
Abstract
Complement overactivation, has been verified in COVID-19 patients. Complement regulatory proteins, including CD55, control complement overactivation thus eliminating complement deposition and cell lysis. We investigated complement regulatory protein expression in COVID-19 for potential deregulated expression patterns driving disease pathogenesis. Single-cell RNA-seq revealed increased PBMCs CD55 expression in severely and critically ill patients. This increase was also detected upon integrated subclustering analysis of monocyte, T cell and B cell populations. FACS analysis confirmed the significant upregulation of CD55 expression in CD4+ and CD8+ T cells and monocyte populations of severely and critically ill COVID-19 patients. This upregulation was associated with decreased expression of type-I IFN-stimulated genes (ISGs) in patients with severe and critical COVID-19, indicating a suppressor effect of CD55. Silencing of CD55 in T cells from COVID-19 severely ill patients in vitro and sensitization with SARS-CoV-2 peptides resulted in significantly augmented expression of ISGs and a reversal of their expression to levels similar to control or higher. The present study uncovers, to the best of our knowledge, a novel regulatory effect of CD55 on type-I IFN responses of severely ill COVID-19 patients, thus indicating its contribution to COVID-19 pathogenesis, and identifies a novel mechanistic pathway in the COVID-19 immune response.
Similar content being viewed by others


Introduction
Complement overactivation was confirmed in patients with severe and critical COVID-19, by determining elevated levels of C3a and C5a and increased C5b-9 levels in serum and plasma patient samples1,2,3. Furthermore, significant deposition of complement factors including C3b, C3d, C4d, C5b-9 and mannan-binding lectin serine protease 2 (MASP2) has been detected in lung tissue samples of critical COVID-19 patients with a co-localisation of C4d and C5b-9 with SARS-CoV-2 spike protein4,5.
Complement regulatory proteins (CRegPs) CD55, CD59, CD46, and complement receptor type 1 (CR1) are a group of glycoproteins safeguarding the balanced complement activation by promoting cleavage and decay of complement factors6. CR1, CD55, and CD46 act on the C3 and C5 cascade steps, thereby limiting the extent of complement cascade activation7,8,9,10, while CD59 acts exclusively at the final step, preventing formation of C5b-9, also known as membrane attack complex, and therefore cell lysis11,12.
Apart from their known role as complement activation controllers, CRegPs have also been implicated as modulators of the immune response13,14. CD55 has been reported as a suppressor of T cell immunity in vivo15, while similar observations have been reported for CD46 and T cell immune responses during viral infection16. Furthermore, CD55 has been implicated in the suppression of Toll-like receptor (TLR) signalling by repression of M1 anti-inflammatory polarisation17 and in models of inflammatory injury in vivo18.
The increased complement activation observed in severe and critical COVID-19 patients raises a question over a dysregulated expression of CRegPs contributing to complement overactivation. Using single-cell RNA-sequencing (scRNA-seq) on PBMCs isolated from COVID-19 patients at different disease states, we assessed CRegPs expression signatures in PBMC populations and investigated CRegPs involvement in COVID-19 pathogenesis.
Results
CD55 expression in PBMCs of COVID-19 patients
PBMCs isolated from whole blood samples of subjects enroled in the discovery cohort were utilised for scRNA-seq analysis (Fig. 1A), while whole blood samples from two separate cohorts of COVID-19 patients were utilised for validation of the scRNA-seq findings. Cohort A served for validation of target gene expression at the mRNA level by Real-time PCR amplification, and Cohort B for assessment of target molecule expression at the protein level by flow cytometric analysis (Fig. 1A).

A Schematic representation of the experimental design for single cell RNA sequencing (scRNA-seq) analysis of PBMCs isolated from blood samples of donors with mild (n = 4), severe (n = 4), critical (n = 4) COVID-19 and healthy donors (n = 4). Study validation cohorts include 80 additional donors (n = 40 for flow cytometric analysis, n = 40 for Real-time PCR amplification) and six additional donors for the functional experiments (n = 3 for patient samples and n = 3 for healthy controls). B Major immune cell subsets were identified and visualised in 2D by UMAP. C UMAP representation of isolated PBMCs from healthy, mild, severe, and critical COVID-19 patients. D Stacked Bar charts showing the relative abundances (%) of cell clusters across disease states as indicated. E Expression levels of CD55, CD46, CD59 and CR1 in COVID-19 patients and controls. Mean expression bar plots, with error bars representing the 95% bootstrapped confidence intervals around the mean. Statistical analysis performed by the Wilcoxon rank sum test ****p < 0.0001, numbers next to asterisks indicate log fold changes. F Dot plot representing CD55 expression in healthy and COVID-19 patients of different states; the dot size represents the fraction of cells in the clusters, mean expression is colour coded as indicated. G Bar plots showing relative CD55 mRNA levels in whole blood samples isolated from severely and critically ill COVID-19 patients compared to healthy controls (mean ± SD). **p < 0.01, ***p < 0.001. Statistical analysis was performed by Kruskal–Wallis non-parametric test for more than two groups comparisons. Fisher’s least significant difference test was used for post-hoc analysis. H Receiver operating curve analysis for prediction of ICU admission by CD55 mRNA expression levels.
scRNA-seq analysis initially identified the PBMC transcriptomic profiles of COVID-19 patients and healthy controls. Demographic and clinical data for patients enroled for scRNA-seq analysis are shown in Supplementary Fig. 1A. Integrated analysis of all samples revealed 13 transcriptionally distinct PBMC populations (Fig. 1B) and identified alterations between healthy controls and COVID-19 patients of different disease severity groups (Fig. 1C, D) using specific annotation markers (Supplementary Fig. 1B) and validation against deposited datasets by COVID-19 patients PBMC analyses19,20.
A significant upregulation of CD55 and CR1 expression levels in the total PBMC population of COVID-19 patients versus healthy controls was observed, followed by a significant downregulation of CD46 while no difference was shown for CD59 (Fig. 1Ε). CD55 upregulation was maximal in severely ill patients, and although slightly decreased in critically ill patients, it remained high compared with healthy controls (Fig. 1F). A similar pattern of upregulation in the severe COVID-19 group of patients was observed for CD46 albeit to a lesser extent, while variations in CD59 and CR1 could not be assessed due to very low expression levels. The profound increase of CD55 and its relatively higher expression levels in PBMCs compared to the other CRegPs prompted us to focus on CD55 for the rest of the analysis.
The upregulation of CD55 was confirmed by bulk RNA sequencing analysis of PBMCs (Supplementary Fig. 2A). Real-time PCR amplification on whole blood samples from a separate cohort of severely (n = 20) and critically ill (n = 20) COVID-19 patients (Validation Cohort A) further confirmed the significant upregulation of CD55 mRNA expression in critically ill patients while a lesser increase was observed in severely ill patients (Fig. 1G). Receiver operating characteristic (ROC) analysis for the association of CD55 mRNA expression levels in COVID-19 patients with prediction of admission to ICU, revealed a high AUC value (AUC = 0802, p = 0.002) (Fig. 1H).
CD55 upregulation in T cell populations of COVID-19 patients
We next assessed whether the observed CD55 increase in whole PBMCs of severely and critically ill COVID-19 patients also occurred in PBMC subpopulations such as T cells, monocytes, and B cells. Therefore, integrated subclustering analysis was performed. T cell integrated analysis identified CD4+ and CD8+ subpopulations (Fig. 2A) and eight distinct clusters, including CD4+ and CD8+ naïve and cytotoxic effector cells, CD8+ memory cells, Tregs, and exhausted CD8+ T cells (Fig. 2B, E, F), which varied with disease state (Fig. 2C, D).

A UMAP representation of 31,763 Τ cells coloured by cell type and B cluster assignment. C UMAP representation of all the T cells analysed across different disease states as indicated (healthy group: 11,180 cells, mild disease group: 13,687 cells, severe disease group: 2470 cells and critical disease group: 4426 cells). D Stacked bar plot representing T cell cluster quantitative changes (%) in each disease state as indicated, E Pearson correlation plot of scaled expression values followed by hierarchical clustering, for the most variable genes identified in the T cell subpopulations integrated. Colour spectrum represents positive correlations in red, to no correlation in white, to negative correlation in blue. F scRNA-seq heatmap showing the average scaled expression for selected marker genes of each subpopulation; mean expression is colour coded as indicated. G Feature plots showing CD55 gene expression in the T cell subpopulation UMAP space. H Dot plot depicting expression levels of CD55 in all T cell clusters across disease state; the dot size represents the fraction of cells in the clusters, mean expression is colour coded as indicated. I Matrix plot depicting differential expression of CD55 across the different T cell subpopulations depending on the disease state; mean CD55 expression levels and disease states, are colour coded, as indicated. J CD55 expression levels in each T cell cluster, in healthy and severe donors as indicated. Mean expression bar plots, with error bars representing the 95% bootstrapped confidence intervals around the mean. Statistical analysis performed by the Wilcoxon rank sum test *p < 0.05, **p < 0.01, ****p < 0.0001. K Side-by-side plots of flow cytometry histograms showing CD55 expression in CD4+ (top panel) and CD8+ T (lower panel) cell populations; severe disease patient sample (blue histogram), critical disease patient sample (red histogram) and healthy control sample (grey histogram). L Bar plots depicting quantitation of CD55 protein expression levels in CD4+ and CD8+ T cells determined by flow cytometric analysis in severe (n = 20) and critical (n = 20) COVID-19 patient cohorts (mean ± SD); Statistical analysis was performed by one-way ANOVA testing for more than two groups comparisons. Post-hoc analysis was performed by Fisher’s least significant difference test. *p < 0.05, **p < 0.01, ***p < 0.001, ****p < 0.0001.
CD55 expression was observed in almost all T cell clusters, as shown in the T cell subpopulation feature plots for CD55 (Fig. 2G). Upregulation of CD55 was identified in severely and critically ill COVID-19 patients in the total T cell subpopulations (Fig. 2H). This was further confirmed by verification in a large publicly available dataset of scRNA-seq data (Supplementary Fig. 2B, E)19. Significantly elevated CD55 expression levels were also observed in the severely and critically ill groups of patients in the large dataset, compared to healthy controls (Supplementary Fig. 2B, E). CD55 expression levels varied between the identified CD4+ and CD8+ T cell clusters and disease states (Fig. 2I) while the increase of CD55 expression was significant in all T cell clusters of severely ill patients in comparison to healthy controls apart from the exhausted CD8+ T cell cluster (Fig. 2J).
We next confirmed the upregulation of CD55 at the protein level by FACS analysis in a separate cohort of COVID-19 patients (Validation Cohort B) (Fig. 2K, L). Blood samples from patients with severe (n = 20) and critical COVID-19 (n = 20) were isolated and analysed with FACS for CD55 expression in CD4+ and CD8+ T cells. A significant increase of CD55 expression was observed in CD4+ T cells in severely (p < 0.01) and critically ill (p < 0.001) COVID-19 patients compared with healthy controls (Fig. 2L). CD8+ T cells showed significantly increased CD55 expression in severely and critically ill patients versus healthy controls, (p < 0.05 and p < 0.0001, respectively), while the increase in critically ill patients was also significant compared to severely ill (p < 0.01) (Fig. 2L).
CD55 expression in the monocyte population of COVID-19 patients
Analysis of the monocyte population identified classical (CD14+), intermediate (CD14+CD16+) and non-classical (CD16+) monocytes (Fig. 3A) and a total of 13 clusters (Fig. 3B, E, F). Differences of the various monocyte subpopulations were observed according to disease state (Fig. 3C, D).

A UMAP representation of 19,303 monocytes coloured by cell type and B cluster assignment, as indicated on the figure. C UMAP representation of all the monocytes analysed across different disease states as indicated (healthy group: 3060 cells, mild disease group: 5750 cells, severe disease group: 2289 cells and critical disease group: 8204 cells). D Stacked bar plot representing monocyte cluster quantitative changes (%) in each disease state as indicated. E Pearson correlation plot of scaled expression values followed by hierarchical clustering, for the most variable genes identified in the monocytes subpopulations integrated. Colour spectrum represents positive correlations in red, to no correlation in white, to negative correlation in blue. F scRNA-seq heatmap showing the average scaled expression for selected marker genes of each subpopulation; mean expression is colour coded as indicated. G Feature plots showing CD55 gene expression in the monocytes subpopulation UMAP space. H Dot plot depicting expression levels of CD55 in all monocytes clusters across disease state; the dot size represents the fraction of cells in the clusters, mean expression is colour coded as indicated. I CD55 expression levels in each monocyte cluster, in healthy and severe donors as indicated. Mean expression bar plots, with error bars representing the 95% bootstrapped confidence intervals around the mean. Statistical analysis performed by the Wilcoxon rank sum test *p < 0.05, **p < 0.01, ****p < 0.0001. J Side-by-side plots of flow cytometry histograms showing CD55 expression in monocytes; severe disease patient sample (blue histogram), critical disease patient sample (red histogram) and healthy control sample (grey histogram). K Bar plots depicting quantitation of CD55 protein expression levels in monocytes determined by flow cytometric analysis in severe (n = 20) and critical (n = 20) COVID-19 patient cohorts (mean ± SD); Statistical analysis was performed by one-way ANOVA testing for more than two groups comparisons. Post-hoc analysis was performed by Fisher’s least significant difference test. *p < 0.05, **p < 0.01, ***p < 0.001, ****p < 0.0001.
The expression of CD55 was observed in almost all monocyte subpopulations at all disease states, as shown by feature plots of CD55 (Fig. 3G). An increased expression of CD55 in all COVID-19 states compared to healthy controls was observed, with the most profound increase in patients with severe COVID-19 (Fig. 3H). This was also confirmed in the large publicly available dataset of scRNA-seq data19 (Supplementary Fig. 2C, F). The increase of CD55 expression in monocytes of severely ill patients was significant in comparison to the healthy individuals in all monocyte clusters identified apart from one CD14+ cluster (CD14+ IL1B) and two intermediate monocyte clusters CD14+CD16+C1Q and CD14+CD16+CXCL10 (Fig. 3I). In line with our scRNA-seq observations, FACS analysis on monocyte CD55 protein expression (Fig. 3J, K) revealed, a significant increase of CD55 protein expression in monocytes of severely ill COVID-19 patients compared with healthy controls (p < 0.05) (Fig. 3K).
CD55 expression in B-cell populations of COVID-19 patients
Subclustering analysis of the B cell population resulted in its discrimination into seven distinct subpopulations (Fig. 4A, D, E) that varied with disease state (Fig. 4B, C). A marked CD55 upregulation in the severe COVID-19 group of patients was observed (Fig. 4F). An increase in CD55 expression was also shown in all B cell clusters of the severely ill COVID-19 group of patients compared to healthy controls (Fig. 4G) albeit not significant. FACS analysis for CD55 protein expression levels in B cells (Figs. 4H, 6I) showed a significantly increased CD55 protein expression in the critically ill patients group compared to severely ill (p < 0.05) and healthy controls (p < 0.05) (Fig. 4I).

A UMAP representation of 3,038 B cells coloured by cluster assignment, as indicated. B UMAP representation of all the B cells analysed across different disease states, as indicated (healthy group: 617 cells, mild disease group: 1328 cells, severe disease group: 289 cells and critical disease group: 804 cells). C Stacked bar plot representing B cell clusters quantitative changes (%) in each disease state as indicated. D Pearson correlation plot of scaled expression values followed by hierarchical clustering, for the most variable genes identified in the B cells subpopulations integrated. Colour spectrum represents positive correlations in red, to no correlation in white, to negative correlation in blue. E scRNA-seq heatmap showing the average scaled expression for selected marker genes of each subpopulation; mean expression is colour coded as indicated. F Dot plot depicting expression levels of CD55 in all B cell clusters across disease state; the dot size represents the fraction of cells in the clusters, mean expression is colour coded as indicated. G CD55 expression levels in each B cell cluster, in healthy and severe donors as indicated. Mean expression bar plots, with error bars representing the 95% bootstrapped confidence intervals around the mean. Statistical analysis performed by the Wilcoxon rank sum test; ns=non-significant. H Side-by-side plots of flow cytometry histograms showing CD55 expression in B cells; severe disease patient sample (blue histogram), critical disease patient sample (red histogram) and healthy control sample (grey histogram). I Bar plots depicting quantitation of CD55 protein expression levels in B cells determined by flow cytometric analysis in severe (n = 20) and critical (n = 20) COVID-19 patient cohorts (mean ± SD); Statistical analysis was performed by one-way ANOVA testing for more than two groups comparisons. Post-hoc analysis was performed by Fisher’s least significant difference test. *p < 0.05, **p < 0.01, ***p < 0.001, ****p < 0.0001.
CD55 upregulation in severely and critically ill COVID-19 patients is associated with suppression of type-I interferon (IFN) responses
The increase of CD55 expression observed in the subpopulations of severely and critically ill patients prompted us to investigate its potential association with altered immune responses. It has been reported that critically and severely ill COVID-19 patients exhibit impaired type-I IFN responses21,22. Furthermore, CD55 has been reported as a suppressor of T cell immune responses in vivo15. We therefore examined a potential association of upregulated CD55 expression and type-I IFN responses suppression in our data set. Initial gene set enrichment analysis (GSEA) in specific clusters of the T cell (CD4+ effector and CD8+ effector clusters) (Fig. 5A, B), monocyte (classical monocyte CD14+IL1B cluster and non-classical CD16+ cluster) (Figs. 5C D) and B cell (mature and naive B cell clusters) (Fig. 5E, F) subpopulations revealed a suppression of IFN-γ and α responses in the critical group of COVID-19 patients compared to the mild group.

Bar plots representing quantitative analysis produced by gene set enrichment analysis (GSEA) performed using gene lists derived by comparison of critical versus mild COVID-19 in: A CD4+ effector T cell cluster, B CD8+ effector T cell cluster, C classical monocyte CD14+IL1B cluster, D non-classical CD16+ cluster, E mature B cells cluster and F naive B cell cluster; FDR ≤ 0.05. G Dot plot depicting expression levels of ISGs, in the total PBMC population, across disease state; the dot size represents the fraction of cells in the clusters, mean expression is colour coded as indicated. H Feature plots representing ISGs expression on the UMAP space in each disease state analysed.
We further explored the potential suppression of type-I IFN responses by CD55 at the COVID-19 stages in which we observed CD55 overexpression. A selection of specific type-I IFN-stimulated genes (ISGs) was used21. Nine ISGs (IFIT1, IFI6, IFI27, IFIT3, IFI44L, IFITM3, ISG15, STAT2 and ISG20) were chosen for assessment of their expression levels in the various COVID-19 patients’ groups. Initial analysis in total PBMCs revealed upregulated ISGs expression in the mild COVID-19 patient group and a reduction in severely and critically ill patients (Fig. 5G, H) mainly located in T cells and monocytes of the mild COVID-19 group (Fig. 5H). Real-time PCR amplification in whole blood samples from Validation Cohort A was performed on six out of the nine ISGs chosen for analysis and confirmed the reduction of ISGs mRNA expression in the critical COVID-19 group of patients (Supplementary Fig. 3A). The same data demonstrated that suppressed ISGs expression levels are also observed at the severe state of the disease in which a large proportion of the patients showed ISG levels similar to those of the control individuals (Supplementary Fig. 3A).
Integrated analysis revealed a major increase in ISGs expression of the T cell subpopulation in the mild COVID-19 group of patients with a subsequent reduction in the severe and critical COVID-19 groups (Fig. 6A, D). The reduced T cell ISGs expression coincided with the increase of T cell CD55 expression identified by scRNA-seq analysis in the severe and critical groups of patients (Supplementary Fig. 3B), also confirmed by FACS analysis (Fig. 2I). Apart from ISG20, the expression of all ISGs showed a decrease in the severe and critical groups of patients in all T cell clusters when compared to the mild group (Fig. 6A and Supplementary Fig. 3B). This observed decrease coincided with augmented expression of CD55 as shown for CD4+ effector and naïve clusters as well as the CD8+ naïve cluster (Supplementary Fig. 3B).

Dot plot depicting expression levels of ISGs in the: A T cell subpopulation, B monocyte subpopulation, and C B cell subpopulation, across disease state. The dot size represents the fraction of cells in the clusters, mean expression is colour coded as indicated. D ISG score changes in COVID-19 patients of different disease severity and healthy controls in the T cell subpopulation, E monocyte subpopulation and F the B cell subpopulation. Mean expression box plots, with error bars representing the 95% bootstrapped confidence intervals around the mean. Statistical analysis performed by the Mann–Whitney–Wilcoxon test two sided with Bonferroni correction ****p < 0.0001.
An increase of ISGs expression in the mild COVID-19 group with a relative decline in the severe and critical COVID-19 groups was also observed in the monocyte subpopulation (Fig. 6B, E and Supplementary Fig. 3C). The relative decline in ISGs expression was concurrent with the increase of CD55 expression in the same cells (Supplementary Fig. 3C). As shown in Fig. 6B, the increase of CD55 expression levels observed in the monocyte clusters of the severe COVID-19 group of patients was concurrent with almost absent ISG expression, contrary to the mild stage in which ISGs expression was augmented. Furthermore, the CD16+ cluster also exhibited a significantly increased expression of CD55 in the severe state simultaneously with almost complete absence of the ISGs expression (Fig. 6E). This was in striking contrast to the mild stage in which increased CD16+ monocyte ISG expression coincided with a weaker CD55 expression (Fig. 6E and Supplementary Fig. 3C).
Similar findings were observed in the B cell population. A direct decrease of ISGs expression could be associated with the increased CD55 expression for all B cell clusters in the severe group of COVID-19 patients (Fig. 6C, F and Supplementary Fig. 3D). This follows the contrast in the mild group in which lower levels of CD55 coincided with increased ISG expression.
CD55 suppresses type-I IFN responses in SARS-CoV-2 viral antigen-exposed T cells
To confirm the potential regulatory effect of CD55 on type-I IFN responses, functional experiments were performed, and the expression of ISGs was assessed. Specifically, T cells from patients with severe COVID-19 were transfected with siRNA for CD55 and stimulated by SARS-CoV-2 viral antigens in vitro. IFI6, IFI27, IFI44L, IFIT3, ISG15 and STAT2 expression were then assessed. Transfection of T cells with siRNA for CD55 resulted in silencing of CD55 mRNA expression (Supplementary Fig. 4). siCD55-transfected T cells, derived from COVID-19 patients with severe disease, PBMC solutions, and control subjects, were stimulated with pools of SARS-CoV-2 peptides covering the spike and nucleoprotein, to examine the effect of CD55 absence on type-I IFN responses. Mock-transfected T cells from patients with severe COVID-19 were also incubated with SARS-CoV-2 peptides and compared with siCD55-transfected T cells obtained from control subjects, who were healthy but previously exposed to SARS-CoV-2, individuals. Incubations in the presence of SARS-CoV-2 peptides did not affect ISGs expression in the mock-transfected T cells of COVID-19 patients for all genes assessed (Fig. 7A) with the exception of IFIT3, which showed an increase, albeit non-significant. In striking contrast, a statistically significant increase in the expression of all ISGs examined was observed in SARS-CoV-2-peptide-sensitised, siCD55-transfected, T cells of COVID-19 patients (Fig. 7A) (analysis versus mock-transfected patient control). ISGs mRNA expression was augmented in the siCD55-transfected T cells from COVID-19 in the presence of SARS-CoV-2 peptides to levels above those of both the unsensitised transfected T cell sample and the mock controls for IFI6, IFI27, IFI44L, ISG15 and STAT2 (Fig. 7A, B). The same effect was observed in peptide incubations of siCD55 transfected T cells obtained from the control subjects (previously exposed to SARS-CoV-2 healthy individuals), confirming the regulatory effect of CD55 on the expression of type-I ISGs (Fig. 7B). Furthermore, the expression of type-I ISGs in T cells of severe COVID-19 patients was markedly reduced in comparison to control individuals, confirming the impairment of type-I IFN responses in these patients (Fig. 7B). Taken together, the results from the functional experiments confirm the observations from our scRNA-seq analysis.

PBMCs isolated from patients with severe COVID-19 (n = 3) and control individuals (n = 3) were transfected with siRNA for CD55 and subsequently sensitised with SARS-CoV-2 peptide pools. Following incubations, relative mRNA levels were assessed by Real-time PCR amplification for IFI6, IFI27, IFI44L, IFIT3, ISG15 and STAT2 as indicated. Relative ISG expression is shown versus (A) patient control (mock-transfected PBMCs from COVID-19 patients) and (B) healthy control (mock-transfected PBMCs from healthy individuals). The bars represent mean values ± SEM as calculated. Statistical analysis was performed with One-way ANOVA. Post hoc analysis was performed by Fisher’s least significant difference test. *p < 0.05; **p < 0.01; ***p < 0.001; ****p < 0.0001.
Discussion
Little is known about the role of CRegPs during viral infections regarding both their regulatory activity on complement activation and their direct effect on antiviral and immune responses. We identified a distinct COVID-19-specific expression pattern for CD55 in severely and critically ill patients. Previous investigation of PBMCs CRegP expression patterns in viral and bacterial infection reported no effect on CD55 expression levels in monocytes, lymphocytes, and neutrophils of patients with viral infection compared to healthy controls23. The study included 26 patients with confirmed viral infections from various unrelated viruses. In contrast, we revealed that PBMCs isolated from severely and critically ill COVID-19 patients displayed increased CD55 expression (Fig. 1). Upregulated CD55 expression was observed in the individual subpopulations (monocytes, T cells, and B cells) resolved by scRNA-seq (Figs. 2, 3, 4) for severely ill patients and for critically ill patients in T cells and monocytes compared to healthy controls, and this was further confirmed by FACS analysis. Taking into account the overactivation of complement in these patients24 the upregulation of CD55 expression observed could be explained as a potential protective mechanism for the cell populations in response to uncontrolled complement activation. Increased levels of C3a, C3c, and C5b-9 have been reported in COVID-19 patients in comparison to healthy controls1 as well as in non-survivors25. Significantly high levels of circulating C5a and C5b-9 have also been reported in COVID-19 compared to influenza patients and ICU patients with non-COVID-19 respiratory failure26, while others have shown increased deposition of complement factors in tissue samples from COVID-19 patients, including lungs, liver, kidneys, and the endothelium4,27, thus rendering complement activation a distinctive feature of COVID-19. Increased complement deposition was also identified in monocytes of COVID-19 patients of various disease states28. Lage et al. reported significant C1q and C3 levels in monocytes of patients with severe COVID-19 compared to healthy controls28, which persisted even after patients’ recovery. The upregulation of CD55 observed in our study may therefore serve to eliminate further activation and deposition of complement in this cellular population. However, previous reports on the involvement of CD55 in the modulation of immune responses prompted us to investigate a potential such role in the COVID-19 immune response.
Delayed and dysregulated type-I IFN responses have been linked to COVID-19 severity22,29. Hadjaj et al. demonstrated decreased expression of ISGs in patients with severe and critical COVID-19 following a marked increase in patients with mild disease21. The same reduction of ISGs expression in monocytes and T lymphocytes in severely ill COVID-19 patients compared to patients with mild disease was shown in Xu et al.30. Galani et al. also reported the delayed type-I and type-III IFN responses in severe COVID-19 patients22. We observed the same profile of reduced type-I IFN responses in severely and critically ill patients following a marked increase in the mild COVID-19 group by analysis of the expression of nine ISGs in total PBMCs (Fig. 5G) as well as in the monocyte, T, and B lymphocyte subpopulations (Fig. 6). The reduction of ISGs expression in the severe and critical COVID-19 groups of patients coincided with the upregulation of CD55 expression, also confirmed at the protein level by FACS analysis in each PBMC subpopulation. In order to assess the possible involvement of CD55 in the repression of type-I IFN response signalling we chose the T cell subpopulation for our functional experiments, as the upregulation of CD55 expression was confirmed in both CD4+ and CD8+ T cells of the severe and critical groups of patients by FACS analysis compared with controls (Fig. 2) and previous studies have reported its suppressive effect on T cell immunity15. The results from the in-vitro functional experiments of our study confirm the suppressive effect of CD55 on type-I IFN T cell responses in COVID-19 patients as silencing its expression by siRNA for CD55 resulted in the marked increase of the expression of ISGs following sensitisation with viral peptides (Fig. 7). The fact that this increase was observed in transfected and sensitised T cells of both the COVID-19 patients and the controls further indicates a potential regulatory effect of CD55 on type-I IFN responses independent of disease state. Furthermore, the control group for the functional experiments consisted of healthy, but previously exposed to SARS-CoV-2, individuals by both vaccination and infection, which resulted in mild disease. The marked decrease in the expression of the ISGs observed in the T cells obtained from the severely ill patients confirmed the inability for ISGs induction in these patients. A recent study by Lin et al. identified SOCS3 as a possible suppressor of type-I IFN responses31. This elegant study involved longitudinal sc-RNA-seq analysis of severe and critical COVID-19 samples and reported an association of SOCS3 upregulation with reduced type-I IFN responses in severely and critically ill COVID-19 patients. Although the study confirmed this association in various other datasets, the functional experiments assessed the effect of SOCS3 on SARS-CoV-2 replication. Using SARS-CoV-2-infected HEK293T Angiotensin-Converting Enzyme 2 (HEK-ACE2) epithelial cells, previously silenced for the CD55 gene, the study observed reduced viral replication of SARS-CoV-2 in vitro31 but its direct effect on type-I IFN responses was not assessed.
CD55 has been linked to the suppression of adaptive immune responses in vivo. In an initial study involving CD55 knock-out (KO) mice, CD4+ T cells were reported to excessively produce IFN-γ and IL-2 in response to active immunisation15. Subsequently, it was shown that lack of CD55 on antigen-presenting cells (APCs) and T lymphocytes, during primary T cell activation, promotes proliferation and increases effector cells32. Furthermore, in CD55 KO mouse model studies of CD8+ T cell immune responses to viral infection, a CD8+ T cell expansion in spleen and lymph nodes was observed alongside an increased number of antigen-specific CD8+ T cells. This expansion resulted in a rapid clearance of viral infection33. A subsequent study by the same group demonstrated that treatment of APCs from CD55 KO mice with an inflammatory stimulus led to aggravated T cell responses34. Finally, CD55 has also been linked to the suppression of NK cell responses35.
Our study identifies a novel role for CD55 in COVID-19 immune responses and, therefore, a novel mechanism driving disease progression and possibly outcome. This role was confirmed in T cells of COVID-19 patients. However, our scRNA-seq data strongly suggest that the same suppressive effect could be taking place in other cellular populations, such as monocytes and B cells. Although we confirmed the regulatory effect of CD55 on type-I IFN responses of COVID-19 T cells, we did not identify potential mediators of this interaction. Previous reports on the suppressive effect of CD55 on TLR signalling17,18, which mediates type-I IFN responses, suggest that TLR signalling might be a plausible candidate, but further research is needed to verify this hypothesis.
A limitation of our study involves the limited number of subjects included in the scRNA-seq analysis. Thus, we further examined the validity of our observations in a large dataset of scRNA-seq analysis19. The study involved a comprehensive scRNA-seq analysis of PBMCs from 102 COVID-19 patients, and we confirmed the expression pattern obtained for CD55 in monocytes and T cells but not B cells. Furthermore, the samples from the two separate cohorts of patients for verification of CD55 expression at the mRNA and protein levels were selected at different time periods. Therefore, the FACS data involve samples from patients during the third wave of SARS-CoV-2, during which the main SARS-CoV-2 circulating variants were the Delta and the Omicron variants, whereas the samples for validation of mRNA expression levels were collected during the second wave of the pandemic, same as the scRNA-seq patient samples during which the main circulating variant was the Alpha variant36. Furthermore, the samples utilised for the functional experiments were obtained from COVID-19 patients with the recent Omicron variant. However, the fact that the data from the various cohorts all support the upregulation of CD55 observed by scRNA-seq analysis and the suppression of ISGs could possibly indicate that our observations of the suppressive effect of CD55 upregulation take place independent of the circulating SARS-CoV-2 strain and support the important role of CD55 in the COVID-19 immune response.
In summary, the present scRNA-seq study identified a novel mechanistic role of CD55 in COVID-19 immune response by suppression of type-I IFN responses and thus in COVID-19 pathogenesis. Our observations strengthen the importance of complement activation in COVID-19 and introduce novel molecules of the complement cascade as COVID-19 progression mediators. Given the diverse array of complement-targeted therapeutic strategies, our findings may point towards novel therapies in the fight against COVID-19.
Materials and methods
Study approval
118 individuals were enroled in the study, of whom 95 were COVID-19 patients and 23 were controls. Ethics approval was obtained from the Ethics Committee of Evangelismos General Hospital (approval number: 360, study title: COVID-19 and Immunological profile), and all procedures were carried out according to the Declaration of Helsinki. A written informed consent was obtained from all patients or the patient’s next of kin, and all ethical regulations relevant to human research participants were followed.
scRNA-seq subjects
12 patients were recruited for PBMC isolation for scRNA-seq analysis and served as the discovery cohort (Fig. 1A). Ethical approval for the study was granted by the Ethics Committee of Evangelismos Hospital (approval number: 435, Study title: Gene expression identification of COVID-19 patients by single-cell RNA sequencing analysis). Study participants were recruited between 20/09/20 and 24/9/20. Controls were recruited among hospital staff age-matched to the COVID-19-positive study participants. A written informed consent was obtained from all patients or the patient’s next of kin. All patients had a positive polymerase chain reaction (PCR) test for SARS-CoV-2 performed on a nasopharyngeal sample. Classification of patients was performed according to criteria in line with WHO guidelines. Patients were grouped into those with mild disease, admitted to the hospital ward without need for oxygen supply (n = 4), severe COVID-19 patients who required oxygen supplementation but not intensive care unit (ICU) admission (n = 4) and critically ill (n = 4) patients admitted to the ICU who required intubation and mechanical ventilation (n = 4). Healthy individuals (n = 4) served as controls. Samples were all obtained within the first 24 h of admission of patients in the ward or the ICU.
Validation cohort subjects
A total of 80 patients were enroled for validation of scRNA-seq observations in two separate cohorts (n = 40 each). Patient classification was performed by the same criteria as the subjects enroled for the scRNA-seq study. Validation Cohort A (n = 40) consisted of study participants for verification of scRNA-seq findings by analysis at the mRNA level and were recruited between 22 September 2020 and 6 November 2020. Validation Cohort B served for verification of findings at the protein level by flow cytometric (FACS) analysis and consisted of study participants (n = 40) enroled between 3 January 2022 and 27 March 2022. (Fig. 1A). Ethical approval was obtained by the Ethics committee of Evangelismos Hospital (approval number: 360, Study title: COVID-19 and Immunological profile). Patients were classified by the same criteria into two groups of patients: the severe COVID-19 group of patients (n = 20) and the critical COVID-19 group of patients (n = 20).
Three more COVID-19 patient samples were obtained for functional experiments. Patients were enroled between 1 September 2023 and 30 October 2023. Controls were recruited among hospital staff attending age-matched to the COVID-19-positive study participants for both cohorts and the functional experiments patients’ samples. Blood samples were obtained within 24 h of admission to either the hospital or ICU and processed immediately for all patient samples of this study.
PBMCs isolation for scRNA-seq analysis
PBMCs were isolated following a standard protocol. Briefly, 20 ml of whole blood drawn in heparin-coated tubes were layered on top of 15 ml of Lymphoprep and separated by gradient centrifugation (700 × g, 30 min). The central band containing PBMCs was extracted, using a sterile Pasteur pipette, into Hanks balanced salt solution (HBSS) (10 ml) and the suspension was centrifuged (700 × g, 10 min). Cells were counted and processed immediately for scRNA-seq analysis.
Single cell suspension preparation and generation of droplet-based scRNA-seq data
Four male individual samples per condition were processed (healthy n = 4, mild n = 4, severe n = 4, and critical n = 4). Isolated PBMCs were observed and counted with an hemocytometer prior to loading. A range of total 106 to 2 × 106 cells were isolated in all 16 samples and were resuspended to a concentration of 1000 cells/µl in 0.04% BSA and directly processed for scRNA-seq. Four sample pools were prepared, each aimed to yield 3000 cells/individual from four individuals (12,000 cells). Each sample pool was loaded into a different lane of a 10× chip (Single Cell G Chip Kit for v3.1). The 10x Chromium controller (10x Genomics), in combination with v3.1 reagents, was used to capture the single cells and generate Single-Indexed sequencing libraries, according to the manufacturer’s instructions (document CG000204, RevD). Sequencing was performed with a 150 bp paired-end kit using a custom programme (28-8-0-150) on the Illumina NextSeq 500/550 at pMedGR (Medical School, NKUA, Athens, Greece).
Alignment
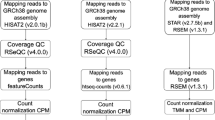
Droplet libraries were processed using 10x Genomics Cell Ranger 4.0.0. Reads were aligned to the GRCh38 human genome. The filtered feature matrices were used.
Cell doublet detection
Scrublet37 (v0.2.3 version) was used for the identification of cell doublets on each separate sample using the raw counts. Keeping the automatic threshold on the generated doublet score, 8642 cells were identified as doublets and removed, thus ending up with a total of 17,048, 22,997, 7784 and 16,337 cells for the samples derived from the healthy, mild, severe, and critical groups of patients, respectively.
Quality control, preprocessing, and label transferring
The Python package Scanpy38 was used for analysis. Combined raw data (64,166 cells) were filtered to remove cells that expressed fewer than 200 genes, genes that were expressed in less than three cells, cells with >20% mitochondrial reads, and cells with >5000 n genes by counts. Counts were normalised and log +1 corrected, and highly variable genes (HVGs) were identified. The percentage of mitochondrial reads and the number of total counts were regressed out, and the counts were scaled. Using Scanpy’s ingest function, which maps labels and embeddings from reference data to query data, we annotated our data on two PBMCs scRNA-seq datasets20 that were available at the time, with 647, 366, 44, 741 cells, respectively. Keeping only those cells sharing the same broad annotation in the two reference datasets on the following cell types: monocytes, T cells, B cells, DCs, stem cells, RBCs and platelets for the downstream analysis. The label-transferring annotations were confirmed by the expression of known marker genes. As for the cells for which the annotation was different between the two different reference datasets, the expression of mixed markers led us to remove them. A total of 61,022 single cells passed quality control and were used in the analysis. The mild group consisted of 22,570 sequenced single cells, while the severe and critical groups consisted of 7350 and 15,397 cells, respectively. Moreover, 15,705 single cells were sequenced in the healthy group.
Integration and sub-clustering
We then subset the three cell types of interest (monocytes, T cells and B cells) and analysed them separately. There was an evident batch effect between the four different conditions, so beginning with raw counts and using the same preprocessing steps, we integrated the data using the batch removal tool Batch Balanced KNN39 (BBKNN). Ridge regression for improvement40 of the integration was also performed prior to the final BBKNN step. Clustering was performed using the Leiden algorithm, with the resolution being decided based on the expression of differentially expressed genes, which were calculated using the Wilcoxon rank sum test. Although doublets were removed in the pre-processing step, clusters from B cells and T cells that expressed mixed markers with other cell types were also removed from further analysis. Annotation of individual clusters was based on literature-established marker genes and differentially expressed genes (DEGs). ISG scores were calculated using the Scanpy’s tl.score genes and R package UCell41. For the differential expression of CD55 in monocytes, besides the Wilcoxon rank-sum test (Scanpy), MAST, DESeq2 and edgeR from R package Libra42 were also used.
Gene Set Enrichment Analysis (GSEA)
Online at WebGestalt43 using the p value and logFC of the Wilcoxon rank-sum test, we calculated a score by multiplying the −log10 (p value) with the logFC. Then we ordered the genes in descending order and ran the GSEA using the Hallmark50 Functional Database.
Isolation of RNA and bulk 3′ RNA sequencing
Isolated PBMCs utilised for the scRNA-seq analysis also served for the generation of the RNA samples. Four individual RNA samples per condition (mild, severe, critical) were prepared from isolated COVID-19 patients PBMCs and healthy controls using the RNeasy mini kit (QIAGEN), according to the manufacturer’s instructions. The quantity and quality of RNA samples were analysed using Agilent RNA 6000 Nano kit with the bioanalyzer from Agilent. RNA samples with RNA integrity number (RIN) > 7 were used for library construction using the 3′ mRNA-Seq Library Prep Kit Protocol for Ion Torrent (QuantSeq-LEXOGEN™) according to the manufacturer’s instructions. The DNA High Sensitivity Kit in the bioanalyzer was used to assess the quantity and quality of libraries, according to the manufacturer’s instructions (Agilent, Santa Clara, CA, USA). Libraries were then pooled and templated using the Ion PI™ IC 200 Kit (Thermo Fisher Scientific, Waltham, MA, USA) on an Ion Proton Chef Instrument or Ion One Touch System. Sequencing was performed using the Ion PI™ Sequencing 200 V3 Kit and Ion Proton PI™ V2 chips (Thermo Fisher Scientific) on an Ion ProtonTM System, according to the manufacturer’s instructions.
Computational analysis of bulk RNA sequencing data
The quality of the FASTQ files was assessed with the fastqc software (available online at: http://www.bioinformatics.babraham.ac.uk/projects/fastqc/). Reads that were aligned to the mm10 genome were performed with the Hisat2 aligner. FeatureCounts was utilised for the step of read summarisation at the gene level. Differential expression analysis was conducted by DESeq2. For each contrast, differentially expressed genes were defined by applying the following thresholds: |Log2FC| > 0.58 and p value < 0.05.
RNA extraction on the Cohort A samples
For analysis of CD55 mRNA levels by Real-time PCR amplification, RNA was extracted from whole blood samples isolated from severe (n = 20) and critical (n = 20) COVID-19 patients. Whole blood samples were collected in Tempus Blood RNA Tubes (Applied Biosystems, Waltham, MA, USA) and stored at −80 °C. RNA was extracted according to the manufacturer’s instructions. RNA concentration was determined for each sample prior to reverse transcription using NanoDrop One.
Reverse transcription and Real-time PCR amplification
Reverse transcription reactions were performed using 4 µl of the 5x FastGene® Scriptase II ReadyMix (Nippon Genetics, Duren, Germany) and 100 ng of RNA for each reaction. Reactions were carried out in a CFX90 cycler (BioRad, Hercules, CA, USA) at the following conditions: 25 °C for 10 min, 42 °C for 60 min and 85 °C for 5 min. Real time PCR reactions were carried out in a CFX90 cycler. Each reaction consisted of 1 μl primer-probe assay mix (IDT, Coralville, IA, USA), 10 μl Luna Master Mix (Biolabs, Waltham, MA, USA) and 1 μl cDNA. GAPDH was used as a housekeeping gene for data normalisation. The sequences for the Real time PCR primers and probes for CD55 mRNA are as follows: forward primer: 5′- CTC ATA TTC CAC AAC AGT ACC GA -3′, reverse primer: TGG TCA GAT ATT GAA GAG TTC TGC -3′, probe: /56-FAM/TGC ATC CCT /ZEN/CAA ACA GCC TTA TAT CAC TC/3IABkFQ/. The TaqMan assays used for assessment of ISGs mRNA levels were all predesigned assays purchased from IDT. ISGs TaqMan assay IDs are provided in Supplementary Table 1. Reactions were carried out in triplicate, and results were analysed by the ΔΔCT method.
Flow cytometric analysis for CD55 protein expression
For validation of the single-cell analysis by FACS, whole blood samples were obtained from patients in the ward with characteristics matching those in the severe COVID-19 group of patients (n = 20) (mean age 74.4 ± 12.58) or from the ICU (n = 20) (mean age 65.35 ± 21.37). Samples were processed immediately for detection of CD55 and CD59 on monocytes or stored in the −80 °C for detection of CD55 in CD4+ and CD8+ T cells and B cells. In order to determine levels of CD55 on the various cell types, we utilised two separate FACS protocols. A standard protocol used in routine clinical practice for detection of CD55 in monocytes was used in which 500 µl of freshly drawn blood was added to standard volumes of antibodies (Supplementary Table 2) and incubated in the dark for 15 min. Upon completion of incubation, FACS lysing solution (BD Biosciences, Franklin Lakes, NJ, USA) was added, and a further incubation for 15 min in the dark was performed. Samples were analysed in the flow cytometer immediately after lysing. The same procedure was utilised for the detection of CD55 in CD4+ and CD8+ T cells and B cells, with the difference that samples were thawed at room temperature before addition of antibodies. Antibodies used for detection are shown in Supplementary Table 3. The FACS Canto II flow cytometer (BD Biosciences) was used for analysis. Gating strategies are shown in Supplementary Figs. 5 and 6. FlowJo software was utilised for analysis of monocyte and granulocyte populations, whereas the BD FACSDiva software was used for analysis of the CD4+ and CD8+ T cells and B cell populations.
Transfection of T cells by nucleofection
PBMCs isolated from whole blood samples by centrifugation were transfected with siRNA for CD55 (IDT) using the Amaxa T cell nucleofection kit and a nucleofector according to the manufacturer’s instructions (Lonza, Bazel, Switzerland). Briefly, following isolation, 5 × 106 PBMC were centrifuged and washed with 0.5% BSA/PBS twice. Cell pellets were resuspended in 100 μl of nucleofection solution and siRNA and electroporated using the recommended nucleofector programme. Cells were immediately added to 2 ml of pre-warmed RPMI medium supplemented with 10% foetal bovine serum. The following day, cells were collected in order to determine transfection efficiency or used further for T cell sensitisation assays. Mock controls consisted of electroporated cells with nucleofection solution in the absence of siRNA.
T cell sensitisation assays
Following transfection, peptide pools (spike and nucleocapsid) (200 μl) were added to siCD55-transfected T cells and mock controls. The spike protein peptide mix (Spike XBB.1.5) contained peptides with the amino acid mutations present in the Spike protein of the Omicron XBB.1.5 variant, and the nucleoprotein (NCAP B.1.1.529/BA.1/Omicron) peptide pool contained amino acid mutations present in the nucleoprotein of the BA.1/Omicron strain and were obtained from JPT (JPT, Berlin, Germany). T cells (4 × 105) were incubated in the presence of peptide pools spanning the SARS-COV-2 spike protein (Spike XBB.1.5) and nucleoprotein (NCAP B.1.1.529/BA.1/Omicron) in 1640 RPMI medium containing 2 mmol/l LGlutamine,5% (v/v) human male AB serum, 1% MEM Non-Essential Amino Acids Solution (100X), and 1 mM Sodium Pyruvate Solution (100 mM). Incubations were performed for six hours, following which cell pellets were collected for RNA extractions with the Qiagen RNeasy kit according to the manufacturer’s instructions (Qiagen, Hilden, Germany). RNA concentration was determined for each sample prior to reverse transcription using NanoDrop One.
Statistical analysis
Results are reported as absolute numbers, medians, or means and standard deviations, as appropriate. Statistical analysis for sc-RNA-seq data was performed by a two-sided Wilcoxon rank sum test in R. Statistical analysis for Real-time PCR and FACS data was performed using the GraphPad Prism 8.0 software for Windows. Data were tested for normality using the Shapiro-Wilks test. One-way Anova or Kruskal-Wallis analysis of variance was used in the case of data displaying normality or not, respectively, in case of more than two groups comparisons. The Fisher’s least significant difference test was used for post-hoc analysis. Students t-test was used in the case of two-group comparisons. Receiver operating characteristic (ROC) analysis was performed using ICU admission as the classification variable and CD55 mRNA levels on admission as prognostic variables. P < 0.05 was considered statistically significant.
Reporting summary
Further information on research design is available in the Nature Portfolio Reporting Summary linked to this article.
Data availability
The full dataset associated with the scRNA-seq and bulk RNA sequencing analysis of the present study has been deposited and is available from the Gene Expression Omnibus (GEO). Accession numbers: GSE293707 and GSE293708. Protein expression raw data values from FACS analysis and gene expression raw data values from Real-time PCR analysis are available in the Supplementary Data file.
References
de Nooijer, A. H. et al. Complement activation in the disease course of coronavirus disease 2019 and its effects on clinical outcomes. J. Infect. Dis. 223, 214–224 (2021).
Alosaimi, B. et al. Complement anaphylatoxins and inflammatory cytokines as prognostic markers for COVID-19 severity and in-hospital mortality. Front. Immunol. 12, 668725 (2021).
Detsika M. G. et al. C3a and C5b-9 differentially predict COVID-19 progression and outcome. Life 12, 1335 (2022).
Magro, C. et al. Complement associated microvascular injury and thrombosis in the pathogenesis of severe COVID-19 infection: a report of five cases. Transl. Res. J. Lab. Clin. Med. 220, 1–13 (2020).
Ge, X. et al. Complement and complement regulatory proteins are upregulated in lungs of COVID-19 patients. Pathol. Res. Pract. 247, 154519 (2023).
Zipfel, P. F. & Skerka, C. Complement regulators and inhibitory proteins. Nat. Rev. Immunol. 9, 729–740 (2009).
Geller, A. & Yan, J. The role of membrane-bound complement regulatory proteins in tumor development and cancer immunotherapy. Front. Immunol. 10, 1074 (2019).
Hourcade, D. E., Mitchell, L. M. & Medof, M. E. Decay acceleration of the complement alternative pathway C3 convertase. Immunopharmacology 42, 167–173 (1999).
Liszewski, M. K., Post, T. W. & Atkinson, J. P. Membrane cofactor protein (MCP or CD46): newest member of the regulators of complement activation gene cluster. Annu. Rev. Immunol. 9, 431–455 (1991).
Ahearn, J. M. & Fearon, D. T. Structure and function of the complement receptors, CR1 (CD35) and CR2 (CD21). Adv. Immunol. 46, 183–219 (1989).
Davies, A. et al. CD59, an LY-6-like protein expressed in human lymphoid cells, regulates the action of the complement membrane attack complex on homologous cells. J. Exp. Med. 170, 637–654 (1989).
Merle, N. S., Church, S. E., Fremeaux-Bacchi, V. & Roumenina, L. T. Complement system Part I - molecular mechanisms of activation and regulation. Front. Immunol. 6, 262 (2015).
Cho, H. Complement regulation: physiology and disease relevance. Korean J. Pediatrics 58, 239–244 (2015).
Ricklin, D. & Lambris, J. D. Complement in immune and inflammatory disorders: pathophysiological mechanisms. J. Immunol. 190, 3831–3838 (2013).
Liu, J. et al. The complement inhibitory protein DAF (CD55) suppresses T cell immunity in vivo. J. Exp. Med. 201, 567–577 (2005).
Marie, J. C. et al. Linking innate and acquired immunity: divergent role of CD46 cytoplasmic domains in T cell induced inflammation. Nat. Immunol. 3, 659–666 (2002).
An, F. Q. et al. KLF4 and CD55 expression and function depend on each other. Front. Immunol. 14, 1290684 (2023).
Zhang, X. et al. Regulation of Toll-like receptor-mediated inflammatory response by complement in vivo. Blood 110, 228–236 (2007).
Stephenson, E. et al. Single-cell multi-omics analysis of the immune response in COVID-19. Nat. Med. 27, 904–916 (2021).
Wilk, A. J. et al. A single-cell atlas of the peripheral immune response in patients with severe COVID-19. Nat. Med. 26, 1070–1076 (2020).
Hadjadj, J. et al. Impaired type I interferon activity and inflammatory responses in severe COVID-19 patients. Science 369, 718–724 (2020).
Galani, I. E. et al. Untuned antiviral immunity in COVID-19 revealed by temporal type I/III interferon patterns and flu comparison. Nat. Immunol. 22, 32–40 (2021).
Nuutila, J. et al. Use of complement regulators, CD35, CD46, CD55, and CD59, on leukocytes as markers for diagnosis of viral and bacterial infections. Hum. Immunol. 74, 522–530 (2013).
Holter, J. C. et al. Systemic complement activation is associated with respiratory failure in COVID-19 hospitalized patients. Proc. Natl. Acad. Sci. USA 117, 25018–25025 (2020).
Sinkovits, G. et al. Complement overactivation and consumption predicts in-hospital mortality in SARS-CoV-2 infection. Front. Immunol. 12, 663187 (2021).
Ma, L. et al. Increased complement activation is a distinctive feature of severe SARS-CoV-2 infection. Sci. Immunol. 6, 2021.
Macor, P. et al. Multiple-organ complement deposition on vascular endothelium in COVID-19 patients. Biomedicines 9, 1003 (2021).
Lage, S. L. et al. Activation of complement components on circulating blood monocytes from COVID-19 patients. Front. Immunol. 13, 815833 (2022).
Trouillet-Assant, S. et al. Type I IFN immunoprofiling in COVID-19 patients. J. Allergy Clin. Immunol. 146, 206–208.e202 (2020).
Xu, G. et al. The differential immune responses to COVID-19 in peripheral and lung revealed by single-cell RNA sequencing. Cell Discov. 6, 73 (2020).
Lin, Q. X. X. et al. Longitudinal single cell atlas identifies complex temporal relationship between type I interferon response and COVID-19 severity. Nat. Commun. 15, 567 (2024).
Heeger, P. S. et al. Decay-accelerating factor modulates induction of T cell immunity. J. Exp. Med. 201, 1523–1530 (2005).
Fang, C., Miwa, T., Shen, H. & Song, W. C. Complement-dependent enhancement of CD8+ T cell immunity to lymphocytic choriomeningitis virus infection in decay-accelerating factor-deficient mice. J. Immunol. 179, 3178–3186 (2007).
Fang, C., Miwa, T. & Song, W. C. Decay-accelerating factor regulates T-cell immunity in the context of inflammation by influencing costimulatory molecule expression on antigen-presenting cells. Blood 118, 1008–1014 (2011).
Finberg, R. W., White, W. & Nicholson-Weller, A. Decay-accelerating factor expression on either effector or target cells inhibits cytotoxicity by human natural killer cells. J. Immunol. 149, 2055–2060 (1992).
Bali Swain, R., Lin, X. & Wallentin, F. Y. COVID-19 pandemic waves: identification and interpretation of global data. Heliyon 10, e25090 (2024).
Wolock, S. L., Lopez, R. & Klein, A. M. Scrublet: computational identification of cell doublets in single-cell transcriptomic data. Cell Syst. 8, 281–291.e289 (2019).
Wolf, F. A., Angerer, P. & Theis, F. J. SCANPY: large-scale single-cell gene expression data analysis. Genome Biol. 19, 15 (2018).
Polanski, K. et al. BBKNN: fast batch alignment of single cell transcriptomes. Bioinformatics 36, 964–965 (2020).
Park, J. E. et al. A cell atlas of human thymic development defines T cell repertoire formation. Science 367, eaay3224 (2020).
Andreatta, M. & Carmona, S. J. UCell: robust and scalable single-cell gene signature scoring. Comput. Struct. Biotechnol. J. 19, 3796–3798 (2021).
Squair, J. W. et al. Confronting false discoveries in single-cell differential expression. Nat. Commun. 12, 5692 (2021).
Wang, J., Vasaikar, S., Shi, Z., Greer, M. & Zhang, B. WebGestalt 2017: a more comprehensive, powerful, flexible and interactive gene set enrichment analysis toolkit. Nucleic Acids Res. 45, W130–W137 (2017).
Acknowledgements
We acknowledge financial support of this work by The Greek Research Infrastructure for Personalised Medicine (pMedGR) (MIS 5002802), funded by the Operational Programme ‘Competitiveness, Entrepreneurship and Innovation’ (NSRF 2014-2020) and co-financed by Greece and the European Union (European Regional Development Fund). We also acknowledge support by the Hellenic Foundation for Research and Innovation (H.F.R.I.) under the ‘1st Call for H.F.R.I. Research Projects to support Faculty members and Researchers and the procurement of high-cost research equipment’ (project Single.Out, #3780, to GK).
Author information
Authors and Affiliations
Contributions
MGD performed most of the experimental work, data analysis, and statistical analysis and wrote the manuscript. MS assisted with experimental work for scRNA-Seq analysis with 10X, data interpretation, and drafting of the manuscript. VT and DK performed the bioinformatics analysis. EG and KP performed part of and assisted with FACS analysis. AT, GK and AK provided resources. EJ provided access to all clinical samples of the study. Supervision was provided by ID, SEO, AT, GK and AK. All co-authors assisted with reviewing and editing the manuscript.
Corresponding authors
Ethics declarations
Competing interests
All authors declare no competing interests.
Peer review
Peer review information
Communications Biology thanks the anonymous reviewers for their contribution to the peer review of this work. Primary Handling Editors: Jian-Da Lin and Mengtan Xing.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Detsika, M.G., Sakkou, M., Triantafyllidou, V. et al. CD55 upregulation in T cells of COVID-19 patients suppresses type-I interferon responses. Commun Biol 8, 690 (2025). https://doi.org/10.1038/s42003-025-08066-z
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s42003-025-08066-z
