
Abstract
This study evaluates the impact of video-based approaches on health education. PUBMED, Web of Science, EMBASE, CENTRAL, and LILACS databases were searched from their inception until November 2022. Randomised controlled trials (RCTs) and non-randomized studies on interventions were included in this review. Studies were grouped according to their reported learning outcomes. A random effects meta-analysis was performed. Meta-regression analyses were used to explore the effects of confounding variables on the overall estimates. Forty studies were included in this meta-analysis. The results showed that video-based learning (VBL) has a significant effect on ‘knowledge acquisition’ in dentistry (Cohen’s d = 2.18), moderate effect in medicine (Cohen’s d = 0.67); moderate effect on ‘skills development’ in medicine (Cohen’s d = 0.76) and nursing (Cohen’s d = 0.59); overall moderate effect on ‘attitude’ (Cohen’s d = 0.74). Egger’s test was performed to assess potential publication bias. VBL offers a valuable educational tool for knowledge acquisition, skill development, and attitude changes in health education. The theoretical and practical implications of these findings are also discussed. To strengthen the evidence base, future research should address the limitations found, such as the high risk of bias (RoB), and employ rigorous study designs when investigating the role of multimedia learning in various academic disciplines.
Similar content being viewed by others


Background
Video-based learning (VBL) has emerged as a powerful tool in education, providing a dynamic and engaging medium for delivering content1. As its popularity grows, it is important to understand what VBL is and to explore its potential applications in specific areas, such as health education2. VBL refers to the knowledge or skills acquired through teaching via Video3. This involves the use of videos to convey information, demonstrate concepts, and engage learners in a multimedia format4. Video-based approaches encompass a variety of methods and strategies used to enhance students’ engagement and learning through video, which is particularly useful in areas that involve practical skills such as health education5,6,7. This approach promotes critical thinking, dialogue, and peer-to-peer learning8,9,10. In addition to being learner-centred, VBL approaches offer several benefits, including increased engagement, accessibility and flexibility in learning1,11,12. These approaches cater to different learning preferences and can be accessed anytime and anywhere, making them valuable tools for modern education and training.
In the realm of educational psychology, the Cognitive Theory of Multimedia Learning posits that the use of multimedia, such as video, can enhance learning by engaging multiple sensory channels, thereby improving knowledge retention and comprehension13. When applied to health education, this theory suggests that the combination of visual and auditory elements in VBL can facilitate a deeper understanding of complex medical concepts, thereby fostering more effective knowledge acquisition. Furthermore, the Theory of Experiential Learning aligns with VBL’s capacity to bridge theoretical knowledge and practical application. This theory, developed by David Kolb, underscores the importance of hands-on, experiential learning. VBL allows students to witness medical procedures and clinical practices through video, providing them with a virtual firsthand experience. By engaging learners in practical scenarios, VBL can encourage the application of knowledge in real-world health settings14.
In health education, VBL holds great promise for improving knowledge acquisition and skill development. By harnessing the visual and auditory elements of video, health professionals and students can access a wide range of educational resources15. By demonstrating medical procedures and techniques to present complex concepts in a simplified manner, videos can potentially bridge the gap between theory and practice in health education16.
In the domains of psychology and social sciences, Attitude Change Theories play a significant role in understanding how individuals’ attitudes, beliefs, and behaviors can be influenced through persuasive communication and observational learning. For example, the Elaboration Likelihood Model17, emphasizes the central and peripheral routes to persuasion. When applied to health education, this theory can help us assess how video-based messaging influences the cognitive processing of health information, potentially leading to attitude changes and informed decision-making. The Social Cognitive Theory18 focuses on observational learning and the influence of role models on learning. In the context of health education, this theory suggests that VBL can offer students the opportunity to observe and learn from experts and role models in the medical field, potentially affecting their attitudes, self-efficacy, and motivation.
The impact and effectiveness of VBL in health education has been the focused of several randomized trials. An opportunity emerges to comprehensively assess the existing evidence in this regard, providing useful and focused information on the benefits, challenges, and outcomes associated with VBL in health education. Such evidence-based synthesis may provide relevant insights into instructional design strategies, curriculum development, and the integration of technology into health education programmes3,19,20 .
Herein, we report the results of a systematic review of the impact of VBL on several educational outcomes compared to non-VBL approaches. Our primary research question, structured as a PICO framework, was as follows: “Among students majoring in health education (Population), does the utilization of a VBL approach (Intervention) yield superior learning outcomes when compared to non-VBL approaches (Comparator)?” The outcomes of interest encompass various aspects of learning outcomes (Outcomes).
The significance of this study is multi-faceted. It serves as a response to the pressing need for evidence-based guidance in the utilization of video-based learning (VBL) in health education. Although VBL has gained recognition as a valuable tool, its specific impact on learning outcomes remains an area of uncertainty. By systematically analyzing a wide range of studies, our meta-analysis sought to consolidate and clarify the often mixed findings in the VBL literature. This study was designed to bridge gaps in our current understanding, offering a comprehensive view of VBL’s effectiveness in health education. It addresses the need for practical insights that can influence instructional design, curriculum development, and the integration of technology into health education programs.
This research contributes to the advancement of knowledge in this field and provides the basis for informed decision-making in educational practice and healthcare delivery. In addition, the reported findings can guide policymakers, educators, and practitioners in adopting evidence-based approaches to enhance the learning experience and improve health outcomes21.
Methods and findings
This systematic review protocol was previously determined by all the authors and was registered at the National Institute for Health Research PROSPERO, International Prospective Register of Systematic Reviews (http://www.crd.york.ac.uk/PROSPERO, ID Number: CRD42021230675). The review design followed the Cochrane Handbook of Systematic Reviews of Interventions22 and was reported in accordance with the updated Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA)23. The PRISMA checklist is provided as a supplemental file (Table S1).
Type of studies, type of intervention, and inclusion criteria
The types of studies considered for inclusion in this research encompassed both randomised controlled trials (RCTs) and non-randomized studies of intervention. RCTs are widely recognized as the gold standard for evaluating the effectiveness of interventions, as they involve randomly assigning participants to either an intervention or a control group. On the other hand, non-randomized studies of intervention, employ alternative methodologies that do not involve randomization, such as quasi-experimental designs or observational studies. By including both types of studies, we aimed to comprehensively evaluate the effectiveness of video-based learning approaches using various research designs.
This study focused on video-based learning approaches. These approaches involve the use of videos as educational tools to deliver instructional content or to facilitate learning experiences.
To ensure that the selected studies were relevant to our research objectives, we applied specific inclusion criteria. Studies had to: (1) report on interventional approaches using VBL; (2) be a controlled study of intervention, enabling a comparison of VBL vs. non-VBL; (3) include a baseline analysis, which would provide essential information on the participants’ characteristics and establish a starting point for assessing the intervention’s effects; (4) report learning outcomes measures, to allow estimation of effect size; and (5) be publicly available through the library archive.
In case of additional data clarifications, the corresponding author of the included study was contacted via e-mail, and if unsuccessful, one week later.
Primary and secondary outcomes
The primary outcome of this systematic review was the impact of VBL on knowledge acquisition in health education. The secondary outcomes include the usefulness of VBL, skills development, knowledge application, attitude, anxiety and motivation in the same setting.
Information sources search
The search strategy sought to identify all studies reporting the impact of VBL approaches in health education that were conducted and published until November 2022. By setting this time limit, we ensured that the review captured the most recent evidence in the field.
Detailed search strategies were conducted without language restrictions using the following electronic databases: PubMed, Web of Science, LILACS (Latin-American scientific literature in health sciences), Embase and the Cochrane Central Register of Controlled Trials (CENTRAL). The search algorithm, developed using keywords and the Medical Subject Headings (MeSHs), was: (video OR “video learning” OR “e-learning” OR “educational video” OR “online lectures” OR multimedia) AND student* AND (health OR medic* OR dent* OR nurs*) AND (education[MeSH] OR teaching[MeSH]) AND (results OR test OR grades OR marks OR “examination results” OR assessment OR “academic performance” OR “academic achievement” OR “educational outcomes”) AND (randomised OR randomized OR randomly OR trial). For the remaining databases the search was adapted accordingly. In addition, a grey literature search was conducted to ensure comprehensive coverage of the available evidence. Resources listed on the NIH Library’s systematic review services page, which provides access to databases and tools designed to capture grey literature, including unpublished studies, conference proceedings and other non-traditional published materials, were used. The grey literature search also included OpenGrey, a dedicated repository for grey literature in Europe.
By including grey literature in the search strategy, this systematic review aimed to minimise publication bias and capture a wide range of evidence, including sources not typically indexed in standard databases.
Study selection
Two researchers independently selected the relevant articles by screening all the titles and abstracts, excluding irrelevant studies. Any paper classified as potentially eligible by either reviewer was appraised by a full-text reading, and the reasons for exclusion were fully detailed. Each study was excluded based on one or more of the following criteria: studies that did not report on the specific learning outcomes we were investigating were excluded due to lack of outcomes of interest; studies with designs that did not meet the methodological standards for our review, such as literature and systematic reviews (as these were deemed to have inappropriate designs); studies that did not provide baseline measurements, making it impossible to assess changes over time or the impact of the intervention were excluded due to lack of baseline data; studies that combined VBL approaches with other educational interventions, making it difficult to isolate the effects of VBL; studies that lacked an independent control group against which to compare the effects of the VBL intervention; studies for which the full text was not accessible, preventing thorough analysis and extraction of relevant data; and studies that reported results in a way that was unsuitable for data extraction and synthesis in our review. These exclusion criteria ensured that we maintained a high standard of methodological rigour and relevance, focusing on studies that could reliably contribute to answering our research question about the effectiveness of VBL approaches in health education. Any disagreement was resolved through discussion with a third reviewer, and a decision was arrived at by consensus.
Data extraction process and data items
The studies that fulfilled the inclusion criteria were organized into evidence tables describing the characteristics and results of each study, including study identification (i.e., first author’s name and publication year), country of origin of the research, country coordinates, inclusion and exclusion criteria, characteristics and number of participants, and outcome measures. We later added the methodological risk of bias of the study (detailed in 2.6 Risk of Bias assessment). All disagreements were resolved by discussion with a third reviewer.
Field of study, intervention and control type, outcomes and type of assessment
This section provides a comprehensive overview of the different components and methods used in the study. It explains the types of intervention and control (Tables 1 and 2 respectively), outcomes (Table 3) and types of evaluation (Table 4) used to investigate the research objectives.
Risk of bias assessment
The methodological quality of the included studies was assessed by two independent reviewers using the Cochrane risk-of-bias tool for randomised trials (RoB 2)48, since all of the included studies were RCTs. Disagreements were resolved by discussion with a third reviewer.
The RoB 2 tool is designed to assess the methodological quality and potential sources of bias in individual trials. The RoB 2 tool consists of five domains, each of which assesses specific aspects of study design and conduct, namely the randomisation process (considering whether the allocation sequence was truly random, concealed and correctly implemented, minimising selection bias); deviation from intended interventions (considering whether any deviations from the planned protocol may have introduced bias); missing outcome data (considering the methods used to measure the outcomes of interest, assessing the impact of missing data on the study results and the potential for bias); measurement of the outcome (considering the validity, reliability and precision of the outcome measures used, and the potential for bias in their assessment); and selection of the reported outcome (considering the potential for selective reporting of outcomes that may introduce bias and distort the overall results)48.
Each item in the RoB 2 tool was assessed independently, and a judgement of low risk of bias, some concern, or high risk of bias was made for each domain.
The overall risk of bias in a study was determined using the following criteria: a study was considered to have a low risk of bias if it was methodologically sound and credible in all domains for a given outcome. If a study raises some concerns in at least one domain for a particular outcome but does not meet the criteria for high risk of bias in any domain, it is classified as having some concerns. However, a study is considered to have a high risk of bias if it has significant methodological flaws or limitations in at least one domain for a particular outcome. This finding indicates the presence of significant biases that may substantially reduce confidence in the study’s findings and affect the reliability and trustworthiness of the results48.
Statistical analysis
The extracted data was organized into evidence tables. Because of the existence of learning outcome measures we could not assume the existence of a true effect size, thus we employed a random effects model49, as previously described50. All random-effects meta-analysis and forest plots were performed in R version 3.4.1 using ‘meta’ package50. The percentage of total variability due to between-study heterogeneity was explored using the I2 index and Cochrane’s Q statistic (p < 0.1), and χ2 test for the overall homogeneity22. Substantial between-study heterogeneity was defined as I2 > 50%. All tests were two-tailed, with an alpha value set at 0.05 (5%).
We conducted a series of a priori sensitivity analyses to examine the effect of the risk of bias on overall estimates. Meta-regression was used to explore the adjusting effects of particular confounding variables on the learning outcomes, particularly time of intervention, latitude, longitude and study sample size.
Whenever the number of included trials prevented conducting meta-analyses, we employed the synthesis without meta-analysis (SWiM) in systematic reviews guideline51.
Findings
Study selection
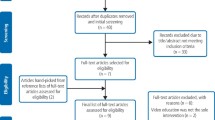
The electronic searches resulted in a total of 4,035 records (1,134 from PubMed, 1,204 from CENTRAL, 1,077 from Embase and 620 from Web of Science) (Figure S1). After removing duplicates, 1,957 articles were excluded based on the title/ abstract assessment and 30 articles could not be accessed through the library. Of the remaining articles, 283 articles were excluded from the full-text appraisal, because they did not meet the inclusion criteria (with the respective reason detailed in Table S2). Finally, a total of 40 articles38,52,53,54,55,56,57,58,59,60,61,62,63,64,65,66,67,68,69,70,71,72,73,74,75,76,77,78,79,80,81,82,83,84,85,86,87,88,89,90 were included in the qualitative and quantitative analyses of the present systematic review.
Study characteristics
Studies from 23 different countries in Asia, America, Europe, Australia and Africa were included (Table 5). Europe accounts for the majority of included studies with 37.5% of the total, with the United Kingdom (n = 4) and Germany (n = 3) being prominent contributors. Asia follows with 27.5%, with Iran (n = 3) being the most prominent contributor. North America accounts for 22.5%, mainly represented by the United States (n = 8). Oceania and South America contribute 7.5% and 5.0% respectively, with Australia (n = 3) and Brazil (n = 2) being prominent contributors.
The classification shown in Table 6 highlights the economic diversity of the countries included in the systematic review and provides valuable insights into the study characteristics within different economic contexts. High-income countries (HIC) have a significant presence, accounting for 72.5% of the total number of studies (n = 29). Upper middle income countries (UMIC) contribute 12.5% with 5 studies, while lower middle income countries (LMIC) account for 15.0% with a total of 6 studies included.
When categorising the background of the participants (Table 7), medicine dominates (62.5%; n = 25), focusing on different sub-domains such as surgery (n = 7), clinical practice (n = 6) and emergency medicine (n = 2) . Nursing contributes 20.0% (n = 8), mainly in clinical practice. Dentistry, at 10.0% (n = 4), covers areas such as clinical practice (n = 1), ergonomics (n = 1), oral cancer (n = 1) and restorative dentistry (n = 1). The combined field of medicine/nursing accounts for 2.5%, with an emphasis on emergency medicine. Psychology and Veterinary Medicine each contribute 2.5%, exploring neurogenerative diseases and anaesthesia respectively. This diverse distribution of participants’ backgrounds underlines the comprehensive nature of the systematic review, covering different areas of health services research. Among the 40 included studies, there is a notable focus on practice areas, particularly clinical practice (30.0%; n = 12) and surgery (20.0%; n = 8).
Table 8 shows the distribution of studies according to the course stage of the participants. The majority of studies, 42.2%, involve participants in the preclinical stage, emphasizing basic education and early clinical exposure (n = 19). The basic course stage accounts for 20.0%, highlighting the importance of basic knowledge (n = 9). Participants in the clinical phase account for 24.4%, indicating active engagement in clinical training and practice (n = 11). Postgraduate studies account for 4.4%, demonstrating a focus on advanced training and specialisation (n = 2). Notably, 8.9% of the studies do not specify the course stage of the participants, adding variability to the dataset (n = 4). Some studies were conducted at several levels of study.
The distribution of participants’ year of study is characterised in Table 9. Second year participants have the highest representation with 23.2% of the included studies, followed by first year participants with 17.9%. The distribution gradually decreases for subsequent years, with the third, fourth, fifth and sixth years representing 16.1%, 14.3%, 7.1% and 7.1% respectively. Residents make a minimal contribution of 1.8%. It is noteworthy that 12.5% of the studies do not specify the year of study of the participants.
Risk of bias
Thirty studies were considered to have a moderate risk of bias38,52,53,54,55,57,59,61,62,63,64,65,67,69,70,71,72,74,76,78,79,80,81,81,83,84,85,86,87,88,90, 5 studies were considered to have a low risk of bias56,66,68,77,82, while 5 studies58,60,73,75,89 were considered to have a high risk of bias (Figure S2 and Figure S3). The majority of studies had shortcomings mainly in the area of randomization process, which accounted for 57.5% (n = 23) of the included studies. In addition, deviations from the intended interventions accounted for 47.5% (n = 19) of the studies. On the other hand, failures in the domain of missing outcome data were relatively low, accounting for 30.0% (n = 12), and failures in the domain of outcome measurement accounted for 40.0% (n = 16). Overall, a suboptimal risk of bias was found in 57.5% (n = 23) of the included studies. Inter-observer reliability in risk of bias assessment was considered excellent (κ score = 0.87, 95% CI: 0.61-1.00).
Pooled estimates
We began our analysis by exploring the impact of the methodological quality in the overall pooling estimates. Overall, low risk trials (Effect size [ES] = 1.20, 95% CI: 0.69–1.71; I2 = 99.9%) reported significantly lower difference (p = 0.0379) compared to moderate (Effect size [ES] = 0.48, 95% CI: 0.21–0.75; I2 = 0.0%) and high risk studies (Effect size [ES] = 1.02, 95% CI: -0.01-2.05; I2 = 96.7%). Following the Cochrane Handbook instructions, we decided to report data as overall (that is, including all studies regardless of the methodological quality) and results stratified by risk of bias level91.
In addition, we assessed whether sample size could influence the overall results through meta-regression, yet we observed no significance on this association (estimate = -0.00, SE = 0.00, p = 0.281).
Overall, seven outcomes were reported among the included trials: ‘Knowledge Acquisition’ (n = 20), ‘Skills Development’ (n = 16), ‘Attitude’ (n = 9)38,52,56,57,59,62,65,66,67,68,69,70,75,78,79,81,82,83,84,87,89,902], ‘Anxiety’ (n = 3)38,58,63, ‘Motivation’ (n = 2)82,89, ‘Knowledge Application’ (n = 1)88 and ‘Usefulness’ (n = 1)38. Two studies reported data for 3 outcomes38,82, while eight studies reported data for 2 outcomes52,59,65,67,68,70,87,89. We report estimates based on analyses including more than 3 studies. The remaining outcomes were narratively described as per the SWiM guideline51.
Knowledge acquisition
The test results examined the effect of VBL on the ‘Knowledge Acquisition’ outcome in several areas: dentistry, medicine, nursing, psychology, and a combination of medicine and nursing (Table 10). Overall, VBL appeared to be effective in dentistry and medicine, but further research is needed for nursing, psychology and the combined domain of medicine/nursing. Due to the small sample sizes in dentistry (n = 3) and nursing (n = 3), cautious interpretation is warranted, highlighting the need for further research to determine the true effectiveness of video-based learning in these fields.
Egger’s test was performed to assess potential publication bias concerning ‘Knowledge Acquisition’ outcome. The ‘Overall RoB’ results of Egger’s test showed a statistically significant asymmetry in the funnel plot (Egger’s test estimate = -18.57, SE = 4.91, p = 0.0014). This indicates strong evidence of publication bias, suggesting that smaller studies with more significant results may be over-represented in the meta-analysis. When analysing the studies classified as having “Some concerns” RoB, the results of the Egger’s test showed a non-significant association between effect size and its standard error (Egger’s test estimate = -6.46, SE = 5.21, p = 0.2233). The non-significant p-value suggests that there is no strong evidence of publication bias in the meta-analysis. When the studies in the ‘Medicine’ area were analysed for publication bias, the results of the Egger’s test showed a statistically significant association between the effect size and its standard error (Egger’s test estimate = 1.23, SE = 0.34, p = 0.0011), indicating strong evidence of publication bias.
Skills development
The test results examined the effect of VBL on the ‘Skills Development’ outcome in several areas: dentistry, medicine, nursing, psychology, and a combination of medicine and nursing (Table 11).
VBL had a moderately high effect on ‘Skills Development’ in medicine with a Cohen’s d of 0.76, close to the 0.8 threshold. The 95% CI indicated that the true effect size is likely to fall between 0.15 and 1.34 with 95% confidence. There was a moderate level of heterogeneity (τ2 = 0.35) among the studies in medicine, suggesting some variability in the effect of VBL on ‘Skills Development’ across the included studies. In nursing, VBL also had a moderate effect on ‘Skills Development’, with a Cohen’s d of 0.59. Notably, there was no heterogeneity (τ2 = 0) among the studies in nursing, indicating consistent results across the included studies.
The findings suggest that VBL has a positive impact on ‘Skills Development’ in both medicine and nursing, with moderate effect sizes observed in both areas. However, it is important to interpret the results with caution, especially in dentistry where only one study was included in this systematic review. In medicine, the moderate heterogeneity indicates some variation in the effect across the studies, and in nursing, the absence of heterogeneity suggests more consistent findings. Further research is warranted to explore the factors contributing to heterogeneity and to identify effective video-based learning approaches tailored to each healthcare discipline. Due to the small sample sizes in dentistry and nursing, cautious interpretation is warranted, highlighting the need for further research to determine the true effectiveness of video-based learning in these fields.
Egger’s test was performed to assess potential publication bias concerning ‘Skills Development’ outcome. The ‘Overall RoB’ results of Egger’s test showed no significant evidence of publication bias in the analysis of the effect of video-based learning on ‘Skills Development’ across the areas of dentistry, medicine, nursing, psychology, and the combination of medicine and nursing (Egger’s test estimate = 0.44, SE = 0.31, p = 0.1799). When analysing the studies classified as having “Some concerns” RoB, the results of the Egger’s test showed a non-significant association between effect size and its standard error (Egger’s test estimate = 1.73, SE = 0.97, p = 0.1025). When the studies in the ‘Medicine’ area were analysed for publication bias, the results of the Egger’s test showed no significant evidence of publication bias (Egger’s test estimate = 2.08, SE = 1.74, p = 0.2628).
Attitude
The test results examined the effect of VBL on the ‘Attitude’ outcome in several areas: dentistry, medicine, nursing, psychology, and a combination of medicine and nursing (Table 12). Video-based learning had an overall positive effect, with a moderate effect size (Cohen’s d = 0.74), high heterogeneity (τ2 = 0.57, I2 = 97.0%) and a narrow confidence interval [0.20, 1.27]. Specifically, in dentistry and medicine the effect considered null due to its confidence interval of [-0.34, 0.94] and [-0.10, 0.82], respectively, despite observing a a small effect size in dentistry (Cohen’s d = 0.30) and medicine (Cohen’s d = 0.35). No heterogeneity was found across the studies in dentistry (τ2 = 0, I2 = 0.0%), suggesting consistent results among the included studies, while there was moderate heterogeneity across the studies in medicine, (τ2 = 0.22, I2 = 78.2%), suggesting some variation in the effect of VBL on ‘Attitude’ among the included studies. The results imply that VBL can positively influence “Attitude” in health education, without being specifically attributable to a particular area. While dentistry showed consistent results, medicine exhibited some variability across the studies. Further research and larger sample sizes may help provide a more comprehensive understanding of the effect of video-based learning on ‘Skills Development’ in these areas.
Given the low number of studies reporting ‘Attitude’, the Egger’s test was not performed to assess potential publication bias.
Additional analysis
We conducted a series of moderation analyses to explore possible sources of heterogeneity (Table 13).
For all three outcomes (‘Knowledge Acquisition’, ‘Skills Development’, and ‘Attitude’), none of the independent variables (‘Total number of participants’, ‘Time Span of Intervention’, ‘Latitude’ and ‘Longitude’) showed statistically significant associations (i.e., p-values less than 0.05). This means that the included independent variables did not significantly explain the heterogeneity observed in the outcomes of the studies.
For ‘Knowledge Acquisition’, the meta regression analysis on the total number of participants (n) yielded a nonsignificant effect (p = 0.267), indicating that the sample size did not significantly influence the observed effect size for this outcome. This suggests that the impact of VBL on ‘Knowledge Acquisition’ remains consistent across studies of varying sample sizes. The duration of the VBL intervention (Time of Intervention) also showed a nonsignificant effect (p = 0.879), suggesting that the duration of the intervention did not significantly affect this outcome. Geographical factors, such as latitude and longitude, also showed no significant impact on ‘Knowledge Acquisition’ (p = 0.208 and p = 0.284, respectively).
Similarly, in the analysis of ‘Skills Development’, the meta-regression results mirrored those for ‘Knowledge Acquisition’, with nonsignificant effects observed for n (p = 0.198), t (p = 0.968), Latitude (p = 0.897), and Longitude (p = 0.504). This implies that these factors did not significantly contribute to the variation in the effect sizes related to skills development through VBL.
In the case of ‘Attitude’ outcomes, a similar pattern emerged. The meta-regression analysis showed nonsignificant effects for n (p = 0.926), t (p = 0.426), Latitude (p = 0.740), and Longitude (p = 0.844). These findings suggest that the factors examined in the meta-regression analyses had no substantial impact on the effect sizes associated with ‘Attitude’ changes through VBL.
In summary, our meta-regression analyses indicated that the observed effects of VBL on ‘Knowledge Acquisition’, ‘Skills Development’, and ‘Attitude’ in health education were not significantly influenced by independent variables such as sample size, the length of the intervention, or geographical location. These results suggest that the effectiveness of VBL in health education is a robust educational approach that transcends these potential sources of variation.
Discussion
Summary of main results
The findings of the meta-analysis indicate that VBL has a significant positive effect on ‘Knowledge Acquisition’ in dentistry, with a large effect size and low heterogeneity. Similarly, in medicine, VBL showed a moderate effect on ‘Knowledge Acquisition’, with a relatively narrow confidence interval. However, for nursing, the effect was considered null.
This result aligns with the Cognitive Theory of Multimedia Learning13, as dental education videos likely utilize visuals, such as 3D models or clinical demonstrations, accompanied by audio explanations or narrations. By engaging both the visual and auditory channels, these multimedia elements may promote deeper understanding and retention of dental concepts, procedures, and techniques. Moreover, the low heterogeneity observed in this domain suggests a consistency in the effectiveness of VBL, reinforcing the potential impact of multimedia integration. Similarly, in the field of medicine, VBL demonstrated a moderate positive effect on ‘Knowledge Acquisition’. While the effect size was not as large as in dentistry, the Cognitive Theory of Multimedia Learning still provides an explanation for this finding13. Medical education videos often combine textual information with dynamic visualizations, surgical simulations, or case presentations, accompanied by spoken explanations. This multimedia approach likely facilitates cognitive processing and assists learners in grasping complex medical concepts and procedures, contributing to improved knowledge acquisition. The null results in nursing and inconclusive results in psychology and the combined domain of medicine/nursing might be attributed to a multitude of factors, including variations in multimedia presentation styles, content complexity, and instructional strategies. The Cognitive Theory of Multimedia Learning emphasizes the importance of well-designed multimedia presentations that consider the coherence principle, the modality principle, and other relevant principles to optimize learning outcomes13. Inconsistent results in these fields might indicate a need for more tailored and targeted approaches in incorporating multimedia elements into video-based education.
The moderate effect sizes observed in ‘Skills Development’ for medicine and nursing suggest that VBL has a positive impact on this outcome in both areas. However, cautious interpretation is warranted due to the limited number of studies available for dentistry and nursing. The presence of heterogeneity in the effect of VBL on ‘Skills Development’ in medicine warrants further investigation into potential contributing factors.
These findings are consistent with the principles of the Experiential Learning Theory14. By providing learners with concrete experiences (via video demonstrations), encouraging reflection, and promoting active experimentation, VBL can effectively support skills development in the healthcare domain. Furthermore, the cautious interpretation due to the limited number of studies available for dentistry and nursing indicates the need for more research to explore the effectiveness of video-based learning in these specific health education areas. The Experiential Learning Theory emphasizes the importance of contextualized experiences, and therefore, conducting more studies on VBL’s impact on ‘Skills Development’ in dentistry and nursing would help validate its effectiveness in these contexts. The Experiential Learning Theory offers valuable insights into skills development in health education through VBL14. By following the experiential learning cycle, learners can actively engage with video-based content, reflect on their observations, form abstract concepts, and experiment with applying the acquired skills, ultimately leading to improved skills development in medicine and nursing.
Regarding ‘Attitude’, the results show that VBL had an overall positive effect, without being specifically attributable to a particular area (i.e. dentistry and medicine), with null effect observed in both areas. This finding is consistent with the idea that attitude change can be a gradual process and may require repeated exposure to instructional materials, including video-based content. VBL can be a powerful tool to deliver educational content in a visually engaging and memorable way, leading to a positive shift in learners’ attitudes over time, aligned with Attitude Change Theories17,18, and Health Behavior Theories92,93. However, the limited number of studies reporting attitude outcomes points to the need for additional research to establish more robust conclusions. A broader and more comprehensive body of research is essential to understanding the precise role of video-based learning in influencing attitudes effectively in dentistry and medicine.
Despite the positive findings in dentistry, medicine, and nursing, the review highlighted potential limitations in the included studies, primarily related to the risk of bias. The shortcomings, particularly in randomization processes and deviations from intended interventions, could impact the internal validity of the results. Therefore, future research in video-based learning should aim to address these limitations and adopt rigorous study designs to provide more robust evidence on the role of multimedia learning in different academic disciplines.
Evidence quality and potential bias in the review process
Thirty studies were considered to have a moderate risk of bias38,52,53,54,55,57,59,61,62,63,64,65,67,69,70,71,72,74,76,78,79,80,81,83,84,85,86,87,88,90, 5 studies were considered to have a low risk of bias (Bahar et al., 2017; Fernandez et al., 2016; Hadvani et al., 2021; Peine et al., 2016; Schlafer et al., 2021, while 5 studies58,60,73,75,89 were considered to have a high risk of bias (Figure S3). While some studies showed strong methodological rigour with a low risk of bias, a significant number of studies had a moderate or high risk of bias, which highlights potential limitations in their designs. Researchers and readers should consider these limitations when interpreting the results and drawing conclusions from the studies included in this systematic review.
A major concern is the presence of publication bias, particularly in the ‘Overall RoB’ meta-analysis, which suggests that smaller studies with more significant results may be over-represented, potentially leading to an overestimation of the effect of video-based learning. It highlights the need for caution in interpreting overall results and the importance of conducting studies with more robust methodologies to avoid bias.
Egger’s test was performed to assess potential publication bias concerning ‘Skills Development’ outcome, however no significant association between effect size and its standard error was found. Given the low number of studies reporting ‘Attitude’, the Egger’s test was not performed to assess potential publication bias.
Limitations
Limitations of this systematic review with meta-analysis include the lack of meta-regression, which hinders a deeper exploration of sources of heterogeneity and variation in effect sizes between studies. In addition, inadequate reporting of participant characteristics, such as demographics and previous experience with VBL, may limit the generalisability of the results to specific subgroups. Inadequate information about participants’ exposure to VBL could affect understanding of the relationship between exposure and its effect on knowledge acquisition.
In addition, the heterogeneity of intervention methods, including different video formats, lengths and delivery styles, may make it difficult to draw specific conclusions about the most effective approaches. Variation in outcome assessment tools or methods used to measure knowledge acquisition may also affect the comparability of study results. This heterogeneity in the intervention makes it challenging to group studies and perform subgroup analyses based on the nature of VBL.
Publication bias is also a concern and may bias the overall effect size estimate and interpretation of results, as studies with positive or statistically significant results are more likely to be published.
Due to these constraints, conducting analyses on participant characteristics and the nature of Video-Based Learning was unattainable. Recognizing the significance of these factors in evaluating VBL effectiveness, awareness of these limitations is vital for interpreting review results and guiding future research and educational practices involving video-based learning in these populations.
Conclusion
This systematic review and meta-analysis shed light on the potential benefits of multimedia learning in health education settings. In conclusion, the findings demonstrate that video-based learning has a significant positive effect on knowledge acquisition in dentistry and medicine. The Cognitive Theory of Multimedia Learning provides valuable insights into understanding the impact of video-based education in these domains, emphasizing the importance of incorporating well-designed multimedia elements to enhance learning outcomes13. Additionally, the Experiential Learning Theory further support the effectiveness of video-based learning in promoting skills development in medicine and nursing, while cautious interpretation is necessary due to the limited number of studies available for dentistry and nursing14. In terms of attitude change, video-based learning shows promise in health education, aligned with relevant Attitude Change Theories17,18 and Health Behavior Theories92,93. However, the limited number of studies reporting attitude outcomes necessitates further research to establish more robust conclusions regarding the influence of video-based learning on attitudes in these fields.
While the findings are encouraging, potential limitations in the included studies are identified, particularly related to the risk of bias. To strengthen the evidence base, future research should address these limitations and employ rigorous study designs when investigating the role of multimedia learning in various academic disciplines.
In summary, video-based learning offers a valuable educational tool for knowledge acquisition, skills development, and attitude change in health education. The integration of multimedia elements, adherence to principles such as those based in the Experiential Learning Theory, and more rigorous research designs will contribute to maximizing the potential benefits of video-based education in dentistry, medicine, nursing, and other academic fields.
Data availability
The data that support the findings of this study are available from the corresponding author, MM, upon reasonable request.
References
Brame, C. J. Effective educational videos: principles and guidelines for maximizing student learning from video content. CBE—Life Sci. Educ. 15, es6 (2016).
Liu, Q., Geertshuis, S., Gladman, T. & Grainger, R. Student video production within health professions education: a scoping review. Med. Educ. Online. 27, 2040349 (2022).
Sablić, M., Mirosavljević, A. & Škugor, A. Video-based learning (VBL)—Past, Present and Future: an overview of the Research published from 2008 to 2019. Technol. Knowl. Learn. 26, 1061–1077 (2021).
Abdulrahaman, M. D. et al. Multimedia tools in the teaching and learning processes: a systematic review. Heliyon. 6, e05312 (2020).
Schmid, R. F. et al. The effects of technology use in postsecondary education: a meta-analysis of classroom applications. Comput. Educ. 72, 271–291 (2014).
Söderlund, A. et al. Exploring the activities and outcomes of digital teaching and learning of practical skills in higher education for the social and health care professions: a scoping review. Discov Educ. 2, 2 (2023).
Stockwell, B. R., Stockwell, M. S., Cennamo, M. & Jiang, E. Blended Learn. Improves Sci. Educ. Cell. 162, 933–936 (2015).
DeLozier, S. J. & Rhodes, M. G. Flipped classrooms: a review of Key ideas and recommendations for Practice. Educ. Psychol. Rev. 29, 141–151 (2017).
Nugraha, A., Wahono, I. A., Zhanghe, J., Harada, T. & Inoue, T. Creating dialogue between a tutee agent and a tutor in a lecture video improves students’ attention. in Collaboration Technologies and Social Computing: 26th International Conference, CollabTech Tartu, Estonia, September 8–11, 2020, Proceedings 26 96–111, (2020).
Zipp, G. P. Z. & Maher, C. Use of video-based cases as a medium to develop critical thinking skills in health science students. J. Coll. Teach. Learn. TLC. 7, (2010).
Guseva, Y. & Kauppinen, T. Learning in the Era of online videos: How to Improve teachers’ competencies of producing educational videos. in Proceedings of the 4th International Conference on Higher Education Advances (HEAd’18) (Universitat Politècnica València, doi: (2018). https://doi.org/10.4995/HEAD18.2018.8096
Lewis, N., Lewis, R. & Luca, C. Impact of video-based learning in business statistics: a longitudinal study. Humanit. Soc. Sci. Commun. 10, 1–10 (2023).
Mayer, R. The future of multimedia learning. J. Appl. Instr Des.https://doi.org/10.59668/423.10349 (2022).
Kolb, D. A. Experiential Learning: Experience as the source of learning and development (Prentice-Hall, 1984).
Haleem, A., Javaid, M., Qadri, M. A. & Suman, R. Understanding the role of digital technologies in education: a review. Sustain. Oper. Comput. 3, 275–285 (2022).
Hochbaum, G. M., Sorenson, J. R. & Lorig, K. Theory in health education practice. Health Educ. Q. 19, 295–313 (1992).
Petty, R. E. & Cacioppo, J. T. The Elaboration likelihood model of persuasion. in Advances in Experimental Social Psychology (ed Berkowitz, L.) vol 19 123–205 (Academic, (1986).
Bandura, A. & Y 1SP United Kingdom. Social Cognitive Theory. in Handbook of Theories of Social Psychology: Volume 1 349–374 (SAGE Publications Ltd, 1 Oliver’s Yard, 55 City Road, London EC1, doi: (2012). https://doi.org/10.4135/9781446249215.n18
Adam, M., McMahon, S. A., Prober, C. & Bärnighausen, T. Human-centered design of video-based health education: an iterative, collaborative, community-based Approach. J. Med. Internet Res. 21, e12128 (2019).
Guze, P. A. Using technology to meet the challenges of medical education. Trans. Am. Clin. Climatol Assoc. 126, 260–270 (2015).
Lehane, E. et al. Evidence-based practice education for healthcare professions: an expert view. BMJ Evid. -Based Med. 24, 103–108 (2019).
Higgins, J. P. T. & Cochrane Collaboration. Cochrane Handbook for Systematic Reviews of Interventions (Wiley-Blackwell, 2019).
Page, M. J. et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ n71 doi: (2021). https://doi.org/10.1136/bmj.n71
Hartling, L., Spooner, C., Tjosvold, L. & Oswald, A. Problem-based learning in pre-clinical medical education: 22 years of outcome research. Med. Teach. 32https://doi.org/10.3109/01421590903200789 (2010).
Harn, B. & Meline, M. Developing critical thinking and reflection in teachers within teacher preparation: in Advances in Higher Education and Professional Development (eds. Mariano, G. J. & Figliano, F. J.) 126–145IGI Global, doi: (2019). https://doi.org/10.4018/978-1-5225-7823-9.ch007
Sharpnack, P. A., Goliat, L., Baker, J. R., Rogers, K. & Shockey, P. Thinking like a nurse: using Video Simulation to rehearse for Professional Practice. Clin. Simul. Nurs. 9, e571–e577 (2013).
Global Encyclopedia of Information Science and Technology, Fourth Edition: (IGI doi: (2018). https://doi.org/10.4018/978-1-5225-2255-3
Huang, W. Cultivating Teaching Presence and Social Presence Through Multimedia Intervention. in Early Warning Systems and Targeted Interventions for Student Success in Online Courses: (eds. Glick, D., Cohen, A. & Chang, C.)IGI Global, doi: (2020). https://doi.org/10.4018/978-1-7998-5074-8
Pilote, B. & Chiniara, G. The Many faces of simulation. in Clinical Simulation (Second Edition) (ed. Chiniara, G.) 17–32Academic Press, doi: (2019). https://doi.org/10.1016/B978-0-12-815657-5.00002-4
Global Handbook of Research on Virtual Training and Mentoring of Online Instructors. (IGI doi: (2019). https://doi.org/10.4018/978-1-5225-6322-8
Koukourikos, K. et al. Simulation in clinical nursing education. Acta Inf. Med. 29, 15–20 (2021).
Shute, V. J. Focus on formative feedback. Rev. Educ. Res. 78, 153–189 (2008).
Wong, C. & Purdy, L. Teaching professionalism: comparing written and video case-studies. J. Med. Educ. Curric. Dev. 8, 23821205211020740 (2021).
Reo, J. A. & Mercer, V. S. Effects of Live, videotaped, or written instruction on learning an upper-extremity exercise program. Phys. Ther. 84, 622–633 (2004).
World Health Organization. WHO Global Model Regulatory Framework for Medical Devices Including in Vitro Diagnostic Medical Devices (World Health Organization, 2017).
Brulé, J. F. & Blount, A. Knowledge Acquisition (McGraw-Hill, 1989).
Boose, J. H. A survey of knowledge acquisition techniques and tools. Knowl. Acquis 1, 3–37 (1989).
Cosford, K., Briere, J., Ambros, B., Beazley, S. & Cartwright, C. Effect of instructional format on veterinary students’ task performance and emotional state during a simulation-based canine endotracheal Intubation laboratory: handout versus video. J. Vet. Med. Educ. 47, 239–247 (2020).
Sinha, K. & PriyaDarshani, M. Impact of Information and communication technology in the Indian education system during COVID-19: in Advances in Library and Information Science (ed. Holland, B.) 358–375IGI Global, doi: (2021). https://doi.org/10.4018/978-1-7998-6449-3.ch019
Hurst, D. C., Clapperton, R., Dixon, R. J. & Morpurgo, M. T. Why a Virtual Co-Op? A case study on an artificially-Intelligent work integration simulation. in Dev.Virtual Learn. Environ. Global Workplace 289–309IGI Global, doi: (2021). https://doi.org/10.4018/978-1-7998-7331-0.ch015
Becerra-Fernandez, I. & Sabherwal, R. Knowledge Management: Systems and Processes (Routledge, 2014).
UNESCO International Bureau of Education. General Education System Quality Analysis/Diagnosis Framework (GEQAF). (2015).
Norris, J. et al. The development and validation of the interprofessional attitudes scale: assessing the interprofessional attitudes of students in the health professions. Acad. Med. 90, 1394 (2015).
Spielberger, D. Manual for the state-trait Anxietry, Inventory. Consult Psychol. (1970).
Global Handbook of Research on Enhancing Teacher Education with Advanced Instructional Technologies: (IGI doi: (2015). https://doi.org/10.4018/978-1-4666-8162-0
Buchwald, P. & Schwarzer, C. Impact of assessment on students’ test anxiety. in International Encyclopedia of Education (Third Edition) (eds. Peterson, P., Baker, E. & McGaw, B.) 498–505Elsevier, Oxford, doi: (2010). https://doi.org/10.1016/B978-0-08-044894-7.00304-3
APA Dictionary of Psychology. xvi, 1024 American Psychological Association, Washington, DC, US, (2007).
Sterne, J. A. C. et al. RoB 2: a revised tool for assessing risk of bias in randomised trials. BMJ. l4898https://doi.org/10.1136/bmj.l4898 (2019).
Schwarzer, G., Carpenter, J. R. & Rücker, G. Meta-Analysis with R (Springer International Publishing, 2015). https://doi.org/10.1007/978-3-319-21416-0
Schwarzer, G. meta: an R package for meta-analysis. R News. 7, 40–45 (2007).
Campbell, M. et al. Synthesis without meta-analysis (SWiM) in systematic reviews: reporting guideline. BMJ. l6890https://doi.org/10.1136/bmj.l6890 (2020).
Aghababaeian, H. et al. Triage live lecture versus triage video podcast in pre-hospital students’ education. Afr. J. Emerg. Med. 9, 81–86 (2019).
Alharbi, H. A., Shehadeh, F. & Awaji, N. Y. Immediate knowledge retention among nursing students in live lecture and video-recorded lecture: a quasi-experimental study. Nurse Educ. Pract. 60, 103307 (2022).
Alnabelsi, T., Al-Hussaini, A. & Owens, D. Comparison of traditional face-to-face teaching with synchronous e-learning in otolaryngology emergencies teaching to medical undergraduates: a randomised controlled trial. Eur. Arch. Otorhinolaryngol. 272, 759–763 (2015).
Assadi, T. et al. The comparison between two methods of Basic Life Support instruction: video self-instruction versus traditional method. Hong Kong J. Emerg. Med. 22, 291–296 (2015).
Bahar, A., Arslan, M. & Gokgoz, N. Do Parenteral Medication Administration Skills of Nursing Students Increase with Educational Videos Materials? in (2017).
Bingener, J. et al. Randomized double-blinded trial investigating the impact of a curriculum focused on error recognition on laparoscopic suturing training. Am. J. Surg. 195, 179–182 (2008).
Casado, M. I., Castaño, G. & Arráez-Aybar, L. A. Audiovisual material as educational innovation strategy to reduce anxiety response in students of human anatomy. Adv. Health Sci. Educ. 17, 431–440 (2012).
Clark, N. P., Marks, J. G., Sandow, P. R., Seleski, C. E. & Logan, H. L. Comparative effectiveness of instructional methods: oral and pharyngeal Cancer examination. J. Dent. Educ. 78, 622–629 (2014).
Danley, D., Gansky, S. A., Chow, D. & Gerbert, B. Preparing dental students to recognize and respond to domestic violence. J. Am. Dent. Assoc. 135, 67–73 (2004).
Davis, J., Crabb, S., Rogers, E., Zamora, J. & Khan, K. Computer-based teaching is as good as face to face lecture-based teaching of evidence based medicine: a randomized controlled trial. Med. Teach. 30, 302–307 (2008).
De Lopes, L. Efficacy of a video during bed bath simulation on improving the performance of psychomotor skills of nursing undergraduates: a randomized clinical trial. Int. J. Nurs. Stud. 99, 103333 (2019).
De Souza Teixeira, C. R. et al. Anxiety and performance of nursing students in regard to assessment via clinical simulations in the classroom versus filmed assessments. Investig Educ. En Enferm 32, 270–279 (2014).
Delasobera, B. E. et al. Evaluating the efficacy of simulators and multimedia for refreshing ACLS skills in India. Resuscitation. 81, 217–223 (2010).
Dwyer, C. P. et al. Effects of biopsychosocial education on the clinical judgments of medical students and GP trainees regarding future risk of disability in chronic lower back pain: a randomized control trial. Pain Med. 21, 939–950 (2020).
Fernandez, A., Tan, K. A., Knaak, S., Chew, B. H. & Ghazali, S. S. Effects of brief Psychoeducational program on stigma in Malaysian pre-clinical medical students: a randomized controlled trial. Acad. Psychiatry 40, 905–911 (2016).
Flores, R. L., DeMoss, P., Klene, C., Havlik, R. J. & Tholpady, S. Digital animation versus textbook in teaching plastic surgery techniques to novice learners. Plast. Reconstr. Surg. 132, 101e–109e (2013).
Hadvani, T. et al. Effectiveness of modalities to teach evidence based Medicine to Pediatric Clerkship students: a randomized controlled trial. Acad. Pediatr. 21, 375–383 (2021).
Hansen, M. et al. Enhancement of medical interns’ levels of clinical skills competence and self-confidence levels via Video iPods: Pilot Randomized Controlled Trial. J. Med. Internet Res. 13, e29 (2011).
Herbstreit, F., Fassbender, P., Haberl, H., Kehren, C. & Peters, J. Learning endotracheal intubation using a Novel Videolaryngoscope improves intubation skills of medical students. Anesth. Analg. 113, 586–590 (2011).
Kam, J. et al. Portable video media versus standard verbal communication in surgical teaching: a prospective, multicenter, and randomized controlled crossover trial. J. Surg. Educ. 76, 440–445 (2019).
Khatib, M. et al. Validation of open inguinal hernia repair simulation model: a randomized controlled educational trial. Am. J. Surg. 208, 295–301 (2014).
Leinonen, J. et al. Live lectures and videos do not differ in relation to learning outcomes of dental ergonomics. Clin. Exp. Dent. Res. 6, 489–494 (2020).
Leszczyński, P. et al. Analysis of web-based learning methods in emergency medicine: randomized controlled trial. Arch. Med. Sci. 14, 687–694 (2018).
Lwin, A. T. et al. Self-Directed interactive video-based instruction Versus instructor-led teaching for Myanmar house surgeons: a randomized, noninferiority trial. J. Surg. Educ. 75, 238–246 (2018).
Peahl, A. F., Tarr, E. E., Has, P. & Hampton, B. S. Impact of 4 components of instructional design video on medical student medical decision making during the Inpatient rounding experience. J. Surg. Educ. 76, 1286–1292 (2019).
Peine, A., Kabino, K. & Spreckelsen, C. Self-directed learning can outperform direct instruction in the course of a modern German medical curriculum - results of a mixed methods trial. BMC Med. Educ. 16, 158 (2016).
Pelloux, S. et al. Peripheral venous catheter insertion simulation training: a randomized controlled trial comparing performance after instructor-led teaching versus peer-assisted learning. Anaesth. Crit. Care Pain Med. 36, 397–402 (2017).
Phillips, A. W. et al. Individualised expert feedback is not essential for improving basic clinical skills performance in novice learners: a randomized trial. J. Surg. Educ. 74, 612–620 (2017).
Rad, R. F. et al. Comparative study of virtual and face-to-face training methods on the quality of healthcare services provided by Kermanshah pre-hospital emergency staff (EMS): randomized educational intervention trial. BMC Med. Educ. 22, 203 (2022).
Rosenberg, B. H., Landsittel, D. & Averch, T. D. Can Video games be used to predict or improve laparoscopic skills? J. Endourol. 19, 372–376 (2005).
Schlafer, S., Pedersen, K., Jørgensen, J. N. & Kruse, C. Hands-on live demonstration vs. video‐supported demonstration of an aesthetic composite restoration in undergraduate dental teaching. J. Dent. Educ. 85, 802–811 (2021).
Schlickum, M. K., Hedman, L., Enochsson, L. & Kjellin, A. Felländer-Tsai, L. systematic video game training in surgical novices improves performance in virtual reality endoscopic surgical simulators: a prospective randomized study. World J. Surg. 33, 2360–2367 (2009).
Shippey, S. H. et al. Teaching subcuticular suturing to medical students: Video versus expert instructor feedback. J. Surg. Educ. 68, 397–402 (2011).
Sugathapala, R. D. U. P. & Chandrika, M. G. R. Student nurses’ knowledge acquisition on oral medication administration: comparison of lecture demonstration vs. video demonstration. BMC Nurs. 20, 9 (2021).
Sullivan, K. & O’Conor, F. Providing education about Alzheimer’s disease. Aging Ment Health. 5, 5–13 (2001).
Tan, A. J. Q. et al. Designing and evaluating the effectiveness of a serious game for safe administration of blood transfusion: a randomized controlled trial. Nurse Educ. Today. 55, 38–44 (2017).
Weidenbusch, M. et al. Can clinical case discussions foster clinical reasoning skills in undergraduate medical education? A randomised controlled trial. BMJ Open. 9, e025973 (2019).
Yoo, M. S., Park, J. H. & Lee, S. R. The effects of case-based learning using video on clinical decision making and learning motivation in undergraduate nursing students. J. Korean Acad. Nurs. 40, 863 (2010).
Zhao, X. & Cong, L. Effect of problem and scripting-based learning combining wearable technology on orthopedic operating room nurses’ learning outcomes. Nurse Educ. Today. 73, 13–16 (2019).
Higgins, J. Incorporating ‘risk of bias’ assessments into meta-analyses. Assess. Risk Bias Cochrane Rev. Loughb. (2012).
Ajzen, I. The theory of planned behavior. Organ. Behav. Hum. Decis. Process. 50, 179–211 (1991).
Rosenstock, I. M. health belief model. in Encyclopedia of psychology, Vol. 4. 78–80 (American Psychological Association, Washington, DC, US, doi:https://doi.org/10.1037/10519-035. (2000).
McGuinness, L. A. & Higgins, J. P. T. Risk-of-bias VISualization (robvis): An R package and shiny web app for visualizing risk-of-bias assessments. Res. Synth. Methods n/a, (2020).
Author information
Authors and Affiliations
Contributions
M.M., contributed to data acquisition, and interpretation, drafted and critically revised the manuscript; J.B., contributed to conception, design, data acquisition, and analysis, drafted and critically revised the manuscript; V.M., contributed to conception and design, critically revised the manuscript; J.M., critically revised the manuscript.; O.A. critically revised and validated the manuscript; L.P., contributed to data analysis and interpretation, critically revised the manuscript. All authors gave final approval and agree to be accountable for all aspects of the work.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Morgado, M., Botelho, J., Machado, V. et al. Video-based approaches in health education: a systematic review and meta-analysis. Sci Rep 14, 23651 (2024). https://doi.org/10.1038/s41598-024-73671-7
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-024-73671-7
