
Abstract
Rotationplasty is a surgical technique used to salvage the limb following resection of a sarcoma or to address congenital defects. The procedure repurposes the ankle as a new knee, while fusing the thigh and shank musculature to achieve ‘knee’ flexion/extension. Most unique is the retainment of original innervations of the distal and proximal musculature, thus requiring spinal reorganization to coordinate the separate muscles as a single tensile unit. Lower body kinematics, intersegmental coordination, and electromyography (EMG) derived muscle synergies of nine participants are quantified during overground walking. Half the sample exhibited ‘normal’ ‘knee’ kinematics with fused muscles exhibiting synced temporal dynamics of EMG activity in the surgical limb. The congruent EMG activity between fused muscles, especially the gastrocnemius with the rectus femoris, suggests successful spinal reorganization to achieve cooperative contraction as a single tensile unit. Conversely, a few individuals were categorized as ‘low’ knee function categorized by low dynamic peak range of the knee joint which may be explained by the observed discordant EMG activity between the fused muscles. The most substantial characteristic differences between the ‘high’ and ‘low’ knee functioning individuals were age and time since surgery, with the ‘low’ being younger and having a shorter time since surgery.
Similar content being viewed by others
Introduction
The Van Nes Rotationplasty is a surgical technique used to address congenital deformity or bone loss (i.e., sarcoma resection, infection, trauma) that involves a transection of the femur and a 180° rotation of the tibia repurposing the ankle joint as the new knee joint1,2,3,4 (see Fig. 1). A hallmark of rotationplasty is the fusion of the resected thigh musculature to resected shank musculature (i.e., connecting quadriceps to plantar flexors and hamstrings to dorsiflexors) while retaining their original innervations. Thus, multilevel spinal segment projections must coordinate muscle activity between these two segments as a single tensile unit to achieve ‘knee’ flexion/extension. Despite this neural and operational complexity, rotationplasty is considered a viable and sustainable option to salvage the lower limb, especially if the goal of the patient is greater levels of physical activity4,5,6,7. However, the procedure is rarely performed due to low prevalence of pediatric sarcoma8 and discomfort regarding limb cosmesis1. Moreover, the procedure is predominantly performed in children and adolescents as that is when bone sarcomas are most likely to occur. Importantly, alternative procedures such as above-knee amputation exist with limited complications but have poorer gait related functional outcomes5,7,9,10,11. Further, rotationplasty may be preferred over above-knee amputation or limb salvage surgery with endoprosthetic reconstruction by individuals who desire comparable physical activity levels to healthy populations and the ability to engage in dynamic activities (i.e., sports)9,12. Indeed, ~ 85% of individuals with rotationplasty participate in sports ~ 7 years after their procedure was performed13. Therefore, it is imperative to better understand coordination between segments and fused muscles to assess motor control following rotationplasty to uncover potential factors to enhance rehabilitation.

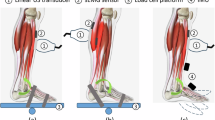
Surgical Images and Radiographs of Rotationplasty About the Knee. Panel (A) is an intra-operative image of the patient with the affected tissue removed and blood vessels and nerves preserved. Panel (B) is an image of rotationplasty following surgical completion. Panel (C) are anterior to posterior and lateral view post-surgical radiographs. Salvaged femur is measured from the superior aspect of the femoral head (green arrow) to the junction site of the fused femur and tibia (red arrow). Salvaged tibia is measured from the junction site of the fused femur and tibia (red arrow) to the inferior aspect of the tibia (tibial plafond—yellow arrow). Note that when muscles are fused there is not a clear scar line as the ends of each muscle are overlayed.
Surgical decision making regarding the amount of tissue salvaged during the rotationplasty procedure is mostly dictated by the insult (i.e., tumor, infection, or trauma)1, however, surgeons do have a degree of latitude regarding resection levels and planning for new extremity length based on remaining tibia, femur, and expected remaining growth compared to contralateral (unaffected) limb in pediatric patients. Given the fusion of thigh to distal musculature to create a new knee extensor and flexor muscle unit, some surgeons have anecdotally hypothesized that retaining more of the distal segment (i.e., tibia and lower leg musculature) will yield better functional outcomes. This postulation is based on the premise that the individual will have less proximal musculature that requires neural circuitry reorganization to adjust timing to coincide with the distal musculature that is ‘coded’ for that joint in addition to retaining the origin and innervation for the anterior and posterior compartments of the leg that power new ‘knee’ flexion/extension. For example considering the quadriceps and gastrocnemius, fiber type composition and muscle spindle abundance are similar14,15,16, but somatosensory encoding to regulate gait will differ due to their distinct phase dependent contributions17,18,19,20,21,22. Specifically, appropriate stance-to-swing transition muscle activation is achieved via rectus femoris muscle spindles at a critical point of hip extension23 and unloading of the limb detected by the plantar flexors’ muscle spindles and golgi tendon organs afferents24,25 which is now altered by shifting the ankle to the knee in rotationplasty. To date it is still unclear how the fused muscles (quadriceps-ankle plantar flexors fused group and hamstrings-ankle dorsiflexors fused group) coordinate with each other despite retaining their original innervations that project from different spinal segment levels. Moreover, it is unknown if the thigh to shank length ratio plays a role in this relationship.
Previous research has focused on basic spatiotemporal outcomes such as gait velocity, stance time, and swing time4; and/or discrete joint/muscle outcomes independently following rotationplasty surgery26. In a cohort of 43 individuals with rotationplasty, the gastrocnemius and soleus had synchronicity between each other and the tibialis anterior coincided with ‘knee flexion’ for the surgical limb26. However, this study considered each muscle independently and did not examine the relationship between fused muscles (e.g., rectus femoris-gastrocnemius or medial hamstring-tibialis anterior). Moreover, discrete kinematic variables such as peak knee flexion and joint excursion were assessed observing comparable biomechanics to healthy individuals26. Discrete outcomes characterize average behavior of the lower extremity during gait but fail to capture execution of movement to achieve these outcomes. For example, continuous relative phase (CRP), which determines the angular position-velocity segment orientation relationship between two segments in regard to their movement27,28, has been used to demonstrate differences in coordination between injured and non-injured runners when discrete outcomes were similar between groups29. Further, non-negative matrix factorization can assess electromyography (EMG) of muscle activity to determine muscle synergy composition30,31,32. Given the unique circumstance of rotationplasty with thigh and shank musculature fused into a single muscle, it is important to understand the consequences to coordination throughout the entire gait cycle.
The primary purpose of this investigation was to examine kinematics, intersegmental coordination, and muscle synergies in the surgical and intact limbs of individuals who received a rotationplasty during overground walking tasks. The secondary purpose was to provide descriptive/qualitative analysis between ‘high’ knee functioning and ‘low’ knee functioning individuals who had a rotationplasty to elucidate potential factors contributing to post-surgery dysfunction. We hypothesized that the surgical limb would have lesser peak knee flexion during swing phase and a more in phase coupling of the thigh-shank segment compared to the intact limb. Likewise, we hypothesized that the surgical limb would have greater muscle synergy complexity due to the fusing of muscles from different limb segments. To that end, we expected that individuals categorized as ‘low’ functioning would have merged synergies or excessive co-contractions that compete with normal segment coupling and that ‘low’ functioning individuals have greater femur tibial length.
Results
General
Following rotationplasty, the surgical limb generally had a longer tibia than femur (evidenced by the FTR < 1) and the participants achieved a self-selected walking speed of 1.11 ± 0.22 m/s (refer to Table 1). Eight of the participants used a solid ankle cushioned heel (SACH) prosthetic. These eight individuals completed the gait trials with their normal athletic footwear on both their intact foot and the prosthetic foot. One participant used a blade prosthetic.
Discrete kinematics
See Fig. 2 for the mean sagittal plane hip, knee, and ankle angle waveforms of an entire stride for all participants. Refer to Table 2 for the mean and standard deviation of all discrete variables stratified by limb. Regardless of limb, participants executed similar mean step lengths (p = 0.77, d = 0.10, 95% CI − 0.08 to 0.06) and step length variability (p = 0.68, d = 0.14, 95% CI − 0.01 to 0.01) between limbs. However, when considering the entire stride, stance phase accounted for a greater percentage of the stride in the intact limb (p = 0.003, d = 1.36, 95% CI 3.70 to 13.26) compared to the surgical limb. The hip and ankle of the surgical limb had reduced mean joint excursion (DPR) in the sagittal plane compared to the intact limb (hip: p = 0.003, d = 1.39, 95% CI − 12.27 to − 3.54; ankle: p < 0.001, d = 2.63, 95% CI 4.82 to 8.80). Additionally, the intact limb had greater (p = 0.004, d = 1.34, 95% CI 0.42 to 1.56) ankle DPR variability than the surgical limb.

Sagittal Plane Joint Angle Waveforms. Each line represents a different participant, with red lines representing participants from the ‘High’ knee functioning group while the blue lines represent participants from the ‘Low’ knee functioning group. The vertical line indicates the transition from stance phase to swing phase. The ankle angle is represented as degrees of plantarflexion (PF; positive values) and degrees of dorsiflexion (DF; negative values). For the knee and hip, flexion is positive, and extension is negative. All participants’ intact limb knee joints had a first peak of knee flexion for shock attenuation (~ 5–20% of gait) followed by gradual full extension into push-off with a passively flexing knee through swing (second peak) evidenced by the steep ascending and descending slope. Conversely, only half the cohort had this knee behavior in the surgical limb knee (rotated ankle). Specifically, three individuals’ surgical limb knee joint remain flexed throughout stance phase (~ 10–58% gait cycle) while another participant’s knee remained almost fully extended throughout the entire gait cycle.
Conversely, there was no difference in knee DPR between limbs (p = 0.08, d = 0.66, 95% CI − 34.29 to 2.51). Likewise, there was no difference in mean peak knee flexion during swing between limbs (p = 0.19, d = 0.48, 95% CI − 5.81 to 24.71). However, the intact limb had greater peak knee flexion variability across strides compared to the surgical limb (p = 0.03, d = 0.88, 95% CI 0.16 to 2.33). Moreover, peak knee flexion occurred earlier during swing phase in the surgical limb compared to the intact limb (p = 0.003, d = 1.43, 95% CI 3.35 to 6.62). While the knee reached peak knee flexion at a similar knee flexion velocity (i.e., ascending swing slope) for both limbs (p = 0.11, d = 0.60, 95% CI − 1.85 to 0.22), the surgical limb extended slower than the intact limb following peak knee flexion (p = 0.01, d = 1.14, 95% CI 0.04 to 2.11).
Coordination
See Fig. 3 for shank-foot, thigh-shank, and pelvis-thigh coupling CRP plots of the entire sample stratified by limb. During swing phase, the surgical limb shank-foot coupling had greater (p < 0.001, d = 2.11, 95% CI 7.14 to 15.32) mean phase compared to the intact limb. Additionally, during swing phase, the surgical limb thigh-shank coupling had lesser (p = 0.01, d = 1.05, 95% CI − 50.27 to − 7.72) mean phase compared to the intact limb.

Continuous Relative Phase (CRP) Plots. Solid line indicates the sample mean and the shaded areas are the sample standard deviation. CRP at 0 indicates in-phase or both segments rotating together at the same rate in the same direction. ± 180 indicates anti-phase (segments rotating in opposite directions simultaneously at the same rate) between both segments; if the value is positive then the proximal segment is leading the distal segment; if the value is negative then the distal segment is leading the proximal segment. Shank-Foot and Thigh-Shank couplings demonstrated similar behaviors between limbs. However, the surgical limb Thigh-Shank coupling exhibited greater variability across subjects verified by different dynamic peak ranges of the knee. Additionally, the surgical limb shank-foot coupling was predominantly in phase for the entirety of swing phase (~ 57–100%) which is likely due to the passive feature of the prosthetic ankle joint. By contrast, for the Pelvis–Thigh coupling, the intact limb was more pelvis led while the surgical limb was more thigh led. Both limbs had greater variability across subjects compared to the other two couplings suggesting the Pelvis–Thigh coupling as the modulator for optimizing gait to compensate for the surgical knee (rotated ankle).
Muscle synergies
Two participants data were removed from the analysis due to unusable EMG data due to interaction with the socket contaminating the signal. Refer to Fig. 4 for merged plots of the sample mean knee angle waveform and the sample mean EMG waveforms separated by extensor and flexor muscles.

Knee Kinematics and EMG Waveform Merged plots. Waveforms (knee kinematic and EMG signals) are the mean across all participants. Intact limb extensors had traditional behavior with the knee extensors activating during load acceptance (1–30% of gait)20 and the gastrocnemius increasing activity at toe-off for propulsion21,22 leading to passive knee flexion during swing (second peak of knee angle waveform). Similarly, the flexors of the intact limb had traditional behavior with the tibialis anterior activating more during early stance and again during swing to clear the toes while the hamstrings activate in early stance. For the surgical limb, the extensors were excited during early stance with vastus lateralis and gastrocnemius peaks coinciding, suggesting cooperation between the resected muscles. However, during swing the vastus lateralis and gastrocnemius had divergent behavior. The flexors in the surgical limb had the greatest discontinuity with tibialis anterior and medial hamstring peaks rarely aligning despite their physical connection. There was extended activity of the tibialis anterior during swing, initially providing ‘knee’ flexion but then resisting extension (possibly explaining the shallower descending slope).
When considering two synergies, greater variance (p < 0.001, d = 6.40, 95% CI 2.8 to 10.00) was accounted for by the surgical limb compared to the intact limb. Two synergies accounted for 95% of the variance in the surgical limb and only 59% in the intact limb. One synergy accounted for 90% of the variance in the surgical limb and over 65% in the intact limb. With the surgical limb, two synergies increased the accounted for variance indicating a more complex coordinative pattern whereas it decreased in the intact limb.
‘High’ versus ‘low’ knee functioning
Participants were categorized as ‘High’ knee functioning with a knee DPR > 40° and ‘Low’ knee functioning with a knee DPR < 40° with 5 participants classifying as ‘high’ knee functioning and 4 participants classifying as ‘low’ knee functioning. See Table 1 for sample characteristics stratified by functional group. Briefly, ‘high’ knee functioning individuals (0.8 ± 0.3) had smaller FTR than ‘low’ knee functioning (1.2 ± 0.6). Likewise, the ‘high’ knee functioning group had a greater time since surgery compared to the ‘low’ knee functioning group on average (High: 6.6 ± 6.1; Low: 2.8 ± 0.8). Lastly, the ‘high’ knee functioning group had an average age of 19.5 ± 3.3 years whereas the ‘low’ functioning group had an average age of 11.0 ± 2.0 years at the time of analysis.
See Table 2 for discrete outcomes stratified by functional level. Refer to Fig. 5 for the CRP plots stratified by functional level. In the surgical limb the most pronounced differences between ‘high’ and ‘low’ knee functioning were for mean peak swing knee flexion (High: 62.24 ± 5.54°; low: 36.42 ± 16.66°), mean time to peak knee flexion during swing (high: 68.49 ± 1.97%; low: 55.61 ± 7.37%), mean step length (high: 0.65 ± 0.18 m; low: 0.53 ± 0.03 m), mean knee DPR (high: 61.07 ± 8.01°; low: 23.37 ± 14.26°), mean ascending swing slope (high: 2.50 ± 0.69; low: 0.34 ± 0.51), and mean descending swing slope (high: -2.15 ± 0.40; low: -0.54 ± 0.45). Despite the large differences between groups in the surgical limb, the differences between groups in the intact limb were not as pronounced. However, ‘low’ knee functioning group demonstrated the opposite behavior in the intact limb compared to the surgical limb with ‘low’ having greater mean knee DPR (high: 59.53 ± 6.31°; low: 61.05 ± 8.35°), mean Hip DPR (high: 34.84 ± 5.63°; low: 38.73 ± 5.85°), mean ascending swing slope (high: 2.33 ± 0.52; low: 2.38 ± 0.43) and mean descending swing slope(high: -2.64 ± 0.35; low: -2.77 ± 0.63).

Continuous Relative Phase (CRP) plots. Both groups had nearly identical shank-foot coupling in the surgical limb which is to be expected given the passive ankle joint of the prosthesis, which cannot be actively controlled. The thigh-shank coupling of the surgical limb highlights the level of dysfunction (low dynamic peak range) in the ‘low’ knee functioning group as the segments are almost completely in phase (rotated in same direction at same rate) the entire stride whereas the ‘high’ knee functioning group exhibits more anti-phase behavior with the thigh leading the shank similar to optimal functioning thigh-shank coupling (see intact limb Fig. 3). The pelvis-thigh coupling of the surgical limb also demonstrated differences between groups with the ‘high’ group exhibiting more variability in coordination strategy at load acceptance (1–30% of gait cycle) and swing (~ 55–100% of gait cycle). Variability across ‘high’ functioning participants was constrained during propulsive phase (~ 30–60% of gait cycle). Conversely, the ‘low’ group had more variability during propulsive phase and early swing. For the shank-foot and thigh-shank couplings of the intact limb both groups had similar coordination with the proximal segments leading the distal segments through most of the gait cycle. One exception to proximal leg coordination was late swing phase (80–100% of gait cycle) for the shank-foot coupling. The obvious difference between groups for the intact limb is in the pelvis-thigh coupling. For the ‘low’ knee functioning group the coupling was pelvis led (evidenced by positive CRP angle), whereas the thigh led the coupling in the ‘high’ knee functioning group.
To qualitatively assess differences in muscle function between ‘high’ and ‘low’ knee functioning, only participants with usable EMG data were considered. Refer to Figs. 6 and 7 for the merged plots of the extensor and flexor muscles respectively stratified by functional level.

Knee Kinematics and EMG Waveform Merged plots of Fused-Extensor Muscles. ‘Low’ knee functioning were participants with < 40° dynamic peak range in the surgical limb knee joint (rotated ankle). In the ‘low’ group surgical limb, gastrocnemius and vastus lateralis activity is greater in the early portion of stance phase but is low during swing phase in contrast to the ‘high’ group. Although extensor activity during swing would seem counterproductive, the late spike following peak knee flexion may aid in knee extension in preparation for heel-strike evidenced as the more natural knee angle waveform in the ‘high’ group. Moreover, the rectus femoris in the ‘high’ group surgical limb is upregulated during the ascending slope of knee flexion waveform during swing whereas it is low in the ‘low’ group.

Knee Kinematics and EMG Waveform Merged plots of the Fused-Flexor Muscles. In the ‘low’ group tibialis anterior (TA) activity is higher near toe-off (59% of gait cycle). However, medial hamstring activity does not match the TA suggesting a discontinuity in the resected muscle action. Despite the higher TA activity in the ‘low’ group the knee achieves little flexion indicating the necessity of the cooperation of the two resected muscles to produce meaningful force. In the ‘high’ group there is once again a late synchronous spike in TA and medial hamstrings activity following peak knee flexion.
Discussion
The purpose of this investigation was to examine kinematics, intersegmental coordination, and muscle synergies in the surgical and intact limbs of individuals who have undergone a rotationplasty during overground walking tasks while providing a descriptive analysis of ‘high’ and ‘low’ knee functioning participants. The entire sample demonstrated positive function (i.e., comparable walking speeds to healthy populations) and relatively symmetric sagittal plane joint behavior between limbs (see Table 2) in support of previous research11,26,33. Further, EMG activity and muscle synergy analysis indicated that the fused muscles (VL-gastroc and MH–TA) were synergistic (see Fig. 4). When considering the whole sample, together these findings suggest optimal spinal synaptic network re-organization during gait. However, when participants were stratified by functional level based on sagittal DPR of the surgical limb knee, new patterns emerged indicating that spinal circuits reorganization resulted in a suboptimal gait pattern. This latter point is evidenced by the discordant EMG activity of fused knee extensor muscles around the transition from stance to swing phase in the ‘low’ knee function group (see Fig. 6). Consequently, the thigh-shank coupling of the ‘low’ group is mostly in phase throughout the gait cycle in direct contrast to the intact limb and ‘high’ knee function group (see Fig. 5).
Walking speed has long been considered a critical measure of health and functional status for a multitude of populations with higher self-selected walking speeds (> 0.8 m/s) associated with better health and participation outcomes34. Previous cohorts of individuals with rotationplasty observed self-selected walking speeds of ~ 0.92 m/s11,33, which exceeds walking speeds of people with above-knee amputation11. In contrast, our sample walked at 1.11 m/s (range 0.76–1.31 m/s; see Table 1), which is comparable to healthy age-similar populations who typically walk at ~ 1.23 m/s11,33. Furthermore, walking speeds of 1.11 m/s fall within categories of being able to perform household activities and independently execute community ambulation34. It is unclear why our sample walked at higher self-selected walking speeds, but it may be due to our sample having a greater time since surgery (see Table 1) compared to previous cohorts. Regardless, our results support previous research that rotationplasty is a suitable treatment option for limb salvage when pursuing maximal post-surgical physical function.
Another important component to functional outcomes is the kinematic behavior of the joints. In a sample of 43 individuals with rotationplasty, the intact limb and surgical limb exhibited knee DPR of 59.7 ± 5.0° and 58.1 ± 11.6° respectively26. Similarly, our sample had a knee DPR of 60.2 ± 6.8° for the intact limb and 44.3 ± 22.4° for the surgical limb equating to < 1° and ~ 14° difference in the intact and surgical limb respectively compared to the other cohort. This greater difference in surgical limb behavior, while not entirely surprising given the anatomy of the joint, is likely due to our smaller sample size that was skewed by a few participants who had altered knee kinematics (refer to Figs. 6 and 7) reflected by the larger standard deviation of 22° (see Table 2). Likewise, the aforementioned sample observed 42.0 ± 8.2° and 42.4 ± 8.0° of sagittal hip excursion for the intact and surgical limb respectively26. Consistent with the knee kinematics, our sample’s hip excursion had ~ 5° less in the intact limb and ~ 13° less in the surgical limb (see Table 2) compared to previous cohorts, again likely driven by the smaller sample size. Nevertheless, most of our participants had coordinative behavior (see Figs. 2,3,4 and 5) with a definitive first flexion peak to attenuate force20, followed by the knee extending to aid in propulsion (albeit slightly less than an intact limb), followed by a passively flexing knee as the limb advances through swing phase (evidenced by the comparable ascending slope of knee angle [refer to Table 2]).
Prosthetic design is a critical factor to consider when assessing coordination35. In the present cohort, eight of the participants used a SACH design while one participant used a blade design. Importantly, participants were instructed to wear the prosthesis and footwear that they used on a regular basis for their normal activities of daily living to improve ecological validity. However, Fig. 2 demonstrates that some participants did achieve ankle excursion throughout the gait cycle despite the fixed position of the ankle on the prosthetic. Anecdotally, some participants did not tie their shoes as tight allowing extraneous movement of the prosthetic foot within the shoe. This movement within the shoe, coupled with markers tracking the foot placed on the shoe results in ‘dorsiflexion’ and ‘plantar flexion’. It is unclear if this was done purposefully by participants to mimic more ‘normal’ ankle kinematics, or purely coincidental. Nonetheless, while this would enhance ankle kinematics it will diminish propulsion and may explain the increased activity of the fused rectus femoris and gastrocnemius activity during early swing (see Fig. 4), especially participants in the ‘high’ group (see Fig. 5), which are likely advancing the limb through swing phase to compensate for the lack of propulsion that usually generates passive knee flexion and limb advancement36,37. Moreover, both ‘high’ and ‘low’ knee functioning individuals had similar foot-shank couplings for the surgical limb (see Fig. 5), which is expected given the passive ankle design. Yet some individuals were able to adapt successfully to this uncontrolled segment and achieve a greater knee DPR which is potentially explained by neurophysiological changes (see Figs. 6 and 7).
Paramount to rehabilitated and healthy gait is veridical perception and (re)calibration to internal and external perturbations, which is reliant on peripherally derived somatosensory information38. A key component of rotationplasty is the salvaging of the distal nerves (e.g., tibial nerve, common peroneal nerve), which are inevitably lost with a traditional amputation. Thus, if the sensory receptors are intact, afferent information can still be obtained. However, the rotation and attachment to the proximal segment would, at least initially until re-organization occurs through synaptic plasticity, result in improperly transcoded information. Limited or abnormal sensory information can affect timing and amplitude of surgical limb musculature resulting in altered motor patterns39,40,41. Therefore, large deviations in neural circuitry may ultimately lead to motor incoordination39,40,41, which may explain some of the unusual muscle activity observed in the ‘low’ knee functioning participants (see Figs. 6 and 7) who had altered gait patterns. Absent direct measurement of somatosensory receptors and their proprioceptive acuity, their role in the observed gait dysfunction following rotationplasty is conjecture. Nonetheless, synchronous peaks between the gastrocnemius, a stance phase muscle17, and rectus femoris during swing phase in the ‘high’ knee functioning group surgical limb (see Fig. 6) suggests spinal reorganization of the motor circuits which may include improved accuracy of somatosensory input. Future research should directly measure somatosensory behavior, specifically reflex excitability and proprioception accuracy in individuals who have received a rotationplasty.
Intriguingly, the ‘low’ knee functioning participants were ~ 7 years younger (11.0 ± 2.0 years) on average than the ‘high’ functioning participants (19.5 ± 3.3 years). Due to the cross-sectional design, it cannot be determined if poor surgical limb coordination is a consequence of biological age (i.e., state of physical maturity) or the surgery being performed at a younger age. Alternatively, time since surgery may influence function but similar to age, the cross-sectional design makes it difficult to ascertain its true impact. The ‘high’ knee functioning group was ~ 4 years greater for time since surgery than ‘low’ knee functioning on average. However, the 6-year standard deviation of the ‘high’ group warrants further examination to appropriately interpret the role of this factor in functional level (see Table 1). Moreover, two participants were assessed > 3 years after surgery but were in the ‘low’ knee functioning group whereas two participants in ‘high’ knee functioning group were assessed < 2 years after surgery (see Table 1). While gait does stabilize by age 3–842,43, maturity of the locomotor system continues to develop to young adulthood42,44,45. Specifically, there is ~ 58% reduction in stride interval variance (which is modulated by the coordinative patterns of lower limb segments) from 3–4 to 11–14 year olds46. Thus, a large reduction in gait variability occurs from prepubescence to adolescence with the majority of stabilization happening during the prepubescent stage46. Moreover, muscle coactivation is higher in children compared to adults, especially during dynamic multi-joint actions47. In the ‘low’ knee functioning group we observed evidence of coactivation at inappropriate phases of gait (see Figs. 6 and 7) supporting this notion that biological age influences functional outcomes following rotationplasty. Furthermore, biological age could explain some of our divergent results from previous studies as our sample was on average 5–10 years younger26,48. However, prospective research is needed to confirm if biological age or age at surgery is the key determinant in gait function.
Lastly, it was speculated that greater shank to thigh length ratio would be beneficial to functional outcome as this would indicate greater retainment of distal musculature and requiring less spinal reorganization to achieve optimal coordination between the fused muscles. When stratified by knee functional level, the ‘low’ and ‘high’ group had a FTR of 1.2 ± 0.60 and 0.8 ± 0.30 respectively. Values > 1 indicate a longer femur compared to the tibia following rotationplasty. Although the FTR was larger for the ‘low’ group, the large standard deviation and range for both groups dispel any clear trend (see Table 1). This finding, despite failing to support our hypothesis, should be interpreted with some optimism as it suggests that the ratio of tissue from one segment over the other, a factor mostly out of the control of the surgeon, doesn’t necessarily impact functional outcomes. Nevertheless, future research should examine the influence of salvaged femur, tibia, quadricep, hamstring, ankle plantar flexor and dorsiflexor length on functional outcomes in a larger cohort.
Limitations of this study must be acknowledged that warrant caution for interpretations. Firstly, the sample size was small, all male, and the age range at the time of analysis was large. While these features of the sample are not ideal, rotationplasty is a rare procedure used to treat even rarer conditions. The prevalence of pediatric osteosarcoma is only 15%8 which translates to approximately 560 cases per year in the United States49. Further, only 42% and 19% of this population experience osteosarcoma at the distal femur and proximal tibia respectively50,51 and it is more prevalent in males52. Additionally, not all survivors will choose rotationplasty as the treatment option, in particular a prior report has indicated that females tend to choose alternative treatment options despite better functional outcomes of rotationplasty due to psychological discomfort/concern surrounding the appearance of the limb1. Participants were instructed to wear the prosthetic and footwear they used the most for everyday activity to improve ecological validity. Anecdotally, some participants did not tie their shoes as tight allowing the prosthetic foot to shift within the shoe essentially creating ‘dorsiflexion’ as they walked. Moreover, one participant used a blade prosthetic which will alter coordination compared to a SACH construct. Therefore, we must acknowledge that this lack of standardization to prosthetic componentry and footwear will lessen internal validity. However, this is the first study to directly assess the coordination and muscle synergies of the surgical and intact limbs of individuals who received a rotationplasty. To confirm the findings of this investigation, future research should utilize longitudinal designs with assessments occurring at the same relative time points (i.e., time since surgery). Furthermore, individuals with rotationplasty should be compared to age-matched healthy typically developing individuals.
The idea that rotationplasty when utilized as a limb salvage procedure can yield positive functional outcomes, is further supported by the results of this investigation. Not only can individuals with a rotationplasty execute self-selected walking speeds analogous to healthy age-similar populations but ‘normal’ segmental coordination can be achieved as well for the new ‘knee’ joint (i.e., rotated ankle). In ‘high’ knee functioning individuals, fused muscle synergies can be observed that coincide with optimal knee mechanics. Furthermore, congruent muscle activity in the surgical limb of the ‘high’ knee functioning individuals, especially the gastrocnemius with the rectus femoris (see Fig. 6) evidence spinal reorganization. Conversely, ‘low’ knee functioning individuals had incongruent temporal dynamics of resected muscle activation that resulted in poor surgical limb knee function (i.e., DPR of the knee < 40°). While the mechanism behind poor adaptation to rotationplasty has not yet been elucidated, biological age at the time of surgery or time since surgery may be a strong indicator of ‘knee’ function.
Methods
Participants
Nine male participants who had received a rotationplasty at a single institution for tumor, trauma, or infection were recruited for this study to execute a series of overground walking trials at self-selected pace (see Table 1 for all participant characteristics). Participants were excluded if they were currently undergoing chemotherapy, had compromised neurovascular status, and/or were unable to walk independently in their prosthesis as evaluated by a physical therapist exam. Due to the rarity of this procedure, there were no exclusion criteria regarding age. The study was approved by the Colorado Multiple Institutional Review Board (COMIRB) and written informed consent/assent was obtained from the participant and parent/guardian prior to their participation. All experimental protocols were performed in accordance with the relevant guidelines and regulations including the Declaration of Helsinki.
Procedures
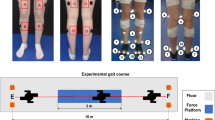
Participants executed a series of overground walking trials at self-selected pace with biomechanics data obtained via marker-based motion capture. Participants were instructed to wear the prosthesis and footwear that they used regularly for everyday activities of daily living and in the fashion they normally would to improve ecological validity. Kinematics were captured via 13 infrared cameras (Vicon, Oxford, UK) sampling at 120 Hz utilizing a modified Helen-Hayes marker-set consistent with the conventional gait model (see Fig. 8); kinetics were captured via 10 force plates (Bertec, OH, USA) sampling at 2160 Hz; muscle EMG activity was captured via 10 wireless sensors (Trigno Mini Sensor, Delsys, MA, USA) sampling at 2160 Hz. EMG was collected for Gastrocnemius (gastroc), Medial Hamstrings (MH), Anterior Tibialis (TA), Rectus Femoris (RF), and Vastus Lateralis (VL) in both the intact and surgical limbs. For muscles that would reside within the prosthetic socket, the low-profile sensor tail was placed over the target muscle and secured with liquid adhesive while the amplifier was placed outside of the socket. All EMG sensors were placed by the study physician or physician’s assistant guided by physical exam and participant post-surgical notes. Following placement of the sensors, manual muscle testing was performed on each muscle using an isolated movement to verify the sensors were reading the appropriate muscle.

Participant Prosthetic Marker-Setup. Panel A is the marker location for a blade construct and panel B is the marker location for a solid ankle cushioned heel construct.
Additionally, participant medical charts were reviewed for pertinent demographic and clinical information including reason for rotationplasty and date of surgery. Post-surgical femur and tibia length measurements of the surgical limb were obtained from radiographic images (see Fig. 1) and a femur to tibia length ratio (FTR) was calculated as femur length divided by tibia length.
Data reduction
Kinematics, kinetics, and EMG data were processed in Visual3D (C-Motion, Germantown, MD, USA) and analyzed in MATLAB (Mathworks, Inc., Natick, MA) with custom scripts. Biomechanical models were constructed utilizing a linked model for the trunk and lower extremities using 3D coordinates of reflective markers to calculate kinematics of the pelvis, thigh, shank and foot. Heel-strike was identified by vertical ground reaction forces (vGRF) exceeding 10N. Sagittal plane joint angle waveforms were constructed for each stride (heel-strike to ipsilateral heel-strike). Toe-off was identified by first instance of vGRF < 10N following ipsilateral heel-strike. Heel-strike and toe-off were visually identified for strides by two independent members of the research team when the participant did not strike the force plate directly. Mid-stance was considered 50% of stance phase (heel-strike to toe-off). Joint dynamic peak range (DPR) was calculated from peak extension and flexion in the sagittal plane during stance phase. A minimum of 10 strides were assessed per limb. Additionally, the swing ascending and descending knee angle slopes were calculated as the slope from toe-off to peak knee flexion and peak knee flexion to peak knee extension during swing phase respectively.
Continuous relative phase (CRP) was calculated to assess segment coupling (i.e., coordination) for the foot-shank, shank-thigh, and thigh-pelvis in the sagittal plane following the guidelines detailed by Li28. CRP is conducted by constructing phase-plane portraits of normalized angular displacement and angular velocity of each segment from a single stride normalized to 101 data points. Phase portraits were then normalized to minimum and maximum values in each axis and phase angles calculated from the normalized phase-plane trajectories of each segment. Finally, CRP was calculated by subtracting the phase angle of the distal segment from the phase angle of the proximal segment at each instant of time. Visual assessment of CRP-plots can yield critical qualitative differences between limbs/conditions29 but calculating mean absolute relative phase [phase dynamic] and deviation phase [variability] allows for quantitative comparison of CRP-plots53,54. Thus, once CRP plots were constructed, mean phase (the mean relative phase of all strides) and deviation phase (mean standard deviation of all strides) were calculated for four specific phases of gait: (i) stance phase, (ii) swing phase (toe-off to heel-strike), (iii) load acceptance phase (first 50% of stance phase), and (iv) propulsion phase (last 50% of stance phase).
All EMG data were first separated into strides, filtered with a bandpass (30 and 400 Hz), rectified, filtered with a low-pass (10 Hz), then magnitude normalized by peak amplitude, and normalized to 101 data points30. To calculate muscle synergies, non-negative matrix factorization was used which is commonly used for examining muscle synergies during gait (refer to55 for greater detail). Simply, this algorithm calculates the weight of synergies (W) and the activation level of those synergies (H). W generates a m × n matrix with m representing the number of muscles (5 in the present study) and n is the specified number of synergies (two in the present study). H generates a n × t matrix with t representing the number of time points (101 in the present study). Variance accounted for (VAF) scores (one minus the ratio of the sum of squared errors and the total sum of squares of the EMG data) were calculated up to two synergies.
Additionally, the sample was divided into two groups, ‘low’ knee functioning and ‘high’ knee functioning. Participants were classified as ‘low’ functioning if their surgical limb knee DPR was < 40°, indicative of a stiff knee gait56 or crouch gait pattern57. Likewise, participants were classified as ‘high’ functioning if their surgical limb knee DPR was > 40° which is typically observed in healthy populations58,59.
Statistical analysis
All data were assessed for normality and mean ± standard deviation was calculated for each outcome. Paired-sample T-tests were performed comparing the surgically repaired limb to the intact limb on spatiotemporal characteristics, joint angles, mean relative phase, deviation phase, and VAF scores separately. A secondary exploratory descriptive analysis was performed to qualitatively compare the ‘high knee functioning’ versus ‘low knee functioning’ individuals within this cohort. Cohen’s d effect size was calculated with d < 0.5 represents a small effect, d = 0.51–0.79 represents a medium effect, and d ≥ 0.80 represents a large effect. Alpha set at p ≤ 0.05.
Data availability
Data is available upon reasonable request by contacting the corresponding author.
References
Gupta, S. K., Alassaf, N., Harrop, A. R. & Kiefer, G. N. Principles of rotationplasty. J. Am. Acad. Orthop. Surg. 20, 657–667. https://doi.org/10.5435/JAAOS-20-10-657 (2012).
Sakkers, R. & van Wijk, I. Amputation and rotationplasty in children with limb deficiencies: Current concepts. J. Child. Orthop. 10, 619–626. https://doi.org/10.1007/s11832-016-0788-7 (2016).
Shanmugam, S., Govindasamy, G. & Van Kumar, P. S. Ness rotationplasty as limb salvage procedure for locally advanced extremity osteosarcoma—Case report. J. Cancer Res. Ther. 13, S127–S128 (2017).
Filis, P. et al. Rotationplasty outcomes assessed by gait analysis following resection of lower extremity bone neoplasms. Bone Jt. Open 4, 817–824. https://doi.org/10.1302/2633-1462.411.BJO-2023-0101.R1 (2023).
Hopyan, S., Tan, J. W., Graham, H. K. & Torode, I. P. Function and upright time following limb salvage, amputation, and rotationplasty for pediatric sarcoma of bone. J. Pediatr. Orthop. 26, 405–408. https://doi.org/10.1097/01.bpo.0000203016.96647.43 (2006).
Kotz, R. Rotationplasty. Semin. Surg. Oncol. 13, 34–40. https://doi.org/10.1002/(sici)1098-2388(199701/02)13:1%3c34::aid-ssu6%3e3.0.co;2-5 (1997).
Akahane, T. et al. Evaluation of postoperative general quality of life for patients with osteosarcoma around the knee joint. J. Pediatr. Orthop. B. 16, 269–272. https://doi.org/10.1097/BPB.0b013e3280925670 (2007).
Marko, T. A., Diessner, B. J. & Spector, L. G. Prevalence of metastasis at diagnosis of osteosarcoma: An international comparison. Pediatr. Blood Cancer 63, 1006–1011 (2016).
Lindner, N. J. et al. Limb salvage and outcome of osteosarcoma. The university of muenster experience. Clin. Orthop. Relat. Res. 358, 83–89. https://doi.org/10.1097/00003086-199901000-00011 (1999).
Ginsburg, J. P. et al. A comparative analysis of functional outcomes in adolescents and young adults with lower-extremity bone sarcoma. Pediatr. Blood Cancer 49, 964–969 (2007).
McClenaghan, B. A., Krajbich, J. I., Pirone, A. M., Koheil, R. & Longmuir, P. Comparative assessment of gait after limb-salvage procedures. J. Bone Jt. Surg. Am. 71, 1178–1182 (1989).
Jamshidi, K., Bahrabadi, M. & Mirzaei, A. Long-term results of osteoarticular allograft reconstruction in children with distal femoral bone tumors. Arch. Bone Jt. Surg. 5, 296–301 (2016).
Hillmann, A., Weist, R., Fromme, A., Volker, K. & Rosenbaum, D. Sports activities and endurance capacity of bone tumor patients after rotationplasty. Arch. Phys. Med. Rehabil. 88, 885–890. https://doi.org/10.1016/j.apmr.2007.04.004 (2007).
Voss, V. H. Tabelle der absoluten and relativen Muskelspindelzahlen der menschlichen Skelettmuskulatur. Anat. Anz. 129, 562–572 (1971).
Tucker, K. J., Tuncer, M. & Turker, K. S. A review of the H-reflex and M-wave in the human triceps surae. Hum. Mov. Sci. 24, 667–688. https://doi.org/10.1016/j.humov.2005.09.010 (2005).
Kissane, R. W. P., Charles, J. P., Banks, R. W. & Bates, K. T. Skeletal muscle function underpins muscle spindle abundance. Proc. Biol. Sci. 289, 20220622. https://doi.org/10.1098/rspb.2022.0622 (2022).
Capaday, C. The special nature of human walking and its neural control. Trends Neurosci. 25, 370–376. https://doi.org/10.1016/s0166-2236(02)02173-2 (2002).
Ten Donkelaar, H. J., Broman, J. & van Domburg, P. In Clinical Neuroanatomy: Brain Circuitry and Its Disorders 171–255 (Springer International Publishing, 2020).
Nene, A., Mayagoitia, R. & Veltink, P. Assessment of rectus femoris function during initial swing phase. Gait Posture 9, 1–9. https://doi.org/10.1016/s0966-6362(98)00042-3 (1999).
Nene, A., Byrne, C. & Hermens, H. Is rectus femoris really a part of quadriceps? Assessment of rectus femoris function during gait in able-bodied adults. Gait Posture 20, 1–13. https://doi.org/10.1016/S0966-6362(03)00074-2 (2004).
Kepple, T. M., Siegel, K. L. & Stanhope, S. J. Relative contributions of the lower extremity joint moments to forward progression and support during gait. Gait Posture 6, 1–8 (1997).
Neptune, R. R., Kautz, S. A. & Zajac, F. E. Contributions of the individual ankle plantar flexors to support, forward progression and swing initiation during walking. J. Biomech. 34, 1387–1398. https://doi.org/10.1016/s0021-9290(01)00105-1 (2001).
Kriellaars, D. J., Brownstone, R. M., Noga, B. R. & Jordan, L. M. Mechanical entrainment of fictive locomotion in the decerebrate cat. J. Neurophysiol. 71, 2074–2086. https://doi.org/10.1152/jn.1994.71.6.2074 (1994).
Pearson, K. G. Proprioceptive regulation of locomotion. Curr. Opin. Neurobiol. 5, 786–791. https://doi.org/10.1016/0959-4388(95)80107-3 (1995).
Duysens, J., Clarac, F. & Cruse, H. Load-regulating mechanisms in gait and posture: Comparatative aspects. Physiol. Rev. 80, 83–133 (2000).
Hillmann, A. et al. Electromyographic and gait analysis of forty-three patients after rotationplasty. J. Bone. Jt. Surg. Am. 82, 187–196. https://doi.org/10.2106/00004623-200002000-00004 (2000).
Hein, T. et al. Using the variability of continuous relative phase as a measure to discriminate between healthy and injured runners. Hum. Mov. Sci. 31, 683–694 (2012).
Li, L., Van Den Bogert, E. C., Caldwill, G. E. V., Emmerik, R. E. & Hamill, J. Coordination patterns of walking and running at similar frequencies. Hum. Mov. Sci. 18, 67–85 (1999).
Hamill, J., van Emmerik, R. E., Heiderscheit, B. C. & Li, L. A dynamical systems approach to lower extremity running injuries. Clin. Biomech. 14, 297–308 (1999).
Steele, K. M., Rozumalski, A. & Schwartz, M. H. Muscle synergies and complexity of neuromuscular control during gait in cerebral palsy. Dev. Med. Child. Neurol. 57, 1176–1182. https://doi.org/10.1111/dmcn.12826 (2015).
Ting, L. H. et al. Neuromechanical principles underlying movement modularity and their implications for rehabilitation. Neuron 86, 38–54. https://doi.org/10.1016/j.neuron.2015.02.042 (2015).
Ting, L. H. & Chvatal, S. A. Decomposing Muscle Activity in Motor Tasks: Methods and Interpretation (Oxford University Press, 2010).
Catani, F. et al. Gait analysis in patients after van nes rotationplasty. Clin. Orthop. Relat. Res. 296, 270–277 (1993).
Middleton, A., Fritz, S. L. & Lusardi, M. Walking speed: The functional vital sign. J. Aging. Phys. Act. 23, 314–322. https://doi.org/10.1123/japa.2013-0236 (2015).
Price, M. A., Beckerle, P. & Sup, F. C. Design optimization in lower limb prostheses: A review. IEEE Trans. Neural. Syst. Rehabil. Eng. 27, 1574–1588. https://doi.org/10.1109/TNSRE.2019.2927094 (2019).
Campanini, I., Merlo, A. & Damiano, B. A method to differentiate the causes of stiff-knee gait in stroke patients. Gait Posture 38, 165–169. https://doi.org/10.1016/j.gaitpost.2013.05.003 (2013).
Fujita, K. et al. Differences in causes of stiff knee gait in knee extensor activity or ankle kinematics: A cross-sectional study. Gait Posture 98, 187–194. https://doi.org/10.1016/j.gaitpost.2022.09.078 (2022).
Gosgnach, S. et al. Delineating the diversity of spinal interneurons in locomotor circuits. J. Neurosci. 37, 10835–10841. https://doi.org/10.1523/JNEUROSCI.1829-17.2017 (2017).
Hohne, A., Ali, S., Stark, C. & Bruggemann, G. P. Reduced plantar cutaneous sensation modifies gait dynamics, lower-limb kinematics and muscle activity during walking. Eur. J. Appl. Physiol. 112, 3829–3838. https://doi.org/10.1007/s00421-012-2364-2 (2012).
Dietz, V., Muller, R. & Colombo, G. Locomotor activity in spinal man: Significance of afferent input from joint and load receptors. Brain 125, 2626–2634. https://doi.org/10.1093/brain/awf273 (2002).
Frigon, A. & Rossignol, S. Experiments and models of sensorimotor interaction during locomotion. Biol. Cybern. 95, 607–627 (2006).
Sutherland, D. H., Olshen, R., Cooper, L. & Woo, S. L. The development of mature gait. J. Bone Jt. Surg. Am. 62, 336–353 (1980).
Bach, M. M., Daffertshofer, A. & Dominici, N. The development of mature gait patterns in children during walking and running. Eur. J. Appl. Physiol. 121, 1073–1085. https://doi.org/10.1007/s00421-020-04592-2 (2021).
Beck, R. J., Andriacchi, T. P., Kuo, K. N., Fermier, R. W. & Galante, J. O. Changes in the gait patterns of growing children. J. Bone Jt. Surg. Am. 63, 1452–1457 (1981).
Preis, S., Klemms, A. & Muller, K. Gait analysis by measuring ground reaction forces in children: Changes to an adaptive gait pattern between the ages of one and five years. Dev. Med. Child Neurol. 39, 228–233 (1997).
Hausdorff, J. M., Zemany, L., Peng, C. & Goldberger, A. L. Maturation of gait dynamics: Stride-to-stride variability and its temporal organization in children. J. Appl. Physiol. 1985(86), 1040–1047. https://doi.org/10.1152/jappl.1999.86.3.1040 (1999).
Woods, S., O’Mahoney, C., McKiel, A., Natale, L. & Falk, B. Child-adult differences in antagonist muscle coactivation: A systematic review. J. Electromyogr. Kinesiol. 68, 102727. https://doi.org/10.1016/j.jelekin.2022.102727 (2023).
Rock, K. et al. Quantifying muscle strength, size, and neuromuscular activation in adolescent and young adult survivors of musculoskeletal sarcoma: Identifying correlates and responses to functional strengthening. Knee 40, 270–282. https://doi.org/10.1016/j.knee.2022.11.024 (2023).
Horner, M. J. et al. SEER Cancer Statistics Review 1975–2006 (National Cancer Institute, 2009).
Taran, S. J., Taran, R. & Malipatil, N. B. Pediatric osteosarcoma: An updated review. Indian J. Med. Paediatr. Oncol. 38, 33–43. https://doi.org/10.4103/0971-5851.203513 (2017).
Ottaviani, G. & Jaffe, N. The epidemiology of osteosarcoma. Cancer Treat. Res. 152, 3–13. https://doi.org/10.1007/978-1-4419-0284-9_1 (2009).
Menendez, N., Epelman, M., Shao, L., Douglas, D. & Meyers, A. B. Pediatric osteosarcoma: Pearls and pitfalls. Semin. Ultrasound CT MR 43, 97–114. https://doi.org/10.1053/j.sult.2021.05.010 (2022).
Galgon, A. K. & Shewokis, P. A. Using mean absolute relative phase, deviation phase and point-estimation relative phase to measure postural coordination in a serial reaching task. J. Sports Sci. Med. 15, 131–141 (2016).
Ghanavati, T. et al. Intra-limb coordination while walking is affected by cognitive load and walking speed. J. Biomech. 47, 2300–2305 (2014).
Lee, D. D. & Seung, H. S. Learning the parts of objects by non-negative matrix factorization. Nature 401, 788–791. https://doi.org/10.1038/44565 (1999).
Goldberg, S. R., Ounpuu, S. & Delp, S. L. The importance of swing-phase initial conditions in stiff-knee gait. J. Biomech. 36, 1111–1116. https://doi.org/10.1016/s0021-9290(03)00106-4 (2003).
Cherni, Y. et al. Lower limb extension is improved in fast walking condition in children who walk in crouch gait. Disabil. Rehabil. 41, 3210–3215. https://doi.org/10.1080/09638288.2018.1493158 (2019).
Kerrigan, D. C., Todd, M. K. & Della Croce, U. Gender differences in joint biomechanics during walking: Normative study in young adults. Am. J. Phys. Med. Rehabil. 77, 2–7. https://doi.org/10.1097/00002060-199801000-00002 (1998).
Perry, J. & Davids, J. R. Gait analysis: Normal and pathological function. J. Pediatr. Orthop. 12, 815 (1992).
Acknowledgements
This project was funded by the Colorado School of Mines/Children’s Hospital Colorado Collaboration Pilot Award.
Author information
Authors and Affiliations
Contributions
KTK processed the data, performed statistical analysis, interpreted results and wrote the manuscript. NR, MAL, and AR coordinated the investigation, assisted with data collection and edited the manuscript. JJC helped design the study, interpreted results and edited the manuscript. LAS, LM, and SK assisted with data collection/processing and edited the manuscript. DRH, SWT, PMC, edited the manuscript. AKS and NJD acquired funding, conceived/designed the study, interpreted results and edited the manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Krajewski, K.T., Rogers, N., Lundin, M.A. et al. Examining muscle synergy composition and segmental coordination during overground walking in individuals with a rotationplasty about the knee. Sci Rep 15, 26891 (2025). https://doi.org/10.1038/s41598-025-11800-6
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-11800-6
