
Abstract
Background
The incidence of kidney cancer, which is 34% attributable to obesity and smoking, has been steadily increasing over the past few decades in many countries in Europe, North America and Oceania. In recent years, there have been several reports of increasing incidence of early-onset cancer in young adults aged <50 years. We conducted a retrospective population-based cohort study to examine whether there have been changes in the incidence of kidney cancer in England during the past four decades.
Methods
Individual-level, national (population-based) cancer registration data for patients diagnosed with kidney cancer (ICD-10 code, C64) in England from 1985–2020 were obtained from the Office for National Statistics/Public Health England. Average annual incidence rates (AAIR) were calculated by two age categories (<50, 50+ years) and gender during the six five-year time periods (1985–89 to 2010–14) and the recent six-year period (2015–20). The percentage change in the incidence rates in each age group and gender was calculated as the change in the AAIR from the first (1985–89) to the last time period (2015–20). The Average Annual Percentage Change (AAPC, year-on-year increase in incidence rates during 1985–2000) was estimated using the slope of the linear trend line fitted to the incidence rates by year of diagnosis.
Results
During the 36-year study period (1985–2020), a total of 206,816 cases (62.4% males, 37.6% females) of kidney cancer were registered in England. In young adults aged <50 years, the AAIRs (per 100,000 population) increased by 157% in males and 133% in females (from 1.4 in 1985–89 to 3.6 in 2015–20 in males and from 0.9 in 1985–89 to 2.1 in 2015–20 in females). In older adults aged 50+ years, the AAIRs increased by 127% in males and 144% in females (from 24.5 in 1985–89 to 55.5 in 2015–20 in males and from 11.9 in 1985–89 to 29.0 in 2015–20 in females). The AAPC during the 36-year period was 5.0% in people aged <50 years compared to 4.7% in those aged 50+ years.
Conclusion
There has been a steady and substantial increase in the incidence of kidney cancer in England over the past four decades. This was partly driven by the largest and unexpected increase in the incidence of early-onset kidney cancer in young adults aged <50 years, which was steepest in males. Some of this increase is in analogy with the increasing prevalence of obesity; nevertheless, other causes driving this increase in early-onset kidney cancer in young adults remain elusive and need further investigation.
Similar content being viewed by others
Introduction
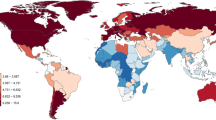
Over the past four decades, the overall incidence of kidney cancer (or renal cell carcinoma, ICD-10 code, C64) has been increasing steadily in many countries in Europe, North America and Oceania [1]. In recent years, there have been many reports in the literature and commentaries and reviews in online/print media regarding the increasing incidence of early-onset cancer in young adults aged <50 years [2]. Worldwide, kidney cancer is the 14th most common cancer – there were an estimated 434,840 new cases (2.6% of all cancers) and 155,953 deaths (1.6% of all cancer deaths) from kidney cancer in the year 2022, and a five-year prevalence of 1,369,974 cases [1]. In Europe, kidney cancer is the 8th most common cancer – there were an estimated 145,721 new cases (3.3% of all cancers) and 52,347 deaths (2.6% of all cancer deaths) from kidney cancer in 2022, and a five-year prevalence of 473,212 cases [1]. The highest age-standardised incidence rates (standardised to the World standard population) of kidney cancer are observed in North America and Europe (12.6 and 9.7 per 100,000 population, respectively) and the lowest in Asia and Africa (2.6 and 1.6 per 100,000 population, respectively) [1, 3]. A recent analysis of the GBD data showed that the burden of kidney cancer is increasing in countries with low to middle Sociodemographic Index (SDI), and regions such as North Africa and Middle East are experiencing the fastest growing burden of kidney cancer [4]. In the UK, kidney cancer is the 6th most common cancer with about 13,800 new cases (4% of all cancers) and 4700 deaths (3% of all cancer deaths) in 2019 [5]. The estimated cumulative (lifetime) risk of being diagnosed with kidney cancer by age 74 is 3% (1 in 38) for males and 1% (1 in 68) for females [5].
The aetiology of kidney cancer is complex and multifaceted and involves an interplay of genetic predisposition, environmental exposures, lifestyle factors, and underlying medical conditions [6]. Important risk factors for kidney cancer include hereditary syndromes (e.g., von Hippel-Lindau disease), family history (i.e. first-degree relative), polycystic (or chronic) kidney disease, environmental/occupational exposures (e.g. trichlorethylene, asbestos, cadmium, arsenic, radon, nitrates, herbicides), diets high in red and processed meats, use of analgesics (paracetamol/non-steroidal anti-inflammatory drugs), obesity, tobacco smoking, and hypertension [7,8,9,10,11,12,13,14]. It has been estimated that 34% of all kidney cancer cases in the UK are attributable to modifiable risk factors [24% to overweight/obesity (i.e. 2500 cases/year) and 13% to smoking (i.e. 1300 cases/year)] and are therefore potentially preventable [14].
We conducted a comprehensive and up-to-date analysis of the national cancer registration data for England (population, 56.5 Million) for the past four decades (1985–2020), to determine the changing epidemiology and trends in age- and gender-specific incidence rates of kidney cancer – with an objective to inform the development of health education/promotion and primary/secondary prevention initiatives (e.g. control of hypertension, obesity, and smoking), and public health policy to control exposure to certain chemicals in the population to reduce the burden of kidney cancer. It is anticipated that the study will also improve understanding of the aetiology of kidney cancer and guide commissioning and resource allocation of health/oncology services for patients.
Methods
Data sources
Individual level, national (population-based) cancer registration data for all patients diagnosed with kidney cancer (International Classification of Diseases (ICD) 10th revision code: C64) in England, during the 36-year period 1985–2020, were obtained from the Office for National Statistics (ONS) and Public Health England (PHE) Office for Data Release – which is responsible for the collection and collation of registrations from the nine regional population-based cancer registries in England. From October 2021, responsibility for the management of the National Disease Registration Service transferred from PHE to NHS Digital. These regional registries collect information on all cancer patients in their geographic area directly from primary/secondary care records, pathology reports and healthcare professionals. Since the early 1970s, cancer registration in England has been of a consistently high standard with over 98% completion proportions [15]. Items of data obtained included: patient ID number, gender, age at diagnosis, calendar year of diagnosis, topography (ICD-10 code), morphology codes (International Classification of Diseases for Oncology, 3rd Edition, ICD-O-3), laterality, grade and stage of cancer and Index of Multiple Deprivation (IMD, based on geographical area of area of residence). For the calculation of incidence rates, the corresponding annual mid-year national population estimates by age, gender and calendar year (i.e. the denominator data) were obtained from the Population Estimates Unit, ONS. Age-standardised (2013 European standard population) incidence and mortality rates of kidney cancer were obtained from Cancer Research UK [5].
Statistical analysis
Frequency distribution (N and %) and average annual incidence rates (AAIR, per 100,000 population) were calculated according to the two broad age categories (0–49 years and 50+ years) and gender during the six five-year time periods (1985–89 to 2010–14) and the recent six-year period, 2015–20, for which the data were available. The percentage change in the incidence rates in each age group and gender was calculated as the change in the AAIR from the first (1985–89) to the last time period (2015–20). The Average Annual Percentage Change (AAPC) in incidence rates (i.e. year-on-year increase in incidence during the 36-year study period) in each age group was estimated using the slope of the linear trend line fitted to the incidence rates by year of diagnosis. The incidence rates, calculated for each time period, were regressed against the mid-year of the corresponding time period. The statistical software SPSS (IBM SPSS Statistics, version 29) was used for data management and coding, Microsoft Excel (Microsoft Office 360) was used for the calculation of AAIRs and percentage chance in incidence rates, and SAS (version 9.4) was used for the calculation of AAPC.
Results
During the 36-year study period (1985–2020), a total of 206,816 cases of kidney cancer (62.4% males, 37.6% females; M:F ratio, 1.7:1) were registered in England. The average annual number of new cases increased from 365/year in 1985–89 to 998/year in 2015–20 in young adults aged <50 years (an increase of +173%), and from 2613/year in 1985–89 to 8504/year in 2015–20 in older adults aged 50+ years (an increase of +226%). The average annual number of new cases increased from 1847/year in 1985–89 to 6015/year in 2015–20 in males (an increase of +226%), and from 1132/year in 1985–89 to 3487/year in 2015–20 in females (an increase of +208%) (Table 1).
Trends in incidence by age and gender
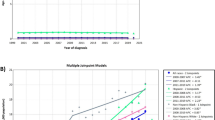
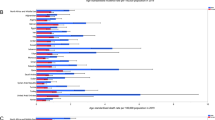
Table 1 and Fig. 1 show the trends in the number of cases and average annual incidence rates (AAIR per 100,000 population) of kidney cancer by two broad age groups (0–49 and 50+ years) and gender during the period 1985–2020. In young people aged 0–49 years, there was a steady and linear increase in incidence over this period: the incidence rates increased by +157% in males and +133% in females (from 1.4/100,000 in 1985–89 to 3.6/100,000 in 2015–20 in males and from 0.9/100,000 in 1985–89 to 2.1/100,000 in 2015–20 in females). The Average Annual Percentage Change (AAPC) in incidence rates was +5.1% in males and +4.4% in females. Similarly, in older people aged 50+ years, the incidence rates increased by +127% in males and +144% in females (from 24.5/100,000 in 1985–89 to 55.5/100,000 in 2015–20 in males and from 11.9/100,000 in 1985–89 to 29.0/100,000 in 2015–20 in females). The AAPC was +4.2% in males and +5.0% in females. Overall (i.e. for all ages combined), the magnitude of increase was slightly higher in males compared to females – during the study period, the incidence rates increased by +175% (with an AAPC of +5.7%) in males (from 8.0/100,000 in 1985–89 to 22.0/100,000 in 2015–20) and +162% (AAPC, +5.5%) in females (from 4.7/100,000 in 1985–89 to 12.3/100,000 in 2015–20). For comparison with other European populations, Table 2 presents the trends in age-standardised (2013 European standard population) average annual incidence rates (per 100,000 population) by age-group and gender during the period 1985–2020.

a Age 0–49 years, b Age 50+ years, c Both genders combined, d All ages combined.
Trends in mortality by age and gender
For most cancers, trends in mortality reflect trends in incidence and survival (which is the function of the stage/grade at diagnosis and efficacy of treatment). For example, increasing mortality may reflect increasing incidence and stable survival, and decreasing (or stable) mortality may reflect increasing incidence and increasing survival (due to early diagnosis, e.g. by screening, and improved treatment). With regard to the stage at diagnosis, the large majority (57.8%) of cases (in 2015–17) were diagnosed at an early stage, 1 or 2 and 42.2% were diagnosed at late stage 3 or 4. Table 3a shows the trends in age-standardised (2013 European standard population) average annual mortality rates (per 100,000 population) of kidney cancer by gender during the period 1985–2019. In males, the mortality rates increased by +28% (from 8.2/100,000 in 1985–89 to 10.5/100,000 in 2015–19; and in females the mortality rates increased by +31% (from 3.9/100,000 in 1985–89 to 5.1/100,000 in 2015–19). Table 3b presents trends in age-standardised (2013 European standard population) average annual mortality rates (per 100,000 population) of kidney cancer by age-group during the period 1985–2019. It appears that during the study period there was a small decrease in mortality rates in people aged 0–69 years, whereas there was an increase in mortality in people aged 70+ years, which may be (in part) a function of multi morbidity at older ages. Compared with the substantial increase in the incidence rates of kidney cancer (Table 1), which is the function of the aetiology of the disease, the trends in the mortality rates imply that there has been a substantial improvement in the survival/prognosis of kidney cancer in England over the past four decades – most likely due to the early diagnosis and improvements in the treatment of the disease.
Discussion
This retrospective population-based cohort study included 206,816 cases of kidney cancer diagnosed during the 36-year period (1985–2020) and presents the most comprehensive and up-to-date analysis of the latest trends in the incidence and changing epidemiology of the disease by age (0–49 years and 50+ years) and gender in England (population, 56.5 million). The study showed that overall (i.e. all ages and genders combined), there has been a steady and substantial increase (+171%) in the incidence of kidney cancer in England during the past four decades, which was partly driven by the unexpected increasing incidence in young adults aged <50 years (+155%). The highest increase was observed in young males aged <50 years compared with young females (+157% vs +133%). To our knowledge, this is the first report to document the increasing incidence of early-onset kidney cancer in young adults aged <50 years in England.
The strength of this study includes comprehensive analysis of the national population-based cancer registration dataset including 206,816 cases of kidney cancer, allowing the calculation of accurate incidence rates and the trends in incidence over four decades. While the cancer registration system in England is of a consistently high standard with over 98% completion rates, there is a possibility that information on a small number of cancer cases exclusively diagnosed and treated in private hospitals may be incomplete [15]. This is unlikely to have a material impact as over 99% of primary and secondary care activity (with regard to cancer referral/diagnosis/treatment) in England is funded by the National Health Service (NHS) [15]. All NHS healthcare providers are mandated to submit cancer data to NHS Digital, and this also includes NHS-funded activity in private hospitals. The cancer registration system is an opt-out scheme – i.e. NHS Digital can collect data on individuals without their consent, unless they choose to opt-out. This is also unlikely to have a material impact, as the rate of opt-out is <1/10,000 people [15]. There is also the possibility of overdiagnosis of kidney cancer (i.e., the detection and treatment of conditions that would not ultimately affect an individual’s health), particularly in cases of small renal masses and/or small renal cell carcinomas that may be indolent [16]. This has been suggested to be due to widespread use of cross-sectional imaging performed especially in elderly and/or comorbid patients (e.g., with hypertension, diabetes, etc.) [17]. It is noteworthy that our study is based on patients diagnosed with malignant kidney cancer on the basis of histology of the primary tumour (69.0%), clinical investigations (25.2%), and histology of metastasis (4.0%).
Our finding of the overall increasing incidence of kidney cancer in England during the past four decades is consistent with reports of increasing incidence in many countries in Europe, North America and Oceania [5, 18, 19]. For example, in the USA, the overall incidence rate of kidney cancer increased from 9.0/100,000 in 1985 to 16.1/100,000 in 2020 (an increase of +79%) [20]. Our finding of substantially increasing incidence of early-onset kidney cancer in young adults aged <50 years is in analogy with recent reports in the literature and commentaries and reviews in online/print media regarding the increasing incidence of early-onset cancers (often defined as cancers diagnosed in adults <50 years of age) including, cancers of the breast, colon, oesophagus, kidney, liver, and pancreas in several (particularly high-income) countries. These reports have highlighted that the incidence of early-onset cancers has dramatically increased around the world, with the rise beginning around 1990 [2, 21, 22]. This has been attributed to a birth cohort effect – for example, people born in the 1960s and 1970s experienced a higher risk of cancer before they reached 50 years of age than those born in the 1950s, and it has been predicted that this risk will continue to rise in successive generations [2].
Cancer incidence rate measures the rapidity (or ‘speed’) of the occurrence of new cases of cancer in the population within a specified time period. Increase in the incidence of a particular cancer (e.g., kidney cancer) in a population can be due to a variety of factors, which may include: in-migration of susceptible people, a change in diagnostic criteria, improved surveillance/case ascertainment, introduction of a new screening/diagnostic test, introduction of new, or changes in exposure to existing aetiological agent(s). In addition, as the incidence (i.e., risk) of most cancers in adults increases exponentially with age, there would be some expected increase in cancer incidence in older adults (i.e., aged 50+ years), as a function of the ageing population/increasing life expectancy. In our study, we not only observed increasing incidence of kidney cancer in older adults aged 50+ years, but also a substantial and unexpected increase in the incidence of early-onset kidney cancer in people aged <50 years. In a recent report, it was determined that the global incidence of early-onset cancer increased by 79% between 1990 and 2019 [23]. Possible risk factors for early-onset cancers being explored include early life and young adulthood exposures, air pollution, dietary factors, gut microbiome, physical inactivity, obesity, tobacco use and alcohol consumption [2, 23]. Considering cancer is a multifactorial disease, it has been suggested that since the middle of the last century, substantial multigenerational changes in the exposures have occurred, including changes in diet, lifestyle, obesity, environment and the microbiome, all of which might interact with genomic and/or genetic susceptibilities to increase the risk of early-onset cancer [2, 23].
It has been estimated that 34% of all kidney cancers in the UK are attributable to potentially modifiable (i.e. preventable) risk factors [7, 14]. Among these, obesity is considered to be the strongest risk factor for kidney cancer – accounting for 24% of all cases. In a population-based cohort study including 1.1 million adolescent males, a BMI during adolescence of >27.5 kg/m2 (relative to <22.5 kg/m2) was significantly associated with an increased risk of kidney cancer (at a mean of 44 years of age at diagnosis) [24]. The study concluded that preventing childhood obesity is important to decreasing the burden of kidney cancer in young adults. In an umbrella review of systematic reviews and meta-analyses, obesity was strongly associated with an increased risk of kidney cancer in both males and females – a 5-unit increase in BMI increased the risk by 24% in males and 33% in females [25]. Several mechanisms and exposures have been suggested to explain this strong association with obesity – including elevated insulin levels, a greater concentration of growth factors in adipose tissue, hypertension, cholesterol metabolism abnormalities, immune malfunction, higher oestrogen levels and increasing availability/consumption of ultra-processed foods [26]. In a recent study from the UK, ultra-proceeded foods accounted for almost 66% of adolescents’ daily caloric intake [27]. Positive association between ultra-processed foods and excess body weight was also demonstrated in a meta-analysis of observational studies [28]. There has been an enormous increase in the consumption of ultra-processed foods over the past four decades, driven by advancement in food technology/production, aggressive marketing by the food industry, globalization/urbanization, and changes in consumer dietary habits and lifestyles – ultra-processed foods have replaced unprocessed foods and traditional cooking in many countries, and now account for about half of the estimated total calories intake in most high- and middle-income countries, with children consuming more ultra-processed foods than older generations. This shift towards increased consumption of ultra-processed foods is consistent with increasing prevalence of obesity/overweight and other nutrition-related diseases [29].
Over the past four decades, there has been a steady and significant increase in the prevalence of overweight (BMI, 25–<30 kg/m2) and obesity (BMI, ≥30 kg/m2) in England – the prevalence of obesity in adult males and females aged 16+ years increased from about 6 and 9% in the early 1980s to 27 and 29% in 2019, respectively [30,31,32,33] (Fig. 2). During the same period, the prevalence of severe obesity (BMI, ≥40 kg/m2) increased 7-fold in males and 3-fold in females [30]. In the recent (2021) Health Survey for England, males were more likely to be either overweight or obese (69%) compared with females (59%) [33]. Similarly, in children aged 0–15 years, the prevalence of childhood overweight/obesity increased from 26% in 1995 to 32% in 2019 [34]. In a recent blog from the UK Department of Health and Social Care, it was reported that obesity costs the National Health Service (NHS) around £6.5 billion a year and is the second biggest preventable cause of cancer after tobacco consumption (healthmedia.blog.gov.uk/2023/06/07/). It is noteworthy that our finding of the increasing trend in the incidence of kidney cancer over the past four decades parallels the increasing trend in the prevalence of overweight/obesity in England [Figs. 1 and 2].

Trends in the prevalence (%) of obesity (three-year rolling averages) in adults aged 16+ years in England, 1993–2019 (Source: Office for Health Improvement and Disparities, OHID).
Tobacco smoking is considered to be the second most important modifiable risk factor for kidney cancer – accounting for 13% of all cases [14, 35]. In parallel with the significant increase in the prevalence of obesity over the past four decades, the prevalence of smoking has steadily declined in England – the prevalence of smoking in adult males and females aged 18+ years declined from about 35 and 31% in the mid–1980s to 14 and 11% in 2022, respectively [36, 37]. Among the current smokers, the median number of cigarettes smoked per day also declined during this period [36, 37].
Amongst the other factors associated with an increased risk of kidney cancer, the prevalence of doctor-diagnosed hypertension in adults has been fairly stable (and similar for males and females) in England over the past four decades (around 25–30%) [37]. A recent systematic review of modifiable risk factors associated with the incidence of kidney cancer, categorized obesity and hypertension as overwhelmingly harmful, smoking as harmful, diabetes as detrimental, diet (including red and processed meats) as indeterminate, and physical activity as beneficial [38]. In a recent cohort study of more than 1.6 million patients with type 2 diabetes, who had no prior diagnosis of 13 obesity-associated cancers, patients treated with the glucagon-like peptide receptor agonist (GLP-1RA) class of pharmaceuticals vs insulin had a significant risk reduction in 10 of the 13 obesity-associated cancers, which also included kidney cancer [39]. The authors concluded that their findings provided preliminary evidence of the potential benefit of GLP-1RAs for cancer prevention in high-risk groups and supported further preclinical and clinical studies for the prevention of certain obesity-associated cancers [39].
Conclusions and clinical and public health policy implications
In conclusion, this comprehensive and most up-to-date population-based cohort study of the age- and gender-specific trends in the incidence of kidney cancer (or renal cell carcinoma) in England showed that overall (i.e. all ages combined) there has been a substantial increase (+171%) in the incidence of the disease in both genders during the past four decades – which was partly driven by the largest and unexpected increase in the incidence of early-onset kidney cancer in young adults aged <50 years (+155%), with an annual year-on-year increase in incidence of +5.0% during the period 1985–2020. This increase was steepest in young males (+157%) compared with young females (+133%). Considering the trends in the prevalence of the three most important modifiable risk factors for kidney cancer (i.e. obesity, smoking and hypertension) over the past four decades, it appears that some of this increase in the incidence of kidney cancer is in analogy with the increasing prevalence of obesity in England during this period. Nevertheless, other causes (or reasons) driving this substantial and unexpected increase in the incidence of early-onset kidney cancer in young people remain elusive and need further investigation.
Considering that 34% of all kidney cancer cases are attributable to modifiable risk factors and are therefore potentially preventable (i.e. 4,692 of the 13,800 cases/year), this study has quantified the potential benefits of effective and sustained primary and secondary prevention efforts at the individual and population level to substantially reduce the burden of the disease (in the population and health services). These efforts may include maintaining a healthy weight (through a balanced diet and regular physical activity), combating factors that promote obesity in childhood/adolescence, better management of obesity (with lifestyle modifications and use of new medications such as GLP-1 receptor agonists), smoking cessation and monitoring and control of blood pressure (with diet, exercise and medication).
Data availability
Data used in the study are available from the Office for National Statistics and NHS Digital.
References
Ferley J, Ervik M, Lam F, Laversanne M, Mery L, Pineros M, et al. Global cancer observatory: cancer over time. Lyon, France: International Agency for Research on Cancer; 2024. https://gco.iarc.who.int/overtime/en. Accessed 18 March 2025.
Ugai T, Sasamoto N, Lee HY, Ando M, Song M, Tamimi M, et al. Is early-onset cancer an emerging global epidemic? Current evidence and future implications. Nat Rev Clin Oncol. 2022;19:656–73.
Bray F, Colombet M, Aitken JF, Bardot A, Eser S, Galceran J, et al. (eds.) (2023), Cancer Incidence in Five Continents, Vol. XII (IARC CancerBase No. 19). Lyon: International Agency for Research on Cancer. Available from: https://ci5.iarc.who.int. Accessed 18 August 2024.
Zhao H, Wei Q. Global and regional burden of kidney cancer: Analysis and future predictions based on GBD data from 1990 to 2021. JCO. 2025;43:21–521.
Cancer Research UK, Kidney cancer statistics (2024). https://www.cancerresearchuk.org/health-professional/cancer-statistics/statistics-by-cancer-type/kidney-cancer. Accessed 20 August 2024.
Safiri S, Kolahi AA, Mansournia MA, Almasi-Hashiani A, Ashrafi-Asgarabad A, Sullman MJM, et al. The burden of kidney cancer and its attributable risk factors in 195 countries and territories, 1990–2017. Sci Rep. 2020;10:13862.
Brown KF, Rumgay H, Dunlop C, Ryan M, Quartly F, Cox A, et al. The fraction of cancer attributable to modifiable risk factors in England, Wales, Scotland, Northern Ireland, and the United Kingdom in 2015. Brit J Cancer. 2018;118:1130–41.
Iliopolis O. Diseases of hereditary renal cell cancers. Urol Clin N Am. 2023;50:205–25.
Clague J, Lin J, Cassidy A, Matin S, Tannir N, Tamboli F, et al. Family history and risk of renal cell carcinoma: results from a case-control study and systematic meta-analysis. Cancer Epidemiol Biomarkers Prevent. 2009;18:801–7.
Yu T, Chuang Y, Yu M, Chen C, Yang C, Huang S, et al. Risk of cancer in patients with polycystic kidney disease: a propensity-score matched analysis of a nationwide, population-based cohort study. Lancet Oncol. 2016;17:1419–25.
Deb A, Okechukwu C, Emara S, Abbas SA. Occupational exposure as risk factor for kidney and bladder cancer: a systematic review and meta-analysis. Urol Nephrol Open Access J. 2019;7:143–51.
Dominik A, Colleen C. Quantitative assessment of red meat or processed meat consumption and kidney cancer. Cancer Detection Prevent. 2009;32:340–35.
Toni C, Je Y, Cho E. Analgesic use and the risk of kidney cancer: a meta-analysis of epidemiologic studies. Int J Cancer. 2014;134:384–96.
Cancer Research UK, Risks and causes of kidney cancer (2024). https://www.cancerresearchuk.org/about-cancer/kidney-cancer/risks-causes. Accessed 21 August 2024.
Henson KE, Elliss-Brookes L, Coupland VH, Payne E, Vernon S, Rous B, et al. Data resource profile: national cancer registration dataset in England. Int J Epidemiol. 2020;49:116–16.
Sohlberg EM, Metzner TJ, Leppert JT. The harms of overdiagnosis and overtreatment in patients with small renal masses: a mini-review. Eur Urol Focus. 2019;5:943–5.
Rosiello G, Larcher A, Montorsi F, Capitanio U. Renal cancer: overdiagnosis and overtreatment. World J Urol. 2021;39:2821–3.
Jani C, Abdallah N, Mouchati C, Jani R, Sharma R, Bhatt P, et al. Trends of kidney cancer burden from 1990 to 2019 in European Union 15+ countries and World Health Organization regions. Sci Rep. 2022;12:22368.
Shelton J, Zotow E, Smith L, Johnson A, Thomson S, Ahmad A, et al. 25 year trends in cancer incidence and mortality among adults aged 35-69 years in the UK, 1993-2018: retrospective secondary analysis. BMJ. 2024;384:e076962.
National Cancer Institute. Cancer stat facts: kidney and renal pelvis cancer (2024). https://seer.cancer.gov/statfacts/html/kidrp.html. Accessed 17 August 2024.
Kira S. Dramatic rise in cancer in people under 50. Brigham and Women’s Hospital Communications. 2022. https://news.harvard.edu/gazette/story/2022/09/researchers-report-dramatic-rise-in-early-onset-cancers/. Accessed 1 September 2024.
The Guardian. Cancer rates among under-50s in UK have risen 24% since 1995, figures show (2024). https://www.theguardian.com/society/article/2024/jun/02/cancer-rates-under-50s-rise-24-percent-obesity-junk-food-inactivity#:~:text=The%20number%20of%20under%2D50s,which%20affect%20the%20digestive%20system. Accessed 29 August 2024.
Zhao J, Xu L, Sun J, Song M, Wang L, Yuan S, et al. Global trends in incidence, death, burden and risk factors of early-onset cancer from 1990 to 2019. BMJ Oncol. 2023;2:e000049.
Leiba A, Kark J, Afek A, Derazne E, Barchana M, Tzur D, et al. Adolescent obesity and paternal country of origin predict renal cell carcinoma: a cohort study of 1.1 million 16 to 19-year-old males. J Urol. 2013;189:25–9.
Kyrgiou M, Kalliala I, Markozannes G, Gunter J, Paraskevaidis E, Gabra H, et al. Adiposity and cancer at major anatomical sites: umbrella review of the literature. BMJ. 2017;356:j477.
Moyad MA. Obesity, interrelated mechanisms, and exposures and kidney cancer. Semin Urologic Oncol. 2001;19:270–9.
Chavez-Ugalde IY, de Vocht F, Jago R, Adams J, Ong KK, Forouhi NG, et al. Ultra-processed food consumption in UK adolescents: distribution, trends, and sociodemographic correlates using the National Diet and Nutrition Survey 2008/09 to 2018/19. Eur J Nutr. 2024;63:2709–23.
Askari M, Heshmati J, Shahinfar H, Tripathi N, Daneshzad E. Ultra-processed food and the risk of overweight and obesity: a systematic review and meta-analysis of observational studies. Int J Obes. 2020;44:2080–91.
Baker P, Machado P, Santos T, Sievert K, Backholer K, Hadjikakou M, et al. Ultra-processed foods and the nutrition transition: global, regional and national trends, food systems transformations and political economy drivers. Obes Rev. 2020;21:e13126.
UK Health Security Agency. Patterns and trends in excess weight among adults in England (2021). https://ukhsa.blog.gov.uk/2021/03/04/patterns-and-trends-in-excess-weight-among-adults-in-england/. Accessed 16 August 2024.
NHS Digital. Health Survey for England. 2018. https://digital.nhs.uk/data-and-information/publications/statistical/health-survey-for-england/2018. Accessed 16 August 2024.
Office for Health Improvement and Disparities. Obesity profile (2024). https://fingertips.phe.org.uk/profile/national-child-measurement-programme/data#page/1/gid/1938133368/pat/159/par/K02000001/ati/15/are/E92000001/yrr/1/cid/4/tbm/1. Accessed 2 September 2024.
NHS Digital. Health survey for England. 2021. https://digital.nhs.uk/data-and-information/publications/statistical/health-survey-for-england/2021. Accessed 1 September 2024.
Broadbent P, Shen Y, Pearce A, Katikireddi SV. Trends in inequalities in childhood overweight and obesity prevalence: a repeat cross-sectional analysis of the Health Survey for England. Arch Dis Childhood. 2024;109:233–9.
Cumberbatch MG, Rota M, Catto JW, La Vecchia C. The role of tobacco smoke in bladder and kidney carcinogenesis: a comparison of exposures and meta-analysis of incidence and mortality risks. Eur Urol. 2016;70:458–66.
NHS Digital. Health survey for England, 2022 part 1. 2022. Available from: https://digital.nhs.uk/data-and-information/publications/statistical/health-survey-for-england/2022-part-1
NHS Digital. Health survey for England. 2019. https://digital.nhs.uk/data-and-information/publications/statistical/health-survey-for-england/2019. Accessed 12 August 2024.
Al-Bayati O, Hasan A, Pruthi D, Kaushik D, Liss MA. Systematic review of modifiable risk factors for kidney cancer. Urological Oncol. 2019;37:359–37.
Wang L, Xu R, Kaelber DC, Berger NA. Glucagon-like peptide 1 receptor agonists and 13 obesity-associated cancers in patients with type 2 diabetes. JAMA Netw Open. 2024;7:e2421305.
Funding
Brighton and Sussex Medical School.
Author information
Authors and Affiliations
Contributions
AM conceived and designed the study and obtained the data. YS and AM conducted the literature search and data management and analysed the data. AM and YS wrote the initial draft manuscript. AM responded to the Reviewers’ comments and revised the manuscript. MB and PZ critically reviewed the manuscript for intellectual content and verified the findings. All authors reviewed the manuscript. AM guided and supervised the overall work.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Memon, A., Salari, Y., Bawa, M. et al. Increasing incidence of early-onset kidney cancer in young adults aged <50 years in England: an analysis of the national cancer registration data by age and gender, 1985–2020. BJC Rep 3, 32 (2025). https://doi.org/10.1038/s44276-025-00149-y
Received:
Revised:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s44276-025-00149-y
