
Abstract
Narrative medicine has become a meaningful solution to promote medical students’ professional and personal growth. However, there is a lack of study on how students benefit from the narrative medicine approach when developing identities. This study aimed to establish and implement an integrated English reading and writing curriculum based on collaborative reflection and discussion using the narrative medicine approach, exploring how students presented and constructed physician identities by performing speech acts. First-year undergraduate students majoring in clinical medicine were recruited. Collaborative reflection and discussion were conducted in the integrated course involving 14 pieces of medical-related narrative works, along with essential elements that guided the students to engage in classroom activities. In the following analysis, the qualitative analysis software NVivo was used to identify the main speech acts and their frequency to analyze students’ perception and recognition of different physician identities. Our analysis presented 33 major speech acts and revealed their frequency and characteristics, which we summarize in five interrelated physician identities. The fine-grained analysis showed how these identities were influenced by the narrative medicine approach, which provides enlightenment for supporting students to develop their professional identities. Another unique contribution of this study was to present the teaching basis and essential elements in an integrated humanistic curriculum. The results helped clarify the relationship between speech acts and physician identity and suggested that collaborative reflection and discussion using the narrative medicine approach improved the humanistic component that was in short supply in medical education through its interdisciplinary advantages, thus promoting professional identity development that can lead to higher-quality medical and emotional care.
Similar content being viewed by others

Introduction
Physician identity is “a representation of self, achieved in stages over time during which the characteristics, values, and norms of the medical profession are internalized” (Cooke et al. 2010). Many medical education commissions and associations encourage medical educators to ensure the ongoing development of appropriate professional behaviors for students in medical and health professions because the cultivation of physician identities, including professional values, actions, and aspirations, is the backbone of medical education (Cooke et al. 2010). Medical students with a professional identity are more confident in what they do as doctors, which affects their relationships with colleagues, patients, professional groups, and society (Monrouxe, 2010). They show concern for ethical principles and a willingness to interact with patients and co-workers to achieve professional growth (Cruess et al. 2002).
One of the reasons for the difficulty in professional identity development can be found in medical education, for it has become a source of biased teaching and learning (An et al. 2008). The students are trained to excel in medical and treatment technology, while social value and humanistic aspects of medicine are excluded (Ferry-Danini, 2018; Thibault, 2019). Medical educators have criticized “dehumanization in medicine” by calling on doctors to be scientific in their way of thinking as well as to learn to conduct ethical analysis and moral judgment (Amin et al. 2021; Pellegrino, 1984; Serodio et al. 2016). Therefore, academic attention should be paid to medical humanities. It is necessary to make educational suggestions for cultivating future doctors who pay more attention to patients.
As a theoretical and operative approach, narrative medicine plays a role in interdisciplinary learning from medicine, education, and humanities. Narrative medicine’s innovative model includes training in close reading and reflective writing. On the one hand, by reading virtual records of possible clinical situations, medical students are trained in the four essential abilities of attention, representation, reflection, and affiliation (Charon, 2005). Therefore, they can look outward at patients and inward at themselves (Langellier, 2009). On the other hand, medical students may not only gain emotional benefits (e.g., empathy) but also understand the patient’s experience and spiritual journey of themselves in career growth (Charon, 2008). In addition, using narrative medicine as a medical education tool includes potential benefits such as the perception of ethical challenges (Daryazadeh et al. 2020), identification with peers and broader professional communities (Lukolyo et al. 2019), and enhanced communication and reasoning skills (Welch and Harrison, 2016). Evidence from the structured model for narrative-based medicine interventions has shown that collaborative reflection and discussion further enrich the teaching strategies of close reading and corresponding reflective writings (Balmer and Richards, 2012; Milota et al. 2019). Opportunities are created for medical students to promote reflective thinking and their awareness of professional identity, thereby influencing their learning of professionalism (Huang et al. 2021). Close reading, reflective writing, sharing, and discussion help students have a broader view of patients and diseases in clinical practice, understand what the physician profession means, and comprehend the discourse of medicine and the society it serves (Charon, 2001). Students can think, act, and feel like a doctor under the positive influence of narrative medicine.
More attention has been put on the effects of narrative medicine interventions in recent years. There are many studies on its implementation for students during clinical practice, such as cultivating professionalism (Huang et al. 2021), its impact on patient care (Chretien et al. 2015; Fioretti et al. 2016), and increasing a sense of empathy (McDonald et al. 2015). It has also applied to teachers, helping them reflect in a unique space and gain support for their professional growth (Balmer and Richards, 2012; Holdren et al. 2023). Few studies have been conducted on how medical students in pre-clinical years benefit from the narrative medicine approach when developing identities. Pre-clinical students’ professional identity as preliminary doctors has not been fully developed (Park and Hong, 2022). Therefore, students need to perceive humanistic values and construct a professional identity for their future careers by having a rich knowledge of medical humanities, strengthening their ability to reflect and discuss with others, and enhancing listening, interpreting, absorbing, and imaginative skills (Miller et al. 2014).
Therefore, the study focuses on narrowing the gap in humanities education for pre-clinical students who lack sufficient opportunities to develop their professional identity and clarifying to what extent students externalize humanistic literacy into virtual clinical practice. We encourage students to integrate reading and writing practice into narrative medicine. Apart from improving English reading and writing abilities, with collaborative reflection and discussion (CRD) using the narrative medicine approach, students can also pay more attention to the reflection on medical-related stories, think about the attitudes, emotions, and values of the characters, gaining an awareness of professional identity. CRD refers to students inspiring and complementing each other through self-examination and peer interaction to generate new ideas, usually in the form of group and classroom discussions. This study designed a 32-week English reading and writing course to explore what physician identities students may develop from the analytical perspective of speech acts in the CRD corpus. Our study focused on the following questions:
(1) What are the repeated speech acts in CRD using the narrative medicine approach? How about their frequency?
(2) What physician identities do medical students develop through repeated speech acts?
Methods
Study design and context
This curriculum innovation experiment was conducted during the 2022–2023 academic year at Hangzhou Medical College in China. Based on the theory and practice of narrative medicine, an integrated English reading and writing curriculum was designed to explore how to adapt English teaching to medical education to avoid traditional grammar and vocabulary teaching. In our preliminary study (Zhong, 2021), we negotiated the main challenges and participatory changes involved in such an integrated course. As an implicit goal of medical education, professional identity is often taught in reliance on humanities, such as Ethics and Psychology. It is also the implicit teaching goal of this innovative curriculum partly because the characteristics of language learning help researchers to observe the relationship between students’ perception of physician identity and their language use and partly because the interdisciplinary characteristics of the integrated course help students improve their ability to explain and reflect on medical behavior from the stories and their ability to use metaphors and symbolic tools for future medical practice which may bring practical benefits to their identity transformation (Jones, 2013).
Participants
Fifty-six first-year undergraduate students majoring in clinical medicine from the same class participated in this research. The usual duration of their studies was five years. In addition to electives, the participants studied seven basic courses like Psychological Health Education, six specialized courses like Topological Anatomy, and had a two-week clinical clerkship. None of the participants took courses related to narrative medicine. All participants provided written informed consent before participating in the study.
Procedure
Narrative medicine was introduced into the weekly English reading and writing course, which was compulsory for the participants. The teacher used the narrative medicine approach to organize reading and writing activities with the explicit goal of nurturing the ability to read and write in English to improve communicative skills and the implicit goal of developing an awareness of physician identity. The medical-related texts were selected from the successful experiences of narrative medicine researchers and our preliminary study to cater to the needs of general medical students. The participants were divided into groups of five to six students to participate in CRD, the basis and teaching elements of which are described as follows:
CRD is based on a series of curriculum activities (Table 1). First, students understood the theoretical background of narrative medicine and the analysis methods of narrative works and simulated the process of narrative reading and writing. The focus was to give students a preliminary understanding of narrative medicine, laying the foundation for CRD. Then, we encouraged the medical students to adopt the narrative medicine approach, read and discuss narrative works in groups and with the class, engage in reflective writing, and share and comment on their writings with peers. The purpose was to promote medical students’ better understanding of their feelings and attitudes toward patients and doctors and of peers’ reflective discourse.
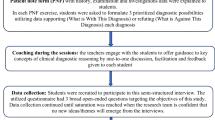
The essential elements of CRD were set according to the principles and teaching framework of narrative medicine based on the previous studies of Charon et al. (2016) (Fig. 1).

The arrows in the left panel reflect two contexts (i.e., close reading and reflective writing) involved in the three phases; the upper box in the right panel refers to the four elements of close reading centering on the goal of raising the awareness of physician identity through CRD; the lower box in the right panel refers to the four elements of reflective writing centering on the goal of exploring the physician identity through CRD.
After the students interpreted and absorbed the information through close reading, one researcher trained in teaching narrative medicine guided the students to engage in CRD around the four elements of narrative reading (Charon et al. 2016): time, space, metaphor, and voice. The aim of CRD in English reading was to encourage students to be aware of the role of medical staff in society and organizations.
The corresponding writing tasks enhanced students’ reflective ability. The subsequent CRD created a reflective space wherein students could explore the dimension and depth of narrative works and involved the following elements: reflection that helped students notice and shape their perceptions of medical behavior and organizational behavior; comment on the patient’s illness experience that helped construct empathy; and discussion that encouraged students to share their writings focusing on the understanding of plot, situation, illness, and death. The teacher provided supportive and non-judgmental mentoring and helped students develop an awareness of professional identity through interactions.
Data Sources
The corpus source is 24 CRD from October 2022 to June 2023 (Table 2). One of the researchers guided the students to engage in 24 CRD in the classroom; the other two took turns observing and recording the discussions via stenography, with a focus on students’ speech acts.
Fourteen pieces of medical-related narrative works were discussed (Table 3). The identities mentioned and discussed by the students include doctors, patients, patient’s relatives and friends, nurses, judges, and so on. All the discussions were tape-recorded. We transcribed the tape recordings into the corpus from which identifiable personal information was hidden.
Data analysis
Analytical perspectives
The analytical perspectives are “speech acts” and speech acts as “acts of identity.” Although there are many analytical tools for communication and conversation in medicine, such as the Roter interactive analysis system (Roter and Larson, 2002) applied to general clinical practice, speech acts analysis is a more direct and effective tool to analyze the CRD of medical students in the field of education.
Speech Act Theory, an important pragmatic theory, suggests that human language is not simply a combination of “sound and meaning” and that language can produce behavior because if the speaker says something meaningful and acceptable, his words will have a behavioral result. Austin (1975) called the behavior “speech acts” (SA) and divided it into three categories: the locutionary act is the act of speaking words, phrases, and clauses, expressing literal meaning through syntax, vocabulary, and phoneme; the illocutionary act is the act of expressing the speaker’s intention, which means people carry out specific acts when speaking, such as informing, ordering, and warning; the perlocutionary act has the consequences or changes brought by utterances. We focused more on the illocutionary act, as it is more conventional for us to judge and distinguish from the other two acts as connected with the production of effects in certain senses (Austin, 1975). For example, “She can read some poems” in our study implied the speaker’s intention that the doctor can recommend this patient to read poetry, and it revealed the student’s perception of physician identity on this occasion. The classification and examples of the illocutionary act provide us a reference to an analysis: Austin (1975) divided the illocutionary act into five categories; Searle (1979) further classified them in greater detail. Besides, a person can also realize the same intention through different locutionary acts, but there are often some typical expressions. In our study, speech acts were conducted within speech events (Hymes, 1968) in which medical-related works were discussed, so descriptions and explanations could be made to understand students’ attitudes and values.
All speech acts are “acts of identity”—linguistic behaviors contribute to constructing complex identities (Walters, 1987). “Identity” refers to an individual identifies with a social group, such as ethnicity, race, and class, containing two meanings: one is that an individual can be identified as a member of a social group while the other is that an individual regards himself as part of a group. These “acts of identity” emphasize the structural impact of social groups and are limited and influenced by contexts and situations within the class in our study. It included the identity that an individual student readily chose in communication, presenting and constructing important identities by repeatedly performing some SA in their discourse.
Analytical process
Our analysis began with familiarization of the data, where we re-read, made notes, and added comments on the content of classroom discussions to identify recurring SA as students used them through reading and writing activities. Reviewing these preliminary records of SA, all authors collaboratively identified descriptive codes to develop our first cycle coding. These initial codes, including SA of close reading and SA of reflective writing, were intended to capture our perceived fragments of an association between SA and physician identity within the teaching framework of CRD. Using the software NVivo, we then applied the first cycle coding scheme, coded independently, generating various codes and having regular discussions about these codes. We generated codes at the locutionary act level, for example, literal meanings that had typical expressions to realize intentions, and at the illocutionary act level, exploring students’ intentions (for example “his needs should come first” indicated doctors should prioritize patients’ needs). This step was used to examine how students’ SA over different narrative works revealed their physician identity. We refined the second cycle coding scheme by sharing coding to illustrate the relationships among CRD elements, SA, and physician identity, and then collaboratively defined the second cycle codes. To address reliability issues, the team discussed a section of the initial coding of the data conducted by Shanshan Li to modify and refine our coding definitions as the team negotiated conflicts in applying the coding scheme. We then applied the second cycle codes, building nodes classified by theme, and supplemented, merged, revised, and finalized the coding. For example, the sub-node of “reflect on how to help the ill” was placed under the tree node of “medical behavior” when it was initially coded, but after our in-depth discussion of the data, it was placed under the tree node of “illness and death.” We finally calculated the frequency of repeated SA, namely, how many CRDs contained the repeated SA. Based on these SA, we analyzed students’ perception and identification of physician identity.
Reflexivity
The stenography of all lessons made by two authors was allowed to capture real-time experiences by minimizing all authors’ voices. The writing assignments students handed in allowed for the validation of CRD fragments. All authors checked transcripts with original audio files to ensure data accuracy and met regularly to engage reflexively in reviewing data from multiple perspectives and challenging interpretations that may result from potential biases. Diversity in the research backgrounds of the authors limited personal or disciplinary bias: Shanshan Li was trained in English language and literature at the bachelor’s level and educational sciences at the master’s level, and Libo Zhong was trained in English language and literature at the doctoral level. Both work as teachers and researchers in undergraduate medical education and conduct research projects on narrative medicine. Yaping Cai works as a professor in education with expertise in curriculum theory and boundary crossing. All researchers have experience in qualitative research. Trustworthiness was addressed by collaborative interrogation of our perception of data derived from diverse positionalities and by rigorous analytical steps. The research was approved by the institutional review board and followed ethical approvals.
Findings
SA and frequency
Many characteristics can be seen in Table 4. Some SA appeared with high frequency in 24 CRD, which shows a distinct feature of the narrative medicine approach. For example, the SA of “focus on the time and speed of illness process (1)” appeared in 22 out of 24 discussions. SA with a percentage higher than 70% can be considered to be the most repeated parts of CRD, including “focus on the time and speed of illness process (1),” “analyze the patient’s physical changes (4),” “identify the different voices (6),” “know the attitude of the patient (13),” “understand the plot and situation deeply (15),” “increase the level of empathy (19),” “attention to details of illness and death, such as word choice (22),” “reflect on what kind of attitude doctors should have toward the patient (29),” and “think about communication and connection (32)”.
The frequency of SA varies widely, but it is not easy to distinguish which SA is necessary for students to use in CRD. One reason may be related to the contextual differences. If the narrative works provided the context in the first person of the patient, students need not “confirm that the patient is aware of the illness status (2)”; if there were no apparent conflicts in attitudes or interests, students need not “rank the wishes of the patient and others (14)”. The examples demonstrate that although some SA seems important, the narrative works do not guarantee the necessity to use them. The perspective of thinking also influences the choice of SA. For example, “give spatial information in a region (5)” and “identify the voices that influence the patient (10)” were usually not directly related to the medical knowledge that aroused students’ interest, but were often proposed by the teacher who guided the discussion. Students may choose SA that seems related to their major, or the one that is easier to identify from the elements of CRD. As a rough estimate, SA with a frequency of more than 60% (bold in Table 4) is necessary for CRD.
Physician identity
Based on the frequency of SA and the CRD corpus, we summarized the main physician identities as follows.
The spokesperson for the patient’s wishes
Students noticed that when patients did not clearly state their wishes for subjective or objective reasons, doctors should take the initiative to inquire and presume the patient’s wishes from the details. The identity of the spokesperson can be seen in confirming that the patient is aware of the illness status (2), presuming the patient’s wishes (11), knowing the attitude of the patient (13), ranking the wishes of the patient, and others (14), and being aware of the rights and interests of the patient (17). Students tried to analyze the patient’s wishes while taking notes of other people. Even when the patient did not express any wishes, the students speculated about his possible expression based on his educational background and life experience. When patients and doctors choose different medical options, students realize that they need to communicate with the patients (32), prioritize their wishes (14), and consider inviting their relatives regarded as people who know them best to participate in medical decisions (10).
Example 1a: The doctor’s objectivity and the patient’s suffering (CRD on How the Poor Die)
Student: Based on all we know about him (10), he would refuse cupping therapy (11). But his resistance had no effect (15), and he suffered too much (19).
Teacher: Did Orwell say anything? Why did you make this judgment?
Student: He knew he was seriously ill (2), but he didn’t want to be treated like the No. 57 patient (13) whose belly is the only valuable part to the doctor and interns (15). I think the doctor should ask for Orwell’s permission (32).
Student: Case teaching is inevitable, but the way the doctor performed was not beneficial for Orwell (17).
Teacher: What did he do for Orwell?
Student: Ask him to take fundamental drugs. But I’m afraid the doctor wanted to take him to the autopsy room after he died (14, 15).
Teacher: What did Orwell expect?
Student: His needs should come first (13, 14). If possible, any of his relatives or friends should also be there to help (10).
After closely reading How the Poor Die, the students identified that patients in free wards were treated with no dignity, and presumed Orwell’s wishes based on his life background and experience in public hospitals (11). After reviewing the details, they confirmed that he knew the illness status (2). The student perceived that the treatment chosen by the doctor or the medical institution did not necessarily correspond to the rights and interests of the patient (17). Therefore, after examining the doctor’s medical behavior in the story (15), they knew the patient’s attitudes by checking the medical context (13) and found that the wish of the patient was different from that of the doctor (14). The students were aware that, in diagnosis and treatment, the doctor should ask patients and their relatives about their wishes, putting the patient’s wish first in the ranking process (14).
The students found the hybrid identities of doctors challenging; they viewed the doctor as a scientist and researcher who should take a distant and objective attitude when communicating with the patient; on the other hand, they realized it was far from the patient-centered concept required by the clinical practice as it showed no respect for the patient. The students wrote in reflection (Example 1b): “This is a story told from the patient’s perspective as if to warn us what should be the first concern of a doctor (12,15)”; “Scientific descriptions and research are important, but ignoring the emotional demands of patients can lead to doctor-patient conflicts (9) and undermine doctors’ efforts to respect patients (17).” The students tried to understand complex expressions and the plot in the stories (12,15), coming to a consensus that, by inquiring and presuming the patient’s wishes, doctors not only prioritize the patient’s rights and interests (14,17) but also protect doctors’ safety by avoiding possible risks (29).
The guide for patients in the face of illness and death
Most students learned about different diseases and their consequences for the first time by reading a novel or watching a movie. They read detailed descriptions of the illness and tried to understand patients’ psychological states like emotions, perceptions, and expectations. Therefore, the physician identity as a guide was developed in CRD as the students learned how to help patients increase courage in the face of illness and death, and how to advise on possible arrangements as the disease got worse. It can be seen in focusing on the time and speed of illness development (1), examining how patients experience sick time (3), analyzing the patient’s physical changes (4), accepting and promoting the concept of palliative care (23), raising the issue of caring for patients (25), suggesting arrangements or activities (27), and paying attention to the patient’s hobbies or the final wishes (28).
Example 2a: Noticing, finding, and advising arrangements (CRD on Breathe)
Student: In just ten minutes of the film, Robin was infected with the polio virus and paralyzed (1), with only a slight head movement (3,4). It’s so sad (19).
Student: Without a ventilator, he would die in two minutes (1,4).
Teacher: So what is the narrative focus of Breath?
Student: It’s about how they faced the disease (12). It’s good for them to do everything they can, leaving no regrets (27). What the doctors can do is trying to keep death from coming too soon (25).
Student: But Robin was lucky (19). Diana took care of everything with the help of their friends (25). Relatives can do more than doctors (25).
Teacher: What happened then?
Student: He finally decided to say goodbye to the world (1,13) because relying on the ventilator for such a long time made his lungs extremely susceptible to infection (1,4).
Student: At least he saw his son growing up. It may be what he wanted most (13,28). The near-death stage should not be prolonged (23). If I were Robin, I would do the same (19).
In Example 2a, the elements of “time” and “space” (1,4) were discussed several times as students constantly found new details of the progression of the disease and the physical changes of the patient. The students empathized with the loss of the patient’s health (19), tried to know the best that the doctor and caregivers could do in different stages of illness (25), noticed the patient’s final wishes (28), and accepted and promoted the concept of palliative care (23). By directly observing the dynamic changes of the disease and the patient’s experience of illness, the students proposed the arrangement (27) concerning emotional care and finally accepted and respected the patient’s decision to say goodbye to the world (13). Students developed an understanding of the doctor’s responsibility as a guide for patients. In the CRD of reflective writings (Example 2b), students realized that doctors need to communicate with patients on the topic of illness and death (32), reflect on what kind of attitude doctors should have toward the patient (29), and guide patients to vent their feelings when they are in sickness:
Example 2b: Guide patients to think about illness and death
• I think what the author wants to say is that the meaning of death is letting life explode more brightly in an increasingly limited time (12,15). Death is not a negative existence; it’s a “good night.” If we convey such positive emotions to the patient (29,32), it is also a form of medical help and treatment (16). (CRD on Do Not Go Gentle into That Good Night)
• When the doctor informed the patient of the bad news, he encouraged the patient to face reality bravely rather than using technical terms (32). I was deeply impressed by his solicitude. A doctor’s verbal language can help a patient calm down and encourage him (16,29). (CRD on What the Doctor Said).
The students’ SA were often targeted, usually from doctors’ perspectives, such as informing diagnosis, body language, medical or life advice, and palliative care. Students can understand that the doctor should be with the patient in the face of illness or death as their guide during medical treatment.
The listener for multiple voices
The students often searched for medical knowledge related to the narrative works and briefly exchanged information with peers (33) to prepare for a better understanding of diverse voices. They identified different voices (6), confirmed the speaker’s rights and obligations (7), noticed the gap between the speaker and the listener (8), and observed the effects of the speaker’s encounter with the listener (9) to understand all the voices in the story. Through deeper reading and writing, they noticed the patient’s difficulties (26) and communication issues (32). Students were thus able to ensure that all voices were taken into account in the virtual medical context and realized that they should listen to multiple voices before taking responsibility for healthcare decisions.
Example 3a: An understanding of all voices (CRD on the Children Act)
Teacher: Adam’s parents were supposed to know Adam best (10). What choice did they make?
Student: They would refuse blood transfusion because of religious beliefs (6).
Teacher: So what choice did others make?
Student: The hospital filed a lawsuit, so Fiona decided to force blood transfusions (6).
Teacher: We seemed to ignore Adam’s wishes (11).
Student: He refused the treatment (13).
Teacher: What did he say? Why did you make this judgment?
Student: He would accept blood transfusion treatment (11) because Fiona had become his new faith (15). But when he wrote or talked to her, Fiona thought it was not her job (6,26), so he refused (13).
Student: Fiona did not listen to Adam’s story (8). She ignored Adam’s emotional needs (7). There’s a big gap between them (8,26).
Teacher: But she finally changed. Do you know why?
Student: Her conversation with her husband showed that she had changed (9). If she had changed earlier, the result might have been different (29,32).
The students discovered the hidden voices between the lines and the intricate background behind them. The student first pointed out that Adam had leukemia and briefly shared relevant medical knowledge, noting that it should be a recurrent case (33). After identifying the voices of Adam, his parents, the court, Fiona, and her husband (6), they pointed out that Fiona, as a professional, refused to listen to Adam (26), which prevented the patient’s voice from being heard, and that she did not fulfill her duty as a listener (7,8). As a result, the students shared an in-depth reflection on Adam’s refusal of blood transfusion (9), which prompted them to think about how to communicate and connect with others as doctors (32). One student shared his writing excerpts in the class (Example 3b): “When Adam wanted to talk to Fiona, what Fiona thought about was the proprieties and dignity of her professional identity (26,32). Children are vulnerable. In addition to the physical well-being, we must provide them with spiritual well-being (29)”.
Different voices that need to be heard by doctors also arise among students who presume they are doctors. In the 22nd CRD on You Don’t Know Jack, many students believed that Jack patiently listened to each patient’s words and understood their wishes and interests, so making euthanasia legal was acceptable. However, some expressed concern about the technical aspects of communicating with the patients and understanding their choices and wishes. They finally concluded that doctors should pay attention to all the voices, on which they could make prudent healthcare decisions.
The Empathizer who offers love and help
Some SA showed students’ empathy for patients’ emotions like pain and loneliness. Being an empathetic doctor who can offer love and help to patients was also what medical students realized when developing the awareness of physician identity. The identity of the empathizer can be seen in their new or changed knowledge to help the patient (16), their perception of the patient’s experience (18), an increased level of empathy (19), an increased understanding of the elderly and the seriously ill (20), and reflection on how to help the ill (24). The discourse in Example 4 came from the 3rd CRD about how people help each other to overcome difficulties together.
Example 4: Giving care, love, and empathy to patients (CRD on The Way We Live Now)
• There are no words warning visitors of the possibility of infection now. It’s hard to imagine what it was like for him to live in an environment of discrimination before such changes happened (19).
• During his hospitalization, he began to keep a diary, recording his feelings since he was diagnosed with AIDS, and writing down his regrets (3,15). Will it be of great help if we encourage patients to read or write poems or diaries to vent their feelings or get inspiration (16,24)?
• He may think he was alienated and isolated (18), but the doctor was kind, patient, and optimistic about his condition (15). Good qualities such as respect, compassion, and companionship are valuable for the patients (16,24).
The students analyzed from all perspectives: how “his” lover, friends, the hospital, and doctors were concerned about his illness in different ways. They focused on how to provide “him” with continual love and assistance. The above SA with strong empathy included open-ended questions (“What it was like for him to …?”) and more implied questions (“Is it of great help if …?”). Such emotional insights left room for reflection and reminded students to offer love and help to patients. “Good qualities … are valuable” is not only the affirmation of the doctor’s medical behavior but also an invitation for all future doctors to give care and empathy to the patients.
The reflective doctor who reinterprets the process
To develop the ability to describe the clinical process in non-technical language, the students learned to describe the causes and effects, disease progression, and the care process, reinterpreting and thinking reflectively based on “time and speed of illness process (1),” “spatial information (5),” “complex and metaphorical expression (12),” “the plot and contextual situation (15),” and “details of illness and death such as word choice (22).” The students explored the way they reinterpreted the process in the discussions, which may contribute to their reflection on illness, diagnosis, and death:
Example 5a: Reinterpretation of the story (CRD on The Masque of the Red Death)
• During the plague (1), the king welded the bolt and reveled inside the castle, leaving people to die outside (5,15). The strike of midnight (1) suggested his death (12). “Red” (12,22) is the color of blood from killing all people (12), but behind the masque was empty. Does it indicate that the king was not killed by the “Red Death” but by his ruthlessness and brutality (12)?
Through reflection and discussion, students noticed something they were unaware of and re-understood the complicated information. Sometimes, they invited their peers to pay attention and listen to their reflections (30), and they responded to the invitations (31). In this process (Example 5b), the students often examined their reinterpretations from a distance or from the point of view of another student to verify whether their perceptions were accurate and adequate:
Example 5b: The dilemma of oncologists (CRD on Wit)
• She reviewed her life in the hospital bed (3), talking to her father, first teacher, students, and “us” in the classroom (5). Passing away with the teacher reading her favorite childhood story (1,3) was the best send-off she could have imagined (28). I felt a deep sadness (19). I think oncologists love cancer cells more than patients because the former is the victor and the strong (15). Do you agree (30)?
• It’s true that doctors should be calm, objective, and rational, but most also have compassionate hearts. Sometimes, patients only need someone to be with them (16,19).
Some students took great pride in their reflective writings and were adept at capturing what they saw in narrative works and sharing it with others (30); some commented on their peers’ concerns and reinterpretation (31). They responded to the call of the suffering patients and tried to understand what the doctor should do to echo the call.
Discussion
While most medical-related narrative works provide opportunities for medical students to improve their level of empathy and sense of humanistic literacy (Milota et al. 2019), the students often have little support in systematically considering how they might utilize theory and knowledge of narrative medicine to influence their perceptions as a doctor and maintain an awareness of self-reflection with the help of peer-learning in the school context. Integrating CRD using the narrative medicine approach into the teaching of medical humanities, we intentionally targeted the professional identity development of medical students as the implicit teaching goal, leveraging the tool of speech acts to reveal students’ SA and their frequency. By intentionally enhancing the listening, interpreting, absorbing, and imaginative skills of the students through close reading and reflective writing, we summarized the physician identities from the CRD corpus—the spokesperson for the patient’s wishes, the guide for patients in the face of illness and death, the listener for multiple voices, the empathizer who offers love and help, and the reflective doctor who reinterprets the process. Through the analysis of SA frequency and CRD corpus, we summarized some speech acts and explored the process of students’ reflection and discussion. The above analysis and our work on curriculum integration provided implications for supporting medical students’ professional identity development.
First, a sustained commitment to providing students with poetry, novel, and film narratives related to illness and death while utilizing literary texts to discuss is imperative for developing students’ abilities to reflect on medical contexts and physician identities. Previous studies have shown that the fictional world created by narrative works may expand students’ knowledge of self and others and of self and the world around them, regardless of the limitations of time and space, which is conducive to professional identity development and the effective prevention of job burnout (Oyebode and Pourgourides, 1996; Charon, 2000). As for the physician’ss identity as the spokesperson, many SA show that medical students presumed, confirmed, and respected patients’ wishes; they tried to understand the patients and thought about how to communicate with them rather than being objectively alienated researchers. CRD supported by the narrative medicine approach helped students acquire the tacit knowledge that cannot be obtained from books: students can recognize that doctors should prioritize patients’ interests and wishes to avoid risks that may take place between doctors and patients. For another example, reflection and observation of the dynamic changes of disease deepen their understanding of life and death, training themselves to be the guide for patients in the face of illness and death, which may bring a new point of view for their future clinical practice.
It can be assumed that these narrative works imperceptibly convey ethical and moral values through CRD, inspiring students to think deeply about the process of diagnosis and treatment and re-understand patient narratives and the role of doctors. By targeting the creation of reflective space and positioning CRD as an opportunity to co-construct group identity, medical students can engage in the process of conceptual change (Sinatra and Pintrich, 2003) that promotes professional identity development. The study also confirmed the previous research results that narrative-based medical education has a positive impact on the cultivation of professional identity (Miller et al. 2014).
Second, guidance for medical students on the recognition of balance and interrelation among different physician identities is necessary. It can improve their sensitivity to medical situations and their capacity to find possible cause-and-effect relationships. Furthermore, the guidance can facilitate the students to identify the signal of what actions a doctor should take at some point and thus make more well-rounded judgments and diagnoses.
The interrelated physician identities as the listener for multiple voices and the empathizer who offers love and help, both of which reflected the benefits of using the narrative medicine approach—attention, reproduction, and affiliation (Charon, 2005): by focusing on the patients and their illness experience, listening to multiple voices in and out of the illness stories, sharing and discussing reflective writings, in the process being able to increase the understanding of the ill and re-understand the patients’ viewpoints and behaviors; attention and reproduction spiral into an affiliated relationship between the patient and the future doctors, medical students can understand the patient’s wishes and difficulties, empathize with them by examining their behavior and thoughts in the whole process, and tend to become reflective doctors who reinterpret the medical stories. This study illustrates that CRD using the narrative medicine approach may promote a more systematic and comprehensive understanding of physician identity among medical students. However, some studies have also pointed out that maintaining the steady development of these understandings through continuous training is also crucial (Xue et al. 2023).
In addition, we recommend that engaging in collaborative learning should provide more opportunities for students to repeatedly use some SA to develop an awareness of different physician identities, especially high-frequency SA as they are easier to identify from the elements of CRD. If the teacher guides the students to an in-depth discussion of the plot and situation, they must be prepared to understand discourse, mental activity, silence, metaphor, and implication of the virtual medical story. Therefore, speech acts with high repetition, such as “know the attitude of the patient” and “understand the plot and situation deeply,” are useful to explain more accurately their views and attitudes towards patients, diagnosis, and treatment, focusing their attention on the physician identity that they were unaware of—doctors who listen to patients’ description of pain or who are good at observing details. Students can be trained as reflective doctors who reinterpret the medical process by using frequent SA like “focus on the time and speed of illness,” “analyze the patient’s physical changes,” and “observe the effects of the speaker’s encounter with the listener.” Students can develop the habits of paying attention to the patient’s emotional demands rather than only focusing on the scientific description and morphological characteristics of the disease by repeatedly using SA such as “presume the patient’s wishes” and “pay attention to the patient’s hobbies or final wishes,” so the great decline in empathy levels may not occur. Students’ speech acts are not merely a reflection of the objective world, because language users are engaged in social activity while conveying information, creating a perspective filled with specific meanings, thus revealing their social identity (Gee, 2014). This study can be used as a non-linear model to consider how to expand SA through CRD, thereby encouraging more diverse identities of being a doctor, which may challenge the scientific learning experience these future doctors are very familiar with in their daily study and work.
Finally, we also recommend that encouraging students’ participation in the context of close reading and reflective writing be imperative for developing the capability of making the implicit learning of physician identity explicit for medical students by using the tool of language and literature. Influencing factors include the support for the ability of students to notice and negotiate different perceptions of the virtual medical stories, and the selection of narrative works. On the one hand, by organizing activities involving collaborative learning and reflective learning like CRD, students can discuss what they perceive from the role of a doctor, such as attitudes, behaviors, and values, through negotiation as critical peers. Isolated reflections and learning experiences can be challenging and uncertain without conceptual change processes, resulting in fewer opportunities for generative learning (Sinatra and Pintrich, 2003). Medical students can be provided the opportunities to feel what the group feels, mitigating some of the risks of interpersonal relationships brought about by critical friendship (Swaffield, 2007). On the other hand, considering that narrative works are reading materials and discussion contents, teachers should select narrative works and corresponding English versions that meet students’ English levels. By targeting medical narratives with sufficient details and ethical dimensions as opportunities for reflective and collaborative learning, teachers can help students engage in elaboration and description processes that improve narrative skills (Charon, 2008), constituting a valuable source of the implicit learning goal of professional identity for students in interdisciplinary environments.
Limitations
First, there were few interdisciplinary collaborations among different medical majors and few collaborations with experts who have diverse experiential and academic expertise that may occur in clinical practice. Introducing such collaboration may act as a catalyst for critical reflection on physician identity, resulting in producing a more comprehensive understanding of SA. Second, our study only investigated pre-clinical students, so further study can focus on the interns to produce more exciting ideas. Third, since there is no systematic and theoretical guidance for the selection of medical-related narrative works, we relied on the successful experience of narrative medicine researchers and our previous teaching experiments. Further research can be conducted on teaching contents and syllabi. Finally, it lacks an assessment of the long-term effects of the integrated curriculum and repeated use of SA, which may have implications for transferring the positive characteristics from classroom settings to clinical practice contexts to maintain sustainable development of professional identity.
Conclusion
The results of this qualitative study illustrated the benefits and value of the CRD approach based on narrative medicine theory and helped clarify the relationship between the frequent use of some SA and different physician identities to promote the professional identity development of medical students. This study used close reading and reflective writing adopting the narrative medicine approach to guide students in collaborative reflection, and in evaluating and discussing doctors’ clinical behaviors and patients’ experiences within the teaching framework of the integrated course, thereby bringing potential benefits for medical students’ personal and professional development.
Thus, many humanities courses with interdisciplinary strengths in medicine and literature, including English reading and writing, create conditions for teachers to use the narrative medicine approach through CRD to encourage students to view illness stories with humility and empathy and reflect on the attitudes, emotions, and values of healthcare professionals. Students can thereby gain an awareness of professional identity that may lead to higher-quality medical and emotional care. It is low-cost and easy to implement. Teachers can build a CRD corpus when implementing an integrated curriculum by collecting SA data to understand how the implicit goal of professional identity development is achieved. It is relatively simple and can be updated over time. We must give priority to favorable conditions, such as the selection of medical-related narrative works conducive to CRD, and the construction of teaching teams to achieve the desired results.
The fact that most Chinese medical schools have a requirement to learn English is more conducive to developing CRD using the narrative medicine approach in interdisciplinary courses. Although change is necessary in language courses that seem to have nothing to do with medicine, it is particularly vital in changing teaching methods and establishing the implicit goal because traditional instructional practices often fail to use medical-related works to influence students’ perception of physician identity. Traditional grammar and vocabulary teaching is not enough as it is divorced from the actual needs of medical education. Therefore, by integrating curriculum and updating teaching methods, the study tries to narrow the gap in medical humanities education for pre-clinical students and provides some references for professional identity and professionalism.
Data availability
Due to conditions on participant consent and other ethical restrictions required by the funder and the medical school, the datasets generated and analyzed during the current study are not publicly available. If you have any database data requirements, please contact the corresponding author of this study.
References
Amin S, Chin J, Terrell MA, Lomiguen CM (2021) Addressing challenges in humanistic communication during COVID-19 through medical education. Front Commun 6:619348. https://doi.org/10.3389/fcomm.2021.619348
An JH, Kwon I, Lee SN, Han JJ, Jeong JE (2008) Study on the medical humanities and social sciences curriculum in Korean medical school: current teaching status and learning subjects. Korean J Med Educ 20(2):133–144. https://doi.org/10.3946/kjme.2008.20.2.133
Austin JL (1975) How to do things with words. 2nd edn. Harvard University Press, Massachusetts
Balmer DF, Richards BF (2012) Faculty development as transformation: lessons learned from a process-oriented program. Teach Learn Med 24(3):242–247. https://doi.org/10.1080/10401334.2012.692275
Charon R (2000) Literature and medicine: origins and destinies. Acad Med. 75(1):23–27. https://doi.org/10.1097/00001888-200001000-00008
Charon R (2001) Narrative medicine: a model for empathy, reflection, profession, and trust. JAMA: J Am Med Assoc 286(15):1897–1902. https://doi.org/10.1001/jama.286.15.1897
Charon R (2005) Narrative medicine: attention, representation, affiliation. Narrative 13(3):261–270. https://doi.org/10.2307/20079651
Charon R (2008) Narrative medicine: honoring the stories of illness. Oxford University Press, New York
Charon R, DasGupta S, Hermann N, Irvine C, Marcus ER, Colsn ER, Spencer D, Spiegel M (2016) The principles and practice of narrative medicine. Oxford University Press, New York
Chretien KC, Swenson R, Yoon B, Julian R, Keenan J, Croffoot J, Kheirbek R (2015) Tell me your story: a pilot narrative medicine curriculum during the medicine clerkship. J Gen Intern Med 30(7):1025–1028. https://doi.org/10.1007/s11606-015-3211-z
Cooke M, Irby DM, O’Brien BC (2010) Educating physicians: a call for reform of medical school and residency. Jossey Bass, San Francisco
Cruess SR, Johnston S, Cruess RL (2002) Professionalism for medicine: opportunities and obligations. Med J Aust 177(4):208–211. https://doi.org/10.5694/j.1326-5377.2002.tb04735.x
Daryazadeh S, Adibi P, Yamani N, Mollabashi R (2020) Impact of a narrative medicine program on reflective capacity and empathy of medical students in Iran. J Educ Eval Health Prof 17:3. https://doi.org/10.3352/jeehp.2020.17.3
Ferry-Danini J (2018) A new path for humanistic medicine. Theor Med Bioeth 39(1):57–77. https://doi.org/10.1007/s11017-018-9433-4
Fioretti C, Mazzocco K, Riva S, Oliveri S, Masiero M, Pravettoni G (2016) Research studies on patients’ illness experience using the narrative medicine approach: a systematic review. BMJ Open 6(7):e011220. https://doi.org/10.1136/bmjopen-2016-011220
Gee JP (2014) An introduction to discourse analysis: theory and method. Routledge, London. https://doi.org/10.4324/9781315819679
Holdren S, Iwai Y, Lenze NR, Weil AB, Randolph AM (2023) A novel narrative medicine approach to DEI training for medical school faculty. Teach Learn Med 35(4):457–466. https://doi.org/10.1080/10401334.2022.2067165
Huang CD, Jenq CC, Liao KC, Lii SC, Huang CH, Wang TY (2021) How does narrative medicine impact medical trainees’ learning of professionalism? A qualitative study. BMC Med Educ 21(1):391. https://doi.org/10.1186/s12909-021-02823-4
Hymes DH (1968) The ethnography of speaking. In: J Fishman (ed.) Readings in the sociology of language. De Gruyter Mouton, Berlin, Boston, pp.99-138. https://doi.org/10.1515/9783110805376.99
Jones AH (2013) Why teach literature and medicine? Answers from three decades. J Med Hum 34:415–428. https://doi.org/10.1007/s10912-013-9241-9
Langellier KM (2009) Performing narrative medicine. J Appl Commun Res 37(2):151–158. https://doi.org/10.1080/00909880902792263
Lukolyo H, Keating EM, Rees CA (2019) Creating a collaborative peer writing group during residency. Med Educ Online 24(1):1563421. https://doi.org/10.1080/10872981.2018.1563421
McDonald P, Ashton K, Barratt R, Doyle S, Imeson D, Meir A, Risser G (2015) Clinical realism: a new literary genre and a potential tool for encouraging empathy in medical students. BMC Med Educ. 15:112. https://doi.org/10.1186/s12909-015-0372-8
Miller E, Balmer D, Hermann N, Graham G, Charon R (2014) Sounding narrative medicine: Studying students’ professional identity development at Columbia University College of Physicians and Surgeons. Acad Med 89(2):335–342. https://doi.org/10.1097/acm.0000000000000098
Milota MM, van Thiel GJMW, van Delden JJM (2019) Narrative medicine as a medical education tool: A systematic review. Med Teach 41(7):802–810. https://doi.org/10.1080/0142159x.2019.1584274
Monrouxe LV (2010) Identity, identification and medical education: Why should we care? Med Educ 44(1):40–49. https://doi.org/10.1111/j.1365-2923.2009.03440.x
Oyebode F, Pourgourides C (1996) Literature and medicine. Lancet 348(9031):894. https://doi.org/10.1016/s0140-6736(00)04584-0
Park GM, Hong AJ (2022) “Not yet a doctor”: medical student learning experiences and development of professional identity. BMC Med Educ. 22(1):146. https://doi.org/10.1186/s12909-022-03209-w
Pellegrino ED (1984) The humanities in medical education: Entering the post-evangelical era. Theor Med 5(3):253–266. https://doi.org/10.1002/chp.4760020317
Roter D, Larson S (2002) The Roter interaction analysis system (RIAS): Utility and flexibility for analysis of medical interactions. Patient Educ Counsel 46(4):243–251. https://doi.org/10.1016/S0738-3991(02)00012-5
Searle JR (1979) Expression and meaning: studies in the theory of speech acts. Cambridge University Press, Cambridge, England
Serodio A, Kopelman BI, Bataglia PUR (2016) The promotion of medical students’ moral development: a comparison between a traditional course on bioethics and a course complemented with the Konstanz method of dilemma discussion. Int J Ethics Educ 1(1):81–89. https://doi.org/10.1007/s40889-016-0009-8
Sinatra GM, Pintrich PR (2003) The role of intentions in conceptual change learning. In: Sinatra GM, Pintrich PR (eds.) Intentional Conceptual Change. Lawrence Erlbaum, Mahwah, New Jersey, pp. 1-18
Swaffield S (2007) Light touch critical friendship. Improv Sch. 10(3):205–219. https://doi.org/10.1177/1365480207077845
Thibault GE (2019) Humanism in medicine: What does it mean and why is it more important than ever? Acad Med. 94(8):1074–1077. https://doi.org/10.1097/acm.0000000000002796
Walters K (1987) RB Le Page and Andrée Tabouret-Keller. Acts of identity: Creole-based approaches to language and ethnicity. Cambridge: Cambridge University Press, 1985. pp. x+275. Lang Soc 16(4):569–571. https://doi.org/10.1017/S0047404500000403
Welch TJ, Harrison SL (2016) Teaching medicine through the study of literature: Implementing a fourth-year distance learning elective. Acad Med: J Assoc Am Med Coll 91(3):360–364. https://doi.org/10.1097/ACM.0000000000001030
Xue M, Sun H, Xue J, Zhou J, Qu J, Ji S, Bu Y, Liu Y (2023) Narrative medicine as a teaching strategy for nursing students to developing professionalism, empathy and humanistic caring ability: a randomized controlled trial. BMC Med Educ 23(1):38. https://doi.org/10.1186/s12909-023-04026-5
Zhong LB (2021) An integrated curriculum of British and American literature and narrative medicine. Mod Commun 23:13–16. https://doi.org/10.3969/j.issn.1009-5349.2021.23.xiandaijj202123006
Acknowledgements
This work was supported by the Teaching Commission of Hangzhou Medical College under Grant number XJJG202216.
Author information
Authors and Affiliations
Contributions
Shanshan Li substantially contributed to the conception, data collection, data analysis, interpretation, drafting, and critical revision of the paper. Libo Zhong substantially contributed to the conception, methodology, data collection, data analysis, review, and editing of the manuscript. Yaping Cai was involved in the data collection, data analysis, and interpretation of the manuscript. All authors read and approved the final manuscript, and agreed to be accountable for all aspects of the research.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethical approval
The study conducted was approved by the local ethics committee of Hangzhou Medical College. Throughout the study, all methods followed the approved methodology and adhered to the relevant guidelines and regulations.
Informed consent
All participants provided written informed consent prior to participating in the study.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Li, S., Zhong, L. & Cai, Y. Collaborative reflection and discussion using the narrative medicine approach: speech acts and physician identity. Humanit Soc Sci Commun 11, 651 (2024). https://doi.org/10.1057/s41599-024-03046-w
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1057/s41599-024-03046-w
