
Abstract
Patients with Wilms tumour have benefited from the results of decades of large collaborative clinical trials, leading to improved care. In the National Wilms Tumor Study Group and now Children’s Oncology Group (COG) trials, risk stratification evolved and expanded with each generation of studies and, therefore, ensuring that each patient receives the appropriate therapy has become increasingly complex. A new risk stratification system has been developed that forms the basis of the upcoming COG favourable-histology Wilms tumour (FHWT) study. Topics of diagnostic and prognostic uncertainty, such as the findings of tumour pulmonary emboli or extra-abdominal lymphadenopathy at diagnosis, will be integrated into the central review determination of staging of FHWT by committee consensus to facilitate clinical classification for therapeutic studies. Clear documentation of the elements of current risk stratification are of particular importance as refinement of the classification of patients with FHWT continues in an effort to optimize research, personalize treatment and provide an educational resource.
Similar content being viewed by others


Introduction
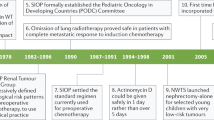
Great advances have been made in the field of paediatric oncology in the treatment of patients with Wilms tumour through sequential, collaborative group clinical trials conducted by the National Wilms Tumor Study (NWTS) Group (NWTSG), Children’s Oncology Group (COG) and the International Society of Paediatric Oncology (SIOP) Renal Tumour Study Group (RTSG)1,2,3. Most patients (~94%) with Wilms tumour have favourable-histology Wilms tumour (FHWT)4, and tremendous progress in its treatment has occurred, with survival now exceeding 90%, despite very few new chemotherapy agents being introduced in the past six decades. Most of this progress is attributable to serial randomized clinical trials, the results of which helped to define optimal treatment of patients with FHWT, and enabled the refinement of risk-stratification.
In NWTSG trials, risk stratification was based on stage, then also histology, and subsequently age and tumour weight were integrated. Tumour molecular analysis5 and metastatic site response to chemotherapy6 have now also been incorporated into COG trial risk stratification (Tables 1 and 2). In the completed COG FHWT studies AREN0532 and AREN0533 studies, both intensified and de-intensified treatment strategies were examined, with an overarching goal of maintaining or improving outcomes while decreasing toxic effects for patients with FHWT7,8,9. Novel prognostic features were discovered for subsets of patients enrolled in those studies10,11,12, and from ongoing analyses of previous studies13,14, leading to the need to further refine risk stratification for FHWT.
In this Consensus Statement, we describe the details of the evolution of risk-based treatment of FHWT and outline the rationale for the new risk stratification that will be used in the recently opened COG therapeutic trial for FHWT, AREN2231. We highlight prognostic factors that have previously been studied in prospective clinical trials, and those that have been identified through retrospective analyses of trial data but will be incorporated into risk-adapted treatment for the first time on AREN2231. Additionally, we highlight areas of diagnostic and prognostic uncertainty, albeit rare, which, out of necessity for clinical classification for therapeutic studies, have been integrated into the central review determination of staging of FHWT by expert consensus rather than based on conclusive data. These topics are of particular importance as we aspire to continue to refine patient classification to optimize treatment and research.
Methods
This review of risk stratification has been developed by a multidisciplinary group of COG Renal Tumor Committee members, including paediatric oncologists, surgeons, radiologists, pathologists, radiation oncologists, biostatisticians and other investigators. The Renal Tumor Committee has a structured leadership with appointed Chair, Vice Chair and leads for each of the disciplines. Committee members are invited to the committee based on demonstrated interest and expertise in the care and study of children and young adults with renal tumours. Primary authors of this paper were members of the FHWT working group, most of whom are also primary authors of the current COG therapeutic trial AREN2231 (Risk Adapted Therapy for Unilateral FHWT). The FHWT working group was established by Renal Tumor Committee leadership to include current and past committee chairs and vice chairs, current and past study chairs and vice chairs of FHWT tumour trials, as well as relevant committee discipline leads and members. This group has extensive collective experience in the conduct and analysis of clinical trials for FHWT, including designing and implementing the AREN03B2 risk assignment processes and determinations for patients with FHWT over the last 20 years. COG study AREN03B2, the Renal Tumor Classification, Biology and Banking study, opened in 2006 as an overarching study to classify patients with renal tumours through real-time expert panel review and risk stratification, to define eligibility for, and support conduct of, therapeutic trials, and to develop a well-annotated tumour bank to support clinical and translational research into children with renal tumours1,15.
To develop a new COG study for patients with FHWT, this group revised the risk stratification system that was developed and adopted for the first generation of COG ‘AREN’ therapeutic studies16. Through deliberations in regular videoconferences and teleconferences and at annual, multiple-day, in-person meetings, the study committee designed the revised system based on new data that became available through both prospective and retrospective analyses of patients with FHWT treated or followed from the NWTS-5, AREN03B2, AREN0532, AREN0533 and AREN0534 clinical trials. We reviewed and have included pertinent literature when available, including relevant publications from the NWTSG, COG and SIOP, when applicable. Each potential risk factor was discussed to reach a unanimous agreement amongst the multidisciplinary study committee about which factors should be used for risk stratification in the prospective therapeutic trial under development. In the very rare situation in which definitive data guiding whether to integrate a particular clinical feature into risk stratification was absent, the feature was debated based on available data as well as on real-world stratification challenges faced in AREN03B2 until unanimous expert agreement (or lack of dissent) was reached among the multidisciplinary members of the study committee.
Risk stratification
Risk stratification has become increasingly complex since the first NWTSG study, NWTS-1 (Table 2).
Evolution of risk stratification
In NWTS-1 and NWTS-2, patients were only stratified by stage17,18. In the subsequent two studies, NWTS-3 and NWTS-4, tumour histology (favourable or unfavourable) was incorporated into stratified treatment19,20. Finally, in NWTS-5, two new variables, patient age and tumour nephrectomy weight (TNW), were added to stratification5,21. The results of these five NWTSG studies established the clinical and biological features employed for risk stratification in the initial series of COG ‘AREN’ therapeutic studies16 (Table 1). These features include stage, histology (including post-chemotherapy histology for patients with bilateral or predisposed Wilms tumour), age, TNW, loss of heterozygosity (LOH) of 1p and 16q, response of pulmonary metastases to chemotherapy and the presence of extrapulmonary metastases. Chemotherapy regimens studied and currently used in risk-adapted, first-line treatment of FHWT include EE-4A, DD-4A, VAD, regimen I and regimen M (Table 3).
Evidence from previously conducted studies has informed the newly developed recommendations regarding the prognostic factors included in risk stratification, including prospectively studied factors, retrospectively studied factors and factors of less certain importance.
Prospectively studied prognostic factors
The prognostic features of stage, histology, age, TNW, LOH of 1p and 16q, response of pulmonary metastases to chemotherapy and the presence of extrapulmonary metastases have all been previously studied in prospective NWTSG or COG therapeutic studies, which has informed their use in the updated model.
Stage
In NWTSG and COG, FHWT is staged using a combination of radiological and surgicopathological staging (Table 4). Cross-sectional imaging of the chest, abdomen and pelvis is required for all patients, to determine the resectability of the tumour and for detection of metastatic and bilateral disease. Local (abdominal) stage is determined using surgicopathological staging from an initial diagnostic procedure. In the first NWTSG studies, patients with metastatic disease clearly had worse outcomes than those with localized disease treated with the same chemotherapy, although the study was not designed to demonstrate this difference17. Observations from subsequent studies have enabled narrowing of the outcome gap between patients with stages I and IV disease by use of intensified therapy strategies for increased stages8,9,11,22,23,24. Notably, either chest X-ray or CT scans were accepted for diagnosis of pulmonary metastases in the NWTS studies22. Results of the SIOP 2001 study showed that patients with CT-only lung nodules (nodules visible on CT but not visible on chest X-ray) had better outcomes than those with lung nodules visible on chest X-ray and worse outcomes than those with localized disease25. In NWTS study results, patients with CT-only lung nodules had improved event-free survival (EFS) when treated with intensified chemotherapy, thereby supporting prognostic value and enhancing risk stratification; therefore, CT scans are now required for staging22.
Patients with stage V (bilateral) FHWT have historically experienced poor outcomes26. In AREN0534, the first prospective study involving these patients, an intensified neoadjuvant chemotherapy regimen was adopted and delayed nephrectomy histology was incorporated to determine the subsequent treatment regimen27. Markedly improved outcomes (4-year EFS 84.2%) were achieved using this approach compared with patients treated using NWTSG study approaches (4-year EFS 65%)27. Except when explicitly stated, throughout this manuscript the discussion of features incorporated into risk stratification pertain to unilateral FHWT. The influence of features such as LOH of 1p and 16q and lung metastatic response to chemotherapy on bilateral FHWT is currently uncertain but is an area of active investigation.
Subtle changes to staging definitions have occurred over time; therefore, stage shifting needs to be considered. For example, in NWTSG studies, intraoperative local tumour spill that was confined to the flank, which also applied to the rare patients who had a biopsy and then subsequently underwent complete nephrectomy before starting chemotherapy, was not considered an indication for stage III designation11. However, in COG studies, any biopsy or local tumour spill was designated as stage III, after recognizing that patients who had local tumour spill but otherwise met stage II criteria experienced an increased risk of local recurrence28,29,30 (Table 4). The terms ‘spill’ and ‘rupture’ have historically been inconsistently defined and used, and at times conflated in previous studies and analyses; thus, ‘spill’ will be clearly defined in future COG studies to be an intraoperative event involving tumour capsule disruption at the time of surgery (including biopsy), whereas ‘rupture’ will be defined as a preoperative event leading to tumour capsule disruption, determined either intraoperatively by the surgeon or identified by a pathologist. Because ‘rupture’ (regardless of symptoms or imaging findings) is an indication for whole-abdomen irradiation (WAI), this distinction is important for accurate risk stratification and therapy decisions. This distinction will be further emphasized in future COG studies to improve data collection and treatment decisions. Additionally, with widespread availability of CT scans and improved outcomes with detection of CT-only lung nodules, COG requires chest CTs for accurate staging.
Lymph-node sampling (LNS) is important for accurate staging. The presence of tumour within abdominal lymph nodes confers a local stage III designation and is a predictor of EFS and overall survival (OS)11,24. In NWTSG and COG staging, the finding of a non-viable tumour within a lymph node is considered lymph-node involvement. Enlarged abdominal lymph nodes on imaging are well established to be frequently reactive rather than involved with tumour; thus, surgical sampling is required for accurate staging31. In a Surveillance, Epidemiology and End Results and Florida Cancer Data System study, survival was observed to be lower for patients who did not undergo LNS than for those who did (5-year OS 87%) versus 1–5 (91%); 6–10 (93%); or >10 (95%) lymph nodes sampled (P = 0.005). A survival advantage for patients having 1–5 lymph nodes (hazard ratio (HR) 0.6, P = 0.016), 6–10 lymph nodes (HR 0.521, P = 0.048), and >10 lymph nodes (HR 0.403, P = 0.039) sampled compared with patients with zero lymph nodes examined was shown on multivariate analysis32. In NWTS-5, failure to sample lymph nodes was associated with an increased risk of relapse in patients with stages I or II disease, suggesting that some patients had undetected lymph node involvement (that is, really had stage III disease) owing to the absence of LNS33. Similarly, in AREN0532, a non-statistically significantly reduced EFS was observed in patients who did not have LNS, with 4-year EFS of 84% among patients with stage III disease without LNS (n = 148) versus 89% (n = 387, P = 0.067) in those with LNS11. A combined analysis of AREN03B2 and AREN0532 showed improved outcomes for patients with stage III disease who had LNS (4-year EFS 90.3%) relative to those without LNS (EFS 80.0%, P = 0.0037)34.
A review of the National Cancer Database showed that lymph nodes are not sampled in 10–15% of patients35, and in AREN03B2, failure to sample lymph nodes was the most common surgical protocol violation36. The likelihood of finding a positive lymph node increases with increasing number of lymph nodes sampled37,38, en bloc sampling increases the number of lymph nodes sampled39, and sampling between 6 and 10 lymph nodes decreases the false-negative rate to <10%35. Formal lymph-node dissection (such as retroperitoneal lymph-node dissection) is not necessary; however LNS is required for accurate staging. In previous NWTSG and COG Wilms tumour studies, patients were staged and enrolled without LNS as if their lymph nodes were negative, meaning that a patient could be assigned stages I or II without examination of an uninvolved lymph node40. For future COG unilateral FHWT trials, patients will be ineligible if LNS does not occur. Any patient either ineligible for enrolment (upfront nephrectomy without LNS) or removed (enrolled, delayed nephrectomy without LNS) will receive whatever treatment their treating institution or team recommends. The COG is a research organization and does not provide guidance regarding individual patient management outside the confines of research protocols.
Histology
The presence of anaplasia was first recognized as an adverse prognostic factor owing to the results of NWTS-1 (ref. 41). It was subsequently shown to indicate chemotherapy resistance and tumour aggressiveness42, and incorporated into risk stratification. Tumours with anaplasia were classified as unfavourable histology in NWTS-3 and subsequent studies19. Identification of anaplasia, and its classification as focal or diffuse43, can be a challenge. Tumour heterogeneity means that anaplasia is often not discovered on biopsy but is identified subsequently, when the entire tumour is removed42,44, which is one reason among others why the COG advocates for upfront nephrectomy. Additionally, use of central pathology review has identified that many patients with diffuse anaplasia are not recognized as having anaplasia on institutional pathology review42,45, which highlights the value of pathological expertise in making this diagnosis. This observation is a key factor that prompted the requirement for centralized pathology review for eligibility in COG Wilms tumour trials.
The COG integrates post-chemotherapy histology into risk stratification for patients with bilateral FHWT, treating these patients with neoadjuvant chemotherapy and resection, followed by adjuvant treatment based on stage and histological classification, which has been adapted from the SIOP classification but is not identical to it2,46,47,48. In the upcoming unilateral FHWT trial, histological types that affect potential de-escalation or escalation of therapy will include upfront epithelial Wilms tumour, and post-chemotherapy completely necrotic or blastemal-predominant Wilms tumour.
Age
In NWTS-1, age <2 years was identified as a favourable prognostic factor in a subset of patients with stage I disease17, although the results of NWTS-2 suggested that the inferior outcomes observed among patients of increased age were attributable to advanced stage or anaplastic histology18. In one United Kingdom Childhood Cancer Study Group (UKCCSG) analysis, increased age was associated with poor survival in those with stage I disease when treated with vincristine only49, with results of other UK studies showing age >4 years to be an independent risk factor49,50. Age has not been shown to be significant in other multivariate analyses30,51,52. In SIOP–RTSG studies, age cohorts with cut-off points of 2, 4 or 10 years of age were associated with inferior EFS compared with age 6 months to 2 years in multivariate analyses; however, OS was not significantly different except in patients >4 years50. In NWTS-4, age >4 years lost significance as an adverse prognostic factor when adjusted for histology and lymph-node involvement53. For patients with stage I FHWT enrolled in AREN03B2, no association with age and EFS was demonstrated54.
Age has not been used in risk stratification for patients with high-stage FHWT. Some data indicate that substantially older (≥15 years) patients with Wilms tumour (‘adult Wilms tumour’ or ‘adolescent and adult Wilms tumour’) have poor outcomes55,56; however, the reasons for this observation are unclear. Hypotheses for differential outcomes include possible differences in tumour genetics or treatment tolerance55,57,58,59.
Tumour nephrectomy weight
The combination of age <2 years and TNW (the weight of the nephrectomy specimen including tumour and kidney) <550 g was identified as a favourable characteristic of FHWT in the 1970s60,61. Increasing intensity of treatment did not improve the outcome of patients with these characteristics; therefore, chemotherapy might not be necessary61. An initial study including eight patients with these characteristics treated without chemotherapy resulted in only one recurrence, which occurred as a metachronous tumour in the contralateral kidney in a child with a genitourinary anomaly, raising the possibility of a genetic predisposition (new primary tumour rather than relapse)62. Analyses of NWTSG studies suggested that the risks of adjuvant chemotherapy might outweigh the benefits for this subset of patients63,64, subsequently termed having very-low-risk (VLR) Wilms tumour.
Validation of a very-low-risk subgroup
In NWTS-5 patients with VLR Wilms tumour were hypothesized to maintain excellent outcomes without chemotherapy21. Results showed that 5-year EFS was 84% and 5-year OS was 98% among 77 patients with VLR disease treated initially with surgery alone65. The study was closed when the EFS fell below 85% meeting prespecified study closure parameters; however, because OS remained high, the strategy of surgery only was further studied in AREN0532, in which 116 patients with VLR disease (requiring real-time central review confirming negative lymph nodes, and lack of a predisposition syndrome or radiological contralateral nephrogenic rests) were enrolled7. The results of this study demonstrated excellent results, with 4-year EFS of 89.7% and 4-year OS of 100%7.
Loss of heterozygosity of 1p and 16q
Analysis of NWTS-3 and NWTS-4 studies showed that LOH of 1p or 16q, present in 12% and 17% of patients with FHWT, respectively, was associated with reduced relapse-free survival and OS66. In NWTS-5, the hypothesis that LOH at these loci was associated with a poor prognosis was prospectively tested5. Risk of relapse and death was increased with either, and the worst outcomes occurred in patients with combined LOH of both 1p and 16q (henceforth referred to as ‘combined LOH’)5. In AREN0532 and AREN0533, intensified therapy for patients with combined LOH was prospectively studied, improving survival to a 4-year EFS of 87.3% for stages I or II (versus 68.8% in NWTS-5, P = 0.042), and 90.2% for stages III or IV (versus 61.3% in NWTS-5, P = 0.001)9.
Lung metastatic response to chemotherapy
In NWTSG studies, all patients with pulmonary metastases identified on chest X-ray were treated with whole-lung irradiation (WLI), whereas radiotherapy for CT-only lung metastases was left to the discretion of the treating institution22. Differential outcomes for patients with complete versus incomplete response of lung nodules to an initial 6 weeks of chemotherapy were first identified in SIOP studies67. In AREN0533, de-intensification of therapy (continued DD-4A with omission of WLI) for patients with lung-only metastases with rapid complete response (RCR) of pulmonary nodules to two cycles of chemotherapy, and intensification (regimen M with WLI) for those whose pulmonary disease had a slow incomplete response (SIR) after two cycles, were prospectively studied. Patients with RCR had a 4-year EFS of 79.5% (versus an expected 85% based on NWTS-5) and an OS of 96%; and those with SIR had an EFS of 90% (versus an expected 75%) and OS of 96%8. 1q status had a substantial effect on the EFS of patients with RCR, but not those with SIR.
Extrapulmonary metastases
Most patients with stage IV FHWT present with pulmonary metastases alone, but others present with extrapulmonary metastases with or without lung involvement, with liver being the most common extrapulmonary metastatic site68. In NWTS-4 and NWTS-5, there was no significant difference in EFS or OS between patients with stage IV FHWT with liver (with or without lung metastases) (n = 96) and those with stage IV FHWT with lung-only metastases (n = 513)68. In AREN0533, patients with extrapulmonary metastases were assigned to chemotherapy with regimen M, intensified from DD-4A received in NWTS-5. In a COG analysis in which patients with extrapulmonary metastases from NWTS-5, AREN0533 and AREN03B2 were pooled, outcomes were inferior for patients with extrapulmonary metastases (observed 4-year EFS of 77.3%)69, compared with those with lung-only stage IV (EFS 85.4%) treated using the AREN0533 treatment strategy8. No statistical differences in EFS or OS were found between patients with extrapulmonary metastases treated in AREN0533 compared with those in NWTS-5, but the small cohort sizes, heterogeneous patient characteristics and metastatic sites, flawed data collection, and lack of consistent local control management confounded assessment of the role of regimen M; thus, the optimal chemotherapy for patients with extrapulmonary metastases remains uncertain69. The role and quality of evidence supporting local treatments of sites of extrapulmonary metastases vary by metastatic site. Radiotherapy is recommended for nearly all metastatic sites, but the role of surgery for extrapulmonary metastases is not certain, and has not been strictly prescribed or reported in past studies.
Apart from metastatic sites of the liver, brain and bones, the specifics of what defines extrapulmonary metastasis have not been clearly established. For the purposes of AREN03B2 and AREN0533, certain findings (such as pulmonary tumour emboli, malignant pleural effusions and extra-abdominal lymph nodes (cervical and intrathoracic or mediastinal)), when identified at institutional review, were consistently designated as extrapulmonary metastases, a decision made by consensus opinion of the central reviewers, and not based on data. Notably, peritoneal implants or pelvic tumours identified at diagnosis, presumed to be a result of local ‘drop mets’ from tumour rupture rather than haematogenous spread, are not considered sites of extrapulmonary metastases.
Retrospectively studied prognostic factors
Some prognostic features of FHWT have been identified retrospectively, and have yet to be prospectively studied or integrated into risk stratification. These include epithelial histology; 1q gain; LOH 11p15; combination of LN involvement with isolated LOH of 1p or 16q; and post-chemotherapy blastemal-predominant histology in the COG treatment context.
Features relevant to very-low-risk disease
Features relevant to VLR disease include molecular characteristics, epithelial histology and TNW.
Molecular features of VLR disease can be used to predict risk of relapse. The results of AREN0532 validated findings from NWTS-5 that LOH of 11p15 is associated with relapse in patients with VLR Wilms tumour treated without chemotherapy5,7. LOH of 11p15 was present in 37% of patients with VLR Wilms tumour (40 of 108), with 20% (8 of 40) experiencing disease relapse, accounting for 67% of all VLR relapses (8 of 12)7. Loss of imprinting of 11p15 was present in 7.4% (8 of 108 patients), and was also associated with relapse in 25% (2 of 8 patients). Combined LOH of 1p and 16q was rare in patients with VLR (3 of 108); 33% (1 of 3 patients) relapsed, but small numbers preclude statistical conclusions from being drawn7. Last, 1q gain, a poor prognostic factor in stage I (non-VLR) disease in NWTS-5 (ref. 53) and in higher stage disease14, was found in 5.5% (6 of 108) of patients with VLR. Of these 6 patients, 1 experienced relapse, but small numbers limit conclusions about its prognostic influence in patients with VLR disease7.
Regarding epithelial histology, Wilms tumours are designated as ‘predominant’ for a particular histopathological component (epithelial, blastemal or stromal) if that component comprises >66% of the tumour histology45. The importance of post-chemotherapy Wilms tumour histological classification is well-described by SIOP46 and increasingly in the COG context, but the importance of pre-chemotherapy histology is less clear. To evaluate the hypothesis that epithelial-predominant Wilms tumours might not require adjuvant chemotherapy70, patients with stage I epithelial-predominant Wilms tumour in AREN03B2 (n = 177) were analysed. The results revealed a 4-year EFS of 96.2% and OS of 100%71. Overall, 117 patients received regimen EE-4A (4-year EFS of 96.1%), and 57 had nephrectomy only (4-year EFS of 98.2%); P = 0.549 (ref. 71). Low-risk epithelial Wilms tumour has been associated with TRIM28 loss-of-function mutations72, further supporting the view that epithelial Wilms tumour is a distinct and favourable FHWT subtype, which can also be distinguished from metanephric tumours that harbour BRAF V600E mutation73,74,75.
Tumour weight was not prognostic in multivariate analysis of patients with stage I disease treated with vincristine monotherapy in a UKCCSG study49, despite previous results suggesting that it might be60,61,76. Analysis of 658 patients with stage I FHWT enrolled in AREN03B2 demonstrated that TNW had no significant association with EFS54. As TNW does not influence risk stratification for any other FHWT subgroups, whether TNW is a prognostic factor when other variables (for example, tumour biology) are considered is now uncertain.
1q gain
Retrospective analysis of data from NWTS-5 showed that 1q gain was associated with increased stage, present in 20%, 26%, 32% and 44% of stages I, II, III and IV, respectively, and had an adverse effect on survival (8-year EFS 77% versus 90%, P < 0.001) that was observed across stages14. This analysis showed that 1q gain and combined LOH are not independent events, and that in patients with 1q gain, combined LOH no longer influenced outcomes (however, it remains prognostic in the absence of 1q gain). The influence of 1q gain on survival is greatest among patients with stage IV disease (EFS 64% versus 91% and OS 74% versus 92%; all patients treated with DD-4A)14. Similar prevalence and differences in outcome by 1q gain status have been observed in SIOP studies77,78.
1q status was not prospectively incorporated into AREN0533, but retrospective examination of its influence in the stage IV lung-only group revealed that among patients with RCR (who received DD-4A without WLI), those with 1q gain had strikingly lower 4-year EFS than those without 1q gain (EFS 57% versus 86%, P = 0.0013)8. Patients in the SIR group (who received regimen M and WLI) with 1q gain had statistically similar outcomes to those without 1q gain (4-year EFS of 86% versus 92% (P = 0.15), and OS 93% versus 96% (P = 0.45))8, suggesting that the intensified regimen overcame the adverse prognostic importance of 1q gain in this subgroup.
Combination of lymph node involvement with isolated loss of heterozygosity
Data from AREN0532 demonstrated that patients with stage III disease with abdominal lymph nodes positive for tumour and with LOH of 1p or 16q (henceforth referred to as ‘isolated LOH’) had reduced EFS of 74% (OS 92%), whereas those with negative lymph nodes and without LOH had outstanding outcomes (EFS 97% and OS 99%)11. A subsequent analysis, in which data from similarly treated patients from AREN03B2 and AREN0532 were combined, supported the observation that patients with positive lymph nodes and isolated LOH have significantly worse 4-year EFS (77% versus 91%) than those with stage III disease with negative lymph nodes or no LOH (HR 3.01, P = 0.0004)34. These results reinforced the importance of LNS for prognostication and risk stratification.
Post-chemotherapy histology
A minority of patients (~20%) in the COG setting undergo upfront tumour biopsy and delayed nephrectomy after neoadjuvant chemotherapy11, owing to surgical contraindications to upfront nephrectomy. The influence of post-chemotherapy histology (classified using a system analogous to the one developed by SIOP2,11,46,48) was examined in AREN0532 for such patients with stage III disease resulting from initial diagnostic biopsy to confirm FHWT11. Low-risk histology was defined as completely necrotic, high-risk histology as blastemal-predominant histology and intermediate-risk histology encompassing all other non-anaplastic histologies. Outcomes varied by histology, with particularly poor outcomes among patients with high-risk histology (7 patients, 4-year EFS 28.6%) and favourable outcomes among those with low-risk (7 patients, EFS 100%) or intermediate-risk (63 patients, EFS 90.5%) histologies11.
Another retrospective study of data from patients with overall stage III or IV disease enrolled in AREN0532, AREN0533 or AREN03B2-only who underwent delayed nephrectomy supported the notion that patients with post-chemotherapy blastemal-predominant histology have the worst outcomes compared with other histologies, and patients with low-risk histology have the best outcomes12.
Peritoneal and pelvic metastases
Peritoneal and pelvic metastases are rare but should be looked for and noted by the surgeon at the time of the diagnostic procedure, as they confer a stage III designation and are an indication for WAI. Increased intra-abdominal recurrences occurred in NWTS-2 when radiotherapy fields were ‘too small’ (that is, flank radiotherapy when WAI was indicated)79. A review of patients with abdominal stage III disease enrolled in NWTS-4 and NWTS-5 showed that 57 of 1,584 (3.5%) had peritoneal metastases. The use of WAI for the majority (82%) of patients with peritoneal metastases in NWTS-4 and NWTS-5, along with resection and DD-4A chemotherapy resulted in EFS and OS that were similar to those with abdominal stage III disease without peritoneal metastases28.
Features of less certain importance
In staging Wilms tumour, several findings, such as tumour pulmonary emboli, pleural effusions, malignant ascites and enlarged extra-abdominal lymph nodes, with uncertain prognostic importance, are occasionally encountered, and their inclusion in staging decisions has been made for patients enrolled in AREN03B2 to facilitate cohesive clinical classification for therapeutic studies. For these situations, staging decisions were made by expert consensus among the multidisciplinary AREN03B2 study committee and central review expert panel in the absence of definitive published data (Table 5). Because these decisions determined disease stage, in some scenarios, they would have affected assigned treatments, including chemotherapy regimen and/or receipt of radiotherapy69.
Pleural effusions
In one single-centre study including 233 patients with Wilms tumour, pleural effusions were identified in 4.3% of patients, all occurring on the side of the primary kidney tumour. Only 2 of the 10 patients underwent thoracentesis (both were negative for tumour cells), and all 10 survived with stage-based treatment that was not adjusted for the effusion80. In a larger, multicentre study including 1,259 patients with Wilms tumour, 7.5% presented with a pleural effusion at diagnosis81. Overall, 14 of 94 underwent thoracentesis; 3 of these had malignant cells identified using cytology, all of whom had concomitant pulmonary metastatic disease81. Thoracentesis might help from a therapeutic perspective, but the diagnostic and prognostic implications are uncertain based on the existing literature. Nonetheless, current consensus is that pleural fluid with histologically identified malignant cells is considered a site of extrapulmonary metastasis and an indication for radiotherapy to the involved lungs and pleura.
Tumour pulmonary emboli
Tumour pulmonary emboli can be identified using diagnostic chest CT, particularly when performed with contrast medium. Because they are, by definition, haematogenous tumour spread, they have been, and will continue to be, considered extrapulmonary metastases and therefore an indication for radiotherapy69. The optimal radiotherapy field, either WLI or involved lungs, remains uncertain as it has not been specified or studied in previous FHWT trials.
Extra-abdominal lymph nodes
Lymph nodes outside the abdominal cavity (such as mediastinal, supraclavicular or cervical) that are pathologically confirmed to be Wilms tumour are considered to be extrapulmonary metastases; however, extra-abdominal lymph nodes are an uncommon site of Wilms tumour spread at initial presentation69 and not always pathologically examined. Furthermore, enlarged abdominal lymph nodes on imaging are frequently reactive rather than tumour metastases31. Thus, the prognostic and staging importance of enlarged extra-abdominal lymph nodes on cross-sectional imaging without pathological confirmation of Wilms tumour is uncertain, and providers must make a staging determination based on the clinical context of the patient.
Peritoneal fluid
The presence and characteristics of peritoneal fluid should be noted at the time of surgical resection as it can suggest preoperative tumour rupture82. Peritoneal fluid is sometimes sampled for cytology in patients with Wilms tumour83, although it occurs at the discretion of the surgeon and data surrounding this practice are limited. The finding of malignant cells in peritoneal fluid cytology can be a false positive (mononuclear and mesothelial cells can be difficult to distinguish)84, and even when truly positive, it is of uncertain importance83. Caution should be taken before deciding to alter therapy based on cytological evaluation (such as upstaging and/or consideration of WAI), because of poor evidence of the need or benefit of therapy intensification. Thus, in the upcoming COG unilateral FHWT trial, peritoneal fluid cytology will not be evaluated, nor will disease be upstaged or treatment altered based on the presence of malignant ascites.
Partial nephrectomy for unilateral Wilms tumour
In COG protocols, partial nephrectomy for unilateral Wilms tumours is only recommended for patients with Wilms tumour-predisposing conditions or a single functioning kidney in the setting of a nephron-sparing treatment approach, and should occur following neoadjuvant chemotherapy to maximize preservation of kidney parenchyma. In a study including 60 patients who did not have a condition predisposing them to Wilms tumour and had small tumours that were stage I after complete nephrectomy, just 5 (8%) were amenable to an upfront partial nephrectomy85, indicating that this approach should only rarely be considered. Performance of an upfront partial nephrectomy does not automatically yield a stage or risk adjustment, but positive margins are frequently found, which requires a designation of local stage III. In a study including 39 patients not predisposed to Wilms tumour in AREN03B2 who underwent an upfront partial nephrectomy, 9 (of the 11 with stage III disease) were upstaged for intraoperative tumour spill and/or microscopic residual tumour that probably would have been avoided with complete nephrectomy, exposing them to avoidable treatment intensification86. In the SIOP renal tumour protocols, partial nephrectomy for unilateral Wilms tumour is allowed; however, <3% of patients are deemed eligible by pre-defined criteria87.
The small tumours that might be amenable to upfront partial nephrectomy could also meet criteria for VLR Wilms tumour and be treated with nephrectomy only with excellent survival, and long-term kidney failure rates <1%7,65,88. Evidence suggests that in addition to loss of nephrons, reasons for eventual kidney failure include exposure to radiotherapy or anthracyclines89,90, so preventing treatment intensification for avoidable positive margins will also aid in the preservation of kidney function. Thus, partial nephrectomy for non-predisposed unilateral Wilms tumour is generally discouraged, but can be considered provided that the risks (including being ineligible for treatment with nephrectomy only in a study) and benefits are carefully considered and discussed with the family.
Unilateral multifocal tumours
Patients with unilateral multifocal Wilms tumour, defined as more than one discrete tumour in a single kidney91, were eligible for the nephron-sparing treatment approach in AREN0534 owing to the concern that they could be at an increased risk of developing of bilateral disease47. Treatment in COG unilateral protocols was also permitted for patients who underwent an upfront complete nephrectomy92,93. In AREN0534, patients treated with a nephron-sparing approach received preoperative EE-4A chemotherapy47; however, among the 10 enrolled patients only 4 underwent partial nephrectomy (6 underwent complete nephrectomy), with one experiencing relapse in the abdomen associated with a positive partial nephrectomy margin47. Examination of patients enrolled in AREN03B2 with unilateral multifocal Wilms tumour who underwent an upfront complete nephrectomy has not occurred. Defining who may benefit from a nephron-sparing surgical approach and who may be more optimally be managed with an upfront complete nephrectomy remains an area of active investigation. When upfront nephrectomy reveals multifocal tumours that are all FHWT, some clinicians perform molecular testing on more than one tumour94. The prognostic implication of disparate molecular findings is currently uncertain, so this practice is not considered standard. When performed, the highest risk biological feature should be incorporated into risk stratification.
Staging of multifocal tumours of different histologies
Pathological examination of multifocal tumours within a single kidney sometimes enables identification of different histologies (anaplastic versus FHWT) and stages for discrete tumours95. The overall stage and histology for each kidney is designated as the highest stage and ‘worst’ histology found, such that a kidney with a stage II tumour with diffuse anaplasia and a stage III tumour with FHWT would be classified as a stage III diffuse anaplastic Wilms tumour27,96.
Contralateral nephrogenic rests
Some patients with a large unilateral renal tumour are found to have a small lesion in the contralateral kidney on imaging97,98,99. Small lesions examined pathologically are often nephrogenic rests; however, the accuracy of imaging in the diagnosis of nephrogenic rests remains poor100. Some data indicate an optimal size cut-off of 1.75 cm to distinguish a nephrogenic rest from a Wilms tumour100. In AREN03B2, lesions ≥1 cm were centrally defined as ‘tumour’; however, final determination was performed by the sites for the purposes of treatment protocol risk assignments27. In AREN0534, the management of contralateral lesions depended on the number of lesions, their size, and the age of the patient27. Given the subjective nature of these criteria, until future data emerge, decisions concerning how to manage a patient with contralateral nephrogenic rests must be individualized.
Venous extension: inferior vena cava thrombus and renal vein margin
Tumour invasion of the renal vein, inferior vena cava (IVC) and atrium creates special treatment challenges. Renal vein tumour thrombi have been noted in 11% of patients with Wilms tumour, and caval and atrial involvement in 5% and 1% of patients with Wilms tumour, respectively101,102. Preoperative ultrasonography and CT will usually help to identify intravascular tumour extension; however, the renal vein and IVC should still be carefully palpated intraoperatively before ligation to rule out tumour extension82. Tumour extension into the renal vein and proximal IVC can in most cases be removed en bloc with the kidney33,103,104, affording the chance to be stage II when a negative margin is achieved. However, primary resection of tumours that extend up the IVC to the retro-hepatic IVC and particularly to the atrium is associated with increased operative morbidity102. In these circumstances, preoperative chemotherapy is the recommended approach (after biopsy of the primary tumour) to decrease the size and extent of the tumour thrombus and facilitate safer excision102.
After division of the renal vein, the vein border can retract103. In the setting of renal vein tumour thrombus extending towards the IVC, vein retraction can make the determination of margin status difficult. Direct communication between the surgeon and pathologist is crucial to determine the extent of invasion of the vein wall and tumour thrombus margin status for correct disease staging.
Tumours in the renal collecting system
Wilms tumours can extend into the renal pelvis and down the ureter105. During resection, the ureter should be palpated before its division to prevent transection of the tumour and upstaging of the tumour to stage III82,105. Gross haematuria might be a sign of tumour extension into the collecting system and warrants consideration of intraoperative, pre-nephrectomy cystoscopy with retrograde pyelogram, which could delineate the presence and extent of invasion105. Cystoscopic tumour biopsy results in a stage III designation.
Adrenal gland
Adrenal involvement is not an independent factor for poor prognosis106, and is designated stage II if resected en bloc with the tumour with a negative margin107. The adrenal gland can be left in situ at the time of nephrectomy; however, if it is abutting the tumour it should be removed en bloc with the tumour to avoid a positive margin106.
Extrarenal Wilms tumour
Wilm tumour sometimes originates outside of the kidney, most commonly in the retroperitoneum, but also in the pelvis and paraspinal or inguinal regions, among others108,109. Evidence suggests an association between extrarenal Wilms tumour and horseshoe kidneys, with coexistence of the two seen in almost 13% of reported instances in one series108. Most have favourable histology108, and patient outcomes are similar to those with intrarenal Wilms tumour109. Staging of extrarenal Wilms tumour has not always been defined in previous clinical trials, but for COG Wilms tumour studies, extrarenal Wilms tumour cannot be stage I as they are outside the renal parenchyma, and are stage II if resected with a negative margin, or stage III if biopsied or resected with a positive margin107. Given their rarity, no standardized treatment exists, although most seem to be managed similarly to intrarenal Wilms tumour108,109. Despite the limited data, extrarenal Wilms tumours are eligible for the upcoming FHWT clinical trial and will undergo the same risk stratification as intrarenal tumours, including the requirement for at least one lymph node to be sampled and pathologically confirmed on central review.
Genetic predisposition to Wilms tumour
Many children with Wilms tumour have syndromes that predispose to the development of Wilms tumour110, including Beckwith–Wiedemann syndrome/spectrum; idiopathic hemihypertrophy/isolated lateralized overgrowth; Denys–Drash syndrome; WAGR (Wilms tumour, aniridia, genitourinary anomalies, range of developmental delays) syndrome; trisomy 18; Simpson–Golabi–Behmel syndrome; and Bohring–Opitz syndrome111, with novel genes and syndromes emerging112. The presence of a predisposition syndrome has not been used in risk stratification per se; however, predisposed patients have been ineligible for the nephrectomy-only treatment strategy for VLR Wilms tumour, with the premise that nephron-sparing surgery should be prioritized in the management of patients who have a predisposition syndrome owing to their risk of chronic kidney disease88, and the belief that chemotherapy might prevent new tumour development113. Additionally, in AREN0534, for patients who underwent biopsy of a bilateral Wilms tumour (many of whom had a genetic predisposition), the biopsy was not (by itself) an indication for radiotherapy, whereas radiotherapy is indicated for all others who undergo biopsy27. This approach was based on the added risk of chronic kidney disease from radiotherapy to the preserved kidney.
Levels of evidence for factors that influence FHWT staging and treatment differ, but for the purposes of therapeutic clinical trial development in which similar patients must be assigned the same treatments, standardized and precisely defined staging is needed. The staging definitions used for the study and recommended surgical approaches to diagnostic nephrectomy are outlined in the protocol to help clinicians treating these patients.
Risk stratification recommendations
An updated FHWT risk stratification built on all the available data was needed to justify and support prospective clinical trials, and to inform accurate prognostication in routine clinical care. To develop the recently opened COG FHWT study AREN2231 the study committee reviewed outcomes from the first generation of COG AREN‘0’ clinical trials, including detailed analyses of patients who were similarly treated and followed only on the AREN03B2 study. The results of these analyses have resulted in an enhanced and expanded risk stratification schema (Table 6) that will be implemented and studied.
The updated risk stratification model
Analyses of features and outcomes of patients enrolled in the ‘AREN0’ studies have resulted in an enhanced and expanded risk stratification schema (Table 6) that will be implemented and studied in AREN2231. This new model incorporates biological and clinical features not included in the first-generation risk stratification, and modifies or omits some features previously used (Table 2). The COG 2024 FHWT risk stratification schema (Table 6) incorporates stage, histology, age, LOH of 1p and 16q, response of pulmonary metastases to chemotherapy, presence of extrapulmonary metastases, post-chemotherapy histology, LOH of 11p15, gain of 1q and lymph-node involvement. It eliminates TNW and includes modifications to how histology and age are used to stratify some patients.
The updated risk stratification model is primarily based on current established data; however, some aspects of risk stratification have been implemented without data-driven explorations (Table 5), owing to a compelling need for a consistent clinical staging classification to facilitate therapeutic study enrolment. For these clinical features, such as the presence of pleural effusions, malignant ascites, or tumour pulmonary emboli, the committee considered how staging has been assigned in previous studies, and in the absence of clinical data indicating a change to prior practices was indicated, chose to maintain consistency with prior staging decisions. This choice was unanimous, and motivated by the fact that some of the planned statistical analyses in AREN2231 will be compared with outcomes derived from the historical control cohort. We hope that by documenting these decisions and standardizing the staging definitions for these elements, we can generate needed data to consider future changes to the risk classification and treatment of additional FHWT subgroups. At a minimum, the transparency about how these decisions have been made for these small groups of patients will help to inform the care of patients with FHWT.
Recommendations to enable risk stratification
Accurate patient-specific information is required to ensure that each patient receives appropriate clinical care or clinical trial stratum assignment. To support AREN2231 and the clinical care of patients with FHWT, the study committee developed unanimous recommendations for the surgical management of Wilms tumour, collection of necessary tumour molecular biomarkers, and expert review of all clinical information that goes into risk stratification (Box 1).
First, all patients with a new unilateral renal tumour that could be Wilms tumour should have histological confirmation of the diagnosis, unless the patient has a known or suspected condition that predisposes to Wilms tumour. This recommendation is a longstanding in NWTSG and COG, and is not new to this study or risk stratification system. Second, the recommended upfront diagnostic procedure is a nephrectomy with LNS unless a contraindication to doing so exists. When upfront nephrectomy is not felt to be safe or feasible, tumour biopsy should be performed for histological confirmation, and should not be performed by fine-needle aspiration. These recommendations regarding diagnostic procedures are also consistent with NWTSG and COG practices and recommendations over recent decades.
Owing to the risk of missing anaplasia42,45, and for potential clinical trial eligibility, central review of histology by an expert renal tumour pathologist is recommended, which can occur through the COG APEC14B1 Project: EveryChild study for eligible patients. Once FHWT is diagnosed, diagnostic tumour tissue should be sent for molecular testing, which can detect prognostic abnormalities that are relevant for risk stratification, including LOH of 1p, 16q and 11p15, and gain of 1q. LOH of 1p and 16q have been previously studied in a prospective trial9, but the retrospective data on LOH of 11p15 (ref. 7) and gain of 1q (refs. 8,14) support changing clinical management for some patients with FHWT based on the results. Routine performance of this molecular testing has been recommended by the National Comprehensive Cancer Network clinical practice guideline for Wilms tumour114.
For patients with lung metastases at diagnosis, based on high-quality evidence from AREN0533 (ref. 8), a CT scan should be done after two cycles (6 weeks) of DD-4A chemotherapy to evaluate the response of these nodules, to determine the appropriate chemotherapy, radiation and surgical plans. Finally, because of the multidisciplinary nature of the management of FHWT and the way in which sometimes subjective decisions (for example, about which nodules count as metastases, or whether there was pre-operative tumour rupture) can influence staging and treatment, all patients’ tumour pathology, surgical findings, biology and imaging should be reviewed among all care providers, ideally in the context of a multidisciplinary tumour board.
Together these recommendations can ensure that each patient receives the most evidence-based and individualized care.
Conclusions
The overarching goal of clinical investigations into FHWT is to improve care by increasing survival for the patients who fare less well with current therapy than other patients with Wilms tumour, and minimizing potential toxic effects and late effects with reduction of therapy for subgroups who do very well with current therapy while preserving good clinical outcomes.
Updated risk stratification algorithms can help to ensure that patients receive accurate diagnostic, staging and biological assessments, leading to optimal treatment. The new risk stratification outlined in this Consensus Statement will enable enhanced personalized medicine. Findings from the COG study AREN2231 will probably lead to further refinement of this risk stratification in the future.
Last, the importance of risk stratification to improve care strongly underscores the crucial need for a multidisciplinary team approach to the care of patients with FHWT. Each subspecialty has a key and specific role in the risk stratification process. For optimal care, tumour pathology, surgical findings, biology and imaging should be reviewed among all care providers, ideally in the context of a multidisciplinary tumour board. This multidisciplinary article helps to facilitate the accurate determination of stage and risk stratification and ensures optimization of personalized treatment plans.
References
Dome, J. S. et al. Impact of the first generation of Children’s Oncology Group clinical trials on clinical practice for Wilms tumor. J. Natl Compr. Canc. Netw. 19, 978–985 (2021).
Dome, J. S. et al. Advances in Wilms tumor treatment and biology: progress through international collaboration. J. Clin. Oncol. 33, 2999–3007 (2015).
van den Heuvel-Eibrink, M. M. et al. Position paper: rationale for the treatment of Wilms tumour in the UMBRELLA SIOP-RTSG 2016 protocol. Nat. Rev. Urol. 14, 743–752 (2017).
Mullen, E. A. et al. Comprehensive update of pediatric renal tumor epidemiology: analysis of the first 4000 patients on Children’s Oncology Group renal tumor risk stratification and biology protocol AREN03B2. Pediatr. Blood Cancer 61, S166 (2014).
Grundy, P. E. et al. Loss of heterozygosity for chromosomes 1p and 16q is an adverse prognostic factor in favorable-histology Wilms tumor: a report from the national Wilms tumor study group. J. Clin. Oncol. 23, 7312–7321 (2005).
Verschuur, A. et al. Treatment of pulmonary metastases in children with stage IV nephroblastoma with risk-based use of pulmonary radiotherapy. J. Clin. Oncol. 30, 3533–3539 (2012).
Fernandez, C. V. et al. Clinical outcome and biological predictors of relapse after nephrectomy only for very low-risk Wilms tumor: a report from Children’s Oncology Group AREN0532. Ann. Surg. 265, 835–840 (2017).
Dix, D. B. et al. Treatment of stage IV favorable histology Wilms tumor with lung metastases: a report from the Children’s Oncology Group AREN0533 study. J. Clin. Oncol. 36, 1564–1570 (2018).
Dix, D. B. et al. Augmentation of therapy for combined loss of heterozygosity 1p and 16q in favorable histology Wilms tumor: a Children’s Oncology Group AREN0532 and AREN0533 study report. J. Clin. Oncol. 37, 2769–2777 (2019).
Perlman, E. J. et al. WT1 mutation and 11P15 loss of heterozygosity predict relapse in very low-risk Wilms tumors treated with surgery alone: a Children’s Oncology Group study. J. Clin. Oncol. 29, 698–703 (2011).
Fernandez, C. V. et al. Outcome and prognostic factors in stage III favorable-histology Wilms tumor: a report from the Children’s Oncology Group study AREN0532. J. Clin. Oncol. 36, 254–261 (2018).
Evageliou, N. et al. Post-chemotherapy blastemal-predominant Wilms tumor in the Children’s Oncology Group (COG) context: pooled outcomes data from studies AREN0532, AREN0533 and AREN03B2. Pediatr. Blood Cancer 69, S66–S67 (2022).
Gratias, E. J. et al. Gain of 1q is associated with inferior event-free and overall survival in patients with favorable histology Wilms tumor: a report from the Children’s Oncology Group. Cancer 119, 3887–3894 (2013).
Gratias, E. J. et al. Association of chromosome 1q gain with inferior survival in favorable-histology Wilms tumor: a report from the Children’s Oncology Group. J. Clin. Oncol. 34, 3189–3194 (2016).
Geller, J. I. et al. Children’s Oncology Group’s 2023 blueprint for research: renal tumors. Pediatr. Blood Cancer 70, e30586 (2023).
Dome, J. S. et al. Children’s Oncology Group’s 2013 blueprint for research: renal tumors. Pediatr. Blood Cancer 60, 994–1000 (2013).
D’Angio, G. J. et al. The treatment of Wilms’ tumor: Results of the national Wilms’ tumor study. Cancer 38, 633–646 (1976).
Breslow, N. et al. Prognosis for Wilms’ tumor patients with nonmetastatic disease at diagnosis — results of the second National Wilms’ Tumor Study. J. Clin. Oncol. 3, 521–531 (1985).
D’Angio, G. J. et al. Treatment of Wilms’ tumor. Results of the third national Wilms’ tumor study. Cancer 64, 349–360 (1989).
Green, D. M. et al. Effect of duration of treatment on treatment outcome and cost of treatment for Wilms’ tumor: a report from the National Wilms’ Tumor Study Group. J. Clin. Oncol. 16, 3744–3751 (1998).
Green, D. M. et al. Treatment with nephrectomy only for small, stage I/favorable histology Wilms’ tumor: a report from the National Wilms’ Tumor Study Group. J. Clin. Oncol. 19, 3719–3724 (2001).
Grundy, P. E. et al. Clinical significance of pulmonary nodules detected by CT and not CXR in patients treated for favorable histology Wilms tumor on national Wilms tumor studies-4 and -5: a report from the Children’s Oncology Group. Pediatr. Blood Cancer 59, 631–635 (2012).
Green, D. M. The treatment of stages I–IV favorable histology Wilms’ tumor. J. Clin. Oncol. 22, 1366–1372 (2004).
Ehrlich, P. F. et al. Clinicopathologic findings predictive of relapse in children with stage III favorable-histology Wilms tumor. J. Clin. Oncol. 31, 1196–1201 (2013).
Smets, A. M. et al. The contribution of chest CT-scan at diagnosis in children with unilateral Wilms’ tumour. Results of the SIOP 2001 study. Eur. J. Cancer 48, 1060–1065 (2012).
Hamilton, T. E. et al. The management of synchronous bilateral Wilms tumor: a report from the national Wilms tumor study group. Ann. Surg. 253, 1004–1010 (2011).
Ehrlich, P. et al. Results of the first prospective multi-institutional treatment study in children with bilateral Wilms tumor (AREN0534): a report from the Children’s Oncology Group. Ann. Surg. 266, 470–478 (2017).
Kalapurakal, J. A. et al. Outcomes of children with favorable histology Wilms tumor and peritoneal implants treated in National Wilms Tumor Studies-4 and -5. Int. J. Radiat. Oncol. Biol. Phys. 77, 554–558 (2010).
Green, D. M. et al. Outcome of patients with Stage II/favorable histology Wilms tumor with and without local tumor spill: a report from the National Wilms Tumor Study Group. Pediatr. Blood Cancer 61, 134–139 (2014).
Shamberger, R. C. et al. Surgery-related factors and local recurrence of Wilms tumor in National Wilms Tumor Study 4. Ann. Surg. 229, 292–297 (1999).
Gow, K. W. et al. Local staging of Wilms’ tumor-computerized tomography correlation with histological findings. J. Pediatr. Surg. 35, 677–679 (2000).
Zhuge, Y. et al. Improved survival with lymph node sampling in Wilms tumor. J. Surg. Res. 167, e199–e203 (2011).
Ehrlich, P. F. et al. Quality assessment for Wilms’ tumor: a report from the National Wilms’ Tumor Study-5. J. Pediatr. Surg. 40, 208–212 (2005).
Evageliou, N. et al. Prognostic impact of lymph node involvement and loss of heterozygosity of 1p or 16q in stage III favorable histology Wilms tumor: a report from Children’s Oncology Group Studies AREN03B2 and AREN0532. Cancer 130, 792–802 (2024).
Saltzman, A. F. et al. Patterns of lymph node sampling and the impact of lymph node density in favorable histology Wilms tumor: an analysis of the national cancer database. J. Pediatr. Urol. 14, 161.e1–161.e8 (2018).
Ehrlich, P. F. et al. Surgical protocol violations in children with renal tumors provides an opportunity to improve pediatric cancer care: a report from the Children’s Oncology Group. Pediatr. Blood Cancer 63, 1905–1910 (2016).
Kieran, K. et al. Lymph node involvement in Wilms tumor: results from National Wilms Tumor Studies 4 and 5. J. Pediatr. Surg. 47, 700–706 (2012).
Irtan, S. et al. Number of lymph nodes sampled in SFCE/SIOP 2001 patients with Wilms tumour: Is the goal of more than six achievable? Pediatr. Blood Cancer 70, e30107 (2023).
Stewart, C. L. & Bruny, J. L. Maximizing lymph node retrieval during surgical resection of Wilms tumor. Eur. J. Pediatr. Surg. 25, 109–112 (2015).
Renfro, L. A. et al. Associations of patient age, tumor nephrectomy weight, and tumor diameter with event-free and overall survival in stage I or II favorable histology Wilms tumor: a pooled analysis of Children’s Oncology Group Studies AREN0532 and AREN03B2. Ann. Surg. https://doi.org/10.1097/SLA.0000000000006726 (2025).
Beckwith, J. B. & Palmer, N. F. Histopathology and prognosis of Wilms tumors: results from the First National Wilms’ Tumor Study. Cancer 41, 1937–1948 (1978).
Dome, J. S. et al. Treatment of anaplastic histology Wilms’ tumor: results from the fifth National Wilms’ Tumor Study. J. Clin. Oncol. 24, 2352–2358 (2006).
Faria, P. et al. Focal versus diffuse anaplasia in Wilms tumor — new definitions with prognostic significance: a report from the National Wilms Tumor Study Group. Am. J. Surg. Pathol. 20, 909–920 (1996).
Hamilton, T. E. et al. Bilateral Wilms’ tumor with anaplasia: lessons from the National Wilms’ Tumor Study. J. Pediatr. Surg. 41, 1641–1644 (2006).
Perlman, E. J. Pediatric renal tumors: practical updates for the pathologist. Pediatr. Dev. Pathol. 8, 320–338 (2005).
Vujanic, G. M. et al. Revised International Society of Paediatric Oncology (SIOP) working classification of renal tumors of childhood. Med. Pediatr. Oncol. 38, 79–82 (2002).
Ehrlich, P. F. et al. Results of treatment for patients with multicentric or bilaterally predisposed unilateral Wilms tumor (AREN0534): a report from the Children’s Oncology Group. Cancer 126, 3516–3525 (2020).
Vujanic, G. M. et al. Pathology of Wilms’ tumour in International Society of Paediatric Oncology (SIOP) and Children’s Oncology Group (COG) renal tumour studies: similarities and differences. Histopathology 80, 1026–1037 (2022).
Pritchard-Jones, K. et al. Older age is an adverse prognostic factor in stage I, favorable histology Wilms’ tumor treated with vincristine monochemotherapy: a study by the United Kingdom Children’s Cancer Study Group, Wilm’s Tumor Working Group. J. Clin. Oncol. 21, 3269–3275 (2003).
Hol, J. A. et al. Prognostic significance of age in 5631 patients with Wilms tumour prospectively registered in International Society of Paediatric Oncology (SIOP) 93-01 and 2001. PLoS ONE 14, e0221373 (2019).
Breslow, N. et al. Prognostic factors in nonmetastatic, favorable histology Wilms’ tumor. Results of the Third National Wilms’ Tumor Study. Cancer 68, 2345–2353 (1991).
Reinhard, H. et al. Outcome of relapses of nephroblastoma in patients registered in the SIOP/GPOH trials and studies. Oncol. Rep. 20, 463–467 (2008).
Weeks, D. A., Beckwith, J. B. & Luckey, D. W. Relapse-associated variables in stage I favorable histology Wilms’ tumor. A report of the National Wilms’ Tumor Study. Cancer 60, 1204–1212 (1987).
Vallance, K. et al. Updated risk stratification in children with stage I favorable histology Wilms tumors. A report from the Children’s Oncology Group AREN0532 and AREN03B2 studies. Pediatr. Blood Cancer 68, e29349 (2021).
Reinhard, H. et al. Wilms’ tumor in adults: results of the Society of Pediatric Oncology (SIOP) 93-01/Society for Pediatric Oncology and Hematology (GPOH) study. J. Clin. Oncol. 22, 4500–4506 (2004).
Mitry, E. et al. Incidence of and survival from Wilms’ tumour in adults in Europe: data from the EUROCARE study. Eur. J. Cancer 42, 2363–2368 (2006).
Gooskens, S. L. et al. in Wilms Tumor Ch. 2 (ed van den Heuvel-Eibrink, M. M.) (Codon, 2016).
Sudour-Bonnange, H. et al. Standard of care for adult Wilms tumor? From adult urologist to pediatric oncologist. A retrospective review. Bull. Cancer 108, 177–186 (2021).
Kalapurakal, J. A. et al. Treatment outcomes in adults with favorable histologic type Wilms tumor — an update from the National Wilms Tumor Study Group. Int. J. Radiat. Oncol. Biol. Phys. 60, 1379–1384 (2004).
Cassady, J. R. et al. Considerations in the radiation therapy of Wilms’ tumor. Cancer 32, 598–608 (1973).
Green, D. M. & Jaffe, N. The role of chemotherapy in the treatment of Wilms’ tumor. Cancer 44, 52–57 (1979).
Larsen, E. et al. Surgery only for the treatment of patients with stage I (Cassady) Wilms’ tumor. Cancer 66, 264–266 (1990).
Green, D. M. et al. Treatment outcomes in patients less than 2 years of age with small, stage I, favorable-histology Wilms’ tumors: a report from the National Wilms’ Tumor Study. J. Clin. Oncol. 11, 91–95 (1993).
Green, D. M. et al. The relationship between microsubstaging variables, age at diagnosis, and tumor weight of children with stage I/favorable histology Wilms’ tumor. A report from the National Wilms’ Tumor Study. Cancer 74, 1817–1820 (1994).
Shamberger, R. C. et al. Long-term outcomes for infants with very low risk Wilms tumor treated with surgery alone in National Wilms Tumor Study-5. Ann. Surg. 251, 555–558 (2010).
Grundy, P. E. et al. Loss of heterozygosity for chromosomes 16q and 1p in Wilms’ tumors predicts an adverse outcome. Cancer Res. 54, 2331–2333 (1994).
Warmann, S. W. et al. Tumor biology influences the prognosis of nephroblastoma patients with primary pulmonary metastases: results from SIOP 93-01/GPOH and SIOP 2001/GPOH. Ann. Surg. 254, 155–162 (2011).
Ehrlich, P. F. et al. Hepatic metastasis at diagnosis in patients with Wilms tumor is not an independent adverse prognostic factor for stage IV Wilms tumor: a report from the Children’s Oncology Group/National Wilms Tumor Study Group. Ann. Surg. 250, 642–648 (2009).
Benedetti, D. J. et al. Treatment of children with favorable histology Wilms tumor with extrapulmonary metastases: a report from the COG studies AREN0533 and AREN03B2 and NWTSG study NWTS-5. Cancer 130, 947–961 (2024).
Beckwith, J. B., Zuppan, C. E., Browning, N. G., Moksness, J. & Breslow, N. E. Histological analysis of aggressiveness and responsiveness in Wilms’ tumor. Med. Pediatr. Oncol. 27, 422–428 (1996).
Parsons, L. N. et al. Outcome analysis of stage I epithelial-predominant favorable-histology Wilms tumors: a report from Children’s Oncology Group study AREN03B2. Cancer 126, 2866–2871 (2020).
Armstrong, A. E. et al. A unique subset of low-risk Wilms tumors is characterized by loss of function of TRIM28 (KAP1), a gene critical in early renal development: a Children’s Oncology Group study. PLoS ONE 13, e0208936 (2018).
de Jel, D. V. C. et al. Paediatric metanephric tumours: a clinicopathological and molecular characterisation. Crit. Rev. Oncol. Hematol. 150, 102970 (2020).
Goldstein, J. A. et al. BRAF exon 15 mutations in the evaluation of well-differentiated epithelial nephroblastic neoplasms in children: a report from the Children’s Oncology Group study AREN03B2. Arch. Pathol. Lab. Med. 148, e362–e366 (2024).
Marsden, L. et al. BRAF exon 15 mutations in pediatric renal stromal tumors: prevalence in metanephric stromal tumors. Hum. Pathol. 60, 32–36 (2017).
Garcia, M., Douglass, C. & Schlosser, J. V. Classification and prognosis in Wilms’s tumor. Radiology 80, 574–580 (1963).
Segers, H. et al. Gain of 1q is a marker of poor prognosis in Wilms’ tumors. Genes Chromosomes Cancer 52, 1065–1074 (2013).
Chagtai, T. et al. Gain of 1q as a prognostic biomarker in Wilms tumors (WTs) treated with preoperative chemotherapy in the International Society of Paediatric Oncology (SIOP) WT 2001 trial: a SIOP renal tumours biology consortium study. J. Clin. Oncol. 34, 3195–3203 (2016).
Thomas, P. R. et al. Abdominal relapses in irradiated second National Wilms’ Tumor study patients. J. Clin. Oncol. 2, 1098–1101 (1984).
Corey, B., Yang, C. H., Wilimas, J. A., Davidoff, A. & Dome, J. S. Significance of pleural effusion at diagnosis of Wilms tumor. Pediatr. Blood Cancer 42, 145–148 (2004).
Al-Hadidi, A. et al. Incidence and management of pleural effusions in patients with Wilms tumor: a pediatric surgical oncology research collaborative study. Int. J. Cancer 151, 1696–1702 (2022).
Aldrink, J. H. et al. Critical elements of radical nephroureterectomy for pediatric unilateral renal tumor. Semin. Pediatr. Surg. 32, 151339 (2023).
Hadley, L., Steenhuisen, K., Shrives, L. & Ramdial, P. Peritoneal fluid cytology in children with Wilms tumour after neoadjuvant chemotherapy. Pediatr. Blood Cancer 47, 384 (2006).
Hallman, J. R. & Geisinger, K. R. Cytology of fluids from pleural, peritoneal and pericardial cavities in children. A comprehensive survey. Acta Cytol. 38, 209–217 (1994).
Ferrer, F. A. et al. Image based feasibility of renal sparing surgery for very low risk unilateral Wilms tumors: a report from the Children’s Oncology Group. J. Urol. 190, 1846–1851 (2013).
Ehrlich, P. et al. Unilateral Wilms tumor treated by partial nephrectomy enrolled on the Children’s Oncology Group (COG) renal tumor biology and classification study AREN03B2. Pediatr. Blood Cancer 61, S112–S113 (2014).
Wilde, J. C. et al. Nephron sparing surgery (NSS) for unilateral Wilms tumor (UWT): the SIOP 2001 experience. Pediatr. Blood Cancer 61, 2175–2179 (2014).
Breslow, N. E. et al. End stage renal disease in patients with Wilms tumor: results from the National Wilms Tumor Study Group and the United States renal data system. J. Urol. 174, 1972–1975 (2005).
Dieffenbach, B. V. et al. Late-onset kidney failure in survivors of childhood cancer: a report from the childhood cancer survivor study. Eur. J. Cancer 155, 216–226 (2021).
Wu, N. L. et al. Development and validation of a prediction model for kidney failure in long-term survivors of childhood cancer. J. Clin. Oncol. 41, 2258–2268 (2023).
Welter, N. et al. The pathophysiology of bilateral and multifocal Wilms tumors: what we can learn from the study of predisposition syndromes. Pediatr. Blood Cancer 70, e29984 (2023).
Scott, R. H. et al. Surveillance for Wilms tumour in at-risk children: pragmatic recommendations for best practice. Arch. Dis. Child. 91, 995–999 (2006).
Scott, R. H., Stiller, C. A., Walker, L. & Rahman, N. Syndromes and constitutional chromosomal abnormalities associated with Wilms tumour. J. Med. Genet. 43, 705–715 (2006).
Murphy, A. J. et al. Genetic and epigenetic features of bilateral Wilms tumor predisposition in patients from the Children’s Oncology Group AREN18B5-Q. Nat. Commun. 14, 8006 (2023).
Romao, R. L. P. et al. Bilateral Wilms tumor with anaplasia: a report from the Children’s Oncology Group study AREN0534. Pediatr. Blood Cancer 71, e30981 (2024).
Perlman, E. et al. Paediatric renal tumours histopathology reporting guide. ICCR https://www.iccr-cancer.org/datasets/published-datasets/paediatrics/paediatric-renal-tumours (2023).
Artunduaga, M. et al. Imaging of pediatric renal tumors: a COG Diagnostic Imaging Committee/SPR Oncology Committee white paper focused on Wilms tumor and nephrogenic rests. Pediatr. Blood Cancer 70, e30004 (2023).
Servaes, S. et al. Comparison of diagnostic performance of CT and MRI for abdominal staging of pediatric renal tumors: a report from the Children’s Oncology Group. Pediatr. Radiol. 45, 166–172 (2015).
Watson, T., Oostveen, M., Rogers, H., Pritchard-Jones, K. & Olsen, O. The role of imaging in the initial investigation of paediatric renal tumours. Lancet Child Adolesc. Health 4, 232–241 (2020).
Sandberg, J. K. et al. Imaging characteristics of nephrogenic rests versus small Wilms tumors: a report from the Children’s Oncology Group study AREN03B2. AJR Am. J. Roentgenol. 214, 987–994 (2020).
Naik-Mathuria, B. et al. Management and outcomes of Wilms tumor with suprarenal intravascular extension: a pediatric surgical oncology research collaborative study. Ann. Surg. 279, 528–535 (2024).
Shamberger, R. C. et al. Intravascular extension of Wilms tumor. Ann. Surg. 234, 116–121 (2001).
Gehle, D. B. et al. Wilms tumor with vena caval intravascular extension: a surgical perspective. Children 11, 896 (2024).
Pio, L. et al. Surgical management of Wilms tumors with intravenous extension: a multicenter analysis of clinical management with technical insights. Ann. Surg. Oncol. 31, 4713–4723 (2024).
Ritchey, M. et al. Ureteral extension in Wilms’ tumor: a report from the National Wilms’ Tumor Study Group (NWTSG). J. Pediatr. Surg. 43, 1625–1629 (2008).
Kieran, K. et al. Is adrenalectomy necessary during unilateral nephrectomy for Wilms tumor? A report from the Children’s Oncology Group. J. Pediatr. Surg. 48, 1598–1603 (2013).
Glick, R. D. et al. Current surgical approaches to pediatric renal tumors. Pediatr. Blood Cancer 72, e31118 (2025).
Shojaeian, R., Hiradfar, M., Sharifabad, P. S. & Zabolinejad, N. in Wilms Tumor Ch. 6 (ed. van den Heuvel-Eibrink, M. M.) (Codon, 2016).
Karim, A. et al. Pediatric extra-renal nephroblastoma (Wilms’ Tumor): a systematic case-based review. Cancers 15, 2563 (2023).
Hol, J. A. et al. Prevalence of (epi)genetic predisposing factors in a 5-year unselected National Wilms Tumor Cohort: a comprehensive clinical and genomic characterization. J. Clin. Oncol. 40, 1892–1902 (2022).
Kalish, J. M. et al. Update on surveillance for Wilms tumor and hepatoblastoma in Beckwith–Wiedemann syndrome and other predisposition syndromes. Clin. Cancer Res. 30, 5260–5269 (2024).
Brzezinski, J. J. et al. Update on surveillance guidelines in emerging Wilms tumor predisposition syndromes. Clin. Cancer Res. 31, 18–24 (2025).
Ehrlich, P. F. et al. Kidney preservation and Wilms tumor development in children with diffuse hyperplastic perilobar nephroblastomatosis: a report from the Children’s Oncology Group study AREN0534. Ann. Surg. Oncol. 29, 3252–3261 (2022).
Balis, F. et al. Wilms tumor (nephroblastoma). NCCN https://www.nccn.org/guidelines/guidelines-detail?category=1&id=1500 (2025).
D’Angio, G. J. et al. The treatment of Wilms’ tumor: results of the second National Wilms’ Tumor Study. Cancer 47, 2302–2311 (1981).
Green, D. M. et al. Comparison between single-dose and divided-dose administration of dactinomycin and doxorubicin for patients with Wilms’ tumor: a report from the national Wilms’ tumor study group. J. Clin. Oncol. 16, 237–245 (1998).
Burns, P. B., Rohrich, R. J. & Chung, K. C. The levels of evidence and their role in evidence-based medicine. Plast. Reconstr. Surg. 128, 305–310 (2011).
Acknowledgements
E.A.M. discloses support for the research of this work from the Solder True Life Foundation. J.S.D. discloses support for the research of this work from the National Institutes of Health Clinician Scientist Research Specialist award [grant R50CA275931]. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Author information
Authors and Affiliations
Contributions
D.J.B., N.G.C., P.F.E., L.A.R., J.S.D., J.I.G. and E.A.M. researched data for the article. D.J.B., N.G.C., J.I.G. and E.A.M. contributed substantially to discussion of the content. D.J.B., N.G.C., N.E., L.N.P., A.C.P., J.K.S., and E.A. wrote the article. All authors reviewed and/or edited the manuscript before submission.
Corresponding author
Ethics declarations
Competing interests
N.G.C.’s spouse is a senior medical officer for Janssen. The other authors declare no competing interests.
Peer review
Peer review information
Nature Reviews Urology thanks Daniel Green, Gordan Vujanic and the other, anonymous, reviewer(s) for their contribution to the peer review of this work.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Benedetti, D.J., Cost, N.G., Ehrlich, P.F. et al. Updated favourable-histology Wilms tumour risk stratification: rationale for future Children’s Oncology Group clinical trials. Nat Rev Urol 22, 775–788 (2025). https://doi.org/10.1038/s41585-025-01055-1
Accepted:
Published:
Version of record:
Issue date:
DOI: https://doi.org/10.1038/s41585-025-01055-1
This article is cited by
-
Long-term adverse effects of modern Wilms tumour therapies: implications for monitoring
Nature Reviews Urology (2026)
-
Adult Wilms tumor in an eighty-year-old man: A case report and literature review of recent elderly-onset cases
International Cancer Conference Journal (2025)
