
Abstract
Two large clinical studies showed that fenofibrate, a commonly used peroxisome proliferator-activated receptor α (PPARα) agonist, has protective effects against diabetic retinopathy. However, the underlying mechanism has not been clarified. We performed genome-wide analyses of gene expression and PPARα binding sites in vascular endothelial cells treated with the selective PPARα modulator pemafibrate and identified 221 target genes of PPARα including THBD, which encodes thrombomodulin (TM). ChIP-qPCR and luciferase reporter analyses showed that PPARα directly regulated THBD expression via binding to the promoter. In the rat diabetic retina, treatment with pemafibrate inhibited the expression of inflammatory molecules such as VCAM-1 and MCP1, and these effects were attenuated by intravitreal injection of small interfering RNA targeted to THBD. Furthermore, pemafibrate treatment inhibited diabetes-induced vascular leukostasis and leakage through the upregulation of THBD. Our results indicate that PPARα activation inhibits inflammatory and vasopermeable responses in the diabetic retina through the upregulation of TM.
Similar content being viewed by others

Introduction
Diabetic retinopathy (DR) is the main cause of blindness among working-age adults, and the worldwide prevalence is approximately 35% in patients with diabetes1. DR is characterized by the combination of increased vessel permeability and progressive vascular occlusion. However, the molecular mechanisms underlying the pathways associated with DR have not been fully elucidated. Several biochemical mechanisms have been proposed to modulate the pathogenesis of DR through effects on cellular metabolism, signaling, and growth factors2. Implicated pathways include the accumulation of sorbitol and advanced glycation end-products, oxidative stress, protein kinase C activation, and upregulation of the renin-angiotensin system and vascular endothelial growth factor (VEGF). Among them, VEGF strongly promotes angiogenesis, a key mediator of the progression of DR. Inhibition of VEGF (e.g., anti-VEGF therapies) was shown to be effective in the management of DR in numerous studies3,4,5,6,7. However, some DR patients respond poorly or incompletely to anti-VEGF therapy. Accordingly, there is still substantial unmet medical need in patients with DR.
Peroxisome proliferator-activated receptor α (PPARα) is a ligand-activated transcription factor that regulates lipid metabolism8. PPARα is highly expressed in the liver and is also expressed in the retina9. Recently, two large, prospective clinical trials have demonstrated that fenofibrate, a canonical synthetic PPARα agonist, has protective effects against DR in type 2 diabetes patients. The Fenofibrate Intervention in Event Lowering in Diabetes (FIELD) Study reported that fenofibrate therapy significantly reduced the cumulative need for laser therapy for DR10. The Action Control Cardiovascular Risk in Diabetes (ACCORD) Lipid Study of combination simvastatin and fenofibrate demonstrated a greater reduction in the progression of proliferative DR in type 2 diabetes patients compared with simvastatin alone11. Thus, PPARα may be an emerging therapeutic option in DR.
Recently, it has been reported that PPARα is downregulated by microRNA in the retina of diabetic animal models12. Previous studies showed that PPARα exerts protective effects against endothelial dysfunction, neovascularization, vasoregression, and vascular hyperpermeability9,13,14,15. Another recent study has also found that important factors in DR such as VEGF and TNFα are downregulated by PPARα activation in the retina of diabetic animal models16. However, the mechanisms by which PPARα activation exerts protective effects against DR are not fully understood.
Fenofibrate, which has a long history of clinical use as a lipid-lowering drug, has poor PPAR subtype selectivity17. Fenofibrate treatment sometimes results in elevation of the transaminase, homocysteine, and creatine levels in patients. On the other hand, pemafibrate, a novel selective PPARα modulator, has greater PPARα activation potency and higher subtype selectivity than fenofibrate18,19,20. Therefore, pemafibrate may reduce inflammation and angiogenesis more effectively than fenofibrate in DR patients.
Thrombomodulin (TM) is a transmembrane protein expressed on the surface of endothelial cells and is encoded by the THBD gene21. TM converts thrombin to the anticoagulant form to reduce blood coagulation and inhibits inflammation in blood vessels22,23,24,25,26. Recently, recombinant TM has been developed and can potentially be used to treat patients with inflammatory and thrombotic diseases27,28.
In the current study, we performed genome-wide analyses of gene expression and PPARα binding sites in vascular endothelial cells treated with pemafibrate and found that PPARα directly regulates the expression of THBD in endothelial cells. Furthermore, PPARα activation inhibited retinal inflammation through the upregulation of TM in a rat model of DR. Thus, upregulation of TM by PPARα activation can be a potential therapeutic strategy against DR.
Results
Genome-wide analysis of PPARα-targeted genes in vascular endothelial cells
To investigate the mechanism of the protective effects against DR by PPARα activation, we performed DNA microarray analysis and ChIP-seq of PPARα in HUVECs treated with pemafibrate. Microarray analysis showed that pemafibrate treatment for 24 h upregulated 1,062 genes (> 1.5-fold, Fig. 1a, pemafibrate-induced genes) and downregulated 477 genes (> 1.5-fold) compared with DMSO treatment (control). Pemafibrate-induced genes included known direct targets of PPARα such as PDK418. The top 50 upregulated and downregulated genes are listed in Tables 1 and 2, respectively.

Genome-wide analysis of PPARα binding sites in HUVECs. (a) Venn diagram representation of 1,062 pemafibrate-induced genes (≥ 1.5-fold) and 4,186 PPARα-bound genes in HUVECs treated with pemafibrate (10 μM). (b) Genome-wide distribution of PPARα binding sites in pemafibrate-treated HUVECs. Ups, upstream; dws, downstream. (c) Genome browser representation of PPARα and RXRα binding on THBD in HUVECs treated with pemafibrate (pema) or vehicle for 24 h.
In ChIP-seq analysis, peak calling by SICER identified 6,017 genomic regions as significant binding sites of PPARα in pemafibrate-treated HUVECs, and these binding sites were annotated to 4,186 genes (Fig. 1a, PPARα-bound genes). The PPARα genomic binding regions were localized mostly on intergenic regions (49%), and partly on proximal promoters (18%), and intragenic regions (31%) (Fig. 1b). Among PPARα-bound genes, 221 overlapped with pemafibrate-induced genes (Fig. 1a and Table 3). These target genes of PPARα in HUVECs included PDK4, ECH1, and ANGPTL4, which are known metabolic genes induced by peroxisome proliferators18,29,30. We also identified THBD encoding TM as a target gene of PPARα. A genome browser shot showed pemafibrate-dependent PPARα binding near the transcription start site (TSS) of THBD (Fig. 1c).
We also performed ChIP-seq of retinoid X receptor α (RXRα), which is a heterodimer partner of PPARα, and found RXRα binding near the TSS of THBD regardless of pemafibrate treatment (Fig. 1c). Because TM is reported to inhibit inflammation in blood vessels23,26, we hypothesize that the upregulation of TM by PPARα activation could inhibit the inflammatory response in the diabetic retina.
PPARα directly upregulates THBD expression
A combination of DNA microarray and ChIP-seq analyses of HUVECs identified THBD as one of the target genes of PPARα. To confirm this, we performed immunoblot analysis and showed that pemafibrate treatment upregulated TM protein expression in HUVECs as well as HRMECs (Fig. 2a,b). Q-PCR analysis revealed that the upregulation of THBD by pemafibrate was blunted when PPARα was knocked down by small interfering RNA (siRNA) targeted to PPARα in HUVECs and HRMECs (Fig. 2c,d). Thus, pemafibrate-mediated induction of THBD is dependent on PPARα in HUVECs and HRMECs. To determine whether PPARα directly regulates THBD expression, we examined the physical and functional interactions of PPARα with THBD in ChIP-qPCR and luciferase reporter analysis, respectively. ChIP-qPCR analysis confirmed PPARα binding on the promoter region of THBD in HUVECs treated with pemafibrate (Fig. 2e).

PPARα directly transactivates THBD expression. (a,b) Immunoblot analysis showing the expression of TM in HUVECs (a) and HRMECs (b) treated with pemafibrate (10 μM) or vehicle for 24 h. Expression of TM was increased by pemafibrate treatment in both HUVECs and HRMECs. (c,d) HUVECs (c) and HRMECs (d) were transfected with siRNA targeted to human PPARα (5 nM) or control siRNA and treated with pemafibrate or vehicle for 24 h. THBD mRNA was measured using RT-qPCR. Cyclophilin mRNA was used as the invariant control. Knockdown of PPARα canceled pemafibrate-mediated upregulation of THBD in HUVECs and HRMECs. (e) PPARα binding on the THBD promoter was evaluated by ChIP-qPCR. ChIP signals are presented as fold enrichment. Cyclophilin was used as a negative binding region. PPARα was bound approximately 100 bp upstream from the TSS of THBD. (f) Alignment of promoter sequences of human THBD, mouse Thbd, and rat Thbd containing two putative DR1 motifs. The DR1 motifs at positions – 1,135 to – 1,123 bp and – 189 to – 177 bp of human THBD are conserved in mouse and rat Thbd. (g) Alignment of the two putative DR1 motifs in the human THBD promoter. At the consensus site, the consensus nucleotide found in the PPARα binding sequences is represented by black letters. (h) Luciferase reporter analysis using the human THBD promoter. HUVECs were transfected with the luciferase reporter containing wild-type THBD promoter or indicated deletion and mutations in DR1 motifs together with PPARα and RXRα expression plasmids. After transfection, HUVECs were treated with fenofibric acid for 24 h and subjected to the luciferase reporter assay. The luciferase activity with fenofibric acid was divided by the activity without fenofibric acid and is presented as fold activation. (Results are expressed as mean ± SD of three independent experiments. *p < 0.05. Mann–Whitney U test).
PPARα preferentially binds DNA as a heterodimer to the PPAR-responsive element (PPRE), which is composed of two nuclear receptor consensus half-sites of AGGTCA organized as a direct repeat (direct repeat 1 [DR1])31. PPARα forms heterodimers with RXRα, and the heterodimers bind the PPRE located in PPARα-regulated genes. Scanning of the promoter sequences of human THBD identified two putative DR1 motifs (– 189 bp to 177 bp and – 1,135 bp to – 1,123 bp from the TSS) (Fig. 2f). The former motif is conserved in mouse and rat Thbd genes, while the latter is not (Fig. 2g). Accordingly, we generated a reporter plasmid containing the promoter of THBD (~ 1.3 kb) and performed luciferase reporter analysis (Fig. 2h). Because pemafibrate affected the control reporter activities (i.e., renilla luciferase and β-gal) (data not shown), we used fenofibric acid as a PPARα agonist in the luciferase reporter assay. HUVECs were transfected with the reporter plasmid together with expression plasmids of PPARα and RXRα and then treated with fenofibric acid to determine PPARα-mediated transactivation. Treatment with fenofibric acid increased the activity of the luciferase reporter containing the THBD promoter by threefold. Deletion of two putative DR1 motifs blunted the transactivation by fenofibric acid. Mutation in the DR1 motif at – 1,135 bp from the TSS alone had no effect on fenofibric acid-mediated transactivation, while mutation in the DR1 motif at – 189 bp from the TSS or mutations in both DR1 motifs abolished transactivation. These results indicate that PPARα directly upregulates THBD expression in a ligand-dependent manner by binding to the DR1 motif at – 189 bp from the TSS in HUVECs.
Pemafibrate inhibits TM-dependent retinal inflammation in diabetic rats
Cell culture experiments showed that PPARα directly upregulated TM, which has antiinflammatory effects. We hypothesized that PPARα activation by pemafibrate could inhibit inflammation through upregulation of TM in the diabetic retina. To examine this, we first administered oral pemafibrate to rats via their feed and showed that pemafibrate (10 mg/kg or 30 mg/kg) significantly increased mRNA expression of PPARα target genes such as Pdk4 and Thbd in the retina (Fig. 3a,b). Next, we set up a TM knockdown system in the rat retina by intravitreal injection of siRNA. Intravitreal injection of 500 pmol of siRNA targeted to Thbd for 14 days successfully decreased the protein expression of TM (Fig. 3c). In the STZ-induced diabetic rat model, the protein levels of inflammatory molecules such as ICAM, MCP1, and VCAM-1 in the retina were elevated compared with the retinas of nondiabetic rats (Fig. 3d), as previously reported32,33. Oral intake of pemafibrate in STZ-induced diabetic rats markedly inhibited the elevation of inflammatory molecules, indicating that PPARα activation inhibits inflammatory responses in the retinas of diabetic rats. Furthermore, knockdown of TM in diabetic rats attenuated the pemafibrate-mediated inhibition of elevation of inflammatory molecules. These results indicate that the inhibition of PPARα activation by pemafibrate inhibits inflammation through the upregulation of TM in diabetic rat retinas.

Pemafibrate inhibits expression of inflammatory molecules by upregulating TM in the diabetic retina. (a) RT-qPCR analysis showing mRNA expression of Pdk4 in rat retinas treated with the indicated doses of pemafibrate. PDK4 is a known PPARα target gene. Pemafibrate treatment significantly upregulated Pdk4 in the rat retina. (b) RT-qPCR showing mRNA expression of Thbd in rat retinas treated with pemafibrate. Pemafibrate significantly upregulated Thbd in the retina. (c) Immunoblot analysis showing expression of TM protein in the retinas of rats intravitreally injected with siRNA targeted to Thbd for 3, 7, and 14 days. β-Actin was used as a loading control. The intravitreal injection of siRNA reduced TM protein in the rat retina. (d) Immunoblot analysis showing expression of ICAM, MCP2, and VCAM-1 proteins in the retina of control and diabetic rats. β-Actin was used as a loading control. ICAM, MCP2, and VCAM-1 proteins were evaluated in the retinas of diabetic rats compared with control rats. Pemafibrate treatment inhibited elevation of these proteins in the retina of diabetic rats. Knockdown of Thbd by siRNA canceled pemafibrate-mediated inhibition of the elevation of these proteins. (Results are expressed as mean ± SD of two independent experiments [a,b]. *p < 0.05. Mann–Whitney U test).
Pemafibrate inhibits TM-dependent retinal vascular leukostasis and leakage
Vascular leukostasis and leakage increase cumulatively with the progression of DR34. To determine whether PPARα activation inhibits vascular leukostasis and leakage in the retina, we examined them in diabetic rats treated with pemafibrate. FITC-labeled adherent leukocytes were not observed in control rats, while they were clearly observed in the retinal vasculature of untreated diabetic rats (Fig. 4a). Pemafibrate treatment significantly reduced the number of leukocytes in the rat retinas (p < 0.05) (Fig. 4a,b), indicating that it inhibits vascular leukostasis in diabetic rats. TM knockdown by siRNA attenuated the pemafibrate-mediated reduction of leukocytes in the retinal vasculature of diabetic rats (p < 0.05) (Fig. 4a,b), while control siRNA treatment did not, indicating that PPARα activation by pemafibrate inhibits vascular leukostasis through TM in the retina of diabetic rats.

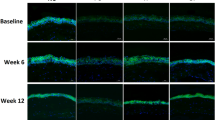
Pemafibrate inhibits retinal vascular leukostasis by upregulating TM. (a) Fluorescence microscopy images showing retinal adherent vascular leukocytes in diabetic rats. STZ-induced diabetic rats were treated with pemafibrate or vehicle and intravitreally injected with control siRNA or siRNA targeting Thbd. The retinal vascular adherent leukocytes were stained with FITC-conjugated concanavalin-A. Representative images of retinal flat mounts from nondiabetic rats (upper left), untreated diabetic rats (upper right), diabetic rats treated with pemafibrate and control siRNA (lower left), and diabetic rats treated with pemafibrate and siThbd (lower right) are shown. Arrows indicate adherent leukocytes. Scale bar = 50 μm. (b) Quantification of adherent leukocytes in retinal images (n = 6 per group). (Results are expressed as mean ± SD. *p < 0.05. Mann–Whitney U test).
Next, we examined whether pemafibrate treatment reduces retinal vascular leakage in diabetic rats. The fluorescence intensity of FITC-dextran in the retinal vessels was significantly increased in diabetic rats compared with control rats (p < 0.05), indicating increased vascular leakage in the former (Fig. 5a,b). Pemafibrate treatment significantly reduced the florescence intensity of FITC-dextran in diabetic rats (p < 0.05) (Fig. 5a,b), indicating that PPARα activation by pemafibrate inhibits vascular leakage. In addition, TM knockdown by siRNA attenuated pemafibrate-mediated inhibition of vascular leakage in diabetic rats (p < 0.05) (Fig. 5a,b). These results revealed that PPARα activation by pemafibrate inhibits retinal vascular leukostasis and leakage via TM in diabetic rats.

Pemafibrate inhibits retinal vascular leakage by upregulating TM. (a) Fluorescent images showing retinal vascular leakage in diabetic rats. STZ-induced diabetic rats were fed pemafibrate or vehicle. STZ-induced diabetic rats treated with pemafibrate or vehicle were then intravitreally injected with control siRNA or siRNA targeting Thbd. Vascular leakage was visualized by staining with FITC-dextran. Retinas were examined using fluorescence microscopy. Representative images of retinas from nondiabetic rats, untreated diabetic rats, diabetic rats treated with pemafibrate and control siRNA, and diabetic rats treated with pemafibrate and siThbd are shown. The square areas in the top row are magnified and shown in the bottom row. Scale bar = 100 μm. (b) Retinal permeability was quantified by measuring the fluorescence intensity of FITC-dextran in the images on the bottom row (n = 4 per group). (Results are expressed as mean ± SD of three independent experiments. *p < 0.05. Mann–Whitney U test).
Discussion
In the current study, we identified THBD encoding TM as one of the direct target genes of PPARα in vascular endothelial cells. PPARα activation by pemafibrate in a rat model of DR upregulated THBD and inhibited retinal inflammation and vascular leukostasis and leakage. To the best of our knowledge, this is the first report showing the novel molecular mechanism by which PPARα activation protects against DR.
PPARα is a ligand-activated transcription factor, and its target genes are involved in fatty acid metabolism in tissues with high oxidative rates such as the liver, heart, skeletal muscle, and kidney8,9. PPARα is also expressed in other tissues and cells including the intestine, vascular endothelium, and immune cells15. Large clinical trials and several reports revealed that PPARα activation by an agonist has protective effects against DR in type 2 diabetes patients10,11, although the mechanisms of action of the PPARα agonist were unclear. Because DR is characterized by progressive loss of vascular cells and infiltration of inflammatory cells, we specifically focused on vascular endothelial cells and performed genome-wide analyses of PPARα binding sites and gene expression using ChIP-seq analysis and DNA microarray. Our ChIP-seq analysis identified 6,017 genomic PPARα binding sites, which were assigned to 4,186 proximal genes. Microarray analysis revealed 1,062 genes with expression levels upregulated by pemafibrate treatment in HUVECs.
The majority of PPARα binding sites identified by ChIP-seq were located at intragenic regions or 5′ proximal regions (< 10 kb from the TSS) in HUVECs, consistent with previous ChIP-seq analysis in human hepatoma cells35. These results are in line with several studies showing that transcription factor binding sites are generally distributed around the TSS36,37. Among 4,186 genes annotated as bound by PPARα, 221 including THBD were upregulated by pemafibrate treatment, indicating that these genes are direct PPARα targets in HUVECs. However, pemafibrate treatment did not affect the expression of the majority of genes annotated as bound by PPARα. Some PPARα binding sites may participate in transcriptional regulation of distal genes or in other mechanisms such as noncoding RNA and DNA methylation. It is also possible that our ChIP-seq analysis contained false-positive signals due to the nonspecific binding of antibody. Therefore, the functional relevance of PPARα binding sites needs to be elucidated further.
VEGF has been shown to be one of predominant factors regulating pathological conditions including chronic inflammation and resulting abnormal vasopermeable and angiogenic responses in DR. Our microarray analysis identified 1,062 upregulated and 477 downregulated genes in HUVECs treated with pemafibrate. VEGF mRNA was not altered in the present microarray analysis. Since it is possible that PPARα has transcriptional and nontranscriptional roles in protection against DR, more detailed protein analyses are needed to confirm the direct effects of PPARα activation on VEGF expression. In contrast, the inhibitory effects of PPARα on VEGF expression were clearly demonstrated in in vivo settings. Chen et al. reported the inhibitory effects of fenofibrate on HIF-1 and VEGF expression in the whole retina in a type 1 diabetes rat model and mouse oxygen-induced retinal angiogenesis model38. Tomita et al. found that VEGF is suppressed by PPARα activation, which inhibits HIF activity through serum FGF 12 induced and secreted in the liver39. Another study showed that PPARα ligands may suppress angiogenesis indirectly by inhibiting tumor cell production of VEGF and FGF2 and by increasing thrombospondin-140. Although we need further detailed protein expression analyses in in vitro studies, these data may indicate that PPARα activation alone does not substantially affect VEGF expression, although it exerts obvious inhibitory effects through cross-reaction with other cytokines and organs. PPARα effects on VEGF-induced intracellular signaling have not been reported and remain to be elucidated.
Among 221 direct PPARα target genes, we focused on THBD that encodes TM. TM is an integral membrane protein expressed on the surface of endothelial cells and exerts antiinflammatory effects via several mechanisms22,23,24,25,26. TM inhibits inflammation through the activation of protease-activated receptor-1 (PAR-1) in the form of activated protein C (APC)23,24. Moreover, TM is a critical cofactor for thrombin-mediated activation of the thrombin-activatable fibrinolysis inhibitor (TAFI)21. The proinflammatory mediators are inactivated by TAFI25. TM, via thrombin-mediated activation of protein C and TAFI, provides protection against inflammation. Thrombin is an important inflammatory factor in retinal vascular diseases including DR41. It was reported that thrombin and prothrombin were increased in the vitreous of patients with proliferative DR compared with nondiabetic individuals42. Additionally, it was found that the lectin-like domain of TM sequesters inflammatory factors such as high-mobility group-B1 (HMGB-1) protein and lipopolysaccharide43,44. HMGB-1 promotes the process of cell apoptosis by activating the transcription factor nuclear factor-κB after binding to its receptors45,46. For these reasons, we hypothesized that PPARα activation inhibited the retinal vascular damage caused by retinal inflammation and apoptosis via the regulation of TM.
In the transcriptional regulation of THBD, our studies revealed that PPARα binds to the TSS upstream of THBD to activate gene expression. Furthermore, our luciferase reporter assay showed that the DR1 motif at 189 bp from the TSS is responsible for transactivation of the THBD promoter by PPARα. Previous studies demonstrated that other transcriptional factors (e.g., Kruppel-like factor 2 and RXRs) also bind to this region to transactivate the THBD promoter47,48, suggesting the importance of this region for the activity of the THBD promoter in vascular endothelial cells.
We used the rat model of DR to show that pemafibrate treatment prevents the upregulation of inflammatory molecules as well as vascular leukostasis and leakage. It was reported that CCL2, VCAM-1, and ICAM-1 are key inflammatory molecules in the diabetic retina which lead to leukocyte adhesion and vascular leakage32,33. Inflammatory mediators such as thrombin and HMGB-1 induce these inflammatory molecules43,45,46, while TM has inhibitory effects on inflammatory molecules. Therefore, we performed TM knockdown experiments in diabetic rats to determine whether the antiinflammatory effect of pemafibrate is mediated via the action of TM. In vivo experiments demonstrated that the antiinflammatory effect of pemafibrate was canceled by intravitreal injection of Thbd siRNA. These results suggest that the upregulation of TM is one mechanism of the protective effects of PPARα modulators (e.g., pemafibrate) against DR and that a modulator upregulating TM could be a novel therapeutic option for DR treatment. Further studies will be required to elucidate other mechanisms by which PPARα activation protects against DR.
Methods
Chemical reagents
Pemafibrate and fenofibric acid were kindly provided by Kowa Co., Ltd. (Nagoya, Japan).
Cell culture
Human umbilical vein endothelial cells (HUVECs) and human retinal microvascular endothelial cells (HRMECs) were purchased from Lonza (Walkersville, MD, USA) and cultured in EGM-2 MV medium (Lonza) containing 5% FBS at 37 °C in 5% CO2.
siRNA-mediated knockdown of PPARα and THBD
Stealth small interfering RNA (siRNA) (5 nM) targeting human THBD mRNA (HSS110719, Invitrogen, Carlsbad, CA, USA) were transfected into HUVECs or HRMECs using RNAiMAX reagent (Invitrogen), and cells were harvested 24 h after transfection. Control siRNA (Med GC) was obtained from Invitrogen. For in vivo experiments, 500 pmol of siRNA targeting rat Thbd (RSS331106, Invitrogen) or control siRNA (sc-37007, Santa Cruz Biotechnology, Santa Cruz, CA, USA) was intravitreally injected into streptozotocin (STZ)-induced diabetic rats.
DNA microarray analysis
HUVECs were treated with 10 μM of pemafibrate or vehicle (DMSO) for 24 h, and total RNA was isolated using Isogen (Fujifilm Wako Chemicals, Osaka, Japan). Preparation of cRNA and hybridization of the probe arrays were performed according to the manufacturer’s instructions (Affymetrix, Santa Clara, CA, USA)49. Affymetrix Genechip Human Genome U133 plus 2.0 arrays containing over 54,000 sets were used. Data analysis was performed using GeneSpring GX 12.5 (Agilent Technologies, Santa Clara, CA, USA).
Chromatin immunoprecipitation
HUVECs were treated with 10 μM of pemafibrate for 24 h and crosslinked with 1% formaldehyde for 10 min at room temperature. After neutralization by the addition of 0.2 M glycine, cells were harvested, resuspended in lysis buffer (13.6 mM Tris–HCl, 166.7 mM Nacl, 0.8% SDS, 1.2 mM EDTA, 0.9% Triton X-100; pH 8.0). Chromatin DNA was sonicated with Sonifier 250 (Branson, Danbury, CT, USA) (output 4, duty cycle 60%, 20 s × 6 times) to generate approximately 0.5-kb fragments. Chromatin immunoprecipitation (ChIP) was performed using the antibodies listed in Supplementary Table S1 prebound to Dynabeads Protein G (Life Technologies/Thermo Fisher Scientific, South San Francisco, CA, USA). ChIP DNA was purified with the QIAquick PCR Purification Kit (Qiagen, Germantown, MD, USA) and quantified using a Qubit Fluorometer and dsDNA HS assay Kit (Life Technologies/Thermo Fisher Scientific). ChIP sequencing (ChIP-seq) was performed with an Illumina/Solexa sequencer as previously described20,21,22,23,24,25,26,27,28,49,50,51.
ChIP-qPCR analysis
ChIP samples were analyzed by quantitative PCR using the gene-specific primers listed in Supplementary Table S2. ChIP signals were divided by no-antibody signals (input DNA) and presented as fold enrichment.
Quantitative RT-PCR
Total RNA was isolated using Isogen (Fujifilm Wako Chemicals) according to the manufacturer’s protocol49. cDNA was synthesized from 1 μg of total RNA using oligo-dT primers and SuperScript II reverse transcriptase (Life Technologies). Quantitative PCR was performed using an ABI PRISM 7900HT sequence detection system (Applied Biosystems, Foster City, CA, USA). PPIB or ACTB was used as an invariant control. A list of primers for quantitative RT-PCR used in this study is shown in Supplementary Table S3.
Immunoblot analysis
Protein samples obtained from HUVECs, HRMECs, or rat retinas were separated on 10% SDS-PAGE and electrophoretically transferred onto nitrocellulose membranes. The membranes were blocked with 5% skim milk in PBS containing 0.1% (v/v) Tween-20 for 1 h and incubated with primary antibody at 4 °C for 24 h. After washing, the membranes were incubated with secondary antibody conjugated with horseradish peroxidase at room temperature for 1 h. Immunoblots were visualized by chemiluminescence using Super Signal West Dura Extended Duration Substrate (Thermo Fisher Scientific), and luminescent images were analyzed with an ImageQuant LAS 4000mini (GE Healthcare, Piscataway, NJ, USA). A list of primary antibodies used in this study is shown in Supplementary Table S1.
Luciferase reporter assay
The luciferase reporter assay was performed with the Beta-Glo assay system (Promega, Madison, WI, USA). HUVECs seeded on 24-well plates at 50% confluence in Opti-MEM (Life Technologies/Thermo Fisher Scientific) were transfected with 0.2 µg of reporter plasmid. HUVECs were incubated for 24 h in normal growth medium and then treated with 100 μM of fenofibric acid or vehicle (DMSO). Luciferase assays were performed 48 h after fenofibric acid treatment. Luciferase activity was normalized to the β-gal activity level.
Type 1 diabetes rat model
Type 1 diabetes was induced in male Wistar rats by an intraperitoneal injection of STZ (60 mg/kg). Briefly, 6 to 8 weeks after STZ injection, the rats were fed pemafibrate (10 mg/kg) for 2 weeks. Intravitreal injection of control or Thbd siRNA was performed 6 and 7 weeks after STZ injections. The rats were euthanized 8 weeks after STZ injection. Rats in which blood glucose levels were greater than 300 mg/dl at tissue harvesting were defined as diabetic and used for the experiments.
Retinal vascular leukostasis ssay
The retinal vascular leukostasis assay was performed as described previously38. Briefly, rats were deeply anesthetized, and PBS was injected into the left ventricle. The anesthetized rats were perfused with PBS to remove nonadherent leukocytes in vessels. After injection of PBS, FITC-conjugated concanavalin-A (40 μg/ml) (Vector Laboratories, Burlingame, CA, USA) was injected into the left ventricle. The retinas were surgically isolated and then flat mounted. FITC-labeled adherent leukocytes in the vasculature were counted under a fluorescence microscope by an operator masked to treatment allocation.
Measurement of vascular leakage in the retina
Vascular leakage in the rat retinas was investigated using fluorescein angiography, as previously described52. Briefly, rats were deeply anesthetized, and FITC-dextran (Sigma-Aldrich, St. Louis, MO, USA) was injected into the left ventricle. After 5 min, the retinas were flat mounted and observed under a fluorescence microscope. Vascular leakage was quantitatively analyzed using Image J software by determining florescence intensities of FITC-dextran in the retina vessels.
Study approval
All animal protocols in this study were performed in accordance with the institutional guidelines and were approved by the St. Marianna University Graduate School of Medicine Institutional Animal Care and Use Committee.
Data availability
All data generated or analyzed during this study are included in the published article (and its supplementary files).
References
Yau, J. W. et al. Meta-analysis for eye disease (META-EYE) study group global prevalence and major risk factors of diabetic retinopathy. Diabetes Care 35, 556–564 (2012).
Fong, D. S., Aiello, L. P., Ferris, F. L. III. & Kleon, R. Diabetic retinopathy. Diabetes Care 27, 2540–2553 (2004).
Elman, M. J. et al. Expanded 2-year follow-up of ranibizumab plus prompt or deferred laser or triamcinolone plus prompt laser for diabetic macular edema. Ophthalmology 118(4), 609–614 (2011).
Brown, D. M. et al. Long-term outcomes of ranibizumab therapy for diabetic macular edema: the 36-month results from two phase III trials: RISE and RIDE. Ophthalmology 120(10), 2013–2022 (2013).
Schmidt-Erfurth, U. et al. Three-year outcomes of individualized ranibizumab treatment in patients with diabetic macular edema: the RESTORE Extension Study. Ophthalmology 121(5), 1045–1053 (2014).
Korobelnik, J. F. et al. Intravitreal aflibercept for diabetic macular edema. Ophthalmology 121(11), 2247–2254 (2014).
The Diabetic Retinopathy Clinical Research Network. Aflibercept, bevacizumab, or ranibizumab for diabetic macular edema. N. Engl. J. Med. 372, 1193–1203 (2015).
Kersten, S. & Stienstra, R. The role and regulation of the peroxisome proliferator activated receptor alpha in human liver. Biochimie 136, 75–84 (2017).
Hiukka, A., Maranghi, M., Matikainen, N. & Taskinen, M. R. PPARalpha: an emerging therapeutic target in diabetic microvascular damage. Nat. Rev. Endocrinol. 6(8), 454–463 (2010).
Keech, A. C. et al. Effect of fenofibrate on the need for laser treatment for diabetic retinopathy (FIELD study): a randomized controlled trial. Lancet 370, 1687–1697 (2007).
Chen, E. Y. et al. Effects of medical therapies on retinopathy progression in type 2 diabetes. N. Engl. J. Med. 363, 233–244 (2010).
Chen, Q. et al. Pathogenic role of microrna-21 in diabetic retinopathy through downregulation of PPARα. Diabetes 66(6), 1671–1682 (2017).
Bordet, R. et al. PPAR: a new pharmacological target for neuroprotection in stroke and neurodegenerative disease. Biochem. Soc. Trans. 34, 1341–1346 (2006).
Mysiorek, C. et al. Peroxisome-proliferator-activated receptor-alpha activation protects brain capillary endothelial cells from oxygen-glucose deprivation-induced hyperpermeability in the blood-brain barrier. Curr. Neurovasc. Res. 6, 181–193 (2009).
Lefebvre, P., Chinetti, G., Fruchart, J. C. & Staels, B. Sorting out the roles of PPAR alpha in energy metabolism and vascular homeostasis. J. Clin. Invest. 116, 571–580 (2006).
Deng, G. et al. Therapeutic effects of a novel agonist of peroxisome proliferator-activated receptor alpha for the treatment of diabetic retinopathy. Invest. Ophthalmol. Vis. Sci. 58(12), 5030–5042 (2017).
Knopp, R. H. et al. Effect of fenofibrate treatment on plasma lipoprotein lipids, high-density lipoprotein cholesterol subfractions, and apolipoproteins B, AI, AII, and E. Am. J. Med. 83(58), 75–84 (1987).
Raza-Iqbal, S. et al. Transcriptome analysis of K-877 (a novel selective PPARalpha modulator (SPPARMalpha))-regulated gene in primary human hepatocytes and mouse liver. J. Atheroscler. Thromb. 22, 754–772 (2015).
Takei, K. et al. Effects of K-877, a novel selective PPARα modulator, on small intestine contribute to the amelioration of hyperlipidemia in low-density lipoprotein receptor knockout mice. J. Pharmacol. Sci. 133(4), 214–222 (2017).
Honda, Y. et al. Pemafibrate, a novel selective peroxisome proliferator-activated receptor alpha modulator, improves the pathogenesis in a rodent model of nonalcoholic steatohepatitis. Sci. Rep. 14(7), 42477 (2017).
Sadler, J. E. Thrombomodulin structure and function. Thromb. Haemost. 78(1), 392–395 (1997).
Beffa, M. C., Burke, B. & Haudenschild, C. C. Prevention of thrombomodulin antigen on vascular and extravascular surfaces. J. Histochem. Cytochem. 25(11), 1267–1276 (1987).
Riewald, M., Petrovan, R. J., Donner, A. & Ruf, W. Activated protein C signals through the thrombin receptor PAR1 in endothelial cells. J. Endotoxin. Res. 9(5), 317–321 (2003).
Cheng, T. et al. Activated protein C blocks p53-mediated apoptosis in ischemic human endothelium and is neuroprotective. Nat. Med. 9(3), 338–342 (2003).
Bajzar, L., Manuel, R. & Nesheim, M. E. Purification and characterization of TAFI, a thrombin-activated fibrinolysis inhibitor. J. Biol. Chem. 270(24), 14477–14484 (1995).
Myles, T. et al. Thrombin activatable fibrinolysis inhibitor, a potential regulator of vascular inflammation. J. Biol. Chem. 278(51), 51059–51067 (2003).
Inoue, Y., Matsunawa, M., Sano, F. & Miura, I. Efficacy of recombinant human soluble thrombomodulin in treating disseminated intravascular coagulation complicating allogenic hematopoietic stem cell transplantation. Acta Haematol. 140(2), 121–127 (2018).
Yasuda, N. et al. The efficacy and safety of antithrombin and recombinant human thrombomodulin combination therapy in patients with severe sepsis and disseminated intravascular coagulation. J. Crit. Care 36, 29–34 (2016).
Lu, Y. F. et al. Icariin is a PPAR activator inducing lipid metabolic gene expression in mice. Molecules 19(11), 18179–18191 (2014).
Inoue, Y. et al. Cross-enhancement of ANGPTL4 transcription by HIF1 alpha and PPAR beta/delta is the result of the conformational proximity of two response elements. Genome Biol. 15(4), R63 (2014).
Schoonjans, K. et al. PPARalpha and PPARgamma activators direct a distinct tissue-specific transcriptional response via a PPRE in the lipoprotein lipase gene. EMBO J. 15(19), 5336–5348 (1996).
Yoshida, S., Yoshida, A., Ishibashi, T., Elner, S. G. & Elner, V. M. Role of MCP-1 and MIP-1 alpha in retinal neovascularization during postischemic inflammation in a mouse model of retinal neovascularization. J. Leukoc. Biol. 73, 137–144 (2003).
Miyamoto, K. et al. Prevention of leukostasis and vascular leakage in streprozotocin-induced diabetic retinopathy via intercellular adhesion molecule-1 inhibition. Proc. Natl. Acad. Sci. USA 96(19), 10836–10841 (1999).
Schmidt-Erfurth, U. et al. Guidelines for the management of diabetic macular edema by the European Society of Retina Specialists (EURETINA). Ophthalmologica 237(4), 185–222 (2017).
van der Meer, D. L. et al. Profiling of promoter occupancy by PPARalpha in human hepatoma cells via ChIP-chip analysis. Nucleic Acids Res. 38(39), 2839–2850 (2010).
Hamza, M. S. et al. De-novo identification of PPARgamma/RXR binding sites and direct targets during adipogenesis. PLoS ONE 4(3), e4907 (2009).
Zeller, K. I. et al. Global mapping of c-Myc binding sites and target gene networks in human B cells. Proc. Natl. Acad. Sci. USA 103(47), 17834–17839 (2006).
Chen, Y. et al. Therapeutic effects of PPAR agonist on diabetic retinopathy in type 1 diabetes models. Diabetes 62(1), 261–272 (2013).
Tomita, Y. et al. Pemafibrate prevents retinal pathological neovascularization by increasing FGF21 level in a murine oxygen-induced retinopathy model. Int. J. Mol. Sci. 20(23), 5878 (2019).
Panigrahy, D. et al. PPARalpha agonist fenofibrate suppresses tumor growth through direct and indirect angiogenesis inhibition. Proc. Natl. Acad. Sci. USA 105(3), 985–990 (2008).
Murugesan, N., Ustunkaya, T. & Feener, E. P. Thrombosis and hemorrhage in diabetic retinopathy: a perspective from an inflammatory standpoint. Semin. Thromb. Hemost. 41(6), 659–664 (2015).
Bastiaans, J. et al. The role of thrombin in proliferative vitreoretinopathy. Invest. Ophthalmol. Vis. Sci. 55(7), 4659–4666 (2014).
Abeyama, K. et al. The N-terminal domain of thrombomodulin sequesters high-mobility group-B1 protein, a novel anti-inflammatory mechanism. J. Clin. Invest. 115(5), 1267–1274 (2005).
Shi, C. S. et al. Lectin-like domain of thrombomodulin binds to its specific ligand Lewis Y antigen and neutralizes lipopolysaccharide-induced inflammatory response. Blood 112(9), 3661–3670 (2008).
Yang, H., Wang, H., Chavan, S. S. & Andersson, U. High mobility group box protein 1 (HMGB1): the prototypical endogenous danger molecule. Mol. Med. 21, 6–12 (2015).
Palumbo, R. et al. Cells migrating to sites of tissue damage in response to the danger signal HMGB1 require NF-kappaB activation. J. Cell. Biol. 179, 33–40 (2007).
Lin, Z. et al. Kruppel-like factor 2 (KLF-2) regulates endothelial thrombotic function. Circ. Res. 96(5), e48-57 (2005).
Horie, S. et al. Acceleration of thrombomodulin gene transcription by retinoid acid: retinoid acid receptors and Sp1 regulate the promoter activity through interactions with two different sequences in the 5’-flanking region of human gene. J. Biol. Chem. 276(4), 2440–2450 (2000).
Abe, Y. et al. JMJD1A is a single-sensing scaffold that regulates acute chromatin dynamics via SWI/SNF association for thermogenesis. Nat. Commun. 7(6), 7052. https://doi.org/10.1038/ncomms8052 (2015).
Okamura, M. et al. COUP-TFII acts downstream of Wnt/beta-catenin signal to silence PPARgamma gene expression and repress adipogenesis. Proc. Natl. Acad. Sci. USA 106(14), 5819–5824 (2009).
Wakabayashi, K. et al. The peroxisome proliferator-activated receptor gamma/retinoid X receptor alpha heterodimer targets the histone modification enzyme PR-set7/Setd8 gene and regulates adipogenesis through a positive feedback loop. Mol. Cell. Biol. 29(13), 3544–3555 (2009).
Lee, Y. J. et al. Essential role of transglutaminase 2 in vascular endothelial growth factor-induced vascular leakage in the retina of diabetic mice. Diabetes 65(8), 2414–2428 (2016).
Acknowledgements
We thank Dr. Jiro Kogo, Dr. Yasushi Kitaoka, and Yukari Hari for helpful discussions. Dr. Hitoshi Takagi is the guarantor of this work and as such had full access to all the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis.
Author information
Authors and Affiliations
Contributions
Y.M., T.I., T.T., T.K., J.S., and H.T. conceived of and planned the experiments. A.S., R.S., H.S., Y.A., and Y.M. performed the experiments. A.S., Y.M., and H.T. wrote the manuscript. T.I., T.T., T.K., H.A., and J.S. helped supervise the project.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Shiono, A., Sasaki, H., Sekine, R. et al. PPARα activation directly upregulates thrombomodulin in the diabetic retina. Sci Rep 10, 10837 (2020). https://doi.org/10.1038/s41598-020-67579-1
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-020-67579-1
This article is cited by
-
Impact of Selective Peroxisome Proliferator-Activated Receptor (PPAR)-α Modulators and Fibrates on Microvascular Disease: Is There Still Room?
Current Atherosclerosis Reports (2025)
-
Lessons from PROMINENT and prospects for pemafibrate
Cardiovascular Diabetology (2024)
-
Blood protein profiles related to preterm birth and retinopathy of prematurity
Pediatric Research (2022)
-
Pemafibrate prevents retinal neuronal cell death in NMDA-induced excitotoxicity via inhibition of p-c-Jun expression
Molecular Biology Reports (2021)
