
Abstract
Extracorporeal cardiopulmonary resuscitation (ECPR) is an effective treatment for cardiac arrest (CA). Percutaneous left ventricular (LV) assist devices such as the Impella ECP (intravascular CPR [ICPR]) have been proposed as a less invasive alternative. The aim of this study was to explore the haemodynamic differences between ECPR and ICPR using a large animal model of electrically induced CA. Fourteen juvenile female German landrace pigs (72.4 ± 9.8 kg) were subjected to electrically induced CA for 5 mins followed by either ECPR (veno-arterial extracorporeal membrane oxygenation [VA-ECMO]) or ICPR (Impella ECP). Haemodynamic parameters and echocardiographic ventricular function indicators were monitored. Mechanical circulatory support (MCS) was continued until five hours after the return of spontaneous circulation (ROSC), when the devices were removed. Resuscitation outcomes and the haemodynamic effects of ECPR and ICPR were compared. The cannulation time for ECMO (469 ± 129 s) was significantly longer than the time for Impella device implantation (153 ± 64 s, p < 0.001). ECPR facilitated ROSC in 6/6 animals, whereas ICPR facilitated ROSC in 6/8 animals (p = 0.19). Echocardiography revealed no difference in LV or right ventricular (RV) dysfunction between the ECPR- and ICPR-treated animals after resuscitation (LV-global longitudinal strain [GLS] 3 h post-ROSC: ICPR: − 16.5 ± 5.6% vs. ECPR: − 13.7 ± 5.9%, p = 0.99; RV-GLS 3 h post-ROSC: ICPR: − 15.9 ± 3.3% vs. ECPR: − 17.3 ± 10.6%, p = 0.99). MCS using VA-ECMO and the Impella device both provided effective haemodynamic support during CA and post-ROSC in this large animal model. Despite LV unloading conferring a hypothetical advantage for ICPR, no significant differences in myocardial recovery were observed.
Similar content being viewed by others


Introduction
Extracorporeal cardiopulmonary resuscitation (ECPR), i.e., mechanical circulatory support (MCS) using veno-arterial extracorporeal membrane oxygenation (VA-ECMO), during cardiac arrest (CA) has successfully been implemented in the clinical practice of cardiopulmonary resuscitation (CPR)1,2. Recent studies have indicated that ECPR in comparison to conventional chest compressions may result in superior survival rates and a more favourable neurologic outcome in selected patients3,4. In addition to the rise of ECPR, percutaneous left ventricular assist devices (pLVADs) have been proposed as an option for MCS during resuscitation (intravascular CPR [ICPR]) instead of chest compressions, with promising results5,6,7,8,9.
In principle, ICPR could offer several advantages over ECPR due to its distinct mode of operation: the direction of physiological blood flow generated by transaortic pLVADs leads to left ventricular (LV) unloading and antegrade blood flow in the ascending aorta. In contrast, peripheral cannulated ECMO generates retrograde, non-physiological blood flow in the aorta, increasing LV afterload and ventricular work10. After the return of spontaneous circulation (ROSC), the function of the myocardium is often severely impaired11,12. VA-ECMO can negatively affect LV function through ECMO-generated afterload, which may further restrict LV function and hinder recovery. Furthermore, ECPR requires at least two large-bore vascular cannulas, increasing the risk of severe complications such as limb ischaemia or major bleeding13. On the other hand, ICPR requires a single vascular access point with a smaller diameter, potentially reducing the vascular access time and complication rate. However, a noteworthy limitation of ICPR is its inability to generate an active right ventricular (RV) output. Consequently, systemic perfusion during ICPR depends on Fontan-like passive pulmonary circulation, which enables LV filling. Therefore, the aim of our study was to explore the differences in resuscitation and post-resuscitation haemodynamics between ECPR and ICPR, utilizing a well-established large animal model of electrically induced CA5,14,15,16.
Methods
This trial was conducted in 14 juvenile female German landrace pigs. Eight swine were resuscitated using a pLVAD (expandable Impella CP [Impella ECP], Abiomed Europe GmbH, Aachen, Germany) (74.2 ± 6.7 kg), and six were resuscitated using VA-ECMO (70.0 ± 13.3 kg). The Impella ECP pLVAD is a novel, self-expandable microaxial pump. The procedural methodology for device implantation has been presented in a separate publication17. The experimental design received approval from the responsible governmental institution (approval no. 84-02.04.2017.A300; North Rhine-Westphalia Office of Nature, Environment and Consumer Protection, LANUV NRW). The experiments comply with the ARRIVE guidelines and were carried out in adherence to the EU Directive 2010/63/EU for animal experiments.
Preparation
After sedation with intramuscular 6 mg/kg azaperone (Stresnil, Janssen-Cilag GmbH, Neuss, Germany), the animals underwent ear vein cannulation, and narcosis was induced (2 mg/kg propofol, propofol 1% MCT, Fresenius Kabi Austria GmbH, Graz, Austria; 5 µg/kg fentanyl, Fentanyl-Jannsen, Janssen-Cilag GmbH). Anaesthesia was maintained throughout the whole experiment by propofol (5 mg/kg/h) and fentanyl (5 µg/kg/h), accompanied by Ringer’s solution at an infusion rate of 4 mL/kg/h. Mechanical ventilation (Cato, Dräger, Lübeck, Germany) via an endotracheal tube (inspired oxygen fraction, 0.3; tidal volume, 10 mL/kg; positive end-expiratory pressure, 5 cmH2O) was implemented. We adapted the respiratory frequency to preserve physiologic end-tidal carbon dioxide levels (35–40 mmHg). Body temperature was maintained at 38.2 ± 0.2 °C using convective heating (Warm Touch 5300A, Covidien, Dublin, Ireland).
A venous sheath (9F percutaneous sheath introducer set, Arrow, Reading, PA, USA) in the right femoral vein was used to advance a hexalumen Swan-Ganz catheter (744HF75, Edwards Lifesciences, Irvine, CA, USA) connected to a Vigilance VGS2 monitor (Edward Lifesciences) into the pulmonary artery. A 4F arterial catheter (arterial leadercath; Vygon, Ecquen, France) was inserted into the right femoral artery. Subsequently, 100 IU/kg heparin (B. Braun, Melsungen, Germany) was administered. Defibrillation electrodes (QUIK-COMBO, Physio-Control, Redmond, WA, USA) were attached to the animals and linked to a defibrillator (Lifepak 12, Medtronic, Minneapolis, MN, USA). Depending on the experimental group, the animals received either ICPR or ECPR for MCS during and after resuscitation (Fig. 1), as described below.

Illustration of the experimental setup. (A) Animals were prepared as illustrated here and received either resuscitation by an Impella pLVAD (ICPR) or veno-arterial ECMO (ECPR). (B) The flowchart visualizes the individual steps of the experiment: after completion of the preparation, the animals were exposed to electrically induced cardiac arrest for 5 min via the induction of ventricular fibrillation (VF). Depending on the treatment group, Impella (ICPR) or veno-arterial ECMO (ECPR) was then used for resuscitation. After the return of spontaneous circulation (ROSC), the animals were observed for 5 h until the devices were stopped, and the animals were sacrificed 6 h post-ROSC. Echocardiography was performed at the indicated time points during the experiment. CPR cardiopulmonary resuscitation; ECMO extracorporeal membrane oxygenation; pLVAD percutaneous left ventricular assist device; ROSC return of spontaneous circulation; VF ventricular fibrillation (created with BioRender.com).
ICPR (Impella ECP): A 10F introducer sheath (10F Introducer Avanti; Cordis, Miami Lakes, FL, USA) was used in the left femoral artery, and a 9F sheath was used in the right jugular vein.
ECPR (VA-ECMO): A 19F ECMO cannula (Venous HLS Cannula PVS 1938, Maquet Cardiopulmonary GmbH, Rastatt, Germany) in the right jugular vein, a 17F ECMO cannula (Arterial HLS Cannula PAS 1715, Maquet) in the left femoral artery, and a 9F sheath in the left jugular vein were used. The ECMO cannulas were flushed and connected to the ECMO circuit (Maquet Cardiohelp, Intervention set BIOLINE COATING standard, Maquet). The oxygenator was connected to a heat exchanger set to 38.2 °C The ECMO cannulas remained clamped during preparation. We measured the cannulation time i.e. the time from the needle entering the skin for arterial or venous puncture until final sheath or cannula placement for both experimental groups.
Experimental protocol
Following an equilibration period, the animals received a second injection of 100 IU/kg heparin. After electric induction of ventricular fibrillation (VF), ventilation and fluid administration were ceased. The CA remained untreated for 5 min. Resuscitation was then initiated by ventilation with 100% oxygen and the administration of Ringer’s solution at a rate of 200 mL/min. To ensure comparable no-flow times in the ICPR and ECPR groups, a non-randomized approach was employed, and ICPR experiments were performed first. After 5 min of untreated CA, the Impella ECP device was introduced via the previously placed femoral introducer sheath, and resuscitation was performed. The experiments in the ECPR group were subsequently conducted with the initiation of VA-ECMO after a total of 6 min of CA to achieve comparable no-flow times to those in the ICPR group. No animals in either group received chest compressions. MCS was initiated according to the respective treatment protocol for ICPR or ECPR:
ICPR: Immediately after fluoroscopic guided placement, the Impella device was activated with the maximum achievable flow. Norepinephrine (Arterenol; Sanofi, Frankfurt, Germany) (1 mg) was administered. An electric shock (360J, biphasic) was administered after 2 min of MCS and repeated every 2 mins if unsuccessful. If VF persisted after the second shock, another dose of norepinephrine was administered, and resuscitation was continued for another 2 min until the next shock. This protocol was continued until either 10 min of CPR had elapsed or ROSC was achieved. When ROSC was observed the ventilator settings from the preparation phase were resumed and fluid administration was limited to 4 mL/kg/h. No vasopressors were administered after ROSC. The animals were monitored for another five hours, when the Impella device was removed. Following observation for one hour after device removal, the animals were sacrificed by an intravenous administration of pentobarbital.
ECPR: ECMO treatment was initiated 60 s after the start of resuscitation to synchronize the ischaemia time with that in the ICPR group. Then, the cannula clamps were released, and VA-ECMO was initiated (FiO2 = 1.0; 1 L/min sweep gas flow; 3 L/min targeted blood flow). Vasopressor treatment and defibrillation were conducted using the same protocol as that used in the ICPR group. Following ROSC, the ECMO flow was reduced to a targeted blood flow of 2.5 L/min, the sweep gas flow FiO2 was reduced to 0.5, and the ventilator the ventilator settings from the preparation phase were resumed. No vasopressors were administered after ROSC. ECMO weaning and cannula clamping were conducted 5 h after ROSC. The animals were observed for another hour without ECMO support before the animals were euthanized by an intravenous administration of pentobarbital.
Measurements
A small subxiphoidal access point was prepared for repeated echocardiographic examinations. Echocardiography was conducted using a transthoracic ultrasound probe (4Vc-D, GE Healthcare Chicago, IL, USA) attached to a GE Vivid E9 system (GE Healthcare). Echocardiography was carried out at the following time points: baseline; 30 min post-ROSC; and 3 h, 5 h and 6 h post-ROSC. Body surface area (BSA) indexed values were calculated using the following formula for BSA estimation: BSA = 0.0734 × bodyweight0.65618
Continuous monitoring via electrocardiogram (ECG), pulse oximetry and cerebral oximetry-near-infrared spectroscopy (NIRS) (INVOS 5100c cerebral oximeter; INVOS cerebral oximetry adult sensors, Medtronic, Dublin, Ireland) was conducted throughout the experiment. Femoral, pulmonary arterial and central venous pressures were monitored throughout the study (LabVIEW 2010, National Instruments, Austin, TX, USA; RedLab 1616HS-BNC, Meilhaus Electronic, Puchheim, Germany). The coronary perfusion pressure (CPP) was estimated by subtracting the mid-diastolic right atrial pressure from the mid-diastolic femoral pressure19. Owing to the lack of pulsatility in the blood pressure signal of the non-contracting ventricle during resuscitation, we used the mean right atrial pressure and the mean femoral pressure for this measurement. Arterial and mixed venous blood samples were drawn at baseline, 10 min and 30 min after ROSC, and every hour thereafter for blood gas analysis (ABL 700, Radiometer, Copenhagen, Denmark) and the collection of serum samples. Blood count analysis was performed at baseline and 6 h after ROSC (Celltac-alpha VET MEK-6550 K, Nihon Koden, Rosbach, Germany). Alanine transaminase (ALT), aspartate transaminase (AST), albumin, creatinine, creatine kinase (CK), and creatine kinase-MB (CK-MB) levels were measured in sera (Laboratory of Hematology at the Institute of Laboratory Animal Science and Experimental Surgery, RWTH Aachen University, Faculty of Medicine, Aachen, Germany). S100B and myoglobin levels were analysed using commercially available ELISA kits (porcine S100B (MBS2501779) and porcine myoglobin (MBS9425685), Biotrend, Cologne, Germany).
Statistical analysis
GraphPad PRISM 9 (GraphPad Software, San Diego, CA, USA) was used for statistical analysis and graphical presentation of the data. The data are presented as the means ± standard deviations (SDs) unless otherwise stated. The normality of the data distribution was assessed using diagnostic plots and the Kolmogorov‒Smirnov test. Two-way analysis of variance (ANOVA) or a mixed model with Greenhouse–Geisser correction followed by Sidak’s test for multiple comparisons was applied for continuous variables. A t test was used for comparisons of two values. Categorical variables were analysed using the chi2 test. The null hypothesis was rejected at p < 0.05 (*p < 0.05, **p < 0.01, ***p < 0.001).
Results
No relevant differences in weight, haemodynamic parameters, blood gas results or serum indicator levels were observed at baseline between the animals in the ICPR group and those in the ECPR group. Echocardiography confirmed that ventricular function was comparable between the experimental groups.
Preparation of the animals for the experiment was performed without any complications, and CA was successfully induced electrically in all the animals. The cannulation time for the arterial and venous ECMO cannulas (469 ± 129 s) was significantly longer than that for the single arterial pLVAD introducer (153 ± 64 s) (p < 0.001). Since ECMO cannulation and pLVAD introducer placement were performed before the induction of CA while the heart was beating, the duration did not impact resuscitation outcomes. The implantation time for the Impella ECP device via the previously placed femoral introducer sheath was 58 ± 31 s. Therefore, ECMO was initiated 60 s after the start of CPR to achieve a comparable no-flow time in both groups.
MCS during resuscitation
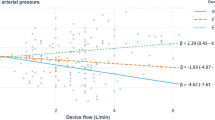
Within the first 3 mins of CA, the mean arterial pressure (MAP), central venous pressure (CVP) and pulmonary arterial pressure (PAP) equalized (Fig. 2), and the calculated CPP decreased to < 1 mmHg. After the initiation of MCS and vasopressor administration, the MAP and calculated CPP increased similarly in both groups (p > 0.99 until 4 min after the intervention started). Although the ECMO flow was greater than the pLVAD flow at the beginning of MCS (Fig. 2B), neither the MAP nor the calculated CPP was significantly greater in the ECMO group (Fig. 2B,C). No difference in cerebral oxygenation measured by NIRS was observed during resuscitation between the two groups (Fig. 2D).

Resuscitation data of 8 swine treated with Impella ECP and 6 swine treated with veno-arterial ECMO. (A) Percentage of subjects with ROSC over time. (B) Mean arterial blood pressure and Impella/ECMO device flow. (C) Calculated coronary perfusion pressure. (D) Cerebral oxygenation. The data are presented as the means ± standard errors of the means. BL baseline; ECMO extracorporeal membrane oxygenation; MAP mean arterial pressure; ROSC return of spontaneous circulation.
75% of the animals supported by Impella ECP achieved ROSC (6/8), whereas all animals resuscitated with ECMO exhibited ROSC (6/6) (survival, ICPR vs. ECPR, p = 0.186) (Fig. 2A). In one unsuccessfully resuscitated ICPR animal, Impella ECP damage during insertion led to inadequate device flow; in the other unsuccessfully resuscitated ICPR animal, ROSC was not established within 10 min of resuscitation. ECPR required less vasopressors during resuscitation (ICPR vs. ECPR: 1.8 ± 0.4 vs. 1.0 ± 0 mg norepinephrine, p = 0.015) and demonstrated a trend towards the need for fewer defibrillations (3.5 ± 2.0 vs. 2.2 ± 0.4, p = 0.136).
MCS after ROSC
After ROSC, the animals in both groups stabilized without the use of vasopressors. Temporal tachycardia, mild arterial hypotension and lactatemia were observed in the animals in both treatment groups (Fig. 3A,B; Table 1). Cerebral oxygenation mildly decreased 30 min post-ROSC, which was associated with mild hypotension (Fig. 3A,C). The Swan Ganz catheter-derived cardiac index (CI) of the pulmonary circulation was greater in the ICPR group (ICPR vs. ECPR PR 10:5.5 ± 0.8 L/min vs. 4.9 ± 0.6 L/min, p = 0.03; PR 300:4.1 ± 0.4 L/min vs. 2.9 ± 0.4 L/min, p = 0.003). The flow generated by VA-ECMO was added to the pulmonary CI to estimate the systemic CI, and no differences were observed between the two treatment groups (Fig. 3D). Haemodynamics and blood gas values were stable in both groups after termination of MCS 5 h post ROSC. Echocardiography revealed a similar restriction of LV and RV systolic function after ROSC in both groups (Fig. 4A,B, Table 2; LV-global longitudinal strain [GLS] 3 h post-ROSC ICPR: -16.5 ± 5.6% vs. ECPR: − 13.7 ± 5.9%, p = 0.99; RV-GLS 3 h post-ROSC ICPR: − 15.9 ± 3.3% vs. ECPR: − 17.3 ± 10.6%, p = 0.99), which recovered during the observation period. No relevant differences were observed in the parameters of diastolic dysfunction (Fig. 4C,D). Together with native cardiac output, both treatments generated sufficient systemic perfusion, resulting in adequate lactate clearance and haemodynamic stabilization (Table 1). Lactate levels returned to baseline within 4 h post-ROSC in both groups (p > 0.99). ALT, creatinine, CK and CK-MB levels were not different between the ICPR and ECPR groups (Table 3). However, AST levels increased post ROSC in the ICPR group (10 min post-ROSC ICPR vs. ECPR: p = 0.028; Table 3). S100B and myoglobin levels did not differ substantially between ICPR and ECPR groups (S100B p = 0.27; myoglobin p = 0.19).

Post-resuscitation data of swine supported either by the Impella ECP (n = 6) or veno-arterial ECMO (n = 6). (A) Mean arterial blood pressure. (B) Lactate. (C) Cerebral tissue oxygenation. (D) Cardiac index measured by pulmonary thermodilution (CI in the ECMO group containing the ECMO device flow). The data are presented as the means ± standard errors of the means. BL baseline, ECMO extracorporeal membrane oxygenation.

Echocardiographic parameters of 8 swine treated with Impella ECP and 6 swine treated with veno-arterial ECMO. (A) Left-ventricular global longitudinal strain. (B) Right-ventricular global longitudinal strain. (C) E/A ratio. (D) E/e’ ratio. The data are presented as the means ± standard errors of the means. BL baseline, ECMO extracorporeal membrane oxygenation, GLS global longitudinal strain, LV left ventricle, RV right ventricle.
All successfully resuscitated animals (12/12) survived until the end of the experiment. No ischaemic complication or bleeding caused by vascular access was observed in the ICPR group. In the ECPR group, limb ischaemia was detected in 1 of 6 animals.
Discussion
This exploratory animal study aimed to compare the effects of MCS by pLVAD and peripheral VA-ECMO during CA and in the post-resuscitation period. Although VA-ECMO is clinically used for resuscitation, there is clearly a need for additional research and refinement of this highly invasive technology. In this study, both therapeutic options successfully facilitated ROSC after defibrillation and provided adequate haemodynamic stabilization after ROSC without the use of catecholamines, ultimately resulting in successful weaning from MCS in all resuscitated subjects.
The effectiveness of MCS during CA has been demonstrated for both transvalvular microaxial pumps5,8,9,20,21 and peripheral VA-ECMO22,23. While ECPR has gained acceptance in clinical practice24, the utilization of pLVADs is rare and is based on the individual decisions of attending physicians. From a mechanistic perspective, the two mechanical circulatory devices differ in the direction of the generated blood flow, and there is a possibility of additional oxygenation, decarboxylation and temperature control when ECMO is employed. Both devices induce a non-pulsatile flow that is influenced by the remaining cardiac activity and the degree of mechanical support. However, ICPR involves blood withdrawal from the LV and anterograde delivery to the ascending aorta after passive passage through the pulmonary circulation. The passive pulmonary blood circulation is known to limit the maximum achievable blood flow of the Impella device. In a previous study by our group, the maximum Impella flow during resuscitation could be increased by the application of inhaled nitric oxide, a pulmonary vasodilator6. Lotun et al. and Gottula et al. reported greater achievable pLVAD flows and greater CPPs when pLVADs were combined with manual chest compressions than when pLVADs were used alone25,26. This finding is consistent with observations from this study, in which ECMO was able to generate a greater blood flow during resuscitation, although the Impella ECP device utilized can theoretically generate equally high flow rates with optimal LV filling. Packer et al. compared an LV Impella device with a biventricular Impella device during CA. They reported a greater pLVAD flow during biventricular support but a lower LV myocardial perfusion pressure and lower ROSC rates than those of the LV Impella device alone27. Although blood withdrawal from the LV by the Impella device has been shown to increase CPP28, which should facilitate the likelihood of successful defibrillation, our study did not show a favourable outcome regarding the probability of successful defibrillation in the ICPR group.
ECMO support requires two vascular cannulas, necessitating a longer cannulation time than that required for the single vascular access point for ICPR. In our study, placement of the pLVAD took approximately 2.5 min, whereas the placement of both ECMO cannulas took almost 8 min (p < 0.001). The effect of the longer ECMO cannulation time on the resuscitation outcome was excluded in this study since cannulation was performed before CA was induced. However, in a clinical scenario, a longer cannulation time would be associated with a longer low-flow state, most likely translating into an adverse resuscitation outcome. In addition, outside of a controlled experimental setting, a high rate of vascular complications can likely be expected during cannulation in an emergency. Reliable data on vascular complications such as bleeding, dissection or limb ischaemia for implantation of both devices during CA are currently lacking. When used during cardiogenic shock, vascular complications occur in 39.5% of patients with ECMO and 16.7% of patients with the Impella device (p = 0.001)13,29. In our study, no bleeding occurred during cannulation, but limb ischaemia was observed in one of the ECPR animals.
After ROSC, the haemodynamic characteristics of the devices change: systemic perfusion is no longer solely dependent on the output of the mechanical devices but rather enhanced by them. In cases where CA is triggered by a myocardial infarction, LV unloading before reperfusion may reduce the extent of the myocardial scar30,31,32,33, a benefit that is not achievable with ECMO34. In comparison, ECMO can increase LV afterload, leading to increased myocardial work and oxygen consumption35,36. In contrast, the Impella device reduces LV wall tension, thereby diminishing microvascular resistance and enhancing myocardial perfusion28,37. Consequently, quicker recovery of LV function could be expected in Impella-treated animals. However, we did not observe any significant difference in LV echocardiographic function or pulmonary capillary wedge pressure (PCWP) between the two treatment groups post-ROSC, indicating that there were only minor differences in myocardial dysfunction36,38. This lack of disparity may be attributed to the relatively short absolute ischaemia time of less than 10 min and the utilization of young and healthy animals. This result would also explain why patients present more frequently with cardiogenic shock after ECPR, a situation that can be resolved by using an LV Impella in addition to ECMO39,40,41.
Several limitations should be considered when interpreting the findings of this trial. First, out-of-hospital CA tends to occur in elderly individuals with pre-existing conditions such as coronary artery disease or heart failure. In contrast, the animals in this study were young and free from preexisting conditions. However, replicating the complexity of preexisting conditions in an animal model is inherently challenging. Second, we chose to deviate from a randomized approach for the study design because of the need for comparable ischaemia times for both treatment groups. We contend that a randomized experimental design with unequal ischaemia times in both groups would have led to a significant bias regarding the comparability of the haemodynamic effects. Longer no-flow times lead to a reduction on the CPP and the ROSC rates. Both the arterial sheath for the pLVAD and the ECMO cannulas were implanted prior to the induction of CA. In this respect, our approach differs from the clinical setting, limiting its direct transferability. Furthermore, in a clinical setting chest compressions would have been performed before MCS was inducted, that were not part of our study protocol. Finally, our study does not offer insights into neurological outcomes after resuscitation. Owing to the haemodynamic focus of the study, the experimental protocol involved only a short period of untreated global ischaemia of approximately 5 min. Cerebral sequelae were expected to be relatively minor in both groups, leading to challenges in detecting clinically relevant differences. Therefore, we refrained from conducting a final neurological examination of the animals without anaesthesia.
Conclusions
This experimental study compared the effects of LV Impella- and VA-ECMO-based MCS during cardiopulmonary resuscitation and subsequent ROSC. Both the Impella device and VA-ECMO generated adequate perfusion pressure during resuscitation, facilitating ROSC. Post-ROSC, both devices provided sufficient circulatory support, and all resuscitated animals survived until the end of the study. No significant hemodynamic differences were detected between the treatments. More research is needed to determine whether there are indications where patients may benefit from one of these devices rather than the other.
Data availability
The authors declare that they have full control of all primary data, and they agree to allow the journal to review their data if requested. The dataset is available from the corresponding author on reasonable request.
Abbreviations
- ALT:
-
Alanine transaminase
- AST:
-
Aspartate transaminase
- BSA:
-
Body surface area
- CA:
-
Cardiac arrest
- CI:
-
Cardiac index
- CK:
-
Creatine kinase
- CPP:
-
Coronary perfusion pressure
- CVP:
-
Central venous pressure
- ECG:
-
Electrocardiogram
- ECPR:
-
Extracorporeal cardiopulmonary resuscitation
- GLS:
-
Global longitudinal strain
- ICPR:
-
Intravascular cardiopulmonary resuscitation
- LV:
-
Left ventricle
- MAP:
-
Mean arterial pressure
- MCS:
-
Mechanical circulatory support
- NIRS:
-
Near-infrared spectroscopy
- PAP:
-
Pulmonary arterial pressure
- pLVAD:
-
Percutaneous left ventricular assist device
- ROSC:
-
Return of spontaneous circulation
- RV:
-
Right ventricle
- SD:
-
Standard deviation
- VA-ECMO:
-
Veno-arterial extracorporeal membrane oxygenation
- VF:
-
Ventricular fibrillation
References
Rao, P. et al. Venoarterial extracorporeal membrane oxygenation for cardiogenic shock and cardiac arrest. Circ. Heart Fail. 11(9), e004905 (2018).
Abrams, D., Combes, A. & Brodie, D. Extracorporeal membrane oxygenation in cardiopulmonary disease in adults. J. Am. Coll. Cardiol. 63(25), 2769–2778 (2014).
Yannopoulos, D. et al. Advanced reperfusion strategies for patients with out-of-hospital cardiac arrest and refractory ventricular fibrillation (ARREST): A phase 2, single centre, open-label, randomised controlled trial. Lancet 396(10265), 1807–1816 (2020).
Chen, Y. S. et al. Cardiopulmonary resuscitation with assisted extracorporeal life-support versus conventional cardiopulmonary resuscitation in adults with in-hospital cardiac arrest: An observational study and propensity analysis. Lancet 372(9638), 554–561 (2008).
Derwall, M. et al. Doubling survival and improving clinical outcomes using a left ventricular assist device instead of chest compressions for resuscitation after prolonged cardiac arrest: A large animal study. Crit. Care 19, 123 (2015).
Derwall, M. et al. Inhaled nitric oxide improves transpulmonary blood flow and clinical outcomes after prolonged cardiac arrest: a large animal study. Crit. Care 19, 328 (2015).
Davidsen, C. et al. Impella use in acute myocardial infarction complicated by cardiogenic shock and cardiac arrest: Analysis of 10 years registry data. Resuscitation 140, 178–184 (2019).
Kamran, H. et al. Outcomes of Impella CP insertion during cardiac arrest: A single center experience. Resuscitation 147, 53–56 (2020).
Panagides, V. et al. Impella CP implantation during cardiopulmonary resuscitation for cardiac arrest: A multicenter experience. J. Clin. Med. 10(2), 339 (2021).
Ostadal, P. et al. Increasing venoarterial extracorporeal membrane oxygenation flow negatively affects left ventricular performance in a porcine model of cardiogenic shock. J. Transl. Med. 13, 266 (2015).
Kern, K. B. et al. Postresuscitation left ventricular systolic and diastolic dysfunction. Circulation 95(12), 2610 (1997).
Laurent, I. et al. Reversible myocardial dysfunction in survivors of out-of-hospital cardiac arrest. J. Am. Coll. Cardiol. 40(12), 2110–2116 (2002).
Cheng, R. et al. Complications of extracorporeal membrane oxygenation for treatment of cardiogenic shock and cardiac arrest: A meta-analysis of 1,866 adult patients. Ann. Thorac. Surg. 97(2), 610–616 (2014).
Derwall, M. et al. Neuroprotective effects of the inhalational anesthetics isoflurane and xenon after cardiac arrest in pigs. Crit. Care Med. 36(11 Suppl), S492–S495 (2008).
Fries, M. et al. Neurocognitive performance after cardiopulmonary resuscitation in pigs. Crit. Care Med. 36(3), 842–847 (2008).
Fries, M. et al. Xenon reduces neurohistopathological damage and improves the early neurological deficit after cardiac arrest in pigs. Crit. Care Med. 36(8), 2420–2426 (2008).
Billig, S. et al. The self-expandable Impella CP (ECP) as a mechanical resuscitation device. Bioengineering (Basel) 11(5), 456 (2024).
Kelley, K. W. et al. Body surface area of female swine. J. Anim. Sci. 36(5), 927–930 (1973).
Niemann, J. T. et al. Coronary perfusion pressure during experimental cardiopulmonary resuscitation. Ann. Emerg. Med. 11(3), 127–131 (1982).
Manzo-Silberman, S. et al. Severe myocardial dysfunction after non-ischemic cardiac arrest: Effectiveness of percutaneous assist devices. J. Clin. Med. 10(16), 3623 (2021).
Vase, H. et al. The Impella CP device for acute mechanical circulatory support in refractory cardiac arrest. Resuscitation 112, 70–74 (2017).
Dennis, M. et al. Extracorporeal cardiopulmonary resuscitation for refractory cardiac arrest: A multicentre experience. Int. J. Cardiol. 231, 131–136 (2017).
Ouweneel, D. M. et al. Extracorporeal life support during cardiac arrest and cardiogenic shock: A systematic review and meta-analysis. Intensive Care Med. 42(12), 1922–1934 (2016).
Hutin, A. et al. Early ECPR for out-of-hospital cardiac arrest: Best practice in 2018. Resuscitation 130, 44–48 (2018).
Gottula, A. L. et al. Percutaneous left ventricular assist devices in refractory cardiac arrest: The role of chest compressions. Resusc. Plus 16, 100488 (2023).
Lotun, K. et al. Cardiac arrest in the cardiac catheterization laboratory: Combining mechanical chest compressions and percutaneous LV assistance. JACC Cardiovasc. Interv. 12(18), 1840–1849 (2019).
Packer, E. J. S. et al. Left versus biventricular assist devices in cardiac arrest. ASAIO J. 64(4), 489–496 (2018).
Remmelink, M. et al. Effects of left ventricular unloading by Impella recover LP2.5 on coronary hemodynamics. Catheter. Cardiovasc. Interv. 70(4), 532–537 (2007).
Karami, M. et al. Mechanical circulatory support in cardiogenic shock from acute myocardial infarction: Impella CP/5.0 versus ECMO. Eur. Heart J. Acute Cardiovasc. Care 9(2), 164–172 (2020).
Kapur, N. K. et al. Mechanical pre-conditioning with acute circulatory support before reperfusion limits infarct size in acute myocardial infarction. JACC: Heart Fail. 3(11), 873–882 (2015).
Esposito, M. L. et al. Left ventricular unloading before reperfusion promotes functional recovery after acute myocardial infarction. J. Am. Coll. Cardiol. 72(5), 501–514 (2018).
Kapur, N. K. et al. Unloading the left ventricle before reperfusion in patients with anterior ST-segment-elevation myocardial infarction. Circulation 139(3), 337–346 (2019).
Meyns, B. et al. Left ventricular support by catheter-mounted axial flow pump reduces infarct size. J. Am. Coll. Cardiol. 41(7), 1087–1095 (2003).
Kawashima, D. et al. Left ventricular mechanical support with Impella provides more ventricular unloading in heart failure than extracorporeal membrane oxygenation. ASAIO J. 57(3), 169–176 (2011).
Bachmann, K. F., Berger, D. & Moller, P. W. Interactions between extracorporeal support and the cardiopulmonary system. Front. Physiol. 14, 1231016 (2023).
Burkhoff, D. et al. Hemodynamics of mechanical circulatory support. J. Am. Coll. Cardiol. 66(23), 2663–2674 (2015).
Watanabe, S. et al., Left ventricular unloading using an Impella CP improves coronary flow and infarct zone perfusion in ischemic heart failure. J. Am. Heart Assoc. 7(6), (2018).
Nakashima, T. et al. Effect of percutaneous ventricular assisted device on post-cardiac arrest myocardial dysfunction in swine model with prolonged cardiac arrest. Resuscitation 193, 110010 (2023).
Garan, A. R. et al. Prospective comparison of a percutaneous ventricular assist device and venoarterial extracorporeal membrane oxygenation for patients with cardiogenic shock following acute myocardial infarction. J. Am. Heart Assoc. 8(9), e012171 (2019).
Thevathasan, T. et al. Left-ventricular unloading with Impella during refractory cardiac arrest treated with extracorporeal cardiopulmonary resuscitation: A systematic review and meta-analysis. Crit. Care Med. 52, 464 (2024).
Thevathasan, T. et al. Case report: Refractory cardiac arrest supported with veno-arterial-venous extracorporeal membrane oxygenation and left-ventricular Impella CP((R))-physiological insights and pitfalls of ECMELLA. Front. Cardiovasc. Med. 9, 1045601 (2022).
Funding
Open Access funding enabled and organized by Projekt DEAL.
This work was supported by a research grant from Abiomed Europe GmbH. The sponsor was not involved in the study design; the collection, analysis or interpretation of the data; the writing of the report; or the decision to submit the article for publication. SB was supported by the Clinician Scientist Program of the Faculty of Medicine of the RWTH Aachen University.
Author information
Authors and Affiliations
Contributions
SB Conceptualization, Data curation, Formal analysis, Funding acquisition, Investigation, Methodology, Project administration, Visualization, Writing – original draft Writing – review & editing. AK Investigation, Writing – review & editing. AT Investigation, Writing – review & editing. NH Investigation, Writing – review & editing. SY Investigation, Methodology, Writing – review & editing. KN Investigation, Writing – review & editing. CN Investigation, Writing – review & editing. EBS Investigation, Writing – review & editing. MD Conceptualization, Funding acquisition, Investigation, Methodology, Project administration, Supervision, Writing – review & editing.
Corresponding author
Ethics declarations
Competing interests
CN and EBS are employees of Abiomed Europe GmbH. The remaining authors declare that they have no conflicts of interest.
Ethical approval
The experimental design received approval from the responsible governmental institution (approval no. 84-02.04.2017.A300; North Rhine-Westphalia Office of Nature, Environment and Consumer Protection, LANUV NRW). The experiments comply with the ARRIVE guidelines and were carried out in adherence to the EU Directive 2010/63/EU for animal experiments.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Billig, S., Kanauskas, A., Theißen, A. et al. Comparison of mechanical resuscitation by an LV Impella device to extracorporeal resuscitation using VAECMO in a large animal model. Sci Rep 15, 9513 (2025). https://doi.org/10.1038/s41598-025-93264-2
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-93264-2
