
Abstract
Differentiating between infectious and non-infectious etiologies in systemic inflammatory disorders may be challenging due to overlapping clinical presentations and the lack of reliable discriminating biomarkers. Regulatory T-cells (Tregs) modulate immune responses. Their functionality is governed by specific chemokines, including CCL1 and CCL22. We investigated whether these Treg-attracting chemokines are differentially regulated in infectious versus sterile inflammation. This prospective, single-center biomarker study enrolled patients with sepsis, acute pancreatitis, and hospitalized controls without infectious diseases. Serum samples were collected on days 1, 3, 5, and 7, measuring CRP, IL-6, PCT, CCL1, and CCL22. Between March 2019 and October 2022, 159 patients were enrolled, comprising 45 patients suffering from acute pancreatitis, 15 patients with confirmed sepsis as well as 99 hospitalized controls. Established inflammatory parameters CRP, IL-6 and PCT showed typical kinetics. Decreased CCL1 levels, but not CCL22, distinguished acute pancreatitis from sepsis at all time points. Additionally, CCL1 levels inversely correlated with organ failure severity in sepsis patients. CCL1 shows potential to serve as a biomarker to differentiate sterile and non-sterile inflammation in sepsis and acute pancreatitis. This may support clinical decision-making and allow a more precise use of antibiotics in these patient cohorts.
Similar content being viewed by others


Background
Systemic inflammatory disorders frequently present as fulminant and potentially lethal syndromes, necessitating prompt diagnosis and immediate therapeutic intervention. Among these, both sepsis and acute pancreatitis are acute inflammatory pathologies of increasing epidemiological relevance1,2. Sepsis is defined as life-threatening organ dysfunction caused by a dysregulated host response to infection3. Organ failure is thus a crucial element of sepsis and is determined by using scoring systems such as the SOFA score3. Acute pancreatitis, although in most cases mild or only moderately severe4, may also lead to severe organ failure5,6. Thus, both pathologies represent critical illnesses characterized by complex immune dysregulation. Despite their overlapping clinical features, the management of sepsis and pancreatitis differs substantially. In sepsis, early administration of antibiotics is essential3,7, whereas antibiotics are generally not indicated in pancreatitis5,6. In clinical practice, differentiating between systemic inflammation due to sepsis and that due to acute pancreatitis may prove to be challenging due to their similar clinical presentation. Diagnostic differentiation is further complexified since established inflammatory serum markers, such as C-reactive protein (CRP) and interleukin-6 (IL-6), may be elevated in both pathologies, offering limited diagnostic discrimination.
Regulatory T cells (Tregs) are known to play a crucial role in the maintenance of immune homeostasis and modulation of immune responses8,9,10. Their spatial distribution and tissue recruitment during homeostasis and inflammation is orchestrated by chemokines11. Among these, CCL112,13 and CCL2212,14, both of which belong to the CC chemokine family, are major Treg-attracting chemokines that govern immune regulation during homeostasis and inflammatory conditions such as infection, autoimmunity and cancer12,13,15,16,17,18,19,20,21. CCL1 signals through CCR8 and is produced mainly by activated T cells, monocytes and macrophages, promoting the recruitment of CCR8-expressing cells such as Tregs13,22,23. CCL22 binds to CCR4 and is predominantly secreted by dendritic cells (DCs) and macrophages, where it mediates Treg migration and facilitates Treg-DC interactions24. Current literature paints an ambivalent picture of Treg function in sepsis, since both favorable25,26 as well as unfavorable courses27,28,29,30 in conjunction with elevated Treg numbers have been described. Similarly, Treg function in pancreatitis appears to be conflicting, with both protective31,32 and negative effects33 reported in preclinical models. However, Tregs and their functionality cannot be quantified easily in routine practice. In contrast, their recruiting chemokines are readily detectable in serum and thus may have the potential to serve as practical diagnostic biomarkers.
To identify potential novel biomarkers which reliably discriminate between bacterial sepsis and sterile inflammation due to acute pancreatitis, we conducted a prospective, single-center, exploratory biomarker study examining Treg-attracting chemokines. We found that serum levels of CCL1 and CCL22 were independent of baseline characteristics. While CCL22 was initially suppressed in sepsis, it failed to discriminate between sepsis and acute pancreatitis. In contrast, CCL1 levels were reduced in acute pancreatitis, while they tended to be elevated in sepsis, consistently distinguishing both conditions across all measured time points. Moreover, higher CCL1 levels were inversely correlated with organ dysfunction in sepsis. Thus, CCL1 should in future be evaluated to guide clinical reasoning in patients with inflammation as well as to predict patient prognosis in sepsis.
Results
Study population
159 patients were enrolled between March 2019 and October 2022. Baseline characteristics of our patient cohorts are shown in Table 2. The cohort consisting of hospitalized controls comprises 99 patients. Additionally, 15 patients with confirmed sepsis and 45 patients with acute pancreatitis were included. Our patient cohort demonstrated significant differences in age, active smoking status, regular alcohol consumption as well as presence of coronary heart disease, whereas the majority of epidemiological and medical factors assessed were balanced between the groups. Among the 159 patients enrolled, serum was collected on day 1 in all cases and on day 3 in 121 cases. 24 patients with acute pancreatitis and 10 patients with sepsis had serum collected at days 1, 3 and 5. The median observation period was three days.
Regarding disease etiology, the most frequent source of sepsis was the urinary tract (urosepsis, n = 7), followed by pneumonia (n = 2). The remaining patients presented with mixed or other etiologies. Blood cultures were positive in 9 of 15 patients (60%). In the acute pancreatitis cohort, the most common etiologies were biliary (n = 16) and alcoholic (n = 10), with the remaining patients presenting with mixed etiologies (n = 8) or idiopathic (n = 11).
Of the 15 sepsis patients, 10 were admitted to ICU or IMC at day 1, while 2 patients were not escalated to higher-level care based on medical or personal reasons, and 3 patients were managed outside these units at the time of enrollment. The median overall SOFA score at day 1 was 11 (IQR 9–11). ICU/IMC-admitted patients had a median SOFA score of 11 (IQR 10–13), whereas patients not admitted to ICU/IMC had a median SOFA score of 8.5.
Established inflammatory serum markers show typical kinetics in our cohort
Patients presenting with sepsis and acute pancreatitis are known to have elevated inflammatory serum markers such as CRP, PCT and IL-65,34,35. We measured these parameters in our cohorts on day 1, 3, 5 and 7 (Fig. 2). Medians and interquartile ranges of these parameters are shown in Suppl. Table 1. As expected, CRP was significantly elevated compared to controls in both groups at all measured time points, with higher levels in sepsis patients compared to pancreatitis patients at disease onset (Fig. 2A)34. PCT showed significant elevation compared to controls at all measured time points with significantly higher values in sepsis patients on all days (Fig. 2B). IL-6 levels were elevated only on the first three days of both types of inflammation, with highest values in sepsis patients on day 1 (Fig. 2C). Taken together, established inflammatory parameters show the kinetics expected from a clinician’s perspective34,35, confirming the representability of our patient cohort.

Study Design. A representative study flow chart is shown. Figure created using BioRender.com

Established inflammatory serum markers show typical kinetics in our cohort. Serum levels of (A) CRP, (B) PCT and (C) IL-6 of hospitalized controls (control) and patients with pancreatitis and sepsis were determined at the indicated time points after hospital admission. Graphs show mean ± SEM. Statistical analysis was performed using two-tailed Mann-Whitney-U test
CCL1 potently discriminates acute pancreatitis and sepsis
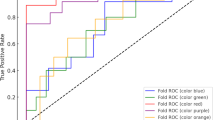
To determine whether Treg-attracting chemokines can serve as diagnostic tools to distinguish between pancreatitis and sepsis, we compared the levels of the chemokines CCL1 and CCL22 between our patient cohorts. All medians and interquartile ranges of these parameters are displayed in Suppl. Table 1. CCL1 was significantly suppressed in acute pancreatitis at all measured time points (Fig. 3). In sepsis, there appears to be a tendency towards elevated CCL1 levels on the first five days, although statistically significant only on day 5. Consequently, acute pancreatitis and sepsis were significantly discriminated by CCL1 levels in the first five days (Fig. 3). CCL22 levels, on the other hand, remain unaffected by inflammation in acute pancreatitis (Suppl. Figure 1). CCL22 levels were significantly suppressed in comparison to controls on days 1 and 3 of sepsis (Suppl. Figure 1), as published previously by our group36 and others37. However, CCL22 was not able to differentiate between acute pancreatitis and sepsis. To further explore the potential diagnostic performance of CCL1, we performed exploratory receiver operating characteristic (ROC) analyses comparing sepsis and acute pancreatitis at the respective time points. CCL1 demonstrated moderate to good discriminative performance, with the highest area under the curve (AUC) observed at day 5 (AUC 0.812), while earlier time points showed lower AUC values (Suppl. Figure 2). However, given the exploratory nature of this study and the limited size of the sepsis cohort, these analyses should be interpreted cautiously.

CCL1 potently discriminates acute pancreatitis and sepsis. CCL1 serum levels of hospitalized controls (control) and patients with pancreatitis and sepsis were determined at the indicated time points after hospital admission. Graphs show mean ± SEM. Statistical analysis was performed using two-tailed Mann-Whitney-U test
Since some baseline characteristics, such as age, smoking status and the presence of coronary heart disease, demonstrated significant differences between our cohorts (see Table 2), we tested all these characteristics for differences in the distribution of serological values. Smokers presented significantly higher PCT values and trended towards increased IL-6 levels (Suppl. Figure 3), while CRP levels were significantly elevated in diabetics (Suppl. Figure 4). In contrast, none of these baseline characteristics was associated with significant differences in serum CCL1 or CCL22 levels (Suppl. Figures 3 and 4). Furthermore, considering the different etiologies of acute pancreatitis and sepsis, we could not identify any correlation leading to significantly different CCL1 or CCL22 levels on the first day of disease in our cohorts (Suppl. Figure 5). Taken together, serum CCL1 levels potently discriminate between acute pancreatitis and sepsis. Additionally, important demographic and medical baseline characteristics did not influence serum CCL1 levels, indicating its applicability in clinical settings.
High CCL1 is associated with less organ failure in sepsis patients
We were further interested whether serum CCL1 is associated with organ failure in sepsis patients. Indeed, CCL1 levels inversely correlate to organ dysfunction, as measured by SOFA score increase at onset in sepsis patients (Fig. 4). Since only one sepsis patient died within the observation period, predictions of the mortality in relation to chemokine levels were not possible. However, we determined the correlation between serum CCL1 and patients’ SOFA score increase on the first day of sepsis as a proxy for the severity of organ failure. Here, serum CCL1 levels inversely correlated with SOFA score increase, meaning that patients with higher CCL1 levels had lower SOFA score increases at disease onset (Spearman r: -0.63, 96% CI -0-87 - -0.16, p = 0.014) (Fig. 4A). Accordingly, the increase of SOFA scores on the first day of sepsis was significantly higher in patients with low CCL1 levels compared to patients with high CCL1 levels (Fig. 4B). In line with this, sepsis patients who were not admitted to an intensive care unit (ICU) or intermediate care unit (IMC) trended towards higher serum CCL1 values than those admitted to ICU or IMC (Fig. 4C). Altogether, serum CCL1 levels correlate with sepsis severity, suggesting a so far unknown biological role of CCL1 in sepsis immune response.

High CCL1 is associated with less organ failure in sepsis patients. (A) CCL1 serum levels and SOFA score increase of sepsis patients at day 1 were determined and plotted against each other. Afterwards, Spearman correlation was performed. (B) Sepsis patients were subdivided into CCL1high and CCL1low patients, according to the median. SOFA increase on day 1 was then determined for both groups. Graph shows mean ± SEM. Statistical analysis was performed using two-tailed Mann-Whitney-U test. (C) CCL1 serum levels in sepsis patients admitted to intermediate care (IMC) or intensive care unis (ICU) and patients treated on normal wards (no IMC/ICU) were determined. Graph shows mean ± SEM. Statistical analysis was performed using two-tailed Mann-Whitney-U test
Discussion
In this prospective biomarker study, we evaluated established inflammatory markers alongside the Treg-attracting chemokines CCL1 and CCL22 in a cohort of 159 patients with sepsis, acute pancreatitis and hospitalized controls. Notably, CCL1 levels showed differing trends between acute pancreatitis and sepsis across all measured timepoints, with discriminative ability progressively improving and reaching its highest level on day 5. Moreover, higher CCL1 levels showed a possible association with reduced early organ dysfunction in sepsis, suggesting a potential prognostic role that requires validation in larger cohorts. Combined with its discriminative ability between sepsis and acute pancreatitis, CCL1 emerges as a candidate biomarker of translational interest.
To our knowledge, systemic CCL1 levels have not previously been studied in patients with sepsis or acute pancreatitis. Previous data have linked elevated CCL1 levels to autoimmune pancreatitis38 and other autoimmune diseases13,20,23,39,40,41, whereas high expression of CCR8, representing the receptor for CCL1, on peripheral blood mononuclear cells (PBMCs), was shown to be associated with severe acute pancreatitis of various etiologies42. The mechanisms underlying the differential regulation of serum CCL1 levels in acute pancreatitis and sepsis in our study remain unclear. Acute pancreatitis is primarily driven by sterile inflammation induced by DAMPs released from injured acinar cells, whereas sepsis is initiated by infection and involves strong PAMP-driven innate immune activation43,44. These distinct upstream signals may generate different chemokine programs. In this context, alveolar macrophages were shown to upregulate CCL1 via Wnt/β-catenin signaling in a murine sepsis model45, a pathway unlikely to be activated in sterile inflammation. Consistent with this, CCL1 was also identified among the chemokines induced by Group B Streptococcus membrane vesicles in a human macrophage cell line upon NLRP3 inflammasome activation46.
Moreover, CCL1 signals through CCR8, which is expressed on regulatory T cells, and CCL1-CCR8 interactions can promote Treg recruitment and suppressive function13. We therefore speculate that reduced circulating CCL1 in acute pancreatitis may reflect reduced systemic induction and/or increased tissue-level consumption of CCL1, whereas higher CCL1 levels in sepsis may reflect stronger immune activation in response to infection-associated stimuli and may be linked to regulatory pathways that modulate excessive inflammation and organ dysfunction. These interpretations remain hypothetical, as this study did not include cellular immune profiling such as PBMC analysis or direct assessment of CCR8 expression and Treg distribution. However, our study is the first to report systemic CCL1 levels in both conditions and to contextualize these findings within an emerging mechanistic framework.
This study reports patients with sepsis and acute pancreatitis along with a large group of hospitalized controls. In the past, controls have often been collected from healthy donors, which might not adequately reflect the inflammatory serum levels in hospitalized patients. Nevertheless, serum CCL1 levels showed notable heterogeneity within the hospitalized control cohort, which may influence the interpretation of circulating chemokine levels and suggests that clinically applicable cut-off values would require validation in larger cohorts. Despite this variability, the inclusion of hospitalized controls provides a more clinically relevant comparison than healthy donors.
Due to its high clinical need, diagnostic parameters to differentiate sepsis from non-infectious inflammation have already been extensively studied in the past. Numerous biomarkers have been evaluated, however the established parameters CRP and PCT often turned out to have the best discriminating potential despite their limitations35. Interpretation of PCT can yet be challenging in certain clinical settings, including advanced kidney disease, major surgery, trauma or other non-infectious inflammatory conditions, where PCT levels may be elevated independently of bacterial infection47. In such situations, additional biomarkers reflecting different aspects of the host immune response may provide complementary diagnostic information. Treg-associated chemokines have not been previously explored in this context. Consistent with the observed differences in circulating CCL1 levels between sepsis and acute pancreatitis, exploratory receiver operating characteristic (ROC) analyses demonstrated moderate to good diagnostic performance of CCL1 for distinguishing both conditions, with the highest AUC observed at day 5. While future diagnostics may rely on multimodal approaches or AI-supported algorithms, evaluation of specific single parameters is essential for healthcare at present. This stresses the translational relevance of CCL1 as discriminating factor in patients with acute pancreatitis and sepsis. In the context of acute pancreatitis, a relevant application could be in biliary pancreatitis, where early identification of concurrent cholangitis is crucial to guide antibiotic use and ERCP5,48. The relatively small number of patients in our sepsis cohort reflects the strict inclusion criteria of this prospective study and limited recruitment during routine clinical practice. Consequently, the present study was not powered for formal diagnostic validation or determination of clinically applicable diagnostic cut-off values, and the ROC analyses should therefore be interpreted as exploratory. Thus, future studies should investigate the utility of CCL1 in this setting.
Tregs, in contrast to their attracting chemokines, have been studied in preclinical pancreatitis models, while findings remain conflicting. A mouse model of acute pancreatitis revealed that depletion of CD4+ T cells surprisingly suppressed disease severity33, an effect attributed to a reduced intrapancreatic Th2 response rather than changes in Treg numbers. In contrast, more recent preclinical data support a protective role of Tregs: Tregs were shown to potently suppress the proinflammatory response in a preclinical model of acute pancreatitis49, and Galectin-3 deficiency was found to attenuate pancreatic injury by promoting intrapancreatic Foxp3 + Treg accumulation and IL-10 production32. Corroborating these experimental findings, a Mendelian randomization study identified resting CD45RA+ Tregs as partial mediators of a genetically determined protective effect against acute pancreatitis31. However, clinical data remain conflicting: whereas elevated Treg numbers in peripheral blood have been associated with less organ failure50, another study reported increased Treg counts specifically in patients with poor outcome51. Pharmacological approaches aimed at enhancing Treg activity, such as Ulinastatin52, which elevates Treg numbers and thereby ameliorates the course of acute pancreatitis, have shown benefit not only in preclinical settings53 but also clinically52. These divergent findings suggest a complex, context-dependent role of Tregs in pancreatitis pathophysiology, both suppressing intrapancreatic and systemic inflammation, but ultimately resulting in possible detrimental immunosuppressive bystander effects. Therefore, the pathogenetic role of the CCL1-CCR8 axis and its impact on local and systemic Treg functionality in acute pancreatitis requires further investigation in preclinical pancreatitis models.
Strikingly, we observed elevated CCL1 levels to be associated with reduced organ dysfunction in sepsis. One possible explanation is that high CCL1 levels reflect effective immune activation due to CCL1 induction upon immune cell activation, supporting bacterial clearance and preventing secondary organ injury. Alternatively, higher CCL1 concentrations may enhance CCR8-dependent recruitment and activation of Treg, thus modulating excessive inflammation and potentially limiting organ injury. This dual interpretation aligns with current literature, where Tregs have been associated with both favorable and unfavorable outcomes in sepsis25,26,27,28,29. It yet remains a compelling observation that CCL1 appears to be relevant for organ function in sepsis, while its blood levels remain unaltered. Functional studies in murine sepsis models as well as human patients regarding Treg distribution and activity are required to answer the mechanistic background of this phenomenon observed in our cohort.
In summary, CCL1 may facilitate clinical reasoning in patients with inflammation and thus contribute to a more precise use of antibiotics in this patient collective. The inverse correlation between CCL1 levels and organ dysfunction in sepsis further suggests a prognostic role, consistent with data indicating a protective function of Tregs during sepsis. Future research yet remains to elucidate the function of CCL1 in systemic inflammation caused by acute pancreatitis and sepsis. An additional promising avenue would be to explore CCL1 as a discriminating biomarker in transplant patients, where differentiation between allograft rejection and infectious complications remains diagnostically challenging. Beyond diagnosis, Tregs and their attracting chemokines may represent druggable targets to attenuate harmful hyperinflammatory responses.
Methods
Study design
We designed a prospective, monocentric, diagnostic study to evaluate Treg-associated chemokines and other laboratory and clinical biomarkers as well as follow-up parameters over the course of seven days after hospital admission. The study design is illustrated schematically in Fig. 1, which was created using BioRender (BioRender.com) and can be accessed using the following link: https://BioRender.com/kb6a9vp.
Three cohorts of patients were included in the study (Table 1): patients with confirmed diagnosis of sepsis, patients with sterile inflammation due to acute pancreatitis and hospitalized control patients with non-inflammatory diseases. Patients with active malignancy, fever of unknown origin and acute coronary syndrome were excluded. Additionally, confirmed infection led to exclusion in case of sterile inflammation as well as controls. Sepsis was defined as confirmed infection (such as pneumonia or cystitis) as well as an increase of SOFA score of at least 2 points, according to the Sepsis-3 consensus guidelines3. Patients in the sepsis and sterile inflammation groups were included within 24 h after hospital admission. Patients’ written informed consent was obtained in all cases.
Blood collection
The first blood collection was performed on the first morning after hospital admission. Blood was collected on day 1, day 3, day 5, day 7 and day 14, unlike the patient was discharged before. Blood from hospitalized controls was collected at two to three timepoints with 48 h interim period in each case.
Measurement of laboratory values and chemokines
Patients’ serum was transferred to the LMU Institute of Laboratory Medicine. C-reactive protein (CRP), interleukin-6 (IL-6) and procalcitonin (PCT) were measured according to routine practice of the institute. Another part of the patients’ serum was aliquoted and frozen at − 80 °C. Subsequently, CCL1 and CCL22 serum levels were determined by ELISA according to the manufacturer’s protocols (Human CCL1/I-309 DuoSet ELISA #DY272, Human CCL22/MDC DuoSet ELISA #DY336, both R&D Systems). For patients in the control cohort, all serologic parameters were measured on at least two separate time points with an interval of at least 48 h, and mean values of all measured time points were created to obtain control values for serologic markers.
Documentation of clinical data
Along with the blood collection, clinical data of patients was documented pseudonymized on days 1, 3, 5, 7, where applicable, in an electronic case report form (eCRF) provided by the Institute of Laboratory Medicine.
Statistics
Statistical analysis was performed using Microsoft Office Excel (Version 16.75.2) as well as R (Version 4.3.1), R Studio (Version 2023.06.0 + 421) and GraphPad Prism Version 10. The following R packages were used: tidyverse, readxl, dplyr, lubridate, writexl, ggplot2, ggpubr, ggsignif, nnet, and pROC. Significance was determined by Wilcoxon test, unless otherwise specified. The measured values of controls were tested for significant inter-individual differences using a two-tailed Student’s t test and since not significant, individual means were calculated and taken as control values. Statistical significance was defined as follows: * = p < 0.05, ** = p < 0.01, *** = p < 0.001 and **** = p < 0.0001. Receiver operating characteristic (ROC) curve analysis was performed to assess the discriminatory performance of serum CCL1 between sepsis and acute pancreatitis at days 1, 3 and 5. Sepsis was defined as the positive outcome and acute pancreatitis as the negative outcome. Area under the curve (AUC) values were calculated for each timepoint.
Ethics
The study was reviewed and approved by the LMU ethics committee on December 12th, 2018 (internal record 698 − 16). All participants provided informed consent prior to participation in the study.
Data availability
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request. Data will be provided in anonymized form to protect participant confidentiality.
Abbreviations
- CCL1:
-
Chemokine (CC motif) ligand 1
- CCL22 :
-
Chemokine (CC motif) ligand 22
- CRP C:
-
Reactive protein
- ELISA :
-
Enzyme linked immunosorbent assay
- ICU:
-
Intensive care unit
- IMC:
-
Intermediate care unit
- IL-6:
-
Interleukin-6
- MDC:
-
Macrophage-derived chemokine, alternate name for CCL22
- PCT:
-
Procalcitonin
- SOFA:
-
Sepsis-related organ failure assessment
- Treg:
-
Regulatory T-cell
References
Rudd, K. E. et al. Global, regional, and national sepsis incidence and mortality, 1990–2017: analysis for the Global Burden of Disease Study. Lancet 395 (10219), 200–211 (2020).
Iannuzzi, J. P. et al. Global Incidence of Acute Pancreatitis Is Increasing Over Time: A Systematic Review and Meta-Analysis. Gastroenterology 162 (1), 122–134 (2022).
Singer, M. et al. The Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). Jama 315 (8), 801–810 (2016).
Sternby, H. et al. Determinants of Severity in Acute Pancreatitis: A Nation-wide Multicenter Prospective Cohort Study. Ann. Surg. 270 (2), 348–355 (2019).
Beyer, G. et al. S3-Leitlinie Pankreatitis (Deutsche Gesellschaft für Gastroenterologie, Verdauungs- und Stoffwechselkrankheiten e.V. (DGVS), 2021).
Lankisch, P. G., Apte, M. & Banks, P. A. Acute Pancreat. Lancet, 386(9988): 85–96. (2015).
Cecconi, M. et al. Sepsis and septic shock. Lancet 392 (10141), 75–87 (2018).
Ohkura, N., Kitagawa, Y. & Sakaguchi, S. Development and maintenance of regulatory T cells. Immunity 38 (3), 414–423 (2013).
Vignali, D. A., Collison, L. W. & Workman, C. J. How regulatory T cells work. Nat. Rev. Immunol. 8 (7), 523–532 (2008).
Huehn, J., Beyer, M. & Corthay, A. Epigenetic and transcriptional control of Foxp3 + regulatory T cells. How do regulatory T cells work? Semin Immunol. 27 (1), 10–18 (2015).
Griffith, J. W., Sokol, C. L. & Luster, A. D. Chemokines and chemokine receptors: positioning cells for host defense and immunity. Annu. Rev. Immunol. 32, 659–702 (2014).
Iellem, A. et al. Unique chemotactic response profile and specific expression of chemokine receptors CCR4 and CCR8 by CD4(+)CD25(+) regulatory T cells. J. Exp. Med. 194 (6), 847–853 (2001).
Gombert, M. et al. CCL1-CCR8 interactions: an axis mediating the recruitment of T cells and Langerhans-type dendritic cells to sites of atopic skin inflammation. J. Immunol. 174 (8), 5082–5091 (2005).
Yoshie, O. & Matsushima, K. CCR4 and its ligands: from bench to bedside. Int. Immunol. 27 (1), 11–20 (2015).
Piseddu, I. et al. Constitutive Expression of CCL22 Is Mediated by T Cell-Derived GM-CSF. J. Immunol. 205 (8), 2056–2065 (2020).
Wiedemann, G. M. et al. Cancer cell-derived IL-1α induces CCL22 and the recruitment of regulatory T cells. Oncoimmunology 5 (9), e1175794 (2016).
Anz, D. et al. Suppression of intratumoral CCL22 by type i interferon inhibits migration of regulatory T cells and blocks cancer progression. Cancer Res. 75 (21), 4483–4493 (2015).
Bischoff, L. et al. Cellular mechanisms of CCL22-mediated attenuation of autoimmune diabetes. J. Immunol. 194 (7), 3054–3064 (2015).
Dogan, R. N. et al. CCL22 regulates experimental autoimmune encephalomyelitis by controlling inflammatory macrophage accumulation and effector function. J. Leukoc. Biol. 89 (1), 93–104 (2011).
Kim, H. O. et al. Expression of CCL1 and CCL18 in atopic dermatitis and psoriasis. Clin. Exp. Dermatol. 37 (5), 521–526 (2012).
Warford, J. et al. Human Brain Chemokine and Cytokine Expression in Sepsis: A Report of Three Cases. Can. J. Neurol. Sci. 44 (1), 96–104 (2017).
Asai, A. et al. CCL1 released from M2b macrophages is essentially required for the maintenance of their properties. J. Leukoc. Biol. 92 (4), 859–867 (2012).
Zen, Y. et al. Possible involvement of CCL1-CCR8 interaction in lymphocytic recruitment in IgG4-related sclerosing cholangitis. J. Hepatol. 59 (5), 1059–1064 (2013).
Rapp, M. et al. CCL22 controls immunity by promoting regulatory T cell communication with dendritic cells in lymph nodes. J. Exp. Med. 216 (5), 1170–1181 (2019).
Jia, W. et al. Regulatory T cells are protective in systemic inflammation response syndrome induced by zymosan in mice. PLoS One. 8 (5), e64397 (2013).
Tatura, R. et al. Relevance of Foxp3(+) regulatory T cells for early and late phases of murine sepsis. Immunology 146 (1), 144–156 (2015).
Chen, K. et al. Prognostic value of CD4(+)CD25(+) Tregs as a valuable biomarker for patients with sepsis in ICU. World J. Emerg. Med. 6 (1), 40–43 (2015).
Huang, H. et al. High circulating CD39(+) regulatory T cells predict poor survival for sepsis patients. Deregulation of T cell response in sepsis. Int. J. Infect. Dis. 30, 57–63 (2015).
Ono, S. et al. Removal of increased circulating CD4 + CD25+Foxp3 + regulatory T cells in patients with septic shock using hemoperfusion with polymyxin B-immobilized fibers. Surgery 153 (2), 262–271 (2013).
Stier, M. T. et al. Metabolic adaptations rewire CD4(+) T cells in a subset-specific manner in human critical illness with and without sepsis. Nat. Immunol. 27 (2), 236–249 (2026).
Milivojcevic Bevc, I. et al. Redefining Immune Dynamics in Acute Pancreatitis: The Protective Role of Galectin-3 Deletion and Treg Cell Enhancement. Biomolecules, 14(6). (2024).
Zhang, H. et al. The m6A regulatory gene YTHDF3 alleviates acute pancreatitis by modulating CD45RA+ resting treg cells: A novel immunomodulatory biomarker. Med. (Baltim). 104 (37), e44443 (2025).
Glaubitz, J. et al. Experimental pancreatitis is characterized by rapid T cell activation, Th2 differentiation that parallels disease severity, and improvement after CD4(+) T cell depletion. Pancreatology 20 (8), 1637–1647 (2020).
Faix, J. D. Biomarkers of sepsis. Crit. Rev. Clin. Lab. Sci. 50 (1), 23–36 (2013).
Pierrakos, C. et al. Biomarkers of sepsis: time for a reappraisal. Crit. Care. 24 (1), 287 (2020).
Piseddu, I. et al. Innate Immune Activation Is a Strong Suppressor of CCL22 and Impedes Regulatory T Cell-Dendritic Cell Interaction (Immunology, 2025).
Bergersen, K. V. et al. Early cytokine signatures and clinical phenotypes discriminate persistent from resolving MRSA bacteremia. BMC Infect. Dis. 25 (1), 231 (2025).
Seleznik, G. M. et al. Lymphotoxin β receptor signaling promotes development of autoimmune pancreatitis. Gastroenterology 143 (5), 1361–1374 (2012).
Komatsu, M. et al. The utility of serum C-C chemokine ligand 1 in sarcoidosis: A comparison to IgG4-related disease. Cytokine 133, 155123 (2020).
Hao, S. et al. A novel polypeptide molecule attenuates atopic dermatitis by targeting CCR8-CCL1 axis. Int. Immunopharmacol. 170, 116051 (2026).
Sha, J. et al. Interaction between nasal epithelial cells and Tregs in allergic rhinitis responses to allergen via CCL1/CCR8. Front. Immunol. 16, 1526081 (2025).
Nalisa, M. et al. Chemokine receptor 8 expression may be linked to disease severity and elevated interleukin 6 secretion in acute pancreatitis. World J. Gastrointest. Pathophysiol. 12 (6), 115–133 (2021).
Chen, G. Y. & Nuñez, G. Sterile inflammation: sensing and reacting to damage. Nat. Rev. Immunol. 10 (12), 826–837 (2010).
Wiersinga, W. J. & van der Poll, T. Immunopathophysiology Hum. sepsis EBioMedicine, 86: 104363. (2022).
Xie, B. et al. Gut-derived memory γδ T17 cells exacerbate sepsis-induced acute lung injury in mice. Nat. Commun. 15 (1), 6737 (2024).
McCutcheon, C. R. et al. Group B Streptococcal Membrane Vesicles Induce Proinflammatory Cytokine Production and Are Sensed in an NLRP3 Inflammasome-Dependent Mechanism in a Human Macrophage-like Cell Line. ACS Infect. Dis. 11 (2), 453–462 (2025).
Schuetz, P., Albrich, W. & Mueller, B. Procalcitonin for diagnosis of infection and guide to antibiotic decisions: past, present and future. BMC Med. 9, 107 (2011).
Miura, F. et al. Tokyo Guidelines 2018: initial management of acute biliary infection and flowchart for acute cholangitis. J. Hepatobiliary Pancreat. Sci. 25 (1), 31–40 (2018).
Glaubitz, J. et al. Activated regulatory T-cells promote duodenal bacterial translocation into necrotic areas in severe acute pancreatitis. Gut 72 (7), 1355–1369 (2023).
Wang, W. et al. CD4 + CD25 + CD127 high cells as a negative predictor of multiple organ failure in acute pancreatitis. World J. Emerg. Surg. 12, 7 (2017).
Minkov, G. A., Yovtchev, Y. P. & Halacheva, K. S. Increased Circulating CD4 + CD25+CD127low/neg Regulatory T-cells as a Prognostic Biomarker in Acute Pancreatitis. Pancreas 46 (8), 1003–1010 (2017).
Bandyopadhyay, S., Samajdar, S. S. & Das, S. Ulinastatin for the treatment of severe acute pancreatitis: a systematic review and meta-analysis. BMC Gastroenterol. 25 (1), 629 (2025).
Pan, Y. et al. Ulinastatin ameliorates tissue damage of severe acute pancreatitis through modulating regulatory T cells. J. Inflamm. (Lond). 14, 7 (2017).
Funding
Open Access funding enabled and organized by Projekt DEAL. This study was supported by grants from the Deutsche Forschungsgemeinschaft (SFB TRR355, to D.A.; SFB TRR338 and SFB TRR237, personnel costs to I.P.), the Bavarian Cancer Research Center (personnel costs, to I.P.), the Friedrich-Baur-Stiftung (Nr. 36/22, to I.P. and D.A.), the LMU intramural doctoral program “FöFoLe” (to I.P. and D.A.), the Else Kröner-Fresenius-Stiftung (IOLIN and 2025_EKEA.16, to I.P.), the Medical Faculty of the LMU Munich (intramural funding, to I.P.), and the Novartis Foundation (InCa prize, to I.P.). The funders did not participate in the design of the study, the data collection and analysis, nor in the interpretation of the data or writing of the manuscript.
Author information
Authors and Affiliations
Contributions
MV, JM and DA designed the study. MV consented the patients. JM and LH collected patient samples and information. CP, JG, AB, PW and LH analyzed patient samples. MV, JM and IP analyzed the data. MV, IP and DA interpreted the data and wrote the manuscript. All authors critically reviewed and approved the final version of the manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study was reviewed and approved by the LMU ethics committee on December 12th, 2018 (internal record 698 − 16). All participants provided informed consent prior to participation in the study. The research was conducted in accordance with the Declaration of Helsinki and applicable regulatory requirements.
Competing interests
The authors declare no competing interests.
Data availabilitiy
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request. Data will be provided in anonymized form to protect participant confidentiality.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Vornhülz, M., Müller, J., Takken, L.L. et al. Serum CCL1 discriminates infectious and sterile systemic inflammation in sepsis and acute pancreatitis. Sci Rep 16, 14391 (2026). https://doi.org/10.1038/s41598-026-47750-w
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-026-47750-w
