
Abstract
Cognitive impairment and symptoms of psychiatric disorders have been reported frequently as features of post-acute sequelae of SARS-CoV-2 infection. This study aims to investigate subjective memory complaints in COVID-19 survivors and determine if these are more strongly associated with objective cognitive impairment related to sequelae of SARS-CoV-2 infection or with symptoms of psychiatric conditions. A total of 608 COVID-19 survivors were evaluated in-person 6–11 months after hospitalization, with 377 patients assigned to a “no subjective memory complaint (SMC)” group and 231 patients assigned to an SMC group based on their Memory Complaint Scale scores. Follow-up evaluations included an objective cognitive battery and scale-based assessments of anxiety, depression, and post-traumatic stress symptoms. We found the perception of memory impairment in COVID-19 survivors to be more strongly associated to core symptoms of psychiatric conditions rather than to primary objective cognitive impairment. Univariate analysis indicated significant differences between the “no SMC” and SMC groups, both for the psychiatric symptom evaluations and for the cognitive evaluations (p < 0.05); however, the psychiatric symptoms all had large partial eta-squared values (ranging from 0.181 to 0.213), whereas the cognitive variables had small/medium partial eta-squared values (ranging from 0.002 to 0.024). Additionally, multiple regression analysis indicated that only female sex and depressive and post-traumatic stress symptoms were predictors of subjective memory complaints. These findings may help guide clinical evaluations for COVID-19 survivors presenting with memory complaints while also serving to expand our growing understanding of the relationship between COVID-19, subjective memory complaints, and the risk of cognitive decline.
Similar content being viewed by others

Introduction
It is now widely recognized that COVID-19 can have lasting symptoms persisting months or years after recovery [1,2,3,4,5]. These symptoms, known as post-acute sequelae of SARS-CoV-2 infection (PASC), are heterogenous and may appear through direct multi-organ injury, inflammation/immune dysregulation, gut dysbiosis, and viral persistence [5]. Regarding central nervous system manifestations, both symptoms characterizing psychiatric disorders (e.g. depression, anxiety, and post-traumatic stress disorder) and cognitive impairment have been reported frequently as features of PASC [2, 4,5,6]. Cognitive symptoms themselves might be both transitory and persistent [7], with the latter being further explained due to a high positivity of Alzheimer’s disease (AD) biomarkers indicative of brain injury by SARS-CoV-2 [8].
Core symptoms of anxiety and depression may emerge in elders as prodromal features of AD, and depressive and anxiety disorders across the life cycle are seen as risk factors for dementia in late life [9, 10]. Self-reported subjective memory complaints (SMC), which are common in elderly populations, are clinically relevant as they may be predictive of the future development of dementia and specifically AD [11,12,13,14]. However, several investigations have shown that SMC may also be a corollary of psychiatric disorders, such as anxiety and depression, that do not necessarily emerge as prodromal manifestations of future dementia [15]. For instance, a three-year follow-up study on SMC in patients between 35 and 75 years old found that, while the risk of patients with SMC developing dementia within three years was low, they exhibited higher rates of psychosocial stress, leading to the proposal that psychosocial stress and anxiety were factors causing SMC in cognitively normal individuals [12, 15]. Similarly, a separate two-year follow-up study showed that individuals with SMC were more likely to report characteristic symptoms of depression and anxiety than individuals without any objective memory deficits [16]. A systematic review and meta-analysis from 2022 demonstrated a significant relationship between SMC and impaired executive performance, which is relevant to the notion that SMC may predict dementia; however, the authors also noted a significant influence of depression on the level of cognitive complaints and concluded that psychiatric conditions could be considered a relevant comorbidity for patients presenting with subjective memory complaints [17]. Finally, a longitudinal twin-cohort study found that, from 56 years of age onwards, SMC correlated more strongly with depressive symptoms than with objective memory deficits; moreover, genetic influences for SMC and psychiatric features were significantly related to each other but not to genetic risk factors for AD [18].
Beyond AD, studies have investigated the relationships between cognitive deficits and psychiatric symptoms in other neurodegenerative disorders. In multiple sclerosis (MS), cognitive impairment and depression are present at a higher rate than in the general population. A systematic review from 2015 found depression and anxiety to be the most prevalent comorbidities in MS [19], and depressive symptoms in MS patients have been associated with worse objective cognitive outcomes compared to patients who do not present with any symptoms of depression [20]. Furthermore, worsening mood has been related to worsened executive control and vice versa [21]. SMC and objective cognitive deficits can also both present as features associated with human immunodeficiency virus (HIV) infection; in the condition known as HIV-associated neurocognitive disorder (HAND), common deficits are seen in the domains of concentration, attention, and memory [22]. Studies have shown that SMC in adults infected with HIV are significantly correlated with depressive symptoms, and depression and apathy are the most frequent psychiatric comorbidities of HAND [23, 24].
Since COVID-19 has been suggested to be a potential risk factor for dementia as a whole and specifically AD [25], it is highly relevant to evaluate the relationship between SMC, objective cognitive deficits, and core manifestations of psychiatric disorders in the same sample of COVID-19 survivors examined prospectively in the long term after the acute disease. Previous studies on the topic have utilized small samples of patients with variable levels of acute COVID-19 severity and have reported conflicting findings. A study conducted in Spain evaluated 80 intensive care unit (ICU) COVID-19 survivors one year after hospitalization and found that 30% of them exhibited objective cognitive impairment. However, there were no significant differences in SMC between patients with and without objective cognitive deficits, suggesting SMC may not be strongly related to objective cognitive impairment in PASC [26]. Another study with 63 patients with SMC in Spain after an average of 187 days following COVID-19 of varying levels of severity found frequent cognitive deficits at objective testing; there was no significant relationship between anxiety and cognitive impairment and only a weak relationship between depression and processing speed [27]. Furthermore, few studies of PASC documented cognitive deficits using objective standardized tests conducted during in-person assessments of relatively modest samples; the vast majority of large-scale investigations used questionnaires and scales evaluating self-reported, subjective accounts of cognitive inefficiency, often referred to as brain fog [4, 28, 29]. A recent study by Gonçalves et al. evaluated a large sample of 1105 individuals and proposed the possibility of self-limiting and persistent cognitive deficits in PASC; however, the follow-up assessment was based solely on telephone interviews with the patient (10-point cognitive screener (10-CS)) or the caregiver (AD8 dementia screening interview) [7]. Conversely, there is one notable study conducted by Muschel et al. [30] which used the Patient Assessment of Own Functioning Inventory (PAOFI) to assess the presence of cognitive complaints approximately seven months after acute SARS-CoV-2 infection in a sample of 74 participants who also underwent in-person psychiatric symptom assessments and objective cognitive testing. The authors found that the severity of acute COVID-19 symptoms, depression symptoms at the follow-up assessment, and objective deficits in attention and psychomotor processing speed were all independent predictors of cognitive complaints in logistic regression; thus, they concluded that cognitive complaints as sequelae of COVID-19 are likely related both to impaired objective cognitive functioning and depression severity [30].
Understanding how persistent subjective memory complaints in COVID-19 patients relate or not to objective cognitive impairment and core symptoms of psychiatric disorders can assist in guiding future clinical evaluations of elderly populations in routine care. Using subjective and objective data obtained from a large sample of COVID-19 survivors evaluated in-person 6–11 months after hospitalization, the goals of the present study were (1) to document the frequency of subjective memory complaints in the overall sample and investigate whether they were significantly associated with demographic, comorbidity, and acute COVID-19 related variables; (2) to explore if objective cognitive performance differed between COVID-19 survivors presenting with and without subjective memory complaints; and (3) to determine if subjective memory complaints in COVID-19 survivors were more strongly associated with PASC-related objective cognitive impairment or with core symptoms of psychiatric disorders.
Methods
Study design and participants
This study was conducted at the Hospital das Clínicas da Faculdade de Medicina da Universidade de São Paulo (HCFMUSP), the largest public academic medical center in Latin America, and is part of the HCFMUSP PASC Initiative, which is a prospective, multidisciplinary cohort study of severe COVID-19 patients after hospital discharge.
During the first COVID-19 wave in São Paulo, Brazil (between March and August 2020), HCFMUSP’s Central Institute was converted into a specialized COVID-19 inpatient facility with a total of 900 beds, including 300 beds in intensive care units [31, 32]. During that period, 3753 patients over the age of 18 were admitted to HCFMUSP with suspected SARS-CoV-2 infection. Of those patients, 3009 were classified as confirmed cases of COVID-19, defined as either (a) positive reverse-transcriptase polymerase chain reaction (RT-PCR) for SARS-CoV-2 on swab from nasopharyngeal and/or oropharyngeal samples (collected at admission with a minimum of 3 days of symptoms and if negative, repeated after 48 h) [33]; or (b) positive testing by chemiluminescent immunoassays to detect serum antibodies [34], performed for highly suspect cases with at least two negative RT-PCR samples after seven days of symptom onset or in subjects with high clinical suspicion for whom an RT-PCR test was not available up to day 10 of symptom onset. From these 3009 confirmed COVID-19 cases, 1957 survived hospitalization and were discharged.
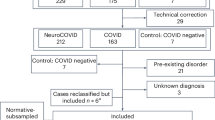
All survivors from the above sample were consecutively invited for an in-person follow-up visit that occurred 6–11 months after their hospital admission. Patients with a previous diagnosis of dementia, postpartum/pregnant patients, patients living in nursing homes or long-term care facilities, and patients with insufficient physical mobility to leave home were excluded. A total of 749 individuals accepted the invitation and were included in the post-COVID-19 cohort for the study of PASC. Further details on the methodology and the post-COVID-19 cohort exclusion criteria can be found in Busatto et al. [35], and Ferreira et al. [35, 36]. For the present study, we specifically excluded subjects who were non-native speakers of Brazilian Portuguese, as well as individuals who presented speech or language complaints, a missing evaluation of subjective memory complaints, or missing data on all psychiatric symptom scales or all objective cognitive tests.
This cohort integrates the results of several research projects led by health specialist teams within HCFMUSP. All projects were approved by the Ethics Committee at HCFMUSP (CAPPesq-HC) (approval numbers 4.270.242, 4.502.334, 4.524.031, 4.302.745, and 4.391.560) and registered at the Brazilian Registry of Clinical Trials (ReBEC). Participants in the post-COVID-19 cohort provided signed informed consent. Taking into account the long-lasting status of COVID-19 pandemics in São Paulo at the time of data collection for the study and in order to preserve the safety and social distancing of subjects and their relatives, subjects were asked to arrive using private transportation, with expenses covered by the research program [35].
Data collection and tests
An institutional database of hospital inpatient information based on patient health records provided data from the initial acute COVID-19 hospitalization including duration of admission, days in the ICU, pulmonary function, comorbidities or other previous diagnoses, and demographics (age and sex). Data on comorbidities were used to calculate the Charlson Comorbidity Index (CCI) [37]. Severity of events during hospitalization (i.e. use of mechanical ventilation, dialysis) was assessed using the WHO Clinical Progression Scale [38].
At follow-up, subjective memory complaints were assessed using the 7-item Memory Complaint Scale (MCS), patient version [12]. This self-report instrument assesses the perception of patients as to how memory difficulties affect their daily behaviors and functioning. Each question is rated with a three-level grade of increasing intensity, with total scores ranging from 0 to 14. Subjects are classified as follows: absence of SMC (0–2), mild SMC (3–6), moderate SMC (7–10), or severe SMC (11–14) [12]. The original, Brazilian version of the scale has a Cronbach’s alpha coefficient of 0.850 indicating good internal consistency, and item-total correlations higher than 0.512 for its seven items [12]. Similar levels of internal consistency have been obtained for the scale when used in studies conducted in other countries [39, 40]. The sample was split into two groups based on their total MCS scores; patients with total MCS scores between 0–6 were categorized as having no/mild subjective memory complaints (“no SMC” group), and patients with MCS scores between 7–14 made up the moderate/severe subjective memory complaint group (SMC group). In order to allow the identification of any patients who presented longstanding memory complaints, one question was added to the MCS (“How is your memory compared to just before the pandemic?”). This question was scored as 0 (same or better), 1 (somewhat worse), or 2 (much worse), similarly to all MCS items. Subjects classified as belonging to the SMC group who answered this question stating that their memory remained the same or improved after COVID-19 were categorized as belonging to a SMC subgroup with longstanding memory inefficiency (“longstanding SMC” subgroup), while SMC subjects with scores of 1 or 2 to this question were included in the “recent SMC” subgroup.
Follow-up evaluations of symptoms of psychiatric disorders included the Hospital Anxiety and Depression Scale (HADS) and the Post-Traumatic Stress Disorder Checklist (PCL-C); scores on these checklists were evaluated as continuous variables.
The objective cognitive battery at the follow-up visit consisted of the subtests of Temporal and Spatial Orientation of the Mini-Mental State Evaluation (MMSE) [41], Trail Making Test A (TMT-A), and the Consortium to Establish a Registry for Alzheimer’s Disease (CERAD) Verbal Fluency Test (VFT) and Word List Memory Task (WL) for delayed memory recall [42,43,44,45]. The TMT-A measured visual attention and processing speed, and we used the completion time in seconds as the outcome measure. The VFT assessed verbal production, semantic memory, and language [43, 44]. We measured the number of correct animals listed in a minute, ignoring for our analysis any mistakes or repetitions. The WL assessed ability to learn and remember verbal information [43, 44]. The number of correct words over the delayed recall trial was utilized in our study. A detailed list of these evaluations with descriptions can be found in Damiano et al. [6].
Additional variables assessed during the follow-up visit included body mass index (BMI), socio-economic status (SES) using the Brazilian Economic Classification Criteria [46], level of education, and self-reported race using the Brazilian Institute of Geography and Statistics criteria [47]. The Post-COVID-19 Functional Status (PCFS) scale [48, 49] was also used, to assess the impact of COVID-19 symptoms on the current functional status of patients and their daily life activities. This simple, ordinal scale measures the degree of self-reported functional limitations experienced by individuals after a COVID-19 infection. The scale’s primary question is, “How much are you currently affected in your everyday life by COVID-19?” [48, 49]. The self-reported responses are categorized into five increasing grades. Grade 0 indicates no limitations in everyday life and no symptoms, pain, depression, or anxiety related to the infection; grade 4 represents severe limitations, where individuals are unable to take care of themselves and are dependent on nursing care or assistance from another person due to symptoms, pain, depression, or anxiety [48, 49].
Statistical analysis
Statistical analyses were performed using IBM SPSS Statistics v29.0.1.0.
For descriptive analyses, we calculated the frequency and percentage for nominal variables, and mean, standard deviation, and minimum and maximum values for continuous variables.
To compare the demographics of the two groups (SMC and “no SMC”), chi-square tests were performed for the variables sex, race, socioeconomic class, and education level, and two-tailed independent samples T-tests were performed on age and BMI. The confidence interval was set at 95%, and statistical significance was established at an uncorrected p-value < 0.05.
Comparisons of psychiatric symptoms and objective cognitive variables between the two groups were conducted using an ANCOVA model with Bonferroni correction (at a p-value of 0.05), including age, sex and education as covariates. Psychiatric symptoms evaluated included HAD total score for Anxiety, HAD total score for Depression, and PCL-C PTSD total scores. The cognitive variables included scores for the MMSE total score for Temporal Orientation, MMSE total score for Spatial Orientation, TMT-A completion time, and number of correct answers on both the VFT and WL.
A multiple logistic regression analysis was performed to assess for potential predictors of MCS scores for the overall sample combining the two groups. Using the backward stepwise selection method, we included as possible predictors two measures of severity of the acute disease—the WHO Clinical Progression Scale and length of inpatient stay—as well as any psychiatric symptom variables and objective cognitive performance variables that showed significant between-group differences on the ANCOVAs described in the paragraph above. Age, sex, and education level were added as forced variables in the model.
We also computed the number of patients in the “no SMC” and SMC groups presenting TMT-A and VFT scores outside of the normal range, based on whether their ratings were lower than the mean values for the Brazilian population across distinct age ranges. Descriptive statistics (frequencies and percentages) and chi-square tests were calculated to test for any significant difference in the frequency of subjects with deficient performance between the “no SMC” group and the SMC group. The cutoff test values used for classifying individual performances as deficient were defined based on the mean values extracted from normative data presented by Zimmermann et al. [50] for the TMT-A in a study with 313 healthy individuals aged from 19 to 75 years [50] and by Brucki et al. [51] for VFT in a study conducted with 336 healthy individuals aged from 15 to 91 years [51]. We did not have access to normative WL data for the Brazilian population; however, due to the critical relevance of this memory task for the current study, we conducted analyses to compare the frequency of patients in the “no SMC” and SMC groups presenting scores outside of the normal range using the mean values from the normative data from two other South American countries (see supplementary material).
Finally, to allow an investigation of the patients who reported longstanding memory complaints in greater detail, patients in the “longstanding SMC” subgroup were individually matched with patients in the remaining SMC group (“recent SMC” subgroup) and patients in the “no SMC” group. The matching was based on sex, education level, and age, with priority decreasing in that order. All of the individuals were matched exactly for sex. For mismatched education levels, the patient with the closest education level was selected. For age range differences greater than ±2 years, two individuals, one older and one younger, were matched to the “longstanding SMC” patient. This was done to maintain a similar mean age between samples. To check for normality in the data, a Shapiro-Wilk test was used. In case the data distribution was not normative, a Kruskal-Wallis test for multiple comparisons was conducted to check for significant differences in age between the “longstanding SMC,” “recent SMC,” and “no SMC” subgroups. The same psychiatric symptom measures and cognitive test variables listed above for the ANCOVA were used in the Kruskal-Wallis. A post-hoc analysis for pairwise comparisons was conducted for any significant differences found. For education level, Fisher’s exact test was used to check for significant differences among the three groups.
Results
Demographic and clinical characteristics of the sample
From the 749 subjects included in the total post-COVID-19 cohort, 608 patients fit additional eligibility criteria specified for the present study. In this final sample of 608 subjects, 377 patients were assigned to the “no SMC” group, and 231 patients were assigned to the SMC group based on their scores on the MCS.
Table 1 summarizes the demographics and clinical characteristics of the two groups. There were no significant between-group differences regarding the interval between hospital discharge and the follow-up assessment. No significant between-group differences were found for age, BMI, race, or education level. Overall, the sample had a significantly higher number of men than women, but there was a significantly higher frequency of women reporting subjective memory complaints (Table 1). For SES, differences between the two groups were seen primarily in the extremes; the “no SMC” group skewed towards higher SES, while the SMC group was skewed towards lower SES. Between-group differences in scores on the CCI and the WHO Clinical Progression Scale were non-significant. For the length of inpatient stay during acute COVID-19, the “no SMC” group had a significantly higher mean number of days and a wider range with a higher maximum (Table 1). Finally, regarding functional status at the time of the follow-up evaluation, there were significant between-group differences in PCFS scores, with responses of the “no SMC” group skewed towards lower functional impact compared to the SMC group’s responses (Table 1).
Comparison of psychiatric symptom ratings and objective cognitive scores between subjects with and without subjective memory complaints
Table 2 shows the results of the between-group comparisons for the eight psychiatric symptoms and objective cognitive variables. With these eight variables, statistical significance for the ANCOVAs with Bonferroni correction was calculated at p < 0.00625. Significant differences between the “no SMC” and SMC groups were found for the psychiatric symptom evaluations HAD Anxiety, HAD Depression, PCL-C, as well as for the cognitive evaluations MMSE Spatial Orientation, VFT, and WL (Table 2). After applying Bonferroni correction, all these variables retained statistical significance except for the VFT test, which remained significant at trend level (p = 0.07). The psychiatric symptoms all had large partial eta-squared values, whereas the cognitive variables had small/medium partial eta-squared values. In addition, the means for all three significant cognitive variables were close in value between the “no SMC” and SMC groups.
Multiple regression model for the prediction of subjective memory complaints
Table 3 presents the results of the multiple logistic regression analysis evaluating potential predictors of subjective memory complaints in the overall sample. This analysis included the six variables identified in the above ANCOVAs as candidates for the multivariate model (HAD total Depression score, HAD total Anxiety score, PCL-C total score, MMSE total Spatial Orientation score, and number of correct answers for both VFT and WL). The multivariate fitting resulted in one model containing, in order of decreasing p-value (increasing significance), the following predictive variables for subjective memory complaint: sex, HAD total Depression score, and PCL-C total score. There were no differential effects for the WHO Clinical Progression Scale (omitted in the final model), total inpatient days, MMSE total Spatial Orientation score, VFT correct answers, WL correct answers, HAD total Anxiety score, age, and education level.
Normative comparisons of objective cognitive tests
Table 4 presents the frequencies of subjects in the two groups who presented values within or outside of the normal range for TMT-A and VFT scores, using the standardized norms for the Brazilian population across distinct age ranges. For the TMT-A, both the “no SMC” and SMC groups had a higher proportion of individuals falling outside of normative values than within. For the VFT, there was a higher proportion of individuals within normative values for both groups. For both cognitive tests, there was a significantly higher frequency of subjects outside the normative data in the SMC group (Table 4). It is worth noting, however, as a whole, our entire sample was more likely to present results outside of normative values than within for those two tests. In addition, out of all the cognitive tests, the TMT-A had the most missing values (5%) and outliers (5.7%), defined as any value outside of 1.5 interquartile range (Table 2). Results of the analyses conducted for WL ratings are presented as supplementary material.
Longstanding SMC
Within the 231 patients in the SMC group, 24 patients (3.94% of the overall sample) were also classified as belonging to the “longstanding SMC” subgroup. These subjects were individually matched with a subgroup of 26 subjects from the remaining SMC group (“recent SMC” subgroup) and a subgroup of 26 subjects from the “no SMC” group (Table 5). According to the Shapiro-Wilk test, most variables were found to have non-normal distributions in the three subgroups. The Kruskal-Wallis for matching confirmed there were no significant differences in age among the “longstanding SMC” subgroup, “recent SMC” subgroup, and “no SMC” subgroup (p = 0.998). The Fisher’s exact test, confirming our matching for educational level, also found no significant differences among subgroups (p = 0.759). Table 5 demonstrates that there were significant differences among the three subgroups in all of the psychiatric symptom measures (HAD total Anxiety score, HAD total Depression score, PCL-C total score), with the “longstanding SMC” subgroup having intermediate scores between the two other subgroups. The post-hoc analysis for pairwise comparisons with Bonferroni correction revealed that for these three tests, the difference was found to be between the “recent SMC” subgroup and the “no SMC” subgroups. TMT-A completion time was the only objective cognitive measure with a significant difference between subgroups, which was found to be between the “longstanding SMC” and the “recent SMC” subgroups.
Discussion
This study reports the findings of a thorough evaluation of SMC experienced by COVID-19 survivors assessed 6–11 months after hospitalization, investigating their relationship with both objective cognitive memory impairments and core symptoms of psychiatric conditions. Differently from most previous studies of COVID-19, we used a standardized metric of SMC (based on scores on the MCS, previously validated for the Brazilian population) [12]. The main findings are as follow: (1) although there were significant differences in objective cognitive performance between COVID-19 survivors with and without SMC, the influence of objective cognitive impairment on SMC was found to be minor; (2) the psychiatric symptoms anxiety, depression, and PTSD were major differentiating factors in subjects with SMC versus individuals with no SMC; (3) in a multiple logistic regression model for the overall sample, female sex, symptoms of depression (depressive symptoms measured by the HAD total Depression score), and PTSD (as measured by the PCL-C) were the only significant predictors of SMC; and (4) similarly to previous findings on psychiatric and cognitive morbidity in PASC [6], indices of clinical severity of acute COVID-19 were not significant predictors of the development of SMC (as a feature of PASC).
As we questioned individuals as to whether SMC were present before the onset of COVID-19, we were able to ascertain that these complaints emerged in most cases following the SARS-CoV-2 infection and hospitalization. Our cohort presented a very high percentage of patients with SMC, with 38% of our 608 patients presenting with memory complaints 6 to 11 months after hospital discharge. The results regarding the frequency of subjective cognitive complaints in COVID-19 survivors corroborate the findings of previous investigations [5, 30, 52,53,54,55,56,57].
The univariate ANCOVA comparisons of core symptoms of psychiatric disorders and objective cognitive tests scores between the SMC and “no SMC” groups showed significant differences for both types of measures after Bonferroni correction, including all psychiatric symptom scales and two objective cognitive tests (namely word list recall and spatial orientation, with verbal fluency retaining trend significance). However, the differences in psychiatric symptom measures all had large partial eta-squared (η2) values while the differences in objective cognitive measures had small/medium partial eta-squared values. Thus, although our cohort did exhibit objective signs of cognitive impairment, the subjective complaint of memory inefficiency itself was found to be more significantly related to core symptoms of psychiatric disorders. In addition, the mean values of the three objective cognitive variables that showed significant differences were close between the “no SMC” and SMC groups, which indicates that scores on the objective cognitive tests differed less between the groups than scores on psychiatric symptom scales. Moreover, the multiple logistic regression evaluating potential predictors of subjective memory complaints in the overall sample showed only depression, PTSD, and sex to be significant predictive variables. These pieces of evidence, obtained in a large sample, indicate that the perception of memory impairment in COVID-19 survivors is detectable mostly in the context of psychiatric symptoms rather than reflecting primary objective cognitive impairment not necessarily related to depression, anxiety, or PTSD. Finally, the significantly higher PCFS scale scores in the SMC group indicate that patients presenting subjective memory complaints in our study had a greater deleterious impact of COVID-19 on their long-term functional status and daily life activities.
The findings of the present study are consistent with previous investigations on COVID-19. In the study by Muschel et al. [30] using the standardized PAOFI assessment to characterize cognitive complaints in COVID-19 patients after 7 months, significant correlations were stronger between cognitive complaints and subjective measures of mental distress, and weaker between cognitive complaints and objective neuropsychologic test performance [30]. A 6 month follow-up study conducted by Pihlaja et al. [57] with COVID-19 patients who presented different degrees of care needs during acute disease (ICU, hospital ward, or home-isolation) showed that depressive and PTSD symptoms at follow-up were equally reported by all three groups and were significantly associated with SMC but not with performance on objective cognitive assessments [57]. Finally, a 2024 prospective observational study of a national cohort of Norwegian COVID-19 patients who demanded ICU care during acute disease described similar findings, as patients who presented depression at 12 months following ICU admission were more likely to report disproportionately high SMC relative to the severity of deficits detected by objective cognitive testing [58].
The findings presented herein are also consistent with the results of previous studies that have investigated SMC in other diseases. For instance, cognitive complaints in patients with HIV infection are significantly correlated with depressive symptoms [23], and a study of 889 HIV-positive adults using multivariable regression models found psychiatric symptoms of depression, anxiety, and PTSD to be significant predictors of subjective cognitive complaints [59]. Although cognitive complaints have been found to correlate significantly with both depressive symptoms and measures of objective cognitive impairment in HIV-positive subjects, multiple regression analyses have shown that symptoms of depression account for the majority of variance in the cognitive complaints [23].
We found a substantially large proportion of women in the SMC group relative to the “no SMC” group. Moreover, aside from HAD total Depression score and PCL-C score, the multiple regression analysis found female sex to be the only other significant predictor of SMC. Previous studies with COVID-19 survivors found that younger women were more likely to present subjective cognitive/psychiatric symptom complaints such as memory loss, brain fog, anxiety, depression, and PTSD [26, 29, 52, 53, 60,61,62,63]. Our findings of increased subjective memory complaints in women reinforce the view that SMC in PASC is more strongly related to psychiatric symptoms than reflective of the perception of individuals of primary objective cognitive impairment developing after COVID-19.
In addition, we found no significant associations of SMC with either the CCI or severity indices of the acute SARS-CoV-2 infection and events during hospitalization. Although the length of inpatient stay was significantly different between the “no SMC” and SMC groups, the multiple regression model found no predictive relationship for the length of inpatient stay with the presentation of SMC. Contrary to expectations, the SMC group had an actually shorter mean number of inpatient days relative to the “no SMC” group. These results reinforce the view that perceived memory impairment is not necessarily reflective of objective cognitive impairment in PASC. Given that prior research has shown hospitalization can cause cognitive impairment, if memory complaints were prominently related to primary objective cognitive deficits, one would expect impairment to be more likely related to a longer inpatient stay [64]. This is consistent with previous findings that memory complaints are not related to severity of the acute SARS-CoV-2 infection [27, 57, 62, 65]. In contrast, Muschel et al. [30] found the severity of acute COVID-19 symptoms to be the most significant independent predictor of cognitive complaints after 7 months; however, the severity of current depressive symptoms was also a significant predictor for cognitive complaints at follow-up [30].
The presence of significantly (albeit modestly) worse performance in three objective cognitive measures in the SMC group relative to the “no SMC” group (word list recall, verbal fluency, and spatial orientation) could be secondary to the greater severity of core psychiatric symptoms in the SMC group. Previous studies have shown cognitive dysfunction can be present during acute episodes of major depressive disorder and persist at a moderate degree through remission. Anxiety has also been shown to be associated with memory and executive dysfunction [66]. Similarly, systematic reviews have found that PTSD is associated with cognitive impairment, with a positive correlation between the severity of PTSD symptoms and degree of cognitive impairment, and a prospective cohort study of 12270 middle-aged women found PTSD to be associated with accelerated cognitive decline [67, 68]. However, our results do not rule out the possibility that the presence of objective cognitive deficits in PASC cases could represent early signs of neurodegeneration; the presence of associated symptoms of depression or anxiety in some of those individuals could be seen as prodromes of dementia [9, 10]. Thus, the interplay between the emergence of psychiatric symptoms in PASC and the risk of long-term cognitive decline may be possibly complex, especially in elderly individuals. Prospective longitudinal follow-up evaluations of samples like ours are mandatory to further investigate this issue. Ideally, these longitudinal studies should include not only objective cognitive evaluations and symptom assessment schedules, but also measurements of biomarkers most commonly related to psychiatric syndromes (e.g. markers of inflammatory pathways) and the biological diagnosis of AD [62, 69].
The identification of a small proportion of “longstanding SMC” patients in our sample (3.94% of the overall sample) allowed us to run comparisons of this subgroup against individually matched subgroups of “recent SMC” (i.e., memory complaints after COVID-19) and “no SMC.” Such comparisons are relevant given previous findings that trait-like dimensions of SMC are strongly associated with affect-related measures, including depression, anxiety and neuroticism [18]. It is also important to note that, in an interim analysis of a large proportion of patients included in the present study (n = 425), we found a small number of patients who reported symptoms consistent with major psychiatric disorders for one year or longer prior to our assessment (as investigated with the Clinical Interview Schedule – Revised), including 3.31% of subjects with moderate to severe depression and 5.98% with generalized anxiety disorder [6]. However, our three-subgroup comparisons showed a significant increase in all psychiatric symptom measures (HAD total Anxiety score, HAD total Depression score, PCL-C total score) only in the “recent SMC” subgroup (but not in the “longstanding SMC” subgroup) relative to the “no SMC” subgroup. These results suggest that the association of SMC and psychiatric manifestations in our study was not due to an excess of subjects with trait-like SMC (who might present prominent psychiatric symptoms). This provides additional evidence highlighting the relationship between incident memory complaints and psychiatric symptoms emerging after hospitalization due to COVID-19.
Our study adds to growing literature on the relationship between COVID-19 and persistent subjective memory complaints and helps to broaden understanding of how long COVID patients who present with memory complaints should be evaluated in clinical settings. The findings suggest that memory complaints in PASC patients who survived after hospitalization due to COVID-19 are strongly related to psychiatric symptom complaints. For such COVID-19 survivors who seek care due to memory complaints, a careful psychiatric evaluation should be considered a priority, guiding the implementation of treatment when appropriate. One important strength of our study is its large sample size, affording adequate power. Previous studies on the topic have utilized small sample sizes, often of less than 100 participants [26, 27]. It should also be noted that there were no significant differences in our sample between the SMC and “no SMC” groups regarding age and education; this indicates that these potentially confounding factors of cognitive performance were controlled for, with the two groups likely presenting similar levels of cognitive reserve.
One particularly relevant limitation of the present study regards to the use of raw data for comparisons of objective cognitive variables rather than to age-standardized Z-scores, as the latter would have allowed us to take into account the non-pathological influence of aging on cognitive performance in young, adult and elderly persons. However, we were not able to collect raw cognitive scores from a non-COVID-19 healthy control group with a wide age range that could be used to parameters for the generation of age-standardized Z-scores. Therefore, we cannot ascertain the degree to which the overall sample of the present study should be considered cognitively impaired in objective terms. As an alternative, we classified the cognitive performance of subjects in both the SMC and “no SMC” groups in comparison to mean normative test data for the Brazilian population across different age ranges, and this indicated that a considerable proportion of our patients presented with values outside the normal range of cognition in both the “no SMC” and SMC groups [50, 51]. However, Brazilian normative data was available only for the TMT-A and VFT scores and not for the other cognitive tests, including the key domain of episodic memory (as assessed by the WL test). In order to conduct similar analyses for the WL test, we had to use normative values based on other urban South American populations (see the supplementary material). Nevertheless, it is important to stress that the comparison of our results with normative data, in order to ascertain the frequency and severity of cognitive impairment following COVID-19, was not the primary focus of the current study. Instead, we primarily aimed to investigate whether memory complaints within a sample of patients who survived hospitalization due to moderate to severe COVID-19 would be most significantly predicted by objective cognitive performance or core symptoms of psychiatric conditions assessed concurrently in the same subjects. For the latter purpose, we honestly believe that it is valid to use raw cognitive data, taking into account the effects of age, sex, and education as we did both in the univariate ANCOVA comparisons reported in Table 2 and in the logistic regression analysis reported in Table 3.
Several other limitations of the present study should be acknowledged. First, the in-person data collection was conducted as part of a comprehensive multidisciplinary evaluation [35]; this imposed time constraints on the objective cognitive battery, and relevant aspects such as executive functioning were not thoroughly evaluated. However, we did manage to objectively assess the key domain of episodic memory in a large sample of PASC patients. Second, the participants did not undergo either a comprehensive psychiatric evaluation with standardized instruments or an assessment with the cognitive battery prior to COVID-19 infection, and we do not therefore know the baseline cognitive performance of our sample. While we formally excluded patients with an existing previous diagnosis of dementia, we cannot rule out the presence of undiagnosed elderly patients in the early stages of dementia. Recent studies have shown that patients with an established dementia diagnosis (particularly Alzheimer’s disease) have a higher risk of COVID-19 infection with more severe presentations and higher rates of hospitalization and mortality [70]. One positive aspect is that speech complaints were included as part of our exclusion criteria to supplement the exclusion of patients with dementia, since some studies have shown speech complaints may be one of the first signs of dementia (e.g. a retrospective review on 80 patients with apraxia of speech due to degenerative neurological disease found that speech-language difficulties were the first symptoms in 80% of patients, and 49% and 50% of the patients presented with aphasia and dysarthria, respectively) [71]. Third, we did not have complete data for each of the 608 patients in our study, and there were more missing data for the objective cognitive tests than for the other measures. Fourth, we did not assess an additional group of COVID-19 patients who were not hospitalized; therefore, we cannot ascertain the degree to which the PASC manifestations reported herein were related to COVID-19 severity and events during the hospitalization. Previous studies have found evidence of an association between hospitalization (both critical and noncritical care) and the development of cognitive decline [64]. Finally, while our study had a large sample size, the groups were comprised of patients from a single hospital site, so the results may not be generalizable or wholly representative of a wider population.
Conclusion
In conclusion, using subjective and objective data obtained from a large sample of COVID-19 survivors evaluated in-person 6–11 months after hospitalization, we found that the perception of memory impairment in COVID-19 survivors is more strongly associated to core symptoms of psychiatric conditions than to primary objective cognitive impairment not necessarily associated with psychiatric disorders. In particular, of the variables assessed, female sex, depression, and PTSD were found to be the only predictors of SMC. Based on our findings, we recommend that a careful psychiatric evaluation should be conducted for COVID-19 survivors seeking care for memory complaints. Our study invites further investigations into the relationship between SMC and the risk of cognitive decline in patients with severe COVID-19.
Data availability
Anonymized data may be made available upon reasonable request to the corresponding author, subject to approval by the relevant ethics committee and in compliance with institutional and legal requirements.
References
Bowe B, Xie Y, Al-Aly Z. Postacute sequelae of COVID-19 at 2 years. Nat Med. 2023;29:2347–57.
Nalbandian A, Sehgal K, Gupta A, Madhavan MV, McGroder C, Stevens JS, et al. Post-acute COVID-19 syndrome. Nat Med. 2021;27:601–15.
Kim Y, Bae S, Chang HH, Kim SW. Long COVID prevalence and impact on quality of life 2 years after acute COVID-19. Sci Rep. 2023;13:11207.
Tavares-Júnior JWL, de Souza ACC, Borges JWP, Oliveira DN, Siqueira-Neto JI, Sobreira-Neto MA, et al. COVID-19 associated cognitive impairment: a systematic review. Cortex. 2022;152:77–97.
Thaweethai T, Jolley SE, Karlson EW, Levitan EB, Levy B, McComsey GA, et al. Development of a definition of postacute sequelae of SARS-CoV-2 infection. JAMA. 2023;329:1934–46.
Damiano RF, Caruso MJG, Cincoto AV, de Almeida Rocca CC, de Pádua Serafim A, Bacchi P, et al. Post-COVID-19 psychiatric and cognitive morbidity: preliminary findings from a Brazilian cohort study. Gen Hosp Psychiatry. 2022;75:38–45.
Gonçalves NG, Aliberti MJR, Bertola L, Avelino-Silva T, Dias MB, Apolinario D, et al. Dissipating the fog: cognitive trajectories and risk factors 1 year after COVID-19 hospitalization. Alzheimers Dement. 2023;19:3771–82.
Furman S, Green K, Lane TE. COVID-19 and the impact on Alzheimer's disease pathology. J Neurochem. 2024;168:3415–3429.
Botto R, Callai N, Cermelli A, Causarano L, Rainero I. Anxiety and depression in Alzheimer’s disease: a systematic review of pathogenetic mechanisms and relation to cognitive decline. Neurol Sci. 2022;43:4107–24.
Mendez MF. The relationship between anxiety and Alzheimer’s Disease. J Alzheimers Dis Rep. 2021;5:171–7.
Schmand B, Jonker C, Geerlings MI, Lindeboom J. Subjective memory complaints in the elderly: depressive symptoms and future dementia. Br J Psychiatry. 1997;171:373–6.
Vale FAC, Balieiro AP, Silva-Filho JH. Memory complaint scale (MCS). Proposed tool for active systematic search. Dement Neuropsychol. 2012;6:212–8.
Warren SL, Reid E, Whitfield P, Moustafa AA. Subjective memory complaints as a predictor of mild cognitive impairment and Alzheimer’s disease. Discover Psychology. 2022;2:13.
Warren SL, Reid E, Whitfield P, Helal AM, Abo H, Tindle R, et al. Cognitive and behavioral abnormalities in individuals with Alzheimer’s disease, mild cognitive impairment and subjective memory complaints. Curr Psychol. 2024;43:800–810.
Elfgren C, Gustafson L, Vestberg S, Passant U. Subjective memory complaints, neuropsychological performance and psychiatric variables in memory clinic attendees: a 3-year follow-up study. Arch Gerontol Geriatr. 2010;51:e110–4.
Yates JA, Clare L, Woods RT. CFAS M. Subjective memory complaints, mood and MCI: a follow-up study. Aging Ment Health. 2017;21:313–21.
Webster-Cordero F, Giménez-Llort L. The Challenge of Subjective Cognitive Complaints and Executive Functions in Middle-Aged Adults as a Preclinical Stage of Dementia: A Systematic Review. Geriatrics. 2022;7:30.
Bell TR, Beck A, Gillespie NA, Reynolds CA, Elman JA, Williams ME, et al. A traitlike dimension of subjective memory concern over 30 years among adult male twins. JAMA Psychiatry. 2023;80:718–27.
Marrie RA, Cohen J, Stuve O, Trojano M, Sørensen PS, Reingold S, et al. A systematic review of the incidence and prevalence of comorbidity in multiple sclerosis: overview. Mult Scler. 2015;21:263–81.
Margoni M, Preziosa P, Rocca MA, Filippi M. Depressive symptoms, anxiety and cognitive impairment: emerging evidence in multiple sclerosis. Transl Psychiatry. 2023;13:264.
Anderson JR, Fitzgerald KC, Murrough JW, Katz Sand IB, Sorets TR, Krieger SC, et al. Depression symptoms and cognition in multiple sclerosis: Longitudinal evidence of a specific link to executive control. Mult Scler. 2023;29:1632–45.
Eggers C, Arendt G, Hahn K, Husstedt IW, Maschke M, Neuen-Jacob E, et al. HIV-1-associated neurocognitive disorder: epidemiology, pathogenesis, diagnosis, and treatment. J Neurol. 2017;264:1715–27.
Rourke SB, Halman MH, Bassel C. Neurocognitive complaints in HIV-infection and their relationship to depressive symptoms and neuropsychological functioning. J Clin Exp Neuropsychol. 1999;21:737–56.
Cysique LA, Brew BJ. Comorbid depression and apathy in HIV-associated neurocognitive disorders in the era of chronic HIV infection. Handb Clin Neurol. 2019;165:71–82.
Pyne JD, Brickman AM. The impact of the COVID-19 pandemic on dementia risk: potential pathways to cognitive decline. Neurodegener Dis. 2021;21:1–23.
Godoy-González M, Navarra-Ventura G, Gomà G, de Haro C, Espinal C, Fortià C, et al. Objective and subjective cognition in survivors of COVID-19 one year after ICU discharge: the role of demographic, clinical, and emotional factors. Crit Care. 2023;27:188.
García-Sánchez C, Calabria M, Grunden N, Pons C, Arroyo JA, Gómez-Anson B, et al. Neuropsychological deficits in patients with cognitive complaints after COVID-19. Brain Behav. 2022;12:e2508.
Ferrando SJ, Dornbush R, Lynch S, Shahar S, Klepacz L, Karmen CL, et al. Neuropsychological, medical, and psychiatric findings after recovery from acute COVID-19: a cross-sectional study. J Acad Consult Liaison Psychiatry. 2022;63:474–84.
Feter N, Caputo EL, Leite JS, Delpino FM, Cassuriaga J, da Silva CN, et al. Incidence of memory complaints during the COVID-19 pandemic in Southern Brazil: findings from PAMPA cohort. Dement Neuropsychol. 2023;17:e20220072.
Muschel C, Lynch ST, Dornbush R, Klepacz L, Shahar S, Ferrando SJ. Frequency, Characteristics, and Correlates of Cognitive Complaints in a Cohort of Individuals with Post-Acute Sequelae of COVID-19. Brain Sci. 2023;14:3.
Miethke-Morais A, Perondi B, Harima L, Montal AC, Baldassare RM, Moraes DP, et al. Overcoming barriers to providing comprehensive inpatient care during the COVID-19 pandemic. Clinics (Sao Paulo). 2020;75:e2100.
Perondi B, Miethke-Morais A, Montal AC, Harima L, Segurado AC. Committee HdCC-CM. Setting up hospital care provision to patients with COVID-19: lessons learnt at a 2400-bed academic tertiary center in São Paulo, Brazil. Braz J Infect Dis. 2020;24:570–4.
Corman VM, Landt O, Kaiser M, Molenkamp R, Meijer A, Chu DK, et al. Detection of 2019 novel coronavirus (2019-nCoV) by real-time RT-PCR. Euro Surveill. 2020;25:2000045.
Lisboa Bastos M, Tavaziva G, Abidi SK, Campbell JR, Haraoui LP, Johnston JC, et al. Diagnostic accuracy of serological tests for covid-19: systematic review and meta-analysis. BMJ. 2020;370:m2516.
Busatto GF, de Araújo AL, Duarte AJDS, Levin AS, Guedes BF, Kallas EG, et al. Post-acute sequelae of SARS-CoV-2 infection (PASC): a protocol for a multidisciplinary prospective observational evaluation of a cohort of patients surviving hospitalisation in Sao Paulo, Brazil. BMJ Open. 2021;11:e051706.
Ferreira JC, Moreira TCL, de Araújo AL, Imamura M, Damiano RF, Garcia ML, et al. Clinical, sociodemographic and environmental factors impact post-COVID-19 syndrome. J Glob Health. 2022;12:05029.
Roffman CE, Buchanan J, Allison GT. Charlson comorbidities index. J Physiother. 2016;62:171.
infection WWGotCCaMoC-. A minimal common outcome measure set for COVID-19 clinical research. Lancet Infect Dis. 2020;20:e192–e7.
Miranda AR, Scotta AV, Cortez MV, Soria EA. Triggering of postpartum depression and insomnia with cognitive impairment in Argentinian women during the pandemic COVID-19 social isolation in relation to reproductive and health factors. Midwifery. 2021;102:103072.
Hwang EH, Kim KH. Effects of cognition, daily-living stress, and health-promotion behavior on subjective memory complaints by community-dwelling elders. J Korean Gerontol Nurs. 2019;21:135–43.
Bertolucci PH, Okamoto IH, Brucki SM, Siviero MO, Toniolo Neto J, Ramos LR. Applicability of the CERAD neuropsychological battery to Brazilian elderly. Arq Neuropsiquiatr. 2001;59:532–6.
AIT- Army Individual Test Battery. Manual of directions and scoring. 1944. Washington, DC: War Department, Adjutant General's Office.
Welsh K, Butters N, Hughes J, Mohs R, Heyman A. Detection of abnormal memory decline in mild cases of Alzheimer’s disease using CERAD neuropsychological measures. Arch Neurol. 1991;48:278–81.
Welsh KA, Butters N, Hughes JP, Mohs RC, Heyman A. Detection and staging of dementia in Alzheimer’s disease. Use of the neuropsychological measures developed for the Consortium to Establish a Registry for Alzheimer’s Disease. Arch Neurol. 1992;49:448–52.
Bernard BA, Goldman JG. MMSE - Mini-Mental State Examination. In Encyclopedia of Movement Disorders. Elsevier Inc. 2010. pp. 187–189.
(ABEP) ABdEdP. Critério de Classificação Econômica no Brasil São Paulo, SP: Associação Brasileira de Empresas de Pesquisa; 2020. https://www.abep.org/criterio-brasil.
(IBGE) IBdGeE. Desigualdades sociais por raça ou cor no Brasil: notas técnicas. Rio de Janeiro, RJ: IBGE; 2019.
Klok FA, Boon GJAM, Barco S, Endres M, Geelhoed JJM, Knauss S, et al. The Post-COVID-19 Functional Status scale: a tool to measure functional status over time after COVID-19. Eur Respir J. 2020;56:2001494.
Battistella LR, Imamura M, De Pretto LR, Van Cauwenbergh SKHA, Delgado Ramos V, Saemy Tome Uchiyama S, et al. Long-term functioning status of COVID-19 survivors: a prospective observational evaluation of a cohort of patients surviving hospitalisation. BMJ Open. 2022;12:e057246.
Zimmermann N, Cardoso CO, Kristensen CH, Fonseca RP. Brazilian norms and effects of age and education on the Hayling and Trail Making Tests. Trends Psychiatry Psychother. 2017;39:188–95.
Brucki SM, Malheiros SM, Okamoto IH, Bertolucci PH. [Normative data on the verbal fluency test in the animal category in our milieu]. Arq Neuropsiquiatr. 1997;55:56–61.
Aiyegbusi OL, Hughes SE, Turner G, Rivera SC, McMullan C, Chandan JS, et al. Symptoms, complications and management of long COVID: a review. J R Soc Med. 2021;114:428–42.
Subramanian A, Nirantharakumar K, Hughes S, Myles P, Williams T, Gokhale KM, et al. Symptoms and risk factors for long COVID in non-hospitalized adults. Nat Med. 2022;28:1706–14.
Premraj L, Kannapadi NV, Briggs J, Seal SM, Battaglini D, Fanning J, et al. Mid and long-term neurological and neuropsychiatric manifestations of post-COVID-19 syndrome: a meta-analysis. J Neurol Sci. 2022;434:120162.
Taquet M, Geddes JR, Husain M, Luciano S, Harrison PJ. 6-month neurological and psychiatric outcomes in 236 379 survivors of COVID-19: a retrospective cohort study using electronic health records. Lancet Psychiatry. 2021;8:416–27.
O’Mahoney LL, Routen A, Gillies C, Ekezie W, Welford A, Zhang A, et al. The prevalence and long-term health effects of Long Covid among hospitalised and non-hospitalised populations: a systematic review and meta-analysis. EClinicalMedicine. 2023;55:101762.
Pihlaja RE, Kauhanen LS, Ollila HS, Tuulio-Henriksson AS, Koskinen SK, Tiainen M, et al. Associations of subjective and objective cognitive functioning after COVID-19: a six-month follow-up of ICU, ward, and home-isolated patients. Brain Behav Immun Health. 2023;27:100587.
Fjone KS, Stubberud J, Buanes EA, Hagen M, Laake JH, Hofsø K. Objective and subjective cognitive status after intensive care unit treatment for COVID-19. Brain Behav Immun Health. 2024;38:100786.
Bryant VE, Fieo RA, Fiore AJ, Richards VL, Porges EC, Williams R, et al. Subjective cognitive complaints: predictors and health outcomes in people living with HIV. AIDS Behav. 2022;26:1163–72.
Asadi-Pooya AA, Akbari A, Emami A, Lotfi M, Rostamihosseinkhani M, Nemati H, et al. Long COVID syndrome-associated brain fog. J Med Virol. 2022;94:979–84.
Ceban F, Ling S, Lui LMW, Lee Y, Gill H, Teopiz KM, et al. Fatigue and cognitive impairment in Post-COVID-19 Syndrome: a systematic review and meta-analysis. Brain Behav Immun. 2022;101:93–135.
Damiano RF, Rocca CCA, Serafim AP, Loftis JM, Talib LL, Pan PM, et al. Cognitive impairment in long-COVID and its association with persistent dysregulation in inflammatory markers. Front Immunol. 2023;14:1174020.
Tsampasian V, Elghazaly H, Chattopadhyay R, Debski M, Naing TKP, Garg P, et al. Risk factors associated with Post-COVID-19 condition: a systematic review and meta-analysis. JAMA Intern Med. 2023;183:566–80.
Mathews SB, Arnold SE, Epperson CN. Hospitalization and cognitive decline: can the nature of the relationship be deciphered? Am J Geriatr Psychiatry. 2014;22:465–80.
Sousa NMF, Maranhão ACPF, Braga LW. Cognitive impairment and neuropsychiatric symptoms among individuals with history of symptomatic SARS-CoV-2 infection: a retrospective longitudinal study. Dement Neuropsychol. 2024;18:e20230053.
Chakrabarty T, Hadjipavlou G, Lam RW. Cognitive dysfunction in major depressive disorder: assessment, impact, and management. Focus (Am Psychiatr Publ). 2016;14:194–206.
Qureshi SU, Long ME, Bradshaw MR, Pyne JM, Magruder KM, Kimbrell T, et al. Does PTSD impair cognition beyond the effect of trauma? J Neuropsychiatry Clin Neurosci. 2011;23:16–28.
Roberts AL, Liu J, Lawn RB, Jha SC, Sumner JA, Kang JH, et al. Association of posttraumatic stress disorder with accelerated cognitive decline in middle-aged women. JAMA Netw Open. 2022;5:e2217698.
García-Gutiérrez MS, Navarrete F, Sala F, Gasparyan A, Austrich-Olivares A, Manzanares J. Biomarkers in Psychiatry: Concept, Definition, Types and Relevance to the Clinical Reality. Front Psychiatry. 2020;11:432.
Toniolo S, Scarioni M, Di Lorenzo F, Hort J, Georges J, Tomic S, et al. Dementia and COVID-19, a bidirectional liaison: risk factors, biomarkers, and optimal health care. J Alzheimers Dis. 2021;82:883–98.
Duffy JR, Peach RK, Strand EA. Progressive apraxia of speech as a sign of motor neuron disease. Am J Speech Lang Pathol. 2007;16:198–208.
Acknowledgements
This work was supported by donations from the general public under the HC-COMVIDA crowdfunding scheme (https://viralcure.org/c/hc). We are thankful for the support received from members of the HCFMUSP COVID-19 Study Group (Eloisa Bonfá, Edivaldo M. Utiyama, Aluisio C. Segurado, Beatriz Perondi, Anna Miethke-Morais, Amanda C. Montal, Leila Harima, Solange R. G. Fusco, Marjorie F. Silva, Marcelo C. Rocha, Izabel Marcilio, Izabel Cristina Rios, Fabiane Yumi Ogihara Kawano, Maria Amélia de Jesus, Ésper G. Kallas, Carolina Carmo, Clarice Tanaka, Heraldo Possolo de Souza, Julio F. M. Marchini, Carlos R. Carvalho, Juliana C. Ferreira, Anna Sara Levin, Maura Salaroli Oliveira, Thaís Guimarães, Carolina dos Santos Lázari, Alberto José da Silva Duarte, Ester Sabino, Marcello M. C. Magri, Tarcisio E. P. Barros-Filho, Maria Cristina Peres Braido Francisco). We are grateful for the infrastructure support from the HCFMUSP COVID-19 taskforce (Antonio José Pereira, Rosemeire K. Hangai, Danielle P. Moraes, Renato Madrid Baldassare, Elizabeth de Faria, Gisele Pereira, Lucila Pedroso, Marcelo C. A. Ramos, Taciano Varro and Vilson Cobello Junior) both during the baseline stage of in-hospital data collection and during the setting-up of the follow-up assessments. We are grateful for the support in organizing the logistics for the follow-up assessments of COVID-19 subjects at HCFMUSP from: Patricia Manga Favaretto, Maria Cristina Coelho de Nadai, Vivian R. B. Saboya, Adriana Ladeira de Araújo and other members of the Diretoria Executiva dos Laboratórios de Investigação Médica; and Michelle Louvaes Garcia and other members of the clinical research center at the Instituto do Coração (InCor). We are also grateful to Katia Regina da Silva for creating and managing the RedCap database used for the study. We thank the teams led by Juliana Carvalho Ferreira, Carlos R. Ribeiro de Carvalho, Heraldo Possolo de Souza, Wilson Jacob Filho, Thiago Avelino-Silva and José Eduardo Pompeu for the input of information into the electronic clinical database for the baseline in hospital stay of COVID-19 subjects.
Author information
Authors and Affiliations
Contributions
Concept and design of the manuscript: GFB, APR, YD Drafting of the manuscript: YD, APR, GFB Critical revision of the manuscript for important intellectual contribution: RFD, AGC, RH, CCAR, APS, BFG, RN, MI, OVF Approval of the final version of the manuscript before submission: all authors.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Dong, Y., Ritto, A.P., Damiano, R.F. et al. Memory complaints after COVID-19: a potential indicator of primary cognitive impairment or a correlate of psychiatric symptoms?. Transl Psychiatry 14, 455 (2024). https://doi.org/10.1038/s41398-024-03154-w
Received:
Revised:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41398-024-03154-w
