
Abstract
Background:
Prostate cancer (PCa) is characterized by high tumor heterogeneity. In 2005, the fusion between the androgen-regulated gene TMPRSS2 and members of the ETS family was discovered in prostate cancer. In particular, fusion of TMPRSS2 with ERG was found in approximately 50% of prostate cancers and considered as an early event in the onset of the disease. The prognostic value of this fusion is still contradictory. Bioinformatics showed that overexpression of SPINK1 gene in a subset of fusion-gene-negative prostate cancers was associated with a poor prognosis. In theory, overexpression of the tumor-associated trypsin inhibitor (TATI) protein encoded by SPINK1 in fusion-gene-negative tumor cells opens the way to selected treatments for genotypically different cases. However, their expression has never been assessed at the cellular level in the same tissue samples.
Methods:
As ERG expression has been shown to be a surrogate of fusion gene occurrence in prostate cancer, we have used double immunohistochemical staining to assess expression of ERG and TATI on a large tissue microarray comprising 4177 cases of localized prostate cancer.
Results:
We did not detect any co-expression of ERG and TATI in the same cancer cells, which confirms previous suggestions from in silico studies. ERG was associated with Gleason score (GS), surgical margins and pathological stage, but had no prognostic value in this cohort. TATI was weakly associated with pathological stage but had no significant association with outcome.
Conclusions:
We here provide a morphological basis for ERG and TATI exclusivity in prostate cancer cells. Future therapies should be based on a combination of different targets in order to eradicate tumor cells with gene fusions and cells expressing other tumor-associated antigens. Further studies are needed to understand why ERG and TATI are not co-expressed in the same prostatic tumor cells.
Similar content being viewed by others


Introduction
Prostate cancer (PCa) is the second most frequently diagnosed cancer, the sixth cause of cancer death in males worldwide and the most common cancer in developed countries.1 At the time of diagnosis, PCa is often multifocal and highly heterogeneous, leading to difficulty in accurately determining the prognosis and the most appropriate form of therapy.2 The disease development can range from slow-growing and localized tumors to rapidly growing and highly metastatic tumors. As a result, there is a need to find biomarkers that can identify aggressive forms of the disease. Thus far, this approach has not produced any widely used clinical tests to accurately predict the progression of the disease; however, many studies have cast light on its biological features.3, 4, 5
PCa, like many other malignancies, is characterized by mutations in genes that promote (oncogenes) or protect against cancer (tumor suppressors). These genetic abnormalities include point mutations and chromosomal aberrations (gain, losses, rearrangements).6 In 2005, TMPRSS2:ETS family gene fusions were discovered in PCa.7 By using cancer outlier profile analysis, members of the ETS family were found to be overexpressed in a subset of PCa types, with ERG being the most common fusion partner. This fusion seems to occur in approximately 50% of PCas8 and since TMPRSS2 is an androgen-regulated gene, this leads to androgen-regulated overexpression of the oncoprotein ERG. It seems to be an early event in the onset of PCa, but results from various studies on its prognostic value are contradicting. Rajput et al.9 found that the ERG fusion gene was more frequent in moderately to poorly differentiated PCas than in well-differentiated tumors. Perner et al.10 found a significant association between TMPRSS2:ERG fusions via deletion and higher tumor stage as well as the presence of metastatic disease involving pelvic lymph nodes. Additionally, Fine et al.11 described an association between the TMPRSS2-ERG gene fusion and low Gleason score. However, others have reported no association with outcome in patients treated by prostatectomy,12 or no association with other clinicopathological parameters.13
Among patients not harboring ETS rearrangements, Tomlins et al.,14 using the cancer outlier profile analysis bioinformatics method, identified SPINK1 as an outlier highly expressed in a subset of cases. Furthermore, this subset of high SPINK1-expressing tumors was associated with an increased risk for biochemical recurrence. Subsequent studies have also investigated the association of tumor-associated trypsin inhibitor (TATI, protein corresponding to the SPINK1 gene) with clinicopathological variables. Leinonen et al.15 showed that in a cohort of patients primarily treated with endocrine therapy, TATI-positive cases had shorter progression-free survival, with TATI falling out as an independent prognostic factor. No association with other clinicopathological variables was observed. The possibility of TATI-positive tumors being selectively targeted by antibodies for therapeutic purposes was demonstrated in an in vitro study showing decreased proliferation, invasion and intravasation16 upon TATI inhibition. The relationship of TATI with other potential biomarkers has also been investigated in castration-resistant PCa. Using consecutive tissue sections and different staining techniques (fluorescence in situ hybridization and traditional immunohistochemistry, IHC),17 it was reported that overexpression of TATI occurred in PTEN-deleted tumors, none of which showed androgen receptor amplification.
Based on bioinformatic analyses, it was suggested that SPINK1 and TMPRSS2:ERG expression were mutually exclusive in prostatic tumors.14 However, to our knowledge, no studies have yet compared the protein expression of TATI and ERG in the same tissue sections. It has recently been shown that ERG staining is highly sensitive and specific as a surrogate marker for TMPRSS2:ERG gene fusion.18, 19 Therefore, co-occurrence of TATI expression and TMPRSS2:ERG gene fusion can now be analyzed at the protein level, as conventional IHC can be used instead of fluorescence in situ hybridization to evaluate fusion gene status on tissue sections.
The aim of our study was to investigate for possibly the first time the expression of TATI and ERG in the same tissue sections by using IHC with double staining in order to determine if they are in fact expressed in different cell populations. This would further support the clinical attempts to selectively treat patients with genotypically different PCa. We have used a large tissue microarray (TMA) consisting of 4177 samples from clinically localized PCa patients who underwent radical prostatectomy.
Materials and methods
Patients
Tissue specimens from primary prostatic tumors were collected from 4177 patients who underwent open radical prostatectomy at the Department of Urology, University Medical Center Hamburg-Eppendorf between 1992 and 2005. Clinicopathological features included pre-operative PSA level, pathological stage (pT) as defined by the American Joint Committee on Cancer in 2002, pathological Gleason score (GS), lymph node involvement (N), surgical margins status (SMS), and, if available, also time to occurrence of metastasis (Table 1). Biochemical recurrence was defined as an increase of postoperative PSA to 0.2 ng ml−1 with a confirmatory value. In total, 913 patients showed BCR with an average time from operation to recurrence of 65.8 months (range 1–219 months).
None of the patients had received neoadjuvant or adjuvant therapy before the prostatectomy and additional therapy was initiated in patients with BCR.
TMAs and IHC
The TMA was constructed as previously described.20 Cones with 0.6 mm diameter were punched out from the area with largest tumor volume and/or worst GS and arranged in nine paraffin blocks. Several consecutive 4-μm-thick sections were arranged on microscope slides. One section from each block was stained with hematoxylin and eosin and another one was processed for IHC using a double-staining procedure for specific demonstration of immunoreactive ERG and TATI. The sections were then stained in a DAKO Autostainer-plus using the EnVision FLEX including Peroxidase-Blocking Reagent (DAKO, Glostrup, Denmark) with a previously characterized TATI monoclonal antibody (6E8 raised in mouse21) at a final concentration of 3 μg ml−1 and a monoclonal antibody specific for ERG (EPR3864 raised in rabbit, Novus Biologicals, Littleton, CO, USA), diluted 1:250 according to the manufacturer. Sections were deparaffinized and pre-treated in the DAKO PT-link module using a standard protocol and buffer supplied by the manufacturer (DAKO).
Detection of ERG immunostaining in endothelial cells and macrophages served as positive control. The intensity of ERG and TATI staining in tumor areas was given a score from 0 to 3 and the percentage of immunostained cancer cells was recorded. Scoring was made by two independent observers (GL and AB) and discordant cases were re-evaluated using an open discussion procedure.
Statistical analysis
Statistical analysis was performed using SPSS (v.20, IBM, Chicago, IL, USA). Kaplan–Meier and log-rank test were used to evaluate the relationship between protein expression and BCR or metastatic disease. Crosstabs were used to show the relationship between protein expression and clinicopathological characteristics, and χ2 test or the Fisher’s exact test was used to assess the significance of differences.
Results
Immunostaining for ERG and TATI
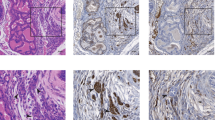
The initial number of patients included was 4177 and the design of the experiment was set to have one core from each patient. Ninety-nine cores were considered benign and 693 were damaged or missing and therefore excluded from analysis. ERG was found to be expressed in 41.7% of the cancer cases (1411/3385), with intensity scores of +1 in 13.9%, +2 in 20.4% and +3 in 7.4%. Staining was found in the nuclei of cancer cells (Figure 1) and in some areas of prostatic intraepithelial neoplasia (PIN). As expected, endothelial cells and macrophages also stained positive for ERG in both benign and malignant areas. We did not observe expression of ERG in any of the benign epithelial structures. Expression of TATI in tumor cells was observed in 5.2% of the cores (175/3385) with the following distribution: +1 in 2.2%, +2 in 1.9% and +3 in 1.0%. As previously demonstrated,22 TATI protein was exclusively localized in the cytoplasm of epithelial cells (Figure 1). A very weak immunostaining for TATI was often found in the cytoplasm of benign luminal epithelial cells.

Immunohistochemical doublestaining for ERG and tumor-associated trypsin inhibitor (TATI). The upper panel shows a core representing a case of prostate cancer positive only for TATI (red staining). TATI is expressed in the cytoplasm of tumor cells. The lower panel shows a core with tumor cells with a cribriform growth pattern and exclusively positive for ERG, which is expressed in the nuclei of the tumor cells.
Interestingly, we identified areas showing transition from benign to PIN and malignant epithelium with ERG expression as the markers of transition (Figure 2). TATI was not found to be overexpressed in any of these areas. Representative immunostainings for ERG and TATI is shown in Figure 1.

Immunohistochemical doublestaining for ERG and tumor-associated trypsin inhibitor (TATI). TATI is not expressed in this case. Only ERG is present in the nuclei of epithelial cells. In the red square, two glandular structures show expression only in some of the cells. This might represent a case of transition towards a malignant lesion.
Associations between ERG and TATI expression and clinicopathological characteristics
Associations of ERG and TATI with preoperative PSA, pathological GS, pT stage, SMS and N-stage were investigated. ERG intensity, dichotomized as negative and positive expression, was not significantly associated with PSA or N stage (χ2 test, P=0.078 and P=0.792, respectively), but there was a significant association with SMS (P=0.004), GS (P<0.0001) and pT stage (P<0.0001), although there was no linear trend. ERG was significantly more often expressed in tumors with GS 3+4 and pT3 stages than in the other subgroups (Table 2). When TATI was tested as a dichotomized variable (positive vs negative) for association with clinicopathological characteristics, TATI turned out to be weakly associated with pT stage (P=0.0496) without a clear linear pattern. However, TATI positivity was not associated with other characteristics (PSA P=0.119, Gleason P=0.948, lymph node P=0.205, surgical margins P=0.769, Table 3).
Association of TATI with ERG is presented in a crosstab format (Table 4). TATI was expressed exclusively in ERG-negative cases.
Expression of ERG and TATI to predict the outcome after radical prostatectomy
We also investigated if expression of ERG or TATI could predict BCR or metastatic events. Kaplan–Meier curves were built on dichotomization where expression of ERG and TATI was either positive or negative. Neither ERG nor TATI predicted BCR (log rank (Mantel–Cox), P=0.689 and P=0.447, respectively, Figure 3) or development of metastatic disease (log rank (Mantel–Cox), P=0.681 and P=0.530, respectively Figure 4). In a univariate Cox regression model, ERG and TATI intensity as a continuous or as a dichotomized variable was not a significant predictor of BCR or of metastatic disease.

Kaplan–Meier curve representing biochemical recurrence (BCR) for patients stratified according to ERG (upper panel) and tumor-associated trypsin inhibitor (TATI) (lower panel) expression. Neither ERG (log rank (Mantel–Cox), P=0.689) nor TATI (log rank (Mantel–Cox), P=0.447) turns out to be a significant predictor of BCR.

Kaplan–Meier curve representing metastatic onset for patients stratified according to ERG (upper panel) and tumor-associated trypsin inhibitor (TATI) (lower panel) expression. Neither ERG (log rank (Mantel–Cox), P=0.681) nor TATI (log rank (Mantel–Cox), P=0.530) turns out to be a significant predictor of metastatic event.
Discussion
Previous studies18, 19, 23 have shown that ERG expression analyzed by IHC is strongly correlated with ERG gene fusion as detected by fluorescence in situ hybridization analysis. Here we applied IHC of ERG on a high-density TMA (n=4177) in order to explore a previously generated hypothesis that TMPRSS2:ERG fusion-positive PCas do not express SPINK1 (TATI protein).14 We successfully performed immunohistochemical double staining for ERG and TATI and demonstrated that these proteins are expressed in a mutually exclusive manner.
The TMA used in our study contains tumor samples obtained from PCa patients who underwent radical prostatectomy at a tertiary referral center (Hamburg) and none of the patients received hormonal treatment prior to surgery. This TMA has proved to be useful for biomarker evaluation and is described in several reports.20, 24, 25 It also extends the TMA used in a previous study by Minner et al.26 The observed expression of ERG (positive in 41.7%) and TATI (positive in 5.7%) is in accordance with results from previous publications, although the frequency is slightly lower. This can be related to the fact that in the TMA used, only one core was available from each patient. If we assume that ERG IHC is a good surrogate marker for TMPRSS2:ERG fusion in PCa, our present results favor the view that the occurrence of this gene fusion in PIN is an early event in tumor development. Our data also confirm the findings reported by Furusato et al.,27 who observed the presence of ERG in PIN and found a strong concordance of ERG-positive foci in PIN with ERG-positive carcinoma. However, our results do not display its usefulness as a prognostic biomarker as previously suggested.26
Our data show that ERG did not predict the course of the disease in radical prostatectomy-treated patients, since it was neither related to BCR nor related to metastatic onset. ERG positivity was significantly associated with pT stage, SMS and GS but not with N stage or with the preoperative PSA value. Even if the expression of ERG was significantly different in the groups with various GSs (⩽6, 3+4, 4+3, ⩾8) and pT stages (pT2, pT3, pT4), there was no clear linear trend. ERG seemed to be more often expressed in tumors with pT3 stage and a Gleason score of 3+4 than in other stages and grades, as previously described.26 As for the association with SMS, it must be interpreted with caution until it has been confirmed in subsequent studies. Of note, our data set is larger than earlier-described ones and seems to exclude the use of ERG staining for stratification of patients for the risk of relapse.
TATI has previously been shown to identify a subgroup with more aggressive cancer. Our data show a significant association (P=0.0496) with pT stage, but the association is weak and it is difficult to draw conclusions. No association was found with BCR or metastatic event.
In silico data from studies on different PCa cohorts have suggested that SPINK1/TATI and TMPRSS2:ERG are expressed in a mutually exclusive manner.14 In this study, we aim to clarify if this pattern of expression is observed at the protein level. Our presented data seem to show that ERG and TATI are expressed in separate tumor cell populations and that further studies are needed to elucidate the underlying tumor biology. Another confirmatory observation is that expression of ERG-positive cells may indicate a transition from benign to PIN or from PIN to malignancy as illustrated in Figure 2.
In conclusion, by using immunohistochemical double staining, we showed that ERG and TATI are exclusively expressed in separate tumor cell populations. However, in this setting, neither ERG nor TATI was a useful predictor of outcome in PCa patients undergoing radical prostatectomy. The results provide a morphological basis for future PCa therapy using a combination of different targets in order to eradicate tumor cells expressing different markers. Further studies are needed to elucidate why ERG and TATI are not co-expressed in the same prostatic tumor cells.
References
Jemal A, Bray F, Center MM, Ferlay J, Ward E, Forman D . Global cancer statistics. CA Cancer J Clin 2011; 61: 69–90.
Arora R, Koch MO, Eble JN, Ulbright TM, Li L, Cheng L . Heterogeneity of Gleason grade in multifocal adenocarcinoma of the prostate. Cancer 2004; 100: 2362–2366.
Shariat SF, Semjonow A, Lilja H, Savage C, Vickers AJ, Bjartell A . Tumor markers in prostate cancer I: blood-based markers. Acta Oncol 2011; 50 (Suppl 1): 61–75.
Bjartell A, Montironi R, Berney DM, Egevad L . Tumour markers in prostate cancer II: diagnostic and prognostic cellular biomarkers. Acta Oncol 2011; 50 (Suppl 1): 76–84.
Roobol MJ, Haese A, Bjartell A . Tumour markers in prostate cancer III: biomarkers in urine. Acta Oncol 2011; 50 (Suppl 1): 85–89.
Mitelman F, Johansson B, Mertens F . The impact of translocations and gene fusions on cancer causation. Nat Rev Cancer 2007; 7: 233–245.
Tomlins SA, Rhodes DR, Perner S, Dhanasekaran SM, Mehra R, Sun XW et al. Recurrent fusion of TMPRSS2 and ETS transcription factor genes in prostate cancer. Science 2005; 310: 644–648.
Mehra R, Tomlins SA, Shen R, Nadeem O, Wang L, Wei JT et al. Comprehensive assessment of TMPRSS2 and ETS family gene aberrations in clinically localized prostate cancer. Mod Pathol 2007; 20: 538–544.
Rajput AB, Miller MA, De Luca A, Boyd N, Leung S, Hurtado-Coll A et al. Frequency of the TMPRSS2:ERG gene fusion is increased in moderate to poorly differentiated prostate cancers. J Clin Pathol 2007; 60: 1238–1243.
Perner S, Demichelis F, Beroukhim R, Schmidt FH, Mosquera JM, Setlur S et al. TMPRSS2:ERG fusion-associated deletions provide insight into the heterogeneity of prostate cancer. Cancer Res 2006; 66: 8337–8341.
Fine SW, Gopalan A, Leversha MA, Al-Ahmadie HA, Tickoo SK, Zhou Q et al. TMPRSS2-ERG gene fusion is associated with low Gleason scores and not with high-grade morphological features. Mod Pathol 2010; 23: 1325–1333.
Gopalan A, Leversha MA, Satagopan JM, Zhou Q, Al-Ahmadie HA, Fine SW et al. TMPRSS2-ERG gene fusion is not associated with outcome in patients treated by prostatectomy. Cancer Res 2009; 69: 1400–1406.
Rubio-Briones J, Fernandez-Serra A, Calatrava A, Garcia-Casado Z, Rubio L, Bonillo MA et al. Clinical implications of TMPRSS2-ERG gene fusion expression in patients with prostate cancer treated with radical prostatectomy. J Urol 2010; 183: 2054–2061.
Tomlins SA, Rhodes DR, Yu J, Varambally S, Mehra R, Perner S et al. The role of SPINK1 in ETS rearrangement-negative prostate cancers. Cancer Cell 2008; 13: 519–528.
Leinonen KA, Tolonen TT, Bracken H, Stenman UH, Tammela TL, Saramaki OR et al. Association of SPINK1 expression and TMPRSS2:ERG fusion with prognosis in endocrine-treated prostate cancer. Clin Cancer Res 2010; 16: 2845–2851.
Ateeq B, Tomlins SA, Laxman B, Asangani IA, Cao Q, Cao X et al. Therapeutic targeting of SPINK1-positive prostate cancer. Sci Transl Med 2011; 3, 72ra17.
Bismar TA, Yoshimoto M, Duan Q, Liu S, Sircar K, Squire JA . Interactions and relationships of PTEN, ERG, SPINK1 and AR in castration-resistant prostate cancer. Histopathology 2012; 60: 645–652.
Park K, Tomlins SA, Mudaliar KM, Chiu YL, Esgueva R, Mehra R et al. Antibody-based detection of ERG rearrangement-positive prostate cancer. Neoplasia 2010; 12: 590–598.
van Leenders GJ, Boormans JL, Vissers CJ, Hoogland AM, Bressers AA, Furusato B et al. Antibody EPR3864 is specific for ERG genomic fusions in prostate cancer: implications for pathological practice. Mod Pathol 2011; 24: 1128–1138.
Fleischmann A, Schlomm T, Huland H, Kollermann J, Simon P, Mirlacher M et al. Distinct subcellular expression patterns of neutral endopeptidase (CD10) in prostate cancer predict diverging clinical courses in surgically treated patients. Clin Cancer Res 2008; 14: 7838–7842.
Osman S, Turpeinen U, Itkonen O, Stenman UH . Optimization of a time-resolved immunofluorometric assay for tumor-associated trypsin inhibitor (TATI) using the streptavidin-biotin system. J Immunol Methods 1993; 161: 97–106.
Paju A, Hotakainen K, Cao Y, Laurila T, Gadaleanu V, Hemminki A et al. Increased expression of tumor-associated trypsin inhibitor, TATI, in prostate cancer and in androgen-independent 22Rv1 cells. Eur Urol 2007; 52: 1670–1679.
Falzarano SM, Zhou M, Carver P, Tsuzuki T, Simmerman K, He H et al. ERG gene rearrangement status in prostate cancer detected by immunohistochemistry. Virchows Arch 2011; 459: 441–447.
Dahlman A, Rexhepaj E, Brennan DJ, Gallagher WM, Gaber A, Lindgren A et al. Evaluation of the prognostic significance of MSMB and CRISP3 in prostate cancer using automated image analysis. Mod Pathol 2011; 24: 708–719.
Erbersdobler A, Isbarn H, Steiner I, Schlomm T, Chun F, Mirlacher M et al. Predictive value of prostate-specific antigen expression in prostate cancer: a tissue microarray study. Urology 2009; 74: 1169–1173.
Minner S, Enodien M, Sirma H, Luebke AM, Krohn A, Mayer PS et al. ERG status is unrelated to PSA recurrence in radically operated prostate cancer in the absence of antihormonal therapy. Clin Cancer Res 2011; 17: 5878–5888.
Furusato B, Tan SH, Young D, Dobi A, Sun C, Mohamed AA et al. ERG oncoprotein expression in prostate cancer: clonal progression of ERG-positive tumor cells and potential for ERG-based stratification. Prostate Cancer Prostatic Dis 13: 228–237.
Acknowledgements
We are grateful to Ms Elise Nilsson (Center for Molecular Pathology, Malmö, Lund University) for the immunohistochemical staining and to Dr Thorsten Schlomm and Pierre Tennstedt at the Martini-Clinic, Prostate Cancer Center, University Medical Center, Hamburg, Germany for kindly providing sections of prostate cancer tissue microarrays and the clinicopathological data set. This work was financially supported by European Union 7 Framework/Marie Curie Initial Training Networks (ITN) PRO-NEST/FP7-PEOPLE Contract no. 238278, and FAST-PATH/FP7-PEOPLE Contract no. 285910, the Swedish Cancer Foundation, the Swedish Research Council, the Lund University/ALF grants, the Malmö University Hospital Research Foundations and the Gunnar Nilsson's Cancer Foundation.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
The authors declare no conflictof interest.
Rights and permissions
This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivs 3.0 Unported License. To view a copy of this license, visit http://creativecommons.org/licenses/by-nc-nd/3.0/
About this article
Cite this article
Lippolis, G., Edsjö, A., Stenman, UH. et al. A high-density tissue microarray from patients with clinically localized prostate cancer reveals ERG and TATI exclusivity in tumor cells. Prostate Cancer Prostatic Dis 16, 145–150 (2013). https://doi.org/10.1038/pcan.2013.7
Received:
Revised:
Accepted:
Published:
Issue date:
DOI: https://doi.org/10.1038/pcan.2013.7
Keywords
This article is cited by
-
Molecular characterization of prostate cancer in Middle Eastern population highlights differences with Western populations with prognostic implication
Journal of Cancer Research and Clinical Oncology (2020)
-
SPINK1 Overexpression in Localized Prostate Cancer: a Rare Event Inversely Associated with ERG Expression and Exclusive of Homozygous PTEN Deletion
Pathology & Oncology Research (2017)
