
Abstract
Dementia is rising sharply in the Middle East and North Africa region (MENA), with cases projected to increase by 367% by 2050. Despite this, research remains fragmented, with limited large-scale studies and methodological inconsistencies. This review synthesizes current knowledge on dementia prevalence, risk factors, and healthcare challenges in MENA, highlighting key issues such as modifiable risk factors, healthcare fragmentation, workforce shortages, and the economic burden of informal caregiving. It also examines the impact of conflict, political instability, and climate change on dementia care. Addressing these gaps requires large-scale epidemiological studies, policy reforms, investment in healthcare infrastructure, and culturally adapted interventions. Strengthening research and healthcare systems is crucial to mitigating the region’s growing dementia crisis.
Similar content being viewed by others

Introduction
Dementia has emerged as one of the most pressing global health challenges of the 21st century, driven by demographic shifts, particularly the aging of populations worldwide. According to the World Health Organization1, over 55 million people currently live with dementia globally, a number projected to nearly triple to 139 million by 2050. This surge will place strain on healthcare systems, economies, and caregivers, particularly in low- and middle-income countries (LMICs), where healthcare infrastructure is often ill-equipped to manage the complex needs of individuals with dementia. Epidemiological trends indicate that the rise in dementia prevalence is closely linked to increasing life expectancy and aging populations, with LMICs expected to bear the brunt of this burden due to rapid demographic transitions and limited resources.
The Middle East and North Africa (MENA) region, a geographically and culturally diverse area spanning North Africa and Western Asia, is of particular concern. For the purposes of this review, the MENA region is defined according to the UNICEF MENA classification2, encompassing 19 countries: Algeria, Bahrain, Egypt, Iran, Iraq, Jordan, Kuwait, Lebanon, Libya, Morocco, Oman, Palestine, Qatar, Saudi Arabia, Sudan, Syria, Tunisia, the United Arab Emirates (UAE), and Yemen. While there is no universally agreed-upon list of MENA countries, countries like Djibouti and Israel that are listed as part of the MENA region by the World Bank3 have distinct linguistic, cultural, and political characteristics that differ from the list set by UNICEF. The classification by UNICEF focuses on Arabic-speaking countries with stronger cultural, linguistic, and socioeconomic ties, making it more suitable for examining dementia prevalence, risk factors, and healthcare challenges across diverse socioeconomic and political contexts.
The MENA region is undergoing significant demographic changes, with its population of older adults growing rapidly. Of the region’s 546 million inhabitants, approximately 29 million (5.3%) are aged 55 and older, while 352 million (64.5%) fall within the working-age bracket of 15–64 years4. According to the National Institute of Aging5, older adults are defined as those aged 65 and above. Although the proportion of older adults (estimated at 3–18%, Table 1 and Fig. 1) is currently lower than in many other regions6, the MENA region is projected to experience one of the fastest increases in dementia cases worldwide. By 2050, dementia prevalence in MENA is expected to rise by 367%, the highest projected increase globally7. This alarming trend is driven by rapid urbanization, improved life expectancy, and the aging of large birth cohorts, coupled with the region’s unique sociocultural and economic dynamics.

Despite these projections, the MENA region remains severely underrepresented in global dementia research. Compared to high-income countries, MENA has limited epidemiological data, low publication output, and a lack of robust studies on dementia prevalence, risk factors, and care systems8. This dearth of research has created significant knowledge gaps, hindering the development of effective public health interventions and culturally sensitive care strategies. The region’s unique combination of rapid urbanization, diverse socioeconomic landscapes, and political instability further complicates efforts to address dementia, as these factors influence healthcare accessibility, disease prevalence, and public health priorities9.
The MENA region is characterized by profound sociocultural, socioeconomic, and political diversity, as well as disparities in healthcare access and infrastructure. These complexities necessitate tailored approaches to understanding and addressing dementia, as global models of care and prevention may not be directly applicable. For instance, the region’s reliance on family-based caregiving, deeply rooted in cultural and religious norms, contrasts with the institutional care models prevalent in high-income countries10. Similarly, the lack of standardized diagnostic tools and culturally adapted cognitive assessments further complicates efforts to accurately measure dementia prevalence and progression.
The purpose of this review is to synthesize available epidemiological data on dementia in the MENA region, highlighting trends, gaps, and limitations in current research. By examining prevalence estimates, age-specific incidence rates, and identified risk factors, this review aims to provide a comprehensive overview of the dementia burden in MENA, contextualized within global trends. Furthermore, this review underscores the urgent need for region-specific, large-scale epidemiological studies to inform effective prevention, screening, and management strategies. Ultimately, the goal is to support the development of culturally sensitive public health policies and healthcare approaches that address the unique challenges of dementia in the MENA region, with a particular focus on underserved populations and at-risk groups across diverse socioeconomic backgrounds.
Methodology and Scope
This literature review employed a structured search strategy to synthesize current evidence on dementia in the MENA region. The search was conducted across multiple databases, including Embase, Embase Classic, PubMed, Scopus, Google Scholar, and MEDLINE. We also consulted select gray literature and preprints from reputable health organizations. Searches were conducted using a detailed query combining terms related to dementia (e.g., “dementia,” “Alzheimer’s disease,” “cognitive decline”) with regional identifiers, including country names and broader geographic terms (e.g., “Middle East,” “North Africa,” “Fertile Crescent”).
The search strategy incorporated Boolean logic and database-specific indexing, such as the following representative example from Embase: (‘dementia’/exp OR ‘amentia’ OR ‘dementia’ OR ‘alzheimer disease’/exp OR ‘alzheimer dementia’ OR ‘alzheimer neurofibrillary degeneration’) AND (‘iraq’/exp OR ‘egypt’:ti,ab,kw OR ‘middle east’/exp OR ‘north africa’:ti,ab,kw). The full query encompassed a wide range of synonyms and variants for dementia and Alzheimer’s disease, as well as all countries typically included in MENA-focused studies.
The review was limited to studies published in English between 2014 and 2024 to ensure linguistic consistency and the inclusion of contemporary research. Only peer-reviewed journal articles and high-quality gray literature were included. Articles focusing on prevalence, risk factors, health systems, care infrastructure, and policy frameworks related to dementia in the region were prioritized.
The MENA region was defined in accordance with the UNICEF MENA classification2, encompassing 19 countries: Algeria, Bahrain, Egypt, Iran, Iraq, Jordan, Kuwait, Lebanon, Libya, Morocco, Oman, Palestine, Qatar, Saudi Arabia, Sudan, Syria, Tunisia, the UAE, and Yemen.
Dementia in the MENA region
Incidence and prevalence
Dementia prevalence in the region varies significantly across age groups, ranging from 1.1% to 2.3% among individuals aged 50 years and older and from 13.5% to 18.5% among those aged 80 and above11. Notably, the prevalence of Alzheimer’s disease (AD) in the region increased by 3.0% (95% UI: 1.5–4.6) between 1990 and 201912,13. According to the Global Burden of Disease Study13, the MENA region exhibited the highest age-standardized disability-adjusted life years (DALY) rates globally, with 387 (95% UI: 172.0–848.5) DALYs per 100,000 population attributable to dementia. Among individuals aged 75 to 79 years, the non-standardized DALY rate reached 3,325.9, reflecting a 177.3% (95% UI: 161.1–215.8) increase from 1990 to 201913,14. These trends underscore the growing public health burden of dementia in the region and highlight the urgent need for targeted interventions.
The economic impact of dementia in the MENA region is substantial, with total direct and indirect costs averaging 12 billion annually across 19 countries. Egypt (1 billion), Saudi Arabia (4.9 billion), and the UAE (4.9 billion), bear the highest financial burdens11. Direct care costs are closely tied to GDP per capita and income classification, with high-income countries such as Saudi Arabia (2039 per capita) and the UAE (2371 per capita) incurring significantly higher expenses compared to lower-middle-income countries like Yemen (223 per capita)11. Regional spending on dementia care and treatment reached 2.1 billion in 2019, marking an 8.2% increase from 2000—a rate that exceeds the global increase of 4.5%. By 2050, these costs are projected to escalate to ~$57.9 billion12, emphasizing the escalating financial strain of dementia care in the MENA region.
Despite these findings, significant gaps remain in understanding the epidemiological disparities in dementia prevalence and DALYs across MENA countries. For instance, Safiri et al. 12 reported a higher prevalence of dementia among women compared to men, potentially linked to factors such as lower education levels, longer life expectancy, and biological differences. However, the underlying mechanisms remain poorly understood. Furthermore, substantial heterogeneity in dementia prevalence and DALYs exists across the region (Table 2, Fig. 2), likely driven by variations in risk factors, aging demographics, genetic predispositions, and disparities in healthcare access12.

Prevalence of most common environmental factors and non-communicable diseases (NCDs) in the Middle East North Africa (MENA) region (hypertension, tobacco use, overweight, insufficient physical activity).
Demographics and socioeconomic drivers
The MENA region has undergone significant demographic and socioeconomic transformations over the past century, characterized by increased life expectancy and reduced infant mortality rates15. While countries such as Syria, Iraq, Palestine, Jordan, and Yemen continue to experience rapid population growth, others like Lebanon, Tunisia, Libya, and Algeria are witnessing aging population trends. These demographic shifts are expected to drive a rise in dementia incidence, as evidenced by Iran, where dementia prevalence increased between 2010 and 201916. Gulf countries, including Bahrain, Kuwait, Oman, Qatar, Saudi Arabia, and the UAE, face unique challenges due to high levels of migration. For example, expatriates constitute nearly 70% of Kuwait’s population17, complicating healthcare planning and resource allocation.
Non-communicable diseases and dementia
Non-communicable diseases (NCDs), such as cardiovascular diseases, diabetes, and cancer, account for ~75% of global deaths18. In the MENA region, the burden of NCDs is particularly pronounced. For example, in Egypt, NCDs contribute to 82% of mortality, driven by cardiovascular diseases, diabetes, cancer, and chronic respiratory illnesses18,19. Similarly, in Jordan, NCDs are responsible for 78% of deaths, primarily due to cardiovascular diseases, diabetes, and cancer20.
The Lancet Commission21 identified 14 modifiable risk factors for dementia, many of which are directly linked to NCDs, including hypertension, diabetes, smoking, alcohol consumption, obesity, physical inactivity and others. As NCD prevalence continues to rise in the MENA region, so does the risk of dementia, underscoring the urgent need for integrated public health strategies. Preventive measures such as cardiovascular health management, lifestyle modifications, and metabolic disease control are essential to mitigating dementia risk. Given the significant overlap between NCDs and cognitive decline, dementia prevention must be incorporated into broader NCD prevention frameworks, ensuring a multidisciplinary approach to reduce disease burden and improve long-term health outcomes.
Hypertension
Despite a decline in DALYs and mortality attributable to high systolic blood pressure between 1990 and 201722, hypertension remains a significant public health challenge in the MENA region, with a prevalence of 24.36% (95% CI: 19.06–31.14)23. Dyslipidemia, another critical cardiovascular risk factor, affected 54.08% (95% CI: 43.83–66.71) of the population, with low-income countries bearing a disproportionately higher burden compared to higher-income nations22,24. Additionally, prehypertension—a precursor to hypertension—affects 40% to 66% of the population, with higher rates observed among men22. Studies from Egypt and Saudi Arabia reveal high rates of undiagnosed and poorly controlled hypertension, although countries like Iran have made progress in improving awareness and treatment22. Hypertension and diabetes have been strongly associated with dementia in studies conducted in Algeria25 and Lebanon26,27. However, research on dyslipidemia remains limited, with most studies originating from Iran, Egypt, Iraq, Lebanon, and Kuwait22.
Physical activity and obesity
Physical inactivity is a significant contributor to dementia, accounting for 12.25% of cases in LMICs28. The MENA region has one of the lowest levels of physical activity globally, with 49.2% of adults and 74.4% of youth classified as physically inactive29. A 1% increase in physical inactivity is associated with 8714 new dementia cases annually in LMICs28. Compounding this issue, the region is grappling with an obesity crisis, with prevalence rates ranging from 18.9% to 40%30. Kuwait ranks among the top 10 most obese nations globally, with similarly high rates observed in Oman and Saudi Arabia, while Yemen reports the lowest prevalence22. Childhood obesity is particularly alarming, with rates reaching 49.4% in Kuwait, followed by Qatar and Jordan. This trend is often linked to higher parental education and socioeconomic status (SES)31,32. In a longitudinal analysis of Global Burden of Disease data from 145 countries, Lloyd-Hazlegreaves et al. 33 found a positive association between dementia prevalence and physical inactivity (coefficient= 2.52 [95% CI: 1.07, 3.96], p = 0.0007), with stronger association in males in higher-income countries. This suggests that wealthier Gulf countries with high obesity and physical inactivity rates may be at a higher risk for dementia and would require different regional public health strategies than lower-middle income MENA countries.
Smoking
Smoking remains a major public health concern in the MENA region, with significant variations in prevalence across countries. Between 1990 and 2019, Egypt experienced an increase of 1.24 million (95% UI: 0.864–1.59) male smokers aged 15–24, while Jordan saw a rise of 116,000 (95% UI: 66.2–174) female smokers34. A large cross-sectional study across nine MENA countries (including Pakistan and Turkey) reported the lowest smoking rates in Morocco (15.3%; 95% CI: 14.2–16.4%) and the highest in Lebanon (53.9%; 95% CI: 51.3–54.6%) among individuals aged 40 and above35. Smoking is more prevalent among men than women, particularly in Jordan, Lebanon, and Syria, where over 50% of male participants and more than 10% of women were smokers35.
Smoking is a well-established risk factor for dementia21,36, with an estimated 17.41% to 19.6% of the adult population in the region being smokers37,38. In a systematic review by El-Metwally et al.39, dementia risk and incidence increased in smokers. The highest smoking prevalence rates are recorded in Iraq (32%; 95% CI: 20.20–50.69) and Jordan (24.8%; 95% CI: 20.30–30.31)37. Countries with higher GDP and educational attainment generally exhibit lower smoking-related deaths and DALY rates, with the exception of Lebanon, where smoking-related health risks remain elevated38. Additionally, second-hand smoke exposure is widespread among adolescents in Gulf countries, including Bahrain, Kuwait, Oman, Qatar, Saudi Arabia, and the UAE, with rates ranging from 12.7% to 65.9%40. However, research on smoking as a risk factor for dementia in MENA remains limited. This highlights the urgent need for targeted tobacco control policies and public health interventions across the region.
Table 2 summarizes the prevalence rates of physical inactivity, smoking, obesity, and hypertension, per country. These health challenges point to a broader public health crisis in the region, characterized by a complex interplay of lifestyle factors, socioeconomic determinants, and insufficient health interventions.
Diabetes
Diabetes is a major public health concern in the MENA region, with an adult prevalence rate of 14.6%. Kuwait, Saudi Arabia, and the UAE report the highest prevalence rates, with Saudi Arabia leading at 21.9% to 23.9%41,42. Egypt has the largest absolute number of diabetes patients in the region, while Gulf countries such as the UAE, Kuwait, Qatar, and Bahrain allocate substantial healthcare resources to diabetes management41,43. Urban populations generally exhibit higher diabetes prevalence compared to rural areas, except in Iran, where socioeconomic factors and lifestyle changes associated with urbanization have led to divergent patterns42,44.
Diabetes is a significant risk factor for AD. A hospital-based study in Saudi Arabia identified diabetes as the most common comorbidity among dementia patients (19.1%), followed by hypertension (16.4%)45. Genetic predispositions also play a role, with genome-wide association studies (GWAS) identifying risk-related single nucleotide polymorphisms in genes such as TCF7L2 (in nine countries) and CDKAL1 (in four countries)44. Additional contributing factors include nutritional transitions, physical inactivity, obesity, and rapid economic development, which have disproportionately affected Gulf countries compared to other LMICs in the region42.
Climate change and air pollution
The MENA region is highly vulnerable to climate change, with older adults facing increased heat-related risks due to declining health and mobility46,47. While natural factors such as windblown dust contribute to air pollution, over 90% of pollution stems from anthropogenic sources, including industrial emissions, urbanization, and traffic48,49. In Egypt, traffic and waste burning are primary contributors, while in Kuwait and Saudi Arabia, industrial oil activities are the main sources of pollution49.
Conflict-related environmental destruction, such as in Gaza, further exacerbates health risks50. The Persian Gulf region (Iran, Oman, UAE, Saudi Arabia, Qatar, Bahrain, Kuwait, and Iraq) consistently records air pollution levels exceeding EU standards51. Long-term exposure to air pollution resulted in an estimated 152,925 deaths in 2012, with Egypt accounting for nearly half49.
Economic growth correlates with rising emissions, with 92–94% of the MENA population exposed to unsafe levels of PM 2.552. Lower socioeconomic communities are disproportionately affected due to disparities in healthcare access and occupational hazards52,53. For example, in Dubai city in UAE, economic expansion and urbanization between 2013 and 2019 initially led to increased air pollution, followed by reductions due to policy interventions—though levels remain above EU standards54. Further research is needed to explore the direct effects of air pollution on dementia prevalence in the region.
Alcohol consumption
Alcohol consumption in the MENA region is relatively low, with an average prevalence of 6.2% (9.5% in males, 2.0% in females), significantly below the global average of 43%55. In 2019, 0.6% (0.5 to 0.8) of all DALYs in the region were attributable to alcohol consumption56 with a low age-standardized prevalence of 593 (CI: 507.9– 683.0) per 100,00057. This low prevalence is largely due to religious and cultural norms, as Islamic laws prohibit alcohol consumption in many MENA countries, leading to strict legal measures and high taxation58. Countries such as Libya, Saudi Arabia, Sudan, and Yemen enforce outright bans on alcohol consumption and distribution, reinforcing societal deterrents59.
However, alcohol bans do not entirely eliminate alcohol-related problems. Some studies indicate an increase in alcohol use in recent years, with Rostam-Abadi et al.55 reporting a doubling of prevalence rates between 2016 and 2023. Similarly, Libya and Iran experienced an increase in alcohol-related DALYs from 1990 to 201956. The lack of comprehensive data on alcohol-related health effects complicates research and policy formulation, as many healthcare professionals avoid discussing alcohol consumption due to religious sensitivities59.
Data availability varies significantly across the region. While countries such as Lebanon, Kuwait, Morocco, Oman, and Saudi Arabia provide limited alcohol consumption data, others like Yemen and Libya enforce alcohol bans but lack published statistics. Additionally, Qatar, Syria, Bahrain, and Algeria, despite having no formal alcohol bans, also exhibit limited data availability55,58. The limited research funding and social stigma surrounding alcohol use hinder efforts to understand its health impacts and develop targeted interventions in the region.
Depression and mental health
Depression is a significant public health concern in the MENA region, with 20.2 million prevalent cases and 29.9 million incident cases recorded in 201960. The overall prevalence and DALYs due to depression in the region exceed global averages, with a prevalence rate of 4348.89 (95% UI: 3807.29–4971.11) per 100,000 compared to the global rate of 3440.05 (95% UI: 95% UI, 3097.01–3817.64), and DALYs of 781.06 (95% UI: 535.18–1075.62) per 100,000 compared to the global rate of 577.75 (95% UI, 405.79–788.88)61. The highest depression prevalence rates in 2019 were reported in Palestine (6296.83 [95% UI: 5462.38–7216.09] per 100,000), Bahrain (5038.74 [(95% UI: 4386.9–5753.18] per 100,000), and Tunisia (5049.41 [95% UI, 4363.94–5811.47] per 100,000)61. A systematic review indicated that 64.6% of older adults in Egypt suffered from depression, with rates increasing to 67% among hospitalized patients62.
Depression is both a risk factor for and a comorbid condition of dementia. Studies in Iran have linked depression to an increased risk of cognitive impairment and AD63. In Egypt, a study of neurological and psychiatric clinics found that 32.5% of AD patients and 72.22% of those with other dementias exhibited depressive symptoms, with female patients experiencing more prolonged depressive episodes64. Additionally, a study in Qatar reported that 52% of home-based dementia patients experienced depression65.
Various sociodemographic factors influence depression prevalence. In Jordan, dementia risk factors included older age, male sex, a family history of dementia, and illiteracy66. In Egypt, depression was associated with low income, unemployment, female sex, and chronic illnesses62. In Bahrain, marital status was linked to cognitive impairment among hospitalized patients67. Social isolation and lack of support were also significant contributors to depression among older adults in Egypt62. Addressing mental health disparities through targeted interventions could help mitigate the burden of depression and its impact on dementia risk in the region.
There is an intricate web of interdependencies and interactions among the different risk factors for dementia that often influence one another in bidirectional or multidirectional ways (Fig. 3). This highlights the need for holistic, multidisciplinary approaches to understand and mitigate these risks effectively in the MENA region.
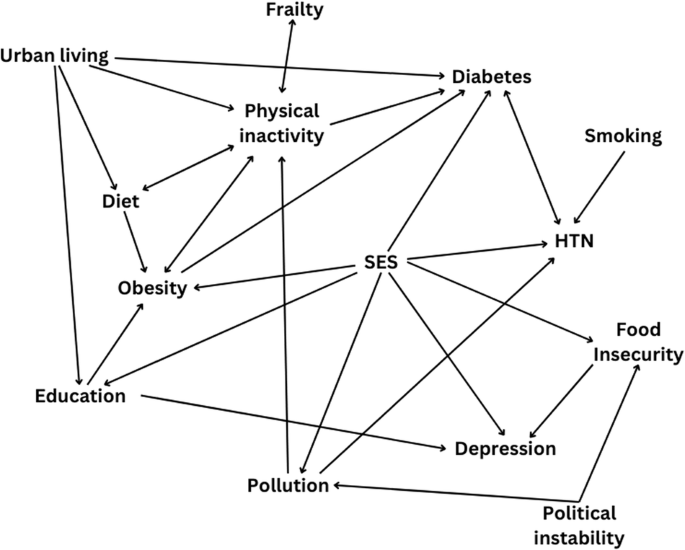
HTN hypertension, SES socioeconomic status.
Challenges
Socioeconomic and environmental factors
Education
Illiteracy rates in the MENA region remain among the highest globally, with approximately 25% of males and 46% of females classified as illiterate68. Reducing illiteracy has significant economic benefits, potentially saving billions of dollars in healthcare and productivity losses69. Illiteracy is more prevalent in rural areas compared to urban centers70, and research indicates a higher prevalence of dementia among illiterate individuals in countries such as Egypt70,71,72, Jordan66, and Oman73. In Lebanon, the number of years spent in education was negatively correlated with the risk of mild cognitive impairment74.
While education itself may not directly prevent dementia, it follows the concept of cognitive reserve and interacts with other protective factors, such as SES, occupation, and lifestyle, as highlighted by Sharp and Gatz’s75 model. Women in the MENA region have historically had less access to education than men. For example, a survey by the Egyptian Labor Market Panel found that only 25% of adults had attained education beyond the primary level, with just 18% of these being women10. However, this gender gap is narrowing among younger generations, reflecting improvements in educational access and literacy rates. Addressing education disparities and promoting lifelong learning opportunities may serve as protective factors against cognitive decline, underscoring the need for region-specific interventions aimed at reducing dementia risk through education policies.
Caregiving, living arrangements and socioeconomic disparities
Socioeconomic disparities play a critical role in shaping dementia prevalence across the MENA region. Factors such as low SES, advanced age, widowhood, and living alone have been consistently associated with increased dementia risk. In Algeria, individuals over the age of 80, widows, those with lower SES, and those with a family history of dementia exhibited a higher likelihood of developing cognitive impairment25. Similarly, low SES was a strong predictor of dementia in Egypt and Jordan, where nursing home residents from higher SES backgrounds demonstrated better cognitive function, as measured by the Montreal Cognitive Assessment (MoCA)76,77,78. Other factors, including marital status (single or widowed), presence of comorbidities, and family history of dementia, have been linked to cognitive decline77.
Caregiving for individuals with dementia in the MENA region is predominantly informal, with family members assuming primary responsibility for their care due to deeply rooted cultural and religious values. The principle of birr al walidein—a core tenet of Islam—emphasizes respect, kindness, and the moral duty of caring for one’s aging parents, shaping family structures and reinforcing home-based caregiving norms10,79,80. Institutionalization of older adults is highly stigmatized and often perceived as neglecting familial obligations, contributing to a strong preference for home care80,81. This preference is evident in Qatar, where healthcare professionals expressed opposition to placing dementia patients in nursing homes, advocating for family-based care instead82.
Despite cultural preferences for family caregiving, older adults in institutional settings tend to exhibit higher rates of cognitive impairment. In Iraq, the prevalence of mental disorders was significantly higher among nursing home residents (55.8%) compared to those living at home (21.5%)83. A similar trend was observed in Iran, where dementia rates among hospitalized patients (22%) in Tehran exceeded community estimates84. In Jordan, 87.4% of older adults residing in nursing homes exhibited mild cognitive impairment (MCI)78, further underscoring the association between institutionalization and cognitive decline.
However, the reliance on family members for dementia care imposes substantial emotional, psychological, and financial burdens. In Egypt, 30% of family caregivers reported moderate to severe burden, 43% experienced anxiety, and 30% reported poor quality of life due to caregiving responsibilities85,86. Similarly, in Oman, 70% of caregivers demonstrated a high level of burden87. Among Syrian refugees in Jordan, fear of dementia was linked to concerns over the strain it would place on already struggling families88. The economic costs of informal caregiving in the Arab world range between $2.2 billion and $5.7 billion, with Saudi Arabia accounting for the highest share at $853 million11. High unemployment rates and economic instability further strain families who must balance caregiving duties with financial obligations89.
Women bear the greatest caregiving burden across the region. In Oman, 54% of dementia caregivers were women87, while in Egypt, 73.5% of caregivers were female86. In Qatar, female caregivers prioritized education, post-diagnosis services, and non-pharmacological symptom management more than their male counterparts90. While caregiving can be emotionally and physically demanding, surveys in Qatar indicate that many caregivers express gratitude for the role, viewing it as a fulfilling duty rather than a burden91. This suggests that reducing caregiver strain does not necessarily require greater institutionalization but rather policies that offer education, emotional and social support, and financial assistance to caregivers within the existing family-oriented care model80.
However, the traditional caregiving model in the MENA region is facing growing challenges due to urbanization, demographic shifts, and socioeconomic changes. The breakdown of extended family structure—historically relied upon for informal caregiving—is reducing available caregiving resources91. In Egypt, older adults are increasingly living alone or with their spouses, with more women than men adopting these living arrangements10. The transition from extended to nuclear family structures has resulted in fewer available caregivers, intensifying the strain on those who remain.
Several additional factors are complicating traditional caregiving models. Increased life expectancy, rising costs of living, and the growing participation of women in tertiary education and the workforce are reshaping family dynamics and reducing the availability of full-time caregivers10,81. As women enter the workforce in greater numbers, they can contribute financially at the same level as men but often at the cost of hands-on caregiving responsibilities10. These evolving economic and social realities necessitate adapted caregiving policies that balance cultural expectations with practical solutions, such as home-based support programs, caregiver training, and flexible employment policies that accommodate caregiving responsibilities.
Environmental and lifestyle factors
Environmental and lifestyle-related determinants further exacerbate dementia risk in the MENA region. Urbanization, air pollution, extreme climate conditions, and cultural norms can create barriers to physical activity, reducing opportunities for engagement in health-promoting behaviors29. Occupational exposure has also emerged as a risk factor, with studies showing that Iranian oil industry workers with over 20 years of service face a heightened risk of dementia92. However, employment or retirement appears to have a protective effect, as unemployment has been linked to a higher prevalence of cognitive decline84.
Dietary patterns and nutritional challenges
Nutritional habits significantly influence dementia risk. The Mediterranean diet, rich in olive oil, fresh produce, and whole grains, has been associated with a lower incidence of dementia, with supporting evidence from Iran and Morocco93,94. However, Western dietary transitions, marked by increased consumption of processed foods, refined sugars, and red meat, are escalating metabolic risks and contributing to cognitive decline across the region95,96. Food insecurity remains a growing concern, particularly in crisis-affected countries such as Lebanon, where economic collapse post-2020 led to widespread malnutrition, and Egypt, where rural populations experience disproportionate food shortages97,98.
Frailty and cognitive decline
Frailty, a condition of age-related physiological decline, is a critical but under-researched risk factor for dementia in the MENA region. While studies linking frailty to cognitive impairment are relatively well-documented in Saudi Arabia, Egypt, and Lebanon, data from other Middle Eastern countries remains scarce99. Frailty not only increases vulnerability to dementia but also contributes to higher rates of disability, falls, and hospitalization, making it an essential target for preventive interventions100.
Addressing socioeconomic, environmental, and nutritional risk factors is vital for reducing dementia prevalence in the region. Future public health strategies should focus on targeted interventions for low-SES populations, policies to improve food security, and greater investment in aging-related research to mitigate the impact of these risk factors on cognitive health.
Lack of public awareness
A major challenge in the MENA region is the widespread perception that dementia and cognitive impairment are natural aspects of aging rather than medical conditions39,79,82,101,102. Public awareness remains limited, leading to stigmatization, misperceptions, and delays in diagnosis and treatment. In Saudi Arabia, individuals with dementia are often viewed as incapable or childlike, reinforcing negative societal attitudes103. Cultural beliefs also play a crucial role in dementia perceptions, with families often seeking treatment from traditional healers rather than medical professionals, further delaying appropriate care82,104. Stigma surrounding dementia can discourage families from seeking formal healthcare services due to fear of social judgment91,103, leading to underreporting of cases, especially in rural and low-income areas with limited healthcare access9.
The lack of access to healthcare services exacerbates the issue. In Egypt, ~78 million people are underserved, with significant healthcare disparities between Cairo and Upper Egypt105,106. Similarly, in Lebanon, only 40% of dementia patients had health insurance, making access to care difficult26. Additionally, families often prioritize physical health issues over cognitive symptoms, resulting in missed diagnoses and exclusion from research studies107. In Egypt, families frequently conceal dementia cases due to lack of awareness and fear of stigma, a trend observed in other mental disorders as well107. Public awareness of modifiable dementia risk factors remains limited. In Makkah, Saudi Arabia, patients and caregivers were unaware of malnutrition symptoms, despite their impact on cognitive health108. In another Saudi Arabian study, while most participants knew AD was linked to depression, only 43.2% were aware of high cholesterol and lifestyle factors as risk factors109. Awareness was highest regarding assessment, treatment, and caregiving, but only 53.25% recognized AD symptoms, and 50.6% were unaware of the role of lifestyle factors101,102. Similar gaps were identified in Egypt and Saudi Arabia, where higher income and education levels correlated with greater dementia knowledge, while rural residents had lower awareness101,110,111. In Palestine, urban medical students had better dementia knowledge than their rural counterparts, with stronger understanding of prevention but weaker knowledge of treatment112.
A survey of Qatari health professionals found that women had higher awareness of dementia risk factors (e.g., hypertension, smoking, depression, and hearing impairment), but common barriers to treatment included lack of understanding (76.5%), time constraints (54%), and low motivation (60.8%)113. These findings indicate that knowledge gaps vary across the region, requiring tailored awareness campaigns to effectively address misconceptions and promote preventive strategies.
Research gaps and methodological limitations
Lack of large-scale, population-based studies
Despite increasing neuroscience research in the MENA region, particularly in Egypt, Tunisia, and Morocco114, large-scale, population-based dementia studies remain scarce. Between 2005 and 2019, only 0.774% of global publications on neurodegenerative diseases originated from Arab countries8. Studies on AD mostly came out of Saudi Arabia (n = 130) and Egypt (n = 103), but most MENA countries produced little (Tunisia = 35) to no studies (Bahrain and Palestine = 0)8. Many existing studies rely on small, non-representative samples, limiting the generalizability of findings. A report by World Alzheimer International115 found that few dementia studies in MENA had sample sizes exceeding 1500 participants, emphasizing the need for more robust epidemiological efforts. Similarly, El-Metwally et al.39 reviewed 18 dementia studies and found that only five had sample sizes above 1500, with just 50% employing rigorous sampling methods. The limited output, small and non-representative sample size, and lack of large-scale studies significantly impacts the reliability of prevalence estimates and hampers the ability of policymakers and healthcare providers to make informed decisions and target interventions.
Some MENA countries have made strides in utilizing national health datasets to estimate prevalence. In Iran, researchers have leveraged Institute for Health Measurement and Evaluation (IHME) data to estimate dementia rates across all districts16. However, most MENA countries lack similar efforts, and many prevalence estimates are derived from door-to-door surveys or patient recruitment at healthcare facilities in limited districts (Table 3). For instance, Egypt’s available dementia data stems from localized studies in Al-Qusair72, Al-Kharga70,116, Upper Egypt desert117, Assiut and Qena118,119, Zagazig76, Cairo120, and Kafr El Sheikh77. Similarly, a systematic review in Iran highlighted regional disparities in dementia prevalence, with estimates ranging from 0.06% to 0.14% across different provinces, largely due to methodological inconsistencies121.
Challenges in sampling and study design
Many dementia studies in MENA rely on hospital-based sampling rather than community-based recruitment, which can introduce selection bias and overestimate prevalence rates45,63,73,122,123. Future research should prioritize community-based epidemiological studies to ensure more representative population estimates. However, resource constraints, poor prioritization of dementia research, and low public awareness of longitudinal studies hinder such efforts.
Additionally, cross-sectional study designs dominate MENA dementia research, limiting the ability to infer causal relationships between modifiable risk factors and dementia onset. Prospective cohort studies are urgently needed to understand long-term dementia risk factors. Most studies on aging populations in the Middle East have been cross-sectional and have focused on related conditions such as depression, malnutrition, and physical disability, with the majority coming from Egypt, Saudi Arabia, and Lebanon99. The lack of longitudinal data makes it difficult to track dementia incidence and progression over time.
High participant dropout rates further challenge longitudinal studies, often driven by urban migration, socioeconomic instability, and loss to follow-up. Despite these challenges, Egypt and Lebanon have taken steps toward addressing this gap, with the launch of the Egyptian Longitudinal Study for Healthy Aging (AL-SEHA)124 and the conclusion of L’SEHA aging study in Lebanon125. Additionally, Iran established the Iranian Alzheimer’s Disease Registry in 2018 to determine prevalence and risk factors in Tehran126.
Gender disparities in dementia research
A critical gap in MENA dementia research is the underrepresentation of gender-specific data, despite well-documented differences in dementia risk, progression, and healthcare access. Most studies fail to explore gender-based disparities, leading to generalized interventions that may not effectively address the unique needs of men and women.
Findings from memory clinics in Qatar underscore significant gender disparities in dementia risk factors. Women enrolled in these clinics were more likely to have lower education levels, higher obesity rates, and greater physical inactivity compared to men. They also reported a higher prevalence of delirium and post-delirium conditions and were more frequently prescribed medications127.
Gender inequalities in healthcare access and service utilization further hinder early screening, diagnosis, and treatment for dementia and other NCDs in the region128. Women in MENA often face barriers to healthcare access, including financial constraints, caregiving responsibilities, and cultural expectations that discourage seeking medical attention. Additionally, many women serve as primary caregivers for family members with dementia, increasing their own risk of stress-related health issues while reducing focus on their cognitive and physical health.
To bridge this gap, future research should integrate gender-sensitive approaches, examining how sociocultural norms impact healthcare-seeking behaviors. A gender-informed approach to dementia research and healthcare can enhance diagnostic accuracy, improve management strategies, and promote equitable access to care.
Healthcare Professionals’ awareness and training gaps
Dementia awareness among healthcare professionals in the MENA region remains insufficient, hindering early diagnosis and intervention efforts. A survey in Qatar found that over 70% of healthcare providers had not received specialized training in neurodegenerative diseases within the past two years, and only 26.7% managed dementia patients annually82. Similarly, in Kuwait, healthcare workers in general hospitals demonstrated significantly lower dementia knowledge than those in specialty hospitals129. Notably, experience levels did not necessarily correlate with dementia knowledge, as even Qatari professionals with over 10 years of experience showed limited understanding of risk factors and prevention strategies113.
A major barrier is the lack of specialized dementia training programs in medical education and continuing professional development. In Kuwait, only 10% of healthcare providers had attended dementia-related conferences or training, and their average knowledge score was just 18.99 out of 50129. Among medical students in Kuwait and Palestine, dementia knowledge was moderate (63–64%), with the least understood domain being risk factors112,130. Given their future role in dementia diagnosis and management, these gaps in medical education raise concerns about MENA’s preparedness for the rising dementia burden.
A lack of specialized faculty, courses, research opportunities, and structured training programs in geriatric medicine and dementia care further limits professional capacity80. Despite the rising dementia burden, most MENA countries lack comprehensive national dementia policies. An exception is Kuwait’s Ministry of Health, which launched a three-year frailty research program to examine cognitive decline in older adults99. However, large-scale, coordinated dementia strategies remain absent across most of the region.
Diagnostic challenges
Diagnostic practices for dementia vary widely across the MENA region, leading to inconsistencies in prevalence estimates and limiting the comparability of data. The absence of standardized diagnostic criteria contributes to both underdiagnosis and misdiagnosis, particularly in areas with limited access to neuropsychological testing. A systematic review of neuropsychological assessments used in the MENA region found that 55% of the tools were either misapplied or inadequately adapted131. The three most commonly used tests—the Trail Making Test (TMT), the Wechsler Memory Scale, and the Wisconsin Card Sorting Test—were frequently employed without appropriate cultural or linguistic modifications. Of the 117 neuropsychological measures utilized in the region, only 53 had been formally adapted and validated.
While Tunisia and Lebanon have developed strong adaptations of the Mini-Mental State Examination (MMSE), the majority of adapted assessments fail to meet the guidelines established by the International Test Commission and the American Educational Research Association131. Key issues include the use of non-standardized or poorly adapted measures, a lack of clarity regarding test versions, failure to cite relevant validation studies, and inadequate documentation of test administration protocols. These shortcomings limit the reliability of cognitive assessments and create challenges in diagnosing dementia accurately across different populations.
Cultural and social factors further complicate dementia assessments in the MENA region. Many existing studies fail to account for variations in lifestyle, dietary habits, literacy levels, healthcare access, and multilingualism, all of which can influence dementia risk and cognitive performance. For instance, a study conducted among Hajj pilgrims in Mecca, Saudi Arabia, found that 29.2% had probable cognitive impairment, increasing their susceptibility to falls, dehydration, and other health complications132. Given that many Hajj pilgrims are older adults, these findings highlight the importance of integrating cognitive health assessments into pilgrimage health services, especially in light of rising temperatures due to climate change47. Addressing such gaps is critical to developing culturally relevant public health interventions tailored to the unique needs of MENA populations.
A significant limitation in dementia research and diagnosis across the region is the reliance on cognitive screening tools originally designed for Western populations, such as the MMSE and the Montreal Cognitive Assessment (MoCA). These tools often fail to account for cultural differences in literacy, language proficiency, bilingualism, and test familiarity, leading to potential false positives or false negatives in dementia diagnosis79,131,133. Despite the pressing need for culturally appropriate assessments, validated versions of these tests remain scarce in the region.
Some progress has been made in adapting cognitive screening tools for local populations. In Iran, the MMSE, Addenbrooke’s Cognitive Examination (ACE-III), MoCA, and Mini-Cog have been validated in Persian134. Egypt has developed adaptations of the m-ACE135 on a small sample, the MoCA136, and the Harmonized Cognitive Assessment Protocol (HCAP)137. Morocco and Lebanon have each adapted the MMSE138,139 and the 10/66 Dementia Research Group’s protocol140,141, with Morocco also validating the MoCA142. In Qatar, studies have employed the MMSE and Mini-Cog143.
However, no validation studies have been identified from Algeria, Bahrain, Iraq, Jordan, Kuwait, Libya, Oman, Saudi Arabia, Sudan, or Syria, leaving significant gaps in regionally adapted cognitive assessments. Without rigorous validation studies and standardized diagnostic frameworks, dementia diagnosis in MENA will continue to suffer from inconsistencies, hampering both clinical management and large-scale epidemiological research efforts.
Political and resource constraints
Conflict and political instability
Conflict and instability in several MENA countries, including Yemen, Sudan, Palestine, and Syria, have severely compromised the feasibility and validity of epidemiological research. The absence of specialized dementia services and the limited training of healthcare workers impede timely diagnosis and care delivery, particularly in conflict-affected and low-resource settings144. Ongoing violence, mass displacement, and resource scarcity create significant barriers to data collection, reduce participation rates, and limit the generalizability of findings. For example, in Lebanon, Phung et al. 26 were unable to expand their research participant pool due to regional conflicts, ultimately restricting their study to two coastal urban cities rather than conducting a nationwide investigation. These challenges are further exacerbated by corruption, lack of democratic governance, and persistent geopolitical tensions, which collectively hinder research output and scientific progress in the region8. Displacement and infrastructure damage also disrupt access to diagnostic services, making it difficult for researchers to reach affected populations or conduct longitudinal studies.
Prolonged violence and instability in countries such as Sudan, Syria, Libya, Yemen, and Palestine have exacerbated healthcare access issues and impeded the establishment of formal dementia care infrastructure145,146,147,148. For instance, in 2022, only 35 hospitals were operating on full capacity in the Gaza strip (1.55 hospital beds per 100,000)149. The ongoing Israeli-Palestinian conflict has resulted in a fragmented healthcare system, compounded by economic hardships and movement restrictions, which severely limit the management of noncommunicable diseases and aging-related conditions147. Families in these regions face displacement, economic hardship, and the psychological toll of war, further straining their ability to provide consistent dementia care. The 2023 Israeli offensive on Gaza disproportionately affected older adults, many of whom were unable to relocate due to physical limitations and faced reduced access to medical services, food, and basic necessities150.
According to the United Nations High Commissioner for Refugees (UNHCR) Report151, 17.4 million refugees, primarily from Syria, Iraq, Yemen, and Libya, were registered in 2021, placing additional strain on already overburdened healthcare systems. Since the 2014 ongoing civil war in Yemen, only 50% of hospitals and health centers are functional, with only 10 hospital beds and 5 physicians per 100,000 people145. Following the April 2023 conflict in Sudan, 30% of the country’s healthcare facilities were forced to close146. The destruction of healthcare facilities and displacement have left many older adults without access to essential medical services151. Similarly, in Palestine, restricted movement, economic blockades, and limited healthcare resources have severely impeded dementia care initiatives152. These challenges highlight the urgent need for targeted interventions to address the unique barriers faced by conflict-affected populations in accessing dementia care and support.
Healthcare systems and resource allocation
The COVID-19 pandemic has further exposed health system vulnerabilities, disrupting access to dementia care and neurological services across underserved regions, including MENA153. Healthcare systems across the region face significant challenges, with issues varying based on income levels and resource availability. In many countries, the private sector has expanded to address gaps in healthcare delivery, but this growth often occurs without adequate oversight, leading to inefficiencies and inequities. For example, countries like Egypt operate within pluralistic healthcare systems that include public, private, and parastatal providers. This fragmented approach results in poor intersectoral coordination and inconsistent service delivery154. Furthermore, many psychiatric hospitals are ill-equipped to meet the needs of dementia patients, highlighting an urgent need for specialized facilities and training103.
Resource constraints, inefficient management, and workforce shortages are prevalent across low- and middle-income countries in the region. There is a critical shortage of neurologists, geriatricians, and social workers trained in dementia diagnostics and care131,155,156. Compounding this issue, burnout and brain drain are significant challenges, with many healthcare professionals emigrating due to economic instability, inadequate wages, and limited career opportunities157,158. These workforce challenges further strain already overburdened healthcare systems, limiting the capacity to provide high-quality dementia care.
Existing healthcare policies in the MENA region often treat dementia as part of broader aging or NCD frameworks, rather than addressing it as a distinct public health priority. This approach has led to limited funding and infrastructure for dementia-specific interventions131,159. The absence of comprehensive national dementia strategies exacerbates these issues, resulting in fragmented research efforts and healthcare services. This underscores the urgent need for targeted policy reforms to prioritize dementia care and allocate resources effectively.
Implications for future research
This review highlights critical gaps that future research must address to improve dementia care in the MENA region. First, there is a pressing need for longitudinal, population-based studies using regionally adapted and validated tools to track dementia progression and establish causality100,160. Such studies should incorporate cultural, linguistic, and genetic differences across the region to generate accurate estimates and inform locally tailored interventions.
Expanding culturally sensitive and locally led research initiatives, such as Lebanon’s dementia cohort160 and Egypt’s AL-SEHA study on climate and cognitive decline19, can help identify region-specific risk profiles. In addition, better representation of Middle Eastern populations in drug trials is necessary, given the over-reliance on pharmacological studies conducted in Western populations156. There is also a need for screening tools that are adapted to local dialects, religions, and caregiving norms131. Translating research into local languages, improving healthcare communication, and increasing rural access to dementia services through enhanced infrastructure are crucial for equitable dementia care161. Future studies should also explore the feasibility and ethical considerations of novel interventions, such as stem cell therapy, which are being evaluated as emerging treatment options in other contexts162.
Public awareness and stigma reduction are essential areas for further exploration. Older adults in the MENA region often depend on informal family caregivers, many of whom lack basic knowledge about dementia symptoms and progression163. Community-based education initiatives, such as Egypt’s Dementia Support Initiative (DSIE), have shown promise through workshops and digital campaigns163. These efforts should be scaled across rural and underserved areas. Research shows that student exposure to dementia workshops can increase interest in dementia-focused careers130.
Strengthening healthcare systems and training professionals is another critical direction. There is a need to develop memory clinics, train specialized health workers, and improve access to neuropsychological assessments39. Digital platforms like Massive Online Open Courses (MOOCs) have demonstrated success in training healthcare providers, especially in resource-limited settings164. Countries like Egypt and Iran have made progress, but others such as Lebanon, Jordan, and Morocco still lack structured dementia training164. Research should evaluate the scalability and effectiveness of such models.
Policy-focused research should address access barriers and healthcare disparities in low-income and conflict-affected areas. Many families struggle to afford dementia care, particularly in countries experiencing political instability81. Efforts to bridge neurological care gaps must prioritize health equity and system-level reform, particularly for marginalized and underserved populations165. Mobile health units, telemedicine, and community networks may provide feasible alternatives. Studies should assess the feasibility and impact of conflict-sensitive dementia care strategies tailored to regions like Yemen, Sudan, and Palestine. The role of environmental exposures such as air pollution and urban stressors also requires more attention, following the lead of the AL-SEHA study19. A summary of all these challenges is illustrated in Fig. 4.

Summary of challenges facing dementia focused research in Middle East North Africa (MENA).
Finally, more research is needed on sociocultural shifts that affect caregiving, including increased female labor force participation and declining multigenerational households91. Integrating religious and cultural practices into caregiving models, such as Islamic caregiving values, may improve acceptance and adherence to care programs10. The use of technology—including telemedicine, mobile apps, and caregiver support platforms—also holds promise. For instance, Tunisia’s adaptation of WHO’s iSupport tool has demonstrated the potential of digital training solutions for caregivers166. In Qatar, 70% of healthcare workers rely on the internet for dementia knowledge, reinforcing the need to invest in accessible online resources113. Figure 5 depicts actionable steps to improve dementia research and care in MENA.

Actionable steps to improve dementia research and care in Middle East North Africa (MENA).
Strengths and limitations
A key strength of this review is its comprehensive scope, synthesizing evidence across epidemiological, socioeconomic, environmental, and policy dimensions. It integrates findings from both peer-reviewed literature and regional reports to present a holistic view of the dementia landscape in MENA. However, limitations include the heterogeneity of available studies, many of which rely on small, non-representative samples or cross-sectional designs. Additionally, significant variation in diagnostic tools and reporting standards limits comparability across countries. Despite these limitations, the review underscores the urgent need for coordinated, evidence-based responses to the growing dementia burden in the region.
Conclusion
Dementia constitutes a significant and rising public health challenge in the MENA region, exacerbated by population aging, high prevalence of noncommunicable diseases, and persistent inequities in healthcare access. This review has identified critical gaps in epidemiological data, diagnostic capacity, and culturally adapted care models that hinder the effective management of dementia across the region. To address these challenges, targeted investments in longitudinal research, standardized cognitive assessment tools, and workforce development are imperative.
Evidence-based policy interventions should prioritize health system strengthening, particularly in underserved and conflict-affected areas, while incorporating sociocultural dimensions to improve care uptake and reduce stigma. Regional collaboration and integration of dementia strategies into national health agendas are essential to promote equitable, sustainable, and context-specific solutions. Advancing this agenda will enhance diagnostic precision, care accessibility, and long-term outcomes for individuals living with dementia in the MENA region.
Data availability
No datasets were generated or analysed during the current study.
References
World Health Organization. World failing to address dementia challenge. https://www.who.int/news/item/02-09-2021-world-failing-to-address-dementia-challenge (2021).
United Nations. ANNUAL REPORT 2023 UNICEF Middle East and North Africa Regional Office. https://www.unicef.org/mena/media/24971/file/MENARO%20-%202023%20Regional%20Office%20Annual%20Report.
World Bank. Middle East & North Africa. https://data.worldbank.org/region/middle-east-and-north-africa?view=chart.
United Nations Populations Fund. World Population Dashboard. https://www.unfpa.org/data/world-population/ (2024).
National Institute of Aging. Aging. https://www.nih.gov/nih-style-guide/age (2025).
World Bank. Population Ages 65 and above (% of Total Population). https://data.worldbank.org/indicator/SP.POP.65UP.TO.ZS (2024).
Nichols, E. et al. Estimation of the global prevalence of dementia in 2019 and forecasted prevalence in 2050: an analysis for the Global Burden of Disease Study 2019. Lancet Public Health 7, e105–e125 (2022).
El Masri, J. et al. The Arab Countries’ Contribution to the Research of Neurodegenerative Disorders. Cureus https://doi.org/10.7759/cureus.17589 (2021)
Katoue, M. G., Cerda, A. A., García, L. Y. & Jakovljevic, M. Healthcare system development in the Middle East and North Africa region: challenges, endeavors and prospective opportunities. Front. Public Health 10, 1045739 (2022).
Khadr, Z. Growing old in an egyptian family: beyond the bare statistics. in Aging Across Cultures (ed. Selin, H.) (Springer International Publishing, 2021).
Qassem, T. et al. Prevalence and economic burden of dementia in the Arab world. BJPsych Open 9, e126 (2023).
Safiri, S. et al. The burden of Alzheimer’s disease and other types of dementia in the Middle East and North Africa region, 1990–2019. Age Ageing 52, afad042 (2023).
Avan, A. et al. The burden of neurological conditions in north Africa and the Middle East, 1990–2019: a systematic analysis of the Global Burden of Disease Study 2019. Lancet Glob. Health 12, e960–e982 (2024).
Moradinazar, M. et al. Epidemiological features of neurological disorders in North Africa and the Middle East from 1990 to 2019: results from the Global Burden of Disease Study 2019. Arch. Iran. Med. 26, 76–85 (2023).
Yüceşahin, M. M. & Tulga, A. Y. Demographic and social change in the Middle East and North Africa: processes, spatial patterns, and outcomes. Popul. Horiz 14, 47–60 (2017).
Taheri Soodejani, M., Rasoulian Kasrineh, M. & Tabatabaei, S. M. Incidence of Alzheimer disease and related dementias in Iran from 2010 to 2019. Alzheimer Dis. Assoc. Disord. 38, 285–287 (2024).
World Population Review. Kuwait. https://worldpopulationreview.com/countries/kuwait.
World Health Organization. Noncommunicable Diseases. https://www.who.int/news-room/fact-sheets/detail/noncommunicable-diseases (2024)
Moustafa, S. A., Boersch-Supan, A. & Salama, M. Aging in an Arab country: knowledge gaps in Egypt. Nat. Aging 3, 1042–1044 (2023).
World Health Organization. Results of Jordan National STEPwise Survey (STEPs) of Noncommunicable Diseases and Their Risk Factors 2019. https://www.emro.who.int/jor/jordan-news/results-of-jordan-national-stepwise-survey-steps-of-noncommunicable-diseases-and-their-risk-factors-2019.html (2020).
Livingston, G. et al. Dementia prevention, intervention, and care: 2024 report of the Lancet standing Commission. Lancet 404, 572–628 (2024).
Azizi, F. et al. Metabolic health in the Middle East and north Africa. Lancet Diab. Endocrinol. 7, 866–879 (2019).
Okati-Aliabad, H., Ansari-Moghaddam, A., Kargar, S. & Mohammadi, M. Prevalence of hypertension and pre-hypertension in the Middle East region: a systematic review & meta-analysis. J. Hum. Hypertens. 36, 794–804 (2022).
Kargar, S. & Ansari, H. Prevalence of dyslipidemias in the Middle East region: a systematic review & meta-analysis study. Diabetes Metab. Syndr. Clin. Res. Rev. 17, 102870 (2023).
Soreya, B., Meriem, T. & Samira Makri, M. Factors associated with dementia among elderly people living in Algiers. Ann. Alzheimers Dement. Care 5, 020–026 (2021).
Phung, K. T. T. et al. Dementia prevalence, care arrangement, and access to care in Lebanon: a pilot study. Alzheimers Dement 13, 1317–1326 (2017).
Chaaya, M. et al. Socio-demographic and cardiovascular disease risk factors associated with dementia: Results of a cross-sectional study from Lebanon. Prev. Med. Rep. 9, 1–5 (2018).
Feter, N. et al. Are gender differences in physical inactivity associated with the burden of dementia in low- and lower-middle income countries? Glob. Public Health 17, 727–737 (2022).
Chaabane, S., Chaabna, K., Abraham, A., Mamtani, R. & Cheema, S. Physical activity and sedentary behaviour in the Middle East and North Africa: an overview of systematic reviews and meta-analysis. Sci. Rep. 10, 9363 (2020).
Nikoloski, Z. Obesity in Middle East. in Metabolic Syndrome (ed. Ahima, R. S.) (Springer International Publishing). https://doi.org/10.1007/978-3-319-12125-3_6-2 (2023).
Alruwaili, B. et al. Prevalence and determinants of obesity and overweight among children and adolescents in the Middle East and North African Countries: an updated systematic review. Diabetes Metab. Syndr. Obes. 17, 2095–2103 (2024).
Nesrine S. F., Lawrence J. C. & Mohamed K. F. A systematic review of childhood obesity in the Middle East and North Africa (MENA) region: Prevalence and risk factors meta-analysis. Adv. Pediatr. Res. https://doi.org/10.12715/apr.2017.4.8 (2017).
Lloyd-Hazlegreaves, P., Hayes, L. & Pearce, M. S. Associations between physical inactivity and dementia prevalence: ecological study using global data. Public Health 225, 299–304 (2023).
Reitsma, M. B. et al. Spatial, temporal, and demographic patterns in prevalence of smoking tobacco use and initiation among young people in 204 countries and territories, 1990–2019. Lancet Public Health 6, e472–e481 (2021).
Khattab, A. et al. Smoking habits in the Middle East and North Africa: results of the BREATHE study. Respir. Med. 106, S16–S24 (2012).
Zhong, G., Wang, Y., Zhang, Y., Guo, J. J. & Zhao, Y. Smoking is associated with an increased risk of dementia: a meta-analysis of prospective cohort studies with investigation of potential effect modifiers. PLOS ONE 10, e0118333 (2015).
Kargar, S. & Ansari-Moghaddam, A. Prevalence of cigarette and waterpipe smoking and associated cancer incidence among adults in the Middle East. East. Mediterr. Health J. 29, 749–756 (2023).
Sultan, Y. et al. Smoking-related disease impact in the eastern mediterranean region: a comprehensive assessment using global burden of disease data. Asian Pac. J. Cancer Prev. 25, 495–505 (2024).
El-Metwally, A. et al. Epidemiology of Alzheimer’s Disease and dementia in arab countries: a systematic review. Behav. Neurol. 2019, 1–14 (2019).
Al-Zalabani, A. H. Secondhand smoke exposure among adolescents in the gulf cooperation council countries: analysis of global youth tobacco surveys. Sci. Rep. 14, 21534 (2024).
Kalan Farmanfarma, K. H., Ansari-Moghaddam, A., Zareban, I. & Adineh, H. A. Prevalence of type 2 diabetes in middle–east: systematic review & meta-analysis. Prim. Care Diabetes 14, 297–304 (2020).
Sherif, S. & Bauer, E. S. Economic development and diabetes prevalence in MENA countries: Egypt and Saudi Arabia comparison. World J. Diabetes 6, 304 (2015).
Jayaraj, R. L., Azimullah, S. & Beiram, R. Diabetes as a risk factor for Alzheimer’s disease in the Middle East and its shared pathological mediators. Saudi J. Biol. Sci. 27, 736–750 (2020).
El-Kebbi, I. M., Bidikian, N. H., Hneiny, L. & Nasrallah, M. P. Epidemiology of type 2 diabetes in the Middle East and North Africa: Challenges and call for action. World J. Diabetes 12, 1401–1425 (2021).
Beigh, S. et al. Dementia and multimorbidity trends in Al-Baha, Saudi Arabia: an analytical retrospective study using records-based data. Cureus https://doi.org/10.7759/cureus.52507 (2024).
World Health Organization. Public Health Advice on Preventing Health Effects of Heat. https://www.who.int/publications/i/item/public-health-advice-on-preventing-health-effects-of-heat (2019).
Ezzeldin, K., Adshead, D. & Smith, P. Adapting to a New Climate in the MENA Region. (2023).
Osipov, S. et al. Severe atmospheric pollution in the Middle East is attributable to anthropogenic sources. Commun. Earth Environ. 3, 203 (2022).
Isaifan, R. J. Air pollution burden of disease over highly populated states in the Middle East. Front. Public Health 10, 1002707 (2023).
United Nations Environment Programme. Damage in Gaza Causing New Risks to Human Health and Long-Term Recovery. https://www.unep.org/news-and-stories/press-release/damage-gaza-causing-new-risks-human-health-and-long-term-recovery (2024).
Lelieveld, J. et al. Severe ozone air pollution in the Persian Gulf region. Atmos. Chem. Phys. 9, 1393–1406 (2009).
Rentschler, J. & Leonova, N. Global air pollution exposure and poverty. Nat. Commun. 14, 4432 (2023).
Hajat, A., Hsia, C. & O’Neill, M. S. Socioeconomic disparities and air pollution exposure: a global review. Curr. Environ. Health Rep. 2, 440–450 (2015).
Akasha, H., Ghaffarpasand, O. & Pope, F. D. Air pollution and economic growth in Dubai a fast-growing Middle Eastern city. Atmos. Environ. X 21, 100246 (2024).
Rostam‐Abadi, Y. et al. Alcohol use, alcohol use disorder and heavy episodic drinking in the Eastern Mediterranean region: a systematic review. Addiction 119, 984–997 (2024).
Safiri, S. et al. Burden of diseases and injuries attributable to alcohol consumption in the Middle East and North Africa region, 1990–2019. Sci. Rep. 12, 19301 (2022).
Degenhardt, L. et al. The global burden of disease attributable to alcohol and drug use in 195 countries and territories, 1990–2016: a systematic analysis for the Global Burden of Disease Study 2016. Lancet Psychiatry 5, 987–1012 (2018).
Ghandour, L. et al. Alcohol consumption in the Arab region: what do we know, why does it matter, and what are the policy implications for youth harm reduction? Int. J. Drug Policy 28, 10–33 (2016).
Alageel, S. & Alomair, N. Muslims perceptions of safe alcohol use: a qualitative study in the Gulf Council Cooperation countries. Harm. Reduct. J. 21, 167 (2024).
Safiri, S. et al. The burden of major depressive disorder in the Middle East and North Africa region, 1990–2019. Acta Neuropsychiatr. 36, 139–152 (2024).
Moradinazar, M. et al. Epidemiological status of depressive disorders in the Middle East and North Africa from 1990 to 2019. Health Promot. Perspect. 12, 301–309 (2022).
Ahmed, H. et al. Depression in geriatrics: a systematic review and meta-analysis of prevalence and risk factors in Egypt. BMC Geriatr 24, 930 (2024).
Gholamzadeh, S., Heshmati, B., Mani, A., Petramfar, P. & Baghery, Z. The prevalence of Alzheimer’s disease; its risk and protective factors among the elderly population in Iran. Shiraz E-Med. J. 18, e57576 (2017).
Elsayed, H., Ibrahim, IbtihalM, A., Abu-Hegazy, M. & Amr, M. Behavioral and psychological characteristics of patients with different types of dementia in Mansoura, Egypt. Egypt. J. Psychiatry 38, 13 (2017).
Al Sulaiti, E. M., Abdelnour, S. & Ramadan, M. A study of dementia in home care patients in qatar with the psychosocial burden on caregivers. Qatar Med. J. 2008, 15 (2008).
Kofahi, R. et al. Annual period prevalence and risk factors of dementia among older jordanian hospitalized patients. Int. J. Gen. Med. 14, 641–647 (2021).
Abulsaad, K., Alsaeed, M. & AlMahmoud, M. Cognitive impairment among elderly patients admitted for post-acute care in Bahrain. Egypt. J. Geriatr. Gerontol. 7, 37–41 (2020).
Abu Hammud, M. & Jarrar, A. G. Fighting Illiteracy in the Arab World. Int. Educ. Stud. 10, 116 (2017).
Suh, S. W. et al. Impacts of illiteracy on the risk of dementia: a global health perspective. J. Alzheimers Dis. 53, 731–741 (2016).
El Tallawy, H. N. et al. Prevalence of dementia in Al Kharga District, New Valley Governorate, Egypt. Neuroepidemiology 38, 130–137 (2012).
Elshahidi, M., Elhadidi, M., Sharaqi, A., Mostafa, A. & Elzhery, M. Prevalence of dementia in Egypt: a systematic review. Neuropsychiatr. Dis. Treat. ume 13, 715–720 (2017).
Hamdy N. E. T. et al. Prevalence of dementia in Al-Quseir city, Red Sea Governorate, Egypt. Clin. Interv. Aging 9, https://doi.org/10.2147/CIA.S48325 (2013).
Shelley, B. P. & Al Khabouri, J. The spectrum of dementia: frequency, causes and clinical profile. Dement. Geriatr. Cogn. Disord. 24, 280–287 (2007).
Assaf, G., El Khoury, J., Jawhar, S. & Rahme, D. Mild cognitive impairment and modifiable risk factors among Lebanese older adults in primary care. Asian J. Psychiatry 65, 102828 (2021).
Sharp, E. S. & Gatz, M. Relationship between education and dementia: an updated systematic review. Alzheimer Dis. Assoc. Disord. 25, 289–304 (2011).
Salem, G., Said, R., Amin, S., Elserafy, T. S. E. & Awadallah, M. Prevalence, types and different predictors of Dementia diseases among people, community based study, Egypt. Egypt. Fam. Med. J. 4, 64–79 (2020).
Tawfik, A. A., Hamza, S. A., Adly, N. N. & Abdel Kader, R. M. Pattern of cognitive impairment among community-dwelling elderly in Egypt and its relation to socioeconomic status. J. Egypt. Public Health Assoc. 99, 4 (2024).
Hayajneh, A. A., Rababa, M., Alghwiri, A. A. & Masha’al, D. Factors influencing the deterioration from cognitive decline of normal aging to dementia among nursing home residents. BMC Geriatr 20, 479 (2020).
Yaghmour, S. M., Bartlett, R. & Brannelly, T. Dementia in Eastern Mediterranean countries: a systematic review. Dementia 18, 2635–2661 (2019).
Shubair, S. A. Dementia care in gerontological social work: emerging issues and challenges in Saudi Arabia. Front. Public Health 11, 1167856 (2023).
Kane, T. et al. Dementia caregiving in the Middle East and North Africa: a scoping review. Transcult. Psychiatry 58, 844–858 (2021).
Paul, P. et al. Knowledge, awareness, and attitude of healthcare stakeholders on Alzheimer’s disease and dementia in Qatar. Int. J. Environ. Res. Public. Health 20, 4535 (2023).
Ibrahim, A. A., AI-Lami, F., Al-Rudainy, R. & Khader, Y. S. Mental disorders among elderly people in Baghdad, Iraq, 2017. Inq. J. Health Care Organ. Provis. Financ. 56, 0046958019845960 (2019).
Kamalzadeh, L. et al. Prevalence of dementia among older patients: a hospital-based study in Iran. Am. J. Alzheimers Dis. Dementias® 34, 500–506 (2019).
Abdelhalim, D. S., Ahmed, M. M., Hussein, H. A., Khalaf, O. O. & Sarhan, M. D. Burden of care, depression, and anxiety among family caregivers of people with dementia. J. Prim. Care Community Health 15, 21501319241288029 (2024).
Ibrahim, A. M., Ibrahim, M. M. & Zaghamir, D. E. F. Burden of care and quality of life among informal caregivers to Alzheimer patients in Egypt. Palliat. Support. Care 22, 182–189 (2024).
Al Maqbali, M. & A-Sinawi, H. Burden of care among relatives of people with dementia attending tertiary care in Oman. Eur. Psychiatry 33, S184–S184 (2016).
Bridi, L. et al. Attitudes toward dementia and cognitive aging among Syrian refugees resettled in Jordan: a qualitative study. BMC Public Health 23, 2307 (2023).
World Bank. Global Economic Prospects- January 2023. https://openknowledge.worldbank.org/server/api/core/bitstreams/254aba87-dfeb-5b5c-b00a-727d04ade275/content (2023).
Al Hamad, H. & Sathian, B. Identifying Dementia research priority for Qatar national dementia research plan: a cross-sectional survey. Nepal J. Epidemiol. 14, 1313–1322 (2024).
Hammad, S. H., Daher-Nashif, S., Kane, T. & Al-Wattary, N. Sociocultural insights on dementia care-giving in Arab and Muslim communities: the perspectives of family care-givers. Ageing Soc 44, 357–384 (2024).
Ghassemzadeh, H. et al. Occupational risk factors for dementia in a sample of older adults covered by the iranian oil industries’ health centers, 2018. Gênero Direito 8, 482–495 (2019).
Hashemi, R., Vahabi, Z., Rasekhi, H., Shiraseb, F. & Amini, M. Dietary patterns and the risk of Alzheimer’s disease in an elderly Iranian population: a case–control study. J. Health Popul. Nutr. 42, 56 (2023).
Talhaoui, A., Aboussaleh, Y., Bikri, S., Rouim, F. Z. & Ahami, A. The relationship between adherence to a Mediterranean Diet and cognitive impairment among the elderly in Morocco. Acta Neuropsychol 21, 125–138 (2023).
Jomaa, L. et al. A Lebanese dietary pattern promotes better diet quality among older adults: findings from a national cross-sectional study. BMC Geriatr. 16, 85 (2016).
Hoteit, M. et al. Dietary intake among lebanese adults: findings from the updated LEBANese natiONal Food Consumption Survey (LEBANON-FCS). Nutrients 16, 1784 (2024).
Hefnawy, G. R. M. Prevalence of malnutrition in community-dwelling Egyptian elderly. Indian J. Public Health Res. Dev. 10, 1240 (2019).
Hoteit, M. et al. Exploring the impact of crises on food security in lebanon: results from a National Cross-Sectional Study. Sustainability 13, 8753 (2021).
Serri, L., Poobalan, A., Soiza, R. & Phyo, K. M. Should Kuwait join global epidemiological research for older people? Kuwait Med. J. 56, 50–53 (2024).
Alshanberi, A. M. Frailty in Kingdom of Saudi Arabia—Prevalence and Management, Where Are We? Healthcare 11, 1715 (2023).
Al-Awad, F. A. et al. Knowledge levels and sociodemographic influences on dementia awareness in the Eastern Province of Saudi Arabia. Electron. J. Gen. Med. 21, em567 (2024).
Mohamad, R. M. et al. Evaluating the general population of Saudi Arabia for their knowledge, attitudes, and practices towards dementia. Cureus https://doi.org/10.7759/cureus.49865 (2023).
Sharif, L. et al. Caring for people living with dementia in Saudi Arabia: the perspective of nurses as primary caregivers. Inq. J. Health Care Organ. Provis. Financ. 61, 00469580241248125 (2024).
Okasha, A., Karam, E. & Okasha, T. Mental health services in the Arab world. World Psychiatry 11, 52–54 (2012).
Shokr, H., Rishworth, A. & Wilson, K. Access to emergency care in Egypt: tiered health care and manifestations of inequity. Soc. Sci. Med. 336, 116212 (2023).
Luqman, M. & Khan, S. U. Geospatial application to assess the accessibility to the health facilities in Egypt. Egypt. J. Remote Sens. Space Sci. 24, 699–705 (2021).
Heikal, S. A., Moghith, A. A. & Salama, M. Perceptions of dementia and their implications on disease management in Egypt. Discov. Med. 2, 15 (2025).
Althaiban, M. A., Aljefree, N. M., Almoraie, N. M. & Shatwan, I. M. Malnutrition is associated with increased disease risk in older people in the Makkah region of Saudi Arabia: a cross-sectional study. Front. Public Health 11, 1149739 (2023).
Alhumaidi, F. S. et al. Public knowledge about Alzheimer disease in Mecca Region, Kingdom of Saudi Arabia: a cross-sectional study. Egypt. J. Neurol. Psychiatry Neurosurg. 56, 89 (2020).
Algethami, W. et al. Factors associated with public knowledge and attitude to dementia: a cross sectional study. Int. J. Med. Dev. Ctries. 952–956 https://doi.org/10.24911/IJMDC.51-1568202042 (2019).
Ashour, A. A. et al. Dementia awareness in Egypt: what do people really know? Egypt. J. Neurol. Psychiatry Neurosurg. 60, 91 (2024).
Abuawad, M. et al. Evaluation of knowledge and attitudes regarding Alzheimer’s disease and related dementia among medical students in Palestine: a cross-sectional study. PLOS ONE 19, e0304012 (2024).
Al Hamad, H. & Sathian, B. Awareness of dementia risk factors among healthcare professionals at Hamad Medical Corporation, Qatar: a cross-sectional survey. Front. Public Health 12, 1443525 (2024).
Aderinto, N., Abdulbasit, M., Olatunji, G. & Edun, M. The landscape of neuroscience research in Africa: current state, progress, and challenges; a perspective. Ann. Med. Surg. 85, 5267–5274 (2023).
Martin P. et al. World Alzheimer Report 2015: The Global Impact of Dementia. Alzheimer’s Disease International. https://www.alzint.org/u/WorldAlzheimerReport2015.pdf (2015).
El Tallawy, H. N. A. et al. Epidemiology of Major Neurological Disorders Project in Al Kharga District, New Valley, Egypt. Neuroepidemiology 35, 291–297 (2010).
El Tallawy, H. N. A. et al. Prevalence of Alzheimer dementia in Upper Egypt (desert areas). Egypt. J. Neurol. Psychiatry Neurosurg. 55, 29 (2019).
Farrag, A.-K. F., Farwiz, H. M., Khedr, E. H., Mahfouz, R. M. & Omran, S. M. Prevalence of Alzheimer’s disease and other dementing disorders: assiut-upper Egypt Study. Dement. Geriatr. Cognit. Disord. 9, 323–328 (1998).
Khedr, E. et al. Prevalence of mild cognitive impairment and dementia among the elderly population of Qena Governorate, Upper Egypt: a Community-Based Study. J. Alzheimers Dis. 45, 117–126 (2015).
Mohammed, F. S. A., Wahba, H. M. F., Gabal, H.-A. M. S. & El Said, S. M. S. Prevalence of cognitive impairment among elderly in primary health care centers in Cairo, Egypt. QJM Int. J. Med. 116, hcad069.272 (2023).
Oshnouei, S., Safaralizade, M., Eslamlou, N. F. & Heidari, M. Uncovering the extent of dementia prevalence in Iran: a comprehensive systematic review and meta-analysis. BMC Public Health 24, 1168 (2024).
El-Zawawi, H. Frequency of dementia among patients admitted to Benghazi Medical Center over a six months period in 2017. J. Neurol. Sci. 429, 119052 (2021).
Alkhunizan, M., Alkhenizan, A. & Basudan, L. Prevalence of mild cognitive impairment and dementia in Saudi Arabia: a Community-Based Study. Dement. Geriatr. Cognit. Disord. Extra 8, 98–103 (2018).
Moustafa, S., Gaballah, N., Deif, R. & Salama, M. Exploring aging dynamics In Egypt: insights from The Al-Seha Pilot Study. Innov. Aging 8, 50–50 (2024).
Chaaya, M. et al. Dementia incidence among a cohort of lebanese older adults: first incidence estimates from the Middle East and North Africa region. Front. Dement. 3, 1494719 (2025).
Fahanik‐Babaei, J. et al. Preliminary report of Iranian Registry of Alzheimer’s disease in Tehran province: a cross‐sectional study in Iran. Health Sci. Rep. 5, e952 (2022).
Al Hamad, H., Nadukkandiyil, N., Chandran, M., Manikoth, P. T. & Sathian, B. One year analysis of prospective memory clinics Registry in Qatar: a critical tool for dementia research and policy planning. Nepal J. Epidemiol. 14, 1323–1332 (2024).
Fattahi, N. et al. Geographical, gender and age inequalities in non-communicable diseases both at national and provincial levels in Iran. J. Diabetes Metab. Disord. 23, 1525–1531 (2021).
Manee, F., Nadar, M., Qadoura, D., Rassafiani, M. & Badr, H. E. Dementia awareness among healthcare professionals in Kuwait. Int. J. Ther. Rehabil. 30, 1–9 (2023).
Manee, F. Dementia knowledge among Kuwait University Students: a descriptive study. Arch. Neurol. Neurosci. 5, 10–33552 (2019).
Fasfous, A. F., Al-Joudi, H. F., Puente, A. E. & Pérez-García, M. Neuropsychological measures in the Arab World: a systematic review. Neuropsychol. Rev. 27, 158–173 (2017).
Alzahrani, A. S., Alhumaidi, F., Altowairqi, A., Al-Malki, W. & AlFadhli, I. Screening for cognitive impairment in Arabic-speaking Hajj pilgrims. Egypt. J. Neurol. Psychiatry Neurosurg. 55, 65 (2019).
Farshad, S. et al. Prevalence of dementia and associated factors among older adults in Iran: National Elderly Health Survey (NEHS). Arch. Iran. Med. 19, 838–844 (2016).
Kamalzadeh, L. et al. Diagnostic accuracy of cognitive screening tools validated for older adults in Iran: a systematic review and meta-analysis. BMC Geriatr. 24, 428 (2024).
Qassem, T. et al. Adaptation and validation of the Mini-Addenbrooke’s cognitive examination in dementia in Arabic Speakers in Egypt. Dement. Geriatr. Cognit. Disord. 49, 611–616 (2020).
Saleh, A. A. et al. Validation of montreal cognitive assessment-basic in a sample of elderly Egyptians with neurocognitive disorders. Aging Ment. Health 23, 551–557 (2019).
Moustafa, S. A. et al. Validation of harmonized cognitive assessment protocol within the Egyptian context. Soc. Psychiatry Psychiatr. Epidemiol. https://doi.org/10.1007/s00127-024-02783-2 (2024).
Rami, Y., Diouny, S., Kissani, N. & Yeou, M. Cross-cultural adaptation of the Moroccan version of the Mini-Mental State Examination: a preliminary study. Appl. Neuropsychol. Adult 31, 595–600 (2024).
El-Hayeck, R. et al. An Arabic version of the mini-mental state examination for the lebanese population: reliability, validity, and normative data. J. Alzheimers Dis. 71, 525–540 (2019).
Oumellal, A., El Alaoui Faris, M. & Benabdeljlil, M. Population normative data of the Moroccan Arabic Version of three components of the 10/66 dementia research group cognitive test battery; with Moroccan Illiterate and Semi-Illiterate Subjects. Adv. Alzheimers Dis. 08, 1–14 (2019).
Phung, K. T. T. et al. Validation of the 10/66 dementia research group diagnostic assessment for dementia in Arabic: a study in Lebanon. J. Geriatr. Psychiatry Neurol. 27, 282–290 (2014).
Khatib, N. et al. The Moroccan MoCA test: translation, cultural adaptation, and validation. Appl. Neuropsychol. Adult 31, 1256–1260 (2024).
Albanna, M. et al. Validation and cultural adaptation of the Arabic versions of the mini-mental status examination-2 and Mini-Cog test. Neuropsychiatr. Dis. Treat. 13, 793–801 (2017).
Kantawala, B. et al. Dementia challenges in Africa: journeying through forgetfulness. Health Sci. Rep. 6, e1561 (2023).
Alsabri, M., Alsakkaf, L., Alhadheri, A., Cole, J. & Burkle, F. Jr. Chronic health crises and emergency medicine in War-torn Yemen, exacerbated by the COVID-19 Pandemic. West. J. Emerg. Med. 23, 276–284 (2022).
Elamin, A. et al. Sudan: from a forgotten war to an abandoned healthcare system. BMJ Glob. Health 9, e016406 (2024).
Juzoor for Health and Social Development. Gaza’s Battle for Survival in a Shattered Health System. https://www.juzoor.org/cached_uploads/download/2024/03/12/03-2024-a-war-on-health-gaza-juzoor-report-1710245501.pdf (2024).
Abdulshafea, M. et al. The epidemiology of common mental disorders in Libya: a systematic review. Egypt. J. Neurol. Psychiatry Neurosurg. 57, 161 (2021).
Palestinian Ministry of Health. 2022 Annual Report, Southern Governorates Gaza Strip. https://www.moh.gov.ps/portal (2023).
Van Boetzelaer, E., Franco, O. H., Moussally, K., Khammash, U. & Escobio, F. The disproportionate vulnerability of older people in humanitarian emergencies. Lancet 402, 1621 (2023).
United Nations High Commissioner for Refugees. The Middle East and North Africa. 96–102 https://reporting.unhcr.org/sites/default/files/ga2021/pdf/Chapter_MENA.pdf.
World Health Organization. Health Conditions in the Occupied Palestinian Territory, Including East Jerusalem, and in the Occupied Syrian Golan. https://apps.who.int/gb/ebwha/pdf_files/WHA76/A76_15-en.pdf (2023).
Uwishema, O. et al. The impact of COVID‐19 on patients with neurological disorders and their access to healthcare in Africa: a review of the literature. Brain Behav 12, e2742 (2022).
Gericke, C. A., Britain, K., Elmahdawy, M. & Elsisi, G. Health system in Egypt. Health Care Syst. Policies (eds. Van Ginneken, E. & Busse, R.). https://doi.org/10.1007/978-1-4614-6419-8_7-1 (Springer, 2018).
Alsalem, Z. A., Alghathber, N. M., Alowain, F. S., Alqahtani, M. S. & Alharbi, N. G. Dementia knowledge among primary healthcare physicians in Riyadh, Saudi Arabia. Cureus https://doi.org/10.7759/cureus.61112 (2024).
Tayeb, H. O. et al. The future of alzheimer disease immunotherapies in Saudi Arabia: consensus statement of the Saudi Chapter of cognitive and behavioral neurology. Neurosciences 28, 77–84 (2023).
Kabbash, I. et al. The brain drain: why medical students and young physicians want to leave Egypt. East. Mediterr. Health J. 27, 1102–1108 (2021).
Ghanbari-Jahromi, M. & Ahmadi Marzaleh, M. Factors affecting brain drain and a solution to reduce it in Iran’s Health System: a qualitative study. Arch. Iran. Med. 27, 427–438 (2024).
Boettiger, D. C. et al. Projected impact of population aging on non-communicable disease burden and costs in the Kingdom of Saudi Arabia, 2020–2030. BMC Health Serv. Res. 23, 1381 (2023).
Chaaya, M. Uncovering the burden of Dementia in the Middle East and North Africa (MENA) Region: current situation, opportunities, and challenges. Alzheimers Dement 19, e081440 (2023).
Javaid, S. F., Al-Zahmi, A. & Abbas, M. Carer empowerment is key to reduce dementia care inequalities in the Middle East. Int. J. Environ. Res. Public. Health 18, 4378 (2021).
Pradhan, A. U., Uwishema, O., Onyeaka, H., Adanur, I. & Dost, B. A review of stem cell therapy: an emerging treatment for dementia in Alzheimer’s and Parkinson’s disease. Brain Behav. 12, e2740 (2022).
Alwerdani, M. et al. Dementia support initiative in Egypt: outreach awareness activity in Egypt. IBRO Neurosci. Rep. 15, S356–S357 (2023).
Naal, H., El Koussa, M., El Hamouch, M., Hneiny, L. & Saleh, S. A systematic review of global health capacity building initiatives in low-to middle-income countries in the Middle East and North Africa region. Glob. Health 16, 56 (2020).
Uwishema, O. & Boon, P. Bridging the Gaps: addressing Inequities in neurological care for underserved populations. Eur. J. Neurol. 32, e70073 (2025).
Gouider, R. et al. Preparing for implementing “iSupport” in Tunisia: experience and needs of caregivers of persons with dementia. Int. Psychogeriatr. 35, 33–34 (2023).
World Health Organization. Global Health Observatory. https://www.who.int/data/gho (2024).
Ebrahimi, H., Tajadini, H., Kamali, H., Khazanehha, M. & Kamali, M. Prevalence and risk factors of Alzheimer ُs disease in elderly people, Kerman, Iran: a house based survey. J. Kerman Univ. Med. Sci. 28, 252–260 (2021).
Al-Qazaz, H., Shanshal, S., Qasim, I. & Saleem, F. Cognitive function among rural people in Nineveh: a cross-sectional survey. Iraqi J. Pharm. 20, 48–52 (2023).
Bou-Orm, I. R., Khamis, A. M. & Chaaya, M. Determinants of poor cognitive function using A-IQCODE among Lebanese older adults: a cross-sectional study. Aging Ment. Health 22, 844–848 (2018).
Institute for Health Metrics and Evaluation (IHME). GBD Results. https://vizhub.healthdata.org/gbd-results/.
Author information
Authors and Affiliations
Contributions
Conceptualization: All Authors. Collecting data: S.M., S.A.M. and M.W. Writing first draft: S.M., S.A.M., M.W., S.H. and M.O. Supervision: M.S. All authors reviewed and approved the final version.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Mowafi, S., Moustafa, S.A., Wahdan, M. et al. Dementia in the MENA region uncharted challenges and emerging insights a literature review. npj Dement. 1, 5 (2025). https://doi.org/10.1038/s44400-025-00009-z
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s44400-025-00009-z
This article is cited by
-
The Egyptian HCAP validation: a case study for culturally-informed neurocognitive assessment in the MENA region
npj Dementia (2026)
-
Geriatric psychiatry and dementia services in Egypt: current evidence, challenges and future directions
Middle East Current Psychiatry (2025)
