
Abstract
Serum presepsin levels are elevated during sepsis and are widely employed in clinical practice. However, the association between urinary presepsin and kidney diseases remains elusive. Given that monocytes/macrophages, primary presepsin producers, are closely associated with the pathophysiology of nephritis, we explored the potential of urinary presepsin as a kidney disease biomarker. In a cross-sectional study involving patients who underwent kidney biopsy (n = 463 patients; 43% female, median age 58 years), the median urinary presepsin/creatinine levels were 590 (interquartile range [IQR], 244–1276), 1023 (IQR, 491–2749), 1429 (IQR, 644–2725), and 3518 (IQR, 2084–6321) ng/g creatinine, indicating minimal (< 5%), mild (5–25%), moderate (26–50%), and severe (> 50%) interstitial inflammatory cell infiltration in biopsy samples, respectively. The area under the curve of urinary presepsin/creatinine (0.81) had a higher accuracy for distinguishing severe interstitial inflammatory cell infiltration than that of the N-acetyl-β-D-glucosaminidase/creatinine (0.70) (P = 0.003). The tubulointerstitial nephritis group had the highest urinary presepsin/creatinine level. Immunofluorescence staining revealed that monocytes and macrophages predominantly expressed presepsin in the kidney interstitium, with the stained area positively and significantly correlated with presepsin/creatinine values (r = 0.57, P = 0.02). Urinary presepsin could be a biomarker for directly assessing monocyte/macrophage infiltration in kidney disease.
Similar content being viewed by others
Introduction
Convenient tests are necessary for diagnosing and managing kidney diseases. Despite the availability of numerous kidney biomarkers1,2,3, nephrologists frequently encounter considerable challenges in diagnosing and understanding the condition owing to the diverse nature of kidney diseases4, highlighting the need for improved diagnostic approaches. Further, according to a systematic review and meta-analysis, percutaneous kidney biopsy (PKB) is mainly associated with bleeding-related complications5. A previous observational study of 2138 consecutive kidney biopsies revealed the timing of bleeding-related complications after PKB: 77.8% of major complications occurred within 6 h; 13% occurred between 6 and 12 h; 7.4% occurred between 12 and 24 h; and 1.9% occurred after 24 h6. Although PKB is occasionally performed as an outpatient procedure, it is preferable to extend the observation period or hospitalize the patient, given that the observation period typically lasts 6–8 h. Therefore, it is not feasible to repeatedly perform PKB easily. Additionally, PKB is unsuitable in cases warranting immediate diagnosis or treatment decisions, given the prolonged time required for pathological diagnostic results after specimen submission. Therefore, novel, highly accurate, minimally invasive, and immediately available biomarkers are urgently required as alternatives or complements to PKB assessment. For instance, urinary CD163 has been previously reported. It has been demonstrated to be associated with glomerular damage and cellular crescents7,8,9.
Accordingly, we focused on presepsin as a novel biomarker. Serum presepsin is mainly secreted from monocytes after phagocytosis, which leads to the cleavage of CD1410. Moreover, serum presepsin levels are specifically elevated during the early stages of and reflect the severity of the condition in patients with sepsis11,12,13,14,15; therefore, it is a valuable biomarker for sepsis. Regarding kidney disease, serum presepsin levels reportedly increase as kidney function declines in both acute kidney injury16,17,18and chronic kidney disease19,20,21. Although a small series of studies reported that urinary presepsin levels were found to be elevated in perinatal asphyxia22and pyelonephritis23, the association between urinary presepsin and kidney diseases remains elusive. Given that monocytes/macrophages play a role in nephritis24,25, we hypothesized that urinary presepsin could be established as a novel biomarker for kidney diseases. Generally, in the majority of kidney diseases, there is marked infiltration by cells of the monocyte/macrophage lineage. Presepsin serves as a marker of macrophage activation and is typically increased during sepsis. Therefore, our objective was to investigate whether urinary presepsin levels are elevated in different kidney diseases and how it correlates with monocyte infiltration, as well as glomerular/interstitial disease.
In the current study, we measured urinary presepsin levels in patients with kidney biopsy-confirmed kidney disease and analyzed the association between urinary presepsin levels and kidney disease. Furthermore, pathological kidney tissue specimens were subjected to immunofluorescence staining to elucidate the site and mechanism of presepsin production in the kidney.
Materials and methods
Study design and settings
This analytical cross-sectional study involved all patients registered in the Nagoya Kidney Disease Registry between March and December 2020 and provided informed consent. The patients underwent kidney biopsy at Nagoya University Hospital and 24 regional core hospitals spanning four prefectures in Japan. This study was approved by the Institutional Review Board of Nagoya University Hospital (approval number: 2010–1135 and 2021–0379), was conducted in accordance with the Declaration of Helsinki, and followed The Strengthening the Reporting of Observational Studies in Epidemiology reporting statement for prognostic studies.
Study samples and data collection
For patients undergoing a kidney biopsy, the attending physicians collected patient data, including demographic data, clinical history, medications, and laboratory results. Levels of 24-h urine protein and/or urinary protein-to-creatinine ratios were measured. In addition to kidney tissue sections, if possible, blood and urine samples were also obtained on the day of the kidney biopsy; samples were then frozen and stored for research purposes. We included cases in which urine samples could be collected on the day of kidney biopsy. Additionally, urine samples were collected from 10 healthy individuals without any evidence of kidney disease.
Presepsin assay
Frozen serum and urine samples were thawed to a liquid state at room temperature before presepsin detection. The presepsin concentration was measured using a compact automated immunoanalyzer, PATHFAST, based on a chemiluminescent enzyme immunoassay (PHC IVD, Japan)26,27. Measurements were performed according to the manufacturer’s manual, and the results were obtained in approximately 17 min. Considering presepsin levels, the upper limit of the reference range was 20,000 pg/mL; therefore, data exceeding 20,000 pg/mL were imputed as 20,000 pg/mL. Urinary presepsin levels were normalized to urinary creatinine levels and were evaluated using urinary presepsin/creatinine levels (ng/g creatinine).
N-acetyl-β-D-glucosaminidase (NAG) assay
The NAG concentration was measured using an enzymatic method with a commercial kit (N-assay L NAG Nittobo; Nittobo Medical, Japan). Considering NAG levels, the lower limit of the reference range was 0.5 U/L; therefore, data below 0.5 U/L were imputed as 0.5 U/L. Urinary NAG levels were normalized to urinary creatinine levels and evaluated using the NAG/creatinine ratio (U/g creatinine).
Preparation of kidney tissue sections
After transporting patient data and samples to Nagoya University Hospital, multiple (at least 3) nephrologists reviewed the data and pathological specimens to establish the diagnosis, degree of interstitial inflammatory cell infiltration, and other relevant factors. Semi-quantitative scores of interstitial inflammatory cell infiltration were assessed according to the proportion of the lesion area relative to the total section area as follows: minimal, < 5%; mild, 5–25%; moderate, 26–50%; and severe, > 50%.
Kidney tissue sections were immunohistochemically stained for presepsin, CD3, CD20, and CD163 to identify the kidney sites and cells where presepsin was produced. Immunofluorescence staining was performed for presepsin alone, with double staining for presepsin and CD3, CD20, or CD163. Briefly, 3-µm sections were fixed with acetone. Subsequently, sections were incubated with 10% blocking solution (Nacalai Tesque) for 30 min, followed by incubation with rabbit anti-presepsin polyclonal antibody (1:100; Mochida Pharmaceutical), mouse anti-CD3 monoclonal antibody (1:10; BioLegend), mouse anti-CD20 monoclonal antibody (1:10; LSBio), and mouse anti-CD163 monoclonal antibody (1:50; Bio-Rad) for 60 min. Next, the sections were incubated with secondary antibodies goat anti-rabbit IgG-Alexa Fluor Plus 488 (1:1000; Thermo Fisher Scientific) and goat anti-mouse IgG-Alexa Fluor Plus 555 (1:1000 for CD3 and CD20 and 1:500 for CD163; Thermo Fisher Scientific) for 30 min. Finally, the sections were stained with 4′,6-diamidino-2-phenylindole and sealed with the VECTASHIELD Antifade Mounting Medium (Vector Laboratories). Images were captured using a TiE-A1R confocal microscope (Nikon). Four specimens were randomly selected from each of the four categories of interstitial inflammatory cell infiltration severity (total of 16 cases), and high-power fields (× 400) of the cortex were captured. The stained area was measured in an automated fashion based on the selection of the fluorescein isothiocyanate component of presepsin, with a minimal threshold set at 2500. The results are expressed as μm2 using Imaris version × 60 7.6.4 (Image analysis software, Oxford Instruments, Japan). We captured at least four fields for each disease and measured the stained areas, presenting the results as averages. To evaluate the association between presepsin and CD163 localization, we assessed the proportion of CD163-positive cells among presepsin-positive cells and positive presepsin staining among CD163-positive cells. To secure presepsin-positive cells, we examined five fields in each of the six cases of tubulointerstitial nephritis (TIN) with severe interstitial inflammation cell infiltration with significantly elevated presepsin levels (total 30 fields).
Statistical analysis
Patient characteristics are presented as medians and interquartile range (IQR) for continuous variables, and as number and percentage (%) for categorical variables with the results of healthy individuals as a reference. Log-transformed urinary presepsin/creatinine level differences between diseases were analyzed using the Kruskal Wallis test.
To detect TIN, we conducted receiver operating characteristic (ROC) curve analyses using urinary biomarker levels among the patients who underwent PKB. In these analyses, the comparator group is diseases other than TIN among all samples. We determined the area under the curve (AUC), sensitivity, specificity, positive predictive value, and negative predictive value using the most discriminating thresholds. We compared NAG, presepsin without correction by urinary creatinine, and presepsin with correction by urinary creatinine as urinary biomarkers. The AUCs between the urinary biomarkers were analyzed using DeLong’s test. For the diagnosis of TIN, we calculated the sensitivity, specificity, positive predictive value, and negative predictive value based on various cutoff values of presepsin/creatinine.
Additionally, we evaluated the correlation between the level of urinary presepsin and the severity of interstitial inflammatory cell infiltration in biopsy samples. By categorizing the groups based on the degree of interstitial inflammatory cell infiltration (minimal, mild, moderate, and severe) in kidney biopsy samples, we compared the level of urinary presepsin in each group.
To predict the pathology findings, we conducted an ordinal logistic regression analysis using urinary presepsin as an explanatory variable. The response variable was the degree of interstitial inflammatory cell infiltration, scored as follows: 1, minimal; 2, mild; 3, moderate; and 4, severe. The explanatory variable was adjusted for age, sex, presence of hypertension, presence of diabetes, albumin, creatinine, C-reactive protein, hemoglobin, and urine protein.
To detect the severe category of interstitial inflammatory cell infiltration, we conducted ROC curve analyses using urinary biomarker levels among the patients who underwent PKB. In these analyses, the comparator group is categories other than target categories.
To determine the correlation between the fluorescent staining area of presepsin and the level of urinary presepsin/creatinine, Spearman’s rank correlation test was performed. From the four groups categorized based on the severity of inflammatory cell infiltration in kidney biopsy samples (minimal, mild, moderate, and severe), four cases were randomly chosen from each group (n = 16). The Imaris software was used to measure the fluorescent staining area.
Double staining was performed to confirm the presence of presepsin-producing cells. Since it is challenging to accurately count the cells when there are insufficient presepsin-positive cells, we selected cases from the TIN group with severe inflammatory cell infiltration (n = 6). The percentage of double-positive cells was calculated using either presepsin-positive cells or CD163-positive cells as the denominator. Visual counts were performed for these positive cells.
To assess the correlation between serum and urinary presepsin levels, we conducted a Spearman’s rank correlation test. Considering that kidney dysfunction can influence presepsin levels, we specifically chose patients from a group with IgA nephropathy (IgAN) who had less advanced kidney damage and a larger sample size (n = 106).
Data from healthy individuals were not subjected to statistical processing. Missing data were handled using pairwise deletion. Data analyses were performed using R version 4.3.1 (R Foundation for Statistical Computing). All statistical tests were two-sided, and P < 0.05 was considered statistically significant. Multiplicity adjustment was performed using the Bonferroni method.
Results
Characteristics of study participants
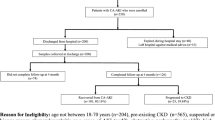
In total, we enrolled 463 participants who underwent kidney biopsy between March 2020 and December 2020 at 25 hospitals, provided informed consent, and had urine samples collected on the day of the kidney biopsy. Subsequently, we excluded 20 patients owing to insufficient urinary samples, measuring NAG levels in 443 patients. Figure 1 presents a flowchart of the study.

A flowchart of the study. AAV, antineutrophil cytoplasmic antibody -associated vasculitis; DMN, diabetic nephropathy; FSGS, focal segmental glomerulosclerosis; IgAN, IgA nephropathy; LN, lupus nephritis; MCNS, minimal change nephrotic syndrome; MN, membranous nephropathy; NSC, nephrosclerosis; TIN, tubulointerstitial nephritis.
Patient characteristics are shown for all patients, normal individuals, and nine representative diseases: antineutrophil cytoplasmic antibody-associated vasculitis, diabetic nephropathy, focal segmental glomerulosclerosis, IgAN, lupus nephritis, minimal change nephrotic syndrome, membranous nephropathy, nephrosclerosis, and TIN (Table 1). Overall, the median patient age was 58 years (IQR, 43–72 years), 43% were females, and IgAN was the most common disease (n = 106, 23%). The proportions of interstitial inflammatory cell infiltration in the minimal, mild, moderate, and severe groups were 37, 36, 16, and 11%, respectively. The TIN group had the highest urinary presepsin/creatinine levels, with a median of 5004 (IQR, 2059–8141) ng/g creatinine. The missing data included C-reactive protein (n = 7), white blood cells (n = 6), hemoglobin (n = 4), and urine protein (n = 6).
Association between urinary presepsin and types of disease
Figure 2 presents the log-transformed urinary presepsin/creatinine levels for each disease. The log-transformed urinary presepsin/creatinine levels were significantly higher in TIN than in focal segmental glomerulosclerosis, IgAN, minimal change nephrotic syndrome, and membranous nephropathy (P < 0.001 for all comparisons).

Violin plot showing the distribution of the log-transformed urinary presepsin/creatinine level in each disease. The red dots indicate that the measurement values have reached the upper limit of PATHFAST®. The P value was calculated using the Kruskal Wallis test. P value adjustment was calculated using the Bonferroni method. *P < 0.05, **P < 0.01, ***P < 0.001. AAV, antineutrophil cytoplasmic antibody -associated vasculitis; DMN, diabetic nephropathy; FSGS, focal segmental glomerulosclerosis; IgAN, IgA nephropathy; LN, lupus nephritis; MCNS, minimal change nephrotic syndrome; MN, membranous nephropathy; NSC, nephrosclerosis; TIN, tubulointerstitial nephritis.
We then assessed the ROC curve to detect TIN among all patients who underwent PKB and compared the biomarkers for the accuracy of TIN diagnosis. The AUCs of urinary presepsin/creatinine (0.83) and urinary presepsin (0.80) were higher than that of NAG/creatinine (0.61) (P < 0.001), whereas the AUCs for urinary presepsin/creatinine and urinary presepsin were not statistically significant (Fig. 3). The AUC, 95% confidence interval, cutoff values, sensitivity, specificity, positive predictive value, and negative predictive value are shown in Supplementary Table S1. The sensitivity, specificity, positive predictive value, and negative predictive value of the urinary presepsin/creatinine levels stratified the cutoff values to detect TIN among all patients who underwent PKB are recorded in Supplementary Table S2.

Receiver operating characteristic curves of urinary presepsin/creatinine, urinary presepsin, and NAG/creatinine levels for tubulointerstitial nephritis diagnosis. The P value was calculated using DeLong’s test. P value adjustment was calculated using the Bonferroni method. aP < 0.001, vs. NAG/creatinine. NAG, N-acetyl-β-D-glucosaminidase; AUC, area under the curve.
Association between urinary presepsin and interstitial inflammatory cell infiltration in kidney biopsy samples
We assessed the urinary presepsin levels based on the categories of interstitial inflammatory cell infiltration in all patients. The median urinary presepsin/creatinine levels were 590 (IQR, 244–1276), 1023 (IQR, 491–2749), 1429 (IQR, 644–2725), and 3518 (IQR, 2084–6321) ng/g creatinine for minimal, mild, moderate, and severe interstitial inflammatory cell infiltration, respectively (P < 0.001). As the severity of interstitial inflammatory cell infiltration increased, the urinary presepsin/creatinine levels increased; we presented the log-transformed urinary presepsin/creatinine levels for each interstitial inflammatory cell infiltration (Fig. 4a).

The association between urinary presepsin and interstitial inflammatory cell infiltration. (a) Violin plot showing the distribution of the log-transformed urinary presepsin/creatinine level in each interstitial inflammatory cell infiltration. The P value was calculated using the Kruskal Wallis test. P value adjustment was calculated using the Bonferroni method. ***P < 0.001. (b) Receiver operating characteristic curves of the urinary presepsin/creatinine and NAG/creatinine levels to distinguish the category of interstitial inflammatory cell infiltration. The P value was calculated using DeLong’s test. aP = 0.003, vs. NAG/creatinine in severe. CI, confidence interval; NAG, N-acetyl-β-D-glucosaminidase.
Subsequently, to predict the pathology findings, we conducted an ordinal logistic regression analysis using urinary presepsin as an explanatory variable, adjusted for age, sex, presence of hypertension, presence of diabetes, albumin, creatinine, C-reactive protein, hemoglobin, and urine protein. Even after accounting for various factors, urinary presepsin was found to be significantly associated with inflammatory cell infiltration into the interstitium of the pathology (P = 0.030). The results are shown in Table 2.
We then assessed and compared the accuracy of distinguishing between the categories of interstitial inflammatory cell infiltration busing ROC curves for the biomarkers. Among all patients, the AUC of the urinary presepsin/creatinine (0.81) was higher than that of the NAG/creatinine (0.70; P = 0.003) for detecting the severe category. The AUCs for urinary presepsin/creatinine and NAG/creatinine in the mild or higher and moderate or higher groups were not statistically significant (Fig. 4b). The AUC, 95% confidence interval, cutoff values, sensitivity, specificity, positive predictive value, and negative predictive value are presented in Supplementary Table S3.
Immunofluorescence staining for presepsin distribution in the kidney
We compared the intensity of presepsin positivity in 16 samples with varying degrees of interstitial inflammatory cell infiltration. Two representative examples are shown in fluorescent stained images. Notably, presepsin positivity was more intense within the interstitium in TIN, characterized by severe interstitial inflammatory cell infiltration, than in IgAN, which was associated with minimal interstitial inflammatory cell infiltration (Fig. 5a). In the immunofluorescence analysis, the presepsin-stained area showed a significant positive correlation with the urinary presepsin/creatinine levels (r = 0.57, P = 0.02) (Fig. 5b).

Presepsin is secreted in the kidney interstitium. (a) Immunofluorescence staining of presepsin. The kidney interstitium was immunostained with presepsin (green). Nuclei were counterstained with DAPI (blue). Scale bar, 50 μm. (b) Correlation analysis between urinary presepsin/creatinine levels and presepsin fluorescent staining area. We randomly selected four cases from each of the four categories of interstitial inflammation cell infiltration severity (n = 16); the average value of the presepsin fluorescent staining area for each case is presented. Values were calculated using Spearman’s correlation coefficient test. DAPI, 4’,6-diamidino-2-phenylindole.
Subsequently, we performed double staining to assess presepsin localization at the blood cell level. Double staining with presepsin and CD163 was detected in the same blood cells for both markers (Fig. 6a). Among presepsin-positive cells, the proportion of CD163-positive cells was 42.3% (IQR, 35.2–51.9); the proportion of presepsin-positive cells among CD163-positive cells was 94.3% (IQR, 89.2–100%) (Fig. 6b). Double staining with presepsin and CD3 or CD20 was observed in distinct areas for each marker (Supplementary Fig. S1).

Presepsin is secreted by blood cells immunostained with CD163. (a) Immunofluorescence staining of presepsin and CD163. Presepsin (green) and CD163 (red) immunostaining can be observed in the same cells. Nuclei were counterstained with DAPI (blue). Scale bars, 50 μm. (b) The double-positive ratio of presepsin-CD163. We selected 6 cases of tubulointerstitial nephritis with severe interstitial inflammatory cell infiltration. The double-positive ratio of five fields for each case is presented (total, 30 fields). DAPI, 4’,6-diamidino-2-phenylindole.
Correlation between serum and urinary presepsin
We also considered the relationship between serum and urine presepsin levels. Kidney function is correlated with urine presepsin levels (Supplementary Fig. S2). In addition, specific diseases in this study showed particularly decreased kidney function (Table 1). Therefore, in order to eliminate the effects of decreased kidney function, we attempted to investigate a group with a single disease (IgAN) with less impaired kidney function. Considering IgAN, we detected no statistically significant correlation between log-transformed serum presepsin levels and urinary presepsin/creatinine levels (r = 0.18, P = 0.07) (Supplementary Fig. S3).
Discussion
Herein, we performed an analytical cross-sectional study targeting kidney diseases with kidney biopsy-confirmed diagnoses to explore the potential of urinary presepsin as a diagnostic marker for various kidney diseases, focusing on its relationship with interstitial inflammatory cell infiltration. Our findings revealed a notable association between urinary presepsin levels and the severity of interstitial inflammatory cell infiltration, as substantiated by immunofluorescence staining. To the best of our knowledge, this is the first study to demonstrate an association between urinary presepsin levels and kidney disease.
Presepsin has been identified as a biomarker in serum and other bodily fluids, such as cerebrospinal fluid28,29, pleural fluid30, and synovial fluid31, predominantly for distinguishing between infections and non-infections. A recent cross-sectional study utilized urinary presepsin to distinguish between pyelonephritis and non-pyelonephritis23. Our study may have shifted the application of presepsin from infection to kidney diseases, potentially offering a novel perspective and suggesting an association between urinary presepsin and kidney diseases.
Herein, our findings suggest that urinary presepsin is locally produced in the kidneys based on the following two reasons. Firstly, presepsin is a 13 kDa protein, presumably filtered by the glomerulus and almost completely reabsorbed and catabolized within proximal tubular cells. Therefore, in patients with impaired kidney function, a reduction in glomerular filtration leads to presepsin accumulation in the bloodstream, resulting in elevated serum presepsin levels32. Consequently, urinary presepsin values in patients with impaired kidney function are assumed to be within the normal or low range. However, in the current study, urinary presepsin values were primarily higher than those in normal individuals. Additionally, no statistically significant correlation was detected between log-transformed serum presepsin and log-transformed urinary presepsin/creatinine levels among the group where the effects of decreased kidney function were eliminated as much as possible (Supplementary Fig. S3). Based on these observations, we considered that there was a reason for the local increase in urinary presepsin other than the increase in blood, We postulate that the increased urinary presepsin levels originate within the kidneys through a mechanism independent of glomerular filtration rather than systemic overflow. We propose that inflammatory cell infiltration in the interstitium of the kidney is responsible for presepsin production. This hypothesis was supported by the finding that urinary presepsin levels increase in proportion to the degree of interstitial inflammatory cell infiltration. Secondly, positive immunofluorescence staining for presepsin in the kidney interstitium and the correlation between urinary presepsin levels and presepsin-positive immunostaining areas further suggested this association. Furthermore, we examined interstitial blood cells at high-power magnification and found that presepsin was positively stained on the same blood cells as CD163, and the proportion of CD163-positive staining among presepsin-positive cells was approximately half. CD163 is a marker for macrophages, while presepsin is produced by cleavage from CD14, and the co-staining of presepsin and CD3 and CD20 was distinct; therefore, we suggest that the remaining half of the presepsin-positive cells, which were negative for CD163 staining, were likely derived from monocytes. Consequently, we propose that the cells responsible for presepsin production are primarily interstitial monocytes/macrophages. Compared with other urinary biomarkers, the classical urinary biomarker NAG is reportedly elevated in association with interstitial inflammatory cell infiltration and has a high diagnostic capacity for TIN; however, as NAG originates from kidney tubular impairment, it indirectly reflects interstitial inflammatory cell infiltration33,34. Urinary CD163 has also gained attention as a biomarker, reflecting glomerular inflammation more than interstitial inflammation7,8,9,35,36,37. Considering the results shown in Fig. 6, which indicate that only approximately half of the presepsin-positive cells are also CD163-positive, and that CD163-positive cells only become positive after the inflammation reaches advanced phase38, urinary presepsin could potentially serve as a marker for detecting inflammation at an earlier stage compared to CD163. Early diagnosis of the disease and prompt treatment are crucial. The significance of urinary presepsin lies in its potential to facilitate early disease diagnosis and treatment. Based on the evidence presented above, urinary presepsin may directly identify the presence of interstitial inflammatory cell infiltration. In the current study, urinary presepsin was associated with better detection of TIN and severe interstitial inflammatory cell infiltration than NAG. We conducted analyses using both urinary presepsin normalized and non-normalized to urinary creatinine to account for potential variations in creatinine excretion, given that these fluctuations could potentially impact the observed results. However, no significant differences were detected between the two approaches; consequently, we also considered non-normalized urinary presepsin to be valuable.
This study had several strengths. First, the assessment of urinary presepsin is entirely non-invasive and provides immediate results within 17 min, unlike kidney biopsy, allowing repeated performance as often as necessary. This extends the applicability of urinary presepsin even to patients who hesitate to undergo a kidney biopsy because of factors such as bleeding tendencies, atrophic kidneys, and communication difficulties. The benefits of these factors are immeasurable to both clinicians and patients. In particular, kidney biopsy is frequently not performed in patients with TIN; therefore, urinary presepsin testing could be a desirable alternative diagnostic method. Second, urinary presepsin levels were compared with pathology diagnostic results of more than 400 kidney biopsies, demonstrating high robustness. Furthermore, we elucidated the mechanism underlying elevated urinary presepsin levels using immunofluorescence staining, which directly linked the mechanism of elevation to the pathological findings. Third, a measurement system to diagnose sepsis using blood samples has been established and is currently covered under insurance in Japan. Therefore, by adapting a blood measurement system, urinary presepsin testing can be undertaken promptly in clinical practice.
This study had several limitations. First, it was limited to specific regions within Japan, potentially impacting its generalizability. However, all specimens and data were centralized at Nagoya University Hospital, ensuring consistency in pathological processing and diagnostic quality. Second, the study population was exclusively comprised of patients who had undergone kidney biopsy; therefore, our results may not apply to individuals who did not undergo kidney biopsy. However, kidney biopsy allows for a definitive diagnosis and comprehensive evaluation of kidney pathology. Third, given that no longitudinal study has been conducted, its association with kidney prognosis remains uncertain. Repeated urinary presepsin measurements may elucidate the underlying pathophysiology, and future longitudinal studies are necessary.
In conclusion, urinary presepsin could be developed as a valuable biomarker for directly assessing monocyte infiltration, as well as CD163 macrophage infiltration, in kidney diseases. Its non-invasive nature, rapid results, and potential as a complement to kidney biopsy make it a valuable tool for clinicians and patients.
Data availability
All data analyzed in this research are included in this article. Reasonable requests for additional data or materials will be fulfilled under appropriate agreements. Requests should be made to the corresponding author.
References
Fassett, R. G. et al. Biomarkers in chronic kidney disease: a review. Kidney Int. 80, 806–821 (2011).
Parikh, C. R. & Garg, A. X. Acute kidney injury: better biomarkers and beyond. Kidney Int. 73, 801–803 (2008).
Ix, J. H. & Shlipak, M. G. The promise of tubule biomarkers in kidney disease: a review. Am. J. Kidney Dis. 78, 719–727 (2021).
Stratta, P. et al. Risk management of renal biopsy: 1387 cases over 30 years in a single centre. Eur. J. Clin. Investig. 37, 954–963 (2007).
Corapi, K. M., Chen, J. L. T., Balk, E. M. & Gordon, C. E. Bleeding complications of native kidney biopsy: a systematic review and meta-analysis. Am. J. Kidney Dis. 60, 62–73 (2012).
Prasad, N. et al. Real-time ultrasound-guided percutaneous renal biopsy with needle guide by nephrologists decreases post-biopsy complications. Clin. Kidney J. 8, 151–156 (2015).
Huang, Y. J., Lin, C. H., Yang, H. Y., Luo, S. F. & Kuo, C. F. Urine Soluble CD163 Is a Promising Biomarker for the Diagnosis and Evaluation of Lupus Nephritis. Front Immunol. 13, 935700 (2022).
Moran, S. M. et al. The Clinical Application of Urine Soluble CD163 in ANCA-Associated Vasculitis. J Am Soc Nephrol. 11, 2920–2932 (2021).
Yokoe, Y. et al. Clinical impact of urinary CD11b and CD163 on the renal outcomes of anti-neutrophil cytoplasmic antibody-associated glomerulonephritis. Nephrol Dial Transplant. 36, 1452–1463 (2021).
Arai, Y. et al. Phagocytosis by human monocytes is required for the secretion of presepsin. J. Infect. Chemother. 21, 564–569 (2015).
Yaegashi, Y. et al. Evaluation of a newly identified soluble CD14 subtype as a marker for sepsis. J. Infect. Chemother. 11, 234–238 (2005).
Shozushima, T. et al. Usefulness of presepsin (sCD14-ST) measurements as a marker for the diagnosis and severity of sepsis that satisfied diagnostic criteria of systemic inflammatory response syndrome. J. Infect. Chemother. 17, 764–769 (2011).
Endo, S. et al. Usefulness of presepsin in the diagnosis of sepsis in a multicenter prospective study. J. Infect. Chemother. 18, 891–897 (2012).
Endo, S. et al. Presepsin as a powerful monitoring tool for the prognosis and treatment of sepsis: a multicenter prospective study. J. Infect. Chemother 20, 30–34 (2014).
Wu, C. C. et al. Comparison of diagnostic accuracy in sepsis between presepsin, procalcitonin, and C-reactive protein: a systematic review and meta-analysis. Ann. Intensive Care 7, 91 (2017).
Nakamura, Y. et al. Usefulness of presepsin in the diagnosis of sepsis in patients with or without acute kidney injury. BMC Anesthesiol. 14, 88 (2014).
Nakamura, Y. et al. Comparison of accuracy of presepsin and procalcitonin concentrations in diagnosing sepsis in patients with and without acute kidney injury. Clin. Chim. Acta. 490, 200–206 (2019).
Kim, S. Y., Hong, D. Y., Lee, K. R., Paik, J. H. & Jung, H. M. Plasma presepsin level predicts acute kidney injury in patients with sepsis in the emergency department. Medicine (Baltimore) 101, e29919; https://doi.org/10.1097/MD.0000000000029919 (2022)
Nagata, T. et al. Clinical impact of kidney function on presepsin levels. PLoS One 10, e0129159; https://doi.org/10.1371/journal.pone.0129159 (2015).
Miyoshi, M. et al. Clinical evaluation of presepsin considering renal function. PLoS One 14: e0215791; https://doi.org/10.1371/journal.pone.0215791 (2019).
Kobayashi, S., Amano, H., Terawaki, H., Kawaguchi, Y. & Yokoo, T. Prediction of presepsin concentrations through commensurate decline in kidney function in the elderly. Clin. Chim. Acta 500, 1–9 (2020).
Botondi, V. et al. Perinatal asphyxia partly affects presepsin urine levels in non-infected term infants. Clin. Chem. Lab. Med. 60, 793–799 (2022).
Yamashita, R., Izumi, Y., Nakada, K. & Hiramoto, J. Utility of urinary presepsin in the diagnosis of pyelonephritis: a cross-sectional study. BMC. Infect. Dis. 23, 365 (2023).
Mysore, V. et al. Monocytes transition to macrophages within the inflamed vasculature via monocyte CCR2 and endothelial TNFR2. J. Exp. Med. 219, e20210562; https://doi.org/10.1084/jem.20210562 (2022).
Shimamura, Y. et al. Mesenchymal stem cells exert renoprotection via extracellular vesicle-mediated modulation of M2 macrophages and spleen-kidney network. Commun. Biol. 5, 753 (2022).
Kurihara, T. et al. Evaluation of cardiac assays on a benchtop chemiluminescent enzyme immunoassay analyzer. PATHFAST. Anal. Biochem. 375, 144–146 (2008).
Okamura, Y. & Yokoi, H. Development of a point-of-care assay system for measurement of presepsin (sCD14-ST). Clin. Chim. Acta 412, 2157–2161 (2011).
Stubljar, D. et al. Diagnostic accuracy of presepsin (sCD14-ST) for prediction of bacterial infection in cerebrospinal fluid samples from children with suspected bacterial meningitis or ventriculitis. J. Clin. Microbiol. 53, 1239–1244 (2015).
Zheng, G., Zhang, C., Zhang, G. & Shao, C. Evaluation of the diagnostic and prognostic value of CSF presepsin levels in patients with postneurosurgical ventriculitis/meningitis. Infect. Drug Resist. 14, 2901–2909 (2021).
Watanabe, N. et al. The usefulness of pleural fluid presepsin, C-reactive protein, and procalcitonin in distinguishing different causes of pleural effusions. BMC Pulm. Med. 18, 176 (2018).
Imagama, T. et al. Synovial fluid presepsin as a novel biomarker for the rapid differential diagnosis of native joint septic arthritis from crystal arthritis. Int. J. Infect. Dis. 102, 472–477 (2021).
Chenevier-Gobeaux, C., Trabattoni, E., Roelens, M., Borderie, D. & Claessens, Y. E. Presepsin (sCD14-ST) in emergency department: the need for adapted threshold values?. Clin. Chim. Acta 427, 34–36 (2014).
Skálová, S. The diagnostic role of urinary N-acetyl-beta-D-glucosaminidase (NAG) activity in the detection of renal tubular impairment. Acta Medica (Hradec Kralove) 48, 75–80 (2005).
Wu, Y. et al. Pathological significance of a panel of urinary biomarkers in patients with drug-induced tubulointerstitial nephritis. Clin. J. Am. Soc. Nephrol. 5, 1954–1959 (2010).
Endo, N. et al. Urinary soluble CD163 level reflects glomerular inflammation in human lupus nephritis. Nephrol. Dial. Transplant. 31, 2023–2033 (2016).
Mejia-Vilet, J. M. et al. Urinary soluble CD163: a novel noninvasive biomarker of activity for lupus nephritis. J. Am. Soc. Nephrol. 31, 1335–1347 (2020).
Aendekerk, J. P. et al. Urinary soluble CD163 and disease activity in biopsy-proven ANCA-associated glomerulonephritis. Clin. J. Am. Soc. Nephrol. 15, 1740–1748 (2020).
Mysore, V. et al. Monocytes transition to macrophages within the inflamed vasculature via monocyte CCR2 and endothelial TNFR2. J Exp Med. 219, e20210562 (2022).
Acknowledgements
The authors thank all attending physicians from the participating hospitals who contributed to data collection and the patients who participated in this study. The participating hospitals were Anjo Kosei Hospital, Chubu Rosai Hospital, Chutoen General Medical Center, Daido Hospital, Gifu Prefectural Tajimi Hospital, Handa City Hospital, Ichinomiya Municipal Hospital, Japanese Red Cross Aichi Medical Center, Nagoya Daiichi Hospital, Kainan Hospital, Kasugai Municipal Hospital, Komaki City Hospital, Konan Kosei Hospital, Masuko Memorial Hospital, Nagoya Central Hospital, Nagoya Kyoritsu Hospital, Nagoya Medical Center, Nagoya Memorial Hospital, Ogaki Municipal Hospital, Tokai Central Hospital, Tosei General Hospital, Toyohashi Municipal Hospital, Toyota Kosei Hospital, Tsushima City Hospital. The authors thank Yuriko Sawa of the Department of Nephrology at Nagoya University Hospital for help with the histology.The authors thank Mochida Pharmaceutical Co., Ltd for providing anti-presepsin polyclonal antibody.
Funding
This study was supported by PHC Holdings Corporation. PATHFAST was rented, presepsin measurement kits were provided free of charge, and we also received a grant.
Author information
Authors and Affiliations
Contributions
SN and AT wrote the draft manuscript. All authors conceptualized the research idea and study design; however, the contribution by KF was particularly significant. All authors collected samples. SN and AT mainly performed the data analysis and performed data management. All authors interpreted the data and contributed important intellectual content to the writing and revision of the manuscript. Thus, all authors are accountable for their contributions.
Corresponding author
Ethics declarations
Competing interests
This study was supported by PHC Holdings Corporation. PATHFAST was rented, presepsin measurement kits were provided free of charge, and we also received a grant.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Niwa, S., Tanaka, A., Furuhashi, K. et al. Urinary presepsin is a novel biomarker capable of directly assessing monocyte/macrophage infiltration in kidney diseases. Sci Rep 14, 30088 (2024). https://doi.org/10.1038/s41598-024-80686-7
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-024-80686-7
Keywords
This article is cited by
-
Urinary presepsin can efficiently detect T-cell-mediated rejection in patients who have undergone kidney transplantation
Clinical and Experimental Nephrology (2025)
