
Abstract
The pathways involved in the pathophysiology of fetal growth restriction (FGR) and small for gestational age (SGA) are incompletely understood. We conduct a systematic review to identify metabolomic signatures in maternal and newborn tissues and body fluids samples associated with FGR/SGA. Here, we report that 825 non-duplicated metabolites were significantly altered across the 48 included studies using 10 different human biological samples, of which only 56 (17 amino acids, 12 acylcarnitines, 11 glycerophosphocholines, six fatty acids, two hydroxy acids, and eight other metabolites) were significantly and consistently up- or down-regulated in more than one study. Three amino acid metabolism-related pathways and one related with lipid metabolism are significantly associated with FGR and/or SGA: biosynthesis of unsaturated fatty acids in umbilical cord blood, and phenylalanine, tyrosine and tryptophan biosynthesis, valine, leucine and isoleucine biosynthesis, and phenylalanine metabolism in newborn dried blood spot. Significantly enriched metabolic pathways were not identified in the remaining biological samples. Whether these metabolites are in the causal pathways or are biomarkers of fetal nutritional deficiency needs to be explored in large, well-phenotyped cohorts.
Similar content being viewed by others

Introduction
The phenotypic term fetal growth restriction (FGR) is used to describe a highly heterogeneous syndrome characterised by the fetus’ failure to achieve its genetic growth potential compared to international growth standards1,2,3. The term small for gestational age (SGA) is used to describe an infant born with a birthweight less than the 10th centile for gestational age and sex. Using such standards1,2,3 to avoid the bias associated with population-specific charts4, it has been estimated that 23.4 million newborns (17.4% of all liveborn babies worldwide) in 2020 were SGA5. Nearly a quarter (22.4%) of the 2.4 million neonatal deaths worldwide were attributable to preterm (<37 weeks’ gestation) or term (≥37 weeks’ gestation) SGA5, and 21.2% of stillbirths at ≥22 weeks’ gestation were SGA6.
Both growth-restricted and SGA fetuses are at higher risk of perinatal morbidity and mortality compared with non-growth-restricted and/or appropriate for gestational age (AGA) fetuses7,8,9,10. In addition, surviving growth-restricted and SGA infants have an increased risk for death, stunting, wasting, neurodevelopmental impairment during childhood, reduced intelligence quotient and cognitive performance, autism spectrum disorders, depression, and chronic diseases in adulthood10,11,12,13,14,15,16,17,18.
A wide range of analytical methods have been employed to screen for FGR; however, none of the biomarkers proposed to date are sufficiently accurate for screening, prevention, treatment development or routine clinical practice19,20. Metabolomics, despite its limited use in clinical practice, may be a more suitable methodology20,21,22 having accelerated understanding of metabolic diseases and detected silent phenotypes (only present in specific physiological conditions)23, thereby establishing biomarkers that precede disease pathology24,25,26.
Therefore, a critical appraisal of the existing metabolomic evidence is required to shed new light on the metabolic pathways involved in the pathophysiology of FGR/SGA13. So, we conducted a systematic review aiming to identify metabolomic signatures in tissues and biofluids of pregnant women, placentas, umbilical cords and newborns associated with FGR/SGA compared to the corresponding reference group.
Results
Selection, characteristics and risk of bias of studies
Figure 1 summarises the process of identification and selection of studies. Our search strategy identified 3134 citations. After removing duplicates and clearly ineligible records, we assessed 115 potentially eligible studies for possible inclusion, from which we excluded 67 based on parameters outlined in our methodology. Forty-eight studies27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51,52,53,54,55,56,57,58,59,60,61,62,63,64,65,66,67,68,69,70,71,72,73,74, which included a total of 4228 women and 820,271 newborns, met the inclusion criteria, reflecting the paucity of mother-offspring dyad studies.

This figure illustrates the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) flow diagram detailing the study selection process. The diagram includes the number of records identified, screened, assessed for eligibility, and included in the systematic review. FGR fetal growth restriction; SGA small for gestational age. Source: Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ 2021;372:n71. doi: 10.1136/bmj.n71. For more information, visit: https://www.prismastatement.org/prisma-2020-flow-diagram.
The main characteristics of included studies are presented in Table 1. Nineteen studies were conducted in Europe28,30,31,32,34,35,36,40,42,43,45,46,49,54,56,58,59,64,69, 14 in Asia37,38,48,51,52,55,60,61,63,66,68,70,72,74, eight in the United States33,44,47,50,57,62,71,73, two in Australasia41,65, four in both Europe and Australasia27,29,53,67, and one in Egypt39. There were 37 case-control studies27,28,29,30,31,32,34,35,36,37,38,39,40,41,43,44,46,47,48,49,50,51,52,53,54,56,57,58,59,60,66,68,69,70,71,72,74, eight cross-sectional studies33,42,45,55,61,62,63,67, two cohort studies64,73 and one case-cohort study65. The sample sizes ranged from 1727 to 87864 women (median, 77) and 1429 to 736,43562 newborns (median, 80). The number of cases ranged from 927 to 147,28762 and the corresponding number of controls ranged from 827 to 589,14862. Thirty-five (73%) studies had <50 FGR or SGA cases.
Metabolomics were assessed in the following biological samples: maternal plasma or serum (19 studies29,31,32,40,42,43,48,49,50,52,53,54,56,64,65,70,72,73,74), maternal urine (three studies36,47,53), maternal hair (two studies37,41), maternal faeces (one study70), amniotic fluid (one study66), placenta (five studies27,57,60,71,72), umbilical cord blood (21 studies29,30,31,32,34,39,40,42,43,44,45,54,56,58,59,63,64,67,72,73,74), newborn dried blood spots (seven studies33,38,51,55,61,62,68), newborn urine (three studies28,35,69), and breast milk (one study46). Fourteen studies29,31,32,40,42,43,53,54,56,64,70,72,73,74 collected multiple biological samples (Table 1). Among the studies that assessed metabolomics in maternal samples, only 7 reported on fasting status at the time of sample collection: in six studies, the time elapsed between last food intake and sampling was at least eight hours31,43,50,53,54,56, whereas in the remaining study74 the samples were collected in a “fasting state”.
Gestational age was determined from the woman’s last menstrual period alone in one study55, from the woman’s last menstrual period and confirmed by ultrasound in the first trimester in 11 studies32,34,36,43,47,49,50,56,60,64,68, and from the woman’s last menstrual period and confirmed by ultrasound in either the first or second trimester in four studies30,40,52,71. The remaining 32 studies did not report on the methods used for determining gestational age. Twenty-one studies included only term infants27,29,31,32,36,37,41,42,43,45,47,49,51,53,54,55,59,61,63,72,74, three included only preterm infants28,33,69, and 24 included both preterm and term infants30,34,35,38,39,40,44,46,48,50,52,56,57,58,60,62,64,65,66,67,68,70,71,73. None of these 24 studies reported results separately for preterm and term infants.
The case definitions included the following: birthweight for gestational age <10th customised (six studies29,36,41,46,53,54) or non-customised (22 studies31,32,33,37,38,39,42,44,45,47,50,51,55,57,61,62,63,64,68,71,73,74) centile; birthweight for gestational age <10th centile plus ultrasound parameters (seven studies28,30,34,35,43,49,58); birthweight for gestational age <5th customised (one study27) or non-customised (two studies65,67) centile; birthweight or estimated fetal weight (EFW) or abdominal circumference (AC) for gestational age <3rd centile (two studies52,60); EFW or AC for gestational age <10th centile (one study66); EFW or AC for gestational age <10th centile plus ultrasound parameters (two studies70,72), others (four studies40,56,59,69); and unreported (one study48). Overall, according to traditional definitions for FGR and SGA outlined in the Methods section, 31 studies included fetuses/infants considered SGA28,29,30,31,32,33,35,36,37,39,41,42,44,45,46,47,50,51,53,54,57,59,61,62,63,64,66,68,71,73,74, 12 included fetuses/infants considered growth-restricted27,34,49,52,56,58,60,65,67,69,70,72, four included both SGA and fetuses/infants considered growth-restricted38,40,43,55 and in one it was unknown48. There were several categories of reference group: birthweight for gestational age between the 10th-90th centiles (19 studies30,32,33,35,38,39,40,45,50,54,55,61,62,64,68,70,71,73,74); birthweight ≥10th centile (eight studies34,44,47,49,56,57,58,63); other intervals of birthweight centiles (seven studies31,42,43,46,51,52,67); “uncomplicated/normal/healthy pregnancies or healthy/AGA newborns” (nine studies27,28,29,37,41,48,53,66,72); birthweight Z-score between −1 and +1 SD (one study59); and unreported (four studies36,60,65,69).
Twenty-six studies used an untargeted metabolomic approach27,28,29,30,31,34,35,36,37,39,41,45,46,47,49,52,53,54,59,60,66,69,70,71,72,74, 18 used a targeted approach32,33,38,40,42,48,50,51,55,58,61,62,63,64,65,67,68,73, and four used both approaches43,44,56,57. The analytical platforms used for metabolite detection included liquid chromatography (ultra/high/ultra-high performance) coupled to mass spectrometry (LC-MS) in 24 studies27,29,30,33,38,39,45,48,49,50,51,52,53,55,59,61,62,63,64,65,68,69,70,74, nuclear magnetic resonance (NMR) spectroscopy in 11 studies28,31,34,35,36,43,46,54,56,60,67, gas chromatography coupled to mass spectrometry (GC–MS) in seven studies32,37,40,47,66,71,72, flow injection analysis (FIA) in one study42, LC-MS and NMR in two studies44,57, LC-MS and FIA in two studies58,73, and LC-MS and GC-MS in one study41.
Multivariate approaches that were used to analyse metabolites individually, as well as the relationships among the individual metabolites, included multivariate linear regression models (15 studies33,36,37,41,42,45,49,50,53,55,56,62,63,67,72), partial least square discriminant analysis (PLS-DA) or orthogonal PLS-DA (seven studies29,43,44,54,57,69,71), principal component analysis (PCA) (three studies27,30,65), and both PLS-DA/orthogonal PLS-DA and PCA (12 studies28,31,34,35,39,46,58,59,60,66,73,74). Software for metabolic pathway analysis was used in 12 studies28,39,44,46,48,57,66,69,70,71,73,74.
The risk of bias in each included study is summarised in Supplementary Fig. 1. No study was judged to be at low risk of bias for all eight domains. Only 13 studies (27%) fulfilled at least six of the eight criteria for low risk of bias29,34,43,45,49,53,55,58,60,69,71,72,74. Eleven studies were deemed to be at low risk of bias for five domains31,33,44,46,47,50,57,65,67,70,73, whereas the remaining 24 studies (50%) had four or more methodological flaws27,28,30,32,35,36,37,38,39,40,41,42,48,51,52,54,56,59,61,62,63,64,66,68. The most common deficiencies were related to unblinded interpretation of metabolomics results to fetal growth status of participants, overfitting in the analyses, and lack of reporting on handling of specimens and pre-analytical procedures.
Among the 13 studies that met at least six of the eight criteria for low risk of bias, 1129,34,43,49,53,55,58,60,71,72,74 provided data for metabolomic profiles and pathway analyses in different biological samples. The remaining two studies did not provide data to these analyses45,69.
Overall, a total of 825 non-duplicated metabolites were significantly altered across the 48 included studies, of which 46% were up- and 54% down-regulated. Eighty significantly altered metabolites were reported in more than one study (fatty acyls, 35%; amino acids, 31%; glycerophospholipids, 21%; others, 13%), 29 in more than two studies (amino acids, 52%; fatty acyls, 24%; glycerophospholipids, 21%; others, 3%), and 20 in more than three studies (amino acids, 60%; glycerophospholipids, 20%; fatty acyls, 20%).
Metabolomic profiles in maternal plasma or serum
Nineteen studies assessed metabolomic profiles in maternal plasma (11 studies29,31,40,43,48,50,53,56,65,73,74) and serum (eight studies32,42,49,52,54,64,70,72): three only ≤20 weeks’ gestation29,53,64, two between 24 and 28 weeks’ gestation52,73, three in the third trimester65,70,74, two collected serial samples in the first, second and third trimester of pregnancy49,50, and nine collected the samples within 24 h before birth, or during or after birth31,32,40,42,43,48,54,56,72 (Table 1).
Six studies (one at ≤20 weeks’ gestation64, one at 24–28 weeks’ gestation73 and four in the peripartum period31,32,42,56) did not identify significantly up- or down-regulated metabolites. In the remaining 13 studies (three at ≤20 weeks’ gestation29,50,53, five at >20 weeks’ gestation49,52,65,70,74, and five in the peripartum period40,43,48,54,72), a total of 156 non-duplicated metabolites had significantly different concentrations between the FGR/SGA and the corresponding reference groups (103 up-regulated and 53 down-regulated). Eight of the 156 metabolites were significantly up- or down-regulated in more than one study (pregnanediol-3-glucuronide in studies at ≤20 weeks’ gestation; malic acid in studies at >20 weeks’ gestation and in the peripartum period; and alanine, isoleucine, lysine, serine, phenylalanine, and 4-aminobutyric acid in studies in the peripartum period) and only one (alanine in studies in the peripartum period) in more than two studies (Table 2).
Metabolomic profiles in maternal plasma or serum at ≤ 20 weeks’ gestation
Five studies29,49,50,53,64, assessed metabolomic profiles in plasma or serum of pregnant women at ≤20 weeks’ gestation (Table 1). Up-regulated metabolites in FGR/SGA pregnancies that were reported in individual studies included cervonyl carnitine and sphingolipids-related metabolites29, plasmalogen49, eicosanoids related to hydroxyeicosatetraenoic and dihydroxyeicosatrienoic acids50, and glycerophospholipids (mainly phosphatidylserines, phosphatidylethanolamines and phosphatidylcholines), sphingolipids, glycerolipids, and fatty acyls53. Two studies29,49 reported that steroids-related metabolites were usually down-regulated in SGA pregnancies. One study64 did not find any significantly altered metabolites between women who subsequently delivered SGA infants and controls at 13 weeks’ gestation.
The total number of metabolites significantly different between the FGR/SGA and reference groups was 52 (45 up- and seven down-regulated), of which only one (pregnanediol-3-glucuronide) was significantly and consistently down-regulated in more than one study (Table 2), primarily likely due to differences in analytical platforms and focus on different metabolite classes of each study from the description provided.
Metabolomic profiles in maternal plasma or serum at > 20 weeks’ gestation and in the peripartum period
Sixteen studies evaluated metabolomic profiles at >20 weeks’ gestation (n = 749,50,52,65,70,73,74) or in the peripartum period (n = 931,32,40,42,43,48,54,56,72) (Table 1). Most studies evaluating metabolomic profiles at 24–28 weeks’ gestation and in the third trimester reported few metabolites significantly altered50,52,65,73,74. Only one study70 identified 13 significantly altered metabolites in the third trimester (nine up- and four down-regulated). Among the nine studies that evaluated metabolomic profiles in the peripartum period, four31,32,42,56 did not find any significantly altered metabolites and three40,43,54 reported only a few altered metabolites. In the remaining two studies, one48 reported 18 significantly altered metabolites (15 up-regulated, mainly amino acids, and three down-regulated) and the other72 reported 31 altered metabolites (13 up-regulated, mostly derivatives of amino acids, keto acids and carboxylic acids, and 18 down-regulated, mostly unsaturated and saturated fatty acids and organic compounds).
The total number of metabolites significantly different between the FGR/SGA and reference groups was 109 (44 at >20 weeks’ gestation [27 up- and 17 down-regulated], and 65 in the peripartum period [32 up- and 33 down-regulated]). Overall, seven metabolites were significantly altered in more than one study, of which five showed a consistent trend (isoleucine, lysine, serine and 4-aminobutyric acid, up-regulated in all studies; and malic acid, down-regulated in all studies) and two an inconsistent trend (alanine, up-regulated in three studies and down-regulated in one; and phenylalanine, up-regulated in one study and down-regulated in one study) (Table 2).
Metabolomic profiles in maternal hair
Two studies investigated the metabolomic profiles of maternal hair samples in SGA cases, one at 26-28 weeks’ gestation37 and the other in the second and third trimesters of pregnancy41 (Table 1). Overall, a total of 33 non-duplicated metabolites had significantly different concentrations between the SGA and reference groups (11 up- and 22 down-regulated), of which only two were significantly altered in more than one study (margaric acid and myristic acid, both up-regulated in the two studies) (Table 2). In one study37, most of the 32 significantly altered metabolites reported were amino acids, amino acid derivatives and fatty acids. The other study41 reported that three metabolites (all long-chain fatty acids) were significantly up-regulated in the second trimester and none in the third trimester.
Metabolomic profiles in maternal urine
Three studies evaluated metabolomic profiles of FGR/SGA in maternal urine, two at ≤20 weeks’ gestation36,53 and one at 10 and 26 weeks’ gestation47 (Table 1). A total of 20 non-duplicated metabolites had significantly different concentrations between the FGR/SGA and reference groups (nine up- and 11 down-regulated). None of these metabolites were significantly altered in more than one study (Table 2). One47 of the three studies found only up-regulated metabolites and two36,53 found only down-regulated metabolites. Lower levels of metabolites involved in nutrient transport and detoxification pathways in women with SGA pregnancies were reported in one study53. The remaining two studies36,47 did not identify any perturbed pathways.
Metabolomic profiles in maternal faeces
Metabolomic profiles of FGR/SGA in maternal faeces were examined in one study70, which reported significant differences in the concentrations of 23 metabolites (seven up- and 16 down-regulated) in women with FGR pregnancies compared to women with AGA pregnancies in the third trimester (Table 1). Pathway analysis showed that lipid, amino acid, sphingolipid, fatty acid, and steroid hormone metabolism was enriched in the FGR group.
Metabolomic profiles in amniotic fluid
Only one study66 evaluated the metabolomic profiles of FGR/SGA pregnancies in amniotic fluid at a mean gestational age of 30 weeks (Table 1). A total of 47 differentially expressed metabolites were identified of which 23 were up-regulated (mainly metabolites involved in glucose metabolism such as malic acid, glycolic acid, maleic acid, and D-glycerate) and 24 down-regulated (mainly amino acids such as glutamate, phenylalanine, valine and leucine).
Metabolomic profiles in placenta
Five studies assessed metabolomic profiles of FGR/SGA in placental samples27,57,60,71,72, of which one27 did not provide clear data on altered metabolites. Overall, a total of 217 non-duplicated metabolites were reported to be significantly altered across studies (38 up- and 179 down-regulated), of which just 10, mostly amino acids, were significantly altered in more than one study (Table 3) and one (taurine) was significantly altered in more than two studies. Importantly, only three metabolites from the initial 217, had a consistent trend: glycerophosphocholine and lactic acid, up-regulated in two studies60,71; and glycine, down-regulated in two studies57,71. The remaining seven significantly altered metabolites (all amino acids) had an inconsistent trend across the included studies (Table 3). Pathway analysis from one study57 revealed abnormalities that were consistent with fetal hepatic dysfunction in suspected FGR. Another study71 reported that metabolic pathways related to the hypoxia response and amino-acid uptake and metabolism were associated with SGA.
Metabolomic profiles in umbilical cord blood
Among the 21 studies that assessed metabolomic profiles in umbilical cord blood, 20 reported significant differences in metabolite concentrations between the FGR/SGA and reference groups. A total of 308 non-duplicated metabolites were significantly altered (155 up- and 153 down-regulated), of which 45 metabolites were significantly altered in more than one study and 18 in more than two studies (Table 4).
The amino acids phenylalanine, alanine, valine, isoleucine, and glutamine, four lysophosphatidylcholines (16:1, 18:1, 18:2, 20:3), and carnitine were the most reported altered metabolites. Of the 46 significantly altered metabolites in more than one study, 24 showed a consistent trend across studies: 17 were down-regulated in all studies (five lysophosphatidylcholines, five phosphatidylcholines, three fatty acids, gamma-linolenic acid, choline, cholesterol, and glucose) and seven were up-regulated in all studies (four amino acids, decanoyl carnitine, dodecanoid acid, and triglyceride). The remaining 22 metabolites showed an inconsistent trend (Table 4).
Metabolomic profiles in newborn dried blood spots
Seven studies, all using a targeted approach, evaluated metabolomic profiles of SGA in dried blood spots taken from a heel prick between 12 hours and 8 days after birth for newborn metabolic screening33,38,51,55,61,62,68. In general, metabolites associated with acylcarnitine were upregulated in most studies. Only one study reported that most acylcarnitines assessed were down-regulated68.
A total of 112 non-duplicated metabolites had significantly different concentrations between SGA and AGA neonates (80 up- and 32 down-regulated), of which 31 were significantly altered in more than one study and 12 in more than two studies (Table 5). Of the 31 significantly altered metabolites in more than one study, 18 showed a consistent trend across studies: 14 were up-regulated in all studies (10 acylcarnitines and four amino acids) and four were down-regulated in all studies (three amino acids and one acylcarnitine). The remaining 13 significantly altered metabolites in more than one study had an inconsistent trend (nine acylcarnitines and four amino acids).
Metabolomic profiles in newborn urine
Three studies evaluated metabolomic profiles of FGR in newborn urine28,35,69. All samples were taken within 48 h of birth. A total of 76 non-duplicated metabolites were significantly altered across studies (31 up- and 45 down-regulated) of which three were significantly and consistently altered in more than one study (myo-inositol, creatinine and creatine, up-regulated in all studies) (Table 5). No metabolite was significantly altered in more than two studies. One study28 reported three metabolic pathways associated with FGR (one involved in the metabolism of arginine and proline, one associated with the urea cycle and the third correlated with the metabolism of glycine, serine and threonine) and another69 reported metabolic pathways related to tryptophan and histidine metabolism and aminoacyl-tRNA and steroid hormone biosynthesis.
Metabolomic profiles in breast milk
Metabolomic profiles of SGA in breast milk were assessed in one study46, which reported significantly different concentrations of seven metabolites (five up- and two down-regulated) in milk/colostrum on the third to fourth day postpartum between mothers of SGA infants and controls (Table 1).
Analysis of metabolic pathways
Despite several metabolic pathways being significantly enriched in unadjusted analyses, only four metabolic pathways were found to be significantly enriched in adjusted analyses (FDR < 0.05): one in umbilical cord blood (biosynthesis of unsaturated fatty acids with an FDR p value of 0.016 and an impact value of 0.0) (Fig. 2 and Supplementary Table 1) and three in newborn dried blood spots (phenylalanine, tyrosine and tryptophan biosynthesis; valine, leucine and isoleucine biosynthesis; and phenylalanine metabolism, with FDR p values of 0.014, 0.021, and 0.021, respectively, and impact values of 1.0, 0.0, and 0.36, respectively) (Fig. 3 and Supplementary Table 2). Dried blood spots were taken for newborn screening of inborn metabolic diseases, although studies reported that newborns with genetic metabolic diseases were excluded from analyses.

The metabolome view shows all matched pathways according to the p values from the pathway enrichment analysis and pathway impact values from the pathway topology analysis. Each circle in the figure represents a metabolic pathway. The colour of the circle indicates the significance level (Raw p) in the enrichment analysis; darker colour (redder) indicates greater significance. The size of the circle reflects the pathway impact value in the topology analysis, such that the larger the circle, the larger the impact value. Only the biosynthesis of unsaturated fatty acids was found to be significantly enriched in adjusted analyses (false discovery rate p value < 0.05). FDR false discovery rate. Source data are provided as a Source Data file.

The metabolome view shows all matched pathways according to the p values from the pathway enrichment analysis and pathway impact values from the pathway topology analysis. Each circle in the figure represents a metabolic pathway. The colour of the circle indicates the significance level (Raw p) in the enrichment analysis; darker colour (redder) indicates greater significance. The size of the circle reflects the pathway impact value in the topology analysis, such that the larger the circle, the larger the impact value. Three metabolic pathways were found to be significantly enriched in adjusted analyses (false discovery rate p value < 0.05): phenylalanine, tyrosine and tryptophan biosynthesis; valine, leucine and isoleucine biosynthesis; and phenylalanine metabolism. FDR false discovery rate. Source data are provided as a Source Data file.
There were no significantly enriched metabolic pathways (FDR ≥ 0.05) in maternal plasma/serum at >20 weeks’ gestation or in the peripartum period (Supplementary Fig. 2 and Supplementary Table 3) and in placenta (Supplementary Fig. 3 and Supplementary Table 4). Pathway analyses in maternal plasma/serum at ≤20 weeks’ gestation, maternal hair, and newborn urine could not be performed because of there were only few significantly and consistently up- or down-regulated metabolites in more than one study in such biological samples.
Discussion
Principal findings
A total of 825 non-duplicated metabolites were significantly altered (46% up- and 54% down-regulated) across the 48 studies included in this systematic review using 10 different human biological samples. Only 56 metabolites (17 amino acids, 12 acylcarnitines, 11 glycerophosphocholines, six fatty acids, two hydroxy acids, and eight other metabolites) were reported to be significantly up- or down-regulated in more than one study with a consistent direction of the association, i.e. up- or down-regulated in all studies reporting that metabolite. Only pregnanediol-3-glucuronide was reported consistently down-regulated in maternal samples at ≤20 weeks’ gestation, a period very relevant for the potential prediction of FGR/SGA. The remaining 55 metabolites were reported in maternal plasma at >20 weeks’ gestation or in the peripartum period (n = 5); maternal hair at >20 weeks’ gestation (n = 2); placenta (n = 3); umbilical cord blood (n = 24); newborn dried blood spots (n = 18), and newborn urine (n = 3) (Supplementary Box 1).
Three amino acid metabolism-related pathways and one related with lipid metabolism were significantly associated with FGR and/or SGA: biosynthesis of unsaturated fatty acids in umbilical cord blood, and phenylalanine, tyrosine and tryptophan biosynthesis, valine, leucine and isoleucine (branched chain amino acids, BCAAs) biosynthesis, and phenylalanine metabolism in newborn dried blood spot. Among these pathways, phenylalanine, tyrosine and tryptophan biosynthesis and phenylalanine metabolism had the highest impact values (1.0 and 0.36, respectively). Significantly enriched metabolic pathways were not identified in the remaining biological samples. Observationally, however, across blood samples, those taken from mothers (at >20 weeks’ gestation), umbilical cord blood, and newborn dried bloodspots, showed perturbation of BCAA metabolism (i.e., the concentrations of isoleucine/valine/leucine). This may be particularly pertinent since BCAAs are essential amino acids and can only be, in humans, derived from the diet. BCAAs are also key for stimulating protein biosynthesis and tissue development75,76,77,78. Moreover, growth-restricted compared to AGA fetuses have lower plasma concentrations of BCAAs in the umbilical artery and vein79. Hence, one can speculate that common perturbations of BCAA metabolism in blood samples identified in this systematic review may contribute to, or reflect, impaired growth of the fetus.
Comparison with existing literature
Only one previous systematic review, including 21 studies, has evaluated metabolomic profiles in FGR80. Eighteen metabolites were identified that were significantly altered (unreported definition of statistical significance) in more than two studies (nine in neonatal studies [cord blood and newborn dried blood spot] and nine in maternal studies [maternal serum/plasma, urine, and hair, placenta and milk]) of which alanine, valine and isoleucine were reported in both maternal and neonatal studies. Other metabolites that were significantly altered in more than two studies included citrate and glycine in maternal studies, and proline, phenylalanine, and glutamine in neonatal studies. The most significantly enriched metabolic pathways with relatively high impact values were glutathione metabolism in maternal studies, glyoxylate and dicarboxylate metabolism and alanine, aspartate, and glutamate metabolism in neonatal studies, and arginine biosynthesis and arginine and proline metabolism in both maternal and neonatal studies. Conversely, our review did not identify any of these metabolic pathways as significantly enriched. Such a discrepancy could be explained by the smaller number of studies included by Yao et al.80; stratification of studies, using different biological samples, into only maternal and neonatal studies; and the inclusion of all significantly altered metabolites in pathway analysis without considering the frequency and consistency of the association.
Strengths and limitations
The major strengths of the present review are: (1) the rigorous methodology used and the complete adherence to the MOOSE guidelines including following the defined format for summarising the evidence22; (2) the inclusion of the largest number of mostly recent studies reported from different populations throughout the world; (3) the inclusion of studies assessing the association between FGR/SGA and metabolomics in 10 different biological samples; (4) the stringent criteria used for including metabolites in pathway analyses; and (5) separating those studies that examined metabolomic profiles in umbilical cord blood from those that used newborn dried blood spot and urine samples.
Despite these efforts, there are specific areas of concern with these data. First, there was substantial heterogeneity among studies in terms of design; sample size; participant characteristics; case, control and outcome definitions; timing of sampling; sample collection and preparation; data acquisition and processing; metabolomic methodologies used; and analytical and statistical approaches used, which limits the possibility of a summary statement. Such large heterogeneity could explain the inconsistent trends and conflicting patterns of metabolites significantly associated with FGR/SGA. Considerably greater efforts are needed to improve the standardised reporting of metabolomic studies following recent suggestions81.
Second, a major source of variation across studies was: (1) the use of very different definitions of FGR and SGA (that are often wrongly used interchangeably in the literature) and categories of reference groups, and (2) the failure to recognise the syndromic nature of these two anthropometric and clinical entities that have multiple inter-related aetiologies and risk factors. These limitations considerably undermine both the internal and external validity of studies. Hence, it is possible that the conflicting results just represent the role of the different aetiological factors associated with sub-groups of FGR/SGA that constitute the underlying risk profile of the samples selected.
Third, several studies only reported the significantly altered metabolites and no information was provided on the metabolites with non-significant differences in concentrations between the FGR/SGA and reference groups (selective non-reporting bias). There is also the risk of publication bias of research findings, depending on the nature and direction of the results, especially in studies exploring predictive biomarkers.
Fourth, although NMR has a significantly lower sensitivity and detects a much smaller number of metabolites than MS-based methods, both approaches are complementary. However, most studies included in our review only used one analytical method and made no comparisons across platforms. This may have resulted in metabolites being identified on one platform and not another, resulting in less consistency across studies.
Finally, there are two highly relevant conceptual issues for interpreting this literature: (1) the reliability of the results of a systematic review is limited by the methodological quality of the studies included. In our review, only just over a quarter of included studies met at least six of the eight criteria for low risk of bias. In addition, most included studies were case-control and cross-sectional, thus limiting the power to verify causal relationships between altered metabolites and FGR/SGA, which means that reverse causality should be carefully examined since metabolites could be the result of FGR/SGA rather than a cause. This limitation is key to maternal samples collected close to birth, as well as umbilical cord blood and newborn samples. Importantly, none of the included studies assessed neurodevelopmental outcomes and only one study58 evaluated postnatal growth patterns up to the age of 12 months. (2) The use of pathway analysis methods has intrinsic limitations, such as arbitrary criteria for defining pathways and p value cut-offs for selecting significant metabolites; input data and parameters used; changes in the background set; reliability of compound identification, and database updates, among others. Moreover, the statistical techniques used in pathway analysis consider only the number of statistically significant metabolites without taking into account the measured fold changes and trend consistency.
It might also be said that the results of pathway models are self-fulfilling: if a metabolomic study, especially if targeted, identifies molecules of related families (such as amino acids, fatty acids, and markers of glucose metabolism) associated with a phenotype, the pathway models will inevitably report that amino acid, lipid, and carbohydrate metabolic pathways are affected by the outcome of interest. Such a summary description of the underlying metabolic processes involved in complex syndromes is not necessarily useful for the identification of therapeutic strategies at the molecular level.
Clinical and research implications
In conclusion, our systematic review identified a number of altered metabolites and metabolic pathways that were associated with FGR and/or SGA. Some of these metabolites appear promising and may provide new insights for understanding the pathophysiology of these syndromes and the development of new therapeutic targets. Promising metabolites include lysophosphatidylcholine 16:1, phosphatidylcholine 36:3, leucine, choline, and triglyceride in umbilical cord blood samples, free carnitine, butyryl carnitine, acetyl carnitine, decenoyl carnitine, propionyl carnitine, and proline in newborn dried blood spot, and pregnanediol-3-glucuronide in maternal early-pregnancy samples. Well-designed and phenotyped studies with a large number of FGR/SGA cases to allow for stratification according to aetiology, especially longitudinal cohort metabolomics in plasma or serum of pregnant women and clinical intervention metabolomics studies, should be carried out to explore novel biomarkers of FGR/SGA and determine target metabolic pathways for prevention and treatment. Integrating metabolomic and other omic data would seem to be the next step to better elucidate networks of molecular mechanisms in FGR/SGA.
Methods
As a systematic review, our study did not involve direct participation of human subjects and focused solely on previously published and publicly available data. It did not require institutional review board approval for this reason. The ethical principles governing this study adhere to the established guidelines for systematic reviews and meta-analyses. This systematic review was registered with PROSPERO (CRD42021275753) on September 23, 2021 (https://www.crd.york.ac.uk/prospero/display_record.php?RecordID=275753) and reported according to the MOOSE guidelines for meta-analyses of observational studies82. Two authors (AC-A and MR) initially examined the relevant literature; AC-A and JV independently reviewed studies for inclusion, assessed their risk of bias, and extracted data. Disagreements were resolved through consensus.
Literature search
We searched MEDLINE, EMBASE, LILACS, CINAHL, Scopus, Web of Science, and the Cochrane Central Register of Controlled Trials (all from 1998, the year that the term metabolomics was introduced, to 31 December 2023) using a combination of keywords and text words related to metabolomics (“metabolomic”, “metabonomic”, “metabolome”, “metabolite”, “lipidomic”, “oxylipins”, “lipid mediators”, “proton nuclear magnetic resonance”, “liquid chromatography”, “gas chromatography”, “high-performance liquid chromatography”, “ultra-performance liquid chromatography”) and FGR and SGA (“fetal growth restriction”, “fetal growth retardation”, “impaired fetal growth”, “intrauterine growth restriction”, “intrauterine growth retardation”, “small for gestational age”, “small for date”, “small for gestation”). Google Scholar, proceedings of congresses and scientific meetings on obstetrics, maternal-fetal medicine and omics technologies, reference lists of identified studies, previously published systematic reviews, and review articles were also searched. We did not use any language restrictions. The initial search was performed from 1 June 2023 to 15 June 2023. Searches were re-run on a monthly basis until 2 January 2024.
Eligibility criteria
We included observational (cohort, case-control and cross-sectional) studies that reported on associations between metabolites measured using any metabolomic technology in tissues and biofluids of (a) women with a singleton pregnancy or (b) singleton newborns (within the first 7 days of life) and FGR or SGA diagnosed by criteria defined by the authors. Acceptable definitions for FGR included EFW or AC or birthweight below the 10th, 5th, or 3rd centiles for gestational age/sex (as reported by the authors) plus indicators of fetal and placental health such as amniotic fluid volume, biophysical profile, maternal and fetal Doppler velocimetry, biomarkers, and placental pathology, among others. Acceptable definitions for SGA included birthweight below the 10th, 5th, or 3rd centiles or less than two standard deviations below the mean for gestational age/sex regardless of birthweight reference or standard used. Analysed samples included maternal blood, urine, faeces and hair, amniotic fluid, placenta, breast milk, umbilical cord blood, and neonatal blood and urine. Studies not using a metabolomics technology, animal studies, studies including multiple pregnancies or neonates that did not report singleton data separately, conference abstracts, case reports, letters, editorials, and reviews were excluded from the review.
Assessment of risk of bias
The risk of bias in each included study was assessed using a modified version of QUADOMICS83, an adaptation of the Quality Assessment of Diagnostic Accuracy Studies (QUADAS)84 tool for studies using omic technologies. A total of eight domains were assessed. Each domain was judged as having a “low,” “high,” or “unclear” risk of bias. The domains evaluated and how they were interpreted were as follows:
1. Selection of participants – “low risk of bias”: all participants were selected from the same population and during the same time period; “high risk of bias”: all participants were not selected from the same population and/or were not selected during the same time period.
2. Description of selection criteria – “low risk of bias”: if detailed information on inclusion/exclusion criteria and sources of samples was reported; “high risk of bias”: if this information was not reported.
3. Description of procedures and timing of biological sample collection with respect to clinical factors – “low risk of bias”: the study report included an analysis of potential factors affecting the metabolite profile, and a procedure to control biases that they might induce; “high risk of bias”: if this information was not reported.
4. Reporting of handling of specimens and pre-analytical procedures and if they were similar for the whole sample – “low risk of bias”: the study reported that the whole set of samples underwent the same pre-analytical process; or the study described in detail any process related to the pre-analytical handling of the samples that could affect the results, and a comparison of the results according to the different procedures was supplied; “high risk of bias”: if this information was not reported.
5. Description of metabolite extraction methods and analytical techniques – “low risk of bias”: if the study reported in detail the metabolite extraction methods and analytical techniques used; “high risk of bias”: if this information was not reported.
6. Blinded interpretation of metabolomic results to fetal growth status of participants – “low risk of bias”: if metabolomic results were interpreted blinded to fetal growth status of participants; “high risk of bias”: if metabolomic results were not interpreted blinded to fetal growth status of participants.
7. Control for potential confounding variables – “low risk of bias”: the main potential confounding variables were identified and accounted for in the design and analysis; “high risk of bias”: the main potential confounding variables were not identified and/or accounted for in the design and analysis.
8. Avoidance of overfitting in statistical models – “low risk of bias”: if the models were validated in an independent set of samples or used some approach to deal with overfitting; “high risk of bias”: if the models were not validated in an independent set of samples or did not use some approach to deal with overfitting; or if the study used the same sample for the training and validation sets.
If there was insufficient information available to make a judgement about these items, then they were scored as “unclear risk of bias”.
Data extraction
Data were extracted from each included study using a specially designed form for capturing information on authors, publication date, study characteristics (experimental design, setting, follow-up period, attrition and exclusions from the analysis, prospective or retrospective data collection, blinded interpretation of metabolomic results), participants (selection, inclusion and exclusion criteria, case definition, control definition, number of women/neonates in each study group, baseline characteristics, and country and date of recruitment), biological samples (sampling time, sample collection and storage, frequency of sampling, handling of specimens, pre-analytical procedures, metabolite extraction methods, and analytical techniques), metabolomics data analysis (feature extraction, compound identification, statistical analysis and interpretation), and metabolites (reported metabolite identity by the authors of the paper (ID), and metabolites with statistically significant differences in concentration between the FGR/SGA and reference/control groups).
Data synthesis
Substantial heterogeneity in the analytical platforms used, variation in multivariate analyses, and incomplete and heterogeneous reporting of metabolite data and summary statistics prevented us from performing a quantitative meta-analysis and precluded us from determining the average fold changes of metabolite levels across all studies for any metabolite.
We separately analysed metabolite alterations as reported in the publications, in 10 types of biological sample: maternal plasma or serum, urine, faeces and hair (collected at ≤20 or >20 weeks’ gestation, or in the peripartum period), amniotic fluid, placenta, umbilical cord blood, neonatal blood and urine, and breast milk. Metabolites were identified according to the reported identity (ID) or common name with a subsequent standardisation conducted by using the Human Metabolomic Database (HMDB) to assign unique identifiers thereby avoiding synonymous names. Given most included studies reported the directionality of the identified metabolites, we initially selected and counted the total number of significantly up- and down-regulated metabolites, as compared with the corresponding reference group, in each study. A metabolite was considered as statistically significantly up- or down-regulated, as reported by the authors of individual studies, regardless of the p value threshold used for defining statistical significance and the use of tests for correcting multiple comparisons. Eighty-one percent of the included studies used a p value < 0.05 to determine significance.
Then, we summarised the significantly up- and down-regulated metabolites that were reported in at least more than one study, grouping them into maternal samples collected at ≤20 or >20 weeks’ gestation/peripartum period, and neonatal samples (all differentiated by the type of biological sample), placental samples, and umbilical cord blood samples, according to the metabolite’s direction of change between studies. The trend of one metabolite was considered “consistent” if it showed the same direction of change in all studies within the same parameter and biological sample (e.g. up- or down-regulated in all studies reporting maternal plasma). Otherwise, the metabolite’s trend was considered “inconsistent”.
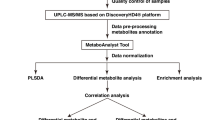
Finally, we imported the significantly up- or down-regulated metabolites in at least more than one study with a consistent trend to MetaboAnalyst 5.0 online software (https://www.metaboanalyst.ca)85 for separate pathway analysis in each of the aforementioned groups of biological samples. The software allows the most relevant pathways involved in the conditions under study to be identified. A metabolic pathway was considered to be significantly enriched if its adjusted p value (false discovery rate, FDR) was <0.05. Since we were testing many pathways at the same time, the statistical p values from enrichment analysis were further adjusted for multiple testing (Holm p, p value adjusted by Holm–Bonferroni method; and FDR p, p value adjusted using false discovery rate). The impact value (from 0.0 to 1.0) represents the relative importance of the pathway: the higher the impact value, the more relevant is the pathway in the condition under study.
Reporting summary
Further information on research design is available in the Nature Portfolio Reporting Summary linked to this article.
Data availability
The findings from this study are supported by data extracted from published literature. The relevant studies were identified through a systematic literature review and can all be accessed online as referenced in the current paper27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51,52,53,54,55,56,57,58,59,60,61,62,63,64,65,66,67,68,69,70,71,72,73,74. Study characteristics of all relevant studies included in the analyses are also provided in Table 1. All data supporting the findings described in this manuscript are available in the article and in the Supplementary Information and from the corresponding authors upon request. Data that support the findings of this study have been deposited in the Mendeley Data Repository: https://data.mendeley.com/datasets/4rsm8zv5x3/1 (https://doi.org/10.17632/4rsm8zv5x3.1). Source data are provided with this paper.
References
Frenquelli, R. et al. Complex perinatal syndromes affecting early human growth and development: issues to consider to understand their aetiology and postnatal effects. Front Neurosci 16, 856886 (2022).
Villar, J. et al. International standards for newborn weight, length, and head circumference by gestational age and sex: the Newborn Cross-Sectional Study of the INTERGROWTH-21st Project. Lancet 384, 857–868 (2014).
Villar, J. et al. INTERGROWTH-21 st very preterm size at birth reference charts. Lancet 387, 844–845 (2016).
Lee, A. C. et al. Estimates of burden and consequences of infants born small for gestational age in low and middle income countries with INTERGROWTH-21st standard: analysis of CHERG datasets. Bmj 358, j3677 (2017).
Lawn, J. E. et al. Small babies, big risks: global estimates of prevalence and mortality for vulnerable newborns to accelerate change and improve counting. Lancet 401, 1707–1719 (2023).
Okwaraji, Y. B. et al. Stillbirths: Contribution of preterm birth and size-for-gestational age for 125.4 million total births from nationwide records in 13 countries, 2000-2020. BJOG. https://doi.org/10.1111/1471-0528.17653.
Sovio, U., White, I. R., Dacey, A., Pasupathy, D. & Smith, G. C. S. Screening for fetal growth restriction with universal third trimester ultrasonography in nulliparous women in the Pregnancy Outcome Prediction (POP) study: a prospective cohort study. Lancet 386, 2089–2097 (2015).
Ruiz-Martinez, S. et al. Clinical phenotypes for risk stratification in small-for-gestational-age fetuses. Ultrasound Obstet Gynecol 59, 490–496 (2022).
Unterscheider, J. et al. Optimizing the definition of intrauterine growth restriction: the multicenter prospective PORTO Study. Am J Obstet Gynecol 208, 290.e1–6 (2013).
Longo, S. et al. Short-term and long-term sequelae in intrauterine growth retardation (IUGR). J Matern Fetal Neonatal Med 26, 222–225 (2013).
Katz, J. et al. Mortality risk in preterm and small-for-gestational-age infants in low-income and middle-income countries: a pooled country analysis. Lancet 382, 417–425 (2013).
Christian, P. et al. Risk of childhood undernutrition related to small-for-gestational age and preterm birth in low- and middle-income countries. Int J Epidemiol 42, 1340–1355 (2013).
Villar, J. et al. Association between fetal abdominal growth trajectories, maternal metabolite signatures early in pregnancy, and childhood growth and adiposity: prospective observational multinational INTERBIO-21st fetal study. Lancet Diabetes Endocrinol 10, 710–719 (2022).
Murray, E. et al. Differential effect of intrauterine growth restriction on childhood neurodevelopment: a systematic review. BJOG 122, 1062–1072 (2015).
Sacchi, C. et al. Association of intrauterine growth restriction and small for gestational age status with childhood cognitive outcomes: a systematic review and meta-analysis. JAMA Pediatr 174, 772–781 (2020).
Jenabi, E., Bashirian, S., Asali, Z. & Seyedi, M. Association between small for gestational age and risk of autism spectrum disorders: a meta-analysis. Clin Exp Pediatr 64, 538–542 (2021).
Su, Y., D’Arcy, C. & Meng, X. Research review: developmental origins of depression - a systematic review and meta-analysis. J Child Psychol Psychiatry 62, 1050–1066 (2021).
Barker, D. J. Adult consequences of fetal growth restriction. Clin Obstet Gynecol 49, 270–283 (2006).
Conde-Agudelo, A., Papageorghiou, A. T., Kennedy, S. H. & Villar, J. Novel biomarkers for predicting intrauterine growth restriction: a systematic review and meta-analysis. BJOG 120, 681–694 (2013).
Smith, G. C. S. Developing novel tests to screen for fetal growth restriction. Trends Mol Med 27, 743–752 (2021).
Priante, E. et al. Intrauterine Growth Restriction: New Insight from the Metabolomic Approach. Metabolites 9, https://doi.org/10.3390/metabo9110267.
Pintus, R., Dessi, A., Mussap, M. & Fanos, V. Metabolomics can provide new insights into perinatal nutrition. Acta Paediatr 112, 233–241 (2023).
Griffin, J. L. et al. Metabolic profiling of rodent biological fluids via 1H NMR spectroscopy using a 1 mm microlitre probe. Analyst 127, 582–584 (2002).
Gonzalez-Covarrubias, V., Martinez-Martinez, E. & Del Bosque-Plata, L. The Potential of Metabolomics in Biomedical Applications. Metabolites 12, https://doi.org/10.3390/metabo12020194.
Roberts, L. D. & Gerszten, R. E. Toward new biomarkers of cardiometabolic diseases. Cell Metab 18, 43–50 (2013).
Roberts, L. D., Koulman, A. & Griffin, J. L. Towards metabolic biomarkers of insulin resistance and type 2 diabetes: progress from the metabolome. Lancet Diabetes Endocrinol 2, 65–75 (2014).
Horgan, R. P. et al. Changes in the metabolic footprint of placental explant-conditioned medium cultured in different oxygen tensions from placentas of small for gestational age and normal pregnancies. Placenta 31, 893–901 (2010).
Dessi, A. et al. Metabolomics in newborns with intrauterine growth retardation (IUGR): urine reveals markers of metabolic syndrome. J Matern Fetal Neonatal Med 24, 35–39 (2011).
Horgan, R. P. et al. Metabolic profiling uncovers a phenotypic signature of small for gestational age in early pregnancy. J Proteome Res 10, 3660–3673 (2011).
Favretto, D. et al. Cord blood metabolomic profiling in intrauterine growth restriction. Anal Bioanal Chem 402, 1109–1121 (2012).
Ivorra, C. et al. Metabolomic profiling in blood from umbilical cords of low birth weight newborns. J Transl Med 10, 142 (2012).
Bobinski, R., Mikulska, M., Mojska, H. & Simon, M. Comparison of the fatty acid composition of maternal blood and cord blood of mothers who delivered healthy full-term babies, preterm babies, and full-term small for gestational age infants. J Matern Fetal Neonatal Med 26, 96–102 (2013).
Ryckman, K. K. et al. The influence of maternal disease on metabolites measured as part of newborn screening. J Matern Fetal Neonatal Med 26, 1380–1383 (2013).
Sanz-Cortes, M. et al. Metabolomic profile of umbilical cord blood plasma from early and late intrauterine growth restricted (IUGR) neonates with and without signs of brain vasodilation. PLoS One 8, e80121 (2013).
Dessi, A. et al. Investigation of the (1)H-NMR based urine metabolomic profiles of IUGR, LGA and AGA newborns on the first day of life. J Matern Fetal Neonatal Med 27, 13–19 (2014).
Maitre, L. et al. Urinary metabolic profiles in early pregnancy are associated with preterm birth and fetal growth restriction in the Rhea mother-child cohort study. BMC Med 12, 110 (2014).
Sulek, K. et al. Hair metabolomics: identification of fetal compromise provides proof of concept for biomarker discovery. Theranostics 4, 953–959 (2014).
Liu, J., Chen, X. X., Li, X. W., Fu, W. & Zhang, W. Q. Metabolomic research on newborn infants with intrauterine growth restriction. Medicine (Baltimore) 95, e3564 (2016).
Abd El-Wahed, M. A., El-Farghali, O. G., ElAbd, H. S. A., El-Desouky, E. D. & Hassan, S. M. Metabolic derangements in IUGR neonates detected at birth using UPLC-MS. Egypt J Med Hum Genet 18, 281–287 (2017).
Visentin, S. et al. Medium chain fatty acids in intrauterine growth restricted and small for gestational age pregnancies. Metabolomics 13, 54 (2017).
Delplancke, T. D. J. et al. Analysis of sequential hair segments reflects changes in the metabolome across the trimesters of pregnancy. Sci Rep 8, 36 (2018).
Lu, Y. P. et al. Cord blood lysophosphatidylcholine 16: 1 is positively associated with birth weight. Cell Physiol Biochem 45, 614–624 (2018).
Miranda, J. et al. Metabolic profiling and targeted lipidomics reveals a disturbed lipid profile in mothers and fetuses with intrauterine growth restriction. Sci Rep 8, 13614 (2018).
Bahado-Singh, R. O. et al. Artificial intelligence and the analysis of multi-platform metabolomics data for the detection of intrauterine growth restriction. PLoS One 14, e0214121 (2019).
Alfano, R. et al. A multi-omic analysis of birthweight in newborn cord blood reveals new underlying mechanisms related to cholesterol metabolism. Metabolism 110, 154292 (2020).
Briana, D. D. et al. Early human-milk metabolome in cases of intrauterine growth-restricted and macrosomic infants. JPEN J Parenter Enteral Nutr 44, 1510–1518 (2020).
Clinton, C. M. et al. Non-targeted urinary metabolomics in pregnancy and associations with fetal growth restriction. Sci Rep 10, 5307 (2020).
Kan, N. E. et al. [Analysis of metabolic pathways in intrauterine growth restriction]. Biomed Khim 66, 174–180 (2020).
Sovio, U. et al. A maternal serum metabolite ratio predicts fetal growth restriction at term. Nat Med 26, 348–353 (2020).
Welch, B. M. et al. Longitudinal profiles of plasma eicosanoids during pregnancy and size for gestational age at delivery: A nested case-control study. PLoS Med 17, e1003271 (2020).
Beken, S. et al. Early postnatal metabolic profile in neonates with different birth weight status: a pilot study. Front Pediatr 9, 646860 (2021).
Byeon, S. K. et al. Maternal serum lipidomics identifies lysophosphatidic acid as a predictor of small for gestational age neonates. Mol Omics 17, 956–966 (2021).
Morillon, A. C. et al. Glycerophospholipid and detoxification pathways associated with small for gestation age pathophysiology: discovery metabolomics analysis in the SCOPE cohort. Metabolomics 17, 5 (2021).
Moros, G. et al. Insights into intrauterine growth restriction based on maternal and umbilical cord blood metabolomics. Sci Rep 11, 7824 (2021).
Schupper, A. et al. Metabolic biomarkers of small and large for gestational age newborns. Early Hum Dev 160, 105422 (2021).
Youssef, L. et al. Paired maternal and fetal metabolomics reveal a differential fingerprint in preeclampsia versus fetal growth restriction. Sci Rep 11, 14422 (2021).
Bahado-Singh, R. O. et al. Metabolomic identification of placental alterations in fetal growth restriction. J Matern Fetal Neonatal Med 35, 447–456 (2022).
Chao de la Barca, J. M. et al. A Metabolomic Profiling of Intra-Uterine Growth Restriction in Placenta and Cord Blood Points to an Impairment of Lipid and Energetic Metabolism. Biomedicines 10, https://doi.org/10.3390/biomedicines10061411 (2022).
Gonzalez-Riano, C. et al. Birth Weight and Early Postnatal Outcomes: Association with the Cord Blood Lipidome. Nutrients 14, https://doi.org/10.3390/nu14183760 (2022).
Karaer, A., Mumcu, A., Arda Duz, S., Tuncay, G. & Dogan, B. Metabolomics analysis of placental tissue obtained from patients with fetal growth restriction. J Obstet Gynaecol Res 48, 920–929 (2022).
Liu, Q. et al. Analysis of amino acids and acylcarnitines profiles in small, appropriate, and large for gestational age neonates. J Matern Fetal Neonatal Med 35, 439–446 (2022).
McCarthy, M. E. et al. The independent and combined influences of small for gestational age and socioeconomic status on newborn metabolite levels. J Matern Fetal Neonatal Med 35, 6192–6198 (2022).
Umeda, N., Hirai, T., Ohto-Nakanishi, T., Tsuchiya, K. J. & Matsuzaki, H. Linoleic acid and linoleate diols in neonatal cord blood influence birth weight. Front Endocrinol 13, 986650 (2022).
Voerman, E. et al. Associations of maternal and infant metabolite profiles with foetal growth and the odds of adverse birth outcomes. Pediatr Obes 17, e12844 (2022).
Bartho, L. A. et al. Plasma lipids are dysregulated preceding diagnosis of preeclampsia or delivery of a growth restricted infant. EBioMedicine 94, 104704 (2023).
Chen, F. et al. Non-Targeted Metabolomic Study of Fetal Growth Restriction. Metabolites 13, https://doi.org/10.3390/metabo13060761 (2023).
Elhakeem, A. et al. Effect of common pregnancy and perinatal complications on offspring metabolic traits across the life course: a multi-cohort study. BMC Med 21, 23 (2023).
Jafri, L. et al. Metabolomics of a neonatal cohort from the Alliance for Maternal and Newborn Health Improvement biorepository: Effect of preanalytical variables on reference intervals. PLoS One 18, e0279931 (2023).
Priante, E. et al. Metabolomic profiling of intrauterine growth-restricted preterm infants: a matched case-control study. Pediatr Res 93, 1599–1608 (2023).
Tao, Z. et al. Alterations in the gut microbiome and metabolisms in pregnancies with fetal growth restriction. Microbiol Spectr 11, e0007623 (2023).
Troisi, J. et al. Placental Metabolomics of Fetal Growth Restriction. Metabolites 13, https://doi.org/10.3390/metabo13020235 (2023).
Yang, Z. et al. Altered distribution of fatty acid exerting lipid metabolism and transport at the maternal-fetal interface in fetal growth restriction. Placenta 139, 159–171 (2023).
Yeum, D. et al. Associations of maternal plasma and umbilical cord plasma metabolomics profiles with birth anthropometric measures. Pediatr Res 94, 135–142 (2023).
Zhai, X. et al. Nontargeted metabolomics reveals the potential mechanism underlying the association between birthweight and metabolic disturbances. BMC Pregnancy Childbirth 23, 14 (2023).
Wu, G. Functional amino acids in nutrition and health. Amino Acids 45, 407–411 (2013).
Hedden, M. P. & Buse, M. G. General stimulation of muscle protein synthesis by branched chain amino acids in vitro. Proc Soc Exp Biol Med 160, 410–415 (1979).
Anthony, J. C. et al. Leucine stimulates translation initiation in skeletal muscle of postabsorptive rats via a rapamycin-sensitive pathway. J Nutr 130, 2413–2419 (2000).
Anthony, J. C., Anthony, T. G., Kimball, S. R., Vary, T. C. & Jefferson, L. S. Orally administered leucine stimulates protein synthesis in skeletal muscle of postabsorptive rats in association with increased eIF4F formation. J Nutr 130, 139–145 (2000).
Mogami, H. et al. Isocaloric high-protein diet as well as branched-chain amino acids supplemented diet partially alleviates adverse consequences of maternal undernutrition on fetal growth. Growth Horm IGF Res 19, 478–485 (2009).
Yao, M. et al. The Exploration of Fetal Growth Restriction Based on Metabolomics: A Systematic Review. Metabolites 12, https://doi.org/10.3390/metabo12090860 (2022).
Alseekh, S. et al. Mass spectrometry-based metabolomics: a guide for annotation, quantification and best reporting practices. Nat Methods 18, 747–756 (2021).
Stroup, D. F. et al. Meta-analysis of observational studies in epidemiology: a proposal for reporting. Meta-analysis Of Observational Studies in Epidemiology (MOOSE) group. JAMA 283, 2008–2012 (2000).
Lumbreras, B. et al. QUADOMICS: an adaptation of the quality assessment of diagnostic accuracy assessment (QUADAS) for the evaluation of the methodological quality of studies on the diagnostic accuracy of ‘-omics’-based technologies. Clin Biochem 41, 1316–1325 (2008).
Whiting, P. F. et al. QUADAS-2: a revised tool for the quality assessment of diagnostic accuracy studies. Ann Intern Med 155, 529–536 (2011).
Pang, Z. et al. MetaboAnalyst 5.0: narrowing the gap between raw spectra and functional insights. Nucleic Acids Res 49, W388–W396 (2021).
Acknowledgements
This research was supported by a grant (INV029003) from the Bill & Melinda Gates Foundation. The funder had no role in the design or conduct of the study; collection, management, analysis, or interpretation of the data; preparation, review or approval of the manuscript or the decision to submit the manuscript for publication.
Author information
Authors and Affiliations
Contributions
A.C-A., J.V., and M.R. conceived and designed the study. A.C-A. and M.R. performed the literature search. A.C-A. and J.V. selected the studies, assessed their risk of bias, and extracted data. A.C-A. performed the data analysis. A.C-A. and J.V. wrote the initial draft. All authors (A.C-A., J.V., M.R., A.T.P., L.D.R., and S.H.K.) contributed to the data interpretation, revised the manuscript for important intellectual content, and approved the final version of the manuscript for publication. J.V. and S.H.K. acquired funding.
Corresponding authors
Ethics declarations
Competing interests
A.T.P. is supported by the Oxford Partnership Comprehensive Biomedical Research Centre with funding from the NIHR Biomedical Research Centre (BRC) funding scheme. The views expressed herein are those of the authors and not necessarily those of the NHS, the NIHR, the Department of Health or any of the other funders. All other authors declare no competing interests.
Peer review
Peer review information
Nature Communications thanks Valentina Bucher and the other anonymous reviewer(s) for their contribution to the peer review of this work. A peer review file is available.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Source data
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Conde-Agudelo, A., Villar, J., Risso, M. et al. Metabolomic signatures associated with fetal growth restriction and small for gestational age: a systematic review. Nat Commun 15, 9752 (2024). https://doi.org/10.1038/s41467-024-53597-4
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41467-024-53597-4
