
Abstract
Background
This study examined associations between anomalous temperatures and under-five mortality (U5M) in low- and middle-income countries (LMICs).
Methods
Between 1998 and 2019, data were collected on 1,745,132 live births across 56 LMICs. The median age was 27.0 months (interquartile range: 12.0, 43.0), and 51.0% were male. Monthly temperature anomalies were calculated as deviations from the long-term average temperature for the same calendar months. We developed a two-dimensional exposure-response function (ERF) based on a varying-coefficient model to examine the relationship between U5M and both long-term average temperatures and anomalous temperatures.
Results
Here we show, in the multicenter model, each 1 °C increase in positive temperature anomalies or decrease in negative temperature anomalies is associated with an 8% (95% confidence interval [CI]: 6%, 11%) or 2% (95% CI: −1%, 4%) excess risk of U5M, respectively. The two-dimensional ERF reveals considerable heterogeneity in the impact of anomalous temperatures on U5M across different temperature zones. Positive temperature anomalies pose a significant hazard to children in warm and hot zones, whereas negative anomalies are primarily hazardous in cold zones but appear protective in hot zones. The sibling-matched model demonstrates nonlinear and heterogeneous effect estimates consistent with the multicenter model findings.
Conclusions
Anomalous temperatures of both heat and cold are associated with an increased risk of child mortality in LMICs, with the effect varying by temperature zone, reflecting the adaptive capacity of populations to local climates. There is an urgent need to develop regionally adaptive strategies to protect child health amid global climate change.
Plain language summary
Climate change is making weather more unstable, especially with unusual changes in temperature. These changes can be harmful to children’s health. While we already know that short-term exposure to very hot or cold weather can increase the risk of death in children, we know less about the effects of longer-lasting unusual temperatures. In this study, we looked at how abnormal temperature changes affect child deaths in low- and middle-income countries. We found that both unusual heat and cold can raise the risk of children dying, and the impact is different in each region depending on the local climate. This means we need climate-based health plans that are tailored to different regions to better protect children’s health.
Similar content being viewed by others

Introduction
Climate change is increasingly recognized as a major public health concern, significantly impacting survival rates worldwide1. It is estimated that climate change has displaced approximately 600 million people beyond the human climate niche, with projections indicating that up to 3 billion people may live outside the ideal temperature range by the end of this century2. From 2013 to 2022, the global 10-year mean temperature rose to 1.14 °C above pre-industrial levels1. Recent estimates suggest that around 1.9 million (95% confidence interval [CI]: 1.7, 2.2 million) premature deaths could be attributed to exposure to non-optimal temperatures globally3. The accelerating pace of global warming has led to unprecedented changes in the intensity and variability of temperature exposure4, with increasingly frequent reports of extreme temperature events across many regions5.
Growing evidence has linked exposure to non-optimal temperatures with increased risks of morbidity and mortality4,6,7,8. However, limited evidence exists on the health effects of temperature anomalies, particularly in the middle to long term, despite the widespread use of anomalies as an indicator of weather stability in climate science4,9,10,11. Moreover, most existing studies focus on developed countries, such as the United States4 and Australia12, and the region of New England10, whereas low- and middle-income countries (LMICs) are disproportionately impacted by climate change and experience the most pronounced temperature anomalies13. LMICs face considerable challenges in adapting to and mitigating climate-related threats due to limited resources. Previous studies have highlighted that children are among the most vulnerable to climate change effects due to their underdeveloped physical and immune systems9,14. According to World Bank estimates, over 98% of under-five mortalities (U5M) occur in LMICs. Therefore, understanding the specific adverse health effects of anomalous temperatures on children in LMICs is crucial for improving child health outcomes and addressing climate-related health inequities. However, quantitative evidence on the association between U5M and anomalous temperature remains limited.
Mitigating climate change requires precise quantification of the attributable disease burden, which in turn relies on accurate estimates of the exposure-response function (ERF) between temperature and mortality6,7,8. One of the key challenges in current ERF estimates is characterizing the geographical heterogeneity in temperature-related health effects. Existing efforts have attempted to address this by incorporating multicenter population data and modeling variations in center-specific effects as an empirical function of geographic features such as climate zone, socioeconomic status, and land use. However, explainable heterogeneities in temperature-related health effects remain underexplored. One important factor is adaptation to the local temperature zone, represented by long-term average temperatures. To clarify this, it is essential to focus on the health effects of temperature variations that are independent of long-term averages. Temperature anomaly, defined as the deviation from the long-term average, captures this partial variation, enabling its effect to be analyzed independently and parametrized by temperature zone. In other words, developing a generalizable and explainable ERF for temperature and mortality requires incorporating the health effects of both average and anomalous temperatures. The resulting ERF between temperature and U5M could support the creation of early warning systems tailored to local climate conditions, helping to mitigate health risks associated with climate change.
In this study, using multicenter data from 1,745,132 live births across 56 LMICs, we examined the heterogeneous association between temperature anomalies and U5M. Employing a varying-coefficient nonlinear model, we derived a two-dimensional ERF that parametrizes the nonlinear effects of temperature anomalies on U5M as a function of temperature zone. Findings from this study provide a foundation for accurately quantifying the burden of child mortality attributable to global temperature changes in the future.
Methods
Study population
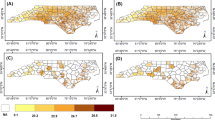
Individual data on 1,745,132 live births across 56 LMICs (Fig. 1) were obtained from demographic and health surveys (DHSs) for this multicenter analysis. Briefly, each DHS survey used a stratified two-stage cluster design to conduct a nationally representative household survey, collecting data on fertility, mortality, reproductive health, and child health in a specific LMIC. Standardized questionnaires were administered by trained fieldworkers to women of reproductive age (15–49 years), gathering household information, fertility history, and the survival status of children born within the five years preceding the survey date. Survey cluster coordinates were routinely recorded in recently surveyed countries using global positioning system devices. To protect respondent confidentiality, the DHS program applied random displacement to the geographic coordinates, introducing a positional error of 0–2 km for urban clusters and 0–5 km for rural clusters. Further methodological details on the child health and geographic information collected by DHS are available on the official website (https://dhsprogram.com/) and in our previously published works15,16,17. The DHS data are publicly accessible, and data collection and use were reviewed and approved by the ICF Institutional Review Board (IRB). Additionally, country-specific DHS survey protocols are reviewed by the ICF IRB and typically by an IRB in the host country. ICF IRB ensures that the survey complies with the U.S. Department of Health and Human Services regulations for the protection of human subjects, while the host country IRB ensures that the survey complies with laws and norms of the nation. Informed consent has been obtained from each participant or from a parent or legal guardian in the case of children and adolescents. Protocol numbers and additional ethical details are available on the official DHS website. All DHS datasets are freely available for research purposes upon registration and approval through the DHS Program’s official data request platform.

In (a), the color of pixels shows the distribution of long-term average temperature respectively, and its transparency shows the corresponding size of population at exposure (i.e., under-5 children). In (b), the color of pixels shows the distribution of average monthly temperature anomalies by positive and negative changes. c, d Display spatial distribution of the analyzed samples of under-5 children from 56 LMICs, for the multicenter design and the siblings-matched design. PER Peru, NGA Nigeria, IND India, and IDN Indonesia.
The study period was restricted to 1998–2019 due to the availability of particulate matter (PM2.5) data, a key confounder in analyzing the association between temperature and mortality. Children were eligible for inclusion if they had valid survival information, accurate geographic data for exposure assessment, and recorded dates of birth. Ultimately, 1,745,132 live births from 142 surveys conducted across 56 LMICs were included in the analyses.
Exposure assessment
The household cluster coordinates of surveyed children were used to assess environmental exposure. These environmental exposure data were then matched to the corresponding health data of children for statistical analysis. The primary exposure period was defined as one month prior to the survey date for surviving children and one month prior to the date of death for deceased children. Monthly temperature data were sourced from the enhanced global dataset for the land component of the fifth generation of European Reanalysis (ERA5-Land)18. ERA5-Land generates state-of-the-art numerical weather estimates by integrating data from in-situ observations, satellite remote sensing, and numerical weather predictions. This dataset provides a highly accurate and consistent view of meteorological variable trends extending back decades to the near present, with a high spatial resolution of approximately 10 × 10 km. Its high temporal and spatial resolution make ERA5-Land a valuable resource for environmental studies.
Following previous studies4,19,20,21,22,23, we calculated monthly temperature anomalies (a) as deviations in the current temperature at a specific location (Ts,y,m) from the historic long-term average for that month (μs,m), based on time-series temperature data from 1998 to 2019 for each pixel. The calculation is represented by the following equations:
where s, y, and m denote indices for the spatial pixel, calendar year, and month, respectively. Unlike the temperature exposure variable, this measure captures variations in the distribution and intensity of extreme temperature shocks across locations and may assume positive or negative values. A positive anomaly indicates that the observed temperature for that month exceeded the location-specific norm, while a negative anomaly indicates a temperature below the location-specific norm. Using 10 × 10 km grid data on monthly average and anomalous temperatures, along with corresponding under-five child population data from WorldPop, we calculated the annually long-term average and anomalous temperatures across the studied LMICs, weighted by the under-five child population. These values were derived as the sum of the product of each grid’s population fraction and the respective annual long-term average or anomalous temperature.
To adjust for environmental confounders, we also collected monthly average precipitation and PM2.5 data for each child. Precipitation data was sourced from the ERA5-Land dataset, whereas PM2.5 data, with a resolution of 1 × 1 km, was obtained from a comprehensive global product. This PM2.5 dataset combines multiple data sources, including satellite retrievals of aerosol optical depth, chemical transport models, and ground-based measurements24.
Statistics and reproducibility
In this study, we utilized two distinct study designs—the multicenter cohort design and the siblings-matched design—to estimate the association between U5M and temperature anomalies among children in LMICs. By comparing the estimates from both designs, we aimed to evaluate the robustness of the findings. The siblings-matched design, which we have applied in previous studies16,25, is a well-established approach to investigate associations between environmental exposures and adverse health outcomes in children. In the siblings-matched design, each deceased child (case) is matched with their surviving siblings from the same mother, who serve as controls. This design allows for a comparison of temporal variations in environmental exposures between deceased cases and their surviving siblings. A primary advantage of this approach is that it inherently controls for observed and unobserved time-invariant household and maternal confounders, such as genetic factors and socioeconomic status. However, this approach only includes a selective subset of the sample, which may affect the representativeness of the data to some extent.
For both study designs, we estimated the linear associations between anomalous temperature and U5M using a Cox regression model with fixed effects, which is equivalent to the conditional Cox regression model. The model can be parameterized as follows:
where hi,j(t) represents the hazard function for the jth child, and t denotes survival time (age in months). Here, a is the level of temperature anomaly exposure, z represents adjusted covariates, θ is the fixed effect, and β and γ are the corresponding coefficients. In the multicenter analysis, i denotes the sampling center index, with θi serving as a fixed effect to control for the center-specific baseline of child mortality. In the siblings-matched analysis, i refers to the family ID (where all children born to the same mother are considered a family unit), and θi functions as a fixed effect to control for family-level invariant risk factors.
The covariates (z) considered in our study included several categories: environmental factors, including PM2.5 concentration and a precipitation variable modeled as a spline function with three degrees of freedom (DF); demographic factors, including child sex and breastfeeding status; pregnancy-related factors, such as delivery method (cesarean section or not), place of delivery, number of antenatal visits, singleton or multiple birth status, and parity (nulliparous or multiparous); maternal factors, including a 3-DF spline for maternal age, a 3-DF spline for birth interval (months), maternal body mass index, and maternal employment status; household factors, encompassing the sex of household head, a 3-DF spline for household head’s age, source of drinking water, type of toilet, and type of cooking fuel; and spatiotemporal factors, which included a 10-DF spline function for survey year, season of survey, and Köppen Climate Zones26. To balance model complexity and accuracy, the degrees of freedom for the spline functions were determined based on both the Akaike Information Criterion and previous studies16,25. To handle missing values in several covariates, we used multivariate imputation by chained equations (MICE) approach and performed a single imputation (i.e., number of imputations set to one)16,27. To ensure data representativeness, household sampling weights provided by the DHS program were incorporated into the Cox regression model using the weights argument in the coxph function. For sensitivity analysis, we adjusted the exposure timeframe to cover the period from 2 to 6 months prior to the outcome dates to explore the lagged effect of anomalous temperature.
To investigate the nonlinear associations between U5M and anomalous temperature, we first stratified the study population based on exposure to either positive or negative temperature anomalies. Then, we developed a V-shaped model to assess the distinct effects of each anomaly type on U5M by incorporating an interaction term between subpopulation type (positive vs. negative anomaly exposure) and anomalous temperature in the Cox regression model. Subsequently, we examined the nonlinear exposure-response relationship between U5M and anomalous temperature by incorporating a natural spline function of temperature anomalies within the Cox regression model. The nonlinear model can be parameterized as follows:
where ns(ai,j, DF = 3) represents the nonlinear natural spline function of temperature anomalies with three degrees of freedom.
Additionally, we explored geographical heterogeneity in the impacts of anomalous temperature on U5M across LMICs. A series of subpopulation analyses were conducted to estimate the heterogeneous associations between U5M and anomalous temperature by different temperature zones and subpopulations with varying socioeconomic status. Using a varying-coefficient regression model, we examined how linear associations between U5M and temperature anomalies varied with long-term average temperature. The varying-coefficient model was parameterized as follows:
where f (ai,j | μi,j) represents the linear association between U5M and anomalous temperature, which varies according to the long-term average temperature (μi,j).
Finally, we assessed geographical heterogeneity in the nonlinear associations between U5M and anomalous temperature. Through subpopulation analysis, we initially examined individual effects of exposure to either positive or negative temperature anomalies on U5M across various temperature zones, and subsequently developed nonlinear ERFs that link U5M to temperature anomalies specific to each temperature zone. Employing a varying-coefficient nonlinear regression model, we incorporated the interaction between average and anomalous temperatures to construct a two-dimensional ERF, capturing the nonlinear impact of temperature anomalies on U5M as a function of temperature zone. This approach enables effect estimates across diverse combinations of average and anomalous temperature exposures. The varying-coefficient nonlinear regression model was achieved by parameterizing f(ai,j | μi,j) in Equation 4 as a cross-product of two spline terms: one for anomalous temperature and another for long-term average temperature.
All statistical analyses were performed using R software (version 4.1.3; The R Foundation for Statistical Computing, Vienna, Austria). The fixed-effects Cox regression model was implemented using the R package survival, and data imputation was conducted with the mice package.
Reporting summary
Further information on research design is available in the Nature Portfolio Reporting Summary linked to this article.
Results
Population characteristics
In the multicenter analysis, a total of 1,745,132 children were included, with a median survival duration of 27.0 months (interquartile range [IQR]: 12.0, 43.0); 890,210 (51.0%) were male. The monthly long-term average temperature for these children was 24.1 °C (standard deviation [SD]: 5.12), and the median temperature anomaly was 0.01 °C (IQR: –0.39, 0.43). Surviving children had a median temperature anomaly of 0.01 °C (IQR: –0.39, 0.43), compared to –0.03 °C (IQR: –0.43, 0.39) for deceased children. Basic population characteristics are provided in Supplementary Data 1. For the siblings-matched design, 120,868 children were analyzed, with an average survival length of 17.0 months (SD: 17.5). The monthly long-term average temperature for this group was 24.6 °C (SD: 4.84), with a median temperature anomaly of –0.02 °C (IQR: –0.40, 0.40). Figure 1 illustrates the spatial distribution of average and anomalous temperature levels across the 56 LMICs included in the study. For these LMICs, the annually long-term average temperature, weighted by the under-five child population, was 22.26 ± 3.23 °C, with weighted average monthly temperature anomalies ranging from –2.14 °C to 1.89 °C.
Associations between U5M and anomalous temperature
Using both the multicenter and siblings-matched designs, we evaluated the nonlinear exposure-response relationship between U5M and temperature anomalies (Fig. 2). Our analysis uncovered a U-shaped relationship, indicating that both positive and negative temperature anomalies contributed to increased U5M risk. Notably, positive temperature anomalies had a pronounced impact on child health, with risk escalating sub-linearly as temperature anomalies intensified. In contrast, the hazardous effects of negative temperature anomalies in our study population did not reach statistical significance. Both the multicenter and siblings-matched designs produced ERFs with comparable trends, underscoring the robustness of our findings.

The nonlinear exposure-response relationships are shown as lines with 95%-CI error ribbons (n = 1,745,132 biologically independent samples for the multicenter design and n = 120,868 for the siblings-matched design).
Additionally, we examined the linear associations between U5M and anomalous temperature across various average temperature levels (Supplementary Figs. S1 and S2). In the fully-adjusted, weighted multicenter model, each 1 °C increase in temperature anomalies corresponded to a 1% excess risk of U5M (95% CI: –1%, 3%) (Supplementary Fig. S1). The siblings-matched model indicated a higher excess risk, estimating a 5% increase in U5M risk (95% CI: 1%, 10%) per 1 °C anomaly increase. The siblings-matched design provided stricter control over family-invariant confounders, thus producing estimates with lower bias but higher variance compared to the multicenter model. In both models, the estimated U5M association with temperature anomalies remained largely consistent across varying levels of confounder adjustments and regression weights, although spatiotemporal heterogeneity impacted these associations. Stratifying the study population based on exposure to positive and negative temperature anomalies (Supplementary Fig. S2) revealed that, in the multicenter model, each 1 °C increase in positive temperature anomalies or decrease in negative temperature anomalies corresponded to an 8% (95% CI: 6%, 11%) and 2% (95% CI: –1%, 4%) excess risk of U5M, respectively, suggesting a U-shaped nonlinear association. Further, lagged effect analysis indicated that the impact of exposure to either positive or negative temperature anomalies on U5M persisted for several months post-exposure (Supplementary Figs. S2 and S3). When using different epidemiological designs, we found various structures of lagged effects (i.e., a 2-months lag reported by the multicenter analysis, and a 4-months lag by the sibling-matched analysis).
Heterogeneous linear effects of anomalous temperature
Our findings indicate substantial heterogeneity in the association between U5M and temperature anomalies, influenced by both temperature zones and certain socioeconomic factors (Fig. 3, Supplementary Figs. S4 and S5). Utilizing a varying-coefficient regression model, we quantified the diverse associations between U5M and temperature anomalies across long-term average temperature levels (Fig. 3). For children residing in warmer regions (long-term average temperatures exceeding 22.5 °C), we observed a positive correlation between U5M and temperature anomalies, indicating elevated mortality risk with increasing anomalies. Conversely, in cooler regions (average temperatures below 22.5 °C), the association was negative. Further stratification by socioeconomic status (Supplementary Fig. S5) revealed that the adverse impact of anomalous temperatures was particularly pronounced among children from lower socioeconomic backgrounds, especially those living in rural areas and in households lacking access to improved sanitation, drinking water, and clean cooking energy sources.

The heterogeneous linear associations between U5M and temperature anomalies by different temperature zones are shown as points with 95%-CI error bars (n = 1,745,132 biologically independent samples for the multicenter design and n = 120,868 for the siblings-matched design). The nonlinear associations between U5M and temperature anomalies across long-term average temperature levels are shown as lines with 95%-CI error ribbons.
We further analyzed the heterogeneous impacts of exposure to either positive or negative temperature anomalies on U5M by temperature zones (Supplementary Fig. S4). Results indicate that positive temperature anomalies exposure was significantly hazardous across both hot and cold regions. Based on the multicenter study, the most pronounced effect of positive temperature anomalies was observed in areas with a long-term average temperature of 25–30 °C. Here, a 1 °C increase in positive temperature anomaly corresponded to a hazard ratio (HR) of 1.16 (95% CI: 1.12, 1.19). The effect was weakest in regions where the average temperature was below 15 °C, showing an HR of 1.09 (95% CI: 1.01, 1.18). Exposure to negative temperature anomalies, on the other hand, primarily posed significant risks in colder regions (average temperatures below 15 °C), with each 1 °C decrease in negative temperature anomaly associated with an HR of 1.32 (95% CI: 1.22, 1.42).
Two-dimensional ERF
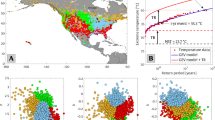
We initially examined heterogeneity in the nonlinear ERFs between U5M and temperature anomalies across various temperature zones, employing a multicenter analysis (Fig. 4a). For children in colder regions, with an average temperature below 12.5 °C, there was a positive association between U5M and negative temperature anomalies, while no significant effect was observed for positive temperature anomalies. In warmer regions, with average temperatures between 12.5 and 27.5 °C, the ERFs displayed a U-shaped pattern: as the average temperature increased, risks associated with positive temperature anomalies intensified, whereas risks related to negative anomalies exposure decreased. In hotter regions, where the average temperature exceeded 27.5 °C, we observed a positive association between U5M and anomalous temperature, with significant risk estimates for negative anomalies but nonsignificant estimates for positive anomalies.

a Shows the estimated nonlinear associations between under-5 mortality (U5M) and anomalous temperature by different temperature zones, based on subpopulation analysis using a multicenter design (n = 1,745,132 biologically independent samples). The exposure-response relationships are shown as solid lines with 95%-CI ribbons. b Shows different slices of the two-dimensional exposure-response function estimated in (c) as solid lines with 95%-CI ribbons. c Shows the varied nonlinear associations estimated by a varying-coefficient nonlinear model. The directly estimated effect are presented both as a two-dimensional function of long-term temperature and its anomaly and as a function of temperature and its long-term average. c Illustrates how to infer the effect of temperature by correlating its fluctuations to variation in U5M.
Using a varying-coefficient nonlinear model, we constructed a two-dimensional ERF that correlates U5M with both average and anomalous temperatures and estimated ERF slices stratified by temperature zones, with a high excess risk of U5M indicating a low capacity of adaptability to anomalous temperature (Fig. 4). The ERF slices derived from the two-dimensional ERF (Fig. 4b) align with the temperature-zone-stratified ERF analysis (Fig. 4a), thereby affirming the robustness of the ERFs in capturing heterogeneity due to long-term adaptation to temperature. The two-dimensional ERF (Fig. 4c) elucidates the differential excess risks of U5M across various combinations of average and anomalous temperature exposures, thus capturing the nonlinear effects of temperature anomalies on U5M across different temperature zones. Here, we emphasize findings from the multicenter analysis, with the sibling-matched analysis results available in the supplement (Supplementary Fig. S6), which showed comparable trends. As shown in Fig. 4c, positive temperature anomalies significantly impacted children in warm and hot regions (average temperature >15 °C, as shown on the x axis of Fig. 4c), whereas negative anomalies were mainly detrimental for children in colder and moderate regions (average temperature <25 °C) but seemed to provide a protective effect for those in hotter regions (average temperature >25 °C).
Discussion
Using nationally representative U5M data from 56 LMICs, this study constructs a two-dimensional ERF linking U5M with both average and anomalous temperatures. Our findings reveal that associations between U5M and anomalous temperature differ across temperature zones, highlighting varying human adaptation capacities to local climates. Positive temperature anomaly is a significant hazard for children in warm and hot regions, whereas negative anomaly predominantly poses risks in colder zones, though it appears to have a protective effect for children in hotter zones. Sensitivity analyses using the siblings-matched model confirm nonlinear and heterogeneous effect estimates consistent with the multicenter model, reinforcing the robustness of our findings.
Temperature anomalies are projected to become more frequent as global climate change progresses. However, there are limited data on how these anomalies affect human health. Using time-series data on mortality and temperature over 38 years (1980–2017) in the USA, Parks et al.23 found that a 1.5 °C anomalously warm year, where each month was 1.5 °C warmer than its long-term average, was associated with an estimated 1601 (95% CI: 1430, 1776) additional injury deaths. They also observed seasonal variations in the relationship between injury deaths and monthly temperature anomalies, with stronger effects of anomalously warm temperatures during hotter months. A cohort study among the Medicare population (aged > 65 years) in New England revealed that a 1 °C increase in the annual anomaly in summer and winter mean temperatures was associated with a 5% (95% CI: 4%, 6%) and a 1.5% (95% CI: 1%, 2%) increased risk of mortality, respectively28. Several epidemiological studies have explored the effects of temperature variations on mortality. A cohort study in older hypertensive patients in China found a significant association between monthly temperature variation (the standard deviation of daily average temperatures) and an elevated risk of mortality (relative risk: 1.097, 95% CI: 1.051, 1.146)29. Based on daily temperature and mortality data from 372 locations across 12 countries/regions, Guo et al.30 assessed weekly temperature variability using the standard deviation of minimum and maximum temperatures during exposure days and found significant associations between mortality and temperature variability in cold, hot, and moderate seasons. They also observed that mortality risks associated with weekly temperature variability were higher in moderate areas than in cold and hot areas. Overall, our results were generally consistent with previous findings, confirming that anomalous temperatures deviating from the long-term local norm were significantly associated with mortality.
Few existing studies have investigated associations between child mortality and temperature, with most focusing on short-term average temperature and extreme temperature exposures14. For example, Dimitrova et al.31 conducted a time-stratified case-crossover analysis to quantify the nonlinear association between daily ambient temperature and neonatal mortality, observing a U-shaped ERF. They estimated that 4.3% of neonatal deaths were associated with non-optimal temperatures across 29 LMICs. Son et al.32 examined mortality from heatwaves in seven major Korean cities and did not observe a significant association between heatwave exposure and mortality in children under 14 years. Although low-income countries are expected to be more vulnerable to environmental threats, evidence is still limited due to challenges in data access. In low-resource settings, where daily exposure data may be inaccessible, monthly exposure data play a crucial role in providing unbiased estimates of the effects of environmental exposures33. Our study adds evidence to the U5M risk associated with anomalous temperature in LMICs.
Previous studies have suggested several biological mechanisms underlying the health impacts of long-term temperature exposure and temperature anomalies34,35. First, both long-term temperature and its variabilities can have direct effects on the respiratory and urinary systems. For instance, positive associations have been observed between non-optimal temperature exposure and respiratory diseases36,37, such as asthma38, and kidney-associated diseases39. Second, the distribution of disease-carrying vectors and the transmission of infectious pathogens are expected to be altered at different temperature zones and variabilities. Infectious diseases associated with these changes tend to disproportionately affect children in general, particularly those from socioeconomically vulnerable backgrounds. Third, non-optimal temperatures and high temperature variability can complicate access to clean food and water, exacerbating child malnutrition and heightening the risk of infections. Additionally, there is substantial evidence that the human thermoregulation system fails to respond effectively when anomalous temperatures of cold or heat exceed their thresholds, which can directly contribute to child mortality4.
Population adaptation plays a crucial role in determining climate-related health risks, yet it has not been explicitly modeled in previous studies. Adaptation to temperature may occur through various mechanisms, such as physiological acclimatization, behavioral adjustments (e.g., clothing choices and spending more time indoors), and planned adaptation measures (e.g., air-conditioning installation and public health interventions such as early warning systems)40,41. In this study, we characterized population adaptation to temperature by examining vulnerability to temperature anomalies. Through the derived nonlinear exposure-response relationship between mortality and temperature anomalies, we observed varying human capacity to adapt to positive and negative temperature anomalies. Geographical differences in the adverse impacts of temperature anomalies across different temperature zones provide valuable insights into how populations in LMICs adapt to local temperature conditions. These findings help clarify previously inconsistent results regarding the link between child mortality and ambient temperature. Additionally, the remarkable variation in geographical and social vulnerability to positive and negative temperature anomalies underscores the potential for targeted interventions to enhance the resilience of communities most at risk. Our study reveals the complexity of temperature-associated health impacts. The two-dimensional ERF between anomalous temperature and mortality offers a framework to understand and characterize the geographical heterogeneity and nonlinearity of health effects of temperature. By incorporating local temperature conditions and population adaptation, the two-dimensional ERF provides broader generalizability across diverse climate regions and can pave the way for more precise quantification of the future burden of child mortality attributable to global temperature changes.
Despite the valuable insights provided by this study, several limitations should be acknowledged. First, the exposure assessment may be biased due to constraints in the DHS data. This potential bias arises from the displacement of global positioning system coordinates for survey clusters and the possibility that participants may have relocated during the study period. Second, we selected a one-month exposure window prior to the outcome to provide a conservative estimate of the effect of anomalous temperature. However, given the lagged effects of temperature anomalies identified in Fig. S2, this approach may underestimate the cumulative impact of both positive and negative anomalies over a longer period. Third, the information on U5M in DHS surveys was self-reported by mothers, which introduces potential recall bias in our outcome assessment. Additionally, some under-five deaths may have been underreported due to social stigma associated with reporting such incidents. Fourth, due to the computational burden of handling a large dataset, we performed a single imputation using the MICE approach. While this method is commonly used in large-scale studies16,27, it may not fully account for the uncertainty associated with imputation, as multiple imputation methods do. This could lead to an underestimation of the variability in the estimated association coefficients. Fifth, the regression models did not account for certain crucial confounders, such as family socioeconomic characteristics, genetic factors, and individual adaptation to climate change, due to data limitations. However, we conducted a sensitivity analysis using a sibling-matched design, which allowed us to adjust for time-invariant household and maternal confounders. Our estimates remained generally robust across different study designs. Sixth, stillbirths were not included in our analyses, which might lead to an underestimation of the U5M burden attributable to anomalous temperature. Finally, we assumed the ERF between U5M and anomalous temperature was homogeneous across different LMICs. However, the generalizability of the estimated ERF may be limited by the disproportionate representation of Asian countries in our sample and the varying adaptation capacities to climate change across different countries. Therefore, cautious interpretation of our findings is necessary when assessing location-specific attributable burdens based on the estimated ERF.
Based on a large-scale dataset from 56 LMICs, this study adds to evidence that temperature anomalies, whether in the form of heat or cold, are associated with an increased risk of child mortality in LMICs. The effect of anomalous temperature varied across different temperature zones, reflecting the capacity of human populations to adapt to local climates. These findings highlight the urgent need for region-specific adaptive strategies to safeguard child health in the face of global climate change.
Data availability
The demographic and health surveys (DHS) datasets used in this study are publicly available on the official DHS website (https://dhsprogram.com/). All DHS datasets are freely available for research purposes upon registration and approval through the DHS Program’s official data request platform. The source data for Fig. 3 is in Supplementary Data 2. Any additional information required for reanalyzing the data reported in this paper is available from the corresponding author on reasonable request.
Code availability
All analyses were conducted using R (version 4.1.3; The R Foundation for Statistical Computing, Vienna, Austria). The R codes for the data collection and epidemiological analyses are available from the corresponding author on reasonable request.
References
Romanello, M. et al. The 2023 report of the Lancet Countdown on health and climate change: the imperative for a health-centred response in a world facing irreversible harms. Lancet 402, 2346–2394 (2023).
Lenton, T. M. et al. Quantifying the human cost of global warming. Nat. Sustain.6, 1237–1247 (2023).
Ferrari, A. J. et al. Global incidence, prevalence, years lived with disability (YLDs), disability-adjusted life-years (DALYs), and healthy life expectancy (HALE) for 371 diseases and injuries in 204 countries and territories and 811 subnational locations, 1990-2021: a systematic analysis for the Global Burden of Disease Study 2021. Lancet 403, 2133–2161 (2024).
Liu, H. et al. Deaths attributable to anomalous temperature: a generalizable metric for the health impact of global warming. Environ. Int. 169, 107520 (2022).
Li, C. et al. Changes in annual extremes of daily temperature and precipitation in CMIP6 Models. J. Clim. 34, 3441–3460 (2021).
Gasparrini, A. et al. Mortality risk attributable to high and low ambient temperature: a multicountry observational study. Lancet 386, 369–375 (2015).
Zhao, Q. et al. Global, regional, and national burden of mortality associated with non-optimal ambient temperatures from 2000 to 2019: a three-stage modelling study. Lancet Planet Health 5, e415–e425 (2021).
Zafeiratou, S. et al. A systematic review on the association between total and cardiopulmonary mortality/morbidity or cardiovascular risk factors with long-term exposure to increased or decreased ambient temperature. Sci. Total Environ. 772, 145383 (2021).
Wu, Y. et al. Global, regional, and national burden of mortality associated with short-term temperature variability from 2000-19: a three-stage modelling study. Lancet Planet Health 6, e410–e421 (2022).
Shi, L., Kloog, I., Zanobetti, A., Liu, P. & Schwartz, J. D. Impacts of temperature and its variability on mortality in New England. Nat. Clim. Change 5, 988–991 (2015).
Zhang, Y., Yu, C., Bao, J. & Li, X. Impact of temperature variation on mortality: an observational study from 12 counties across Hubei Province in China. Sci. Total Environ. 587-588, 196–203 (2017).
Cheng, J. et al. Impacts of heat, cold, and temperature variability on mortality in Australia, 2000-2009. Sci. Total Environ. 651, 2558–2565 (2019).
Bathiany, S., Dakos, V., Scheffer, M. & Lenton, T. M. Climate models predict increasing temperature variability in poor countries. Sci. Adv.4, eaar5809 (2018).
Lewis, J. Z. W., Corey, J. A. B., Melinda, A. J., Chitra, M. S. & Peter, N. L. S. How climate change degrades child health: a systematic review and meta-analysis. Sci. Total Environ.920, 170944–170944 (2024).
Li, P. et al. Source sectors underlying PM2.5-related deaths among children under 5 years of age in 17 low- and middle-income countries. Environ. Int.172, 107756 (2023).
Xue, T. et al. Estimating the exposure-response function between long-term ozone exposure and under-5 mortality in 55 low-income and middle-income countries: a retrospective, multicentre, epidemiological study. Lancet Planetary Health 7, e736–e746 (2023).
Tong, M. et al. Estimating birthweight reduction attributable to maternal ozone exposure in low- and middle-income countries. Sci. Adv.9, eadh4363 (2023).
Muñoz-Sabater, J. et al. ERA5-Land: a state-of-the-art global reanalysis dataset for land applications. Earth Syst. Sci. Data 13, 4349–4383 (2021).
Guo, J. et al. Ambient temperature anomalies induce electrocardiogram abnormalities: findings from a nationwide longitudinal study. Environ. Res. 246, 117996 (2024).
Xue, T. et al. Quantifying the contribution of temperature anomaly to stroke risk in China. Environ. Res. Lett.15, 105014 (2020).
Xue, T. et al. Variation in under-5 mortality attributable to anomalous precipitation during El Niño–Southern Oscillation cycles: Assessment of the intertemporal inequality in child health. Glob. Environ. Change 87, 102879 (2024).
Dimitrova, A., McElroy, S., Levy, M., Gershunov, A. & Benmarhnia, T. Precipitation variability and risk of infectious disease in children under 5 years for 32 countries: a global analysis using Demographic and Health Survey data. Lancet Planet Health 6, e147–e155 (2022).
Parks, R. M. et al. Anomalously warm temperatures are associated with increased injury deaths. Nat. Med. 26, 65–70 (2020).
van Donkelaar, A. et al. Monthly global estimates of fine particulate matter and their uncertainty. Environ. Sci. Technol.55, 15287–15300 (2021).
Xue, T. et al. Estimation of stillbirths attributable to ambient fine particles in 137 countries. Nat. Commun.13, 6950 (2022).
Beck, H. E. et al. Present and future Köppen-Geiger climate classification maps at 1-km resolution. Sci. Data 5, 180214 (2018).
Hurst, M., O’Neill, M., Pagalan, L., Diemert, L. M. & Rosella, L. C. The impact of different imputation methods on estimates and model performance: an example using a risk prediction model for premature mortality. Popul. Health Metrics 22, 13 (2024).
Shi, L., Kloog, I., Zanobetti, A., Liu, P. & Schwartz, J. D. Impacts of temperature and its Variability on Mortality in New England. Nat. Clim. Chang 5, 988–991 (2015).
Qi, X. et al. The effects of ambient temperature on non-accidental mortality in the elderly hypertensive subjects, a cohort-based study. BMC Geriatr. 24, 746 (2024).
Guo, Y. et al. Temperature variability and mortality: a multi-country study. Environ. Health Perspect 124, 1554–1559 (2016).
Dimitrova, A. et al. Temperature-related neonatal deaths attributable to climate change in 29 low- and middle-income countries. Nat. Commun.15, 5504 (2024).
Son, J. Y., Lee, J. T., Anderson, G. B. & Bell, M. L. The impact of heat waves on mortality in seven major cities in Korea. Environ. Health Perspect 120, 566–571 (2012).
Basagaña, X. & Ballester, J. Unbiased temperature-related mortality estimates using weekly and monthly health data: a new method for environmental epidemiology and climate impact studies. Lancet Planet Health 8, e766–e777 (2024).
Helldén, D. et al. Climate change and child health: a scoping review and an expanded conceptual framework. Lancet Planet Health 5, e164–e175 (2021).
Perera, F. & Nadeau, K. Climate change, fossil-fuel pollution, and children’s health. New Engl. J. Med. 386, 2303–2314 (2022).
Tong, M. et al. Hospitalization costs of respiratory diseases attributable to temperature in Australia and projections for future costs in the 2030s and 2050s under Climate Change. Int. J. Environ. Res. Public Health 19, 9706 (2022).
Tong, M. X. et al. Emergency department visits and associated healthcare costs attributable to increasing temperature in the context of climate change in Perth, Western Australia, 2012–2019. Environ. Res. Lett.16, 065011 (2021).
Lu, C. et al. Interaction effect of prenatal and postnatal exposure to ambient air pollution and temperature on childhood asthma. Environ. Int.167, 107456 (2022).
Wen, B. et al. Association between ambient temperature and hospitalization for renal diseases in Brazil during 2000–2015: a nationwide case-crossover study. Lancet Region. Health – Americas 6, https://doi.org/10.1016/j.lana.2021.100101 (2022).
Cordiner, R., Wan, K., Hajat, S. & Macintyre, H. L. Accounting for adaptation when projecting climate change impacts on health: a review of temperature-related health impacts. Environ. Int.188, 108761 (2024).
Wu, Y. et al. Temperature frequency and mortality: assessing adaptation to local temperature. Environ. Int.187, 108691 (2024).
Acknowledgements
This work was supported by the National Key R&D Program of China (2022YFF1203001), and National Natural Science Foundation of China (72474010).
Author information
Authors and Affiliations
Contributions
Pengfei Li: Conceptualization, Formal analysis, Writing original draft, Writing – review & editing, Supervision, Funding acquisition. Jingyi Wu: Formal analysis, Writing original draft, Writing – review & editing. Tao Xue: Conceptualization, Writing – review & editing, Supervision. Tong Zhu: Writing – review & editing. All authors have directly accessed and verified the underlying data reported in the manuscript. All authors confirm that they have full access to all the data in the study and accept responsibility to submit for publication.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Peer review
Peer review information
Communications Medicine thanks Francesco Sera and Michael Tong for their contribution to the peer review of this work.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Li, P., Wu, J., Xue, T. et al. Associations between monthly temperature anomalies and mortality among children younger than five years in low- and middle-income countries. Commun Med 5, 365 (2025). https://doi.org/10.1038/s43856-025-01101-4
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s43856-025-01101-4
