
Abstract
Although there has been an increase in bench test evaluation of mechanical ventilators in recent years, a publication gap remains in assessing Pressure Control Continuous Mandatory Ventilation Modes with a set point targeting scheme PC-CMVs. This study evaluates the operational variability in PC-CMVs of eleven transport and emergency ventilators used in ICU units in Brazil during the COVID-19 pandemic. The assessment involved a comprehensive set of test scenarios derived from existing literature and the NBR ISO 80601-2-12:2014 standard. Nine parameters were computed for five consecutive breaths, offering a comprehensive characterization of pressure and flow waveforms. Most ventilators had Inspiratory pressure and PEEP values that fell outside of the tolerance ranges. Notably, three mechanical ventilators failed to reach the target pressures within the specified inspiratory times during test scenarios with a higher time constant (τ). We observed significant differences among emergency and transport ventilators in all assessed parameters, indicating a performance difference in PC-CMVs modes. The current results might help clinicians determine which ventilator models are suitable for specific clinical situations, particularly when unfavorable circumstances compel doctors to use ventilators that may not provide adequate support for patients in intensive care units.
Similar content being viewed by others

Introduction
PC-CMVs groups all the modes with different commercial names having the same composition and working principle. “PC” represents the control variable, which is pressure. CMV represents Continuous Mandatory Ventilation, which means that the mode is composed only of mandatory breaths (mandatory breaths are started by the machine or the patient, but they are always ended by the machine, in this case by time). Finally, “s” represents the targeting scheme, which tells us that the operator sets the level of pressure, and it will be the same in every breath1. Also, the operator sets the inspiratory time, positive-end expiratory pressure (PEEP), pressurization rate, FiO2, and respiratory rate. Other parameters, such as tidal volume and flow, vary as a function of the patient’s compliance and resistance. During inspiration, the mechanical ventilator inflates the patient’s lungs until the inspiratory time elapses. The degree of steepness can be controlled by pressurization rate adjustment. Nevertheless, the literature shows that how this parameter is configured widely varies among ventilator models, and the performance under the same test scenarios had different outcomes2,3. In the expiratory phase, the ventilator opens the expiratory valve to the environment, reducing the pressure until the PEEP value. The required time to reach the PEEP chiefly depends on the contribution of the lung’s resistive and elastic forces and the expiratory valve’s dynamic behaviour4. This mode is indicated when a patient undergoes general anesthesia and is routinely used after the first 48 h of mechanical ventilation5.
Over time, numerous studies have conducted comparisons between emergency, transport and home-care ventilators in bench tests that assess various assist modes6,7,8,9,10,11. However, these studies have highlighted a noticeable gap, as there is few research specifically addressing mandatory control modes. Most of the published studies used different test scenarios and focused on topline models. To note that it does not reflect the availability of mechanical ventilators in ICUs in low-income countries where many do not have adequate equipment12. Furthermore, the comparison between studies is limited due to the usage of different values of compliance, resistance, and settings during testing.
The lack of standard terminology in mechanical ventilation poses a problem when comparing studies, complicates clinical practice, and hinders communication between manufacturers and clients13. The literature has noted few attempts to address the lack of standard terminology for naming ventilation modes1,13,14 and to establish a standardized vocabulary15. Of note, in this study, we adopted the TAGS proposed by the taxonomy of modes1 to accurately identify the modes.
We hypothesized that an operational variability in PC-CMVs modes exists among different models of mechanical ventilators. This work aims to evaluate a group of variables in the PC-CMVs modes of a broad set of emergency and transport ventilators available in Brazil during the COVID-19 pandemic. To accomplish this goal, we gathered and adapted a range of parameters from the literature6,8,16,17,18 and the NBR ISO 80601-2-12:201419, which allowed us to point out differences in pressure and flow waveforms.
Materials and methods
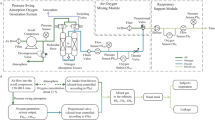
Mechanical ventilators were evaluated at the Institute for Technological Research (IPT) in São Paulo, Brazil. The employed setup is illustrated in Fig. 1. Patient`s compliance and resistance were emulated with a lung model (Dual adult training test lungs, Michigan Instruments, USA). Pressure signals were measured with a pressure transducer (FPM-02PG, Fujikura, Japan) connected to a pickoff adaptor. Flow signals were measured at the Y-piece, proximal to the lung model, using a pneumotachograph (model 3700B, Hans Rudolph, USA) attached to a differential pressure transducer (HCXM100D6V, SensorTechnics, USA). Both signals were conditioned using a signal conditioning module (SC-24, SCIREQ, Canada). Then, a data acquisition module (DAQ) (NI USB-6008, National Instruments, USA) digitized both signals for further processing.

Diagram of the test setup. Pressure and flow signals were acquired with a pressure transducer (FPM-02PG, Fujikura, Japan) and a pneumotachograph (model 3700B, Hans Rudolph, USA) connected to a data acquisition device (DAQ) (NI USB-6008, National Instruments, USA).
Protocol
Prior to each test, the mechanical ventilator’s self-test was accomplished. Then, a verification of the lung model’s compliance spring and a leakage test were performed according to the manufacturer. The pneumotachograph’s calibration was performed by the polynomial method20 employing a 1 L calibrated syringe, ten injection strokes, and a fourth-degree polynomial. The pressure transducer was calibrated with a U-shape water manometer applying a two-point calibration (0 and 20 \(\:{cmH}_{2}O\)). The sampling frequency was set to 100 Hz.
The mechanical ventilators were evaluated in test scenarios in CMV-PC according to standard NBR ISO 80601-2-12:201419, which is a faithful adaptation of the ISO 80601-2-12:201121. Each test scenario presented different settings for the lung model and the mechanical ventilator, as presented in Table 1. Of note, in the newest version of the ISO standard22, the set rate in line 3 was changed from 20 to 12 (breaths/min). For all mechanical ventilators, a medium level of pressurization rate was configured. A non-heated silicone ventilator circuit (22 mm, 1.5 m long) was used. In each test scenario, flow and pressure signals were recorded for 1 min after a 30-cycle stabilization period. A total of 5 breaths were analyzed for each test scenario. Finally, the digital signals underwent processing using a virtual instrument (LabVIEW 2015, National Instruments, USA).
Evaluated mechanical ventilators
All analyzed mechanical ventilator data regarding issue country and intended type of support were presented in Table 2; for each, an ID code was attributed to protect the relation between test results and manufacture. Mechanical ventilator E is technically similar to ventilator B. This equipment has undergone a rebranding process due to a transition from its previous manufacturer.
Evaluated variables
Nine parameters were computed to assess the recorded signals for five consecutive breaths. The start of inspiration (SI) and the start of expiration (SE) for each cycle were designated by a flow threshold of 0.05 L/s. A detailed graphical description of the evaluated parameters is depicted in Fig. 2.
-
\(\:{T}_{90}\): It measures the time needed to attain 90% of the set pressure starting from the initial SI.
-
Positive end-expiratory pressure\(\:\left(PEEP\right)\): The mean airway pressure at the final part of the expiratory phase within the previous 50 ms.
-
Inspiratory pressure: The mean airway pressure towards the end of the inspiratory stage within the previous 50 ms.
-
\(\:IA:\) The area beneath the airway pressure curve over the inspiratory stage.
-
\(\:{EA}_{above}\): The area bounded by the airway pressure and PEEP during the expiratory phase.
-
\(\:{EA}_{below}\): The area below PEEP is limited by the airway pressure during the expiratory phase.
-
\(\:{V}_{T}\): The delivered volume in each controlled breath.
-
Peak inspiratory pressure (PIP): The maximum pressure during the inspiratory stage.
-
Peak inspiratory flow (PIF): The maximum flow during the inspiratory stage.
We included tolerance ranges only for pressure \(\:(\pm\:\left[2+4\%\:of\:set\:pressure\right]\:cm{H}_{2}O)\), and PEEP (\(\pm 1\,cm\, H_2O\)), as these were the only parameters in this study for PC-CMVs modes that had recommendations from past research and normative guidelines6,19,23.
The monitored \(\:{V}_{T}\) displayed by the ventilator was recorded for three consecutive cycles and then compared to measured Vt by calculating the percent error. Accordingly, the Display error (%) was defined as: |(displayed Vt - measured Vt)| x 100% / measured Vt. Most ventilator manuals did not clearly specify the conditions under which volume measurements were taken for control and display. Therefore, we inferred that the conditions mentioned in the manuals apply to both control and display volumes. Ventilators A and F employ body temperature and pressure, dry (BTPD). Ventilators B, C, D and E employ body temperature and pressure, saturated (BTPS). Ventilator G, H, I, J and K employ ambient temperature and pressure, dry (ATPD).

Pressure and flow waveforms depicting the measured variables in the study: \(\:{T}_{90}\), Positive end-expiratory pressure\(\:PEEP\), Inspiratory pressure, \(\:IA\), \(\:EA_{above}\), \(\:EA_{below}\), \(\:{V}_{T}\), Peak inspiratory pressure (PIP) and Peak inspiratory flow (PIF).
Data analysis
Mean values are presented, along with their standard deviation (SD). Non-parametric methods were chosen due to the lack of Gaussian distribution in data from certain ventilators, as indicated by the Shapiro-Wilk test. The Kruskal-Walli’s test and Dunn’s test were employed as a post hoc analysis for conducting multiple comparisons. Statistical analysis was performed using software (Prism 7, GraphPad Software, USA). Hierarchical clustering was done to group mechanical ventilators and evaluate parameters, and the Euclidean distance was chosen. To avoid the dominance of the largest characteristic over others, each parameter is normalized by subtracting the mean value across all mechanical ventilators and dividing it by the standard deviation. Data processing and waveform plotting were performed using MATLAB®.
Results
Pressure and flow waveforms are plotted for all ventilators in Fig. S1 and S2 (supplementary material).
Inspiratory phase
Inspiratory pressure, \(\:{T}_{90}\) and \(\:IA\) differed significantly between mechanical ventilators for each test scenario \(\:\left(\rho<.05\right)\). Measurements are detailed in Table 3 and S2. Mean \(\:{T}_{90}\) for test scenarios 1, 2, 3, and 4 was: 0.69 ± 0.13, 0.61 ± 0.22, 0.55 ± 0.13, and 0.56 ± 0.18 s, respectively. In the first and second test scenarios, mechanical ventilators H, I, and J did not reach 90% of the set \(\:Inspiratory\:pressure\) during the inspiratory time. Moreover, mechanical ventilator I presented similar performance in the third and fourth test scenarios.
The measured Inspiratory pressure was greater than the set pressure only for mechanical ventilator A in the fourth test scenario, and for mechanical ventilator H in the second and fourth test scenarios. Only five ventilators (A, B, D, E and G) maintained \(\:Inspiratory\:pressure\) within the tolerance range (\(\:\pm\:[2+4\%\:of\:set\:pressure]\:cm{H}_{2}O\)) across all four test scenarios. Also, ventilator I presented values out of the recommended values in all test scenarios. Mean \(\:IA\) during the inspiratory phase was: 11.10 ± 1.49, 20.66 ± 1.96, 22.57 ± 2.25 and 28.81 ± 2.23 cmH2O.s for all the test scenarios.
Expiratory phase
In all four test scenarios, we identified significant differences \(\:\left(\rho\:<0.05\right)\) between mechanical ventilators for PEEP, \(\:{EA}_{above}\) and \(\:{EA}_{below}\) (Table S1 and S3 in the supplementary material). Higher values of Inspiratory pressure produced higher values of \(\:{EA}_{above}\) at the same values of PEEP. Mechanical ventilators (B, C, I, J, and K) had PEEP values out of the tolerance range of the set PEEP (\(\:\pm\:1{cmH}_{2}O\)) in at least, one test scenario.
In Fig. 3, mechanical ventilators were indicated as their PEEP concordance (\(\:setPEEP-PEEP\)) and their expiratory area (\(\:{EA}_{above}+{EA}_{below}\)). An ideal pressure waveform would have an immediate pressure change from the inspiratory pressure to PEEP (\(\:{EA}_{above}=0\:cm{H}_{2}O.s)\), and a steady control of PEEP (\(\:{EA}_{below}=PEEP\text{*}expiratory\:time\)). An ideal performance for each test scenario should lay on the center of each graph axis. Otherwise, as the results evidenced, most of the points lay on the right upper quadrant, suggesting that it is common for mechanical ventilators to have lower PEEP values and higher expiratory areas.

Mechanical ventilators are plotted on a plane, test scenarios 1, 2, 3 and 4 are presented in graphs A, C, B and D. The abscissa is the PEEP concordance (\(\:setPEEP-PEEP\)) and the ordinate is the expiratory area (\(\:{EA}_{above}+{EA}_{below}\)). To note that each axis intersection represents an ideal performance for each test scenario.
Volume delivery
Table 4 lists the \(\:{V}_{T}\) and \(\:PIF\) for each test scenarios, significant differences were found for both parameters \(\:\left(\rho<.05\right)\). \(\:{V}_{T}\) ranges were: \(\:0.200-0.636\), \(\:0.428-0.661\), \(\:0.456-0.613\) and \(0.410-0.542 L\); for test scenarios 1, 2, 3 and 4, sequentially. Mechanical ventilators H and J presented the lowest value of \(\:{V}_{T}\) and \(\:PIF\) in most of the test scenarios. Despite having the closest mean \(\:PIF\) values for each test scenario, some mechanical ventilators (C, H, I and K) failed to attain the set Inspiratory pressure within the required inspiratory time.
Display error for \(\:{V}_{T}\) is summarized in Table 5. Only ventilators A, F, and G consistently had differences lower than 10% mL across all test scenarios. Notably, two ventilators (E and J) showed differences greater than 20% in at least one test scenario.
Hierarchical clustering of the evaluated parameters and the mechanical ventilators for each test scenario were computed and presented in Fig. S3 (supplementary material). In each test scenario, we did not observe a defined clustering in function of type of ventilator (transport or emergency) or manufacturer. Regarding the evaluated parameters, in all test scenarios, \(\:{EA}_{below}\) and \(\:PEEP\) were grouped.
Discussion
A proper comparison between emergency and transport mechanical ventilators was not possible in our study due to the limited batch of transport ventilators. However, we observed that transport ventilators (I, J, and K) have the lowest \(\:Inspiratory\:pressure\) and the highest \(\:{T}_{90}\) when compared with emergency ventilators (Table 3). This result emphasized the fact that the usage of transport mechanical ventilators must be done carefully when providing support to critically ill patients.
The assessed mechanical ventilators employed different design approaches to deliver pressure control ventilation governed by a closed-loop system, in which the flow rate is adjusted in function of the feedback taken from the measured airway pressure24. In our study, test scenarios 1 and 2 had higher time constants (τ), so we expected higher rates to inflate the lung model. In the aforementioned test scenarios, flow pattern disparities were observed, particularly for ventilator C, H, I and J (see Fig. S2 supplementary material). To our surprise, these mechanical ventilators did not reach 90% of the set pressure (Table 3), although they shared similar \(\:PIF\) values (Table 4) with the rest of mechanical ventilators. Regarding the monitored \(\:{V}_{T}\), most of the mechanical ventilators overestimated the monitored volume (Table 5).
Significant differences were found for \(\:{T}_{90}\), \(\:Inspiratory\:pressure\) and \(\:IA\). However, to our knowledge, among these parameters, there are only standard prescriptions for \(\:Inspiratory\:pressure\). It is essential to highlight that in our study, only a medium pressurization rate was assessed; so other pressurization rate configurations will have different outcomes of \(\:{T}_{90}\), and \(\:IA\). The selection of a medium pressurization rate was due to the limited time to assess the mechanical ventilators and the lack of a standard pattern to select pressurization rate options among mechanical ventilators; for instance, there were bar charts, percentages, or numbers to choose between pressurization rate levels among models. The clinical impact of our findings is difficult to stay; nevertheless, clinically, there is an agreement on quick times to pressurize the lungs17, and our results pointed out an existing problem with standardization of \(\:{T}_{90}\) between manufacturers.
\(\:PEEP\) was measured as the average pressure over the last 50 ms of the expiration time as it is recommended by the NBR ISO standard21; to note, this analysis will not bring information about the pressure curve prior to that period. This can be observed in the pressure waveforms during expiration in Fig. S1 (supplementary material). Therefore, we computed the \(\:{EA}_{above}\) and \(\:{EA}_{below}\) to characterize the airway pressure waveform over the course of the expiratory stage. The operational variability of these parameters across the batch of mechanical ventilators could be related to the resistance of the expiratory valve that differs between mechanical ventilators and control systems. Based on this line of thought, we may expect that mechanical ventilators of the same manufacturer would have similar values of PEEP, \(\:{EA}_{above}\) and \(\:{EA}_{below}\) (see Table S1 and S3); however, equipment with similar technology: A and F, and B and E had different outcomes.
The cluster analysis evidenced that only \(\:{EA}_{below}\) and \(\:PEEP\) grouped across test scenarios. This suggests that changes in \(\:{EA}_{above}\) may not be informed by \(\:PEEP\) readings. As shown in Fig. 3, there is discordance, between the information provided by measured PEEP about how well the mechanical ventilator deals with the control of airway pressure at the end of the expiratory phase. In all the test scenarios, most of the mechanical ventilators were in the right upper quadrant meaning that the pressurization was greater than the ideal performance. Even more, we found that despite having the closest values of PEEP concordance, a group of mechanical ventilators had different values of \(\:{EA}_{above}+{EA}_{below}\), e.g., in test scenario 3, mechanical ventilators B, H, and J presented this result. Not knowing how the \(\:{EA}_{above}+{EA}_{below}\) varies among different brands and models of mechanical ventilators may impact clinical studies in which specific settings of \(\:PEEP\) will be applied. This finding is particularly worrisome because, as suggested in previous studies, repeated derecruitment due to variation of \(\:{EA}_{above}\) and \(\:{EA}_{below}\) could be not suitable for patient with lung injury25.
The clinical implications of our findings underscore the potential impact of ventilator operational variability on patient support. Inadequate pressure settings often result in insufficient tidal volumes, leading to hypoventilation, hypercapnia, and hypoxemia. These conditions increase the risk of ventilator-induced lung injury (VILI). Incorrect PEEP values, for example, can contribute to alveolar collapse, particularly in patients with acute respiratory distress syndrome (ARDS)26. Proper adjustment of inspiratory pressure or drive pressure is crucial for optimal patient ventilation supports previous evidence in the available literature27,28,29. Therefore, fluctuations or inconsistencies in pressure delivery can negatively impact patient outcomes, potentially causing barotrauma, volutrauma, or atelectrauma. Furthermore, if the mechanical ventilator fails to deliver the target pressure or volume accurately and within the required timeframe (as delimited by NBR ISO 80601-2-12:201419), clinical feedback and ventilatory reliability are compromised. Additionally, hemodynamic instability can ensue due to fluctuating intrathoracic pressures affecting cardiac output. Moreover, patient-ventilator asynchrony often results from a misalignment between patient effort and ventilator support, increasing patient discomfort and effort, and possibly necessitating more analgesia or anesthesia30. Prolonged ventilation with inadequate support increases the risk of ventilator-associated pneumonia31 and delays weaning efforts, prolonging ICU stays and complicating recovery.
The study has significant limitations. First, rather than actual patients, we performed the bench evaluation using a mechanical lung model. This lung model exhibits linear behavior during ventilation, which does not occur when a patient is mechanically ventilated (compliance varies with volume). However, the use of lung models enables the comparison of mechanical ventilators under similar setups. Second, only one mechanical ventilator per model was assessed. While we have verified the equipment through the recommended auto test by the manufacturer, we cannot guarantee that the performance of specific models of mechanical ventilators will be identical. Finally, we only assessed one pressurization rate configuration. The decision was made because of the shortened assessment period permitted by the pandemic limits.
Conclusion
Even though the operational variability of the mechanical ventilator presented in all test scenarios supports previous evidence in the available literature16,17,32, comparing past bench assessments is difficult because of differences in test scenarios and ventilation modes. It is concerning that ventilators exhibited varying performance when tested with a simulated passive patient under identical settings.
Our findings, along with other similar studies, will help clinicians ponder which mechanical ventilators are suitable for specific clinical contexts. Especially when adverse situations, e.g., the COVID-19 pandemic, force clinicians to employ life-support devices that cannot provide the care patients require in intensive care units33. The disparity between set values and actual measurements during mechanical ventilation could potentially pose a threat in patient management31,34.
Data Availability
The datasets used and analyzed during the current study are available from the corresponding author on reasonable request.
Data availability
The datasets used and analysed during the current study available from the corresponding author on reasonable request.
References
Chatburn, R. L., El-Khatib, M. & Mireles-Cabodevila, E. A taxonomy for mechanical ventilation: 10 fundamental maxims. Respir Care. 59, 1747–1763. https://doi.org/10.4187/RESPCARE.03057 (2014).
Gonzales, J. F., Russian, C. J., Marshall, S. G., Collins, K. P. & Farmer, T. A. Comparing the effects of rise time and Inspiratory Cycling Criteria between four different mechanical ventilators. In: Am Thorac Soc. American Thoracic Society, A1704–A1704 (2011).
Gonzales, J. F., Russian, C. J., Gregg Marshall, S., Collins, K. P. & Farmer, T. A. Comparing the effects of rise time and Inspiratory Cycling Criteria on 6 different mechanical ventilators. Respir Care. 58, 465–473. https://doi.org/10.4187/respcare.01345 (2013).
Truwit, J. D. & Marini, J. J. Evaluation of thoracic mechanics in the ventilated patient part II: Applied mechanics. J. Crit. Care. 3, 199–213. https://doi.org/10.1016/0883-9441(88)90092-5 (1988).
Rittayamai, N. et al. Pressure-controlled vs volume-controlled ventilation in Acute Respiratory failure: a physiology-based narrative and systematic review. Chest. 148, 340–355. https://doi.org/10.1378/CHEST.14-3169 (2015).
Garnier, M. et al. Multifaceted bench comparative evaluation of latest intensive care unit ventilators. Br. J. Anaesth.115, 89–98. https://doi.org/10.1093/bja/aev028 (2015).
Krieger, T. J. & Wald, M. Volume-targeted ventilation in the neonate: Benchmarking ventilators on an active lung model. Pediatr. Crit. Care Med.18, 241–248. https://doi.org/10.1097/PCC.0000000000001088 (2017).
Boussen, S., Gainnier, M. & Michelet, P. Evaluation of Ventilators Used During Transport of Critically Ill Patients: A Bench Study. (2013). https://doi.org/10.4187/respcare.02144
Thille, A. W., Lyazidi, A., Richard, J. C. M., Galia, F. & Brochard, L. A bench study of intensive-care-unit ventilators: New versus old and turbine-based versus compressed gas-based ventilators. Intensive Care Med.35, 1368–1376. https://doi.org/10.1007/S00134-009-1467-7/FIGURES/7 (2009).
Takeuchi, M., Williams, P., Hess, D. & Kacmarek, R. M. Continuous positive Airway pressure in New-generation mechanical VentilatorsA lung model study. Anesthesiology. 96, 162–172. https://doi.org/10.1097/00000542-200201000-00030 (2002).
Jaber, S. et al. Performance characteristics of five New Anesthesia ventilators and four intensive care ventilators in pressure-support ModeA comparative bench study. Anesthesiology. 105, 944–952. https://doi.org/10.1097/00000542-200611000-00015 (2006).
Martin-Delgado, J. et al. Campos De Andrade Lourenç Ão Id D, Campos P, Baptista P, Ramirez G, Mira JJ Availability of personal protective equipment and diagnostic and treatment facilities for healthcare workers involved in COVID-19 care: A cross-sectional study in Brazil, Colombia, and Ecuador. (2020). https://doi.org/10.1371/journal.pone.0242185
Chatburn, R. L., Volsko, T. A., Hazy, J., Harris, L. N. & Sanders, S. Determining the basis for a taxonomy of mechanical ventilation. Respir Care. 57, 514–524. https://doi.org/10.4187/RESPCARE.01327 (2012).
Chatburn, R. L. Classification of Ventilator Modes: Update and Proposal for Implementation. Respir Care 52: Respiratory care 52.3 (2007): 301–323 (2007).
International Organization for Standardization. ISO 19223:2019 Lung ventilators and related equipment — Vocabulary and semantics. 1:140 (2019).
Purris Williams, R. R. T. et al. Pressure support and pressure assist/control: are there differences? An evaluation of the newest intensive care unit ventilators. Respir Care. 45, 1169 (2000).
Marchese, A. D., Sulemanji, D., Chipman, D., Villar, J. & Kacmarek, R. M. Performance of current intensive care unit ventilators during pressure and volume ventilation. Respir Care. 56, 928–940. https://doi.org/10.4187/RESPCARE.00981 (2011).
Chatburn, R. L. Simulation-based evaluation of mechanical ventilators. Respir Care. 63, 936–940. https://doi.org/10.4187/RESPCARE.06267 (2018).
Associação Brasileira de Normas Técnicas. NBR ISO 80601-2-12:2014 Requisitos particulares para a segurança básica e o desempenho essencial de ventiladores para cuidados críticos (2014).
Tang, Y., Turner, M. J., Yem, J. S. & Baker, A. B. Calibration of pneumotachographs using a calibrated syringe. J. Appl. Physiol.95, 571–576 (2003).
International Organization for Standardization. ISO 80601-2-12:2011 Medical Electrical equipment — Part 2–12 (Particular requirements for basic safety and essential performance of critical care ventilators, 2011).
International Organization for Standardization. ISO 80601-2-12:2020 Medical Electrical equipment — Part 2–12 (Particular requirements for basic safety and essential performance of critical care ventilators, 2020).
Specification for Rapidly Manufactured Ventilator System (RMVS) & - GOV.UK. https://www.gov.uk/government/publications/specification-for-ventilators-to-be-used-in-uk-hospitals-during-the-coronavirus-covid-19-outbreak/rapidly-manufactured-ventilator-system-rmvs. Accessed 24 Aug 2024.
Stayer, S. A., Bent, S. T., Skjonsby, B. S., Frolov, A. & Andropoulos, D. B. Pressure control ventilation: three anesthesia ventilators compared using an infant lung model. Anesth. Analg. 91, 1145–1150. https://doi.org/10.1213/00000539-200011000-00020 (2000).
Pinède, A. et al. Bench Assessment of Expiratory Valve Resistance of current ICU ventilators in dynamic conditions. Respir Care. 66, 610–618. https://doi.org/10.4187/RESPCARE.08098 (2021).
Briel, M. et al. Higher vs lower positive end-expiratory pressure in patients with acute lung injury and acute respiratory distress syndrome: systematic review and meta-analysis. JAMA. 303, 865–873. https://doi.org/10.1001/JAMA.2010.218 (2010).
Finfer, S. R., Vincent, J-L., Slutsky, A. S. & Ranieri, V. M. Ventilator-Induced Lung Injury. N. Engl. J. Med.369, 2126–2136. https://doi.org/10.1056/NEJMRA1208707 (2013).
Amato, M. B. P. et al. Driving pressure and survival in the Acute Respiratory Distress Syndrome. N. Engl. J. Med.372, 747–755. https://doi.org/10.1056/NEJMSA1410639/SUPPL_FILE/NEJMSA1410639_DISCLOSURES.PDF (2015).
Neto, A. S. et al. Association between Use of Lung-Protective Ventilation with Lower Tidal volumes and clinical outcomes among patients without Acute Respiratory Distress Syndrome: a Meta-analysis. JAMA. 308, 1651–1659. https://doi.org/10.1001/JAMA.2012.13730 (2012).
Chanques, G. et al. Impact of ventilator adjustment and sedation-analgesia practices on severe asynchrony in patients ventilated in assist-control mode. Crit. Care Med.41, 2177–2187. https://doi.org/10.1097/CCM.0B013E31828C2D7A (2013).
Papazian, L., Klompas, M. & Luyt, C. E. Ventilator-associated pneumonia in adults: a narrative review. Intensive Care Med.46, 888–906. https://doi.org/10.1007/S00134-020-05980-0 (2020).
Tung, A., Drum, M. L. & Morgan, S. Effect of inspiratory time on tidal volume delivery in anesthesia and intensive care unit ventilators operating in pressure control mode. J. Clin. Anesth.17, 8–15. https://doi.org/10.1016/J.JCLINANE.2004.02.005 (2005).
Iyengar, K., Bahl, S. & Raju Vaishya, Vaish, A. Challenges and solutions in meeting up the urgent requirement of ventilators for COVID-19 patients. Diabetes Metabolic Syndrome: Clin. Res. Reviews. 14, 499–501. https://doi.org/10.1016/J.DSX.2020.04.048 (2020).
Hu, X. et al. Scoring system to evaluate the performance of ICU ventilators in the pandemic of COVID-19: a lung model study. Front. Med. (Lausanne). 8663608. https://doi.org/10.3389/FMED.2021.663608 (2021).
Acknowledgements
We would like to thank to the members of the laboratory of final uses and energy management at the Institute for Technological Research, Sao Paulo.
Funding
This study was financed in part by the Conselho Nacional de Desenvolvimento Científico e Tecnológico (CNPq - Brazilian National Council for Scientific and Technological Development) - Brazil (380077/2021-3, 133814/2019-0 and 308280/2019-9) and the Coordenação de Aperfeiçoamento de Pessoal de Nível Superior - Brazil (CAPES) - Finance Code 001 (grant number 88887.495969/2020-00).
Author information
Authors and Affiliations
Contributions
All authors contributed to data collection and review of the document. Furthermore, Lino-Alvarado Alembert and Henrique Takachi Moriya took charge of conducting the literature search, formulating the study design, and preparing the manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Lino-Alvarado, A., de Lima Vitorasso, R., de Oliveira Rosa, D.A. et al. Bench assessment of PC-CMVs modes in transport and emergency ventilators under ICU conditions. Sci Rep 14, 22570 (2024). https://doi.org/10.1038/s41598-024-73056-w
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-024-73056-w
