
Abstract
Objective
Obstructive sleep apnea (OSA) and obesity are highly prevalent comorbid conditions associated with major societal and healthcare burden. Positive airway pressure (PAP) therapy is the first-line treatment for OSA. This study evaluated the association between PAP adherence and healthcare resource utilization (HCRU) and costs in patients with OSA and comorbid obesity.
Methods
This retrospective cohort study utilized de-identified claims data linked with cloud-connected PAP usage to analyze adults with obesity (ICD-10 code of obesity or morbid obesity or indicating BMI ≥ 30 kg/m2) newly diagnosed with OSA who initiated PAP between 2015 and 2021. Patients were categorized based on adherence: adherent (met Medicare criteria for all quarters), intermediate (adherent for at least one quarter), or nonadherent. Primary outcomes included all-cause emergency room (ER) visits and hospitalizations. Healthcare costs, including inpatient, ER, and total costs, were secondary outcomes. Inverse probability of treatment weighting was applied to balance baseline characteristics across adherence groups.
Results
Among 173,691 patients, 35.2% were adherent, 39.1% intermediately adherent, and 25.7% nonadherent. After applying inverse probability of treatment weighting (IPTW), in year 1 post-index, adherent patients had significantly fewer ER visits and hospitalizations (0.55 ± 1.77 and 0.10 ± 0.44) compared to nonadherent patients (0.69 ± 1.78 and 0.14 ± 0.56; P < 0.001), and significantly lower total healthcare costs (11,332 ± 21,160 vs 11,927 ± 20,212; P < 0.001). Similar findings were observed after 2 years of therapy with adherent patients having lower HCRU and costs than nonadherent patients. Patients with intermediate adherence had outcomes between those of adherent and nonadherent groups, suggesting a dose-dependent effect.
Conclusions
Greater adherence to PAP therapy is associated with significantly lower HCRU and costs in patients with OSA and obesity, highlighting the importance of implementing strategies to improve long term PAP adherence, potentially reducing economic and clinical burden.
Similar content being viewed by others
Introduction
Obstructive sleep apnea (OSA) is a common, chronic sleep-related breathing disorder characterized by repeated narrowing and obstruction of the upper airway during sleep, resulting in repeated episodes of decreased or completely halted airflow, intermittent oxygen desaturation, and sleep disruption [1, 2]. In the United States (US), an estimated 163.2 million adults aged 30–69 years have mild to severe OSA and almost 24 million have moderate to severe OSA [3]. Obesity, a major modifiable risk factor for OSA [2, 4], is projected to affect half of US adults by 2030 [5]. Approximately 40% of individuals with obesity also have sleep apnea [6], and results from the Wisconsin Sleep Cohort Study indicate that 41% of OSA in adults, including 58% of moderate-to-severe OSA cases, can be attributed to overweight or obesity [7].
Both OSA and obesity are associated with substantial direct and indirect economic burden, driven by healthcare resource utilization (HCRU). OSA remains highly underdiagnosed and undertreated, with an estimated ~80% of affected individuals lacking a formal diagnosis [8]. Undiagnosed OSA alone cost the US ~$149.6 billion in 2015, driven by workplace and motor vehicle accidents, comorbid disease management, and lost productivity [8]. Similarly, the economic and social cost of obesity in the US rose from $0.976 trillion in 2014 to an estimated $1.389 trillion in 2018 [9]. Adults with obesity in the US compared to those without obesity experience significantly higher annual medical care costs, which significantly increase with the severity of obesity [10]. Obesity-related complications, such as type 2 diabetes (T2D), cardiovascular diseases, and other comorbidities, further elevate healthcare resource utilization and associated costs [11].
Positive airway pressure (PAP) therapy is the first-line treatment for OSA, effectively reducing disease severity, daytime sleepiness, systemic blood pressure, and motor vehicle accidents, while significantly improving health- and sleep-related quality of life [12]. In addition, evidence from a large observational study in France demonstrated that long-term adherence to continuous PAP (CPAP) therapy is associated with lower all-cause mortality. Moreover, a recent meta-analysis confirmed the potential beneficial effects of CPAP on both all-cause and cardiovascular mortality in patients with OSA, highlighting its critical role in OSA management [13, 14].
For individuals with both OSA and overweight or obesity, clinical guidelines recommend PAP therapy in conjunction with weight management interventions [4, 15]. Although comprehensive lifestyle modifications, pharmacological interventions, and bariatric surgery can substantially improve OSA severity and related comorbidities, weight loss alone rarely resolves OSA completely [16, 17] Therefore, many patients will require continued PAP therapy even after weight reduction. Regular clinical reassessment, including repeat sleep studies, is essential to guide ongoing treatment decisions objectively [18].
Previous studies have found an association between adherence to PAP therapy and lower HCRU and costs [19]. In a general OSA population, Sterling et al. found during the first year after the start of PAP therapy, PAP adherence was significantly associated with fewer emergency room visits, all-cause hospitalizations and lower total healthcare costs, with similar results in the second year of PAP use [20]. This beneficial relationship has been observed as well, specifically among patients with OSA and comorbid conditions such as chronic obstructive pulmonary disease (COPD) [21], T2D [22], heart failure [23, 24], atrial fibrillation [25], and depression [26].
Given the substantial clinical and economic burden associated with obesity in OSA patients [27, 28], it is important to understand how PAP adherence affects healthcare outcomes in patients with OSA and comorbid obesity. This study was designed to test the hypothesis that adherence to PAP therapy would predict HCRU and costs among patients with obesity who were newly diagnosed with OSA and initiating PAP therapy in a real-world setting.
Methods
Data source
This was a retrospective cohort study conducted among patients with obesity and newly diagnosed OSA who initiated PAP therapy between January 2015 and May 2021. De-identified payer-sourced medical and pharmacy claims data from over 160 Medicare Advantage, Medicaid, and commercial health plans (Inovalon Insights LLC, Bowie, MD) were linked with objective individual patient PAP usage data collected from cloud-connected devices (AirView™; Resmed, San Diego, CA). The claims data included information about healthcare encounters, prescription fills, diagnosis and procedure codes, and the device data included detailed PAP therapy usage metrics. The databases were linked through a tokenization process and the resulting linked database underwent a third-party expert determination to ensure compliance with the Health Insurance Portability and Accountability Act. The study design was reviewed by an institutional review board (IRB) (Advarra, Ref number Pro0004005) and deemed exempt from further IRB oversight.
Study cohort
The study cohort included adults (aged ≥18 years) with obesity who completed a sleep test and subsequently received an OSA diagnosis within 60 days (International Classification of Diseases, Tenth Revision-Clinical Modification [ICD-10-CM]: G47.33), had PAP device setup (index date) within 1 year following the sleep test, used an AirSense™ 10 or 11 PAP device (Resmed, San Diego, CA), and had medical and pharmacy claims data available for ≥1 year prior to and the full 2 years after the index date. As such, all included subjects had data for the full study period, with no censoring. Obesity was identified by the presence of at least 2 healthcare encounter claims with an ICD-10 diagnosis code of obesity or morbid obesity or an ICD-10 code indicating a BMI value ≥ 30 kg/m2 in the year prior to device setup (Supplementary Table 1).
Patients were excluded if they had evidence of central sleep apnea, nocturnal hypoventilation, pregnancy, or weight reduction surgery/procedures at any time during the study period, or evidence of PAP re-supply in the year prior to the sleep test date. Patients were also excluded if they had end-stage renal disease or dialysis, which are associated with high healthcare resource use and costs [29].
PAP adherence
Adherence to PAP therapy over 2 years was the primary predictor of interest. PAP usage was objectively measured by patients’ PAP device for each night of use over the first 2 years. For reimbursement purposes, the US Centers for Medicare and Medicaid Services (CMS) considers a patient adherent to PAP therapy if the device is used ≥4 h per night on ≥70% of nights during a consecutive 30-day period during the first 90 days of initial use [30]. Three levels of adherence were evaluated in this analysis: (1) adherent patients who met CMS criteria for all 8 consecutive 90-day time frames (quarters) within the first 2 years; (2) intermediately adherent patients who met CMS criteria in at least 1 but no more than 7 quarters; and (3) nonadherent patients who did not meet CMS criteria in any of the 8 quarters.
Outcomes
The HCRU primary outcomes of interest were all-cause hospitalizations, and all-cause emergency room (ER) visits within the first and second years after PAP initiation. Healthcare costs were secondary outcomes and included inpatient hospitalizations, ER visits, and total costs (with and without apnea equipment). Proxy costs for all resource use were provided by Inovalon Insights LLC based on their proprietary Proxy Financials algorithm, which is based on CMS Medicare prospective payment system fee schedules.
Covariates
The following covariates were included to control for baseline differences among adherence groups: (1) demographic characteristics (age, region, sex, payer); (2) comorbid conditions based on ICD-10-CM diagnosis codes observed in the year prior to index (Supplementary Table 1; coronary artery disease, atrial fibrillation, pulmonary hypertension, hypertension, cerebrovascular disease, other arrhythmia, atrial flutter, heart failure, stroke, hyperlipidemia, asthma, chronic obstructive pulmonary disease, pneumonia, psychotic disorders, other mood disorders, depression, anxiety, type 1 and type 2 diabetes, hyperlipidemia, gastroesophageal reflux disease (GERD), cancer, musculoskeletal pain, psoriasis, and osteoarthritis); (3) glucagon-like peptide 1 receptor agonist (GLP-1) medication fills; (4) claim for weight management lifestyle intervention (Supplementary Table 2); and (5) pre-index all-cause hospitalizations and ER visits.
Additionally, wellness visits, flu vaccines, and adherence to beta blocker, statin, and antihypertensive medications were included as proxies to control for a possible healthy user effect [31, 32] For each medication category, among patients who filled ≥1 prescription 181–360 days before starting PAP therapy, the proportion of days covered (PDC) was measured from the medication fill date to the end of the measurement year (PDC score range: 0.0–1.00).
Statistical analyses
Baseline demographic and clinical characteristics and covariates were assessed overall, and across adherence groups using descriptive statistics. A multinomial logistic regression model was run to calculate propensity scores estimating the likelihood of being in each adherence group, based on baseline covariates. Using these scores, inverse probability of treatment weighting (IPTW) was applied to balance adherence groups on baseline covariates to control for measured confounding [33, 34]. The IPTW approach weights the sample so that the distribution of covariates is similar across adherence groups and mirrors the distribution of the overall cohort. Balance between groups was assessed using standardized mean differences (SMD), with a value < 0.1 indicating good balance [34]. To assess the association between adherence level and outcomes, pairwise differences (adherent vs intermediately adherent, adherent vs nonadherent, intermediately adherent vs nonadherent) in the mean number of healthcare visits and mean healthcare costs were assessed using weighted Wilcoxon rank-sum tests. In order to assess robustness of results to potential unmeasured confounding, e-values were reported for the adherent to nonadherent comparison. E-values denote the minimum strength of association an unmeasured confounder would need to have with both the predictor and the outcome to fully explain observed differences, beyond any measured covariates [35]. All analyses were performed using R statistical software version 4.2.2, PSWeight version 1.1.8 package [33, 36].
Results
Baseline characteristics
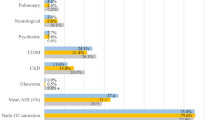
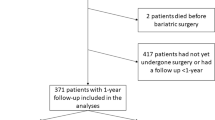
The final cohort included 173,691 patients with obesity and newly diagnosed OSA who initiated PAP therapy (Fig. 1). Of these, 46.6% were female, the mean age was 51.6 ± 12.0 years, and over two-thirds of patients (68.0%) had commercial health insurance (Table 1). Comorbid conditions were common, with 95.3% of patients having at least 1 comorbid condition. The mean number of comorbid conditions was 4.3 (2.7) in the overall cohort, with the most common being hypertension (experienced by 67.0% of patients), hyperlipidemia (56.3%), musculoskeletal pain (55.5%), GERD (31.0%), type 2 diabetes (30.1%), depression (26.8%), and anxiety (26.4%). Almost one-quarter of patients had a claim for a lifestyle intervention for weight management; baseline fills for GLP-1 receptor agonists for the treatment of obesity and/or type 2 diabetes was low (3.8%). During baseline, 34.7% of patients had an ER visit and 12.3% had an inpatient hospitalization for any cause.

BMI body mass index, CSA central sleep apnea, ESRD end stage renal disease, ICD-10 International Classification of Diseases, Tenth Revision, kg/m2 kilograms per meters squared, NH nocturnal hypoventilation, OSA obstructive sleep apnea, PAP positive airway pressure.
In the unadjusted cohort prior to IPTW, patients who were adherent to PAP therapy were significantly more likely than patients who were intermediately adherent or nonadherent to be male, older, and be commercially insured. Baseline healthcare resource use and costs were lower among adherent patients compared to those of intermediate and nonadherent patients. All healthy user proxy variables assessed during baseline (statin medication PDC, antihypertensive medication PDC, beta blocker medication PDC, wellness visit, flu vaccination) differed significantly by adherence group (Table 1). After applying IPTW, the adherence groups were well balanced on all baseline characteristics, including prior year HCRU, and healthy user proxies (absolute value of all SMDs <0.1; Supplementary Table 3).
PAP adherence
In the first 2 years following PAP initiation, 35.2% of patients (n = 61,171) were considered adherent to PAP therapy, 39.1% (n = 67,938) were intermediately adherent, and 25.7% (n = 44,582) were nonadherent. PAP usage overall and for each adherence group is shown in Table 2. In the overall cohort, 67.9% met the CMS criteria for PAP adherence in the first 90 days. In adherent patients, PAP usage was consistent over 2 years, averaging almost daily, full night use. Average PAP use for intermediately adherent and nonadherent patients was lower than that for adherent patients and decreased over time.
PAP adherence and healthcare resource use and costs
After applying IPTW, over the first year of PAP use, patients who were adherent to PAP therapy had significantly fewer (mean ± SD) all-cause ER visits (adherent: 0.55 ± 1.77 vs. intermediate: 0.62 ± 1.68; vs. nonadherent: 0.69 ± 1.78) and hospitalizations (adherent: 0.10 ± 0.44 vs intermediate: 0.13 ± 0.53; vs. nonadherent: 0.14 ± 0.56) than intermediate or nonadherent patients (all p < 0.001). Results were similar in the second year with adherent patients continuing to have significantly fewer ER visits (adherent: 0.50 ± 1.51 vs. intermediate: 0.59 ± 1.60; vs. nonadherent: 0.65 ± 1.69) and hospitalizations (adherent: 0.09 ± 0.40 vs. intermediate: 0.13 ± 0.53; vs. nonadherent: 0.13 ± 0.56) (all p < 0.001). (Table 3, Fig. 2). Healthcare resource use for intermediately adherent patients fell between that of adherent and nonadherent patients, with significantly lower mean all-cause ER visits and hospitalizations compared to patients who were nonadherent to PAP therapy over 2 years. E-values for ER visits were 1.85 and 1.95 and for hospitalizations were 2.22 and 2.52 in the first and second years, respectively.

Annual per-person emergency room visits (A) and all-cause hospitalizations (B) in year prior to, 1st, and 2nd years of positive airway pressure (PAP) therapy after applying inverse probability treatment weighting. All comparisons between adherence groups for ER visits and all-cause hospitalizations were significant at P < 0.001 except for the comparison of intermediate adherence vs non-adherence groups on all-cause hospitalizations, which was significant at P < 0.05.
Total costs in year 1, were significantly lower for adherent patients than intermediately adherent or nonadherent patients (adherent: $11,332 ± $21,160 vs. intermediate: $11,947 ± $19,325 [p = 0.005]; vs. nonadherent: $11,927 ± $20,212 [p < 0.001]), with an absolute difference in mean costs of $595 for adherent vs. nonadherent patients. Results were similar when excluding sleep apnea equipment, with a difference in mean costs of $991 for adherent vs. nonadherent patients (p < 0.001). Inpatient hospitalization costs (adherent: 1384 ± 7022 vs. intermediate: 1854 ± 8902; vs. nonadherent: 2116 ± 9723) and ER visit costs (adherent: 536 ± 2236 vs. intermediate: 608 ± 1794; vs. nonadherent: 677 ± 1852) were also significantly lower (all p < 0.001).
Results in the second year were consistent. Mean total costs for adherent patients were $695 less than for nonadherent patients (10,531 ± 19,106 vs. 11,226 ± 21,706 [p < 0.001]), and $1023 less when excluding sleep apnea equipment (10,092 ± 19,056 vs. 11,115 ± 21,665 [p < 0.001]). Adherent patients also had significantly lower costs compared to intermediately adherent patients when sleep apnea equipment was excluded (10,092 ± 19,056 vs. 11,159 ± 21,319 [p < 0.001]). Inpatient hospitalization (adherent: 1239 ± 6658 vs. intermediate: 1886 ± 9118; vs. nonadherent: 1984 ± 9436) and ER visit (adherent: 503 ± 1935 vs. intermediate: 594 ± 1779; vs. nonadherent: 649 ± 1802) costs remained significantly lower for adherent compared to intermediately and nonadherent patients (all p < 0.001) (Table 3).
Discussion
In this real-world study among patients with obesity and newly diagnosed with OSA, we found that sustained adherence to PAP therapy over 2 years was associated with significantly lower HCRU, including fewer emergency room (ER) visits and hospitalizations, and substantially reduced healthcare costs, compared with patients who did not adhere to PAP therapy. While the per-patient annual savings may be modest at the individual level, ~$600–$700 with equipment in years 1 and 2, respectively, they could translate to substantial cumulative savings at the population level and may represent cost-savings opportunities if the ~80% of OSA patients who remain undiagnosed were treated. For most outcomes, patients with intermediate PAP adherence also demonstrated reductions in HCRU and healthcare costs relative to nonadherent patients, suggesting a dose-dependent relationship. This finding is consistent with previous research indicating measurable clinical and economic benefits even from modest nightly PAP usage (1–3 h of PAP use per night) [37]. The observed decline in PAP adherence over time in the intermediate adherence group underscores the need for targeted interventions, particularly within the first year of treatment, to sustain initial adherence and maximize long-term benefits [38].
Until recently, the impact of untreated or inadequately treated OSA on economic outcomes has been understudied [39, 40]. A limited number of US real-world studies, employing other datasets and methodologies, have found an association between PAP use and/or PAP adherence and lower HCRU and/or healthcare costs [39,40,41]. However these studies have several limitations including small sample sizes, lack of objective PAP adherence data, and inadequate control for confounding factors such as the healthy user bias and PAP adherence [39]. Our study addresses these limitations by leveraging objective PAP adherence data from cloud-connected devices linked to administrative claims and a bigger sample size strengthens the evidence that better adherence is associated with lower HCRU and costs.
Our findings reinforce and expand on previous analyses linking administrative claims data and objective PAP usage, which have demonstrated lower HCRU with better adherence to PAP therapy in a general population newly diagnosed with OSA [20] and in OSA populations with major pre-existing comorbid conditions, including COPD [21], T2D [22], heart failure [23, 24], atrial fibrillation [25], and depression [26]. Across these populations, increased adherence to PAP therapy was consistently and significantly associated with fewer all-cause ER visits and hospitalizations and lower healthcare costs in the first and second years of PAP use. In analyses that included patients with intermediate adherence [23,24,25,26], there was evidence of a dose-dependent relationship, with intermediate patients generally having worse outcomes than adherent patients but better outcomes than nonadherent patients, a pattern consistent with the results of the present analysis which further emphasizes the clinical importance of promoting even modest improvements in adherence.
Lower HCRU and costs among patients who are adherent to PAP therapy may be explained at least in part by improvements in the comorbid conditions associated with OSA and obesity. The combination of untreated OSA and obesity increases the risk of certain conditions (e.g., hypertension, cardiovascular and cerebrovascular disease, atrial fibrillation, T2D, and dyslipidemia) and complications from those conditions. Improvement in symptoms or the progression of comorbid conditions due to treatment for OSA may be reflected in lower HCRU and costs. For example, data from recent meta-analyses have shown that OSA is an independent risk factor for prediabetes and T2D [42], and that treatment with CPAP improves hemoglobin A1c and long-term glycemic control in patients with T2D [43]. Since poor glycemic control has been associated with high direct medical costs of treating T2D [44], the improvements in glycemic control with PAP adherence [42] may partly explain the lower costs observed in our study.
Our findings should be interpreted considering several limitations inherent to observational studies using administrative claims data [45]. First, claims data are primarily generated for billing and reimbursement of purposes and lack detailed clinical information such as patient-reported outcomes, laboratory results, and comprehensive data on social determinants of health. Future studies integrating electronic medical records or patient-reported outcomes data could address these gaps and provide deeper insights. Second, although obesity identification through ICD codes is highly specific, obesity is known to be underreported in claims databases [46]. As a result, our study may not have captured all individuals with obesity, potentially influencing generalizability. However, the high specificity (>97%) of obesity ICD codes provides confidence in the accurate characterization of our sample [46]. Third, the findings represent insured individuals within the US healthcare system, which limits the generalizability to uninsured populations or international contexts. Additionally, healthcare utilization not captured by claims (e.g., out-of-pocket or non-reimbursable services) was not assessed, potentially underestimating true healthcare resource use. Fourth, healthcare cost estimates were derived from Inovalon’s proprietary Proxy Financials algorithm. While this method provides standardized estimates, it may not reflect actual paid amounts and could limit the precision of cost-related results. Observational research inherently carries a risk of healthy user bias—patients adherent to PAP therapy may also engage in other health-promoting behaviors [47, 48]. To control for any potential healthy user bias, we included several proxy variables for healthy user behavior as covariates in our analysis, all of which were well-balanced after IPTW adjustment. Furthermore, based on the calculated E-values, unmeasured confounders, including a healthy user effect, would have to be associated with both PAP adherence and outcomes by at least a factor of ~2 (E-values of 1.85 and 1.95 for ER visits and 2.22 and 2.52 for hospitalizations in the first and second year, respectively) to explain fully the observed effect. This suggests our findings are relatively robust to unmeasured confounding. As this association would have to be beyond any associations already captured, this degree of residual confounding is unlikely given the extensive set of covariates included in this analysis. Finally, patients with Medicare fee-for-service coverage and patients using PAP devices manufactured by other companies were not included in our data set, thereby possibly further limiting the generalizability of these findings.
Despite these limitations, our study has several strengths. Importantly, the use of administrative claims data linked to objective PAP data from cloud-connected devices. Objective PAP use data to classify adherence groups has been shown to perform better in terms of accuracy than claims-based definitions of PAP adherence [49]. The linkage of objective adherence data with comprehensive administrative claims significantly enhances the validity and clinical relevance of our findings. Our large and diverse study cohort in terms of geographic region, payer type, and patient characteristics, enhances the generalizability of findings across the US healthcare landscape. Additionally, our robust analytical approach using IPTW created well-balanced groups and minimized the effects of measured confounding without loss of sample size or statistical power. Use of IPTW also allowed for the analysis of more than 2 groups; including the intermediate adherence group increased the generalizability of the results and better characterized real-world adherence patterns [20].
Conclusion
In this large real-world cohort of patients with obesity and newly diagnosed OSA, sustained adherence to PAP therapy over two years was associated with significantly lower healthcare utilization and costs. These results highlight that supporting long-term PAP adherence, could lead to significant reduction healthcare utilization and costs, and ultimately improve overall patient quality of life for patients living with obesity and OSA.
Data availability
The data that support the findings of this study are available from Inovalon Insights LLC and Resmed Corp, but restrictions apply to the availability of these data, which were used under license for the current study, and so are not publicly available. Data are however available from the authors upon reasonable request and with permission of Inovalon Insights LLC and Resmed Corp.
References
Lévy P, Kohler M, McNicholas WT, Barbé F, McEvoy RD, Somers VK, et al. Obstructive sleep apnoea syndrome. Nat Rev Dis Prim. 2015;1:15015.
Eckert DJ, Malhotra A. Pathophysiology of adult obstructive sleep apnea. Proc Am Thorac Soc. 2008;5:144–53.
Benjafield AV, Ayas NT, Eastwood PR, Heinzer R, Ip MSM, Morrell MJ, et al. Estimation of the global prevalence and burden of obstructive sleep apnoea: a literature-based analysis. Lancet Respir Med. 2019;7:687–98.
Hudgel DW, Patel SR, Ahasic AM, Bartlett SJ, Bessesen DH, Coaker MA, et al. The role of weight management in the treatment of adult obstructive sleep apnea. An official american thoracic society clinical practice guideline. Am J Respir Crit Care Med. 2018;198:e70–e87.
Ward ZJ, Bleich SN, Cradock AL, Barrett JL, Giles CM, Flax C, et al. Projected U.S. state-level prevalence of adult obesity and severe obesity. N Engl J Med. 2019;381:2440–50.
Garvey JF, Pengo MF, Drakatos P, Kent BD. Epidemiological aspects of obstructive sleep apnea. J Thorac Dis. 2015;7:920–9.
Young T, Peppard PE, Taheri S. Excess weight and sleep-disordered breathing. J Appl Physiol. 2005;99:1592–9.
Frost & Sullivan (for the American Academy of Sleep Medicine). Hidden health crisis costing America billions. 2016.
Lopez C, Bendix J, Sagynbekov K Weighing down America: 2020 update. Milken Institute; 2020.
Cawley J, Biener A, Meyerhoefer C, Ding Y, Zvenyach T, Smolarz BG, et al. Direct medical costs of obesity in the United States and the most populous states. J Manag Care Spec Pharm. 2021;27:354–66.
Divino V, Ramasamy A, Anupindi VR, Eriksen KT, Olsen AH, DeKoven M, et al. Complication-specific direct medical costs by body mass index for 13 obesity-related complications: a retrospective database study. J Manag Care Spec Pharm. 2021;27:210–22.
Patil SP, Ayappa IA, Caples SM, Kimoff RJ, Patel SR, Harrod CG. Treatment of adult obstructive sleep apnea with positive airway pressure: an American Academy of Sleep Medicine systematic review, meta-analysis, and GRADE assessment. J Clin Sleep Med. 2019;15:301–34.
Pépin JL, Bailly S, Rinder P, Adler D, Benjafield AV, Lavergne F, et al. Relationship between CPAP termination and all-cause mortality: a French Nationwide Database analysis. Chest. 2022;161:1657–65.
Benjafield AV, Pepin JL, Cistulli PA, Wimms A, Lavergne F, Sert Kuniyoshi FH, et al. Positive airway pressure therapy and all-cause and cardiovascular mortality in people with obstructive sleep apnoea: a systematic review and meta-analysis of randomised controlled trials and confounder-adjusted, non-randomised controlled studies. Lancet Respir Med. 2025;13:403–13.
Qaseem A, Holty JE, Owens DK, Dallas P, Starkey M, Shekelle P. Management of obstructive sleep apnea in adults: a clinical practice guideline from the American College of Physicians. Ann Intern Med. 2013;159:471–83.
Hamilton GS, Edwards BA. The potential impact of GLP-1 agonists on obstructive sleep apnoea. Respirology. 2023;28:824–5.
Al Oweidat K, Toubasi AA, Tawileh RBA, Tawileh HBA, Hasuneh MM. Bariatric surgery and obstructive sleep apnea: a systematic review and meta-analysis. Sleep Breath. 2023;27:2283–94.
Malhotra A, Pettus JH. Continuous positive airway pressure is here to stay. Lancet Respir Med. 2024;12:507–8.
Wickwire EM, Fernandez CR, Huynh N, Watson NF, Duncan I. Association between positive airway pressure therapy and healthcare costs among older adults with comorbid obstructive sleep apnea and common chronic conditions: an actuarial analysis. Sleep. 2025;48:zsaf009.
Sterling KL, Alpert N, Cistulli PA, Pépin JL, More S, Cole KV, et al. Healthcare resource utilisation and costs in patients with treated obstructive sleep apnea. J Sleep Res. 2024;33:e14099.
Sterling KL, Pépin JL, Linde-Zwirble W, Chen J, Benjafield AV, Cistulli PA, et al. Impact of positive airway pressure therapy adherence on outcomes in patients with obstructive sleep apnea and chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2022;206:197–205.
Sterling KL, Cistulli PA, Linde-Zwirble W, Malik A, Benjafield AV, Malhotra A, et al. Association between positive airway pressure therapy adherence and health care resource utilization in patients with obstructive sleep apnea and type 2 diabetes in the United States. J Clin Sleep Med. 2023;19:563–71.
Malhotra A, Cole KV, Malik AS, Pépin JL, Kuniyoshi FHS, Cistulli PA, et al. Positive airway pressure adherence and health care resource utilization in patients with obstructive sleep apnea and heart failure with reduced ejection fraction. J Am Heart Assoc. 2023;12:e028732.
Cistulli PA, Malhotra A, Cole KV, Malik AS, Pépin JL, Kuniyoshi FHS, et al. Positive airway pressure therapy adherence and health care resource use in patients with obstructive sleep apnea and heart failure with preserved ejection fraction. J Am Heart Assoc. 2023;12:e028733.
Sterling KL, Alpert N, Malik AS, Pépin JL, Benjafield AV, Malhotra A, et al. Association between sleep apnea treatment and health care resource use in patients with atrial fibrillation. J Am Heart Assoc. 2024;13:e030679.
Wickwire EM, Cole KV, Dexter RB, Malhotra A, Cistulli PA, Sterling KL, et al. Depression and comorbid obstructive sleep apnea: association between positive airway pressure adherence, occurrence of self-harm events, healthcare resource utilization, and costs. J Affect Disord. 2024;349:254–61.
Pearson-Stuttard J, Banerji T, Capucci S, de Laguiche E, Faurby MD, Haase CL, et al. Real-world costs of obesity-related complications over eight years: a US retrospective cohort study in 28,500 individuals. Int J Obes. 2023;47:1239–46.
Borsoi L, Armeni P, Donin G, Costa F, Ferini-Strambi L. The invisible costs of obstructive sleep apnea (OSA): systematic review and cost-of-illness analysis. PLOS One. 2022;17:e0268677.
Golestaneh L, Alvarez PJ, Reaven NL, Funk SE, McGaughey KJ, Romero A, et al. All-cause costs increase exponentially with increased chronic kidney disease stage. Am J Manag Care. 2017;23:S163–S72.
United States Centers for Medicare and Medicaid Services. Positive airway pressure (PAP) devices: complying with documentation & coverage requirements (ICN 905064). 2016.
Brookhart MA, Patrick AR, Dormuth C, Avorn J, Shrank W, Cadarette SM, et al. Adherence to lipid-lowering therapy and the use of preventive health services: an investigation of the healthy user effect. Am J Epidemiol. 2007;166:348–54.
Platt AB, Kuna ST, Field SH, Chen Z, Gupta R, Roche DF, et al. Adherence to sleep apnea therapy and use of lipid-lowering drugs: a study of the healthy-user effect. Chest. 2010;137:102–8.
Zhou T, Tong G, Li F, Thomas LE, Li F PSweight: an R package for propensity score weighting analysis. arxiv. 2020. https://arxiv.org/abs/2010.08893.
Austin PC, Stuart EA. Moving towards best practice when using inverse probability of treatment weighting (IPTW) using the propensity score to estimate causal treatment effects in observational studies. Stat Med. 2015;34:3661–79.
VanderWeele TJ, Ding P. Sensitivity analysis in observational research: introducing the E-value. Ann Intern Med. 2017;167:268–74.
R-CoreTeam. R: a language and environment for statistical computing. 2021. Available from: https://www.r-project.org.
Malhotra A, Sterling KL, Cistulli PA, Pépin JL, Chen J, Woodford C, et al. Dose-response relationship between obstructive sleep apnea therapy adherence and healthcare utilization. Ann Am Thorac Soc. 2023;20:891–7.
Sterling KL, Benjafield A, Cole KV, Malik A, Chen J, More S, et al. Time to intervene: long-term positive airway pressure adherence in obstructive sleep apnea patients with comorbidities. Am J Respir Crit Care Med. 2022;205:A2572.
Wickwire EM. Value-based sleep and breathing: health economic aspects of obstructive sleep apnea. Fac Rev. 2021;10:40.
Wickwire EM, Albrecht JS, Towe MM, Abariga SA, Diaz-Abad M, Shipper AG, et al. The impact of treatments for OSA on monetized health economic outcomes: a systematic review. Chest. 2019;155:947–61.
An J, Glick HA, Sawyer AM, Arguelles J, Bae CJ, Keenan BT, et al. Association between positive airway pressure adherence and health care costs among individuals with OSA. Chest. 2023;163:1543–54.
Wang C, Tan J, Miao Y, Zhang Q. Obstructive sleep apnea, prediabetes and progression of type 2 diabetes: a systematic review and meta-analysis. J Diab Investig. 2022;13:1396–411.
Herth J, Sievi NA, Schmidt F, Kohler M. Effects of continuous positive airway pressure therapy on glucose metabolism in patients with obstructive sleep apnoea and type 2 diabetes: a systematic review and meta-analysis. Eur Respir Rev. 2023;32:230083.
Oglesby AK, Secnik K, Barron J, Al-Zakwani I, Lage MJ. The association between diabetes related medical costs and glycemic control: a retrospective analysis. Cost Eff Resour Alloc. 2006;4:1.
Datavant. 2023. https://www.datavant.com/blog/claims-data.
Suissa K, Schneeweiss S, Lin KJ, Brill G, Kim SC, Patorno E. Validation of obesity-related diagnosis codes in claims data. Diab Obes Metab. 2021;23:2623–31.
Albrecht JS, Kapur VK. Untangling treatment effect from patient factors: the challenge of the use of observational studies to investigate the impact of positive airway pressure therapy on medical costs. Chest. 2023;163:1358–9.
Shrank WH, Patrick AR, Brookhart MA. Healthy user and related biases in observational studies of preventive interventions: a primer for physicians. J Gen Intern Med. 2011;26:546–50.
Alpert N, Cole KV, Dexter RB, Sterling KL, Wickwire EM. Performance of claims-based algorithms for adherence to positive airway pressure therapy in commercially insured patients with OSA. Chest. 2024;165:1228–38.
Acknowledgements
This study was funded by Resmed.
Funding
Resmed.
Author information
Authors and Affiliations
Consortia
Contributions
Study conception and design; AC, RBD, CW, NA, KLS; data analysis: RBD; interpretation: FSK, AC, RBD, CW, NA, PAC, JLP, AM; drafting the first version of the manuscript: FSK, AC, NA; revised the manuscript and approved the final version: all authors.
Corresponding author
Ethics declarations
Competing interests
FSK, AC, RBD, CW, NA, and KLS are employees of Resmed. JLP is supported by the French National Research Agency (ANR) in the framework of the “FRANCE 2030” program, the “e-health and integrated care” chair of Grenoble Alpes University Foundation and “Sleep Health-AI chair” in “MIAI Cluster” of artificial intelligence (ANR-23-IACL-0006). JLP reports income related to medical education from RESMED, SEFAM, Zoll-Respicardia, Eli Lilly, Idorsia, Pharmanovia and Bioprojet. PAC reports having an appointment to an endowed academic Chair at the University of Sydney that was established by Resmed funding, has received research support from Resmed and SomnoMed, and is a consultant to Resmed, SomnoMed, Sunrise Medical, and Eli Lilly. SHM, BS, SRB and KCW are employees of Boston Strategic Partners, funded by Resmed. LW and CK are independent statisticians, funded by Resmed. TK reports project funding from the Canadian Institute of Health Research and CHEST Foundation. DAJ has received consultancy fees from Idorsia. RH has received speaker or consultancy fees from Resmed, Jazz Pharmaceuticals, Inspire Medical Systems, Bioprojet, Philips, Merck, Nyxoah, Medtronic, Nestlé and Löwenstein. CHL has no conflicts to declare. AM is funded by the National Institutes of Health (NIH). AM also reports income related to medical education from Livanova, Jazz Pharmaceuticals, Zoll and Eli Lilly. Resmed provided a philanthropic donation to UC San Diego, but AM has not received personal income from Resmed or medXcloud.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Sert Kuniyoshi, F.H., Cameron, A., Pépin, JL. et al. Adherence to positive airway pressure therapy and healthcare resource utilization and costs among patients with obstructive sleep apnea and obesity. Int J Obes 50, 741–749 (2026). https://doi.org/10.1038/s41366-025-01985-1
Received:
Revised:
Accepted:
Published:
Version of record:
Issue date:
DOI: https://doi.org/10.1038/s41366-025-01985-1
