant.
Results
A total of 671 patients with heatstroke were included in this study, of whom 120 (17.88%) died. Table 1 details the baseline characteristics of the overall population, survivors, and non-survivors. No significant differences were observed between the two groups in terms of age, sex, heatstroke type, history of diabetes mellitus, first-recorded body temperature, respiratory rate, BMI, exposure duration, cooling measures initiated, or presence of infection. However, compared with survivors, non-survivors exhibited significantly lower systolic blood pressure, diastolic blood pressure, GCS scores, platelet counts, and albumin levels, as well as significantly higher heart rate, serum creatinine, prothrombin time (PT), lactate, potassium levels, and shock index (SI). The rSIG value was significantly lower in non-survivors than in survivors (3.55 vs. 7.56, P < 0.001). In terms of complications, the incidence of respiratory failure, hepatic dysfunction, and renal dysfunction was significantly higher in non-survivors.
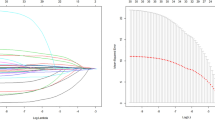
Figure 1 compares the predictive performance of four scoring systems—rSIG, SI, GCS, and qSOFA—for mortality. The area under the curve (AUC) was 0.739 (95% CI: 0.687–0.782) for rSIG, 0.688 (95% CI: 0.639–0.732) for SI, 0.703 (95% CI: 0.653–0.746) for GCS, and 0.613 (95% CI: 0.564–0.658) for qSOFA. An rSIG score of ≤ 7.3 was identified as the optimal cutoff for predicting in-hospital mortality, with a sensitivity of 0.52 (95% CI: 0.44–0.58), a specificity of 0.85 (95% CI: 0.82–0.88), and an overall accuracy of 0.62 (95% CI: 0.58–0.66). Pairwise comparisons using DeLong’s test indicated statistically significant differences in AUC between rSIG and each of the other three scores (all p < 0.05).

Comparison of receiver operating characteristic (ROC) curves for predicting mortality using the reverse shock index multiplied by Glasgow Coma Scale score (rSIG), shock index (SI), Glasgow Coma Scale (GCS), and quick Sequential Organ Failure Assessment (qSOFA) in ICU patients with heatstroke. The area under the curve (AUC) with 95% confidence interval for each score is as follows: rSIG (red solid line), AUC = 0.739 (95% CI 0.687–0.782); SI (blue dashed line), AUC = 0.688 (95% CI 0.639–0.732); GCS (green dotted line), AUC = 0.703 (95% CI 0.653–0.746); qSOFA (purple dash-dot line), AUC = 0.613 (95% CI 0.564–0.658).
Table 2 presents the results of univariate and multivariate logistic regression analyses for risk factors of ICU mortality in heatstroke patients. Univariate analysis revealed that systolic blood pressure, diastolic blood pressure, heart rate, platelet count, creatinine, albumin, prothrombin time (PT), lactate, potassium, and rSIG were significantly associated with mortality. Upon incorporating these significant variables into multivariate analysis, four indicators were ultimately identified as independent predictors of mortality: serum creatinine (Cr) (OR 1.01, 95% CI 1.01–1.01, P < 0.001), prothrombin time (PT) (OR 1.02, 95% CI 1.01–1.04, P = 0.033), lactate (Lac) (OR 1.17, 95% CI 1.08–1.28, P < 0.001), and rSIG (OR 0.86, 95% CI 0.79–0.93, P < 0.001). An odds ratio of less than 1 for rSIG indicates that higher values are associated with reduced mortality risk.
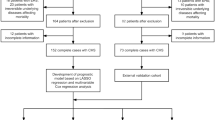
Based on the four independent predictors identified from the multivariate analysis (Cr, PT, Lac, rSIG), we constructed an individualized nomogram prediction model (Fig. 2a). The model enables estimation of individual mortality risk by summing the points corresponding to each variable’s value. The nomogram achieved an AUC of 0.80 (95% CI: 0.77–0.84) in the ROC analysis (Fig. 2b). The model developed on the training set (AUC = 0.80, 95% CI: 0.75–0.84) performed consistently on the validation set (AUC = 0.82, 95% CI: 0.75–0.88). These results are presented in Supplementary Figure S2.

Nomogram Prediction Model; (a) Nomogram Prediction Model Based on Independent Predictors; (b) ROC Curve of the Nomogram Prediction Model. (a) The nomogram was constructed based on four independent predictors identified by multivariate logistic regression: serum creatinine (Cr, µmol/L), prothrombin time (PT, seconds), lactate (Lac, mmol/L), and the reverse shock index multiplied by Glasgow Coma Scale score (rSIG). For each patient, a point is assigned for every predictor according to its value on the top axis. The sum of these points corresponds to a total point value on the bottom axis, which can be projected downward to estimate the individual probability of mortality (range 0.1–0.9). (b) Receiver operating characteristic (ROC) curve evaluating the discrimination performance of the nomogram model. The area under the curve (AUC) was 0.80 (95% confidence interval: 0.77–0.84), indicating good predictive accuracy.
We further assessed the association between rSIG and mortality across predefined subgroups (Fig. 3). In exploratory analyses, the association remained significant in most subgroups. Formal tests for interaction suggested potential effect modification by sex (P for interaction = 0.024) and hypertension status (P for interaction < 0.001), with the association appearing stronger in males and in patients without hypertension. However, these interaction tests were not adjusted for multiple comparisons and should be considered preliminary. No significant interactions were observed for other subgroup variables (all interaction P > 0.05).

Forest Plot of rSIG for Predicting Mortality Across Subgroups. The forest plot displays odds ratios (ORs) with 95% confidence intervals (CIs) for the association between rSIG (per 1-point increase) and mortality, stratified by pre-defined clinical subgroups. An OR < 1 indicates that a higher rSIG score is associated with lower mortality. All odds ratios (ORs) are less than 1, indicating that a higher rSIG score is associated with a lower risk of mortality. The P value for interaction tests the null hypothesis that the association between rSIG and mortality is consistent across subgroups. The size of the data markers corresponds to the subgroup sample size (n). Abbreviations: OR, odds ratio; CI, confidence interval.
Discussion
The main findings of this study are as follows: (1) rSIG showed better predictive performance for ICU mortality compared with conventional SI, GCS, and qSOFA scores in ICU patients with heatstroke; (2) Serum creatinine, prothrombin time, lactate, and rSIG were identified as independent risk factors for mortality; (3) The nomogram model integrating these four factors achieved enhanced predictive accuracy with good calibration, suggesting its potential utility for individualized risk assessment; (4) The association between rSIG and mortality was generally consistent across most clinical subgroups analyzed.
The observed performance of rSIG may be attributed to its integration of key information from both cardiovascular and neurological systems13. The core pathophysiology of heatstroke involves direct thermal toxicity leading to systemic inflammatory response syndrome and multi-organ dysfunction1,5,16,17.A low GCS reflects severe central nervous system injury10, while an elevated SI indicates circulatory instability and shock8,18,19. Therefore, rSIG, by combining these two critical dimensions, might offer a more comprehensive assessment of overall disease severity20. Our findings align with previous applications of rSIG in trauma and sepsis populations9,21,22, supporting further exploration of its role as a composite physiological assessment tool in heatstroke.
In addition to rSIG, our multivariate model identified three crucial laboratory indicators. Elevated lactate levels, reflecting tissue hypoperfusion and anaerobic metabolism23, are commonly observed in severe heatstroke and are associated with increased mortality24,25,26. Similarly, elevated serum creatinine, indicating acute kidney injury, is frequently encountered and linked to poorer outcomes27,28,29. Prolonged prothrombin time reflects coagulopathy, representing an early manifestation of heatstroke-induced liver injury and disseminated intravascular coagulation (DIC)30,31,32. Consequently, the nomogram model effectively integrates key indicators representing neurological, circulatory, renal, and coagulation functions, providing a multidimensional risk stratification tool.
The nomogram model developed in this study demonstrates substantial clinical utility. By inputting readily available parameters—GCS, systolic blood pressure, heart rate, creatinine, PT, and lactate—clinicians can visually estimate a patient’s mortality probability using the nomogram. The nomogram provides direct clinical utility by quantifying mortality risk using routine ICU admission parameters, enabling early risk stratification. It helps identify high‑risk patients for intensified monitoring or therapy escalation.
This study has several important limitations. First and foremost, its retrospective observational design inherently limits causal inference and is susceptible to unmeasured confounding and selection bias. Although we employed multiple imputation for missing data and implemented rigorous data quality control protocols across the 83 participating ICUs, residual bias due to the retrospective nature of the data collection cannot be ruled out. Second, while the multicenter design enhances internal validity, all participating hospitals were located in southwestern China. The generalizability of our findings to other regions requires careful consideration and external validation. Moreover, validating our models in geographically and demographically distinct populations is an essential next step to confirm their broad applicability.
Third, detailed information on specific cooling modalities, timings, and prehospital management was not uniformly available, which could act as unmeasured confounders. Future prospective, multicenter studies that include diverse geographic and demographic populations are essential to validate our findings, establish causality, and assess broader external validity. Fourth, this study did not compare the predictive performance of rSIG or the nomogram against established comprehensive ICU severity scores such as APACHE II or SOFA. Therefore, the relative advantage of our proposed tools within the broader ecosystem of prognostic scores remains to be determined. Fifth, while our models identify patients at higher risk, we did not establish or validate specific clinical decision thresholds (e.g., for care escalation), which is a necessary step before implementation. Finally, our study evaluated the prognostic value of a single rSIG measurement at ICU admission. An important and logical extension would be to investigate the dynamic trajectory of rSIG over the first 24–72 h of care. Future prospective studies designed with protocolized serial assessments are needed to answer this question.
Conclusions
In conclusion, the rSIG score serves as a simple and rapid early-risk screening tool, demonstrating superior predictive performance to SI, GCS, and qSOFA in this study. For a more individualized prognosis when laboratory data are available, the nomogram that incorporates rSIG, creatinine, prothrombin time, and lactate provides enhanced accuracy. Together, these models highlight a set of key prognostic indicators and offer a framework for risk stratification that warrants prospective validation to define clinical action thresholds and assess impact on patient management.
Data availability
The data used and analyzed during this study are available from the corresponding author upon reasonable request.
Abbreviations
- rSIG:
-
Reverse shock index multiplied by glasgow coma scale score
- ICU:
-
Intensive care unit
- SI:
-
Shock index
- GCS:
-
Glasgow coma scale
- qSOFA:
-
Quick sequential organ failure assessment
- ROC:
-
Receiver operating characteristic
- AUC:
-
Area under the curve
- PT:
-
Prothrombin time
- Cr:
-
Creatinine
- Lac:
-
Lactate
- Na:
-
Sodium
- K:
-
Potassium
- Ca:
-
Calcium
- CI:
-
Confidence interval
- OR:
-
Odds Ratio
- SBP:
-
Systolic blood pressure
- DBP:
-
Diastolic blood pressure
- HR:
-
Heart rate
- RR:
-
Respiratory rate
- BMI:
-
Body mass index
- DIC:
-
Disseminated intravascular coagulation
- SD:
-
Standard deviation
- IQR:
-
Interquartile range
References
Epstein, Y., Yanovich, R. & Heatstroke. N Engl. J. Med. 380, 2449–2459 (2019).
Dhainaut, J. F., Claessens, Y. E., Ginsburg, C. & Riou, B. Unprecedented heat-related deaths during the 2003 heat wave in Paris: consequences on emergency departments. Crit. Care Lond. Engl. 8, 1–2 (2004).
Shi, L. et al. Heatstroke: a multicenter study in southwestern China. Front. Public. Health. 12, 1349753 (2024).
Bouchama, A. & Knochel, J. P. Heat stroke. N Engl. J. Med. 346, 1978–1988 (2002).
Bouchama, A. et al. Classic and exertional heatstroke. Nat. Rev. Dis. Primer. 8, 8 (2022).
Bouchama, A. et al. Prognostic factors in heat wave related deaths: a meta-analysis. Arch. Intern. Med. 167, 2170–2176 (2007).
Wang, L. et al. Risk factor analysis and nomogram for predicting In-hospital mortality in ICU patients with heat stroke: a national multicenter study. J. Multidiscip Healthc. 16, 3189–3201 (2023).
Rady, M. Y., Smithline, H. A., Blake, H., Nowak, R. & Rivers, E. A comparison of the shock index and conventional vital signs to identify acute, critical illness in the emergency department. Ann. Emerg. Med. 24, 685–690 (1994).
Matsuda, W., Kimura, A. & Uemura, T. Comparison of the reverse shock index multiplied by glasgow coma scale score, MEWS, and qSOFA as sepsis screening tools for predicting short-term outcomes. OPEN. Access. Emerg. Med. OAEM. 17, 247–255 (2025).
Teasdale, G. & Jennett, B. Assessment of coma and impaired consciousness. A practical scale. Lancet Lond. Engl. 2, 81–84 (1974).
Teasdale, G., Murray, G., Parker, L. & Jennett, B. Adding up the glasgow coma score. Acta Neurochir. Suppl. (Wien). 28, 13–16 (1979).
Seymour, C. W. et al. Assessment of clinical criteria for sepsis: for the third international consensus definitions for sepsis and septic shock (sepsis-3). JAMA 315, 762–774 (2016).
Kimura, A. & Tanaka, N. Reverse shock index multiplied by glasgow coma scale score (rSIG) is a simple measure with high discriminant ability for mortality risk in trauma patients: an analysis of the Japan trauma data bank. Crit. Care Lond. Engl. 22, 87 (2018).
Wu, S. C. et al. The reverse shock index multiplied by glasgow coma scale score (rSIG) and prediction of mortality outcome in adult trauma patients: a cross-sectional analysis based on registered trauma data. Int. J. Environ. Res. Public. Health. 15, 2346 (2018).
Lammers, D. T. et al. Pediatric adjusted reverse shock index multiplied by glasgow coma scale as a prospective predictor for mortality in pediatric trauma. J. Trauma. Acute Care Surg. 90, 21–26 (2021).
Iba, T., Helms, J., Levi, M. & Levy, J. H. Inflammation, coagulation, and cellular injury in heat-induced shock. Inflamm. Res. Off J. Eur. Histamine Res. Soc. Al. 72, 463–473 (2023).
Abdullah, M., Ehaideb, S., Roberts, G. & Bouchama, A. Insights into pathophysiology and therapeutic strategies for heat stroke: lessons from a baboon model. Exp. Physiol. 109, 484–501 (2024).
King, R. W., Plewa, M. C., Buderer, N. M. & Knotts, F. B. Shock index as a marker for significant injury in trauma patients. Acad. Emerg. Med. Off J. Soc. Acad. Emerg. Med. 3, 1041–1045 (1996).
Middleton, D. J., Smith, T. O., Bedford, R., Neilly, M. & Myint, P. K. Shock index predicts outcome in patients with suspected sepsis or community-acquired pneumonia: a systematic review. J. Clin. Med. 8, 1144 (2019).
Hanna, S., Montmayeur, J., Vergnaud, E. & Orliaguet, G. Prognosis and assessment of the predictive value of severity scores in paediatric abdominal trauma: a french national cohort study. Eur. J. Anaesthesiol. 41, 632–640 (2024).
Kokeguchi, H., Toida, C., Tsunoyama, T., Iwashita, M. & Miyake, Y. Reverse shock index multiplied by glasgow coma scale score as a predictor of urgent trauma care and mortality in isolated severe traumatic brain injury: a 10-year nationwide validation study. BMC Emerg. Med. 25, 235 (2025).
Lee, Y. T. et al. Reverse shock index multiplied by glasgow coma scale as a predictor of massive transfusion in trauma. Am. J. Emerg. Med. 46, 404–409 (2021).
Ryoo, S. M. et al. Lactate level versus lactate clearance for predicting mortality in patients with septic shock defined by sepsis-3. Crit. Care Med. 46, e489–e495 (2018).
Hsu, Y. D., Lee, W. H., Chang, M. K., Shieh, S. D. & Tsao, W. L. Blood lactate threshold and type II fibre predominance in patients with exertional heatstroke. J. Neurol. Neurosurg. Psychiatry. 62, 182–187 (1997).
Liu, F. et al. Lactate combined with SOFA score for improving the predictive efficacy of SOFA score in patients with severe heatstroke. Am. J. Emerg. Med. 78, 163–169 (2024).
Heat stroke | the. value of blood lactate and lactate clearance rate in evaluating the prognosis of athletes with heat illness of varying degrees after high-intensity exercise | springermedicine.com. https://www.springermedicine.com/heat-stroke/heat-stroke/the-value-of-blood-lactate-and-lactate-clearance-rate-in-evaluat/50503204
Goto, H., Kinoshita, M. & Oshima, N. Heatstroke-induced acute kidney injury and the innate immune system. Front. Med. 10, 1250457 (2023).
Wu, M. et al. Clinical characteristics and risk factors associated with acute kidney injury inpatient with exertional heatstroke: an over 10-year intensive care survey. Front. Med. 8, 678434 (2021).
Zeng, Q. et al. Nomogram for predicting disseminated intravascular coagulation in heatstroke patients: a 10 years retrospective study. Front. Med. 10, 1150623 (2023).
Iba, T., Connors, J. M., Levi, M. & Levy, J. H. Heatstroke-induced coagulopathy: biomarkers, mechanistic insights, and patient management. EClinicalMedicine 44, 101276 (2022).
al-Mashhadani, S. A. et al. The coagulopathy of heat stroke: alterations in coagulation and fibrinolysis in heat stroke patients during the pilgrimage (haj) to makkah. Blood Coagul Fibrinolysis Int. J. Haemost Thromb. 5, 731–736 (1994).
Li, C. et al. Severe acute liver injury in patients with exertional heat stroke associated with poor short-term prognosis. World J. Emerg. Med. 13, 124–129 (2022).
Acknowledgements
Not applicable.
Funding
This research was supported by Noncommunicable Chronic Diseases-National Science and Technology Major Project (2023ZD0502400/2023ZD0502405).
Author information
Authors and Affiliations
Contributions
LYS and RRW designed this study; LYS carried out the study; MH and ZWZ communicated with patients’ families and got their approval. LYS and XPZ collected data; LYS and RRW performed statistical analyses and drafted the article; MH, SYC and ZWZ critically reviewed the paper; LLC and QYL performed article revisions and language polishing. All authors read and approved the final version of this paper.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
Ethical approval was obtained from the ethics committee of the West China Hospital of Sichuan University (NO: 2022 − 1542).The study was conducted in accordance with the Declaration of Helsinki.
Consent for publication
This retrospective study used anonymized data, and the need for individual consent for publication was waived by the ethics committee.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.


Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Shi, L., Liu, Q., Wang, R. et al. Predictive value of the reverse shock index multiplied by glasgow coma scale score for mortality in ICU heatstroke patients: a multicenter study. Sci Rep 16, 15676 (2026). https://doi.org/10.1038/s41598-026-46072-1
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-026-46072-1

{kind=link}
{kind=link}