
Abstract
Parkinson’s disease, cognitive impairment, and multiple sclerosis are neurodegenerative conditions contributing to a huge health burden globally. Virtual reality rehabilitation has emerged as a promising intervention, but its comparative effectiveness across different types of neurodegenerative conditions must be further elucidated. Relevant studies were retrieved from the PubMed database, Cochrane Library, and Web of Science Core Collection database. Randomized controlled trials, meta-analyses, and systematic reviews investigating virtual reality interventions for neurodegenerative diseases were incorporated and evaluated. Following a thorough, methodical, and systematic screening process, 99 high-quality studies were ultimately incorporated. The findings corroborate the efficacy of immersive, semi-immersive, and non-immersive virtual reality interventions in cognitive and motor rehabilitation for patients with neurodegenerative diseases. Virtual reality rehabilitation shows great potential in improving motor function, cognitive function, and quality of life in patients with neurodegenerative diseases. Future research should focus on standardizing protocols and exploring the underlying neurobiological mechanisms to optimize its clinical use.
Similar content being viewed by others

Introduction
Neurodegenerative diseases are a class of chronic conditions characterized by a progressive loss of brain cells and their connections, involving the sustained and gradual degeneration of specific vulnerable neuronal populations in the brain or spinal cord. These conditions are classified according to their major clinical presentations as follows: Alzheimer’s disease (AD) and related dementias, Parkinson’s disease (PD), multiple sclerosis (MS), amyotrophic lateral sclerosis, spinocerebellar ataxias, and motor neuron disorders1. Neurodegenerative diseases persistently damage the brain, spinal cord, or peripheral nerves, adversely affecting cognition, sensation, socioemotional processing, motor function, and behaviour2. The complexity of these diseases and their extensive impact on neurological functions contribute to their growing societal burden.
The 2021 Global Burden of Disease study revealed that the increasing rate of neurological disorders is worsened by population aging. It also highlighted that over the past decade, the proportion of people aged 55 years and older living with disabilities due to PD and AD has continued to rise globally, with over 55 million people living with AD3,4. The World Health Organization projected that neurodegenerative diseases will become the second leading cause of death in developed nations by 2040, surpassed only by cardiovascular diseases5. The total global cost of dementia exceeded 1.3 trillion USD in 2019, far exceeding the capacity of healthcare systems6. By 2030, the global financial burden of dementia is estimated to rise to over 2.8 trillion USD, as reported by the official website of the World Health Organization. In the European Union, neurological disorders ranked third after cardiovascular diseases and cancers representing 13.3% (10.3–17.1) of total disability-adjusted life-years and 19.5% (18.0–21.3) of total deaths7. Moreover, patients with neurodegenerative diseases frequently exhibit a marked decline in quality of life, and caregivers confront a range of emotional, economic, and social challenges8. These increasing problems underscore the pressing need for novel, effective treatment modalities to support these conditions9.
Traditional pharmacotherapies and conventional rehabilitation for neurodegenerative diseases have shown modest benefits10, but they also have some limitations, such as high costs, low engagement, and poor compliance. These shortcomings collectively drive the need for more innovative, engaging, and accessible treatment approaches. To address these challenges, virtual reality (VR) rehabilitation has gradually been introduced into clinical practice, and its efficacy has been supported by clinical research11,12. By simulating real-life scenarios, VR technology carries therapeutic skills into daily life to enhance patient engagement and provide meaningful feedback. Within the virtual environment, the combined physical and cognitive demands closely mirror the real-world complexity that challenges patients with neurodegenerative diseases. VR systems are highly customizable, enabling therapists to tailor task difficulty to the individual’s evolving capabilities, thereby optimizing the challenge level and promoting neuroplasticity. Moreover, the gamified nature of VR rehabilitation enhances patient motivation, adherence, and enjoyment, overcoming the drawbacks of traditional repetitive exercises.
According to the immersion and presence levels13, VR systems are classified into: a. immersive VR uses head-mounted displays to create interactive synthetic environments with sensory feedback, offering moderate-to-high immersion and high presence at variable costs; b. non-immersive VR employs standard screens for cost-effective solutions such as home rehabilitation; c. semi-immersive VR, which offers greater accessibility and adherence potential, typically combines high-resolution three-dimensional projections on large screens with stereoscopic sound, enabling patients to remain aware of their physical surroundings with moderate sense of presence. Presence is created by task design, communication, and mental involvement. Each VR type serves distinct clinical purposes based on treatment objectives and patient requirements14,15. Higher levels of immersion and presence not only enhance motivation but also improve emotional regulation and foster neuroplasticity16.
VR has emerged in neurorehabilitation as an engaging, interactive, patient-centred, and relatively cost-effective tool that enhances functional recovery17. Studies have confirmed that VR rehabilitation has benefits in strength, balance, and walking ability for patients with PD and MS18,19,20,21,22,23. Besides, VR interventions were effective for regaining upper limb capabilities in patients with MS19,24. VR-based physical and cognitive training substantially improved cognitive function, daily function, and neural efficiency in patients with cognitive impairment (CI)25. Even a short and structured VR intervention can effectively provide emotional well-being in patients with mild CI12. However, the extant literature is constrained by patient heterogeneity, technology disparity, and a narrow range of outcomes, and therefore cannot systematically summarize the comprehensive impact of VR rehabilitation on neurodegenerative diseases. Moreover, existing reviews predominantly study the effects of VR on the motor function in a certain type of neurodegenerative disease, lacking comparisons of therapeutic effects among different types of neurodegenerative conditions and exploration of the therapeutic mechanisms. The present study aimed to systematically evaluate the efficacy of VR rehabilitation for neurodegenerative diseases and to provide the mechanistic insights of VR rehabilitation. This systematic review particularly focused on the various benefits of VR rehabilitation at different levels of immersion and presence for patients with neurodegenerative diseases, such as motor function, cognitive function, mood, and quality of life.
Results
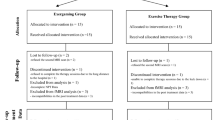
A preliminary search identified 560 articles on PD, 1483 articles on CI, and 419 articles on MS as relevant. Following the removal of duplicates, 1198 titles and abstracts were screened. Further review of 1264 full-text articles was conducted, and the final analysis yielded 20 studies on PD, 43 studies on CI, and 36 studies on MS (Fig. 1). Finally, our research team comprehensively evaluated and synthesized 28 systematic reviews and meta-analyses together with 31 RCTs. The designs and results of the studies included in the final review are listed in Tables 1 and 2.

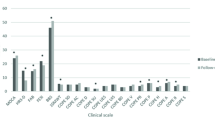
PD Parkinson’s disease, CI cognitive impairment, MS multiple sclerosis.
Among the 31 RCTs included in this study, the VR interventions were classified according to their type as immersive, semi-immersive, and non-immersive VR interventions. Immersive VR interventions had only been implemented in RCTs involving individuals with CI, but not in those with PD or MS. None of the included meta-analyses conducted differentiated analyses among immersive, semi-immersive, and non-immersive VR interventions. Hence, meta-analytic findings regarding CI are presented in the immersive VR intervention section, and those for PD and MS are presented in the semi-immersive VR intervention section.
Immersive VR intervention for neurodegenerative diseases
Immersive VR intervention was principally employed in research involving patients with CI. The principal indicators for evaluating the efficacy of immersive VR rehabilitation were the temporal motor test, Korean cognitive assessment, and Montreal cognitive assessment (MoCA). The primary function of these tests is to assess cognitive function in patients with CI. Four RCTs and 12 meta-analyses were included.
Three RCTs compared immersive VR cognitive training with conventional methods25,26,27, showing a significant higher score on the Korean cognitive assessment in the VR groups (MD = 2.23, P = 0.01)26. VR training also effectively reduced depression scores (MD = -1.70, P < 0.001) and improved daily living skills, such as shopping and financial management (MD = 1.77, P = 0.006)25. The VR groups significantly improved executive function (MD = 26.88, P = 0.032) and increased step frequency during multitasking (MD = -0.08, P = 0.018), indicating enhanced information processing capacity27. Baldimtsi et al.28 found that VR intervention was superior to bicycle exercise for overall cognition with medium effect (0.06 < η²p < 0.14, P = 0.006), particularly in verbal learning, memory strategies, and short-term recall. VR therapy significantly boosted executive function and task-switching with medium effect (0.06 < η²p < 0.14, P = 0.016) compared with baseline28. These findings suggest that immersive VR rehabilitation training substantially enhances cognitive function of patients with CI.
Three meta-analyses reported that immersive VR rehabilitation had a beneficial effect on patients’ memory function29,30,31. Yu et al. found that the VR group had better short-term memory than the control group (MD = 0.64, 95% CI [0.25, 1.03], P = 0.001)29. A 2020 meta-analysis also established that immersive VR rehabilitation significantly enhanced patients’ overall cognitive function (SMD = 0.87, 95% CI [0.33, 1.40], P = 0.002) and executive function (SMD = 1.08, 95% CI [0.13, 2.03], P = 0.025)30. Immersive VR rehabilitation significantly enhanced patients’ grip strength (SMD = 0.35, 95% CI [0.01, 0.69], P = 0.05) and balance function (SMD = 0.79, 95% CI [0.13, 1.45], P = 0.02)31.
Semi-immersive VR intervention for neurodegenerative diseases
In patients with PD, the clinical effectiveness of semi-immersive VR therapy was primarily measured through three key assessment tools: the Unified Parkinson’s Disease Rating Scale (UPDRS) for comprehensive motor symptom evaluation, the Boston Balance Scale (BBS) for balance control, and the Timed Up and Go Test (TUG) for dynamic balance and functional gait ability. Evidence from five RCTs and eight meta-analyses focusing on semi-immersive VR interventions was incorporated in the analysis. Feng et al. showed that the semi-immersive VR group achieved better balance than the traditional rehabilitation group, especially in dynamic balance (MD = 4.14, P < 0.05)32. The VR group also showed greater walking ability improvement (MD = 0.58, P < 0.05) and higher UPDRS-III scores (MD = 0.28, P < 0.05)32. Another study found that combining VR with neurodevelopmental therapy and electrical stimulation further improved static and dynamic balance (MD = 1.70, P < 0.05), daily living skills (MD = 2.40, P < 0.05), and reduced depression (MD = -1.60, P < 0.05)33. These results confirm VR therapy’s clinical value in neurological rehabilitation. Seven meta-analyses demonstrated that the VR intervention group exhibited a significantly enhanced balance ability compared with the control group34,35,36,37,38,39,40. Moreover, the walking function of the VR intervention group was significantly enhanced compared with that of the control group (MD = −1.66, 95% CI [−2.74, −0.58], P = 0.003)40.
In patients with CI, the principal indicators for evaluating the efficacy of semi-immersive VR rehabilitation include executive function and MoCA, which were used to assess cognitive function. Three RCTs were included in the analysis. Compared with the treadmill training group, the VR intervention combined with the treadmill training group demonstrated significant advantages in multiple domains, including running speed, obstacle crossing ability, attention, executive function, lower limb function, and balance ability20. VR cognitive training group exhibited superior cognitive flexibility, visual–motor tracking ability (MD = 2.70, P = 0.045), information processing ability, visual attention ability (MD = -6.10, P = 0.039), information execution ability, task switching ability (MD = −6.20, P = 0.04), and short-term auditory memory capacity and attention span (MD = 1.10, P = 0.011) compared with the traditional cognitive training group41.
In patients with MS, the principal measures for evaluating the efficacy of semi-immersive VR therapy were Beck Depression Inventory, TUG, and MoCA. Seven semi-immersive RCTs and nine meta-analyses were included in the analysis. Compared with the conventional physical rehabilitation group, the semi-immersive VR rehabilitation group exhibited superior outcomes in terms of overall balance ability (MD = 6.28, P < 0.05), vestibular system function (MD = 16.31, P < 0.05), motor control ability, and response to sudden disturbances (MD = 13.16, P < 0.05)42. The benefits of semi-immersive VR rehabilitation were remarkably evident in specific balance assessments (MD = 2.13, P = 0.03)43 and fall risk management (MD = 2.10, P = 0.009)44. Patients receiving VR intervention reduced fall anxiety (MD = 2.70, P = 0.021)44, and accelerated upper limb muscle strength recovery (MD = 1.68, P = 0.004) compared with those receiving conventional cognitive rehabilitation45. In addition, the semi-immersive VR group exhibited marked benefits in the improvement of cognitive dysfunction (MD = 1.50, P < 0.001), depression risk (MD = −2.00, P < 0.001), and visual memory retention (MD = 2.80, P = 0.008)46. There are two additional studies that support this conclusion47,48. A meta-analyses suggested that the balance improvement of the VR intervention group was superior to that of the conventional exercise group49. Another study reported that VR intervention was more effective in enhancing balance ability compared with no intervention (SMD = 0.94, 95% CI [0.21, 1.87], P = 0.02), and also indicated that the enhancement in walking ability of the VR rehabilitation group were superior to those of the conventional exercise group50.
Non-immersive VR intervention for neurodegenerative diseases
The effectiveness of non-immersive VR therapy on patients with PD was evaluated using multiple standardized measures: UPDRS for motor symptoms, BBS for daily living activities, TUG for mobility, Parkinson’s disease quality of life questionnaire for the assessment of quality of life, and 6-minute walk test for walking capacity. This evaluation incorporated data from three RCTs that investigated non-immersive VR interventions, the results revealed that VR rehabilitation was superior to traditional training in improving both static and dynamic balance and reducing fall risk51,52,53.
In patients with CI, the effectiveness of non-immersive VR rehabilitation for cognitive impairment was primarily assessed through two key measures: Korean-Executive Function Performance Test and Korean-Instrumental Activities of Daily Living Scale, which evaluate cognitive function and daily living activities respectively. Findings from two RCTs examining these outcomes were included in the analysis. Choi et al54. found that VR-based yoga exercises significantly enhanced walking function (MD = 1.05, P < 0.001) and balance function (MD = 3.83, P < 0.001) compared with the conventional yoga exercises. The magnitude of these effects was substantial with large effect sizes (η²p > 0.14). Furthermore, the VR-based traditional exercise group showed superior performance in independent living ability (MD = 2.68, P < 0.001) and executive function (MD = 9.94, P < 0.001) compared with the no-intervention control group55.
In patients with MS, the primary measures for evaluating the efficacy of non-immersive VR therapy included the Purcell–Purcell Test (PPT) for hand fine motor coordination, Center for Depression and Anxiety Scale (CES) for depressive symptoms, and Mini-Balance Evaluation Systems Test for balance function. Seven RCTs were included in the analysis. Two RCTs studies demonstrated that VR-based rehabilitation training exhibited significant advantages in multiple hand function indicators over traditional rehabilitation training56,57. The VR intervention group demonstrated enhanced fine motor ability in the affected hand (MD = 1.67, P = 0.032)56. Compared to the control group, the experimental group showed significant improvements in the following domains: bilateral coordination and cooperative work ability (MD = 5.34, P = 0.019), hand function and cognitive–motor integration ability in complex assembly tasks (MD = 7.01, P = 0.008), and dexterity and movement speed of the affected hand (MD = 6.00, P = 0.036)56. Another study established that the VR traditional rehabilitation group exhibited superior outcomes in dynamic sitting balance and trunk adjustment ability, and motor coordination ability compared with the telephone-based remote rehabilitation group58. These findings collectively support the promotional role of VR technology in motor function rehabilitation from multiple perspectives, highlighting its consistent advantages across critical functional indicators, including fine motor skills, coordination, and balance.
Reporting bias assessment
A total of 31 RCTs were included in this study, and their methodological quality was evaluated using the PEDro scale (Supplementary Information). The results showed that 23 studies (74.2%) were rated as high quality (score ≥ 7), and 8 studies (25.8%) were rated as moderate quality (score 4–6). No studies were identified as low quality (score ≤ 3). Overall, the methodological quality of the included RCTs was relatively high, indicating satisfactory performance in aspects such as random allocation, baseline comparability, and outcome reporting. However, the main reasons for lower scores in some studies included: lack of implementation or reporting of allocation concealment, inadequate blinding (particularly of subjects and therapists), and absence of intention-to-treat analysis. These factors are common in rehabilitation-related RCTs, where the nature of the interventions (e.g., physical therapy, exercise training) presents practical challenges to implementing complete blinding59. Figure 2 shows visually presents the risk of bias in the included RCTs.

A Trials included participants with Parkinson’s disease. B Trials included participants with cognitive impairment. C Trials included participants with multiple sclerosis.
This study employed the AMSTAR tool to assess systematic reviews and meta-analyses. A total of 28 studies were included and rated as high quality with AMSTAR scores ranging from 8 to 11 (the highest score). The details are provided in Supplementary Information. Most studies that scored below 11 lost points in the item related to grey literature search, which was rated as “No” or “Can’t Answer”. The absence of grey literature may lead to publication bias, affecting the comprehensiveness and representativeness of the results. In addition, some studies did not use methods such as funnel plots or Egger’s regression to assess publication bias, which may result in an overestimation of the intervention effects.
Discussion
This review evaluated the effectiveness of VR rehabilitation in patients with neurodegenerative diseases, providing a comprehensive analysis of the application of VR rehabilitation in neurodegenerative diseases. A total of 99 studies were included, and VR rehabilitation was mainly applied to patients with PD, CI, or MS. This study demonstrates that immersive VR rehabilitation has benefits in improving cognitive function, alleviating depression risk, and enhancing task execution ability and short-term memory capacity in patients with CI. Semi-immersive VR rehabilitation improves dynamic balance and gait in patients with PD or MS, reduces depression risk in patients with MS, and enhances attention and information-processing ability in patients with CI. Non-immersive VR rehabilitation also improves balance and gait in patients with PD or CI, and enhances physical coordination in patients with MS. Collectively, VR-based interventions exert clinically meaningful benefits across neurodegenerative conditions.
Our study summarized the four most important mechanisms of VR intervention in the treatment of neurodegenerative diseases, as illustrated in Fig. 3. Based on the functional neuroimaging techniques, long-term cognitive training through VR interventions has been proven to effectively activate specific cortical regions involved in cognitive function60. In addition, semi-immersive VR systems can simulate visual and proprioceptive feedback during actual gait. This intervention method has been shown to improve the brain circuit function associated with neurodegenerative diseases (Fig. 3A), including the mesocortical, limbic, and corticobasal ganglia circuits61. Calabrò et al. used electroencephalographic technology to demonstrate that VR rehabilitation can engage several brain areas involved in motor planning and learning, thereby enhancing motor performance62.

Potential therapeutic mechanisms of virtual reality rehabilitation on neurodegenerative diseases.
Immersive VR intervention provides real-time stimulation through multisensory modalities (including visual, auditory, tactile, olfactory, and gustatory inputs), enhancing participants’ sense of reality within the VR environment. This technology can accurately discern the interaction between visual and vestibular systems, thereby facilitating precise evaluations of balance ability63,64. The utilization of visual or auditory stimuli in a VR context has alleviated symptoms of freezing gait in patients with PD. Patients with PD exhibit a high degree of dependence on visual cues. The utilization of visual and auditory stimuli has been demonstrated to enhance patients’ attention, bringing to an improvement in motor function65.
In VR rehabilitation, the incorporation of gamified design and multisensory feedback has been instrumental in creating a rehabilitation experience that is enjoyable and challenging for patients with neurodegenerative diseases. VR-based rehabilitation training can substantially enhance coordination, balance, and gait in patients with neurodegenerative diseases (Fig. 3B). Through high-precision motion capture and real-time feedback systems, VR technology can provide personalized training that target core motor deficits such as gait and balance61,66,67,68,69. Immersive VR environments can simulate walking on different terrains to assist patients in restoring normal gait patterns, thereby significantly enhancing lower limb coordination in patients with moderate-to-severe balance disorders. Grounded in its immersive training scenarios, VR rehabilitation can customize training scenarios (e.g., obstacle avoidance and dual-task training) for patients with neurological disorders to enhance motor–cognitive coordination70,71. Clinical studies demonstrated that this adjustable-scenario VR training model is more effective than fixed-mode or single-scenario task training71,72,73.
Emotional factors represent a pivotal class of internal factors that significantly influence the mental state of patients diagnosed with PD. Negative emotions exert a substantial detrimental influence on the rehabilitation of patients with neurodegenerative diseases. Highly immersive VR systems effectively modulate emotions, reducing maladaptive negative affects like anxiety and fear while enhancing motivation and engagement in rehabilitation training74. This enhanced sense of reality promotes emotional expression, thereby enhancing patients’ motivation to engage in training63. The flow state holds particular significance in the rehabilitation of patients diagnosed with PD. In the flow state, patients experience intrinsic pleasure and satisfaction, which stimulates dopamine release75. As a key neurotransmitter, dopamine regulates emotions and maintains dynamic balance in patients with PD76. The occurrence of flow state depends on task complexity and individual skill, and VR technology precisely adjusts difficulty to keep patients in an optimal flow state and boost compliance, especially in older or reluctant patients77.
The regulation of the dopamine system is closely related to the treatment of PD. Current pharmacological treatment for PD centers on dopaminergic drugs that increase brain dopamine levels78. Dysregulation of the dopaminergic system is associated with poor prognosis in patients with MS79. Reduced dopamine transporter availability is linked to cognitive decline in patients with CI80. Therefore, dopamine levels play a crucial role in the prognosis of neurodegenerative diseases. Positive emotions can promote the generation of dopamine neurons, thereby increasing dopamine levels in the brain81. Cycling exercise has been found to stimulate dopamine release in the caudate nucleus of patients with PD82. Treadmill training can enhance neuroplasticity in dopaminergic signalling, thus improve early symptoms of PD83. Researchers have also observed enhanced dopaminergic signalling in mice subjected to moderate-intensity treadmill exercise84. Therefore, VR-based training could also benefit neurodegenerative diseases by increasing dopamine levels (Fig. 3C). VR integrated with exercise training is pivotal in enhancing neuroprotection and neuroplasticity. One study revealed that VR-based exercise elicits significantly greater increases in brain-derived neurotrophic factor to promote neuroplasticity and the survival of dopamine neurons compared with conventional physical training85.
Neuroinflammation mechanisms are a common pathological basis for various neurodegenerative diseases. Aberrant microglial activation can instigate a sustained neuroinflammatory cascade reaction86. This chronic inflammatory state results in neuronal dysfunction and structural damage to the blood–brain barrier87. Within this pathological milieu, abnormal protein aggregation and mitochondrial dysfunction occur and form a vicious cycle that ultimately results in irreversible neuronal damage88. Immunomodulatory therapy can notably delay disease progression89.
Exercise alleviates oxidative stress and neuroinflammation while promoting protective factors to regulate microglia activity and reduce β-amyloid deposition, thereby exerting neuroprotective effects90. The regular undertaking of rehabilitation exercises can assist in the reduction of systemic inflammatory factors, including interleukin-6 and tumour necrosis factor (Fig. 3D)91. Appropriate exercise benefits the immune system. VR-based rehabilitation allows precise control of exercise intensity, maximizing therapeutic gains while eliminating the overexertion risks common in conventional training.
Despite the continuous growth in the number of clinical studies exploring VR rehabilitation for neurodegenerative diseases, there are limitations that need to be taken into account. Firstly, the effectiveness of VR rehabilitation possibly depends on the disease stage, with early intervention offering good functional outcomes. However, the ideal timing and intensity of VR therapy remain unclear. Secondly, meta-analyses sometimes include low-quality clinical trials, which may weaken the reliability of the findings. This phenomenon highlights the need for strict study designs and high research standards. Thirdly, studies often use different VR devices, introducing technical variability that hampers the generalizability of results. Standardizing VR equipment and intervention protocols would improve consistency across research. Fourthly, the rehabilitation methods based on VR are limited. Future research could consider incorporating some distinctive training modalities with VR devices, such as Tai Chi, rhythmic auditory cueing, and sensorimotor training with proprioceptive enhancement, which have been proven to have therapeutic effects on neurodegenerative diseases10,22,92,93. Finally, sufficient evidence on the mechanisms underlying the therapeutic effects of VR rehabilitation is lacking. Future research could explore the health benefits of VR rehabilitation at the cellular and molecular levels and elucidate its potential neurotic mechanisms through advanced neuroimaging techniques. Addressing these limitations is imperative to enhance the credibility and clinical applicability of VR rehabilitation as a treatment intervention for neurodegenerative diseases.
Overall, VR rehabilitation has demonstrated some benefits in motor performance, cognitive function, and quality of life for people with neurodegenerative diseases. Both immersive and non-immersive VR modalities offer distinct benefits, yet inconsistencies in study designs underscore the need for standardized protocols. The functional improvements brought by VR may be achieved by promoting neural plasticity, integrating sensory-motor functions, regulating emotions and dopaminergic pathways, and controlling neuroinflammation.
Methods
Eligibility criteria
The initial search results indicated that virtual reality rehabilitation is mainly applied to patients with PD, CI, and MS. The inclusion criteria for the literature were as follows: (1) study designs must be restricted to systematic reviews, meta-analyses, and clinical trials (randomized or nonrandomized designs); (2) participants must be diagnosed with PD, CI, or MS included without restrictions on age or disease progression, and CI refers broadly to cognitive impairment; (3) interventions in clinical trials must incorporate VR-based rehabilitation as a therapeutic approach for the specified conditions; (4) only English publications were considered. The exclusion criteria involved the removal of review articles, study protocols, case reports, editorial communications, clinical guidelines, irrelevant data, and inaccessible studies.
Data sources and search strategy
A systematic search was performed on the PubMed database, the Cochrane Library, and the Web of Science Core Collection database as of October 9, 2024. The search terms included “Virtual reality”, “Rehabilitation”, and specific disease terms (“Parkinson’s disease”, “dementia”, “Alzheimer’s disease”, “cognitive impairment”, and “multiple sclerosis”), using appropriate Boolean operators and database-specific syntax. The detailed search strategy is available in the Supplementary Information.
Study selection and data extraction
The study selection process adhered to the PRISMA 2020 statement. Two independent researchers screened titles, abstracts, and full-texts with disagreements resolved through discussion. The selection process is illustrated in Fig. 1. Two researchers independently extracted data on the therapeutic effects of VR rehabilitation for neurodegenerative diseases from the selected meta-analyses and clinical trials. The extracted data included study basic information (authors and year), participant information (disease types and sample size), intervention details (VR type, duration, frequency, and total volume), assessment indicators, and main results. Some specific statistical values, such as standardized mean difference (SMD), mean difference (MD), partial eta squared (η²p), 95% confidence interval (95% CI) with p value, were used to present the therapeutic effect of VR rehabilitation. In addition, our research did not include articles with missing data.
Synthesis methods
We stratified all studies into three VR system types, i.e., immersive, semi-immersive, and non-immersive platforms, and then systematically evaluated the therapeutic effects of VR rehabilitation on various outcomes in different neurodegenerative diseases. The comparative results were quantified using multiple statistical values, including MD, SMD, η²p, and 95% CI. All remarkable findings were reported in the results section. Data were qualitatively described and summarized in tabular form. This study integrated findings from previous literature and provided a systematic synthesis.
Study risk of bias assessment
Two researchers independently conducted quality assessments of these included studies to ensure methodological rigour. Any discrepancies were resolved through consensus discussions. The Assessment of Multiple Systematic Reviews tool (AMSTAR) was applied to appraise systematic reviews and meta-analyses, and the PEDro Scale was used for randomized controlled trials (RCTs). Both instruments comprise 11 criteria, and the total score is 11 points. Studies scoring ≥ 7 points were rated as high-quality evidence, those scoring ≤ 3 points as low-quality evidence, and those scoring 4 ~ 6 points as medium-quality evidence. Furthermore, the Review Manager 5.3 software was used to create the traffic-light plot for visually assessing the risk of bias in the included RCTs.
This systematic review was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-analyses guidelines, and was retrospectively registered on the Open Science Framework platform (registration DOI: 10.17605/OSF.IO/UXY5Z).
Ethics approval and consent to participate
Not applicable.
Data availability
No datasets were generated or analysed during the current study.
References
Dugger, B. N. & Dickson, D. W. Pathology of neurodegenerative diseases. Cold Spring Harb. Perspect. Biol. 9, a028035, https://doi.org/10.1101/cshperspect.a028035 (2017).
The Global, regional, and national burden of disorders affecting the nervous system, 1990-2021: a systematic analysis for the Global Burden of Disease Study 2021. Lancet Neurol. 23, 344–381, https://doi.org/10.1016/s1474-4422(24)00038-3 (2024).
Wu, X. C. et al. The burden of Parkinson’s disease, 1990-2021: a systematic analysis of the Global Burden of Disease study 2021. Front. aging Neurosci. 17, 1596392. https://doi.org/10.3389/fnagi.2025.1596392 (2025).
Hao, M. & Chen, J. Trend analysis and future predictions of global burden of alzheimer’s disease and other dementias: a study based on the global burden of disease database from 1990 to 2021. BMC Med. 23, 378. https://doi.org/10.1186/s12916-025-04169-w (2025).
Mensah-Kane, P. & Sumien, N. The potential of hyperbaric oxygen as a therapy for neurodegenerative diseases. GeroScience 45, 747–756, https://doi.org/10.1007/s11357-022-00707-z (2023).
Wimo, A. et al. The worldwide costs of dementia in 2019. Alzheimer’s. Dement.: J. Alzheimer’s. Assoc. 19, 2865–2873, https://doi.org/10.1002/alz.12901 (2023).
Deuschl, G. et al. The burden of neurological diseases in Europe: an analysis for the Global Burden of Disease Study 2017. Lancet Public Health 5, e551–e567, https://doi.org/10.1016/s2468-2667(20)30190-0 (2020).
Zhang, X. et al. Global burden of Alzheimer’s disease and other dementias attributed to metabolic risks from 1990 to 2021: results from the global burden of disease study 2021. BMC Psychiatry 24, 910. https://doi.org/10.1186/s12888-024-06375-x (2024).
Logroscino, G., Urso, D. & Savica, R. Descriptive Epidemiology of Neurodegenerative Diseases: What Are the Critical Questions?. Neuroepidemiology 56, 309–318, https://doi.org/10.1159/000525639 (2022).
Wang, R., Zhou, H., Wang, Y. C., Chang, X. L. & Wang, X. Q. Benefits of Tai Chi Quan on neurodegenerative diseases: A systematic review. Ageing Res. Rev. 82, 101741. https://doi.org/10.1016/j.arr.2022.101741 (2022).
Park, M. J., Kim, D. J., Lee, U., Na, E. J. & Jeon, H. J. A Literature Overview of Virtual Reality (VR) in Treatment of Psychiatric Disorders: Recent Advances and Limitations. Front. Psychiatry 10, 505, https://doi.org/10.3389/fpsyt.2019.00505 (2019).
Maggio, M. G. et al. Low-Intensity Virtual Reality Exercise for Caregivers of People with Mild Cognitive Impairment: A Pilot Study. J. Funct. Morphol. Kinesiol. 10, 353, https://doi.org/10.3390/jfmk10030353 (2025).
Riva, G., Waterworth, J. A. & Waterworth, E. L. The layers of presence: a bio-cultural approach to understanding presence in natural and mediated environments. Cyberpsychol. Behav.: impact Internet Multimed. virtual Real. Behav. Soc. 7, 402–416, https://doi.org/10.1089/cpb.2004.7.402 (2004).
Pazzaglia, C. et al. Comparison of virtual reality rehabilitation and conventional rehabilitation in Parkinson’s disease: a randomised controlled trial. Physiotherapy 106, 36–42, https://doi.org/10.1016/j.physio.2019.12.007 (2020).
Gómez-Cáceres, B., Cano-López, I., Aliño, M. & Puig-Perez, S. Effectiveness of virtual reality-based neuropsychological interventions in improving cognitive functioning in patients with mild cognitive impairment: A systematic review and meta-analysis. Clin. Neuropsychol. 37, 1337–1370, https://doi.org/10.1080/13854046.2022.2148283 (2023).
Maggio, M. G. et al. The role of virtual reality-based cognitive training in enhancing motivation and cognitive functions in individuals with chronic stroke. Sci. Rep. 15, 25258. https://doi.org/10.1038/s41598-025-08173-1 (2025).
Bargeri, S. et al. Effectiveness and safety of virtual reality rehabilitation after stroke: an overview of systematic reviews. EClinicalMedicine 64, 102220. https://doi.org/10.1016/j.eclinm.2023.102220 (2023).
Truijen, S. et al. Effect of home-based virtual reality training and telerehabilitation on balance in individuals with Parkinson disease, multiple sclerosis, and stroke: a systematic review and meta-analysis. Neurol. Sci.: J. Ital. Neurol. Soc. Ital. Soc. Clin. Neurophysiol. 43, 2995–3006, https://doi.org/10.1007/s10072-021-05855-2 (2022).
Cano Porras, D., Siemonsma, P., Inzelberg, R., Zeilig, G. & Plotnik, M. Advantages of virtual reality in the rehabilitation of balance and gait: Systematic review. Neurology 90, 1017–1025, https://doi.org/10.1212/wnl.0000000000005603 (2018).
Mirelman, A. et al. Addition of a non-immersive virtual reality component to treadmill training to reduce fall risk in older adults (V-TIME): a randomised controlled trial. Lancet 388, 1170–1182, https://doi.org/10.1016/s0140-6736(16)31325-3 (2016).
Ghai, S., Ghai, I. & Lamontagne, A. Virtual reality training enhances gait poststroke: a systematic review and meta-analysis. Ann. N. Y. Acad. Sci. 1478, 18–42, https://doi.org/10.1111/nyas.14420 (2020).
Ghai, S. & Ghai, I. Virtual reality enhances gait in cerebral palsy: a training dose-response meta-analysis. Front. Neurol. 10, 236, https://doi.org/10.3389/fneur.2019.00236 (2019).
Dockx, K. et al. Virtual reality for rehabilitation in Parkinson’s disease. Cochrane Database Syst. Rev. 12, Cd010760, https://doi.org/10.1002/14651858.CD010760.pub2 (2016).
Son, C. & Park, J. H. Ecological Effects of VR-Based Cognitive Training on ADL and IADL in MCI and AD patients: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 19, https://doi.org/10.3390/ijerph192315875 (2022).
Liao, Y. Y., Tseng, H. Y., Lin, Y. J., Wang, C. J. & Hsu, W. C. Using virtual reality-based training to improve cognitive function, instrumental activities of daily living and neural efficiency in older adults with mild cognitive impairment. Eur. J. Phys. Rehabil. Med. 56, 47–57, https://doi.org/10.23736/s1973-9087.19.05899-4 (2020).
Kim, D. R., Moon, E., Shin, M. J., Yang, Y. A. & Park, J. H. Effect of Individual Virtual Reality Cognitive Training Programs on Cognitive Function and Depression in Middle-Aged Women: Randomized Controlled Trial. JMIR Ment. health 10, e48912, https://doi.org/10.2196/48912 (2023).
Liao, Y. Y., Chen, I. H., Lin, Y. J., Chen, Y. & Hsu, W. C. Effects of Virtual Reality-Based Physical and Cognitive Training on Executive Function and Dual-Task Gait Performance in Older Adults With Mild Cognitive Impairment: A Randomized Control Trial. Front. Aging Neurosci. 11, 162, https://doi.org/10.3389/fnagi.2019.00162 (2019).
Baldimtsi, E. et al. Effects of Virtual Reality Physical and Cognitive Training Intervention On Cognitive Abilities of Elders with Mild Cognitive Impairment. J. Alzheimer’s. Dis. Rep. 7, 1475–1490, https://doi.org/10.3233/adr-230099 (2023).
Yu, D., Li, X. & Lai, F. H. The effect of virtual reality on executive function in older adults with mild cognitive impairment: a systematic review and meta-analysis. Aging Ment. health 27, 663–673, https://doi.org/10.1080/13607863.2022.2076202 (2023).
Wu, J., Ma, Y. & Ren, Z. Rehabilitative Effects of Virtual Reality Technology for Mild Cognitive Impairment: A Systematic Review With Meta-Analysis. Front. Psychol. 11, 1811, https://doi.org/10.3389/fpsyg.2020.01811 (2020).
Ren, Y., Wang, Q., Liu, H., Wang, G. & Lu, A. Effects of immersive and non-immersive virtual reality-based rehabilitation training on cognition, motor function, and daily functioning in patients with mild cognitive impairment or dementia: A systematic review and meta-analysis. Clin. Rehabil. 38, 305–321, https://doi.org/10.1177/02692155231213476 (2024).
Feng, H. et al. Virtual Reality Rehabilitation Versus Conventional Physical Therapy for Improving Balance and Gait in Parkinson’s Disease Patients: A Randomized Controlled Trial. Med. Sci. Monit.: Int. Med. J. Exp. Clin. Res. 25, 4186–4192, https://doi.org/10.12659/msm.916455 (2019).
Lee, N. Y., Lee, D. K. & Song, H. S. Effect of virtual reality dance exercise on the balance, activities of daily living, and depressive disorder status of Parkinson’s disease patients. J. Phys. Ther. Sci. 27, 145–147, https://doi.org/10.1589/jpts.27.145 (2015).
Chen, Y., Gao, Q., He, C. Q. & Bian, R. Effect of Virtual Reality on Balance in Individuals With Parkinson Disease: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Phys. Ther. 100, 933–945, https://doi.org/10.1093/ptj/pzaa042 (2020).
Kwon, S. H., Park, J. K. & Koh, Y. H. A systematic review and meta-analysis on the effect of virtual reality-based rehabilitation for people with Parkinson’s disease. J. Neuroeng. Rehabil. 20, 94. https://doi.org/10.1186/s12984-023-01219-3 (2023).
Wang, W., Wong, S. S. -l & Lai, F. H. -y The Effect of Virtual Reality Rehabilitation on Balance in Patients with Parkinson’s Disease: A Systematic Review and Meta-Analysis. Electronics 10, 1003, https://doi.org/10.3390/electronics10091003 (2021).
Wu, J. et al. Benefits of Virtual Reality Balance Training for Patients With Parkinson Disease: Systematic Review, Meta-analysis, and Meta-Regression of a Randomized Controlled Trial. JMIR Serious Games 10, e30882, https://doi.org/10.2196/30882 (2022).
Sarasso, E. et al. Virtual reality balance training to improve balance and mobility in Parkinson’s disease: a systematic review and meta-analysis. J. Neurol. 269, 1873–1888, https://doi.org/10.1007/s00415-021-10857-3 (2022).
Wang, B. et al. Effect of virtual reality on balance and gait ability in patients with Parkinson’s disease: a systematic review and meta-analysis. Clin. Rehabilitation 33, 1130–1138, https://doi.org/10.1177/0269215519843174 (2019).
Lina, C. et al. The Effect of Virtual Reality on the Ability to Perform Activities of Daily Living, Balance During Gait, and Motor Function in Parkinson Disease Patients: A Systematic Review and Meta-Analysis. Am. J. Phys. Med. Rehabil. 99, 917–924, https://doi.org/10.1097/phm.0000000000001447 (2020).
Park, J. S., Jung, Y. J. & Lee, G. Virtual Reality-Based Cognitive-Motor Rehabilitation in Older Adults with Mild Cognitive Impairment: A Randomized Controlled Study on Motivation and Cognitive Function. Healthcare 8, 335, https://doi.org/10.3390/healthcare8030335 (2020).
Ortiz-Gutiérrez, R. et al. A telerehabilitation program improves postural control in multiple sclerosis patients: a Spanish preliminary study. Int. J. Environ. Res. public health 10, 5697–5710, https://doi.org/10.3390/ijerph10115697 (2013).
Lozano-Quilis, J. A. et al. Virtual rehabilitation for multiple sclerosis using a kinect-based system: randomized controlled trial. JMIR Serious Games 2, e12, https://doi.org/10.2196/games.2933 (2014).
Kalron, A., Fonkatz, I., Frid, L., Baransi, H. & Achiron, A. The effect of balance training on postural control in people with multiple sclerosis using the CAREN virtual reality system: a pilot randomized controlled trial. J. Neuroeng. Rehabil. 13, 13. https://doi.org/10.1186/s12984-016-0124-y (2016).
Marcos-Antón, S. et al. sEMG-controlled forearm bracelet and serious game-based rehabilitation for training manual dexterity in people with multiple sclerosis: a randomised controlled trial. J. Neuroeng. Rehabil. 20, 110. https://doi.org/10.1186/s12984-023-01233-5 (2023).
Maggio, M. G. et al. Limb apraxia in individuals with multiple sclerosis: Is there a role of semi-immersive virtual reality in treating the Cinderella of neuropsychology?. Mult. Scler. Relat. Disord. 69, 104405. https://doi.org/10.1016/j.msard.2022.104405 (2023).
Maggio, M. G. et al. Do patients with multiple sclerosis benefit from semi-immersive virtual reality? A randomized clinical trial on cognitive and motor outcomes. Appl. Neuropsychol. 29, 59–65, https://doi.org/10.1080/23279095.2019.1708364 (2022).
Leonardi, S. et al. Cognitive recovery in people with relapsing/remitting multiple sclerosis: A randomized clinical trial on virtual reality-based neurorehabilitation. Clin. Neurol. Neurosurg. 208, 106828. https://doi.org/10.1016/j.clineuro.2021.106828 (2021).
Calafiore, D. et al. Efficacy of Virtual Reality and Exergaming in Improving Balance in Patients With Multiple Sclerosis: A Systematic Review and Meta-Analysis. Front. Neurol. 12, 773459. https://doi.org/10.3389/fneur.2021.773459 (2021).
Castellano-Aguilera, A. et al. Effectiveness of Virtual Reality on Balance and Risk of Falls in People with Multiple Sclerosis: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public health 19, 14192, https://doi.org/10.3390/ijerph192114192 (2022).
Goffredo, M. et al. Efficacy of non-immersive virtual reality-based telerehabilitation on postural stability in Parkinson’s disease: a multicenter randomized controlled trial. Eur. J. Phys. Rehabil. Med. 59, 689–696, https://doi.org/10.23736/s1973-9087.23.07954-6 (2023).
Gandolfi, M. et al. Virtual Reality Telerehabilitation for Postural Instability in Parkinson’s Disease: A Multicenter, Single-Blind, Randomized, Controlled Trial. BioMed. Res. Int. 2017, 7962826. https://doi.org/10.1155/2017/7962826 (2017).
Maranesi, E. et al. The Effect of Non-Immersive Virtual Reality Exergames versus Traditional Physiotherapy in Parkinson’s Disease Older Patients: Preliminary Results from a Randomized-Controlled Trial. Int. J. Environ. Res. Public health 19, 14818, https://doi.org/10.3390/ijerph192214818 (2022).
Choi, W. & Lee, S. The Effects of Virtual Kayak Paddling Exercise on Postural Balance, Muscle Performance, and Cognitive Function in Older Adults with Mild Cognitive Impairment: A Randomized Controlled Trial. J. Aging Phys. Act. 27, 861–870, https://doi.org/10.1123/japa.2018-0020 (2019).
Park, J. H. Does the virtual shopping training improve executive function and instrumental activities of daily living of patients with mild cognitive impairment?. Asian J. Psychiatry 69, 102977. https://doi.org/10.1016/j.ajp.2021.102977 (2022).
Cuesta-Gómez, A. et al. Effects of virtual reality associated with serious games for upper limb rehabilitation inpatients with multiple sclerosis: randomized controlled trial. J. Neuroeng. Rehabilitation 17, 90. https://doi.org/10.1186/s12984-020-00718-x (2020).
Goffredo, M. et al. Non-Immersive Virtual Reality Telerehabilitation System Improves Postural Balance in People with Chronic Neurological Diseases. J. Clin. Med. 12, 3178, https://doi.org/10.3390/jcm12093178 (2023).
Doğan, M., Ayvat, E. & Kılınç, M. Telerehabilitation versus virtual reality supported task-oriented circuit therapy on upper limbs and trunk functions in patients with multiple sclerosis: A randomized controlled study. Mult. Scler. Relat. Disord. 71, 104558. https://doi.org/10.1016/j.msard.2023.104558 (2023).
Herbert, R., Moseley, A. & Sherrington, C. PEDro: a database of randomised controlled trials in physiotherapy. Health Inf. Manag.: J. Health Inf. Manag. Assoc. Aust. 28, 186–188, https://doi.org/10.1177/183335839902800410 (1998).
García-Betances, R. I., Jiménez-Mixco, V., Arredondo, M. T. & Cabrera-Umpiérrez, M. F. Using virtual reality for cognitive training of the elderly. Am. J. Alzheimer’s. Dis. Dement. 30, 49–54, https://doi.org/10.1177/1533317514545866 (2015).
Canning, C. G. et al. Virtual reality in research and rehabilitation of gait and balance in Parkinson disease. Nat. Rev. Neurol. 16, 409–425, https://doi.org/10.1038/s41582-020-0370-2 (2020).
Calabrò, R. S. et al. The role of virtual reality in improving motor performance as revealed by EEG: a randomized clinical trial. J. Neuroeng. Rehabil. 14, 53. https://doi.org/10.1186/s12984-017-0268-4 (2017).
Bauer, A. C. M. & Andringa, G. The Potential of Immersive Virtual Reality for Cognitive Training in Elderly. Gerontology 66, 614–623, https://doi.org/10.1159/000509830 (2020).
Pereira, M. P., Gobbi, L. T. & Almeida, Q. J. Freezing of gait in Parkinson’s disease: Evidence of sensory rather than attentional mechanisms through muscle vibration. Parkinson. Relat. Disord. 29, 78–82, https://doi.org/10.1016/j.parkreldis.2016.05.021 (2016).
Bardakan, M. M. et al. Imaging the neural underpinnings of freezing of gait in Parkinson’s disease. NeuroImage. Clin. 35, 103123. https://doi.org/10.1016/j.nicl.2022.103123 (2022).
Ghai, S., Schmitz, G., Hwang, T. H. & Effenberg, A. O. Auditory Proprioceptive Integration: Effects of Real-Time Kinematic Auditory Feedback on Knee Proprioception. Front. Neurosci. 12, 142, https://doi.org/10.3389/fnins.2018.00142 (2018).
Ghai, S. & Ghai, I. Effects of Rhythmic Auditory Cueing in Gait Rehabilitation for Multiple Sclerosis: A Mini Systematic Review and Meta-Analysis. Front. Neurol. 9, 386, https://doi.org/10.3389/fneur.2018.00386 (2018).
van Gelder, L. et al. Real-time feedback to improve gait in children with cerebral palsy. Gait posture 52, 76–82, https://doi.org/10.1016/j.gaitpost.2016.11.021 (2017).
Mirelman, A., Patritti, B. L., Bonato, P. & Deutsch, J. E. Effects of virtual reality training on gait biomechanics of individuals post-stroke. Gait posture 31, 433–437, https://doi.org/10.1016/j.gaitpost.2010.01.016 (2010).
Mak, M. K. & Hui-Chan, C. W. Cued task-specific training is better than exercise in improving sit-to-stand in patients with Parkinson’s disease: A randomized controlled trial. Mov. Disord. J. Mov. Disord. Soc. 23, 501–509, https://doi.org/10.1002/mds.21509 (2008).
Bonanno, M. et al. Might patients with cerebellar ataxia benefit from the Computer Assisted Rehabilitation ENvironment (CAREN)? A pilot study focusing on gait and balance. Front. Bioeng. Biotechnol. 12, 1385280. https://doi.org/10.3389/fbioe.2024.1385280 (2024).
Fritz, N. E., Cheek, F. M. & Nichols-Larsen, D. S. Motor-Cognitive Dual-Task Training in Persons With Neurologic Disorders: A Systematic Review. J. Neurol. Phys. Ther. : JNPT 39, 142–153, https://doi.org/10.1097/npt.0000000000000090 (2015).
Sasaki, F. et al. Impaired virtual space-tilting perception in Parkinson’s disease with Pisa syndrome. Parkinson. Relat. Disord. 104, 30–34, https://doi.org/10.1016/j.parkreldis.2022.09.002 (2022).
Visch, V. T., Tan, E. S. & Molenaar, D. The emotional and cognitive effect of immersion in film viewing. Cogn. Emot. 24, 1439–1445, https://doi.org/10.1080/02699930903498186 (2010).
Kotler, S., Mannino, M., Kelso, S. & Huskey, R. First few seconds for flow: A comprehensive proposal of the neurobiology and neurodynamics of state onset. Neurosci. Biobehav. Rev. 143, 104956. https://doi.org/10.1016/j.neubiorev.2022.104956 (2022).
Dan, R. et al. Impact of dopamine and cognitive impairment on neural reactivity to facial emotion in Parkinson’s disease. Eur. Neuropsychopharmacol. J. Eur. Coll. Neuropsychopharmacol. 29, 1258–1272, https://doi.org/10.1016/j.euroneuro.2019.09.003 (2019).
Boot, W. R. et al. Video games as a means to reduce age-related cognitive decline: attitudes, compliance, and effectiveness. Front. Psychol. 4, 31, https://doi.org/10.3389/fpsyg.2013.00031 (2013).
Rimal, N., Khanal, S., Bohara, G. & Choi, D. Y. Exendin-4 protects the dopaminergic neurons by attenuating inflammatory responses of microglial cells via activation of AMPK. Neuropharmacology 279, 110643. https://doi.org/10.1016/j.neuropharm.2025.110643 (2025).
Zapanti, E., Dermentzoglou, A., Kazakou, P., Kilindireas, K. & Mastorakos, G. The role of the stress adaptive response in multiple sclerosis. Front. Neuroendocrinol. 78, 101204. https://doi.org/10.1016/j.yfrne.2025.101204 (2025).
Yang, K. C., Yang, B. H., Lan, C. C., Liu, M. N. & Chou, Y. H. Striatal and peripheral dopaminergic alterations related to cognitive impairment in patients with schizophrenia. Psychol. Med. 54, 1–11, https://doi.org/10.1017/s0033291724002228 (2024).
Dar, S. A., Ramakrishna, K. & Shekhawat, Y. S. Impact of positive thinking on synapses. Prog. Brain Res. 293, 17–40, https://doi.org/10.1016/bs.pbr.2025.03.005 (2025).
Sacheli, M. A. et al. Exercise increases caudate dopamine release and ventral striatal activation in Parkinson’s disease. Mov. Disord.: J. Mov. Disord. Soc. 34, 1891–1900, https://doi.org/10.1002/mds.27865 (2019).
Fisher, B. E. et al. Treadmill exercise elevates striatal dopamine D2 receptor binding potential in patients with early Parkinson’s disease. Neuroreport 24, 509–514, https://doi.org/10.1097/WNR.0b013e328361dc13 (2013).
Emmons, H. A. & Fordahl, S. C. Moderate-intensity aerobic exercise enhanced dopamine signaling in diet-induced obese female mice without preventing body weight gain. Neuroscience 555, 1–10, https://doi.org/10.1016/j.neuroscience.2024.07.020 (2024).
Petrova, L. V., Kostenko, E. V., Martynov, M. Y., Pogonchenkova, I. V. & Kopasheva, V. D. The effect of rehabilitation with sensory glove and virtual reality on concentration of brain-derived neurotrophic factor and event related potential P300 in the early rehabilitation period after ischemic stroke]. Z. Nevrol. Psikhiatr. Korsakova 123, 75–81, https://doi.org/10.17116/jnevro202312312275 (2023).
Lewandowski, D. et al. Cathepsins in Neurological Diseases. Int. J. Mol. Sci. 26, 7886, https://doi.org/10.3390/ijms26167886 (2025).
Huang, Q., Wang, Y., Chen, S. & Liang, F. Glycometabolic Reprogramming of Microglia in Neurodegenerative Diseases: Insights from Neuroinflammation. Aging Dis. 15, 1155–1175, https://doi.org/10.14336/ad.2023.0807 (2024).
Gao, C., Jiang, J., Tan, Y. & Chen, S. Microglia in neurodegenerative diseases: mechanism and potential therapeutic targets. Signal Transduct. Target. Ther. 8, 359, https://doi.org/10.1038/s41392-023-01588-0 (2023).
Stephenson, J., Nutma, E., van der Valk, P. & Amor, S. Inflammation in CNS neurodegenerative diseases. Immunology 154, 204–219, https://doi.org/10.1111/imm.12922 (2018).
Sugimoto, S., Yokoshi, M., Maruyama, T., Amemiya, S. & Kita, I. Effects of acute treadmill running following administration of lipopolysaccharide on subsequent changes in microglial activation and depressive-like behavior in rats. Behav. Brain Res. 493, 115718. https://doi.org/10.1016/j.bbr.2025.115718 (2025).
Dhabhar, F. S. Effects of stress on immune function: the good, the bad, and the beautiful. Immunol. Res. 58, 193–210, https://doi.org/10.1007/s12026-014-8517-0 (2014).
Hsieh, C. C. et al. The Effectiveness of a Virtual Reality-Based Tai Chi Exercise on Cognitive and Physical Function in Older Adults with Cognitive Impairment. Dement. Geriatr. Cogn. Disord. 46, 358–370, https://doi.org/10.1159/000494659 (2018).
Ghai, S., Ghai, I. & Effenberg, A. O. Effect of rhythmic auditory cueing on gait in cerebral palsy: a systematic review and meta-analysis. Neuropsychiatr. Dis. Treat. 14, 43–59, https://doi.org/10.2147/ndt.S148053 (2018).
Papaioannou, T., Voinescu, A., Petrini, K. & Stanton Fraser, D. Efficacy and Moderators of Virtual Reality for Cognitive Training in People with Dementia and Mild Cognitive Impairment: A Systematic Review and Meta-Analysis. J. Alzheimer’s. Dis. 88, 1341–1370, https://doi.org/10.3233/jad-210672 (2022).
Hill, N. T. et al. Computerized Cognitive Training in Older Adults With Mild Cognitive Impairment or Dementia: A Systematic Review and Meta-Analysis. Am. J. Psychiatry 174, 329–340, https://doi.org/10.1176/appi.ajp.2016.16030360 (2017).
Zuschnegg, J. et al. Effectiveness of computer-based interventions for community-dwelling people with cognitive decline: a systematic review with meta-analyses. BMC Geriatr. 23, 229. https://doi.org/10.1186/s12877-023-03941-y (2023).
Kim, H., Jung, J. & Lee, S. Therapeutic Application of Virtual Reality in the Rehabilitation of Mild Cognitive Impairment: A Systematic Review and Meta-Analysis. Vision 6, 68, https://doi.org/10.3390/vision6040068 (2022).
Zhong, D. et al. Effects of virtual reality cognitive training in individuals with mild cognitive impairment: A systematic review and meta-analysis. Int. J. Geriatr. psychiatry 36, 1829–1847, https://doi.org/10.1002/gps.5603 (2021).
Yan, M. et al. Effects of virtual reality combined cognitive and physical interventions on cognitive function in older adults with mild cognitive impairment: A systematic review and meta-analysis. Ageing Res. Rev. 81, 101708. https://doi.org/10.1016/j.arr.2022.101708 (2022).
Mura, G., Carta, M. G., Sancassiani, F., Machado, S. & Prosperini, L. Active exergames to improve cognitive functioning in neurological disabilities: a systematic review and meta-analysis. Eur. J. Phys. Rehabil. Med. 54, 450–462, https://doi.org/10.23736/s1973-9087.17.04680-9 (2018).
Casuso-Holgado, M. J. et al. Effectiveness of virtual reality training for balance and gait rehabilitation in people with multiple sclerosis: a systematic review and meta-analysis. Clin. Rehabil. 32, 1220–1234, https://doi.org/10.1177/0269215518768084 (2018).
De Keersmaecker, E. et al. Virtual reality during gait training: does it improve gait function in persons with central nervous system movement disorders? A systematic review and meta-analysis. NeuroRehabilitation 44, 43–66, https://doi.org/10.3233/nre-182551 (2019).
Nascimento, A. S., Fagundes, C. V., Mendes, F. & Leal, J. C. Effectiveness of Virtual Reality Rehabilitation in Persons with Multiple Sclerosis: A Systematic Review and Meta-analysis of Randomized Controlled Trials. Mult. Scler. Relat. Disord. 54, 103128. https://doi.org/10.1016/j.msard.2021.103128 (2021).
Cortés-Pérez, I. et al. Virtual reality-based therapy improves balance and reduces fear of falling in patients with multiple sclerosis. a systematic review and meta-analysis of randomized controlled trials. J. Neuroeng. Rehabil. 20, 42. https://doi.org/10.1186/s12984-023-01174-z (2023).
Zhang, J. et al. Effects of virtual reality-based rehabilitation on cognitive function and mood in multiple sclerosis: A systematic review and meta-analysis of randomized controlled trials. Mult. Scler. Relat. Disord. 87, 105643. https://doi.org/10.1016/j.msard.2024.105643 (2024).
Doherty, F., Lynch, P., Powell, P. & Monaghan, K. Feasibility and effectiveness of telerehabilitation on mobility and balance function in multiple sclerosis: A systematic review and meta-analysis. J. Neurol. Sci. 466, 123214. https://doi.org/10.1016/j.jns.2024.123214 (2024).
Yang, W. C., Wang, H. K., Wu, R. M., Lo, C. S. & Lin, K. H. Home-based virtual reality balance training and conventional balance training in Parkinson’s disease: A randomized controlled trial. J. Formos. Med. Assoc. 115, 734–743, https://doi.org/10.1016/j.jfma.2015.07.012 (2016).
Kashif, M. et al. Effects of virtual reality versus motor imagery versus routine physical therapy in patients with parkinson’s disease: a randomized controlled trial. BMC Geriatr. 24, 229. https://doi.org/10.1186/s12877-024-04845-1 (2024).
Liao, Y. Y. et al. Virtual Reality-Based Training to Improve Obstacle-Crossing Performance and Dynamic Balance in Patients With Parkinson’s Disease. Neurorehabil. Neural Repair 29, 658–667, https://doi.org/10.1177/1545968314562111 (2015).
Gutiérrez et al. A telerehabilitation program by virtual reality-video games improves balance and postural control in multiple sclerosis patients. NeuroRehabilitation 33, 545–554, https://doi.org/10.3233/nre-130995 (2013).
Peruzzi, A., Zarbo, I. R., Cereatti, A., Della Croce, U. & Mirelman, A. An innovative training program based on virtual reality and treadmill: effects on gait of persons with multiple sclerosis. Disabil. Rehabil. 39, 1557–1563, https://doi.org/10.1080/09638288.2016.1224935 (2017).
Waliño-Paniagua, C. N. et al. Effects of a Game-based Virtual Reality Video Capture Training Program Plus Occupational Therapy On Manual Dexterity In Patients With Multiple Sclerosis: A Randomized Controlled Trial. J. Healthc. Eng. 2019, 9780587. https://doi.org/10.1155/2019/9780587 (2019).
Pagliari, C. et al. Effects of home-based virtual reality telerehabilitation system in people with multiple sclerosis: A randomized controlled trial. J. Telemed. Telecare 30, 344–355, https://doi.org/10.1177/1357633x211054839 (2024).
Acknowledgements
This study was supported by the National Key Research and Development Program of China [grant number 2024YFC3607600], the Postdoctoral Fellowship Program of CPSF [grant number GZC20252086], and the Postdoctoral Research Startup Fund of Ningbo Rehabilitation Hospital [grant number BSH-001 and grant number 2025-BSH-ZZ-WR].
Author information
Authors and Affiliations
Contributions
W.R. and T.T.T.X. conceived and designed the study. T.T.T.X., Y.Y., Z.T.T., and L.H.Q. performed the majority of the analyses and visualizations and drafted the manuscript. T.T.T.X., Y.Y., Z.T.T., and L.H.Q. contributed to the development of the analysis strategy. W.W.M. and F.L.L. were responsible for data collection and data management. W.R. and J.S.H. provided guidance during the analysis. T.T.T.X. drafted the manuscript, and W.R. revised the manuscript. All authors reviewed the final version of the manuscript and approved it for publication.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Tu, T., Yang, Y., Zheng, T. et al. Benefits of virtual reality rehabilitation on neurodegenerative diseases: a systematic review. npj Digit. Med. 9, 9 (2026). https://doi.org/10.1038/s41746-025-02171-3
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41746-025-02171-3
