
Abstract
Background
There is large variation in case-fatality rates of breast cancer in young women across the world. The objective of this study was to estimate the ten-year overall survival of women diagnosed with breast cancer before age 40 in six countries, by clinical presentation and by treatments received.
Methods
Data were supplied by seven centers in six countries, including the USA, Canada, Poland, Iceland, Iran and Thailand, totaling 36,861 women diagnosed with breast cancer before age 40, from 1977 to 2020. American patients from the SEER registry were sub-divided into (Non-Hispanic) White and Black. The following factors were compared across countries: year of diagnosis, tumor size, lymph node status, estrogen receptor (ER) status, use of chemotherapy, use of tamoxifen and use of radiotherapy. The Kaplan-Meier method was used to estimate ten-year overall survival for patients in each center. Cross-center comparisons are provided. The Cox Proportional Hazards model was used to estimate the impacts of the various factors on death for each center separately and for all centers combined, for all patients and for patients with stage I breast cancer. For these comparisons, SEER white women were considered the reference group.
Results
The mean age of diagnosis was 35.4 years. The percentage of patients with node-positive breast cancer ranged from 48.5% in Poland to 53.4% in Iceland. Mean tumor size ranged from 2.1 cm in Poland to 3.5 cm in Iran. The percent of patients with ER-negative breast cancer ranged from 34.0% in USA White women to 47.4% in Canada. The use of chemotherapy ranged from 65.4% in Thailand to 78.8% in Poland. Ten-year survival rates ranged from 52.5% (95%CI: 50.4%-54.7%) in Thailand to 77.9% (95%CI: 75.5%-80.3%) in Poland. A two-fold variation in case-fatality across centers persisted after adjusting for year of diagnosis, stage, tumor features and treatment. The difference in case-fatality across countries was greatest for patients with stage I breast cancer (four-fold variation).
Conclusions
There is a wide disparity around the world in the long-term survival of women diagnosed with breast cancer before age 40, which cannot be accounted for by differences in screening, tumor stage at presentation or other tumor features. It is possible that differences in survival are due to inherent ethnic differences and/or differences in cancer management, but more research is required.
Similar content being viewed by others
Introduction
Breast cancer in young women (i.e., diagnosed before age 40) is rare but carries a disproportionate burden due to its relatively poor prognosis, a high prevalence of adverse tumor features, and a greater impact on life expectancy than for older patients [1,2,3]. Young women with breast cancer face unique challenges, including concerns about fertility and early menopause as a result of breast cancer treatments, as well as long-term side effects. Most single-center studies have been too small to permit a comprehensive investigation of those factors that predict survival. Current guidelines recommend chemotherapy be given to most women under 40 with cancers greater than 2 cm in size or with one or more positive nodes [4]. However, chemotherapy decisions are also influenced by tumor subtype, and for hormone receptor–positive disease, by the results of molecular (genomic) assays that help predict chemotherapy benefit. Molecular assays in use today sub-group patients into those under 50 or over 50 at diagnosis; the possibility of de-escalation of chemotherapy for women under 40 deserves our attention.
Among older women with breast cancer, incidence rates are highly variable around the world, but mortality rates are relatively stable [5, 6]. In contrast, in women diagnosed before age 40, incidence rates of breast cancer are relatively stable around the world, whereas mortality rates are variable. International comparisons of treatment and outcomes are a means of identifying factors that may help inform better cancer control strategies and improve outcomes.
In older women, international variation in screening (and the risk of overdiagnosis) is a major factor in driving disparities in case-fatality worldwide, more so than differences in treatment [5, 6]. In contrast, in young women, wide variation in mortality rates exists in the presence of relatively stable incidence rates [7}. Moreover, women under 40 at average risk are not candidates for screening, and most detected breast cancers are palpable, found either by the patient or by their health care provider. As such, variations in survival do not reflect screening patterns, but rather stage at diagnosis, differences in the cancer features, differences in treatment, or possibly inherent ethnic variation.
Treatment patterns and protocols vary considerably around the world; for example, whether or not age at diagnosis should be considered in the decision to prescribe chemotherapy varies across national guidelines [4, 7,8,9]. It is important to determine to what extent variation in treatment protocols in different countries and regions around the world affects survival. Unfortunately, many national cancer registries do not include data on stage, tumor subtypes, treatment, or survival.
In this study, we examine survival outcomes of young women with breast cancer in seven populations in six countries around the world. The sources of the patient populations varied and included national and regional cancer registries and single hospital case records. The years at diagnosis also varied considerably from center to center. We ask to what extent, globally and within each country, the ten-year survival rate is associated with stage at diagnosis, tumor characteristics, or the receipt of various treatments at the time of diagnosis. Differences in treatment may be due to variations in treatment recommendations, in access to care, in patient adherence (for clinical reasons), or treatment abandonment (for reasons other than adherence). To the extent that disparities in survival can be shown to depend on stage at diagnosis and/or variation in treatment, we hope to mitigate the disparity between centers and improve outcomes for young women with breast cancer.
Methods
We collected clinical data on unselected women diagnosed with breast cancer before age 40 from seven historical cohorts in Canada, Poland, the United States (two), Iceland, Thailand, and Iran. In three centers, the data was collected from a single hospital (Canada, Iran, Poland), and in three centers data was collected from national or regional cancer registries (Iceland, USA, Thailand). The data from the USA was extracted from the SEER registry and was divided into Non-Hispanic White (hereafter referred to as “White”) and Black. Details of the individual sources are presented in Supplementary Table 1.
Eligible patients included female patients diagnosed with Stage I to Stage IV invasive breast cancer between 1977-2002 (individual centers’ recruitment dates differ, depending on access to data). Patients must have been diagnosed at or after their twentieth birthday, and before their fortieth birthday. Patients with missing data on year of diagnosis or follow-up years were excluded. Patients with stage 0 breast cancer (DCIS) were excluded. Two centers (Canada and Poland) did not include patients with stage IV breast cancer. Additional details for the databases from which patients were included in this study have been published elsewhere (Thailand [10], Canada [11], Poland [12], Iceland [13], Iran [14]). For the USA sites, the SEER 12 registry was used, November 2022 submission (1992-2020) [15].
For each center, information was requested for each patient on year of diagnosis, age at diagnosis, tumor size, lymph node status, distant metastases (stage at diagnosis), estrogen receptor (ER) status, HER2 status, use of radiotherapy (at diagnosis/within 6 months), use of chemotherapy (at diagnosis/within 6 months), use of endocrine therapy (at diagnosis/within 6 months), current vital status, date of death and follow-up time in months. Data on genetic predisposition or family history were not available.
Using the variables tumor size (continuous), lymph node status (negative/positive), and distant metastasis status (negative/positive), stage at diagnosis was defined as the following:
Stage I: tumor size up to 2.0 cm, lymph node negative, and distant metastasis negative
Stage II: tumor size up to 2.0 cm and lymph node positive, OR tumor size 2.1 cm to 5.0 cm, OR tumor size more than 5.0 cm and lymph node negative (all with distant metastasis negative)
Stage III: tumor size more than 5.0 cm, lymph node positive, and distant metastasis negative
Stage IV: any tumor size, any lymph node status, and distant metastasis positive
Patients were followed from the date of diagnosis to the date of death or the date of last follow-up. The Kaplan-Meier method was used to estimate the five- and ten-year survival rate for all-cause mortality for women from each site and for all sites combined (for Iran, we could estimate five-year survival but not ten-year survival due to a lack of sufficient follow up). Frequency data (tables and graphs) were used to describe the observed differences in tumor features, treatments and survival between institutions. Formal statistical tests were not performed for all comparisons. The Cox proportional hazards model was used to estimate the unadjusted (univariate) and adjusted multivariable hazard ratios for death associated with various factors, including year of diagnosis, center, patient characteristics, clinical presentation, tumor pathology and all treatments received on the risk of all-cause death, first, for all patients and second, for patients with stage I breast cancer only. For comparing hazard ratios by country, the SEER white cohort was used as the reference group.
Ethics approval for the release of data was obtained locally at each site. The Ethics Committee at Women’s College Hospital exempted the analysis of the anonymous secondary data from requiring ethics approval (REB # 2017-0076-E).
Results
We collected data on a total of 36,861 women diagnosed with breast cancer before age 40 at seven centers worldwide (Table 1), including: White women from the USA (N = 27,216), Black women from the USA (N = 4949), the Iceland Cancer Registry (N = 171), Thailand regional cancer registries (N = 2279), the Iran Cancer Institute (N = 711), Women’s College Hospital in Toronto, Canada (N = 231), and the International Hereditary Cancer Center in Szczecin, Poland (N = 1304). Across the seven sites, the median year of diagnosis ranged widely, from 1994 (Canada) to 2017 (Iran). Women were followed for a median of 8.3 years overall, ranging from 5.5 to 10.8 years, according to the site.
Overall, the five-year all-cause survival was 81.8%, and the ten-year all-cause survival was 72.1% (confidence intervals shown in Table 1). Figure 1 shows the variation in five- and ten-year survival rates across the seven centers. Five-year survival rates ranged from to 63.5% (Thailand) to 87.9% (Poland)) (Fig. 1a). Ten-year survival was lowest in Thailand (52.5%) and highest in Poland (77.9%) (Fig. 1b). It was 75.6% in USA White women, was 72.7% in Iceland, was 62.1% in USA Black women, and was 59.0% in Canada. We did not have data on ten-year survival for Iran.

a Five-year survival among women with breast cancer before age 40, by center. b Ten-year survival among women with breast cancer before age 40, by center*. *Iran is not included in this analysis due to a lack of follow-up.
Table 1 also includes five- and ten-year survival estimates after excluding cases with metastatic disease (stage 4) since this data was not available for all centers. Survival for non-metastatic cases is also depicted in Kaplan-Meier curves (Supplementary Fig. 1.) Ten-year survival varied from 56.7% in Thailand to 79.6% in USA white women. When restricted to non-metastatic cases, the pattern across centers was similar as in the entire cohort (Poland, Iceland and USA white women had the highest survival).
Figure 2a–g shows the distribution of key clinical variables by center, sorted according to ten-year survival (excluding Iran), in order to identify those variables that correlate with ten-year survival. (The frequency data and percentages described do not include missing data; the number of subjects with missing data is shown in Table 1).

a mean tumour size (mm). b percent lymph node-positive. c percent stage I at diagnosis. d percent stage IV at diagnosis (excluding Canada and Poland). e percent ER-positve. f percent using chemotherapy. g percent using radiotherapy.
Mean tumor size at diagnosis ranged from 2.1 cm (Poland) to 3.5 cm (Iran). There was some trend for those countries with high mean tumor sizes to have poor ten-year survival, compared to those with smaller mean tumor size (Fig. 2a). The proportion of women presenting with node-positive disease at diagnosis was similar across all countries, and ranged from 48.5% in Poland to 53.4% in Iceland. Node-positivity did not correspond with ten-year survival (Fig. 2b). In contrast, the proportion of patients diagnosed at stage I varied widely, ranging from 11.7% (Thailand) to 34.7% (Poland), and there was a marginal correspondence with this proportion and ten-year survival (Fig. 2c). After excluding stage IV patients (Canada and Poland did not provide data on stage IV patients), the proportion of stage I cases ranged from 12.5% in Thailand to 34.7% in Poland, and the ordering of centers relative to each other did not change.
Among the four centers with data on stage IV cases, the percentage of patients diagnosed with stage IV breast cancer varied from 4.3% (Iceland) to 9.4% (USA Black women), and also marginally corresponded with the trend in ten-year survival (Fig. 2d).
The proportion of women with ER-positive disease ranged from 52.6% (Canada) to 66.0% (USA white), with no clear correlation with ten-year survival (Fig. 2e). In the USA, the percentage of patients with ER-positive disease was 60.8% for Black women.
Three centers provided data on ER-status and tamoxifen use; the proportion of women with ER-positive breast cancer who received tamoxifen ranged widely, from 24.8% in Canada to 84.0% in Iceland and 90.4% in Poland (p < 0.0001). This corresponds with the trend in ten-year survival rates for ER-positive cancers across these three centers. Notably, the median year of diagnosis varied widely across these centers (Canada 1994; Poland 2006; Iceland 2008) indicative of a rise in the use of tamoxifen over the entire study period.
The majority of women received chemotherapy at primary diagnosis (73.0%). Use of chemotherapy ranged from 65.4% (Thailand) to 78.8% (Poland) across the centers and appeared to correlate positively with ten-year survival (Fig. 2f). The proportion of women who received adjuvant radiation ranged widely, from 44.5% (USA Black women) to 80.0% (Iran), but there was no clear correlation with the trend in ten-year survival (Fig. 2g). We did not have data on the use of chemotherapy after distant recurrence.
Among stage 1 patients, five-year survival rates ranged from to 85.4% (Iran) to 100% (Iceland)) (Fig. 3a). Ten-year survival rates for stage 1 patients (excluding Iran) ranged from 78.7% in Canada to 90.1% in USA White women (Fig. 3b). The use of chemotherapy among stage I subjects varied widely; it was low in Canada (32.3%) and in Iceland (43.6%) and was high in Poland (68.6%) and in Thailand (75.3%), however, chemotherapy use did not clearly correspond with the trend in ten-year survival for stage I patients (Fig. 3c).

a five-year survival (sorted high to low). b ten-year survival (sorted high to low; excluding Iran). c percent using chemotherapy sorted by the trend in ten-year survival (excluding Iran).
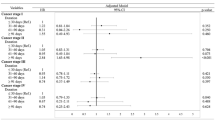
Next, we used a Cox proportional hazards model to examine the impact of the various factors on survival in each center (Supplementary Tables 2a–2g), and in all centers combined (Table 2a). Year of diagnosis, tumor size, node-status, ER status, and use of radiotherapy were significant independent predictors of outcome for all centers combined. Chemotherapy use was not found to predict ten-year survival among all patients combined. In the unadjusted analysis, patients in Iran, Thailand, Canada, and Black women from the USA had relatively poor survival compared to White women from the USA. After adjusting for year of diagnosis, tumor size, node-status, ER-status, and use of radiotherapy, patients from Thailand, Iran, USA Black, Canada, and Poland had significantly worse survival than White women in the USA. Patients from Iceland had similar survival to White women from the USA. The multivariable hazard ratios are depicted graphically in Supplementary Fig. 2a.
In each of the seven centers, in multivariable analyses, larger tumor size and node-positivity were associated with increased risks of death (supplementary Tables 2a–2g). The impact of ER-positivity on survival was not consistent across centers. In the USA, Black and White women, positive ER status was associated with a significantly decreased risk of death. In Poland, Canada, Thailand, Iceland, and Iran, ER-status did not predict death. For Poland, Canada, and Thailand, the models were adjusted for the impact of tamoxifen use. In a separate analysis of the centers from Poland, Canada, and Iceland (supplementary Table 2h), tamoxifen use was associated with a significant reduction in the risk of death (adjusted HR 0.48; 95% CI 0.36–0.65; p < 0.0001).
The observed impact of chemotherapy on the risk of death varied widely across centers in the multivariable analysis (i.e., after adjustment for age at diagnosis, tumor size, lymph nodes, ER status, and use of radiotherapy). In Canada and Iran, there was a significant reduction in the risk of death associated with the use of chemotherapy. In the USA White women had a significantly increased risk of death associated with the use of chemotherapy.
In the USA, women (White and Black) in the multivariable analysis there was a significant reduction observed in the risk of death associated with the use of radiotherapy. In Canada, in Poland, in Iran, and in Iceland, there was no significant impact of radiotherapy use on the risk of death. In Thailand, there was a significant increase in the risk of death associated with radiotherapy. However, we did not have data on the type of surgery (lumpectomy versus mastectomy) and we were unable to restrict this analysis to lumpectomy patients.
Next, we restricted the Cox model analysis to stage I patients (Table 2b). Among stage I patients, recent year of diagnosis was a significant independent predictor of better survival, as were positive ER-status and the use of radiotherapy. Compared to USA White women, women in Canada, USA Black, Thailand and Iran had worse survival after stage I breast cancer. The multivariable hazard ratios for stage I patients are depicted graphically in Supplementary Fig. 2b.
In the USA, White and Black women differed across many of the features examined. Black women had fewer tumors of 2.0 cm or smaller (37.2% vs. 45.8%). The percentage of Black and White patients with node-positive cancer was similar (48.7% for White women vs. 52.5% for Black women). Black women were less likely to be diagnosed at stage I compared to White women (22.4% vs. 29.8%). Black women had more ER-negative tumors than White women (39.2% vs. 34.0%). The use of chemotherapy was similar; 73.7% for White women and 72.3% for Black women. Among ER-positive patients from the USA, use of chemotherapy was 72.7% for White women and 71.4% for Black women. Among ER-negative patients from the USA, use of chemotherapy was 83.8% for White women and 81.5% for Black women. In the USA, the use of radiotherapy was 48.5% for White women and was 44.5% for Black women. Crude survival at 10 years was 62.1% for Black women and was 75.6% for White women. Among stage I patients, crude 10-year survival was 83.1% for Black women and was 90.1% for White women. Compared to White women from the USA (all patients; Table 2a), the univariate hazard ratio for death for Black women was 1.61 (p < 10−4), which did not change after adjustment for size, nodes, ER status, or treatment (multivariable HR 1.54; p < 10−4). Among stage I patients, the univariate hazard ratio for death for Black vs. White women was 1.69 (95% CI 1.45–1.97) and did not change after adjustment.
The year of diagnosis varied considerably for patients across centers. Year of diagnosis was a strong and significant predictor of outcome (Table 2). Ten-year survival increased from 66.1% in 1970-1995 to 74.8% in 2011–2015 (Fig. 4). Consequently, we compared key tumor features according to the year of diagnosis for all patients in the study (Table 3). Mean tumor size increased from 2.7 cm to 3.2 cm with time. Node positive status was relatively stable. Stage I diagnoses decreased over the time from 31.7% to 23.1%, whereas stage 4 diagnoses increased from 3.7% to 8.2%. ER positive status increased from 55.1% to 72.4% across the time periods. HER2 positive status decreased from 32.6% to 26.5%. Tamoxifen use among patients with ER positive breast cancer increased dramatically over time from 15.5% to 95% for the three centers which provided tamoxifen data. Chemotherapy use increased from 66.3% in 1970-1995 to 74.5% in 2001-2005, and stabilized thereafter. Radiotherapy use was relatively stable over time.

Ten-year survival by period of diagnosis (all centers).
Because not all centers were represented in all the time periods, these variables were analyzed by period of diagnosis for White women from the USA only (supplementary Table 3; first for all patients, and then for patients treated with chemotherapy, and then for patients treated without/unknown chemotherapy). The trends seen among USA White women were similar to those seen in the full cohort. The improvement in ten-year survival over time among USA White women was more pronounced for those who received chemotherapy (64.8% vs. 78.8%) than for those who did not receive chemotherapy (78.2% vs. 83.4%).
Discussion
Young-onset breast cancer (i.e., breast cancer before age 40) is characterized by relatively poor survival. This remains true after adjusting for the fact that young women are more likely to have breast cancers diagnosed at an advanced stage and with poor prognostic features, such as high-grade and triple-negative status [2, 3, 16,17,18,19,20,21]. In many previous studies, the relatively poor prognosis of young women was most evident among the subset of women with ER-positive, early-stage tumors [22,23,24,25,26,27,28]. At present, most clinical guidelines do not consider young age to be an independent factor in determining candidacy for chemotherapy [4, 7,8,9].
We sought to determine to what extent treatment (and other features) of breast cancer differ around the world for young women with breast cancer, and whether these differences impact survival rates. In this international, multicenter cohort study of 36,861 women diagnosed with breast cancer before age 40, we observed significant variation in the five- and ten-year survival rates across seven different centers, which span six countries in three continents. Ten-year survival rates varied widely from 70 - 80% in Poland, Iceland, and in US White women, to 50–60% in Canada, Thailand, and USA Black women. There was wide variation seen across countries in terms of year of diagnosis, stage at diagnosis, tumor features (ER status), and treatments received (chemotherapy and radiotherapy); however, even after adjusting for year of diagnosis and these other factors, a significant survival disparity remained. The highest survival was seen for White women from the USA. Compared to White women from the USA, the adjusted hazard ratio for death was 1.5–2.0 (p < 0.0001) for centers in Canada, USA, Black women, Thailand, and Iran. The survival differences were less pronounced for Poland (HR = 1.15, p = 0.03) and for Iceland (HR = 1.05, p = 0.8).
Notably, patients diagnosed in more recent years (2011–2015) experienced much better survival than those diagnosed in earlier periods (1970–1995). This was not accounted for by a trend towards earlier stage at diagnosis; when comparing the key clinical features across the time periods, both for all patients in the study and for White women from the USA only (74% of all patients in the study), the mean tumor size and the proportion diagnosed at stage IV increased over time. There was a minimal trend in the use of radiotherapy or in the proportion of patients presenting with positive node status. HER2 positivity declined marginally over time, and ER-positivity increased over time. This suggests that the improvement in mortality is not due to earlier detection per se but due to changing treatment patterns, and/or improved adherence to treatment. Tamoxifen use and chemotherapy use increased over time. Unfortunately, we did not have information regarding the specific chemotherapy regimens used, nor on the use of adjunct ovarian suppression regimens (pharmaceutical or surgical) or on second line-chemotherapy. These factors will be important to include in future studies. Aromatase inhibitors are not prescribed for premenopausal patients in the absence of ovarian suppression. However, trastuzumab is indicated for young HER2-positive patients. We saw an improvement in the survival of HER2-positive patients in recent years. Trastuzamab and ovarian suppressors are generally more available in the U.S. and higher-income countries than in low and middle-income countries.
A similar trend in survival was also seen in a recent study of 500,000 women with early invasive breast cancer in England [29]. In that study, the annual mortality rate for women ages 18-39 years declined by 2-fold from 1993-1999 to 2010–2015, after adjusting for ER status, tumor size, number of nodes, tumor grade, time since diagnosis, breast cancer laterality, and socioeconomic status. The authors suggest that changing the biology of the disease, new systemic therapies, and/or targeted surgery and radiotherapy could improve mortality [29]. Changing biology of the disease is an interesting but speculative hypothesis, which could be confirmed through genomic analysis of the tumors.
The data on survival of young women with breast cancer reported here are in line with results from most single-center studies [29,30,31,32,33,34]. Previous international comparisons of survival had limited information on the clinical features of the cases in the different countries, leading to speculation about the role that access to, and quality of care, played in explaining differences in survival. In contrast, the current study is the most comprehensive study to date on breast cancer survival in young women, analyzed by country of residence, stage at diagnosis, tumor features and treatments received. The data from this study may help us to evaluate the overall effectiveness of different management approaches of young-onset breast cancer and therefore may be used to help optimize cancer-control strategies worldwide.
Why do breast cancer survival rates differ?
Despite our detailed analysis, the reasons for the observed discrepancies in survival for young women with breast cancer diagnosed in different countries remain unclear. The strongest prognostic factor in our cohort was year of diagnosis; however, adjusting for year of diagnosis did not eliminate the disparity in survival across the countries. Other possible reasons for the survival differences include differences in stage at presentation (e.g. stage I and stage IV), differences in tumor features (ER-status), differences in treatment, and differences in intrinsic disease aggressiveness according to ethnicity. It is also important to consider whether the cases sampled are representative of the entire country and if there are errors or incompleteness in data collection. We consider these possibilities in turn.
Stage at diagnosis
Survival from breast cancer is worse the later the stage of disease at diagnosis, therefore it is expected that overall survival results will depend on the stage distribution. In this study, the proportion of cases diagnosed with stage I breast cancer varied from 11.7% to 34.7% across the different centers. Thailand had the fewest stage I cases, and also had worse survival outcomes. The percentage of patients diagnosed with small tumors (under 2.0 cm) was also lowest in Thailand. However, the difference in survival observed between countries was not reduced after adjusting for size and nodes. Based on this, it is unlikely that the stage at clinical presentation is responsible for the wide disparity seen in survival; however, residual confounding and unmeasured factors may contribute.
Tumor features (ER status)
Differences in tumor features, or the impact of the various tumor features in the different patient populations, could have influenced the survival disparity observed between centers. Positive ER status is usually considered to be a good prognostic indicator among patients with breast cancer; it is often stated that the poor prognosis of young patients is due, in part, to the fact that young women are more likely to have ER-negative tumors than older women. However, we and others have shown that the beneficial prognostic effect of ER status is less profound in young women than in older women [22, 25,26,27,28]. In young women, survival is similar for ER-positive breast cancer and ER-negative breast cancer patients [22].
In our study and in others, the relatively poor prognosis of young women was most profound for the subset of patients with early-stage, ER-positive breast cancer [27, 35,36,37]. In the current study, the prognostic effect of ER status varied from country to country. Due to the overrepresentation of SEER patients in this study and limited power to investigate the impact of ER status on survival in the smaller centers, our overall result showed a reduction in death associated with ER-positive status (adjusted HR 0.85; 95% CI 0.81-0.89). In other studies of the SEER database, there also appears to be a reduction in death associated with ER-positive breast cancer for young women; however, it is noted that the beneficial effect is less than what is seen in older women [26]. The reasons for the conflicting results in SEER versus other studies [22, 25, 27, 28] are unclear, but may reflect a lack of data in the SEER database on tamoxifen use and other potentially confounding variables. The proportion of patients with ER-positive breast cancers in this study varied from 52.6% to 66.0%, however, adjusting for the variation in ER status across cohorts did not account for the survival disparity observed, which is what we would expect if ER-positive status was not an important prognostic factor. There were also variations seen in HER2 status and in the use of tamoxifen among ER-positive patients, but these data were insufficient for robust statistical analysis. We did not study tumor grade due to a lack of data from all sites.
Differences in treatment
Significant variation in the receipt of chemotherapy and radiotherapy was observed between centers.
In randomized trials, both chemotherapy and radiotherapy have been shown to reduce breast cancer mortality in young women [38,39,40]. Radiotherapy was observed to predict reduced mortality in this study, but adjustment for the use of radiotherapy did not impact on the survival differences observed between centers. The benefit of radiotherapy was small, and we were unable to adjust for the uptake of surgery or the type of surgery (lumpectomy versus mastectomy). Radiotherapy is more commonly used in lumpectomy patients - who tend to have better survival. Chemotherapy was not found to be a predictor of survival in the multivariable analysis of all centers combined. This is likely a consequence of the observational nature of the study. It is difficult to evaluate chemotherapy benefit from observational studies. Because there was no benefit found in the model, adjustment for chemotherapy in our model would not be expected to impact the results. This does not mean, however, that chemotherapy did not influence the survival outcomes of patients in this study. Those with chemotherapy are likely to have larger and more aggressive cancers. We also did not have data on neoadjuvant versus adjuvant chemotherapy, nor on the receipt of more recent types of treatment, such as pembrolizumab, CDK4/6 inhibitors, or second-line treatments (after distant recurrence). Variation in the receipt of chemotherapy or other treatments therefor,e may still play a role in the observed variation in survival outcomes. We did not have data on the use of imaging studies at follow-up for detecting invasive cancer recurrence.
Treatment guidelines vary more widely for young women than they do for the general breast cancer population. The inferior prognosis for women under age 40 is especially apparent among early-stage, ER-positive breast cancer patients [22]; however, this subgroup is not typically recommended for chemotherapy unless there is a high-risk indicator, and in many countries, young age alone is not usually considered to be a “high risk” indicator [9]. For example, the most recent ESMO international guidelines for breast cancer in young women (BCY5) reiterate that young age should not be a factor itself when considering chemotherapy, and state that in many cases, young women with low-risk ER-positive breast cancer likely can safely omit chemotherapy [9]. In contrast, the 2024 NCCN guidelines suggest that age may be a factor when considering whether to administer adjuvant chemotherapy in patients with hormone receptor-positive, HER2-negative tumors, along with size, node status, comorbid conditions, and/or the results of a gene expression profile test. However, explicit recommendations about chemotherapy in young women with traditionally “low risk” features is not mentioned [4]. In some guidelines, it is acknowledged that the Oncotype DX recurrence score categories differ for women under and over 50 years; for example, it is stated that among women ages 50 and older, an intermediate score of 11 to 25 does not predict a benefit of chemotherapy in addition to endocrine therapy among ER-positive patients, whereas there might be a benefit for women under age 50 [4, 7]. To our knowledge, no guidelines explicitly state that young women should get chemotherapy. It is notable that despite the introduction of new treatments for ER-positive, triple negative and HER2+ breast cancer patients in the last two decades, there has been no significant increase in the five- or ten-year survival for young women since 2001 in the SEER dataset (or in other countries) (Table 3).
In many guidelines, young women are advised to discuss fertility concerns and fertility preservation when considering chemotherapy [4, 9]. This is not a consideration for postmenopausal women with breast cancer and may be a relevant factor guiding treatment decisions among young women in some populations. For example, due to variations in parity and the average age at childbearing, young women with breast cancer in some populations may be more likely to have fertility concerns than women from other populations, impacting their decisions about chemotherapy and other treatments.
We examined survival rates and conducted Cox regression models predicting mortality separately for stage I patients. Overall, ten-year survival for all stage I patients in our study was 89%. It was 90% for White women from the SEER database. In a previous SEER study, young women with stage I breast cancer were 1.44 times more likely to die of breast cancer than women aged 40 or older with stage I breast cancer [27]. The difference in mortality rates for younger versus older women diminished with more advanced stages of diagnosis. Among stage I patients, women from Canada, Thailand, Iran, and Black women from the USA had relatively poor survival (adjusted HR 1.65–4.17) compared to White women in the USA. This suggests that disparities exist either in the inherent aggressiveness of cancer between patients from those centers or in the treatments received and/or their effectiveness. There was no clear correlation between the risk of death among stage I patients and the receipt of chemotherapy; Iran and Thailand had relatively high rates of chemotherapy use in stage I subjects compared to other centers, but relatively poor survival.
The lack of a clear correlation observed here between treatments received and crude survival does not mean that treatment differences are not relevant. The treatment data in the different centers were limited and did not include information on aspects such as the timing of chemotherapy, delay in treatment, follow-up care, or the specific types of surgery, radiation, or systemic therapies. Our study, although detailed, illustrates the inherent limitations in using observational data to assess outcomes of treatment in cancer patients and emphasizes the ongoing importance of randomized trials.
Ethnic factors
One of the striking findings in this study was the difference in outcome between Black and White women from the USA. This survival difference persisted after adjusting for prognostic factors and treatments. This has been shown in several previous studies, both in the general population of breast cancer patients [41], and in young women specifically [32, 33]. In an analysis of women from the United States diagnosed with breast cancer before age 35 between 1990 and 1998, African American women had an increased hazard of breast cancer death compared with non-Hispanic White women after adjustment for stage, grade, lymph node status, and treatment (HR 1.3; 95% CI 1.1–1.7). This remained elevated after adjusting for age, education, and income (HR 1.3; 95% CI 1.03-1.6) [33]. In the POSH study, 2956 patients aged less than 41 years with breast cancer between 2000 and 2008 from the United Kingdom were followed prospectively. The five-year overall survival was significantly lower for Black patients (71.1%) than for White patients (82.4%; p = 0.02). After adjusting for tumor size, grade, nodal status, and BMI, Black ethnicity remained a significant predictor of poor prognosis (HR 1.5; p = 0.02). In that study, Black ethnicity was a significant independent predictor of poor prognosis in ER-positive patients (HR 1.6; p = 0.035) but not in ER-negative patients (HR 1.3; p = 0.4) [32]. In the POSH study, none of the patients were eligible for breast screening, and all received publicly funded health care.
It is likely therefore that there is an innate difference in the biology and aggressiveness of tumors arising in Black women compared to White women, although we cannot rule out an impact of differences in treatments received (guideline concordant care) or treatment completion (due to non-adherence or abandonment), as well as differences in access to care, or social determinants of health. Ethnicity may also be an independent prognostic factor underlying the survival differences between ethnic groups in this study, such as Iran and Thailand, but this is speculative. Interestingly, ethnicity has been found to be relevant in other subgroups as well. We have previously shown that Asian patients, including Chinese and Filipino women in the US, experience better survival than US white women after adjusting for other prognostic features. In a SEER-based study of Chinese and White women with breast cancer, Chinese women were found to have superior breast cancer-specific survival rates (HR 0.71; p < 0.0001) after matching for all prognostic features in a propensity-matched analysis [42]. Similarly, in an analysis of Filipino and White women in the SEER database, despite presenting with more advanced breast cancers, Filipino women had superior survival compared to white women (propensity-matched HR 0.73; 95% CI 0.66-0.81) [43].
Artifact/chance
Another possible explanation is that the observed differences in survival are due to limitations in the study design. Cases included in the study varied widely in terms of year of diagnosis, and year of diagnosis was a significant predictor of survival in multivariable analysis. However, even after adjusting for year of diagnosis, the survival differences persisted. Another possible explanation could be the completeness of follow-up, which may have varied between centers and impacted the estimated survival rates [44]. Because not all centers reported the cause of death, we used all-cause mortality as the endpoint, but it is expected that fewer than 5% of women under the age of 40 years would die of another cause within ten years (see Table 1).
We included stage IV patients in this analysis, but stage IV patients were not included in the datasets from Canada and Poland. However, we chose to retain the stage IV patients in the other five centers for completeness, and the small number of stage IV patients omitted is unlikely to have unduly influenced our results.
We did not do genetic testing as part of this study, and we did not have mutation status for those who were tested. Founder mutations in BRCA1 and BRCA2 are relatively common in young breast cancer patients in Poland and Iceland [45, 46]. It is our intention to do a follow-up study for carriers versus non- carriers in the Polish patients, all of whom were tested.
We did not report data on PR status, Ki-67, tumor grade, molecular/genomic subtype, and several other tumor features, that may have varied between the centers and influenced the treatments given or the outcomes observed. We did not have data on the number of positive lymph nodes for each site, and this limited our ability to discern between stage II and stage III patients, and therefore our ability to provide stage-specific estimates (beyond stage I). We have noted that there has been a decline in Stage I and an increase in Stage IV with time, this is likely due to changes in staging protocols which are now more sensitive to detecting small positive nodes and distant recurrences.
In terms of treatment, we only included data on the treatments given at the time of diagnosis. Centers based on registry data would have only had treatment data for the first 6 months of diagnosis. We did not include data on type of surgery, on neoadjuvant chemotherapy, or on newer treatments such as CDK4/6 inhibitors and dual-target anti-HER2 treatments. Data on the surgical approach were not available in all centers and were accordingly not included. Access to these treatments may have varied between the cohorts studied, and this may have impacted the survival disparities reported. We did not have data on treatment adherence, and this also may have contributed to the observed survival variation [47]. We also did not have data on tamoxifen for many centers; therefore, it is still a possibility that the survival difference is related to differences in the use of hormonal therapy among ER-positive patients. We did not have data on ovarian suppression, which may be used in young women. We did not have data on the uptake of surgery or the type of surgery (lumpectomy versus mastectomy) for all centers. Our data on chemotherapy and radiotherapy were also grouped as “yes” vs. “no/missing”, as this was the only output available for SEER patients. It is possible that differences in missing treatment data across the centers has skewed the comparative analysis.
Despite a common protocol for submitting the data, some datasets were pre-existing and data was not collected according to a standard protocol. There are also differences from center to center in terms of the way that diagnoses and pathology are performed and recorded, which may have contributed to differences. The clinical stage recorded depends on the extent of investigation, which may vary between centers and countries.
Some centers were relatively small, limiting the analysis of smaller subgroups. The difference in sample size for the different centers may have resulted in power issues when comparing survival outcomes. There was also an over-representation of USA white women in all of the grouped statistics, which would have impacted the results and conclusions. Some centers also had more patients lost to follow-up than others, and shorter follow-up times in general, and this may have impacted the survival estimates. Statistically, we assumed proportionality in our Cox model, which may not have been the case for all variables. However, most established research on these variables is consistent with proportionality in the ten-year range. We had also had variable years of diagnosis. Although disparities persisted after adjustment for year of diagnosis, differences in data sources and health-system contexts limit direct, like-for-like comparisons between centers. We also did not perform statistical tests for between-country comparisons; this is an opportunity for future studies with more and larger datasets. We subdivided the USA cohort into Black and White women, but it was not possible to subgroup patients from other centers according to different ethnic sub-populations (that could have different outcomes) and for these countries we assumed they were genetically homogeneous.
The study is in large part descriptive and for many of the visual representations (Figs. 1 to 4) we did not conduct formal analyses to assess the statistical significance of the differences. Despite these limitations, our study is the first with detailed clinical data looking at long-term survival comparisons across multiple different centers with different socioeconomic status, ethnicities and health care contexts. We report a significant variation in long-term survival among women diagnosed with breast cancer before age 40 in different centers around the world. The differences are not clearly explained by variations in stage at diagnosis or in differences in treatments received. Further studies are required to pinpoint the reason(s) for the disparity and to inform cancer control protocols for this underserved population.
Data availability
The data used in this study, except for the USA SEER data, cannot be shared due to data use agreements. Aggregate data can be shared by the corresponding author upon reasonable request.
References
Sopik V. International variation in breast cancer incidence and mortality in young women. Breast Cancer Res Treat. 2021;186:497–507.
Fredholm H, Magnusson K, Lindström LS, Eaker S, Frisell J, Holmberg L, et al. Long-term outcome in young women with breast cancer: a population-based study. Breast Cancer Res Treat. 2016;160:131–43.
Maggard MA, O’Connell JB, Lane KE, Liu JH, Etzioni DA, Ko CY, et al. Do young breast cancer patients have worse outcomes? J Surg Res. 2003;113:109–13.
Gradishar WJ, Moran MS, Abraham J, Abramson V, Aft R, Agnese D, et al. Breast Cancer, Version 3.2024. J Natl Compr Netw. 2024;22:331–57.
Bray F, Laversanne M, Sung H, Ferlay J, Siegel RL, Soerjomataram I, et al. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2024;74:229–63.
Kim J, Harper A, McCormack V, Sung H, Houssami N, Morgan E, et al. Global patterns and trends in breast cancer incidence and mortality across 185 countries. Nat Med. 2025;31:1154–62.
PDQ® Adult Treatment Editorial Board. PDQ Breast Cancer Treatment. Bethesda, MD: National Cancer Institute. Updated <12/06/2024>. Available at: https://www.cancer.gov/types/breast/hp/breast-treatment-pdq.
Loibl S, André F, Bachelot T, Barrios CH, Bergh J, Burstein HJ, et al. Electronic address: clinicalguidelines@esmo.org. Early breast cancer: ESMO Clinical Practice Guideline for diagnosis, treatment and follow-up. Ann Oncol. 2024;35:159–82.
Paluch-Shimon S, Cardoso F, Partridge AH, Abulkhair O, Azim HA, Bianchi-Micheli G, et al. ESO-ESMO fifth international consensus guidelines for breast cancer in young women (BCY5). Ann Oncol. 2022;33:1097–118.
Virani S, Bilheem S, Chansaard W, Suwanrungruang K, Kamsa-ard S, Khuhaprema T, et al. National and Subnational Population-Based Incidence of Cancer in Thailand: Assessing Cancers with the Highest Burdens. Cancers. 2017;9:108.
Sawka CA, Pritchard KI, Lickley HL, Hazra S, Seltzer MH, Rawlinson E, et al. The Henrietta Banting Breast Centre database: a model for clinical research utilizing a hospital-based inception cohort. J Clin Epidemiol. 1995;48:779–86.
Cybulski C, Kluźniak W, Huzarski T, Byrski T, Gronwald J, Wokolorczyk D, et al. Clinical outcomes in women with breast cancer and a PALB2 mutation: a prospective cohort analysis. Lancet Oncol. 2015;16:638–44.
Sigurdardottir LG, Jonasson JG, Stefansdottir S, Jonsdottir A, Olafsdottir GH, Olafsdottir EJ, et al. Data quality at the Icelandic Cancer Registry: Comparability, validity, timeliness and completeness. Acta Oncol. 2012;51:880–9.
Seyyedsalehi MS, Nahvijou A, Haghjooy Javanmard S, Beiranvand R, Jafari-Koshki T, Hashemi-Besharati M, et al. Clinical Breast Cancer Registry of IR. Iran (CBCR-IR): Study Protocol and First Results. Arch Iran Med. 2023;26:607–17.
Surveillance, Epidemiology, and End Results (SEER) Program (www.seer.cancer.gov) SEER*Stat Database: Incidence - SEER Research Data, 12 Registries, Nov 2022 Sub (1992–2020), National Cancer Institute, DCCPS, Surveillance Research Program, released April 2023, based on the November 2022 submission.
Chung M, Chang HR, Bland KI, Wanebo HJ, De Lellis RA, Huvos A, et al. Younger women with breast carcinoma have a poorer prognosis than older women. Cancer. 1996;77:97–103.
Nixon AJ, Neuberg D, Hayes DF, Gelman R, Connolly JL, Schnitt SJ, et al. Relationship of patient age to pathologic features of the tumor and prognosis for patients with stage I or II breast cancer. J Clin Oncol 12:888-94.
Bharat A, Aft RL, Gao F, Margenthaler JA. Patient and tumor characteristics associated with increased mortality in young women (< or =40 years) with breast cancer. J Surg Oncol. 2009;100:248–51.
Fredholm H, Eaker S, Frisell J, Holmberg L, Fredriksson I, Lindman H. Breast cancer in young women: poor survival despite intensive treatment. PLoS One. 2009;4:e7695.
Narod SA. Breast cancer in young women. Nat Rev Clin Oncol. 2012;9:460–70.
Azim HA Jr, Michiels S, Bedard PL, Singhal SK, Criscitiello C, Ignatiadis M, et al. Elucidating prognosis and biology of breast cancer arising in young women using gene expression profiling. Clin Cancer Res. 2012;18:1341–51.
Sopik V, Sun P, Narod SA. The prognostic effect of estrogen receptor status differs for younger versus older breast cancer patients. Breast Cancer Res Treat. 2017;165:391–402.
Ahn SH, Son BH, Kim SW, Park BW, Kim SI, Lee KS, et al. Poor outcome of hormone receptor-positive breast cancer at very young age is due to tamoxifen resistance: nationwide survival data in Korea-a report from the Korean Breast Cancer Society. J Clin Oncol. 2007;25:2360–8.
Copson E, Eccles B, Maishman T, Gerty S, Stanton L, Cutress RI, et al. Prospective observational study of breast cancer treatment outcomes for UK women aged 18-40 years at diagnosis: the POSH study. J Natl Cancer Inst. 2013;105:978–88.
van der Hage JA, Mieog JS, van de Vijver MJ, van de Velde CJ, Tjan-Heijnen VC, Mansel RE, et al. Efficacy of adjuvant chemotherapy according to hormone receptor status in young patients with breast cancer: a pooled analysis. Breast Cancer Res. 2007;9:R70.
Yu KD, Wu J, Shen ZZ, Shao ZM. Hazard of breast cancer-specific mortality among women with estrogen receptor-positive breast cancer after five years from diagnosis: implication for extended endocrine therapy. J Clin Endocrinol Metab. 2012;97:E2201–9.
Gnerlich JL, Deshpande AD, Jeffe DB, Sweet A, White N, Margenthaler JA. Elevated breast cancer mortality in women younger than age 40 years compared with older women is attributed to poorer survival in early-stage disease. J Am Coll Surg. 2009;208:341–7.
Johansson ALV, Trewin CB, Hjerkind KV, Ellingjord-Dale M, Johannesen TB, Ursin G. Breast cancer-specific survival by clinical subtype after 7 years follow-up of young and elderly women in a nationwide cohort. Int J Cancer. 2019;144:1251–61.
Taylor C, McGale P, Probert J, Kan M, Darby S, Cutter D, et al. Breast cancer mortality in 500 000 women with early invasive breast cancer in England, 1993-2015: population based observational cohort study. BMJ. 2023;381:e074684.
Quinn MJ, Martinez-Garcia C, Berrino F. Variations in survival from breast cancer in Europe by age and country, 1978-1989. EUROCARE Working Group. Eur J Cancer. 1998;34:2204–11.
Richards MA, Wolfe CD, Tilling K, Barton J, Bourne HM, Gregory WM. Variations in the management and survival of women under 50 years with breast cancer in the South East Thames region. Br J Cancer. 1996;73:751–7.
Sant M, Capocaccia R, Coleman MP, Allemani C, Berrino F, Aareleid T, et al. Cancer survival increases in Europe, but international differences remain wide. Eur J Cancer. 2001;37:1659–67.
Copson E, Maishman T, Gerty S, Eccles B, Stanton L, Cutress RI, et al. Ethnicity and outcome of young breast cancer patients in the United Kingdom: the POSH study. B J Cancer. 2014;110:230–41.
Shavers V, Harlan L, Stevens J. Racial/ethnic variation in clinical presentation, treatment and survival among breast cancer patients under age 35. Cancer. 2002;97:134–7.
Abulkhair O, Omair A, Makanjuola D, Al- Idreesi F, Al-Tassan N, Ezzat A, et al. Breast Cancer in Young Women: Is It Different? A Single-Center Retrospective Cohort Study. Clin Med Insights Oncol. 2024;18:11795549241228235 Feb 19.
Liedtke C, Rody A, Gluz O, Baumann K, Nitz U, Koenig K, et al. The prognostic impact of age in different molecular subtypes of breast cancer. Breast Cancer Res Treat. 2015;152:667–73.
Fredholm H, Magnusson K, Lindström LS, Eaker S, Frisell J, Holmberg L. Long-term outcome in young women with breast cancer: a population-based study. Breast Cancer Res Treat. 2016;160:131–43.
Early Breast Cancer Trialists Collaborative Group (EBCTCG). Effects of chemotherapy and hormonal therapy for early breast cancer on recurrence and 15-year survival: an overview of the randomised trials. Lancet. 2005;365:1687–717.
Sparano JA, Gray RJ, Ravdin PM, Makower DF, Pritchard KI, Albain KS, et al. Clinical and genomic risk to guide the use of adjuvant therapy for breast cancer. N Engl J Med. 2019;380:2395–405.
Early Breast Cancer Trialists Collaborative Group DarbyS, McGale P, Correa C, Taylor C, Wang Y, et al. Effect of radiotherapy after breast-conserving surgery on 10-year recurrence and 15-year breast cancer death: meta-analysis of individual patient data for 10,801 women in 17 randomised trials. Lancet. 2011;378:1707–16. Nov 12.
Iqbal J, Ginsburg O, Rochon PA, Sun P, Narod SA. Differences in breast cancer stage at diagnosis and cancer-specific survival by race and ethnicity in the United States. JAMA. 2015;313:165–73. https://doi.org/10.1001/jama.2014.17322.
Lim DW, Giannakeas V, Narod SA. Survival Differences in Chinese Versus White Women With Breast Cancer in the United States: A SEER-Based Analysis. JCO Glob Oncol. 2020;6:1582–92.
Lim DW, Li WW, Giannakeas V, Cil TD, Narod SA. Survival of Filipino women with breast cancer in the United States. Cancer Med. 2023;12:19921–34.
Okuyama A, Barclay M, Chen C, Higashi T. Impact of loss-to-follow-up on cancer survival estimates for small populations: a simulation study using Hospital-Based Cancer Registries in Japan. BMJ Open. 2020;10:e033510.
Thorlacius S, Sigurdsson S, Bjarnadottir H, Olafsdottir G, Jonsson T, Tryggvadottir L, et al. Study of a single BRCA2 mutation with high carrier frequency in a small population. Am J Hum Genet. 1997;60:1079–84.
Szwiec M, Jakubowska A, Górski B, Huzarski T, Byrski T, Cybulski C, et al. Recurrent mutations of BRCA1 and BRCA2 in Poland: an update. Clin Genet 2015;87:288-92.Hershman DL, Shao T, Kushi LH, Buono D, Tsai WY, Fehrenbacher L, et al. Early discontinuation and non-adherence to adjuvant hormonal therapy are associated with increased mortality in women with breast cancer. Breast Cancer Res Treat. 2011;126:529–37.
Chow R, Hasan S, Choi JI, Fox J, Chhabra AM, Marshall DC, et al. Effect of treatment interruptions on overall survival in patients with triple-negative breast cancer. J Natl Cancer Inst. 2023;115:1029–35.
Acknowledgements
The authors thank Eva Maria Gudmundsdottir (Iceland) for valuable data handling and checking.
Funding
V Sopik’s salary for this project was supported by the Ontario Women’s Health Scholarship. Data collection for the study was funded from the Peter Gilgan Centre for Women’s Cancers (S Narod).
Author information
Authors and Affiliations
Contributions
SN and VS conceived and designed the work that led to the submission, played an important role in interpreting the results, drafted and revised the manuscript. P Sun designed the work and drafted the manuscript. JL, JG, TH, CC, LT, KZ, AN, SV, IC, P Sripan, PV, DP, HS, OG, MA, and SN acquired data and revised the manuscript. All authors approved the final version and agreed to be accountable for all aspects of the work.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethics approval and consent to participate
Ethics approval for the release of data was obtained locally at each site. The Ethics Committee at Women’s College Hospital exempted the analysis of the anonymous secondary data from requiring ethics approval (REB # 2017-0076-E). The study was performed in accordance with the Declaration of Helsinki.
Consent for publication
No identifying data is included in this manuscript.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Sopik, V., Lubiński, J., Gronwald, J. et al. An international cohort study of breast cancer survival in young women. BJC Rep 4, 6 (2026). https://doi.org/10.1038/s44276-026-00207-z
Received:
Revised:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s44276-026-00207-z
