
Abstract
To compare the clinical outcomes and radiological findings of selective facet joints and interlaminar fusion using UBE technique with percutaneous pedicle screw fixation (observation group, OG) versus open reduction fusion fixation (control group, CG) in patients with thoracolumbar compression fractures. 110 patients were included, including 56 in the OG and 54 in the CG. The clinical results were evaluated by visual analogue scale score (VAS) and the oswestry disability index score(ODI). Radiographic findings were evaluated by the sagittal cobb angle(CA), the anterior vertebral height(AVH) and the sagittal index(SI). The amount of blood loss and hospitalization days in the OG were significantly lower than those in the CG( p < 0.05). The VAS, ODI, CA, AVH, and SI scores significantly improved after operation in both groups (p < 0.05). Compared with the CG at 1 day and 1 week after operation, OG patients’ VAS score significantly improved ( p < 0.05). 1 week after operation, CA in OG was significantly higher than that in CG( p < 0.05). Selective facet joints and interlaminar fusion using UBE technique combined with percutaneous pedicle screw fixation versus open reduction fusion fixation have achieved good clinical and radiographic results for the treatment of compression thoracolumbar fractures, including improved pain and disability, corrected kyphotic deformity, restored vertebral height, and minimal complications. Additionally, with UBE technology, there is less blood loss, more early back pain relief, and shorter hospital stay.
Similar content being viewed by others

Traumatic thoracolumbar fractures are a leading cause of disability among working-age individuals in developing countries, predominantly affecting men aged 20–50, with approximately 50% of cases leading to significant medical, economic, and social consequences1,2. Type A compression fractures, accounting for 63–82% of cases, frequently occur at the thoracolumbar junction due to its biomechanical vulnerability2,3,4. Traditional surgical approaches (anterior, posterior, or combined) are associated with drawbacks such as infection risk, extensive soft tissue damage, blood loss, delayed recovery, and chronic pain5,6. Minimally invasive percutaneous pedicle screw fixation has gained popularity for reducing trauma and complications, though it may result in correction loss, particularly in severe compression fractures with endplate injury, leading to kyphosis recurrence after implant removal. Fusion therapy is recommended for such cases to mitigate correction loss. Unilateral biportal endoscopy (UBE), an emerging minimally invasive technique, has shown promise in spinal degenerative diseases by enabling precise bone graft fusion through two small incisions7,8. Its potential in spinal trauma surgery remains underexplored.
The primary goal of spinal trauma treatment is to stabilize the spine while minimizing functional loss. Strategies such as reducing fixed segments, selective fusion, timely implant removal, and minimally invasive approaches can better preserve spinal mobility9,10. This study compares clinical outcomes, radiological findings, and complications between UBE-assisted selective facet joint and interlaminar fusion with percutaneous pedicle screw fixation and traditional open reduction fusion in thoracolumbar compression fractures.
Methods
Study group
This case-control study included 120 patients treated at our hospital from January 2017 to January 2023. The observation group (OG, n = 60) underwent selective facet joint and interlaminar fusion using the UBE technique combined with percutaneous pedicle screw fixation, while the control group (CG, n = 60) received the same fusion procedure via a posterior median incision with pedicle screw fixation. Four patients in the OG and six in the CG were lost to follow-up (Fig. 1), resulting in 56 and 54 patients included in the final analysis, respectively. The minimum follow-up period was 18 months, with mean follow-up durations of 18.45 ± 0.68 months in the OG and 19.37 ± 1.70 months in the CG.This study was approved by the Ethics Committee of Chengdu Qingbaijiang District People’s Hospital (approval No. 202118), and was conducted in accordance with the Declaration of Helsinki. Written informed consent was obtained from all participants.
Inclusion criteria were: (1) fresh fractures within 12 days; (2) single-level T11–L3 compression fractures (AO/Magerl classification A1, A3, B2) with superior endplate injury or abnormal disc signals; (3) absence of neurological symptoms; (4) age 18–65 years; (5) vertebral height loss > 40%, kyphotic deformity > 20%, or posterior longitudinal ligament complex rupture; and (6) implant removal approximately one year postoperatively with at least six months of follow-up after removal. Exclusion criteria included: (1) pathological fractures due to tumors, infections, or osteoporosis; (2) fractures with > 50% spinal canal compromise and neurological symptoms; and (3) multilevel fractures (Table 1)11.

Flow chart of this study.
Surgical technique
Selective facet joints and interlaminar fusion using UBE technique combined with percutaneous pedicle screw internal fixation
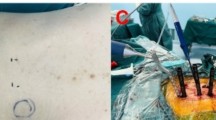
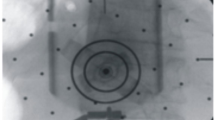
After general anesthesia, the patient was positioned prone on the operating table with limbs fixed and the abdomen suspended using silicone pads under the shoulder joints and anterior iliac spines. C-arm fluoroscopy was used to identify the articular facet joints, pedicles, and laminae of the fractured and adjacent vertebrae. The surgical area was disinfected and draped in a U-shaped manner to facilitate drainage (Fig. 2A). The lower limbs were gently pulled upward at 30 degrees, and manual pressure was applied to reduce the fracture, confirmed by C-arm imaging (Fig. 2B). Pedicle entry points were marked under fluoroscopy, and 1–1.5 cm incisions were made. Guide needles were inserted and confirmed by C-arm (Fig. 2C, D), followed by pedicle screw placement (Fig. 2E, F). Reduction and fixation were performed using instruments, with final confirmation by C-arm (Fig. 2G, H). The skin and subcutaneous tissue were incised (Fig. 2I) to expose the laminae and facet joints between the fractured and adjacent vertebrae (Fig. 2J). A high-speed drill was used to decorticate the facet joints and laminae (Fig. 2K, L), and allograft bone was placed and compacted onto the prepared surfaces (Fig. 2M). The wound was irrigated and sutured (Fig. 2N). The same procedure was repeated on the contralateral side.



Selective facet joints and interlaminar fusion using UBE technique combined with percutaneous pedicle screw internal fixation. The surgical area was U-shaped to facilitate drainage (A); C arm reconfirmation (B); The guide needle was inserted, and after the fluoroscopy of the C-arm was confirmed (C, D), the pedicle screw was inserted (E, F), and then the instrument was used for proper reduction and fixation; C arm reconfirmation (G, H); The skin and subcutaneous tissue were sequentially separated (I), exposing the laminae and facet joints (J). A high-speed drill was used to polish the facet joints and laminae (K, L); The allograft bone was placed on the polished facet joints and laminae (M); Wound irrigation and suture (N).
Selective facet joints and interlaminar fusion using open reduction internal fixation
After general anesthesia, the patient was positioned prone on the operating table with limbs fixed and the abdomen suspended using silicone pads under the shoulder joints and anterior iliac spines. C-arm fluoroscopy was used to locate the articular facet joints, pedicles, and laminae of the fractured and adjacent vertebrae. A 6–8 cm posterior median incision was made centered on the fractured vertebra (Fig. 3A, B). The skin, subcutaneous tissue, and paraspinal muscles were dissected to expose the laminae and facet joints. A positioning needle was placed along the articular process and confirmed by C-arm fluoroscopy. Pedicle screws were inserted, and instruments were used for reduction and fixation, with final confirmation by C-arm. A high-speed drill was used to decorticate the facet joints and laminae, and allograft bone was placed and compacted onto the prepared surfaces. The same procedure was performed on the contralateral side (Fig. 3C, D, E). The wound was irrigated, drained, and sutured.

Selective facet joints and interlaminar fusion using open reduction internal fixation. A posterior median incision was made centered on the fractured vertebra, about 6–8 cm long (A); C arm reconfirmation (B). The allograft bone was placed on the polished facet joints and laminae and pressed tightly (C); Final C arm reconfirmation (D, E).
Data collection and evaluation method
General data, including sex, age, injury cause, fracture classification (AO/Magerl), BMI, follow-up time, operation time, blood loss (intraoperative blood loss + 1-day postoperative drainage), and hospital stay, were recorded for both groups. Preoperative, 1-day, 1-week, 6-month postoperative, and 6-month post-implant removal VAS scores were collected. ODI scores were assessed preoperatively, 6 months postoperatively, and 6 months after implant removal. Radiological parameters, including CA (sagittal angle between the upper and lower endplates of the injured vertebra), AVH (anterior vertebral height ratio), and SI (angle between the lower endplates of the fractured and upper vertebrae), were measured preoperatively, 1 day and 6 months postoperatively, and 1 week and 6 months after implant removal. SI was adjusted based on baseline sagittal contour: thoracic level (− 5°), T12–L1 (direct measurement), and lumbar level (+ 10°)12.
Preoperative evaluation included lateral and anteroposterior X-rays, CT, and MRI. Postoperative monitoring involved dynamic X-rays or CT scans(Conduct follow-up rechecks monthly for the initial three months post-operation, and subsequently, perform rechecks every three months), with patients beginning ambulation with braces at 3 months. Internal fixation was removed approximately 12 months post-surgery after confirming fracture healing on imaging(continuous callus formation), followed by at least 6 months of monitoring.
Statistical analysis
In this study, two distinct groups were established: the observation group (OG) and the control group (CG). The independent variable serves as the grouping variable, while the dependent variable represents the outcome or observed variable. There were 56 cases in the OG and 54 cases in the CG, with a relatively small sample size.
Data analysis was performed using SPSS software, version 22.0. The associated p-values, along with skewness and kurtosis metrics, are presented in the figure (P > 0.05 was considered to indicate normality). Additionally, the results section includes the shape of the histogram and the pattern observed in the Q-Q plot(In the figure, the points are nearly on a straight line, suggesting they exhibit normality). The histograms and Q-Q plots are presented in the supplementary figures. Descriptive statistics for measurement data were expressed as mean ± standard deviation, while categorical data were presented as percentages. The Student’s t-test was employed to compare two groups when the sample data followed a normal distribution; otherwise, the the bootstrap Welch t-test was applied. If there are too many outliers, use the Yuen-Welch approach approach. The chi-square test was utilized to assess differences in frequency distributions between the two groups. For repeated measurement data, analysis of variance (ANOVA) was conducted if the data were normally distributed; otherwise, Robust ANOVA was used. A significance level of P < 0.05 was set for all statistical analyses.
Results
The study included 56 patients in the OG and 54 in the CG. Demographic data are shown in Table 1. The histograms and Q-Q plots of the age and BMI for the two groups are as follows(Supplementary Fig. 1,2).The mean age was 46.05 ± 7.10 years in the OG and 45.62 ± 6.53 years in the CG, with no significant differences in age, sex, BMI, injury cause, AO/Magerl classification, or fracture segment between groups (p > 0.05, Table 1).
Clinical outcomes are shown in Table 2. The histograms and Q-Q plots of the operation time, estimated blood loss, hospital stay, VAS score, and ODI score for the two groups are as follows (Supplementary Figs. 3–13). The OG had a significantly longer operation time than the CG (102.05 ± 9.52 vs. 64.37 ± 7.20, p < 0.05) but significantly less blood loss (103.57 ± 9.50 vs. 258.85 ± 24.05, p < 0.05) and shorter hospitalization (4.25 ± 0.83 vs. 7.55 ± 1.14 days, p < 0.05). VAS scores showed no significant differences preoperatively, 6 months postoperatively, or 6 months after implant removal (p > 0.05). However, the OG demonstrated significantly better VAS scores at 1 day (5.43 ± 0.54 vs. 7.06 ± 0.19, p < 0.05) and 1 week postoperatively (2.94 ± 0.67 vs. 4.24 ± 0.77, p < 0.05). ODI scores improved significantly in both groups postoperatively (p < 0.05), with no significant differences between groups at any time point (p > 0.05).
Radiological results are shown in Table 3. The histograms and Q-Q plots of CA, AVH and SI for the two groups are as follows (Supplementary Figs. 14–34). Both groups demonstrated significant improvements in CA, AVH, and SI postoperatively (p < 0.05), with no significant differences in the total correction index or correction loss between groups (p > 0.05). At 1 week postoperatively, CA was significantly higher in the OG than in the CG (7.19 ± 0.86 vs. 6.79 ± 0.97, p < 0.05). At 6 months post-implant removal, AVH was significantly lower in the OG than in the CG (89.98 ± 1.95 vs. 90.64 ± 1.33, p < 0.05). To better understand our research, we now present some radiological images from postoperative follow-up (Figs. 4 and 5).


This patient was treated with traditional open reduction fusion fixation. Preoperative CT showed compression fracture of the 12th thoracic vertebra with rupture of the upper endplate (A, B); The CT reexamination one day after the operation showed good reduction (C, D); The 6-month follow-up showed continuous callus formation (E, F); The 12-month follow-up showed that the fracture had healed (G, H).


This patient was treated with UBE technology-assisted fusion fixation. Preoperative DR Showed a severe vertebral fracture of lumbar 1 (A); The X-ray reexamination one day after the operation showed good reduction (B, C); The 6-month follow-up showed continuous callus formation (D, E); The 12-month follow-up showed that the fracture had basically healed (F, G).
Complications are summarized in Table 4. In the CG, four cases of superficial soft tissue infection caused by Staphylococcus aureus were successfully treated with dressing changes and oral antibiotics. In the OG, one patient with a type A3 fracture developed screw loosening at 6 months postoperatively (Fig. 6A, B); the fracture had healed on X-ray, and symptoms improved after implant removal. No instances of screw/rod breakage or nerve injury occurred in either group.

At 6 months after operation, 1 patient with type A3 fracture in the OG developed screw loosening (A, B).
Discussion
Most spinal fractures occur in the thoracolumbar region, with compression fractures being the most common13. Surgical intervention improves reduction and long-term outcomes, but traditional open surgery has significant drawbacks, including muscle stripping, substantial blood loss, denervation, ischemia, and potential long-term muscle atrophy and scarring, leading to chronic back pain and dysfunction. The posterior muscles and ligaments of the thoracolumbar region are critical for stability and should be preserved during surgery. Compared to open surgery, minimally invasive techniques provide quicker functional recovery, effective kyphotic correction, and stable fixation, aligning with orthopedic rehabilitation principles14,15,16,17,18,19. A meta-analysis by Phan et al.10 found that percutaneous fixation preserves paraspinal muscles, minimizing postoperative atrophy, and results in less blood loss, smaller incisions, lower infection rates, better pain relief, and shorter hospital stays. Additionally, VAS and ODI scores further improve after implant removal20,21,22.
Fusion therapy is recommended for patients with severe vertebral height loss (> 40%), kyphotic deformity (> 20%), posterior ligament complex rupture, disc signal abnormalities, or upper endplate injury. However, minimally invasive percutaneous fusion techniques often require additional incisions. Zhang et al.23 demonstrated that minimally invasive posterior laminofusion with auxiliary incisions effectively prevented kyphotic recurrence and implant failure in thoracolumbar fractures, though it still involved significant trauma. The UBE technique, a recent advancement in spinal endoscopy, has proven effective for lumbar degenerative diseases. It offers advantages such as minimal invasiveness, a broad and clear surgical field, ease of operation, and no need for specialized instruments, while preserving paraspinal muscles and ligaments, making it safer and more effective than traditional open or single-channel surgeries7,24,25.
The primary goal in spinal trauma treatment is to stabilize the spine while minimizing functional compromise. Strategies such as reducing fixed segments, selective fusion, timely implant removal, and minimally invasive approaches to protect ligaments and muscles can better preserve spinal motor function9,10. This study compared clinical outcomes, radiological findings, and complications between UBE-assisted selective facet joint and interlaminar fusion with percutaneous pedicle screw fixation and traditional open reduction fusion in thoracolumbar compression fractures. The UBE approach yielded favorable results, with significantly less blood loss (p < 0.05), shorter hospitalization (p < 0.05), and lower VAS scores at 1 day (p < 0.05) and 1 week postoperatively (p < 0.05), though operation time was longer (p < 0.05). No differences were observed in VAS or ODI scores at other time points. Reduced blood loss is particularly beneficial for high-risk elderly or hypovolemic patients, while minimized muscle trauma and early stabilization promote faster recovery, consistent with previous findings8,22,26,27.
Posterior 4-screw fixation is commonly used for thoracolumbar compression fractures, but long-term follow-up reveals high rates of implant failure and kyphosis, with 50% of patients experiencing moderate to severe pain. Adding pedicle screws at the fracture segment can mitigate these issues. A systematic review by Kapoen et al.28 involving 1,890 patients across 27 studies demonstrated that fracture-level screw placement improves clinical outcomes, reduces pain, and decreases implant failure rates, albeit with slightly increased blood loss and operative time. Fracture-level screws act as a thrust point to restore anterior vertebral height and prevent kyphosis, making them particularly effective for severe compression fractures29,30,31. In this study, the 6-screw configuration was used, though one patient in the OG experienced screw loosening and reduction loss with worsening back pain, which resolved after implant removal. Analysis revealed that high BMI, premature weight-bearing, and inadequate brace use were contributing factors.
Studies indicate that removing pedicle screws after fracture healing can restore spinal mobility and alleviate implant-related discomfort, further improving patient prognosis32,33. However, correction loss post-removal remains a significant challenge and appears inevitable. Aono et al.34 attributed this to intervertebral disc degeneration, while Maestretti et al.35 reported a mean correction loss of 3° in 33 type A fracture cases. Key risk factors for correction loss include disc correction failure and inadequate initial reduction36,37,38.
We recommend a selective fusion protocol using short-segment 6-screw internal fixation to stabilize fractures and restore vertebral height while preserving spinal movement. The fusion segment is determined by the extent of disc and endplate injury, often involving the upper endplate or disc of the fractured vertebra. Our study found significant improvements in CA, AVH, and SI post-operation (p < 0.05). One week post-operation, CA was higher in the open group (OG) compared to the control group (CG) (p < 0.05). However, 6 months after hardware removal, AVH was lower in the OG than in the CG (p < 0.05), suggesting open reduction may be slightly more effective than minimally invasive treatment.
There were no major complications. Four cases of superficial soft tissue infections in the CG healed with dressing changes and antibiotics. Six months post-operation, one OG patient with a type A3 fracture experienced screw loosening, but X-rays confirmed fracture healing, and back pain improved after hardware removal. No screw or rod breakage or nerve injury occurred in either group.
Some limitations exist in this study. Initially, the study implemented a case-control study, which, it should be noted, does not a randomized controlled trial, and the clinical samples utilized were relatively limited in size. The C-arm machine is utilized exclusively for intraoperative fluoroscopy. Due to the malfunction of its copying function, a mobile phone was employed to capture images. These images, taken with a mobile phone, serve solely to illustrate the surgical process and are not used for measuring CA, AVH and SI. Measurements of CA, AVH, and SI are accurately performed on a computer using data from these large X-ray or CT machines in the radiology department after the operation. Subsequently, the procedure of post-hardware removal was conducted based on patient request, thereby lacking complete randomness. The bone mineral density (BMD) is one of the most critical factors influencing both the risk of fracture and the outcome of pedicle screw fixation. For individuals over 50 years, BMD measurement should be conducted for further analysis. In the OG, 14 out of 56 people were over 50, averaging 55.14±4.89 years. In the CG, 11 out of 54 were over 50, with an average age of 54.66±4.47 years. There was not statistically significant between the two groups of people over 50 years old. Additionally, the duration of follow-up post-hardware removal was deemed insufficient, necessitating a more extensive, long-term follow-up for a comprehensive evaluation. Lastly, the study did not include a comparison of vertebra segment movement between the two groups.
Conclusion
Both selective facet joint and interlaminar fusion using UBE technique with percutaneous pedicle screw fixation and traditional open reduction fusion achieved favorable clinical and radiographic outcomes for thoracolumbar compression fractures, including pain relief, functional improvement, kyphotic correction, vertebral height restoration, and low complication rates. The UBE approach demonstrated additional advantages: reduced intraoperative blood loss, faster postoperative pain resolution, and shorter hospitalization compared to open surgery.
Data availability
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
References
Ruiz Santiago, F. et al. Classifying thoracolumbar fractures: role of quantitative imaging. Quant. Imaging Med. Surg. 6 (6), 772–784 (2016).
Aebi, M. Classification of thoracolumbar fractures and dislocations. Eur. Spine J. 19 (Suppl 1), S2–7 (2010).
Muratore, M. et al. Surgical treatment of traumatic thoracolumbar fractures: a retrospective review of 101 cases. Musculoskelet. Surg. 105 (1), 49–59 (2021).
Knop, C. et al. Posterior instrumentation and transpedicular interbody fusion. Clinical and radiological results with utilization of CT scans after implant removal. Orthopade 28 (8), 703–713 (1999).
Taylor, H. et al. The impact of self-retaining Retractors on the paraspinal muscles during posterior spinal surgery. Spine (Phila Pa. 1976). 27 (24), 2758–2762 (2002).
Xu, G. J. et al. Anterior versus posterior approach for treatment of thoracolumbar burst fractures: a meta-analysis. Eur. Spine J. 22 (10), 2176–2183 (2013).
Zheng, B., Zhang, X. L. & Li, P. Transforaminal interbody fusion using the unilateral biportal endoscopic techni Que compared with transforaminal lumbar interbody fusion for the treatment of lumbar spine diseases: analysis of clinical and radiological outcomes. Oper. Neurosurg. (Hagerstown). 24 (6), e395–e401 (2023).
Tian, D. et al. Unilateral biportal endoscopic technique combined with percutaneous transpedicular screw fixation for thoracolumbar burst fractures with neurological symptoms: technical note and preliminary report. J. Orthop. Surg. Res. 18 (1), 584 (2023).
Pesenti, S. et al. Minimal invasive circumferential management of thoracolumbar spine fractures. Biomed. Res. Int. 2015, 639542 (2015).
Phan, K., Rao, P. J. & Mobbs, R. J. Percutaneous versus open pedicle screw fixation for treatment of thoracolumbar fractures: systematic review and meta-analysis of comparative studies. Clin. Neurol. Neurosurg. 135, 85–92 (2015).
Zheng, X. et al. Treatment of thoracolumbar fractures by temporary posterior instrumentation with selective fusion schemes. Br. J. Neurosurg. 38(4), 817–824 (2024).
Farcy, J. P., Weidenbaum, M. & Glassman, S. D. Sagittal index in management of thoracolumbar burst fractures. Spine (Phila Pa. 1976). 15 (9), 958–965 (1990).
Shim, J. H. & Seo, E. M. Efficacy and radiographic analysis of minimally invasive posterior Mono-Axial pedicle screw fixation in treating thoracolumbar burst fractures. J. Clin. Med. 11 (3), 516 (2022).
Jiang, F. et al. The Mini-Open Wiltse approach with pedicle screw fixation versus percutaneous pedicle screw fixation for treatment of neurologically intact thoracolumbar fractures: A systematic review and Meta-Analysis. World Neurosurg. 164, 310–322 (2022).
Hayoun, T. et al. Treatment of thoracolumbar fractures: comparison of the clinical and radiological outcomes of percutaneous versus open surgery. Eur. J. Orthop. Surg. Traumatol. 33 (6), 2393–2397 (2023).
Ricciardi, G. A. et al. Minimally invasive surgery for traumatic thoracolumbar fractures: A Cross-Sectional study of spine surgeons. World Neurosurg. 180, e706–e715 (2023).
Kawaguchi, Y., Matsui, H. & Tsuji, H. Back muscle injury after posterior lumbar spine surgery. A histologic and enzymatic analysis. Spine (Phila Pa. 1976). 21 (8), 941–944 (1996).
Saravi, B. et al. One-Year clinical outcomes of Minimal-Invasive dorsal percutaneous fixation of thoracolumbar spine fractures. Med. (Kaunas). 58 (5), 606 (2022).
Hashmi, S. M. M. et al. Outcome of percutaneous pedicle screw fixation for traumatic thoracic and lumbar fractures -six years experience. Br. J. Neurosurg. 38(6), 1367–1373 (2024).
Fuentes, S. et al. Percutaneous kyphoplasty and pedicle screw fixation for the management of thoraco-lumbar burst fractures. Eur. Spine J. 19 (8), 1281–1287 (2010).
Proietti, L. et al. Posterior percutaneous reduction and fixation of thoraco-lumbar burst fractures. Orthop. Traumatol. Surg. Res. 100 (5), 455–460 (2014).
Chen, L. et al. Minimally invasive decompression and intracorporeal bone grafting combined with temporary percutaneous Short-Segment pedicle screw fixation for treatment of thoracolumbar burst fracture with neurological deficits. World Neurosurg. 135, e209–e220 (2020).
Zhang, W. et al. Minimally invasive posterior decompression combined with percutaneous pedicle screw fixation for the treatment of thoracolumbar fractures with neurological deficits: A prospective randomized study versus traditional open posterior surgery. Spine (Phila Pa. 1976). 41 (Suppl 19), B23–B29 (2016).
Choi, C. M. Biportal endoscopic spine surgery (BESS): considering merits and pitfalls. J. Spine Surg. 6 (2), 457–465 (2020).
Jiang, H. W. et al. Unilateral biportal endoscopic discectomy versus percutaneous endoscopic lumbar discectomy in the treatment of lumbar disc herniation: a retrospective study. J. Orthop. Surg. Res. 17 (1), 30 (2022).
Nourian, S. M. A. et al. Evaluation of postoperative bracing on unstable traumatic lumbar fractures after pedicle screw fixation. Int. J. Burns Trauma. 12 (4), 168–174 (2022).
Mobbs, R. J., Sivabalan, P. & Li, J. Technique, challenges and indications for percutaneous pedicle screw fixation. J. Clin. Neurosci. 18 (6), 741–749 (2011).
Kapoen, C. et al. Pedicle screw fixation of thoracolumbar fractures: conventional short segment versus short segment with intermediate screws at the fracture level-a systematic review and meta-analysis. Eur. Spine J. 29 (10), 2491–2504 (2020).
Dick, J. C. et al. A Biomechanical comparison evaluating the use of intermediate screws and cross-linkage in lumbar pedicle fixation. J. Spinal Disord. 7 (5), 402–407 (1994).
Guven, O. et al. The use of screw at the fracture level in the treatment of thoracolumbar burst fractures. J. Spinal Disord Tech. 22 (6), 417–421 (2009).
Agrawal, H. et al. Long-segment fixation versus short-segment fixation with instrumentation of index vertebra for thoracolumbar fractures. Surg. Neurol. Int. 13, 233 (2022).
Visagan, R. et al. Removal or retention of minimally invasive screws in thoracolumbar fractures? Systematic review and case-control study. Acta Neurochir. (Wien). 165 (4), 885–895 (2023).
Finoco, M. et al. Implant removal after short percutaneous pedicle fixation associated with SpineJack® kyphoplasty: is correction sustained? Arch. Orthop. Trauma. Surg. 143 (7), 4239–4247 (2023).
Aono, H. et al. Temporary short-segment pedicle screw fixation for thoracolumbar burst fractures: comparative study with or without vertebroplasty. Spine J. 17 (8), 1113–1119 (2017).
Maestretti, G. et al. Prospective study of standalone balloon kyphoplasty with calcium phosphate cement augmentation in traumatic fractures. Eur. Spine J. 16 (5), 601–610 (2007).
Aono, H. et al. Risk factors for a kyphosis recurrence after short-segment temporary posterior fixation for thoracolumbar burst fractures. J. Clin. Neurosci. 66, 138–143 (2019).
Xu, B. S., Tang, T. S. & Yang, H. L. Long-term results of thoracolumbar and lumbar burst fractures after short-segment pedicle instrumentation, with special reference to implant failure and correction loss. Orthop. Surg. 1 (2), 85–93 (2009).
Lee, K. Y. et al. The relationship between superior Disc-Endplate complex injury and correction loss in young adult patients with thoracolumbar stable burst fracture. Clin. Orthop. Surg. 9 (4), 465–471 (2017).
Author information
Authors and Affiliations
Contributions
BZ and HZ B performed the operation. BZ and XL Z were major contributors in writing the manuscript. BZ and ZX L helped in completing operation and collection of the data. BZ and HZ analyzed the data and helped in revision of the paper. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Zheng, B., Li, P., Zhang, XL. et al. Selective facet joint and interlaminar fusion using unilateral biportal endoscopy for thoracolumbar compression fractures: a comparative study. Sci Rep 15, 27322 (2025). https://doi.org/10.1038/s41598-025-13326-3
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-025-13326-3
