
Abstract
While ambient fine particulate matter (PM2.5) is linked to obstructive sleep apnea (OSA), the specific roles of its chemical constituents have never been investigated. Using a nationwide smart device-based cohort encompassing 6,395,382 person-days of sleep monitoring from 53,297 adults at moderate-to-severe OSA risk across 313 Chinese cities, we conducted a case time series study to evaluate short-term associations between daily concentrations of PM₂.₅ constituents (organic matter, black carbon, nitrate, sulfate, and ammonium) and OSA exacerbation, apnea–hypopnea index (AHI), and oxygen saturation. All five constituents were significantly associated with adverse OSA outcomes, with organic matter and black carbon exerting the strongest effects. Each interquartile range increase in organic matter (lag 0–1 days) was associated with a 1.92% increase in OSA exacerbation risk (95% CI: 1.56–2.28), a 0.08 events/h increase in AHI (95% CI: 0.06–0.09), and a 0.008% decrease in oxygen saturation (95% CI: 0.007–0.008). Black carbon demonstrated comparably strong adverse effects across all outcomes. The remaining constituents showed weaker but directionally consistent associations, with effect estimates ranging from 1.41% to 1.45% for OSA exacerbation, around 0.06 events/h for AHI, and 0.005–0.006% for oxygen saturation. These findings provide the first evidence that specific PM2.5 constituents contribute differentially to OSA severity, underscoring the importance of targeting carbonaceous particles in air quality management.
Similar content being viewed by others


Introduction
Obstructive sleep apnea (OSA) is a common sleep disorder characterized by recurrent upper airway collapse during sleep, leading to intermittent hypoxia, sleep fragmentation, and activation of the sympathetic nervous system1. Globally, an estimated 936 million adults are affected by OSA, with approximately half experiencing moderate to severe forms of the condition2. OSA not only impairs daytime functioning and quality of life but also represents an independent risk factor for various diseases, including cardiovascular disease3, metabolic dysfunction4, and neurocognitive impairments5, thereby contributing substantially to the global public health burden. Accordingly, identifying risk factors for OSA is critical for its prevention and for mitigating the associated disease burden.
Fine particulate matter (PM2.5, particles ≤ 2.5 µm in aerodynamic diameter) is a ubiquitous air pollutant that has been causally linked to adverse cardiorespiratory outcomes6. PM2.5 penetrates deep into the lungs and can translocate into systemic circulation, exerting detrimental effects through mechanisms such as oxidative stress, systemic inflammation and autonomic imbalance7. Notably, these pathways significantly overlap with the core pathophysiology of OSA8, indicating a biologically plausible link between PM2.5 exposure and OSA severity. Indeed, our previous work established significant associations of short-term exposure to ambient PM2.5 with increased risk of apnea/hypopnea and oxygen desaturation based on a nationwide analysis of smart device-based monitoring, providing direct evidence of the impact of PM2.5 on this condition9.
However, PM2.5 is not a uniform pollutant, but a complex and heterogeneous mixture of chemical constituents such as black carbon (BC), organic matter (OM), sulfate (SO₄²−), nitrate (NO₃−), and ammonium (NH₄⁺)10. These components originate from diverse sources, possess distinct physicochemical properties, and exhibit varying toxicological profiles. For example, Jiang et al.11 reported that carbonaceous components (i.e., OM and BC) were the predominant particulate matter species associated with acute coronary syndrome onset. As such, relying solely on PM2.5 mass concentration may obscure the contributions of specific constituents or source-specific mixtures to health effects, thereby limiting efforts to identify key harmful agents and implement targeted mitigation strategies. Dissecting the PM2.5 mixture to pinpoint the chemical species most strongly associated with OSA severity is therefore critical. However, to date, no study has investigated the associations between individual PM2.5 constituents and the risk of OSA.
Leveraging large-scale, longitudinal OSA monitoring in home settings enabled by a validated smart device technology9, we performed a nationwide case time series analysis to evaluate associations of PM2.5 chemical components with OSA exacerbation, as well as two key severity indicators, the apnea–hypopnea index (AHI) and oxygen saturation12. By evaluating component-specific risks, this study aims to inform targeted public health interventions and more nuanced air quality regulations that go beyond total PM2.5 mass to address the specific contributors to OSA burden.
Results
Descriptive statistics
After removing individuals with fewer than seven valid monitoring days, we included 53,297 adults at moderate-to-severe risk for OSA, yielding 6,395,382 person-days of records collected between December 2019 and October 2022 (Table S1). As previously documented in our earlier publication9, these individuals were drawn from 313 Chinese cities at the prefecture level or above. The average age of the cohort was 45.4 years (SD: 14.0), and the majority were male (95.5%). Additionally, 30.6% had a self-reported history of arrhythmia, 40.1% reported hypertension, 7.8% reported diabetes, and 9.4% reported a history of ischemic heart disease (Table S1).
OSA exacerbation occurred on 46.2% of the total monitored days. The AHI was markedly higher during OSA exacerbation days (median: 29.94 events/h) compared to days without such events (median: 0.93 events/h). Likewise, mean oxygen saturation was lower on days with exacerbation (median: 96.39%) than on non-exacerbation days (median: 96.57%). Concentrations of PM2.5 and its constituents were also elevated on exacerbation days. Detailed comparisons are provided in Table S1. In general, participants who were older, male, obese, or had a history of cardiometabolic diseases exhibited worse OSA outcomes compared to their counterparts (Table S2).
As shown in Table S3, PM2.5 and its constituents were positively correlated with one another, with Spearman correlation coefficients ranging from 0.75 to 0.98. In contrast, ambient temperature (r = −0.26 to −0.42) and relative humidity (r = −0.06 to −0.25) were negatively associated with total PM2.5 mass and its constituents.
The association of PM2.5 and its constituents with OSA-related outcomes
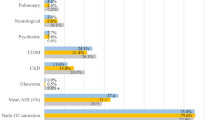
Figure 1 presents the associations of total PM2.5 mass and its constituents with OSA exacerbation, AHI, and oxygen saturation over various lag days. The effects of PM2.5 mass and its components on OSA-related outcomes appeared on the same day as sleep monitoring (lag 0 d), declined sharply by lag 2 d, and were no longer significant for certain outcomes, including OSA exacerbation and AHI. Based on this temporal pattern, we selected the average exposure over lag 0–1 d as the primary exposure window for all subsequent analyses. As shown in Fig. 1, we found that each interquartile range (IQR) increase in PM2.5 mass or its constituents was associated with a 1.41–1.92% higher risk of OSA exacerbation, a 0.06–0.08 events/h increase in AHI, and a 0.005–0.008 reduction in oxygen saturation (%). Among the constituents, OM and BC exhibited the strongest associations across outcomes, whereas SO₄²−, NO₃−, and NH₄⁺ showed comparatively weaker effects. For instance, each IQR increase in OM or BC was associated with approximately a 1.9% higher risk of OSA exacerbation, while the corresponding increase for SO₄²−, NO₃−, and NH₄⁺ was around 1.4% (Fig. 1). These associations remained relatively stable in both the constituent–PM2.5 adjustment models and the constituent–residual models, although confidence intervals were slightly wider (Fig. 2).

A shows the associations with OSA exacerbation, B with apnea–hypopnea index, and C with oxygen saturation. PM2.5 fine particulate matter, OM organic matter, BC black carbon, OSA obstructive sleep apnea. Notes: Associations were presented as percent change in the risk of OSA exacerbation, absolute change of apnea–hypopnea index and oxygen saturation per interquartile range increase in concentrations of PM2.5 total mass and its chemical constituents. Dots are the estimates, and error bars indicate 95% confidence intervals.

The panels show results for A OSA exacerbation, B apnea–hypopnea index and C oxygen saturation in the single-constituent model, the constituent–PM2.5 adjustment model, and the constituent–residual model. PM2.5 fine particulate matter, OM organic matter, BC black carbon, OSA obstructive sleep apnea. Notes: Associations were presented as percent change in the risk of OSA exacerbation, absolute change of apnea–hypopnea index and oxygen saturation per interquartile range increase in concentrations of PM2.5 total mass and its chemical constituents. Dots are the estimates, and error bars indicate 95% confidence intervals.
Figures 2, S1, and S2 depict the exposure–response (E–R) curves for the associations of PM2.5 constituents with OSA exacerbation, AHI, and oxygen saturation, respectively. The E–R curves exhibited similar shapes across different exposures and outcomes, with no apparent threshold below which no risk (Fig. 3). was observed. As concentrations increased, the slopes of these curves gradually leveled off.

The panels display the relationships for A PM2.5 total mass, B OM, C BC, D sulfate, E nitrate and F ammonium. PM2.5 fine particulate matter, OM organic matter, BC black carbon.Notes: The solid lines are the estimated percent change of risk of obstructive sleep apnea exacerbation. The shaded areas indicate95% confidence intervals.
Results of subgroup analyses
No significant effect modification was detected for age or history of cardiometabolic conditions, including arrhythmia, hypertension, diabetes, and ischemic heart disease (Tables 1, S4, and S5). Associations between PM₂.₅ constituents and OSA exacerbation (Table 1) or AHI (Table S4) were more pronounced in males, whereas no clear modification by sex was detected for oxygen saturation. Stronger associations of PM2.5 constituents with OSA exacerbation, but not with AHI or oxygen saturation, were also observed among individuals with lower body mass index (BMI). Seasonal stratification indicated that the effects of most PM₂.₅ constituents on OSA exacerbation and AHI were generally consistent across seasons, except for SO₄²−, which showed markedly stronger associations during warmer periods (Tables 1 and S4). By contrast, the associations between all PM2.5 constituents and oxygen saturation were consistently stronger during the warm season (Table S5). Stratified analyses by region showed that associations between PM2.5 constituents and OSA outcomes were generally stronger in Southern China (Tables 1, S4, and S5), except for NO₃− and NH₄⁺, which exhibited stronger associations with oxygen saturation reduction in Northern China (Table S5).
Discussion
This is the first study to disentangle the effects of specific PM2.5 constituents on sleep apnea severity. Leveraging over six million person-days of home-based sleep monitoring from more than 50,000 individuals across 313 cities in China, we consistently identified OM and BC as the dominant contributors to OSA severity across the single-constituent model, the constituent–PM2.5 adjustment model, and the constituent–residual model. The associations between PM2.5 constituents and OSA severity were more pronounced among males, individuals with lower BMI, residents in Southern China, and during the warm season. These findings provide crucial evidence for developing air quality interventions that target the most harmful PM2.5 constituents to mitigate sleep-disordered breathing.
Building upon our previous findings linking total PM2.5 mass to increased OSA risk9, this study represents the first investigation, to our knowledge, designed to differentiate the effects of specific PM2.5 chemical constituents on OSA severity. Our results clearly identify OM and BC as the dominant contributors among the components assessed, exhibiting the strongest adverse associations with OSA-related outcomes. While prior evidence specifically linking PM2.5 constituents to sleep apnea is lacking, our findings are supported by growing literature on their cardiorespiratory effects11,13,14. For example, although findings are not entirely uniform, accumulating evidence consistently demonstrates often stronger and more robust associations of carbonaceous components (i.e., OM and BC) than secondary constituents (e.g., SO₄²−, NO₃− and NH₄⁺) with increased cardiovascular hospitalization or mortality11,14,15. The stronger effects of OM and BC may be biologically plausible considering their physicochemical characteristics and their role as carriers of reactive and toxic compounds. Specifically, carbonaceous particles originating from incomplete combustion can penetrate deeply into the lower airways, generate oxidative stress, trigger systemic inflammation, and induce autonomic dysfunction13,16,17,18. In addition, OM and BC possess large surface areas and strong adsorptive capacities, enabling them to act as vectors for other co-pollutants such as polycyclic aromatic hydrocarbons and heavy metals, further amplifying their toxicity. In contrast, secondary inorganic aerosols like SO₄²−, NO₃−, and NH₄⁺ are generally more hydrophilic and chemically inert, which may account for their weaker associations due to lower biological reactivity and limited ability to translocate across respiratory barriers. These findings underscore the need for targeted air pollution control strategies, with a particular emphasis on reducing combustion-related emissions to effectively mitigate the burden of sleep-disordered breathing.
We did not observe an apparent threshold below which no risk was detected in the E–R relationships between PM₂.₅ constituents and OSA severity. This underscores the necessity for stringent air quality regulations. Meanwhile, we observed that the slopes of the E–R curves progressively plateaued at higher concentrations. Several mechanisms may explain this attenuation. First, the sources of PM2.5 constituents may vary by concentration level. For instance, at lower concentrations, OM is more likely to originate from photochemical reactions involving volatile organic compounds, forming secondary organic aerosols19. In contrast, at higher concentrations, OM may primarily stem from incomplete combustion of coal, wood, or other biomass fuels that may differ in toxicity20. Second, physiological systems may exhibit biological saturation, wherein incremental increases in exposure no longer elicit proportional health responses, resulting in a flattened E–R slope. Third, behavioral adaptation may lead to exposure misclassification. Individuals exposed to high pollution levels may consciously reduce their exposure (e.g., by staying indoors), thereby weakening the observed associations. Lastly, the “harvesting” effect could also contribute21. Those most susceptible to PM-related OSA exacerbation may be affected at relatively low concentrations, leaving a less vulnerable subgroup at higher exposure levels, which could dampen the apparent population-level effect.
We observed that males and individuals with lower BMI were more vulnerable to the adverse effects of PM2.5 constituents on OSA exacerbation. The heightened susceptibility among males may be attributable to sex-specific differences in upper airway anatomy and physiology22, hormonal influences23, and the higher prevalence of lifestyles (e.g., smoking) that could impair airway defense mechanisms. Moreover, greater levels of outdoor activity among men may increase their exposure to ambient PM₂.₅ constituents. The greater vulnerability observed among individuals with lower BMI, while somewhat counterintuitive, is biologically plausible. One possible explanation is that in individuals with higher BMI, fat deposition around the upper airway structures may become the dominant driver of OSA pathophysiology24, potentially overshadowing the more subtle impacts of environmental exposures. In contrast, individuals with lower BMI may have relatively intact upper airway structures, making them more sensitive to additional environmental insults such as particulate matter exposure, thereby exhibiting more discernible effects.
We also found that associations between PM₂.₅ constituents and OSA severity were generally more evident during the warm season. Several factors likely contribute to this phenomenon. First, higher photochemical activity and ambient temperatures during the warm season can promote the generation of more biologically active secondary species and enhance the toxicity of primary components. For example, elevated temperatures can increase the fraction of oxidized OM, which has been shown to elicit stronger pulmonary inflammatory responses than its unoxidized counterparts25. Second, heat exposure may heighten physiological vulnerability by altering respiratory patterns, increasing metabolic demand, imposing cardiovascular strain, and promoting inflammation in the airway and alveolar endothelium26. These physiological changes may further amplify particle-induced hypopnea/apnea and impairment of oxygen diffusion27,28. Our findings support season-specific regulatory actions targeting air pollution, particularly in the context of climate change. We also observed substantial geographical heterogeneity in the associations between PM₂.₅ constituents and OSA severity. Overall, the risks of OSA exacerbation and AHI elevation were more pronounced in Southern China, which may partly reflect the region’s higher humidity and temperature, as well as potential differences in the toxicity profiles of PM₂.₅ chemical constituents across regions. Interestingly, NO₃− and NH₄⁺ exhibited stronger adverse effects on oxygen saturation in Northern China. This divergence suggests that different chemical components may influence OSA outcomes through distinct pathophysiological mechanisms, or that the specific sources and atmospheric processes generating NO₃− and NH₄⁺ in the North may be particularly detrimental to alveolar gas exchange.
Our study possesses several notable strengths. First, to our knowledge, this is the first investigation to evaluate the impact of PM2.5 constituents on OSA severity. Second, the study leverages an exceptionally large, nationwide database encompassing over six million person-days of objective, home-based sleep monitoring, enhancing the statistical power and generalizability of our findings. Third, the availability of intensively repeated measures of sleep outcomes enabled us to capture within-individual variations over time, thereby improving exposure assessment accuracy and minimizing random measurement error. Fourth, by applying a case time series approach, we accounted for confounders that are stable over time as well as those that vary, which enhanced the strength of our causal inferences. Our study also has several limitations. First, participants were limited to individuals who had purchased and used consumer-grade sleep monitoring devices, potentially introducing selection bias and limiting the generalizability of our findings to the broader population. Second, PM2.5 constituent data were available only at a daily resolution, preventing precise alignment with individual sleep periods. Future studies incorporating hourly constituent data could further enhance exposure assessment accuracy. Third, OSA risk and severity were estimated via smart devices rather than clinically validated polysomnography (PSG). Although the device employed in this study has been validated against PSG and home sleep apnea testing with high accuracy (>87% for moderate-to-severe OSA) and strong correlation (ICC > 0.72), we acknowledge that PPG-based monitoring in home settings may be subject to motion artifacts or signal noise compared to in-lab PSG. Nevertheless, such errors are expected to be random and unrelated to fluctuations in PM2.5 constituents. Consequently, any resulting misclassification would likely be non-differential, biasing the effect estimates toward the null. Fourth, residential location was determined at baseline. Although participants might have moved during the study period, the strict travel restrictions during the concurrent COVID-19 pandemic likely minimized inter-city relocation. Finally, our participants were inherently biased toward urban residents who tend to have greater access to smart wearable devices. As a result, our findings may better reflect urban populations, and their applicability to rural settings should be interpreted with caution.
In conclusion, leveraging over six million person-days of sleep monitoring from a nationwide smart-device-based cohort, this study provides the first evidence that PM2.5 constituents exert distinct effects on OSA severity. Our findings emphasize the significance of constituent-targeted particulate matter control strategies to mitigate the burden of sleep-disordered breathing effectively, with particular attention to carbonaceous components (i.e., OM and BC).
Methods
Study population
This study utilized data from the pre-mobile atrial fibrillation app (mAFA) II registry, which screens users for both atrial fibrillation and sleep apnea via photoplethysmography (PPG) technology embedded in Huawei smart devices. Adult users (aged ≥ 18 years) residing in mainland China and possessing compatible devices were recruited through the freely available mAFA application, accessible via the Huawei AppGallery. We focused on individuals at moderate-to-severe risk of OSA between December 16, 2019, and October 15, 2022, given that moderate-to-severe OSA is more strongly associated with daytime sleepiness and heightened risk of comorbidities compared to mild OSA. Individuals were deemed to have moderate-to-severe OSA risk if, during any 2-week interval with at least five valid monitoring days (defined as 4–12 h of nightly recording), 80% or more of daily AHI measurements exceeded 15 events per hour. To ensure adequate longitudinal data for robust statistical analysis, individuals with fewer than seven eligible monitoring days across the entire study period were excluded.
Ethical approval for the study was obtained from the Central Medical Ethics Committee of the Chinese PLA General Hospital (Approval No. S2017-105-02), and all procedures adhered to the principles outlined in the Declaration of Helsinki.
Health data acquisition
Sleep monitoring was conducted via the Huawei Smartwatch GT2, which is equipped with optical sensors for heart rate and peripheral oxygen saturation, enabling continuous overnight photoplethysmography (PPG) signal collection. Sleep apnea was assessed based on pulse rate variability and oxygen saturation indices derived from these PPG signals. Specifically, apnea and hypopnea events were first identified based on ≥90% and ≥30% reductions, respectively, in the PPG-derived respiratory waveform, which is reconstructed by the device’s proprietary algorithm using pulse rate variability and oxygen saturation signals. Next, the AHI was computed as the average number of such events occurring per hour of recorded sleep. OSA exacerbation was then defined as an AHI greater than 5 events per hour. The validity of PPG-based OSA screening using comparable wearable technology has been supported by previous studies demonstrating high sensitivity and specificity compared to the gold-standard PSG29. In a prior validation subset of our cohort (n = 1628), 92% of participants identified as being at moderate-to-severe risk for OSA through smartwatch-based screening were subsequently confirmed to have OSA by PSG testing conducted in hospital settings, supporting the accuracy and clinical utility of our screening approach9. Additionally, information on demographic characteristics, anthropometric measurements (height and weight), and medical history (e.g., arrhythmia, hypertension, diabetes, and ischemic heart disease) was collected at baseline via questionnaires.
Environmental data
Daily concentrations of PM2.5 and its major chemical constituents (OM, BC, SO42−, NO3−, NH4+) were obtained from the Tracking Air Pollution in China (TAP) dataset (http://tapdata.org.cn)30,31. The TAP dataset provides validated daily estimates (reported correlation coefficients: 0.67–0.80 vs. ground observations) with full national coverage at a 10 × 10 km resolution30. Meteorological variables, including daily mean temperature and relative humidity, were sourced from the fifth-generation European Center for Medium-Range Weather Forecasts atmospheric reanalysis (ERA5)32. Individual exposures were estimated by matching participants’ geocoded addresses to the nearest TAP and ERA5 grid cells. To reduce the influence of outliers, the top and bottom 1% of daily pollutant values were trimmed prior to analysis. Environmental exposures were evaluated for up to three lag days preceding each sleep monitoring day.
Statistical analyses
We utilized a novel case time series design, which partitions each individual’s follow-up period into daily segments, resulting in multiple case-specific time series33. By integrating the strengths of traditional time series and case-crossover approaches, this design inherently controls for time-invariant confounders and permits flexible adjustment for time-varying covariates33. Fixed effects regression models were applied to evaluate the associations of PM2.5 and its constituents with risk of OSA exacerbation, AHI and oxygen saturation. The models incorporated subject/year/month strata intercept to control for individual heterogeneity and yearly/monthly variations. Seasonal and long-term patterns were accounted for using natural splines of calendar day with 8 degrees of freedom per year. Meteorological confounding was addressed by including natural cubic splines of 3-day moving averages of temperature and humidity (6 degrees of freedom), alongside indicator variables for day of the week and public holidays. To evaluate potential lagged associations, we examined exposures on the sleep day and up to three preceding days. To explore potential nonlinear relationships, we additionally fitted E–R curves using natural cubic spline functions with three degrees of freedom.
We subsequently evaluated the independence of constituent-specific effects using two complementary modeling approaches16,34. First, constituent–PM2.5 adjustment models incorporated total PM2.5 mass as a covariate alongside every single constituent, where total mass acts as a surrogate for the remaining particulate mixture to help isolate constituent-specific associations. Second, to mitigate potential collinearity, we employed a constituent–residual modeling technique1. Each constituent was regressed on total PM2.5 mass, and2 the resulting residuals, representing constituent variability independent of total mass, were used as the exposure variables in the primary models to approximate the independent contribution of each constituent.
Furthermore, to identify potential modifiers, we performed subgroup analyses stratified by age (<45 vs. ≥45 years), sex, BMI, calculated as weight in kilograms divided by height in meters squared (kg/m²) and dichotomized at 24 kg/m2, and the presence of arrhythmia, hypertension, diabetes, or ischemic heart disease. We additionally stratified analyses by season (warm season: April–September; cold season: October–March) and by geographical region (Northern vs. Southern China, divided by the Qinling–Huaihe Line). The statistical significance of between-stratum difference was tested using the following formula35:
Here, Q1 and Q2 represent the estimates for the two subgroups, with Se1 and Se2 being their corresponding standard errors. Significance was determined by |Z| > 1.96 (P < 0.05), assuming a standard normal distribution for the Z-statistic.
All models were performed using R software (Version 4.4.1). Effect estimates for OSA exacerbation were presented as percentage changes in risk per IQR increase in PM2.5 and its constituents. For continuous outcomes (AHI and oxygen saturation), absolute changes were reported. P values < 0.05 (two-sided) were considered statistically significant.
Data availability
The exposure and health data used in this study are available on request via email from the corresponding authors.
References
Lévy, P. et al. Obstructive sleep apnoea syndrome. Nat. Rev. Dis. Prim. 1, 15015 (2015).
Benjafield, A. V. et al. Estimation of the global prevalence and burden of obstructive sleep apnoea: a literature-based analysis. Lancet Respir. Med. 7, 687–698 (2019).
Yeghiazarians, Y. et al. Obstructive sleep apnea and cardiovascular disease: a scientific statement from the American Heart Association. Circulation 144, e56–e67 (2021).
Reutrakul, S. & Mokhlesi, B. Obstructive sleep apnea and diabetes: a state of the art review. Chest 152, 1070–1086 (2017).
Kerner, N. A. & Roose, S. P. Obstructive sleep apnea is linked to depression and cognitive impairment: evidence and potential mechanisms. Am. J. Geriatr. Psychiatry 24, 496–508 (2016).
Luo, H., Zhang, Q., Niu, Y., Kan, H. & Chen, R. Fine particulate matter and cardiorespiratory health in China: a systematic review and meta-analysis of epidemiological studies. J. Environ. Sci. (China) 123, 306–316 (2023).
Bhatnagar, A. Cardiovascular effects of particulate air pollution. Annu. Rev. Med. 73, 393–406 (2022).
Lv, R. et al. Pathophysiological mechanisms and therapeutic approaches in obstructive sleep apnea syndrome. Signal Transduct. Target Ther. 8, 218 (2023).
Zhang, Q. et al. Air pollution may increase the sleep apnea severity: a nationwide analysis of smart device-based monitoring. Innov. (Camb.) 4, 100528 (2023).
van Donkelaar, A., Martin, R. V., Li, C. & Burnett, R. T. Regional estimates of chemical composition of fine particulate matter using a combined geoscience-statistical method with information from satellites, models, and monitors. Environ. Sci. Technol. 53, 2595–2611 (2019).
Jiang, Y. et al. Differential effects of fine particulate matter constituents on acute coronary syndrome onset. Nat. Commun. 15, 10848 (2024).
Sateia, M. J. International classification of sleep disorders-third edition: highlights and modifications. Chest 146, 1387–1394 (2014).
Wu, Y. et al. Associations of fine particulate matter and its constituents with airway inflammation, lung function, and buccal mucosa microbiota in children. Sci. Total Environ. 773, 145619 (2021).
Yang, Y. et al. Short-term and long-term exposures to fine particulate matter constituents and health: a systematic review and meta-analysis. Environ. Pollut. 247, 874–882 (2019).
Mo, S. et al. Short-term effects of fine particulate matter constituents on myocardial infarction death. J. Environ. Sci. (China) 133, 60–69 (2023).
Zhang, Q. et al. The effects of fine particulate matter constituents on exhaled nitric oxide and DNA methylation in the arginase-nitric oxide synthase pathway. Environ. Int. 131, 105019 (2019).
Hu, J. et al. Fine particulate matter constituents and heart rate variability: a panel study in Shanghai, China. Sci. Total Environ. 747, 141199 (2020).
Tellabati, A. et al. Acute exposure of mice to high-dose ultrafine carbon black decreases susceptibility to pneumococcal pneumonia. Part Fibre Toxicol. 7, 30 (2010).
Wang, Y. et al. Characterization of secondary organic aerosol tracers over Tianjin, North China during summer to autumn. ACS Earth Space Chem. 3, 2339–2352 (2019).
Makkonen, U. et al. Chemical composition and potential sources of PM2.5 in Hanoi. Atmos. Environ. 299, 119650 (2023).
Chen, R. et al. Fine particulate air pollution and daily mortality. A nationwide analysis in 272 Chinese cities. Am. J. Respir. Crit. Care Med. 196, 73–81 (2017).
Malhotra, A. et al. The male predisposition to pharyngeal collapse: importance of airway length. Am. J. Respir. Crit. Care Med. 166, 1388–1395 (2002).
Mirer, A. G. et al. Menopausal hormone therapy and sleep-disordered breathing: evidence for a healthy user bias. Ann. Epidemiol. 25, 779–784.e1 (2015).
Romero-Corral, A., Caples, S. M., Lopez-Jimenez, F. & Somers, V. K. Interactions between obesity and obstructive sleep apnea: implications for treatment. Chest 137, 711–719 (2010).
Chu, H. et al. Comparison of lung damage in mice exposed to black carbon particles and ozone-oxidized black carbon particles. Sci. Total Environ. 573, 303–312 (2016).
Çelebi Sözener, Z., Treffeisen, E. R., Özdel Öztürk, B. & Schneider, L. C. Global warming and implications for epithelial barrier disruption and respiratory and dermatologic allergic diseases. J. Allergy Clin. Immunol. 152, 1033–1046 (2023).
Li, A. et al. Higher ambient temperatures may worsen obstructive sleep apnea: a nationwide smartwatch-based analysis of 6.2 million person-days. Sci. Bull. (Beijing) 69, 2114–2121 (2024).
Qiu, H. et al. Real-time monitoring of the effects of personal temperature exposure on the blood oxygen saturation level in elderly people with and without chronic obstructive pulmonary disease: a panel study in Hong Kong. Environ. Sci. Technol. 54, 6869–6877 (2020).
Chen, Y. et al. A single-center validation of the accuracy of a photoplethysmography-based smartwatch for screening obstructive sleep apnea. Nat. Sci. Sleep. 13, 1533–1544 (2021).
Liu, S. et al. Tracking daily concentrations of PM2.5 chemical composition in China since 2000. Environ. Sci. Technol. 56, 16517–16527 (2022).
Geng, G. et al. Tracking air pollution in China: near real-time PM2.5 retrievals from multisource data fusion. Environ. Sci. Technol. 55, 12106–12115 (2021).
Hersbach, H. et al. The ERA5 global reanalysis. Q. J. R. Meteorol. Soc. 146, 1999–2049 (2020).
Gasparrini, A. The case time series design. Epidemiology 32, 829–837 (2021).
Zhang, Q. et al. The acute effects of fine particulate matter constituents on circulating inflammatory biomarkers in healthy adults. Sci. Total Environ. 707, 135989 (2020).
Altman, D. G. & Bland, J. M. Interaction revisited: the difference between two estimates. Br. Med. J. 326, 219 (2003).
Acknowledgments
This work was supported by National Key Research and Development Program of China (2022YFC2502800), the National Natural Science Foundation of China (82471130, 82173613, and 82373681), the Shanghai Municipal Health Commission (GWVI-11.2-XD18), and the Shanghai Hospital Development Center (SHDC2023CRS032).
Author information
Authors and Affiliations
Contributions
H.K. is the senior author. H.L, Data verification, Investigation, Formal analysis, Writing—Original Draft & Review & Editing. Z.Z., Data verification, Investigation, Formal analysis, Writing—Original Draft & Review & Editing. A.L., Data verification, Methodology, Writing—Review & Editing. Q.Z-., Data verification, Methodology, Writing—Review & Editing. X.Z., Data verification, Writing—Review & Editing. R.C., Data verification, Methodology, Writing—Review & Editing. H.K., Data verification, Supervision, Writing—Review & Editing. X.S., Conceptualization, Data verification, Supervision, Writing—Review & Editing. Y.G., Conceptualization, Data verification, Supervision, Writing—Review & Editing. Z.W., Conceptualization, Data verification, Funding acquisition, Supervision, Writing—Review & Editing. H.J., Conceptualization, Data verification, Funding acquisition, Supervision, Writing—Review & Editing. All authors have read and approved the final version of the paper. All authors have final responsibility for the decision to submit for publication.
Corresponding authors
Ethics declarations
Competing interests
Huixun Jia is the Guest Editor of BMC Ophthalmology. Huixun Jia was not involved in the journal’s review of, or decisions related to, this paper. The remaining authors declare no competing interests.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Luo, H., Zhang, Z., Li, A. et al. Differential effects of fine particulate matter constituents on obstructive sleep apnea severity: A nationwide analysis of smart device-based monitoring. npj Clean Air 2, 11 (2026). https://doi.org/10.1038/s44407-026-00050-z
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s44407-026-00050-z
