
Abstract
Objective:
To investigate the effects of three weight loss interventions on cardiometabolic risk factors, including blood pressure, lipids, glucose and markers of insulin resistance and inflammation. We also examined whether categories of incremental weight change conferred greater improvements on these parameters.
Methods:
This 2-year trial was conducted in a primary care setting and included 390 obese participants who were randomly assigned to one of three interventions: (1) Usual Care (quarterly primary care provider (PCP) visits that included education about weight management); (2) Brief Lifestyle Counseling (quarterly PCP visits plus monthly behavioral counseling provided by a trained auxiliary health-care provider); or (3) Enhanced Brief Lifestyle Counseling (the same care as described for the previous intervention, plus weight loss medications or meal replacements). The primary outcome was change in cardiometabolic risk factors among groups.
Results:
At month 24, participants in Enhanced Brief Lifestyle Counseling lost significantly more weight than those in Usual Care (4.6 vs 1.7 kg), with no other significant differences between groups. Enhanced Brief Lifestyle Counseling produced significantly greater improvements in high-density lipoprotein (HDL) cholesterol and triglyceride levels at one or more assessments, compared with the other two interventions. Markers of insulin resistance also improved significantly more in this group throughout the 2 years. Collapsing across the three groups, greater weight loss was associated with greater improvements in triglycerides, HDL cholesterol and markers of insulin resistance and inflammation at month 24, but was not significantly associated with reductions in blood pressure, total cholesterol and low-density lipoprotein cholesterol at any time.
Conclusions:
Enhanced Brief Lifestyle Counseling, which produced the largest weight loss, was generally associated with the greatest improvements in cardiovascular risk factors. These findings suggest that an intensive weight loss intervention, delivered in a primary care setting, can help obese individuals improve some cardiometabolic risk factors.
Similar content being viewed by others


Introduction
Weight loss has been found to ameliorate several modifiable cardiovascular disease (CVD) risk factors. It is associated with: reductions in blood pressure; improved glycemic control; decreased total cholesterol, low-density lipoprotein (LDL) cholesterol and triglycerides; and increased high-density lipoprotein (HDL) cholesterol.1, 2, 3 Greater weight loss typically confers larger improvements in cardiometabolic risk factors,3 but even modest weight loss of 5–10% has been shown to produce beneficial effects.3, 4, 5
Numerous studies have demonstrated the efficacy of behavioral interventions to promote weight loss and improve health outcomes in overweight and obese adults.3, 4, 5, 6, 7 However, few trials have been conducted in routine clinical settings.8, 9, 10, 11 To address this need, the National Heart, Lung and Blood Institute (NHLBI) recently supported three independent studies to evaluate the effectiveness of weight loss interventions delivered in primary care settings. The three participating institutions formed a collaborative research group to undertake the Practice-based Opportunities for Weight Reduction (POWER) trials.12 The three individual studies included POWER-UP (University of Pennsylvania), POWER Hopkins (Johns Hopkins) and Be Fit, Be Well (Harvard University/Washington University).12 Common components were used in all three studies to standardize comparisons, but each site implemented its own behavioral intervention.13, 14, 15
The POWER-UP trial provided opportunity to examine the effects of modest weight loss on cardiometabolic risk factors in obese individuals with increased risk for CVD. This 2-year trial included obese men and women who were randomly assigned to a usual care condition or one of two lifestyle interventions of varying intensity (described below). POWER-UP’s methods and main results have been published previously.13 This paper expands upon our previous report of the effects of the three interventions on traditional cardiometabolic risk factors.13 We hypothesized that both lifestyle interventions would result in greater improvements in blood pressure, lipids, glucose and markers of insulin resistance and inflammation than the usual care intervention. We also examined whether greater weight change would confer greater improvements in these parameters.
Materials and methods
Participants
Three hundred and ninety obese adults were recruited from six primary care practices in the University of Pennsylvania Health System to participate in the POWER-UP trial. Eligible participants were aged 21 years and older, had a body mass index of 30–50 kg m−2, an elevated waist circumference (⩾ 102 cm for men; ⩾ 88 cm for women) and at least one other criterion for the metabolic syndrome.16 Main exclusion criteria included having: uncontrolled blood pressure; recent cardiovascular events; weight change ⩾ 5% over the preceding 6 months; active participation in a weight loss program; prior or planned use of bariatric surgery; serious co-morbid conditions (for example, severe psychiatric illness, end-stage renal disease); use of medications known to cause significant (⩾ 5%) long-term changes in weight; or pregnancy. The study was approved by the Institutional Review Board at the University of Pennsylvania, and all participants provided written informed consent.
Interventions
Eligible participants were randomly assigned to one of three interventions, as reported in detail in the main outcomes paper.13 Interventions included: (1) Usual Care, in which participants met quarterly with their primary care provider (PCP) and received approximately 5–7 min of education about weight management; (2) Brief Lifestyle Counseling (Brief LC), which included the quarterly PCP visit and 10–15 min of monthly behavioral counseling delivered by an auxiliary health-care provider (typically a medical assistant) who was trained as a lifestyle coach; and (3) Enhanced Brief Lifestyle Counseling (Enhanced Brief LC), in which pharmacologic therapy (sibutramine or orlistat) or meal replacements were added to the same quarterly PCP visit and behavioral intervention to further enhance weight loss. (Participants who were initially taking sibutramine were switched to orlistat or meal replacements after this medication was withdrawn from the US market in October 2010 amid concerns of increased risk of CVD events. This option was also offered in November 2009 after the Food and Drug Administration issued an alert concerning the safety of sibutramine.)
All participants were prescribed the same diet and physical activity goals but were provided different amounts of behavioral support to reach them. Participants who weighed <113.6 kg were prescribed a balanced diet of 1200–1500 kcal d−1 (1500–1800 kcal d−1 for participants who weighed ⩾113.6 kg), which consisted of approximately 15–20% kcal from protein, 20–35% kcal from fat and the remainder from carbohydrate. All participants were instructed to gradually increase their physical activity to 180 min per week and were given a pedometer, a calorie-counting book17 and handouts from NHLBI’s Aim for a Healthy Weight.18
Outcomes and measurements
The primary outcome was the change in cardiometabolic risk factors including blood pressure, lipids, fasting glucose, markers of insulin resistance and high-sensitivity C-reactive protein (hs-CRP). As a secondary outcome, we quantified the change in cardiometabolic risk factors associated with increasing categories of weight change.
Measurements were obtained in a standardized manner by trained, certified staff members at baseline and months 6, 12 and 24.13, 19 Weight was measured on a calibrated scale (Tanita BWB-800), and height was measured using a wall-mounted stadiometer. Lipids, glucose, insulin and hs-CRP were measured following a 9-h overnight fast by standardized methods described previously.19, 20 All laboratory assays were performed at the William Pepper Laboratory of Clinical Medicine at the Hospital of the University of Pennsylvania. Insulin resistance was estimated using the homeostasis model assessment (HOMA-IR index) formula ([fasting insulin (μU ml−1) × fasting glucose (mmol l−1)]/22.5), with greater insulin resistance indicated by higher HOMA-IR values.21 Demographic data, including gender, age, race/ethnicity, educational level and income level, were collected by a self-report questionnaire at baseline.
Statistical analysis
The distributions of baseline characteristics were examined for each intervention group. Continuous variables were reported as means (s.d.) when normally distributed or as medians (interquartile range) when the distribution was not normal. Categorical variables were reported as frequencies.
Changes in cardiometabolic outcomes at 12 and 24 months in the intention-to-treat (ITT) population were compared with the use of repeated-measures, linear mixed-effects models (for continuous outcomes) and generalized estimating equation models (for categorical outcomes), which controlled for age, sex, race or ethnic group, and study site. Separate mixed-effects models were fit for each outcome. Main effects of treatment group and time, as well as the treatment group × time interaction effect, were examined in the mixed-effects models using the unstructured covariance structure.
We also examined the relationships between categories of weight change and change in cardiometabolic risk factors. Participants were divided into the following categories based on their weight change from baseline to months 12 and 24: (1) gained weight or remained at baseline weight; (2) weight loss <5%; (3) weight loss ⩾5 to <10%; and (4) weight loss ⩾10%. Participants from all three interventions were pooled for this analysis, with adjustment for treatment condition, gender, race and age. Separate linear regression models were fit for weight and the cardiometabolic variables.
Results
Baseline characteristics
The baseline characteristics of participants in each intervention group were similar and have been described in detail.13 As shown in Table 1, participants were predominantly non-Hispanic, white women and had a mean (±s.d.) age of 51.5 (11.5) years, body weight of 107.7 (18.3) kg and body mass index of 38.5 (4.7) kg m−2. Participants in the Usual Care group were significantly heavier and had a greater waist circumference than those in the Enhanced Brief LC group (P<0.05) but did not differ significantly from those in the Brief LC group. Fasting glucose levels were also significantly higher in the Usual Care group, relative to Enhanced Brief LC (P<0.05). Two hundred and eighty-six (73.3%) participants provided complete cardiometabolic data at month 24.
Weight loss
As previously reported,13 mean (±SE) weight losses at month 12 were 2.3 (0.6), 3.4 (0.6) and 7.1 (0.6) kg for the Usual Care, Brief LC and Enhanced Brief LC groups, respectively. Weight loss differed significantly between Enhanced Brief LC and Usual Care at this time (shown in Table 2), as well as between the two lifestyle groups. By month 24, weight regain occurred in all groups, although weight loss remained significantly greater in Enhanced Brief LC than in Usual Care (P<0.05).
Weight change at months 12 and 24 was reanalyzed in the Enhanced Brief LC group after excluding the 44 participants who received sibutramine at any time (data not shown). As reported in the main outcomes paper,13 weight loss was very similar in this group at both time points in both the full ITT and modified ITT populations.
Changes in cardiometabolic risk factors
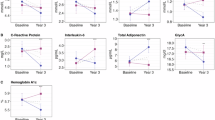
Participants in Enhanced Brief LC achieved the greatest improvements in glycemic parameters (shown in Table 2). Both fasting insulin levels and HOMA-IR declined significantly more at months 12 and 24 in these participants than in the two other conditions, indicating improved insulin resistance. Fasting glucose also declined significantly more in Enhanced Brief LC at month 12, compared with Usual Care, but this benefit was not sustained at month 24. Participants who received Enhanced Brief LC also had significantly greater improvements in HDL cholesterol and triglyceride levels at one or more assessments compared with the other two groups. Substantial reductions in triglycerides (⩾ 0.2 mmol l−1) were observed in all groups over time, but they did not differ significantly between groups at month 24. LDL cholesterol and other markers of atherogenic particles (that is, non-HDL cholesterol) declined modestly (approximately 0.1–0.4 mmol l−1) in all groups at some periods. Blood pressure was essentially unchanged from baseline values in all groups.
Changes in traditional cardiometabolic risk factors (blood pressure, lipids and glucose) also were analyzed in the modified ITT population that excluded participants who had used sibutramine. These findings (also reported in the main outcomes paper) were very similar to those for the entire Enhanced Brief LC group.13 As the magnitude of weight loss was comparable in the Enhanced Brief LC group, with and without participants who used sibutramine, we did not perform additional analyses on markers of atherogenic particles, insulin resistance or inflammation.
Relationship of changes in weight and cardiometabolic risk factors
As shown in Table 3, participants were divided into four categories of weight change to further quantify the associations between incremental percent weight change and improvements in cardiometabolic risk factors. Greater improvements in triglycerides, HDL cholesterol and hs-CRP were observed with increasing categories of weight loss. Insulin resistance, as indicated by HOMA-IR, also improved with greater weight loss. In contrast, the magnitude of improvement in blood pressure, total cholesterol and LDL cholesterol did not significantly differ across categories of weight change. Glucose transiently improved in one of the higher categories of weight loss at month 12, but this effect was not sustained, and there were no differences among groups at month 24. Incremental weight loss had minimal effect on either systolic or diastolic blood pressure.
Discussion
The principal finding of this study was that lifestyle interventions delivered in primary care settings helped patients achieve modest weight losses that were associated with improvements in cardiometabolic risk factors. Enhanced Brief LC, in which meal replacements or weight loss medications were used in conjunction with quarterly PCP visits and monthly brief lifestyle coaching, conferred the largest weight losses and generally the greatest improvements in cardiometabolic risk factors. The largest improvements were seen in markers of insulin resistance, as indicated by reduced fasting insulin levels and decrements in HOMA-IR. These benefits were sustained throughout the duration of the study. Significant changes also were observed in HDL cholesterol over time in the Enhanced Brief LC group.
All three interventions produced modest reductions in total and LDL cholesterol, triglycerides and hs-CRP at one or more times during the trial. Net beneficial effects on lipids and inflammatory markers generally were maintained, despite some weight regain in all groups. In contrast, systolic and diastolic blood pressures were essentially unchanged in all groups.
Our findings of modest reductions in lipid parameters and minimal changes in blood pressure are similar to those reported in the POWER Hopkins study, in which obese participants with at least one cardiovascular risk factor were randomly assigned to a self-directed control group or to one of two behavioral interventions. Weight-loss counseling was provided remotely (via phone, email or web-based applications) or in-person, using group and individual sessions.14 Weight loss at month 24 in the two intervention groups (−4.6 and −5.1 kg, respectively) was similar to that observed in our Enhanced Brief LC participants. We note that baseline values for blood pressure and lipids were near normal in POWER-UP and POWER Hopkins, thus, limiting the capacity to assess the potential benefits of weight loss on these outcomes.
To better describe the associations between weight change and improvements in cardiometabolic risk factors, we also examined the effects of incremental categories of weight loss, irrespective of the treatment condition. Although it is generally accepted that weight loss ⩾5% in obese individuals induces favorable changes in numerous CVD risk factors,1, 2, 3, 4, 5 we observed smaller changes in several metabolic parameters than others have previously described.3 In the Look AHEAD (Action for Health in Diabetes) study, weight loss of 5 to <10% (compared with ⩽2%) was associated with increased odds of achieving clinically significant improvements in systolic and diastolic blood pressure, HbA1c, glucose, triglycerides, LDL cholesterol and HDL cholesterol.3 Larger weight losses (⩾10%) were associated with greater benefits in all of these parameters, with the exception of LDL cholesterol. In contrast, we did not observe significant improvements in blood pressure, total cholesterol, LDL cholesterol and fasting glucose with greater weight loss (that is, ⩾5 and ⩾10%, compared with <5%) in the present study. Total and LDL cholesterol levels tended to improve with weight loss, but there were inconsistencies across graduated categories of weight change (the lack of a dose–response relationship may have been attributable to the differential use of cholesterol medications in the four weight loss categories, but we were not able to confirm this hypothesis). The Look AHEAD study included over 5100 participants and was better powered to detect differences in cardiometabolic risk among categories of weight change. Moreover, as noted previously, POWER-UP participants had near-normal baseline values for many of the cardiometabolic variables examined.
Strengths of the present study include its diverse population, which is generally representative of primary care practices across the country and potentially makes our results generalizable to the broad population. The study also had a very high rate of adherence and follow-up over its 2-year duration, suggesting that it is possible to engage patients in behavioral weight loss programs delivered in primary care practice. Our investigation also had limitations, principally that it was not powered to detect significant differences between groups in cardiometabolic risk factors (The study was powered on differences in weight loss). Thus, our nonsignificant relationships between weight loss and improvements in blood pressure, glucose and lipids should be interpreted with caution.
Despite these limitations, clinically meaningful improvements were observed in the present study in measures of insulin resistance, triglycerides, HDL cholesterol and hs-CRP. These results reaffirm the important benefits of providing lifestyle counseling to appropriate patients to induce weight loss. The Enhanced Brief LC approach, developed in POWER-UP, provides a potentially valuable means of achieving clinically significant weight loss (⩾5%) in primary care practice.
References
Goldstein DJ . Beneficial health effects of modest weight loss. Int J Obes Relat Metab Disord 1992; 16: 397–415.
Van Gaal LF, Mertens IL, Ballaux D . What is the relationship between risk factor reduction and degree of weight loss? Eur Heart J Suppl 2005; 7: L21–L26.
Wing RR, Lang W, Wadden TA, Safford M, Knowler WC, Bertoni AG et al. Benefits of modest weight loss in improving cardiovascular risk factors in overweight and obese individuals with type 2 diabetes. Diabetes Care 2011; 34: 1481–1486.
Knowler WC, Barrett-Connor E, Fowler SE, Hamman RF, Lachin JM, Walker EA et al. Reduction in the incidence of type 2 diabetes with lifestyle intervention or metformin. N Engl J Med 2002; 346: 393–403.
Appel LJ, Champagne CM, Harsha HW, Cooper LS, Obarzanek E, Elmer PJ et al. Effects of comprehensive lifestyle modification on blood pressure control: main results of the PREMIER clinical trial. JAMA 2003; 289: 2083–2093.
Svetkey LP, Stevens VJ, Brantley PJ, Appel LJ, Hollis JF, Loria CM et al. Comparison of strategies for sustaining weight loss: the weight loss maintenance randomized controlled trial. JAMA 2008; 299: 1139–1148.
Tate DF, Jackvony EH, Wing RR . Effects of internet behavioral counseling on weight loss in adults at risk for type 2 diabetes: a randomized trial. JAMA 2003; 289: 1833–1836.
Tsai AG, Wadden TA, Rogers MA, Day SC, Moore RH, Islam BJ . A primary care intervention for weight loss: results of a randomized controlled study. Obesity 2010; 18: 1614–1618.
Ockene IS, Hebert JR, Ockene JK, Saperia GM, Stanek E, Nicolosi R et al. Effect of a physician-delivered nutrition counseling training and an office-support program on saturated fat intake, weight, and serum lipid measurements in a hyperlipidemic population: Worcester Area Trial for Counseling in Hyperlipidemia (WATCH). Arch Intern Med 1999; 159: 725–731.
Martin PD, Dutton GR, Rhode PC, Horswell RL, Ryan DH, Brantley PJ . Weight loss maintenance following a primary care intervention for low-income minority women. Obesity 2008; 16: 2462–2467.
Ashley JM, St Jeor ST, Schrage JP, Perumean-Chaney SE, Gilbertson MC, McCall NL et al. Weight control in the physician’s office. Arch Intern Med 2001; 161: 1599–1604.
Yeh HC, Clark JM, Emmons KE, Moore RH, Bennett GG, Warner ET et al. Independent but coordinated trials: insights from the Practice-based Opportunities for Weight Reduction Trials Collaborative Research Group. Clin Trials 2010; 7: 322–332.
Wadden TA, Volger S, Sarwer DB, Vetter ML, Tsai AG, Berkowitz RI et al. A two-year randomized trial of obesity treatment in primary care practice. N Engl J Med 2011; 365: 1969–1979.
Appel LJ, Clark JM, Yeh HC, Wang NY, Coughlin JW, Daumit G et al. Comparative effectiveness of weight-loss interventions in clinical practice. N Engl J Med 2011; 365: 1959–1968.
Bennett GG, Warner ET, Glasgow RE, Askew S, Goldman J, Ritzwoller DP et al. Obesity treatment for socioeconomically disadvantaged patients in primary care practice. Arch Intern Med 2012; 172: 565–574.
National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III). Third report of the National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III) Final Report. Circulation 2002; 106: 3143–3421.
Borushek A . The CalorieKing Calorie, Fat and Carbohydrate Counter 8th edn. Family Health: Conta Mesa, CA, USA, 2008.
National Heart, Lung, and Blood Institute. Aim for a Healthy Weight. National Institutes of Health: Bethesda, MD, USA, 2005. NIH publication no. 05-5213.
Wadden TA, Berkowitz RI, Womble LG, Sarwer DB, Phelan S, Cato RK et al. Randomized trial of lifestyle modification and pharmacotherapy for obesity. N Engl J Med 2005; 353: 2111–2120.
Vetter ML, Wadden TA, Vinnard C, Moore RH, Khan Z, Volger S et al. Gender differences in relationship between symptoms of depression and high-sensitivity CRP. Int J Obes 2013; 37: S38–S43.
Matthews DR, Hosker JP, Rudenski AS, Naylor BA, Treacher DF, Turner RC . Homeostasis model assessment: insulin resistance and beta-cell function from fasting plasma glucose and insulin concentrations in man. Diabetologia 1985; 28: 412–419.
Acknowledgements
This research was supported by grants U01-HL087072 from the National Heart, Lung and Blood Institute and K24-DK065018 from the National Institutes of Diabetes and Digestive and Kidney Disease. We thank Amos Odeleye for his assistance with statistical analysis.
This article is published as part of a supplement, sponsored by the Center for Weight and Eating Disorders—University of Pennsylvania.
Author information
Authors and Affiliations
Consortia
Corresponding author
Ethics declarations
Competing interests
TAW serves on the advisory boards of Novo Nordisk and Orexigen Therapeutics, which are developing weight loss medications, as well as of Alere and the Cardiometabolic Support Network, which provide behavioral weight loss programs. TAW has also served as a consultant for Boehringer Ingelheim, and has received grant support from the National Institutes of Health (NIH/NIDDK and NIH/NHLBI). DBS discloses relationships with the following companies: Allergan, BariMD, BaroNova, Enteromedics and Galderma. DBS has also received grant support from the National Institutes of Health (NIH). The remaining authors declare no conflict of interest.
Appendix
Appendix
POWER-UP Research Group: Investigators and Research Coordinators
Academic investigators at the Perelman School of Medicine at the University of Pennsylvania were Thomas A Wadden, PhD (principal investigator), David B Sarwer, PhD (co-principal investigator), Robert I Berkowitz, MD, Jesse Chittams, MS, Lisa Diewald, MS, RD, Shiriki Kumanyika, PhD, Renee Moore, PhD, Kathryn Schmitz, PhD, Adam G Tsai, MD, MSCE, Marion Vetter, MD, RD and Sheri Volger, MS, RD.
Research coordinators at the University of Pennsylvania were Caroline H Moran, BA, Jeffrey Derbas, BS, Megan Dougherty, BS, Zahra Khan, BA, Jeffrey Lavenberg, MA, Eva Panigrahi, MA, Joanna Evans, BA, Ilana Schriftman, BA, Dana Tioxon, Victoria Webb, BA and Catherine Williams-Smith, BS.
POWER-UP Research Group: Participating Sites and Clinical Investigators
PennCare–Bala Cynwyd Medical Associates: Ronald Barg, MD, Nelima Kute, MD, David Lush, MD, Celeste Mruk, MD, Charles Orellana, MD and Gail Rudnitsky, MD (primary care providers); Angela Monroe (lifestyle coach); Lisa Anderson (practice administrator).
PennCare—Internal Medicine Associates of Delaware County: David E Eberly, MD, Albert H Fink Jr, MD, Kathleen Malone, CRNP, Peter B Nonack, MD, Daniel Soffer, MD, John N Thurman, MD and Marc J Wertheimer, MD (primary care providers); Barbara Jean Shovlin, Lanisha Johnson (lifestyle coaches); Jill Esrey (practice administrator).
PennCare—Internal Medicine Mayfair: Jeffrey Heit, MD, Barbara C Joebstl, MD and Oana Vlad, MD (primary care providers); Rose Schneider, Tammi Brandley (lifestyle coaches); Linda Jelinski (practice administrator).
Penn Presbyterian Medical Associates: Joel Griska, MD, Karen J Nichols, MD, Edward G Reis, MD, James W Shepard, MD and Doris Davis-Whitely, PA (primary care providers); Dana Tioxon (lifestyle coach); Charin Sturgis (practice administrator).
PennCare—University City Family Medicine: Katherine Fleming, CRNP, Dana B Greenblatt, MD, Lisa Schaffer, DO, Tamara Welch, MD and Melissa Rosato, MD (primary care providers); Eugonda Butts, Marta Ortiz, Marysa Nieves and Alethea White (lifestyle coach); Cassandra Bullard (practice administrator).
PennCare–West Chester Family Practice: Jennifer DiMedio, CRNP, Melanie Ice, DO, Brandt Loev, DO, John S Potts, DO and Christine Tressel, DO (primary care providers); Iris Perez, Penny Rancy and Dianne Rittenhouse (lifestyle coaches); Joanne Colligan (practice administrator).
Rights and permissions
About this article
Cite this article
Vetter, M., Wadden, T., Chittams, J. et al. Effect of lifestyle intervention on cardiometabolic risk factors: results of the POWER-UP trial. Int J Obes 37 (Suppl 1), S19–S24 (2013). https://doi.org/10.1038/ijo.2013.92
Published:
Issue date:
DOI: https://doi.org/10.1038/ijo.2013.92
Keywords
This article is cited by
-
Maternal BMI changes from the prepregnancy to postpartum period are associated with postpartum cardiometabolic risk factors: a longitudinal study
Archives of Gynecology and Obstetrics (2023)
-
Long-term effects (> 24 months) of multiple lifestyle intervention on major cardiovascular risk factors among high-risk subjects: a meta-analysis
BMC Cardiovascular Disorders (2021)
-
Effectiveness of a community-based intervention for weight loss on cardiometabolic risk factors among overweight and obese women in a low socio-economic urban community: findings of the MyBFF@home
BMC Women's Health (2018)
-
Effects of Different Weight Loss Approaches on CVD Risk
Current Atherosclerosis Reports (2018)
-
Associations between weight change and biomarkers of cardiometabolic risk in South Asians: secondary analyses of the PODOSA trial
International Journal of Obesity (2016)
