
Abstract
A global increase in the frequency, severity, and scale of extreme heat raises concerns about human vulnerability to climate change and associated mortality. Heat vulnerability and mortality have largely been studied separately, lacking an understanding of their causation. Here, we create a non-parametric generalized inference approach that links socioeconomic, environmental, and infrastructure factors articulated in vulnerability theory and heat mortality between 2010 and 2020 for counties across the United States. We find that the lack of vegetation coverages drives mortality in the Southern U.S. and among Hispanic people. Limited air conditioning is a key factor in heat-related mortality among White people and the Northern U.S. A combination of poverty and education influences the heat mortality in the Southeastern U.S., while poverty is critical to the heat mortality of Black people. We also find that the effects of vegetation and air conditioning in reducing heat mortality have been on the rise in the past decade. However, socioeconomic factors, in particular poverty and education, remain the most influential constraints. To further explain this transition, a series of regression models is created. The results show that improving 1% in vegetation coverage or air conditioning installation rate can effectively complement the 1.16% negative effect of socioeconomic constraints on heat mortality. A 1% increase in vegetation area is found to be comparable to a 1.5% increase in air conditioning installation in terms of reducing heat-related mortality. Our findings bridge the gap between heat vulnerability theory and mortality, emphasizing the importance of location-based strategies and nature-based infrastructure in mitigating the health burden of extreme heat.
Similar content being viewed by others

Introduction
Extreme heat events have been demonstrated to exert varying degrees of impact on society, ecology, and the economy (Carleton and Hsiang 2016, Liu, Zhang et al. 2024). Of greater concern is the fact that extreme heat has led to an increase in both fatalities and diseases (Kravchenko, Abernethy et al. 2013, Campbell, Remenyi et al. 2018, Edo, Itoje-akpokiniovo et al. 2024). The Intergovernmental Panel on Climate Change (IPCC) reports that extreme heat events are projected to become more severe, frequent, and prolonged by the end of the twentieth century, leading to an anticipated rise in heat-related morbidity and mortality in the future (Marx, Haunschild et al. 2021). Therefore, in the pursuit of effective mitigation and prevention strategies, understanding how extreme heat leads to mortality is critical.
One of the widely adopted methods is to examine the heat vulnerability of people (Reid, O’Neill et al. 2009, Maier, Grundstein et al. 2014, Rosenthal, Kinney et al. 2014, Weber, Sadoff et al. 2015, Nayak, Shrestha et al. 2018, Cheng, Li et al. 2021). Traditional heat vulnerability theories (Weber, Sadoff et al. 2015, Nayak, Shrestha et al. 2018) define vulnerability to extreme heat events as a combination of exposure to high-temperature events, sensitivity to adverse health impacts resulting from socioeconomic characteristics, and adaptive capacity such as infrastructure for preparedness (Harlan, Brazel et al. 2006, Wilhelmi and Hayden 2010, Sampson, Gronlund et al. 2013, Stocker 2014, Weber, Sadoff et al. 2015). Existing literature has demonstrated that those below the poverty line (Curriero, Heiner et al. 2002, O’Neill, Carter et al. 2009, Bezgrebelna, Aliyev et al. 2024), with education levels below high school(Curriero, Heiner et al. 2002, Bell, O’neill et al. 2008, Reid, O’Neill et al. 2009, Leap, Soled et al. 2024), the elderly(Knowlton, Rotkin-Ellman et al. 2009, Lin, Luo et al. 2009, Rosenthal, Kinney et al. 2014, Gronlund, Berrocal et al. 2015, Fuhrmann, Sugg et al. 2016), and individuals living alone(Uejio, Wilhelmi et al. 2011, Weber, Sadoff et al. 2015, Ji, Shin et al. 2025) are very sensitive to extreme heat. Infrastructures, like vegetation (Harlan, Brazel et al. 2006, Chen, Wang et al. 2014, Yu, Chen et al. 2024) and air conditioning installation rates,(Johnson, Wilson et al. 2009, Reid, O’Neill et al. 2009, Rey, Fouillet et al. 2009, Madrigano, Ito et al. 2015) are also considered contributing factors. This definition, rooted in a combination of underlying causes, signifies a pathway through vulnerability to policies that are cause-oriented. For example, Rachel et al. (Tony Wolf, Cottle et al. 2023) examined heat stress vulnerability in both elderly and young populations, explaining the impact of age-related physiological changes on heat vulnerability, which helps to minimize the deleterious impacts of extreme heat events in the elderly population. However, the vulnerability theory is general without a direct connection to heat mortality outcomes (Weber, Sadoff et al. 2015).
The other pathway is to examine the outcomes of extremes through heat-related mortality (Anderson and Bell 2011, Kanti, Alari et al. 2022, Ho, Shi et al. 2023). In contrast to the multidimensional assessment of heat vulnerability, mortality is a single-dimensional measurement but reflects the reality of heat impacts. This pathway, hence, indicates vulnerable population groups and regions with direct evidence of heat-related mortality (Conte Keivabu 2022). For example, Ballester’s research(Ballester, Quijal-Zamorano et al. 2023) quantified the mortality burden associated with high temperatures in Europe in 2022 and uncovered the risks by gender and age groups. While this approach complements vulnerability theory with evidence, this outcome-oriented pathway may struggle to delve deeply into the root causes of heat mortality and derive sufficient insights for targeted policies. The diverse characteristics, like socioeconomic factors, infrastructure conditions, and even population composition in different regions, are crucial for heat-related deaths(Madrigano, Ito et al. 2015, Son, Liu et al. 2019, Salvador, Gullón et al. 2023). Outcome-oriented studies, however, may not be able to link heat mortality with these factors. To this end, we anchor our analysis in the definition of heat vulnerability, taking heat-related mortality outcomes as evidence to bridge the gap between these two pathways, integrating multidimensional measurements of heat vulnerability with heat mortality, and to derive effective insights on how extreme heat impacts people.
Regression models have been adopted to identify the relationship between heat mortality and vulnerability measurements. For example, Rosenthal et al. used bivariate and multivariate ordinary least squares linear regression to assess the relationships between the mortality rate ratio and the vulnerability measures (Rosenthal, Kinney et al. 2014). They analyzed bivariate relationships between the mortality rate ratios and each of the heat-vulnerable variables. This regression method, however, only reveals the correlations between variables but cannot provide evidence for how changes in the vulnerability measurements, such as social, environmental, and infrastructure factors, directly influence heat mortality, which is often called causal effects. The effect of an individual factor should be separated from the effects of all other factors, while the interactions of factors, which indicate how one factor would moderate the effect of another factor, should be quantified as well. This is crucial in policymaking for adaptation to extreme heat, where understanding the impact of interventions or treatments is essential.
In this study, we examine how heat-related mortality across U.S. counties is shaped by a range of socioeconomic, environmental, and infrastructural factors. Specifically, we ask:
-
What are the most decisive vulnerability factors associated with heat mortality at the county level?
-
How do these factors vary by geographic region and racial composition? And
-
To what extent can infrastructural improvements, such as increased vegetation coverage and access to air conditioning, mitigate the adverse effects of socioeconomic disadvantage?
Grounded in vulnerability theory and prior empirical evidence, we hypothesize that counties with higher levels of poverty, lower educational attainment, limited vegetation cover, and insufficient air conditioning access are more likely to experience heat-related deaths. We expect that the relative importance of these factors varies across racial and spatial contexts; for instance, poverty may play a more dominant role in predominantly Black counties, while vegetation may be more critical to heat-related mortality in Hispanic-majority areas. Finally, we anticipate that infrastructure-related improvements can partially offset the effects of social disadvantage, consistent with our hypothesis that the values of diverse decisive factors, to some extent, determine the likelihood of heat mortality occurring in a county.
Here, we create a non-parametric generalized inference approach that links socioeconomic, environmental, and infrastructure data and heat mortality between 2010 and 2020 for counties across the United States. This approach enables identifying the causal effects of individual factors and examining the disparities in heat vulnerability at the county level. We adopt nine factors from heat vulnerability theory, including economic, demographic, climatic, and social variables, and conduct a county pair-matching process. Specifically, the pair-matching matches each heat-vulnerable county with demographically and structurally similar non-heat mortality counties based on the Mahalanobis distance across normalized vulnerability indicators, which allows for isolating the most decisive factor contributing to heat-related mortality by controlling for confounding attributes and identifying significant outliers. These county-level results provide cause-oriented evidence for the most critical determinants of heat mortality. Then, we characterize the spatial and racial distributions of these vulnerability determinants on a national scale to uncover disparities existing among regions and racial groups. To capture potential temporal shifts in the relationships between vulnerability factors and heat-related mortality, we incorporate panel data covering the years 2010 to 2020, which allows us to assess trends and transitions in effect sizes over time. Finally, we examine the interaction of social factors with infrastructure under extreme heat conditions to explain the rising importance of infrastructure in mitigating socioeconomic constraints on heat mortality.
Method
Vulnerable county
In CDC Wonder (Centers for Disease Control and Prevention, https://wonder.cdc.gov/), heat-related mortality among U.S. residents were identified using International Classification of Diseases. The selected case records pertaining to heat-related incidents comprised instances where the underlying cause of death or one of the contributing causes(Vaidyanathan 2020) was identified by ICD-10 codes X30 (excessive natural heat exposure), P81.0 (environmental hyperthermia of newborn), or T67 (effects of heat and light). Records containing ICD-10 code W92 (excessive heat exposure of man-made origin) anywhere on the death certificate were deliberately omitted to narrow down the selection to deaths specifically attributed to natural heat exposure. We obtain data for the years 2010–2020 based on the aforementioned selection criteria. However, the dataset designates values below ten as ‘Suppressed’. Therefore, we define counties with mortality data exceeding zero as heat ‘Vulnerable Counties’, zero as heat ‘non-heat mortality counties’.
It is important to note that the heat mortality data here is derived by aggregating separate statistics on various causes of death from death reports. Due to data limitations and the presence of unrecorded deaths, the heat mortality data is underestimated, and the actual incidence of heat mortality is likely more severe.
County level dataset
We construct a county-level dataset for the mainland of United States for the years 2010–2020 which includes 9 factors of each county and calculate the mean value for every factor in county level:
We obtain EHE data from CDC (https://ephtracking.cdc.gov/Applications/heatTracker/) for the years 2010–2020 in county level. The definition we select for extreme heat events is a consecutive period of at least 2 days when the daily Heat Index is above the 90th percentile of the reference. NDVI data is also collected from CDC, however, only census tract level data for the years 2014-2020 is provided. Therefore, we calculate the area-weighted average NDVIfor each county:
Where \({{NDVI}}_{i}\) is the county level NDVI, \({{NDVI}}_{j}\) is the Census Tract Level NDVI, \({{Area}}_{j}\) is the area corresponding to census j. Considering the negative correlation between NDVI and heat-related death, Lack of Vegetation (1-NDVI) is used as the LoV scale representing each county for calculation.
The levels of Poverty, SOLA, Aging, A&S, Edu and Pop are obtained from the American Community Survey (ACS) from the United States Census Bureau (https://data.census.gov/). We use ACS 5-years Estimates Subject Tables to get estimates for as many counties as possible on an annual basis. For Poverty, estimates are only available for the years 2012-2020, so we utilize data from these nine years for our study. And for Edu, we use the definition that population over 25 years old who did not graduate from high school, but due to the limitation of the data source, we have to resort to using data for all age groups during the period 2010-2014.
For AC (Households with Air Conditioning), due to the lack of data on county-level cooling device installations, we employ two assumptions for experimentation. The first assumption (in main text) is that the state-level rate of air conditioner non-installation is the same as that of its constituent counties (Sailor & Pavlova, 2003). We obtain the 2020 data on state-level air conditioner installation rates from US Energy Information Administration (EIA, https://www.eia.gov/consumption/residential/), The second assumption (detailed in the supplementary materials) is that homes built before 1960 do not have air conditioning installed (Weber, Sadoff et al. 2015). And we obtain this data through ACS.
County pair matching process
For each selected vulnerable county, we compare its population with the population of each non-heat mortality county. If the difference is within ±20%, then these non-heat mortality counties that meet the conditions are considered similar to the vulnerable county in terms of population scale.
Considering that the Mahalanobis distance requires all attributes to be within the same range, and in order to present the true distribution state of the data, we used the max-min normalization treatment for the nine attributes.
Where \({X}_{{norm}}\,\) is the normalized value, X is the original value, \({X}_{\min }\) is the minimum value in the dataset, and \({X}_{\max }\,\) is the maximum value in the dataset. This formula transforms the original data to a range between 0 and 1.
For each vulnerable county, the Mahalanobis distance is calculated one by one for the non-heat mortality counties that have passed the population screening. Based on the distribution characteristics of the matching counties (Table S1), we choose the top 50 to be selected in ascending order of Mahalanobis distances. These non-heat mortality counties are considered to match this vulnerable county in terms of the nine given attributes.
Where \({D}_{M}\,\) is the Mahalanobis distance. \({X}_{{norm}}\) is a vector of observations that includes nine attributes after normalization (a row in a dataset), μ is the vector of mean values of these nine attributes (mean of each column), \({\sum }^{-1}\) is the inverse covariance matrix of these nine attributes. The covariance matrix is a measure of how much each of the dimensions varies from the mean with respect to each other.
Anomalously high values are detected for the vulnerable county, and the attributes exhibiting such values are regarded as the decisive factors contributing to heat-related mortality in that county.
Where i is the index of the nine attributes, and j is the index of the non-heat mortality county, \({{\rm{Diff}}}_{{\rm{i}}}^{{\rm{j}}}\) represents how much each of the nine attributes of the vulnerable county exceeds the non-heat mortality county, \({{Xvul}}_{i}\) is the original data of the nine attributes of the vulnerable county, \({{Xinvul}}_{i}^{j}\) is the original data of the corresponding nine attributes of the every non-heat mortality county.
If and only if there is an “i” that meets the following conditions, the attribute represented by this “I” is regarded as the decisive factor, and the corresponding “j” represents the matching non-heat mortality county:
Where Mean is the average of the \({{Diff}}_{i}\), and Std is the standard deviation.
Bayesian spatial autoregressive model
To account for spatial dependencies inherent in heat-related mortality outcomes across counties, we implement a Bayesian Spatial Autoregressive (SAR) model. The SAR specification incorporates a spatially lagged dependent variable to explicitly model the influence of neighboring counties’ mortality rates, thus addressing potential biases arising from spatial autocorrelation.
The Bayesian SAR model takes the following form:
Where \(y\) represents heat-related mortality, \({Wy}\) is the spatial lag of the dependent variable based on a Queen contiguity weights matric, \(X\) denotes the matrix of covariates (including EHE, LoV, Poverty, AC, and demographic factors), \(\beta\) represents the vector of regression coefficients, and \(\rho\) captures the spatial dependence parameter.
Posterior distributions of the parameters are estimated using Markov Chain Monte Carlo (MCMC) sampling with a No-U-Turn Sampler (NUTS), implemented via PyMC. Priors are set as weakly informative normal distributions for \(\beta\) and a uniform distribution for \(\rho\) constrained within (−1, 1). We run four parallel chains with 2000 draws each, after 1000 tuning steps, ensuring convergence through visual trace inspections and r-hat statistics. Model inference is based on posterior means and 95% Highest Density Intervals (HDIs).
Temporal analysis of decisive factors
Due to improvements in various decisive factors with the development of society, we become curious about whether these improvements would lead to changes in the decisive factors over time. To further investigate the temporal changes in the decisive factors of heat-related deaths, we divide the studied period from 2010 to 2020, spanning a total of eleven years, into two periods, 2010–2015 and 2015–2020. In this case, we can ensure that data for each time period is available for a minimum of two years or more. We take the average of each attribute over six years, but for some attributes with insufficient data, we only take the average of the years with data in the corresponding group. More specifically, for the 2010–2015 group, we utilize the average values of LoV for the years 2014 and 2015, and the average data for Poverty covered the years 2012 to 2015. And as for air-conditioning data, since only state-level data for 2020 is provided, we use the 2020 state-level data for both groups. Subsequently, we calculate the county-level average changes for each decisive factor in each time period. To standardize their means within the range of 0-1, Population will be presented in millions, and EHE will be presented in hundred days. Additionally, we compute the proportion of vulnerable counties, dominated by each factor, in heat-related deaths. Observing the changes in both aspects over time will further assist us in understanding whether investing resources in each factor is worthwhile for achieving better outcomes.
Interaction model
Equation 7 shows the basic model that we are estimating. Because we are interested in interaction effects between social factors and infrastructure under extreme heat, we use the logged value of mortality rate from extreme heat (plus 10−5, reducing interference with 0 deaths). Due to privacy protection, specific data on deaths from 1 to 10 cannot be obtained. Therefore, we assume that the death data in this range are all at the maximum value of 9 to simulate the most severe extreme heat disaster. All data are treated as 1 to simulate the lightest scenario, and the results of three sets of random deaths are included in the supplementary materials (Tables S2-S5).
The only fixed control factor we use is the number of days of extreme heat events. Since the CDC provides detailed extreme heat events from May to September, we divide the number of extreme heat days for all counties by the total number of days from May to September (153 days) to calculate the proportion of extreme heat days. We then normalize this proportion using min-max normalization. Considering the high correlation between education and poverty in social factors, with poverty being almost the main cause of education distribution, we chose Poverty as the only social factor. Vegetation and air conditioning are both considered as infrastructure control factors. By controlling the value of α, we can change the structure of the model, meaning we can obtain a total of 7 models to study the interaction between social factors and infrastructure, as well as effects within infrastructure.
where \({\alpha }_{1}\), \({\alpha }_{2}\), \({\alpha }_{3}\) can be either 0 or 1, representing whether vegetation, air conditioning, and poverty are included in the model.
Structure equation modeling
To explore potential causal pathways linking social vulnerability, infrastructural adaptation, and heat-related mortality, we employed Structural Equation Modeling (SEM) as a robustness check and theoretical validation framework. Specifically, we constructed a path model in which poverty is treated as a key social vulnerability factor hypothesized to influence both infrastructural variables, namely, air conditioning (AC) coverage and vegetation, as measured by the Normalized Difference Vegetation Index (NDVI), as well as the heat-related mortality rate.
In this model, AC coverage and NDVI are conceptualized as infrastructural mediators that may attenuate the effects of poverty on mortality outcomes. In addition to examining these direct effects, we incorporated interaction terms to account for potential moderation effects, specifically the interactions between poverty and AC coverage (Poverty × AC) and between poverty and NDVI (Poverty × NDVI). Thus, the SEM model includes three primary direct effects (Poverty, AC, and NDVI) and two interaction effects (Poverty × AC and Poverty × NDVI), with poverty also modeled as influencing both AC and NDVI. The SEM was estimated using maximum likelihood estimation (MLE) with robust standard errors to account for potential heteroskedasticity. All statistical analyses were conducted using Python.
Results
County matching process
Between 2010 and 2020, 1616 U.S. counties recorded heat-related deaths (Fig. 1) according to CDC Wonder (Wonder online databases provided by the Centers for Disease Control and Prevention), indicating a substantial and geographically widespread mortality burden. These counties are referred to as heat-vulnerable counties in our analysis. The remaining counties, which did not record any heat-related deaths during this period, serve as a comparison group, which is defined as the non-heat mortality count.

a displays a distribution map of heat mortality at the county level in the United States, where varying colors represent the magnitude of death data. In the top-right corner are nine factors typically applied to traditional heat vulnerability assessments. b shows the county matching process, we identify counties with mortality data, labeled as “Vulnerable Counties” (e.g., County A), and those without mortality data, labeled as “ non-heat mortality county “ (e.g., Counties B to Z). We perform a county matching process based on mortality data for vulnerable counties. The matrix on the left represents factors related to heat vulnerability, while counties are listed at the top. The color intensity of each square reflects the magnitude of the factor for each county. Step (1) is population size filtering, where counties with similar population sizes are selected to mitigate population impacts. Step (2) calculates the Mahalanobis distance, identifying the top 50 non-heat mortality counties most similar to each vulnerable county. More detailed explanations are provided in the Method section and the Supplementary Information. Step (3) is outlier screening, sequentially evaluating the 50 counties in the matching pool for exceptionally high values until a suitable match is found. The identified non-heat mortality counties and their corresponding outlier are considered the matching county and the decisive factor for heat deaths in the vulnerable county, respectively.
Using a population-controlled matching framework and multidimensional vulnerability indicators derived from vulnerability theory, including (Table 1) extreme heat events (EHE), lack of vegetation cover (LoV), poverty, air conditioning access (AC), social isolation (SOLA), aging, aging and living alone (A&S), and education, we successfully match 1179 vulnerable counties with demographically similar counterparts. This matching process allows us to isolate decisive vulnerability factors contributing to heat mortality at the county level. The distribution of these matches reveals substantial regional variation in the determinants of heat-related deaths, underscoring the value of localized, factor-specific strategies for heat resilience.
Decisive factors of heat vulnerability
We define the factors that may lead to mortality in a vulnerable county as the decisive factors. Our results (Fig. 2a) show that AC (25.4%, 299), Poverty (23.8%, 351), Education (23.0%, 271), and LoV (17.6%, 208) are the decisive factors of heat-related deaths across county-level U.S., they account for a total of 95.8%, indicating that heat mortality is mainly driven by education, economic status, air conditioning, and vegetation in most of the counties. And in the Housing Assumption, AC (35.2%, 397), Poverty (23.8%, 269), Education (18.7%, 211), and LoV (198, 17.6%) are also the decisive factors of heat-related death, accounting for 95.3%. The decrease in the proportion of AC is foreseeable because we initially overlook the heterogeneity of air conditioning installation within the state, consequently resulting in underestimated results. Nevertheless, it is evident that irrespective of the variation in the methodological assumptions, AC, poverty, education, and LoV remain leading decisive factors. Particularly, heat exposure only accounts for 1.4% (in the Housing Assumption is 2.1%), which indicates that other social, economic, and infrastructure factors play more important roles in heat mortality.

a, b U.S. county-level impacts of the nine decisive factors associated with vulnerability to extreme heat are grouped into impacts on counties with mortality data (a, Vulnerable Counties) and impacts on counties with no mortality data (b, non-heat mortality counties). The vertical coordinates in the middle are the nine decisive factors we select that are frequently used in studies of extreme heat weather vulnerability; the left side represents the number of counties dominated by each factor, indicating the quantity of each factor; the right side represents the mean value of the relative difference between the counties dominated by each decisive factor and their matched counties (Diff), indicating the quality of each factor, and the error bars represent the 95% confidence intervals.
To further identify and demonstrate the distribution of decisive factors across the nation, we calculate the average ‘Diff’ of each decisive factor, the mean value of the relative difference between the counties dominated by each decisive factor and their matched counties. The results show that the distribution of the quality and quantity of differences in 9 decisive factors between vulnerable counties and their matched non-heat mortality counties is similar. The ‘Diff’ of decisive factors such as education, economic status, air conditioning, and vegetation exhibit substantial differences. The p-values of these four factors are all less than 0.005 compared to other factors. This observation suggests that education, economic status, air conditioning, and vegetation are critical, whether across all counties or within those counties where they dominate. The results are consistent when the assumption of housing conditions is taken into account (Fig. S1).
Similar to the distribution of decisive factors in vulnerable counties, in non-heat mortality counties (Fig. 2b), these four decisive factors also account for a large proportion of counties: AC (28.3%, 404), Poverty (21.8%, 311), Education (24.0%, 343), and LoV (11.7%, 167), a total of 85.8% in 1428 non-heat mortality counties. This result shows that education, economic status, air conditioning, and vegetation are the leading factors that make those counties stay away from heat mortality. However, it is notable that while the other factors experience fluctuations due to the increase in the base number, the “Living Alone” factor undergoes only marginal change, from 1 county to 8 counties (0.08% to 0.56%). This slight variation shows that “Living Alone” is almost unable to play a decisive role in heat-related deaths.
In contrast to vulnerable counties, the distribution of the number of decisive factors for non-heat mortality counties exhibits a slightly distinct pattern. Within the realm of non-heat mortality counties encompassing 9 decisive factors, only the quality of Population significantly differs from the rest (p-values less than 0.005 compared to other factors), with it being smaller in comparison to the others. However, among the remaining 8 factors, no statistically significant disparities are discernible. This observation suggests that, in non-heat mortality counties, the influence exerted by their decisive factors, excluding population size, is largely uniform, albeit with certain factors conferring disadvantages to a broader array of counties.
Poverty, lack of air conditioning, poor education, and lack of vegetation are the four decisive factors contributing to heat-related deaths in counties across the U.S. These 4 factors remain the most important even in areas where heat-related deaths were not detected or documented. This result suggests that for the majority of counties within the mainland of the United States, poverty, air conditioning, education, and vegetation play a decisive role in determining the heat vulnerability of counties. The influence of the other 5 factors, Aging, SOLA, A&S, Pop, and EHE, however, cannot be disregarded; they exert a notably substantial effect on heat-related fatalities in specific counties, despite their comparatively modest overall impact in the country. Therefore, it is evident that vulnerable counties exhibit susceptibility to extreme heat due to various factors, and a single definition cannot explain the vulnerability, highlighting the necessity of a detailed and territorial analysis of the targets.
Spatial disparities of decisive factors
We map the decisive factors which effectively display the relationship between ‘Value’, the original county-level mean value for each factor, and ‘Diff’, the mean value of the relative difference, (see Method), of the factors, as well as the heat mortality (Figs. 3, S2). The figure shows that in most counties, ‘Value’ and ‘Diff’ are either both above average or both below average, simultaneously indicating that the size of the ‘Value’ largely determines the size of ‘Diff’, which is consistent with our expectations. Counties with high heat-related mortalities, more than 10 deaths in the past decade, are predominantly (66.7%) situated within the range where both ‘Value’ and ‘Diff’ exceed the average. This result suggests that the severity of heat mortality is influenced by the values of the respective decisive factors.

These are 8 distribution maps of counties dominated by these 8 factors. Since ‘SOLA’ only dominates one county and cannot calculate averages, it is excluded from the figure. We compute the average values of the corresponding factors for vulnerable counties under each decisive factor and the average value of ‘Diff’. Using these two averages as intermediate values, we divided the counties into four groups (as shown in the legend in the middle), representing them on the map with points of corresponding colors. The size of each point indicates the number of heat-related deaths, with larger points representing higher death counts.
Counties where LoV is the decisive factor for heat mortality are mainly located in the southwestern U.S. The Southwest generally exhibits higher levels of LoV influence compared to the national average. Because other contributing factors perform relatively well in this region, the influence of LoV becomes especially pronounced. Heat mortality in counties in the west is dominated by Education or Poverty. Poverty is the decisive factor for heat mortality in counties in the southeast. This geographical pattern could be attributed to relatively high poverty levels in the eastern, especially southeastern U.S. However, AC shows a different pattern with a large proportion in the northeast. EHE, on the other hand, is the decisive factor for counties mainly in Texas, possibly due to the state experiencing particularly severe extreme heat. Aging, A&S, and Pop are unable to show evident patterns in geographic distribution due to a small number of counties.
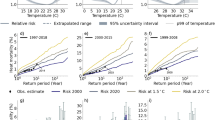
The Bayesian spatial autoregressive (SAR) model reveals significant predictors of heat-related mortality across U.S. counties (Fig. 4). Notably, the frequency of extreme heat events (β = −0.032, 95% HDI: [−0.072, −0.002]) and the prevalence of household air conditioning (β = −0.055, 95% HDI: [−0.086, −0.018]) were both associated with significantly reduced mortality, emphasizing the protective role of adaptive infrastructure. While poverty demonstrated a marginally positive association with mortality (β = 0.039), it did not meet the threshold for statistical significance. Population size was strongly positively associated with mortality (β = 0.407), likely reflecting higher exposure concentrations and baseline vulnerabilities. Additionally, the spatial lag term (β = 0.254, 95% HDI: [0.200, 0.311]) was significant, indicating that heat-related mortality in one county is significantly associated with mortality in its neighbors, highlighting spatial dependencies in heat vulnerability.

Each point represents the mean value of the posterior distribution for each predictor, and the horizontal lines denote the 94% HDI bounds (from the 3rd to the 97th percentile). A red dashed vertical line at zero indicates no association. Lag_Mortality represents the spatially lagged mortality, capturing the influence of neighboring counties’ mortality levels on the mortality outcomes across counties. Positive estimates indicate a positive association, while negative estimates indicate an inverse association with the outcome.
To examine the robustness of the effects of decisive factors on heat vulnerability of counties, we compute the averages of the nine decisive factors separately for vulnerable counties and all U.S. counties, respectively (Figs. 5a, S3). The mean values of each factor among vulnerable counties surpass the national averages, which shows that the performance of each decisive factor in vulnerable counties falls below the national average, such as poverty rate below the average, consistent with our hypothesis that the values of diverse decisive factors to some extent determines the likelihood of heat mortality occurring in the county.

The value of EHE has been divided by 100, and the population size has been divided by 1,000,000 to normalize the range between 0 and 1. And the Data expressed in percentage form, we have expressed as decimals. a compares the nationwide average values (steel blue) of nine mortality-related factors with the average values observed in the corresponding subset of vulnerable counties (light blue), where each subset includes only those counties for which the given factor was identified as the primary determinant of elevated mortality. b displays all the values of vulnerable counties for each attribute through a scatter plot on the chart, with vertical lines representing the range of values. The red box outlines the portions of each attribute that exceed the threshold, as defined in the methodology (Poverty is 20%, and the rest of the factors are county-level mean values of the U.S.). The blue fill indicates the proportion of vulnerable counties for each attribute that exceeds the threshold. Exceeding the threshold indicates that these counties perform poorly in the respective factors.
We also define nine thresholds for these nine factors, considering counties with values exceeding the thresholds to have worse performance. Referring to existing work, we define a county as impoverished if its poverty rate exceeds 20% (U.S. Census Bureau, n.d.; U.S. Department of Agriculture, n.d.; Congressional Research Service, 2018). For other factors, we use the more general average values as their thresholds (Cutter et al., 2003; FEMA, 2025; CDC, 2024). We calculate the proportion of vulnerable counties exceeding the threshold for each factor (Fig. 5b). The results show that the factors in more than 50% of vulnerable counties exceeds the thresholds, which strongly suggests a positive correlation between these nine factors and heat-related mortality—higher values indicating poorer performance, likely exacerbating the probability of heat-related deaths.
Racial disparities of decisive factors
In this study, we focus on three major racial and ethnic groups at the county level: non-Hispanic White, Black, and Hispanic populations, as they constitute the largest and most widely distributed demographic groups across the United States. This selection allows for statistically meaningful comparisons of heat-related vulnerability factors across regions. Other racial groups, including Asian, Native American, and multiracial populations, were excluded from race-stratified analyses due to smaller population sizes and limited spatial representation in the dataset, which may compromise analytical robustness.
We examine the racial disparities of the decisive factors to better address the heterogeneity of heat-vulnerable counties with different population compositions. We calculate the average proportion of each race at the county level, including Hispanic (11.95%), White (72.28%), and Black (8.38%). For each matched vulnerable county, should the proportion of a specific race exceed its average value, we classify it as predominantly inhabited by that specific race. We collect a total of 9 decisive factors and the respective proportions in vulnerable counties (Fig. 6a). Counties populated by White people account for the largest proportion of the vulnerable counties, followed by Black, and Hispanic comes last, which indicates that in areas where the proportion of White exceeds the average, there is a greater susceptibility to the mortality impact of extremely heat, while Hispanic populations are the least affected. The same pattern applies to counties with high mortality rates (Fig. S4). Such a racial disparity may be the result of Whites having a larger population base.

The horizontal scale represents the nine decisive factors and the vertical scale is the proportion of each factor. a mainly examines the proportion of each race within various factors. This proportion is calculated by dividing the number of counties for each race in each factor by the total number of counties for that factor. The dashed lines represent the average proportion of vulnerable counties for each of the three races. b primarily explores the distribution of the nine factors within each race. The proportion is determined by dividing the number of counties for each factor within each race by the total number of counties for that race. Table c displays the specific performance of eight factors of three races. We exclude Population and list two assumptions in AC, namely Housing and state-level AC coverage assumption. ‘Mean’ lists the proportion of counties where each race exceeds the national average for each factor. ‘Δ1’ lists the difference between each factor after min-max normalization and the national average, where positive values indicate performance below the national average and negative values indicate performance above the average. ‘Δ2’ lists the difference between the average of counties with performance below the national average and the national average.
We focus on the four decisive factors here, Edu, AC, LoV, and Poverty, to discuss the details of racial disparities. In counties where Edu is the decisive factor, there is a significant difference in the proportion of the three ethnic groups, with White being the most prominent and Hispanic performing the best. For counties whose heat mortality is mainly dominated by LoV, the proportion of White exceeds that of the other two ethnic groups, signifying a significant impact of air conditioning deficiency in counties where the predominant racial group is White. However, regardless of the great amount of White, LoV, and Poverty are led by other races. In counties where LoV serves as the decisive factor, the proportion of the Hispanic population is larger than others, indicating that heat mortality among Hispanics is most affected by vegetation coverage. The influence of Poverty on heat-related mortality in Black and White counties is nearly equal; both exceed the average level, but Black has a slight advantage. This disparity underscores the necessity for prioritized attention and support toward the poverty situation affecting Black individuals.
Due to the small dataset, there are significant differences in individual factors, EHE, Aging, SOLA, A&S, and Pop. However, this does not affect us from drawing a unified conclusion: the proportion of White is significantly greater than the other two ethnic groups with regard to EHE, SOLA, Aging, and Pop. The substantially higher proportion of White individuals compared to other racial groups has a lot to do with their large population base, but it also speaks to the fact that White needs more attention in this area in terms of the absolute numbers of all three racial groups. However, Black performs much worse in A&S even under such dire circumstances, which means that when considering A&S, Black is the most urgently in need of assistance.
The reason for the consistently high proportion of Whites is speculated to be the overall high representation of the White population in the United States. This results in a high proportion of Whites across various factors. To eliminate the influence of population size among different races, we calculate the proportion of various factors within each race (Fig. 6b). After excluding the impact of population size and the number of counties, the more prominent decisive factors within each race are revealed. LoV takes the lead with 35.5% of the Hispanic group, becoming the most influential factor affecting heat-related mortality. The primary factor contributing to heat-related mortality among White people is the absence of air conditioning, representing 32.31% of cases. Meanwhile, Poverty, with 44.58% of Black people, stands out as the highest among all 27 factors across the three races, further demonstrating the profound impact of high poverty rates on heat-related mortality within the Black population.
After eliminating the influence of population, the results between races also appear different, with the most significant impact being the reduction in the white population base. The most significant differences between races are mainly concentrated on LoV, AC, and Poverty. When considering counties with a predominant Hispanic population, the impact of poverty is minimal among the four decisive factors. Vegetation and air conditioning installation rates are crucial, especially vegetation, which far exceeds the impact on other racial groups. This may contribute significantly to heat-related deaths in these counties. In contrast, poverty is exceptionally important for the Black population, but relatively speaking, air conditioning has a smaller impact on Black individuals. A large variation in air conditioning installation rates exists for the White population, but at the same time, it has a relatively small impact compared to vegetation. Education has a consistently large impact on all three racial groups, but the Black population has a slight lead over the other two races.
We show the values of decisive factors and their contributions to heat mortality (Fig. 6, Table c), aiding our understanding of the importance of mitigating these factors to reduce heat-related deaths. Population is excluded from consideration as it can be seen as an inherent characteristic of a county. Here, we present the disparities between two hypotheses of the AC: state-level AC coverage assumption and Housing, for a robust understanding of AC disparities. We initially compute the percentage and extent to which each factor exceeds the national average for each race. The results show that for Hispanic populations, 72% of counties have LoV exceeding the average, significantly surpassing other factors. This gap between LoV and other factors suggests the critical role of LoV in counties predominantly inhabited by Hispanic, where increasing vegetation coverage can effectively mitigate heat-related mortality. Regarding White populations, the prevalence of elderly populations, Aging and A&S, is of the top place in counties, exceeding 50%, and significantly surpassing other factors except Housing, with the performance of the alternative air conditioning assumption, state-level AC coverage assumption, notably superior. Thus, to further explore the impact of air conditioning and aging on Whites, we further calculate the degree to which the average of counties exceeding the mean surpasses the national average. The results show that Housing and state-level AC coverage assumption significantly exceed A&S and Aging, indicating that counties affected by aging are more widespread, but the situation is more severe in counties with lower air conditioning penetration rates, which emphasizes the importance of caring for the elderly while improving air conditioning availability. Poverty constitutes a significant portion (70%) and performs poorly among Blacks, consistent with its role as the most decisive factor in Black heat-related mortality. Therefore, reducing poverty rates appears to be the most directly effective solution for Blacks. However, EHE performs similarly poorly among Blacks, even worse than Poverty, contrary to its performance in vulnerable counties. We speculate that this contrast is because there are currently effective measures in place to address extreme heat events (EHE) in general.
Evolution of decisive factors
We examine the evolution of decisive factors for heat vulnerability by partitioning the eleven-year timeframe into two distinct periods: 2010-2015 and 2015-2020. We compare the changes in the averages of the 9 decisive factors between these two periods to make the results comparable. (Figs. 7, S5) It must be pointed out that due to the lack of data on the rate of air conditioner non-installation at the county level, the data used for the two assumptions for air conditioning coverage in this study differ. This prevents a unified result from covering every factor. But we are able to derive several relatively consistent findings under the two assumptions.

This dumbbell plot shows the time-varying change of the 9 decisive factors. LoV is 1-NDVI, which indicates that the average NDVI has shown an increase over the past period. Standards in 2015–2020 (large dots) compared with 2010–2015 (small dots) explained the trend of the mortality data (year 2015–2020 is larger than 2010–2015). The colors indicate the direction of change. In the case of a missing yearly value (Proportion of households without air conditioning), we used the closest available yearly value.
First, the changes in the four decisive factors are consistent. The number of counties dominated by Poverty and Education has been decreasing over time, with education being particularly noticeable. On the other hand, counties dominated by AC and LoV exhibit a gradual upward trend, with AC being particularly pronounced. The trend of the 4 decisive factors indicates that over the course of these 11 years of development, although they still persist as the four decisive factors, the overall trend of decisive factors is gradually shifting from social factors, education, and poverty to infrastructure factors, air conditioning, and vegetation.
Second, through a comparative examination of the alterations in the mean values of each factor, it becomes evident that, apart from discrepancies in AC values attributable to data limitations, both poverty rates and educational attainment demonstrate a positive trajectory over the past decade. However, population growth and the acceleration of aging will lead to an increase in single-person and elderly households. Although the resulting contribution to heat-related mortality is not particularly significant when considered alongside other factors, it remains an important aspect that cannot be overlooked.
The evolution of the social factors, Poverty and Edu shows a high degree of consistency with the pattern in their respective mean values, which suggests that reducing the poverty rate and increasing educational attainment have practical and effective effects in reducing heat-related deaths. Although LoV shows a decrease between the two time periods, the number of counties increases. The effects presented by AC in the two assumptions are different, indicating that while the main factors are changing, the current improvements in infrastructure do not appear to be significant in reducing heat-related deaths. The impacts of aging and population growth, although not significant, are still of concern. It is noteworthy to find that the importance of infrastructure and nature in mitigating extreme heat has been increasing over the past decade. Nonetheless, socio-economic factors still persist as the predominant and most crucial interventions.
Interaction between social factors and infrastructure
We conduct a multivariate panel regression (Table 2a) on mortality rate, EHE, AC, NDVI, and poverty to examine the impacts of interactions between social factors and infrastructure on heat-related mortality. In this study, we define ‘infrastructure’ as encompassing both built systems (e.g., air conditioning) and nature-based systems (e.g., vegetation coverage), in alignment with established vulnerability frameworks. Due to the high correlation between educational attainment and poverty rate, we only select poverty as a representative factor for social factors. As shown in Table 1 below, models 1, 2, and 3 demonstrate the impacts of AC, NDVI, and Poverty on heat-related mortality, respectively. The heightened vulnerability is indicated by an elevated incidence of extreme heat events (EHE) as well as an increased poverty rate (Model 3). Similarly, the heat mortality, due to extreme heat, diminishes with the expansion of vegetation (NDVI) (Model 2). The widespread use of air conditioning (AC, pAC = 0.006) also significantly contributes to reducing heat-related mortality (Model 1).
We add AC and NDVI in Models 5 and 6, respectively, as the only additional infrastructure factors while keeping Poverty as the only social factor to understand the interactions between social factors and infrastructure on heat mortality. The results show that the importance of infrastructure remains nearly unchanged (pNDVI = 0.000, pAC = 0.010) whether the social factor (Poverty) is included or not. Instead, Poverty loses its dominant role in heat mortality due to the influence of AC (pPoverty > 0.05). These results demonstrate that infrastructure maintains its paramount importance even under the influence of social factors. Improving 1% in infrastructure can complement the negative effect of 1.16% socioeconomic constraints on heat mortality.
As social factors do not significantly alter the impact of infrastructure, our attention is drawn to the differential effects of infrastructure factors. Model 4 includes two infrastructure factors, HVAC and vegetation. The results reveal that the impact of AC on heat-related mortality changes from significant to nonsignificant under the influence of vegetation (pAC = 0.006 to pAC = 0.091). Hence, a 1% increase in vegetation is found to be comparable to a 1.5% increase in air conditioning installation in terms of reducing heat-related mortality. This shift indicates that, among infrastructure factors, the impacts of vegetation on heat-related mortality surpass those of air conditioning, and improving vegetation is more effective in mitigating heat-related deaths regardless of socioeconomic constraints.
Model 7 incorporates all social and infrastructure factors to assess whether social factors can override the effects of infrastructure solutions. The results of the statistics test for Poverty and NDVI indicate that vegetation exerts a stronger influence on heat-related mortality compared to poverty (pPoverty = 0.050, pNDVI = 0.000). As such, among the factors affecting heat-related mortality rates, the impact of infrastructure surpasses that of social factors. Comparing Model 7 with Model 4, we find that the impact of air conditioning on heat-related mortality is further reduced, while NDVI’s impact is further increased when Poverty is added as the sole additional social factor. This transformation of infrastructural impacts on heat mortality suggests that the interaction between social factors and infrastructure promotes interactions between infrastructure solutions. Specifically, the presence of poverty widens the gap between AC and NDVI, meaning that the influence of AC is gradually diminishing while the influence of NDVI is increasing. Hence, among the factors influencing heat-related mortality, the impact of infrastructure is greater than that of social factors. However, there is a significant polarization between infrastructure factors, influenced by social factors.
The results of the structure equation modeling (SEM) (Table 2b) support the findings from the regression models. Air conditioning coverage (standardized path coefficient = −0.09, p < 0.01) and vegetation (standardized path coefficient = −0.18, p < 0.05) were found to significantly reduce heat-related mortality, while poverty exhibited an insignificant positive direct effect on mortality (standardized coefficient = +0.014, p > 0.05). Additionally, poverty had significant interaction effects on mortality through its interplay with infrastructure, especially vegetation (standardized path coefficient = −0.06, p < 0.01), highlighting its dual role as both a direct and structural constraint. These findings not only confirm the consistency of our results across methodological frameworks but also offer theoretical insight into the mediating role of infrastructure in the relationship between socioeconomic vulnerability and heat-related mortality. The use of SEM thus serves both as a robustness check and as a complementary causal framework in this study.
Discussion
In this study, we create a non-parametric inference model to bridge the measurements in vulnerability theory and heat mortality through experiments on a total of 1179 heat-vulnerable counties. The results show that vegetation, education, air conditioning installation rates, and poverty levels are the four decisive factors. In this section, we embark on an in-depth discussion centered around the pathways of these dominant factors to heat mortality. In contrast to the other three factors, the definition of air conditioning is relatively narrow. Therefore, our primary focus here is on the pathways of the other three dominant factors on heat-related deaths, with the discussion of these three factors also encompassing the influence of air conditioning.
Multifaceted impacts of poverty to heat-related mortality disparities
Poverty affects the acquisition of resources in various ways, thereby influencing vulnerability (Blaikie, Cannon et al. 1994, Leichenko and Silva 2014). Existing research demonstrates that mortality rates associated with temperature, including heat-related deaths, were higher among people residing in nursing homes, and a large effect was also detected for hospitalized subjects (Stafoggia, Forastiere et al. 2006). This implies that the environmental conditions and infrastructure of Healthcare Facilities (HCF) significantly impact heat-related mortality rates. Unfortunately, in low- and middle-income regions, deficiencies in the environmental conditions in HCF seem continuously existing (Cronk and Bartram 2018), which will exacerbate the risk of infections and further lead to an increase in heat-related mortality rates. Also, in numerous locations, the ability of impoverished households and communities to prepare for climate-related threats is hindered by factors such as insufficient income, time constraints, etc (Mileti 1999). The vulnerability of households arises from both their limited financial approaches to prepare for climate-related impacts and the inadequate institutional capacity to provide disaster preparation resources in a manner that is accessible and beneficial to them (Thomas, Hardy et al. 2019).
Another influence of Poverty (Thomas, Hardy et al. 2019) is that people living in poverty often face a higher susceptibility to the impacts of extreme heat events. Places where poor people reside often exhibit higher population density that may lead to excessive crowding. In extreme heat, the human body relies on mechanisms like sweating to dissipate heat and maintain a stable temperature (Wendt, Van Loon et al. 2007, Gagnon and Crandall 2018). However, in crowded living conditions, inefficient air circulation and elevated environmental heat can reduce the body’s ability to cool down effectively (Jana, Sarkar et al. 2022). Additionally, crowded living environments may lack sufficient water resources (McGranahan and Songsore 1994, von Seidlein, Alabaster et al. 2021), making it more challenging for residents to replenish fluids in high-temperature settings, thereby increasing the risk of heat exhaustion and heatstroke. And their residential buildings may be more prone to exposing them to extreme heat events. Low-income individuals may find it challenging to afford the expenses associated with purchasing a house (Herbert and Belsky 2008). However, due to limited availability in the rental market, there are fewer affordable vacancy rates for this demographic. This situation leaves people in poverty at various health risks, such as pests, mold, water leaks, and inadequate heating or cooling systems (Hernández 2016, Studies 2020).
Armani’s research (Hawes, Smith et al. 2019) on racial, poverty, and physical activity disparities suggests that Black individuals are more likely to fall below the poverty line and experience poorer health conditions. Black Americans are predominantly concentrated in the Southern region of the United States (KIANA COX 2022), where the poverty rate has consistently been higher than in other areas (Baker 2019). This spatial pattern results in more Black individuals facing difficulties in accessing healthcare facilities when afflicted by illnesses triggered by extreme heat, leading to heat mortalities. In addition, Black individuals have been shown to be more likely to reside in urban areas (Borrell and Hatch 2005, KIANA COX 2022), exacerbating their housing burdens and consequently increasing their vulnerability to heat-related fatalities when exposed to extreme heat. These observations highlight the prevalence of poverty among Black communities, explaining the disproportionate impacts of poverty on heat-related mortality in the Black population. Among the nine factors within the Black community, Poverty stands out as one of the factors with the highest deviation from the average, and it exhibits significant differences from the other factors (P > 0.005, except EHE), which provides evidence of poverty being the primary influencing factor among the Black population.
Similar but with slight nuances in disparities of education
Education has long been proven to be a significant factor influencing vulnerability (Rosenthal, Kinney et al. 2014, Elo 2009). Those with lower education are anticipated to have shorter life expectancies, experience poorer health, and exhibit reduced resilience to exogenous stressors (Elo 2009, Hummer and Hernandez 2013). For instance, individuals with lower educational attainment are more prone to engaging in unhealthy behaviors such as smoking, having eating disorders, consuming alcohol, or developing health conditions like cardiovascular disease, obesity, and diabetes (Link and Phelan 1995, Son, Liu et al. 2019). These health conditions and behaviors are associated with impaired thermoregulatory function, leading to decreased resilience to extreme temperatures (Cui and Sinoway 2014). An observable educational gradient exists in the seasonal pattern of mortality, suggesting that individuals with a lower education level are less resilient to environmental stressors (Rau 2007).
The spatial distribution of education attainment aligns with the spatial patterns of poverty. Existing research suggests that Black individuals possess lower educational attainment levels on average compared to White counterparts (David Elliott 2020), and are more likely to be enrolled in public insurance programs, suffer from obesity, and be current smokers (Hawes, Smith et al. 2019). Disparities between Hispanic and White populations similarly exist but are comparatively smaller than those between Black and White demographics (David Elliott 2020). This finding provides evidence for the predominance of Black individuals and the minority presence of White individuals in counties where education is the decisive factor. Our results that only the number of White individuals attaining a high school diploma exceeds the national average, while Black individuals fall below the average by a greater margin than Hispanic individuals (Fig. 5, Table c), also help explain racial disparity in heat mortality. Nonetheless, with the progression of educational endeavors, racial disparities have shown a gradual reduction in most states since 2005 (David Elliott 2020), highlighting the importance of education in addressing heat mortality across racial groups.
The uniqueness of vegetation in the Western U.S. and the hispanic
The major infrastructural factor in mitigating heat mortality is the nature-based infrastructure, vegetation (Chen, Wang et al. 2014). Urban greening plays a significant role in cooling cities (Bowler, Buyung-Ali et al. 2010, Aram, García et al. 2019). In a study conducted in New York City (Susca, Gaffin et al. 2011), areas with built infrastructure corresponded to the highest temperatures, while areas with the most vegetation corresponded to the lowest temperatures. In addition, urban greening can effectively alleviate the heat island effect and its associated negative impacts (Akbari, Pomerantz et al. 2001). Experiments conducted in Japan suggest that parks with abundant vegetation can reduce the air conditioning energy consumption of surrounding buildings (Ca, Asaeda et al. 1998). Green spaces not only provide assistance to ecosystems but also contribute to reducing heat-related mortality through their positive impact on psychological well-being and social cohesion. Evidence suggests that engaging in physical activities in green spaces can yield psychological and physiological benefits for individuals (Markevych, Schoierer et al. 2017). Given that high-temperature environments can have a range of effects on mental health, with an increased risk of suicide being among the most significant (Thompson, Hornigold et al. 2018), the construction of green spaces can help mitigate psychological health issues associated with elevated temperatures, thereby reducing the impact of extreme heat. In addition, the construction of green spaces can improve ecosystem services and well-being, strengthen social cohesion, reduce social isolation, and consequently mitigate the impact of extreme heat (Davids, Rouget et al. 2021).
Hispanic populations in the United States tend to concentrate in the Southern and Western regions (Bean and Tienda 1988), which are characterized by an abundance of grasslands and desert terrain. Hence, Hispanic communities in these areas may reside in environments that are more arid and exhibit relatively sparse vegetation coverage. This phenomenon contributes to insufficient cooling of urban areas during extreme heat events, exacerbated by the scarcity of green spaces. Moreover, the limited vegetation in these regions attenuates the positive impacts of green spaces on psychological well-being and social cohesion (Markevych, Schoierer et al. 2017), thereby amplifying the prominent role of vegetation conditions in shaping patterns of heat-related mortality. The vegetation distribution is consistent with observed disparities in counties where vegetation conditions predominate, reflecting both spatial and racial disparities. Our research on vegetation indicates that among the three races, only the vegetation levels of Hispanic individuals are below the national average. Here, we use the complementary of LoV in the analyses, which means that a higher value indicates a lower level of NDVI. The deviation is significantly greater than other factors, except for population-related factors, for heat-related mortality in the Hispanic population (Fig. 5, Table c). These two findings further emphasize the critical need to address LoV disparities among the Hispanic population, both inter-racially and intra-racially.
Related response strategies
Our findings suggest that effective strategies to reduce heat-related mortality must prioritize interventions among socioeconomically disadvantaged groups, with particular attention to Black and Hispanic populations disproportionately exposed to heat risk through multiple vulnerability pathways. Local governments should direct resources to historically marginalized Black communities in the Southern United States, where poverty rates remain persistently high and access to resilient housing and healthcare infrastructure is limited. Expanding subsidized programs for energy-efficient air conditioning installations, combined with targeted retrofitting of aging housing stock to improve thermal resilience, is essential. These efforts should be coupled with strengthening healthcare facility infrastructure in low-income areas to ensure continuity of care during extreme heat events.
Given the observed role of educational attainment in mediating vulnerability, programs aimed at improving heat awareness, health literacy, and adaptive capacity among individuals with lower education levels are also critical. Community-based outreach initiatives that deliver culturally and linguistically tailored information to Black and Hispanic populations, particularly in urban areas, can enhance protective behaviors during heat waves and promote the utilization of cooling resources.
In addition, the pronounced vegetation disparities identified among Hispanic populations in the arid Southern and Western regions highlight the urgent need for nature-based adaptation strategies. Federal and local agencies should prioritize urban greening projects, such as establishing parks, increasing tree canopy coverage, and restoring natural landscapes, in Hispanic-majority communities where vegetation coverage is severely limited. These initiatives would not only reduce ambient temperatures but also address psychosocial stressors exacerbated by heat exposure, ultimately contributing to reductions in heat-related mortality. Strategic placement of green infrastructure in vulnerable neighborhoods, combined with policies to maintain equitable access, is crucial to ensure that ecosystem services benefit those most at risk.
Limitations and future works
Limitations
The ecological nature of the study, coupled with the absence of individual-level health data, limits the ability to draw causal inferences at the household level. The reliance on county-level aggregated data prevents us from capturing within-county heterogeneity and individual-level susceptibility factors. While our analysis is policy-relevant at the regional scale and aligns with the resolution of publicly available data, it cannot replace person-level assessments of risk.
Potential underreporting in CDC heat mortality records, particularly in rural or resource-limited areas, may bias mortality estimates. The heat mortality data used here is derived by aggregating separate statistics on various causes of death from death reports. Due to data limitations and the presence of unrecorded or misclassified deaths, particularly in rural and under-resourced regions, the heat mortality data likely underestimates the true burden. We therefore interpret the observed mortality patterns as conservative estimates.
Another limitation concerns the assumption that state-level air conditioning (AC) coverage rates are applicable to all counties within a state, which may obscure important spatial heterogeneity in access and usage. Moreover, while we used the housing construction year as a proxy for AC access, we recognize that many homes built before 1960 have likely undergone retrofits, potentially weakening this proxy. In addition, our measure of AC presence does not differentiate between central and window units, which vary significantly in cooling efficiency. The mere presence of AC does not guarantee its usage, particularly among households facing high energy burdens or utility shutoffs, leading to a possible overestimation of AC’s protective effects. While this study seeks to infer causal drivers of heat-related mortality through a non-parametric matching framework, unmeasured confounding factors, such as pre-existing health conditions and the urban heat island effect, are not directly included due to data limitations. Although we incorporated proxy variables (e.g., age, single-person households, vegetation cover) to reduce potential confounding, these cannot fully substitute for individual-level health or environmental data.
An additional methodological limitation is the lack of explicit consideration of spatial autocorrelation. While our non-parametric matching framework reduces confounding by comparing counties with similar socio-environmental profiles, it does not model the spatial dependence that may exist across neighboring counties. Given the known spatial clustering of vulnerability factors, such as poverty, vegetation cover, and infrastructure, unmeasured spatial effects may influence our findings. Although our findings provide valuable insights for understanding heat vulnerability across U.S. counties, their generalizability to other countries or regions is limited. The results are based on U.S.-specific socioeconomic, infrastructural, and climatic contexts.
Future work
To address the limitations outlined above, future research should pursue several key directions. Incorporating household-level survey data or electronic health records would enable more precise assessments of individual vulnerability to extreme heat and strengthen causal inference. Fine-scale urban metrics, such as land surface temperature, detailed green space distribution, and built environment characteristics, should also be integrated into future analyses to better capture intra-county variations and account for the urban heat island effect.
To further strengthen causal inference, future studies could leverage natural experiments, such as power outages during extreme heat events, to estimate the impacts of infrastructural disruptions on heat-related mortality with greater precision. These experimental designs would provide stronger identification strategies and complement the structural insights derived from observational matching approaches.
Although this study’s framework is U.S.-specific, the methodological approach, linking non-parametric causal inference with vulnerability indicators, is broadly adaptable. Future research could extend this framework to other regional contexts, provided appropriate local data are available, facilitate cross-regional comparisons and broaden the global understanding of heat vulnerability under varying climatic and socioeconomic conditions.
Data availability
All data generated or analyzed during this study are not included in this submission but are publicly available in Centers for Disease Control and Prevention (CDC: https://www.cdc.gov/), American Community Survey (ACS) from the United States Census Bureau (https://data.census.gov/) and US Energy Information Administration (EIA, https://www.eia.gov/consumption/residential/).
References
Akbari H, Pomerantz M, Taha H (2001) Cool surfaces and shade trees to reduce energy use and improve air quality in urban areas. Sol energy 70(3):295–310
Anderson GB, Bell ML (2011) Heat Waves in the United States: Mortality Risk during Heat Waves and Effect Modification by Heat Wave Characteristics in 43 U.S. Communities. Environ Health Perspect 119(2):210–218
Aram F, García, EH, E Solgi E, Mansournia S (2019). Urban green space cooling effect in cities. Heliyon 5(4)
Baker RS (2019) Why is the American South Poorer? Soc Forces 99(1):126–154
Ballester J, Quijal-Zamorano M, Méndez Turrubiates RF, Pegenaute F, Herrmann FR, Robine JM, Basagaña X, Tonne C, Antó JM, Achebak H (2023) Heat-related mortality in Europe during the summer of 2022. Nat Med 29(7):1857–1866
Bean FD, Tienda M (1988) The hispanic population of the United States, Russell Sage Foundation
Bell ML, O’neill MS, Ranjit N, Borja-Aburto VH, Cifuentes LA, Gouveia NC (2008) Vulnerability to heat-related mortality in Latin America: a case-crossover study in Sao Paulo, Brazil, Santiago, Chile and Mexico City, Mexico. Int J Epidemiol 37(4):796–804
Bezgrebelna M, Aliyev E, Amoah YS, Atkinson D, Chiblow SB, Daley M, Drolet JL, Fletcher A, Harper S, Kenny GP (2024) Climate change, poverty, and health: A scoping review of the Canadian context. J Clim Change Health 20:100348
Blaikie P, Cannon T, Davis I, Wisner B (1994) The Challenge of Disasters and Our Approach
Borrell LN, Hatch SL (2005) Racial/Ethnic Minorities and Health: The Role of the Urban Environment. Handbook of urban health: Populations, methods, and practice, Springer: 63-77
Bowler DE, Buyung-Ali L, Knight TM, Pullin AS (2010) Urban greening to cool towns and cities: A systematic review of the empirical evidence. Landsc urban Plan 97(3):147–155
Ca VT, Asaeda T, Abu EM (1998) Reductions in air conditioning energy caused by a nearby park. Energy Build 29(1):83–92
Campbell S, Remenyi TA, White CJ, Johnston FH (2018) Heatwave and health impact research: A global review. Health place 53:210–218
Carleton TA, Hsiang SM (2016) Social and economic impacts of climate. Science 353(6304):aad9837
Centers for Disease Control and Prevention (2024) CDC/ATSDR Social Vulnerability Index (SVI). https://www.atsdr.cdc.gov/placeandhealth/svi/index.html
Chen D, Wang X, Thatcher M, Barnett G, Kachenko A, Prince R (2014) Urban vegetation for reducing heat related mortality. Environ Pollut 192:275–284
Cheng W, Li D, Liu Z, Brown RD (2021) Approaches for identifying heat-vulnerable populations and locations: A systematic review. Sci Total Environ 799:149417
Congressional Research Service (2018) The 10-20-30 provision: Defining persistent poverty counties. https://www.congress.gov/crs-products/r45100
Conte Keivabu R (2022) Extreme temperature and mortality by educational attainment in Spain, 2012–2018. Eur J Popul 38(5):1145–1182
Cronk R, Bartram J (2018) Environmental conditions in health care facilities in low-and middle-income countries: coverage and inequalities. Int J Hyg Environ health 221(3):409–422
Cui J, Sinoway LI (2014) Cardiovascular responses to heat stress in chronic heart failure. Curr heart Fail Rep. 11:139–145
Curriero FC, Heiner KS, Samet JM, Zeger SL, Strug L, Patz JA (2002) Temperature and mortality in 11 cities of the eastern United States. Am J Epidemiol 155(1):80–87
Cutter SL, Boruff BJ, Shirley WL (2003) Social vulnerability to environmental hazards. Soc Sci Q 84(2):242–261. https://doi.org/10.1111/1540-6237.8402002
David Elliott SW, Forum Agenda (2020) This is what the racial education gap in the US looks like right now. from https://www.weforum.org/agenda/2020/10/us-education-racial-equality-stanford-data-project/
Davids R, Rouget M, Burger M, Mahood K, Ditlhale N, Slotow R (2021) Civic ecology uplifts low-income communities, improves ecosystem services and well-being, and strengthens social cohesion. Sustainability 13(3):1300
Edo GI, Itoje-akpokiniovo LO, Obasohan P, Ikpekoro VO, Samuel PO, Jikah AN, Nosu LC, Ekokotu HA, Ugbune U, Oghroro EEA (2024). Impact of environmental pollution from human activities on water, air quality and climate change. Ecological Frontiers
Elo IT (2009) Social class differentials in health and mortality: Patterns and explanations in comparative perspective. Annu Rev Sociol 35:553–572
Federal Emergency Management Agency (2025). National Risk Index: Technical documentation. https://www.fema.gov/sites/default/files/documents/fema_national-risk-index_technical-documentation.pdf
Fuhrmann CM, Sugg MM, Konrad CE, Waller A (2016) Impact of extreme heat events on emergency department visits in North Carolina (2007–2011). J Community Health 41:146–156
Gagnon D, Crandall CG (2018) Sweating as a heat loss thermoeffector. Handb Clin Neurol 156:211–232
Gronlund CJ, Berrocal VJ, White-Newsome JL, Conlon KC, O’Neill MS (2015) Vulnerability to extreme heat by socio-demographic characteristics and area green space among the elderly in Michigan, 1990–2007. Environ Res 136:449–461
Harlan SL, Brazel AJ, Prashad L, Stefanov WL, Larsen L (2006) Neighborhood microclimates and vulnerability to heat stress. Soc Sci Med 63(11):2847–2863
Hawes AM, Smith GS, McGinty E, Bell C, Bower K, LaVeist TA, Gaskin DJ, Thorpe Jr RJ (2019) Disentangling race, poverty, and place in disparities in physical activity. Int J Environ Res public health 16(7):1193
Herbert CE, ES Belsky ES (2008) The homeownership experience of low-income and minority households: A review and synthesis of the literature. Cityscape: 5–59
Hernández D (2016) Affording housing at the expense of health: exploring the housing and neighborhood strategies of poor families. J Fam Issues 37(7):921–946
Ho JY, Shi Y, Lau KK, Ng EY, Ren C, Goggins WB (2023) Urban heat island effect-related mortality under extreme heat and non-extreme heat scenarios: A 2010–2019 case study in Hong Kong. Sci Total Environ 858:159791
Hummer RA, Hernandez EM (2013) The effect of educational attainment on adult mortality in the United States. Popul Bull 68(1):1
Jana A, Sarkar A, Bardhan R (2022) Evaluating well-being in low-income mass housing in India with specific reference to natural ventilation. Area Dev policy 7(3):267–292
Ji H, Shin SH, Coronado A, Lee HY (2025) Extreme heat, functional disability, and social isolation: risk disparity among older adults. J Appl Gerontol 44(4):561–570
Johnson DP, Wilson JS, Luber GC (2009) Socioeconomic indicators of heat-related health risk supplemented with remotely sensed data. Int J Health Geogr 8:1–13
Kanti FS, Alari A, Chaix B, Benmarhnia T (2022) Comparison of various heat waves definitions and the burden of heat-related mortality in France: Implications for existing early warning systems. Environ Res 215:114359
Kiana Cox, CT (2022) Race is Central to Identity for Black Americans and Affects How They Connect With Each Other. from https://www.pewresearch.org/2022/04/14/black-americans-place-and-community/
Knowlton K, Rotkin-Ellman M, King G, Margolis HG, Smith D, Solomon G, Trent R, English P (2009) The 2006 California heat wave: impacts on hospitalizations and emergency department visits. Environ health Perspect 117(1):61–67
Kravchenko J, Abernethy AP, Fawzy M, Lyerly HK (2013) Minimization of heatwave morbidity and mortality. Am J Prev Med 44(3):274–282
Leap SR, Soled DR, Sampath V, Nadeau KC (2024). Effects of extreme weather on health in underserved communities. Annals of Allergy, Asthma & Immunology
Leichenko R, Silva JA (2014) Climate change and poverty: vulnerability, impacts, and alleviation strategies. Wiley Interdiscip Rev: Clim Change 5(4):539–556
Lin S, Luo M, Walker RJ, Liu X, Hwang S-A, Chinery R (2009) Extreme high temperatures and hospital admissions for respiratory and cardiovascular diseases. Epidemiology 20(5):738–746
Link BG, Phelan J (1995) Social conditions as fundamental causes of disease. Journal of health and social behavior: 80-94
Liu H, Zhang Q, Xia X, Yang X, Yi Z, Yue L, Huang L (2024) ESG performance and organizational resilience——based on an extreme heat event. Borsa Istanb Rev 24(2):304–313
Madrigano J, Ito K, Johnson S, Kinney PL, Matte T (2015) A case-only study of vulnerability to heat wave–related mortality in New York City (2000–2011). Environ health Perspect 123(7):672–678
Maier G, Grundstein A, Jang W, Li C, Naeher LP, Shepherd M (2014) Assessing thE Performance Of A Vulnerability Index During Oppressive Heat across Georgia, United States. Weather, Clim, Soc 6(2):253–263
Markevych I, Schoierer J, Hartig T, Chudnovsky A, Hystad P, Dzhambov AM, De Vries S, Triguero-Mas M, Brauer M, Nieuwenhuijsen MJ (2017) Exploring pathways linking greenspace to health: Theoretical and methodological guidance. Environ Res 158:301–317
Marx W, Haunschild R, Bornmann L (2021) Heat waves: a hot topic in climate change research. Theor Appl Climatol 146(1):781–800
McGranahan G, Songsore J (1994) Wealth, health, and the urban household: weighing environmental burdens in…. Environ: Sci Policy Sustain Dev 36(6):4–45
Mileti D (1999) Disasters by design: A reassessment of natural hazards in the United States, Joseph Henry Press
Nayak SG, Shrestha S, Kinney P, Ross Z, Sheridan S, Pantea C, Hsu W, Muscatiello N, Hwang S-A (2018) Development of a heat vulnerability index for New York State. Public health 161:127–137
O’Neill MS, Carter R, Kish JK, Gronlund CJ, White-Newsome JL, Manarolla X, Zanobetti A, Schwartz JD (2009) Preventing heat-related morbidity and mortality: new approaches in a changing climate. Maturitas 64(2):98–103
Rau R (2007) Seasonal Analysis of Death Counts in the United States. Seasonality in Human Mortality: A Demographic Approach: 83–124
Reid CE, O’Neill MS, Gronlund CJ, Brines SJ, Brown DG, Diez-Roux AV, Schwartz J (2009) Mapping community determinants of heat vulnerability. Environ Health Perspect 117(11):1730–1736
Rey G, Fouillet A, Bessemoulin P, Frayssinet P, Dufour A, Jougla E, Hémon D (2009) Heat exposure and socio-economic vulnerability as synergistic factors in heat-wave-related mortality. Eur J Epidemiol 24:495–502
Rosenthal JK, Kinney PL, Metzger KB (2014) Intra-urban vulnerability to heat-related mortality in New York City, 1997–2006. Health place 30:45–60
Sailor DJ, Pavlova AA (2003) Air conditioning market saturation and long-term response of residential cooling energy demand to climate change. Energy 28(9):941–951
Salvador C, Gullón P, Franco M, Vicedo-Cabrera AM (2023) Heat-related first cardiovascular event incidence in the city of Madrid (Spain): Vulnerability assessment by demographic, socioeconomic, and health indicators. Environ Res 226:115698
Sampson NR, Gronlund CJ, Buxton MA, Catalano L, White-Newsome JL, Conlon KC, O’Neill MS, McCormick S, Parker EA (2013) Staying cool in a changing climate: Reaching vulnerable populations during heat events. Glob Environ Change 23(2):475–484
Son J-Y, Liu JC, Bell ML (2019) Temperature-related mortality: a systematic review and investigation of effect modifiers. Environ Res Lett 14(7):073004
Stafoggia M, Forastiere F, Agostini D, Biggeri A, Bisanti L, Cadum E, Caranci N, de’Donato F, De Lisio S, De Maria M (2006) Vulnerability to heat-related mortality: a multicity, population-based, case-crossover analysis. Epidemiology 17(3):315–323
Stocker T (2014) Climate change 2013: the physical science basis: Working Group I contribution to the Fifth assessment report of the Intergovernmental Panel on Climate Change, Cambridge University Press
Studies H. J. C. f. H. (2020) The state of the nation’s housing 2020. Harvard University Report
Susca T, Gaffin SR, Dell’Osso G (2011) Positive effects of vegetation: Urban heat island and green roofs. Environ Pollut 159(8-9):2119–2126
Thomas K, Hardy RD, Lazrus H, Mendez M, Orlove B, Rivera‐Collazo I, Roberts JT, Rockman M, Warner BP, Winthrop R (2019) Explaining differential vulnerability to climate change: A social science review. Wiley Interdiscip Rev: Clim Change 10(2):e565
Thompson R, Hornigold R, Page L, Waite T (2018) Associations between high ambient temperatures and heat waves with mental health outcomes: a systematic review. Public health 161:171–191
Tony Wolf S, Cottle RM, Fisher KG, Vecellio DJ, Larry Kenney W (2023) Heat stress vulnerability and critical environmental limits for older adults. Commun earth Environ 4(1):486
U.S. Census Bureau. (n.d.). How the Census Bureau measures poverty. https://www.census.gov/topics/income-poverty/poverty/guidance/poverty-measures.html
U.S. Department of Agriculture, Economic Research Service. (n.d.). Poverty area measures - Background and uses. https://www.ers.usda.gov/data-products/poverty-area-measures/background-and-uses/
Uejio CK, Wilhelmi OV, Golden JS, Mills DM, Gulino SP, Samenow JP (2011) Intra-urban societal vulnerability to extreme heat: the role of heat exposure and the built environment, socioeconomics, and neighborhood stability. Health place 17(2):498–507
Vaidyanathan A (2020) Heat-related deaths—United States, 2004–2018. MMWR. Morbidity and Mortality Weekly Report 69
von Seidlein L, Alabaster G, Deen J, Knudsen J (2021) Crowding has consequences: Prevention and management of COVID-19 in informal urban settlements. Build Environ 188:107472
Weber S, Sadoff N, Zell E, de Sherbinin A (2015) Policy-relevant indicators for mapping the vulnerability of urban populations to extreme heat events: A case study of Philadelphia. Appl Geogr 63:231–243
Wendt D, Van Loon LJ, Marken Lichtenbelt WD (2007) Thermoregulation during exercise in the heat: strategies for maintaining health and performance. Sports Med 37:669–682
Wilhelmi OV, Hayden MH (2010) Connecting people and place: a new framework for reducing urban vulnerability to extreme heat. Environ Res Lett 5(1):014021
Yu Z, Chen J, Chen J, Zhan W, Wang C, Ma W, Yao X, Zhou S, Zhu K, Sun R (2024) Enhanced observations from an optimized soil-canopy-photosynthesis and energy flux model revealed evapotranspiration-shading cooling dynamics of urban vegetation during extreme heat. Remote Sens Environ 305:114098
Author information
Authors and Affiliations
Contributions
Conceptualization – JX, CF; methodology – JX, CF; software - JX; data analysis - JX; writing—original draft preparation - JX; writing—review and editing – JX, CF; visualization - JX; supervision – CF, XS, HH; project administration - CF, XS, HH; and funding acquisition - CF. All authors have read and agreed to the published version of the manuscript.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethical approval
This article does not contain any studies with human participants performed by any of the authors. All analyses are based on open-access secondary data.
Informed consent
This article does not contain any studies with human participants performed by any of the authors. All analyses are based on open-access secondary data.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Xu, J., Fan, C., Su, X. et al. An inference approach for assessing place-based vulnerability to heat mortality. Humanit Soc Sci Commun 12, 1324 (2025). https://doi.org/10.1057/s41599-025-05368-9
Received:
Accepted:
Published:
DOI: https://doi.org/10.1057/s41599-025-05368-9
