
Abstract
Intelligent wound management necessitates flexible and personalized wound dressings capable of real-time physiological monitoring and targeted therapeutic interventions. A significant challenge lies in integrating diverse sensing and stimulation components into an all-in-one dressing while maintaining material compatibility and structural interoperability. Here, we present a sophisticated and scalable flexible diagnostic and therapeutic dressing (FDTD) based on modifiable poly(3,4-ethylenedioxythiophene):polystyrene sulfonate (PEDOT:PSS). By tuning the electrical conductivity of the PEDOT:PSS film (1 S/cm to 6.4 kS/cm) while maintaining a low Young’s modulus, we enable the versatile integration of temperature, impedance, and pH sensors alongside electrical and optical stimulators into a single, flexible dressing. Biosensing assays demonstrate high sensitivity (1 Ω/°C, −2 mV/10% volumetric water content, and −30 mV/pH), excellent linearity (R2 > 0.99), and robust reproducibility. In vivo therapeutic efficacy, rigorously assessed using circular and square wound models in Sprague-Dawley rats, reveals that FDTD-mediated electro-optical synergistic therapy achieves greater than 98% wound closure within 8 days, significantly outperforming the control group (<65%) and other reported physical therapies (≤90%). Mechanistically, accelerated regeneration is attributed to improved cellular proliferation, collagen organization, and neovascularization facilitated by electro-optical synergistic treatment. Furthermore, the integration of wireless power transfer and Bluetooth modules enables real-time data acquisition and remote therapeutic modulation, positioning FDTD as a promising platform for transformative wound management.

Similar content being viewed by others


Introduction
Skin wounds arising from acute traumatic injuries or chronic debilitating illnesses affect over 305 million individuals worldwide, placing a substantial burden on healthcare systems1,2,3. While ideal wound healing proceeds through a canonical cascade of inflammation, proliferation, and remodeling, this process is frequently impeded by factors such as bacterial infections, underlying chronic conditions, or suboptimal treatment strategies4. Crucially, the wound’s microenvironment undergoes dynamic alterations throughout the healing trajectory, offering valuable diagnostic insights into the wound’s status and repair stage. Among key indicators, temperature variations reflect the inflammatory status at the wound site, with an elevated temperature being a prominent predictor of infection5,6. Conversely, wound impedance typically increases with epidermal proliferation and granulation tissue formation, decreasing with cell loss and compromised membrane integrity7,8,9. Furthermore, healthy skin exhibits a slightly acidic pH (5.5–6.5), whereas wounds tend towards alkalinity following barrier disruption10,11. Maintaining a balanced pH during healing is crucial for optimal protease activity and effective extracellular matrix remodeling. Regarding wound therapies, non-invasive physical modalities have gained clinical acceptance and U.S. Food and Drug Administration approval for promoting wound healing. However, given the dynamic nature of the healing cascade and complex wound microenvironment, a single physical field therapy may be insufficient to address the multifaceted challenges of wound management. Therefore, targeted physical interventions are urgently needed to optimize healing outcomes. For example, electric field stimulation (ES) can augment the endogenous electric field at the wound site, directing the migration of keratinocytes and fibroblasts (galvanotaxis) and stimulating their proliferation to accelerate re-epithelialization and angiogenesis through the upregulation of growth factors12. Similarly, photobiomodulation (PM) can enhance mitochondrial cytochrome-c-oxidase activity, increase ATP production, and reduce reactive oxygen species (ROS), thereby attenuating inflammatory responses and promoting collagen synthesis and cellular repair13,14. Consequently, effective wound management protocols require portable and integrated platforms that can streamline diagnostic monitoring and therapeutic interventions. However, current clinically available physiological signal sensing technologies and non-pharmacological stimulation techniques often rely on bulky extracorporeal equipment, posing limitations due to the requirement for specialized operator training and complex implementation, hindering their ability to conform to complex wound geometries.
Flexible wound dressings offer a promising alternative, addressing the limitations of existing approaches by providing real-time wound monitoring and active treatment through the integration of multimodal sensors and stimulators15,16,17. Nevertheless, incorporating these diverse components into a single flexible dressing presents significant challenges related to material compatibility and structural interoperability, potentially increasing manufacturing complexity and compromising overall flexibility. Furthermore, many existing designs heavily rely on metallic materials for core circuitry and electrical connections to sensing and stimulation elements18,19. While metals offer high conductivity and established reliability in conventional electronics, their limitations in terms of biocompatibility and mechanical properties render them suboptimal for flexible and wearable healthcare applications. Firstly, metal hypersensitivity predisposes patients to allergic reactions or adverse immune responses, which preclude using metal-based wound dressings in diverse populations20,21 Secondly, despite advances in structural engineering and manufacturing techniques22,23, the stark contrast between the high Young’s modulus of metals (typically in the ~102 GPa range) and the much lower modulus of biological tissues results in mechanical mismatch. This discrepancy can lead to discomfort, irritation, and even skin damage when prolonged contact occurs24,25. To mitigate these concerns, non-metallic conductive materials such as carbon nanotubes, graphene, and MXenes have garnered considerable attention due to their potential to enhance both the performance and biocompatibility of flexible wound dressings. However, while various conductive and functional materials have been explored for wound monitoring and stimulation, their practical implementation remains limited by biocompatibility concerns, mechanical mismatch, and fabrication complexity, particularly when multiple sensing and therapeutic modalities need to be integrated26,27,28,29,30. Although recent studies have attempted to combine different functional units, most existing designs still treat sensing and stimulation as separate modules and rely on heterogeneous material assemblies, preventing the realization of a coherent, fully integrated platform31,32,33,34,35. Consequently, there remains a clear need for a unified system capable of delivering multimodal diagnostics together with coordinated therapeutic interventions in a mechanically compliant and biocompatible format.
Here, we present an all-in-one flexible diagnostic and therapeutic dressing (FDTD) based on modifiable and biocompatible poly (3,4-ethylenedioxythiophene): polystyrene sulfonate (PEDOT:PSS). By sequentially introducing phosphotungstic acid (PTA) and gold nanoparticles (AuNPs) as dopants, the electrical conductivity of large-scale PEDOT:PSS films can be modulated from 1 S/cm to 6.4 kS/cm with a low Young’s modulus (1.7 ± 0.2 GPa)36,37,38,39. A temperature sensor utilized the primary PTA-doped PEDOT:PSS film for diagnostic monitoring, while impedance and pH sensors utilized the secondary PTA/Au-doped PEDOT:PSS. The sensitivities for temperature, impedance, and pH were 1 Ω/°C, −2 mV/10% volumetric water content (VWC), and −30 mV/pH, with all sensors demonstrating excellent detection linearity (R2 > 0.99). The therapeutic intervention was achieved through the integration of a PEDOT:PSS concentric electrode for ES and a 650 nm light-emitting diode (LED) for PM. The efficacy of the FDTD was evaluated using circular and square wound models in Sprague-Dawley (SD) rats. The results demonstrated that the FDTD-mediated ES-PM synergistic therapy (EPST) achieved wound closure rates of 98% and 99% within 8 days for square and circular wounds, respectively. This significantly outperformed the ES groups (76%, 88%), PM groups (75%, 81%), and control groups (54%, 63%). Mechanistic investigations revealed that the FDTD intervention synergistically enhanced the secretion of key growth factors and vascular endothelial marker protein, including platelet endothelial cell adhesion molecule-1 (PECAM-1/CD31), epidermal growth factor (EGF), transforming growth factor-β (TGF-β), and vascular endothelial growth factor (VEGF). Additionally, integrating wireless power transfer and Bluetooth modules enables real-time data acquisition and remote therapeutic modulation, positioning the FDTD as a promising platform for transformative wound management.
Results
Design and fabrication of the FDTD
Figure 1a depicts the proposed FDTD, a multifunctional platform integrating three monitoring modalities: temperature, wound impedance, and pH, as well as three therapeutic modalities: ES, PM, and EPST. This integrated design provides a comprehensive framework for intelligent wound management. The exploded schematic in Fig. 1b details the multilayer structure of the FDTD. The fabrication procedure initiates with blade-coating a primary-doped PEDOT:PSS solution onto glass substrates, followed by thermal annealing at 100 °C. The cured film is subsequently peeled off under moist conditions and transferred to a polyethylene terephthalate (PET) adhesive substrate, which serves as a robust and flexible interlayer to ensure mechanical stability (Fig. S1). This PEDOT:PSS film is then patterned to form a conductive and biocompatible platform ready for personalized modification. During this process, impedance and pH sensors were secondary doped with AuNPs before further modification. In contrast, the temperature sensor still utilized a primary-doped film for higher base resistance by applying photomasks during the secondary doping process. The therapeutic intervention was enabled by integrating a PEDOT:PSS concentric electrode for ES and a 650 nm LED for PM. Finally, the patch was encapsulated with patterned medical-grade polyurethane (PU) tape on the top and bottom surfaces, exposing the functional sensor region to the wound (Fig. S1). The utilization of breathable PU tape ensured moderate moisture vapor transmission, with a WVTR of ~1.6–1.9 × 103 g/m2·24 h that falls within the ideal range for wound dressings40. This breathability provides both wound moisture balance and a stable environment for the PEDOT:PSS functional layer. After fabrication, a microscope captured a three-dimensional image of the assembled FDTD, confirming a highly uniform surface topography across all layers (Fig. 1c). Thickness measurements for each layer reveal that the top PU adhesive layer is 20 μm, the PEDOT:PSS conductive platform layer is 2 μm, the PET intermediate layer is 20 μm, and the bottom PU adhesive layer is 20 μm, resulting in a total thickness of around 62 μm (Fig. 1d).

a Schematics of the overall FDTD system. An illustration of the FDTD in operation (facing down) highlights its multilayer structure (left). Detailed depiction of the device’s physiological monitoring functions, including temperature sensing, wound impedance measurement, and pH detection (middle). Representation of the therapeutic functions of the FDTD, including ES and PM, to promote accelerated wound healing (right). b Exploded illustration of the FDTD (facing up) with specifications of the functions of each layer. From bottom to top: bottom PU encapsulation (skin-contacting base for adhesion and mechanical support), PET interlayer, functional layers (temperature, pH/impedance sensors, and ES/PM modules), and top PU encapsulation with patterned openings above electrode regions for wound contact. c A side-view three-dimensional microscope image of the multilayer structure. d The height profile along the purple line in (c) shows the height of multilayers. e Optical images of a (4 × 4) matrix of the sensors in square and circular geometries. f–h Image of (2 × 2) FDTD matrix under normal, diagonal stretched, and twisted states. i Two FDTDs attached to the dorsal side of a clenched human hand. j Finite-element simulations in Abaqus CAE on the FDTD device under uniaxial tensile strains of 10%, 20%, and 30%. k Fluorescence images of stained fibroblasts cultured on a regular cell culture dish and the extracts from FDTD. l A comparison of normalized cell viability over five days shows excellent FDTD biocompatibility
The streamlined fabrication process also enabled the creation of customizable geometries, including square and circular configurations, which were implemented for clinical wound profiles (Fig. 1e). The low modulus and serpentine geometry can effectively promote structural robustness and minimize flexibility restrictions. Consequently, a 2 × 2 FDTD matrix could withstand diverse deformation conditions, including its original state, diagonal stretching, and multiple twists (Fig. 1f–h and Movie S1). Figure 1i demonstrated the experimental setup where FDTD patches in square and circular geometries were seamlessly attached to the skin. Movie S2 further demonstrates the dynamic functionality of a working FDTD under bending, validating its robust performance during which the FDTD continues to power the red LED. Finite-element simulations under 10-30% uniaxial strain (Fig. 1j and Movie S3) showed that the serpentine interconnects progressively elongate to accommodate deformation, thereby preventing localized stress buildup. The maximum von Mises stress remained ~40 MPa, with most PEDOT:PSS regions below ~20 MPa, which are within or beneath the reported tensile strength range of acid-treated PEDOT:PSS and well below that of the PET substrate, as detailed in Note S141,42. These results confirm that all components operate within their elastic regimes and that the serpentine architecture provides reliable strain tolerance for conformal, skin-mounted applications.
To further ensure operational safety, we assessed the thermal response of the integrated LED. As shown in the Supporting Information (Fig. S2), the LED rapidly reached a stable temperature of 36 °C within 15 s, remaining well below established safety thresholds for skin-contact electronics and significantly lower than pathological wound temperatures (≥38 °C). Beyond mechanical robustness and thermal safety, the biocompatibility of the FDTD was systematically evaluated. In vitro cytotoxicity tests using L929 mouse fibroblast cells cultured with FDTD extracts showed no significant differences in cell viability over 1, 3, and 5 days, as confirmed by quantitative CCK-8 assays (Fig. 1k, l) and fluorescence staining. Two complementary animal studies further validated in vivo compatibility. In the long-term contact test, FDTD patches were applied to the dorsal skin of SD rats. Photographs and histological analyses (H&E and Masson’s trichrome) taken at days 0, 4, and 8 revealed no erythema, edema, or tissue abnormalities (Fig. S3). To assess potential toxicity, FDTD devices were implanted subcutaneously in SD rats, and vital organs were harvested after 2 weeks for H&E staining (Fig. S4). Both tests showed intact tissue structures without inflammation or damage.
Collectively, these results demonstrate that the FDTD combines mechanical resilience, thermal safety, and excellent biocompatibility, supporting its potential for safe and reliable clinical translation in innovative wound management systems.
Modification and characterization of the PEDOT:PSS film
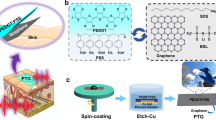
In this study, we introduced a two-step doping strategy to tune the electrical conductivity of the PEDOT:PSS film while maintaining its biocompatibility and practical feasibility. Figure 2a illustrates the conceptual framework, depicting the chemical reactions and material interactions involved in both the primary and secondary doping processes. PTA, a well-known heteropolyacid catalyst43,44, was employed as the primary dopant due to its strong protonic acidity, excellent oxidative potential, and favorable biocompatibility. These properties facilitate enhanced charge carrier mobility and structural ordering within the PEDOT:PSS matrix, thereby improving film conductivity. As shown in Fig. 2b, the sheet resistance (Rs) of the PTA-doped films decreased exponentially from an undoped value of 5 kΩ/sq to 26.8 Ω/sq as the PTA concentration increased from 0 to 1 wt%, and then further declined to a minimum of 1.3 Ω/sq at 6 wt%. Beyond this optimal concentration, Rs rose to 4.2 and 5.7 Ω/sq at 7–8 wt%, respectively. The measurement setup and procedure are schematically illustrated in Fig. S5. Correspondingly, the electrical conductivity could be regulated from 1 S/cm to 3.8 kS/cm with primary doping. The initial reduction aligns with enhanced protonation-driven conductivity, while the rise at higher concentrations may be attributed to excessive protonation disrupting the PEDOT:PSS microstructure and increasing ionic scattering41,45. To evaluate the morphological uniformity of the primary-doped PEDOT:PSS films, scanning electron microscopy (SEM) and atomic force microscopy (AFM) were employed. As shown in the low-magnification SEM image (Fig. 2c), the film exhibits a continuous, smooth surface with no observable aggregation. Higher magnification SEM (Fig. 2d) further confirms the nanoscale uniformity, revealing a consistent topography. The corresponding AFM image (Fig. 2e) displays a finely textured surface with height variations ranging from −10.0 nm to +8.0 nm, indicating relatively low surface roughness. The substantial conductivity improvement and morphological uniformity underscore the efficacy of PTA as a dopant. Consequently, the 6 wt% PTA-doped PEDOT:PSS film was selected for the subsequent secondary doping process. XRD results (Fig. S6) also verified the strengthened PEDOT \({\rm{\pi }}\)–\({\rm{\pi }}\) stacking and compressed PSS lamellae, supporting the improved charge transport.

a The conceptual framework of the doping strategy of PEDOT:PSS film. b Comparison of Rs of different amounts (0–8%wt) of PTA-doped PEDOT:PSS film. c–e SEM and AFM images of primary-doped PEDOT:PSS film. f Comparison of Rs of different amounts of HAuCl4 (0–2.0 mL) added during the secondary doping process of PEDOT:PSS film. g–i SEM and AFM images of secondary-doped PEDOT:PSS film. j SEM image of the cross-sectional view of the secondary-doped PEDOT:PSS film. k SEM image of the boundary between the primary and secondary-doped regions. l EDS result of AuNPs 1 μm under the film surface. m Comparison of the doped PEDOT:PSS film in this work with other reports
For the secondary doping step, AuNPs were generated in situ via UV-assisted reduction of chloroauric acid (HAuCl4) within a pre-reduced PTA solution. This approach enabled the uniform deposition of AuNPs onto the primary-doped PEDOT:PSS film without compromising its structural integrity. Notably, UV light allowed spatially selective doping with patterning capabilities by employing photomasks. The incorporation of AuNPs further enhanced the film’s electrical performance by facilitating charge transport and increasing the density of conductive pathways. As depicted in Fig. 2f, the Rs of the secondary-doped films were measured by applying HAuCl4 to a 1 cm × 1 cm section of the 6 wt% PTA-doped PEDOT:PSS film. The Rs decreased progressively with increasing HAuCl4 volume from 0.5 mL to 1.0 mL and then tended to stabilize, with a minimum Rs of 0.78 Ω/sq achieved at 2.0 mL of HAuCl4. The low-magnification SEM image revealed nano-sized surface features (Fig. 2g), while the high-magnification image confirmed the presence of uniformly distributed, spherical AuNPs with diameters ranging from 100 to 200 nm (Fig. 2h). The AFM image revealed a significantly rougher surface, with height variations ranging from −18.0 nm to +15.0 nm (Fig. 2i). This increased roughness arises from the protruding AuNPs on the film surface, confirming successful and effective secondary doping. Despite these surface modifications, the cross-sectional SEM image indicated that the film thickness remained consistent at ~2 μm (Fig. 2j). Consequently, the corresponding electrical conductivity increased from the primary value of 3.8 kS/cm to 6.4 kS/cm after secondary doping. An additional advantage of this doping method is its compatibility with spatial patterning. As illustrated in Fig. 2k, UV-assisted deposition of AuNPs through a photomask yielded patterned doping regions with well-defined boundaries. SEM analysis of these boundary regions revealed a distinct contrast between primary and secondary-doped areas: the secondary-doped region displayed a dense and uniform distribution of AuNPs, while the primary-doped region exhibited minimal particle presence. This capacity for spatially selective doping creates opportunities for integrating PEDOT:PSS films into advanced device architectures requiring localized functionality. Energy-dispersive spectroscopy (EDS) was performed at various depths to evaluate the distribution of AuNPs within the film. Figure 2l displays the EDS results obtained at a depth of 1 µm, confirming the presence of gold within the film matrix. These findings indicate that the secondary doping process incorporates conductive nanoparticles throughout the film, not solely on the surface. This characteristic is crucial for ensuring the mechanical and electrical stability of the films, particularly in dynamic applications that involve repeated mechanical deformation. Mechanical durability was evaluated through cyclic bending tests, as shown in Fig. S7a–c. The films underwent 1000 bending cycles of deformation, ranging from 10% to 40% of their original length, with an increase in electrical resistance of less than 4%, thereby confirming their mechanical robustness. In addition, the intrinsic stiffness of the ultrathin (~2 µm) PEDOT:PSS films was quantified by tensile testing, yielding a Young’s modulus of ~1.7 GPa (Fig. S7d). Both results demonstrate that the dual-doped PEDOT:PSS films possess both high intrinsic strength and excellent device-level flexibility, supporting their suitability for skin-conformal applications. In summary, the dual-doping strategy presented in this work addresses several limitations of existing PEDOT:PSS modification approaches, introducing a versatile platform for tailoring electrical conductivity between 1 S/cm and 6.4 kS/cm (Fig. 2m)46,47,48,49,50. Overall, this strategy offers a practical, scalable, and multifunctional solution for advancing PEDOT:PSS-based flexible and bioelectronic devices.
Performance characterization of FDTD sensing components
The FDTD system incorporates three PEDOT:PSS-based sensors, enabling the simultaneous and continuous monitoring of temperature, impedance, and pH within the wound microenvironment (Fig. 3). This multimodal sensing capability offers a comprehensive assessment of wound status and healing progression. Temperature, in particular, serves as a highly informative indicator of the inflammatory state. Clinical studies demonstrate that sustained local temperature elevations of 3–4 °C above baseline are indicative of prolonged inflammation, while normal temperature indicates transition into the proliferative healing phase5,6. The PEDOT:PSS-based temperature sensor leverages the material’s intrinsic thermoresistive properties, whereby an increase in temperature results in a predictable and measurable increase in electrical resistance. Both square and circular geometries were fabricated to evaluate their sensing performance. The temperature sensor achieves a high baseline resistance (~830 Ω) through a combination of primary doping of the PEDOT:PSS and a serpentine geometry. Stepwise resistance changes of temperature sensors from 4 FDTDs (F1–F4) in one fabrication batch were recorded across six temperature setpoints, ranging from 30 to 40 °C in 2 °C increments, confirming the expected thermoresistive behavior (Fig. 3a, Fig. S8, Movie S4). Subsequently, the steady-state resistance values at each temperature for four sensors were averaged and fitted to linear calibration curves (R² > 0.99), resulting in an average temperature coefficient of 1.000 ± 0.028 Ω/°C (Fig. 3b). The repeatability and stability of the sensor were validated through three consecutive heating-cooling cycles (30–40 °C) of one representative FDTD temperature sensor. The nearly overlapping traces and negligible baseline drift indicate robust dynamic stability and reliable performance under fluctuating thermal conditions (Fig. 3c).

a Characterization of temperature sensors from four FDTDs over 30–40 °C with 2 °C increments. b Linear analysis of temperature sensors from all four FDTDs. c Stability assessment of a representative FDTD temperature sensor across three consecutive heating-cooling cycles between 30 °C and 40 °C. d Characterization of impedance sensors from four FDTDs over 50% to 100% VWC with 10% increments. e Linear analysis of impedance sensors from all four FDTDs. f Stability assessment of a representative FDTD impedance sensor under three VWC cycling tests between 60% and 90%. g Characterization of pH sensors from four FDTDs exposed to buffer solutions with pH values ranging from 4 to 9 in 1-unit increments. h Linear analysis of pH sensors from all four FDTDs. i Stability assessment of a representative pH sensor under three pH cycling tests between pH 5 and pH 8
Wound impedance is a critical biophysical parameter that reflects the ionic concentration and moisture content of the wound microenvironment51,52. Elevated levels of wound exudate, characterized by high ionic content, lead to a reduced impedance due to increased tissue conductivity. Conversely, a gradual increase in impedance indicates progression into the proliferative phase, as the wound bed begins to dry and granulation tissue forms7,8,9. The FDTD system utilizes a pair of secondary-doped PEDOT:PSS electrodes configured for constant-current voltage sensing to track these impedance changes. To simulate the dynamic moisture conditions during wound healing, in vitro modeling was conducted using a fluid-absorbent sponge substrate with hydration levels tuned to VWC, ranging from 50% to 100% in 10% increments (Fig. 3d). This range represents the physiologically relevant transition from the exudate-rich inflammatory phase to the relatively drier remodeling phase, during which the wound bed gradually regains the moisture profile of intact skin (~50%–60% VWC). The output voltage decreased monotonically with increasing VWC, indicating increased conductivity under moist conditions. The averaged response of four sensors exhibited high linearity (R² > 0.99), with a normalized slope of −1.950 ± 0.058 mV per 10% VWC (Fig. 3e). Repeatability assessment using a single representative FDTD impedance sensor was performed across three hydration cycles, which can represent a typical wound microenvironment within a 60%–90% VWC range (Fig. 3f). The results confirmed sensor’s consistent response and negligible hysteresis. Notably, the impedance electrodes remain unmodified, allowing for further surface functionalization to enable selective detection of specific wound biomarkers. Sharing a reference electrode with the pH sensor enhances system integration while minimizing the spatial footprint.
Local pH fluctuations serve as vital biochemical indicators of wound status, offering insights into infection and the progression of healing. An alkaline pH (>7.5) is often associated with chronic inflammation or infection, whereas healthy skin maintains a mildly acidic environment (pH ~5.5). This sustained acidity promotes fibroblast proliferation and antimicrobial defense, with transient neutralization during normal healing10,11. The pH sensor integrates a secondary-doped PEDOT:PSS working electrode modified by the electropolymerization of pH-sensitive polyaniline53, with its successful deposition confirmed via cyclic voltammetry (Fig. S9a). The reference electrode comprises secondary-doped PEDOT:PSS coated with Ag/AgCl, providing a stable electrochemical potential. Sensor calibration (4–9 in 1 pH unit increments and 5–8 in 0.5 pH unit increments) was conducted in phosphate-buffered saline solutions (Fig. 3g, Fig. S9b). The averaged response of 4 pH sensors exhibited strong linearity across four devices (R² > 0.99), with a mean slope of −29.599 ± 0.175 mV per decade (Fig. 3h). The dynamic repeatability of one representative FDTD pH sensor was demonstrated through three complete pH cycles, revealing stable performance under fluctuating physiological conditions (Fig. 3i).
A comparative analysis (Note S2) with recent literature confirms that the FDTD system achieves multimodal biosignal monitoring using relatively simple materials and fabrication methods15,16,51,54,55,56. Despite this simplicity, the system effectively captures physiologically relevant signals and correlates them with wound status, facilitating intelligent diagnosis and therapy. The FDTD system’s high linearity, stability, and multimodal sensing capability enable precise wound-state mapping throughout the healing trajectory. Integrating thermal, electrical, and biochemical sensors into a compact platform provides real-time, quantitative insight into wound dynamics, offering a foundation for responsive therapeutic feedback and personalized wound care strategies.
FDTD for personalized wound diagnosis and therapy
Leveraging wireless power transfer (WPT) technology, the FDTD was designed for uninterrupted and efficient operation in wound management. As depicted in Fig. 4a, the system comprises a power module featuring a 13.56 MHz WPT coil coupled with a rechargeable battery, providing a stable power supply to sensing and stimulation components. The FDTD detects temperature, impedance, and pH signals from the wound environment, which are then processed by an analog front-end and a microcontroller unit. Subsequently, the real-time monitoring data was transmitted wirelessly via a Bluetooth module to a user interface. The WPT coil was fabricated by laser-patterning a PI/Cu substrate into a serpentine geometry (inner/outer radii: 30/36 mm; line width: 400 μm) (Fig. 4b). This design was meticulously optimized to fulfill two primary constraints: conformal adhesion to dynamically deforming skin and stable electromagnetic resonance at 13.56 MHz. To achieve precise resonance tuning and compliance with established commercial frequency standards, a 1.2 nF parallel capacitor was integrated. Vector network analysis confirmed precise resonance at 13.69 MHz, accompanied by a strong impedance match (S11 = −28.00 dB, Fig. 4c), indicating highly efficient energy coupling between the transmitting and receiving coils. Further validation using an oscilloscope demonstrated a robust peak-to-peak output of 4.0 V at the receiver terminals (Fig. 4d), which is sufficient to charge a 3.7 V rechargeable lithium battery, guaranteeing sustained operation and continuous wound monitoring in practical clinical scenarios.

a Exploded schematic of the fully integrated FDTD system, comprising a wireless power supply module, rechargeable battery, analog front-end, microcontroller, and Bluetooth-based signal transmission module. b The laser-patterned serpentine architecture of the PI/Cu-based wireless receiving coil (inner/outer radii: 30/36 mm). c S11 parameter measurement via vector network analysis under 13.56 MHz excitation. d Oscilloscope measurement of the wireless receiver output under 13.56 MHz driving. e Optical image of an SD rat wearing the FDTD system for in vivo wound monitoring. f Demonstration of FDTD seamlessly applied to the curved dorsal surface of the rat. g Real-time sensing outputs of temperature, impedance, and pH were recorded from both acute and infected wound models under normal and stretched skin conditions. h Representative open-field test result of the FDTD-wearing rats and the control group (n = 4). i Quantitative behavioral analysis comparing total distance traveled (@), time spent in center and periphery (#, $), fast and slow movement durations (&, *), and resting durations (!)
To assess the FDTD system’s mechanical resilience and performance under realistic conditions, in vivo experiments were performed on SD rats with acute and infected wounds. The device was conformally applied onto the curved dorsal surface of the rats (Fig. 4e, f), enabling simultaneous and continuous monitoring of local temperature, impedance, and pH under both resting and mechanically stretched conditions. As depicted in Fig. 4g, the sensing signals remained stable and reliably tracked wound dynamics, demonstrating robustness under physiological motion. These results validate the FDTD’s mechanical durability and sensing reliability, which are essential for long-term practical use in dynamic biological environments. To further investigate biocompatibility and wearable comfort, an open-field test (n = 4) was conducted to assess behavioral responses under unrestricted movement conditions. SD rats were divided into two groups: the FDTD-wearing group and the control group. During a 5-min trial, multiple behavioral parameters were recorded, including total distance traveled (@), time spent in the center and periphery (#, $), fast and slow movement times (&, *), and resting time in each zone(!). Statistical analysis revealed no significant differences between the groups across all parameters (Fig. 4h, i, and Fig. S10), indicating that the FDTD system did not impair natural movement or induce significant stress responses (Movie S5). These results collectively confirm that the FDTD can be comfortably worn without hindering the rats’ natural activities, demonstrating excellent biocompatibility and wearability for preclinical wound monitoring studies.
Prior to initiating in vivo wound healing experiments, COMSOL Multiphysics simulations were conducted to characterize the electric field distributions. As illustrated in Fig. 5a, both square and circular electrode configurations generated electric fields that extended from the outer electrodes toward the central inner electrode, which effectively mimics endogenous bioelectric cues to promote tissue regeneration. The simulation results indicated that the electric field strength reached approximately 300 mV/mm near the inner electrode and remained around 150 mV/mm in the intermediate regions between the electrodes, which were sufficient to promote and accelerate wound healing processes. In parallel with the electric field simulations, the FDTD optical design was assessed to determine the spatial tolerance of the integrated LED module precisely. A calibrated luxmeter was employed to measure angular light distribution from a centrally aligned patch and the FDTD configuration with the LED in the lower-right quadrant. Polar candela plots and quantitative area analysis, performed using ImageJ software, demonstrated a substantial overlap of ~85% in irradiated regions (Fig. 5b), suggesting that the PM coverage delivered by the FDTD system remained remarkably consistent despite a minor spatial offset in the LED’s placement. A comparative animal study was performed using SD rats (n = 4) to experimentally validate the robustness of this design, comparing healing outcomes between a centrally placed LED and an FDTD configuration, as noted in Note S1. The analysis of wound closure over 8 days confirmed no statistically significant differences in therapeutic efficacy between the two configurations (Fig. S11). These findings underscore the system’s spatial adaptability and robustness for practical use across variable wound geometries.

a Electric field distribution simulations for square (right) and circular (left) electrode configurations using COMSOL Multiphysics. b Polar candela plots comparing angular irradiance profiles between a centrally aligned LED and the LED embedded in the FDTD. c Optical images of square (top) and circular (bottom) wounds from EPST, ES, PM, and control groups (n = 4) over 8 days. d Square wound closure progression over 8 days of each treatment group. e Final square wound closure percentages on day 8 of each treatment group. f Circular wound closure progression over 8 days of each treatment group. g Final circular wound closure percentages of each treatment group on day 8. h Representative H&E-stained images of square wound tissues of each treatment group on day 8. i Representative Masson’s trichrome-stained images of square wound tissues of each treatment group on day 8. j Representative H&E-stained images of circular wound tissues of each treatment group on day 8. k Representative Masson’s trichrome-stained images of circular wound tissues of each treatment group on day 8
A systematic experimental strategy was implemented to investigate the therapeutic efficacy of the FDTD system (Fig. S12). For therapeutic efficacy evaluation, full-thickness square and circular wounds (1 cm in edge length or diameter) were created on the dorsal skin of six-week-old SD rats. The rats were randomly assigned to four groups (n = 4): control, ES, PM, and EPST. The control group received no active therapeutic intervention and was covered with medical PU film, while the experimental groups received 1-h daily interventions using the FDTD system for 8 consecutive days. As shown in Fig. 5c and Fig. S13, representative wound images captured on days 0, 2, 4, 6, and 8 showcased differences in the groups’ healing progression. Notably, the EPST group exhibited the most rapid and consistent wound closure, followed by the ES and PM groups. In contrast, the control group displayed the slowest rate of wound closure. Quantitative wound area analysis corroborated these observations, confirming that the EPST group achieved significantly accelerated wound closure compared to ES, PM, and control groups (Fig. 5d, f). From day 2 onward, the experimental groups, which received active treatment with the FDTD system, began to exhibit enhanced rates of wound healing relative to the control group. By day 6 to day 8, the EPST group significantly outperformed both single-modality therapies, providing compelling evidence of cumulative therapeutic synergy. After 8-day treatment, the EPST group achieved near-complete closure (98.80% ± 0.56% for square wounds and 99.37% ± 0.39% for circular wounds), which significantly outperformed ES (75.99% ± 0.17%, 88.43% ± 3.2%), PM (75.18% ± 3.19%, 81.44% ± 3.05%), and control (53.71% ± 10.47%, 63.35% ± 12.05%). Statistical analysis using Ordinary One-Way ANOVA confirmed statistically significant differences between the EPST and other treatment groups (Fig. 5e, g). In addition to the closure analysis, wound microenvironmental parameters (temperature, wound impedance, and pH) were continuously recorded during the treatment study. Representative long-term measurements from the EPST group, spanning 8 days, are provided in Fig. S14, revealing gradual changes in temperature, impedance, and pH throughout the healing process, consistent with the expected resolution of inflammation and wound maturation. Movie S6 and Fig. S15 further demonstrate an SD rat wearing the FDTD patch, with temperature, impedance, and pH signals wirelessly transmitted and displayed in real time. Further benchmarking against previously reported ES and PM studies demonstrated that our FDTD-mediated EPST approach achieved superior wound closure rates within a shorter treatment window (Fig. S16)19,57,58,59,60.
To gain a more comprehensive understanding of the tissue-level regenerative processes induced by the FDTD system, detailed histological analyses were conducted on wound tissue samples harvested on day 8 post-treatment. Hematoxylin and eosin (H&E) staining revealed that wounds in the EPST group displayed markedly enhanced re-epithelialization, denser granulation tissue formation, and stronger epidermis-dermis integration compared to ES, PM, and control groups (Fig. 5h, j, and Fig. S17). Masson’s trichrome staining corroborated these findings, confirming advanced extracellular matrix (ECM) remodeling characterized by dense and well-aligned collagen fiber deposition in the EPST group (Fig. 5i, k, and Fig. S17). In contrast, the ES and PM groups showed incomplete matrix formation and disorganized collagen alignment, while the control group exhibited sparse collagen fibers accompanied by persistent inflammation, indicating delayed wound resolution. Collectively, these findings validate the FDTD as a highly integrated, wearable diagnostic and therapeutic platform capable of facilitating real-time physiological monitoring and synergistic wound repair through the combined application of ES and PM intervention.
Intervention mechanisms for effective wound healing
Wound healing is a dynamic, multistage biological process comprising inflammation, proliferation, and remodeling phases, as schematically illustrated in Fig. 6a. To mechanistically elucidate how EPST effectively modulates this complex cascade, we rigorously correlated cellular and tissue-level responses with each specific therapeutic modality (ES, PM, and EPST). Adhering to the designed experimental framework outlined in Fig. S12, histological and molecular analyses were conducted on day 4 post-intervention. This time point was strategically chosen to characterize mid-stage wound responses, with an explicit focus on the critical transition between the inflammatory and proliferative phases (Fig. 6b, c). These evaluations focused on key vascular and regenerative markers for angiogenesis and tissue repair, including CD31, EGF, TGF-β, and VEGF. Immunohistochemical (IHC) staining of CD31, indicated by the orange arrows and dark brown staining regions in Fig. 6b and Fig. S18, revealed substantially more extensive microvascular formation in the EPST group compared to the ES, PM, and control groups. To quantify these qualitative observations, we performed rigorous quantitative image analysis using ImageJ software. The EPST group exhibited the highest average optical density (42.01 ± 3.96), significantly exceeding that of ES (28.06 ± 1.36), PM (26.53 ± 2.08), and control (14.65 ± 1.56) (Fig. 6d). We conducted immunofluorescence (IFC) analyses to further corroborate these findings and gain additional insights into the molecular mechanisms underlying EPST’s efficacy. As shown in Fig. 6e and Fig. S18, EPST treatment markedly upregulated the expression of EGF, TGF-β, and VEGF, with mean fluorescence intensities of 74.94 ± 5.69, 63.48 ± 4.09, and 71.38 ± 7.05, respectively. In comparison, the ES group exhibited moderate intensities (56.57 ± 3.75, 36.69 ± 3.96, and 39.57 ± 1.72), the PM group showed slightly lower values (49.75 ± 8.68, 34.53 ± 5.31, and 41.56 ± 1.84), while the control group consistently displayed the weakest signals (24.97 ± 3.66, 18.23 ± 2.86, and 23.44 ± 3.88). To further substantiate these fluorescence-based findings, RT-PCR assays were performed to quantitatively determine the relative mRNA expression of EGF, TGF-β, and VEGF, with all values normalized to the control group (Fig. 6f). Consistent with the IHC and IFC results, EPST stimulation produced the greatest upregulation across all three genes. Specifically, ES and PM produced moderate increases in expression, with EGF rising to 4.94 ± 0.86 and 5.19 ± 0.54, TGF-β rising to 4.44 ± 0.68 and 5.60 ± 0.20, and VEGF rising to 3.91 ± 0.71 and 3.68 ± 0.35, while EPST achieved the highest expression levels, reaching 7.31 ± 0.30 for EGF, 7.58 ± 0.75 for TGF-β, and 6.60 ± 0.62 for VEGF. These quantitative results unequivocally demonstrate that EPST significantly enhances both vascularization and the secretion of critical growth factors, thereby creating a highly regenerative microenvironment that accelerates wound healing.

a Schematic illustration of the three canonical phases of wound healing: inflammation, proliferation, and remodeling. b Representative IHC staining images of CD31 expression in square wound tissues on day 4 post-treatment across 4 groups. c IFC staining images showing the expression of EGF, TGF-β, and VEGF in wound tissues across 4 groups on day 4. d Quantitative IHC analysis of CD31 expression by average optical density across 4 groups (n = 3). e Quantitative IFC analysis of EGF, TGF-β, and VEGF expression by average optical density across 4 groups (n = 3). f RT-PCR results of three key growth factors (EGF, TGF-β, and VEGF), with relative mRNA expression levels normalized to the control group and analyzed by one-way ANOVA. g A proposed mechanistic model of how EPST facilitates wound healing
Based on these experimental results, we propose a mechanistic model summarizing how EPST orchestrates the wound healing process (Fig. 6g). ES modulates phase-specific cellular behaviors across the wound healing continuum14. During the initial inflammatory phase, ES directs immune cell dynamics, including cathodal T-lymphocyte migration and edema reduction via cathodal polarization, demonstrating anti-inflammatory efficacy. As the wound transitions into the proliferative phase, ES accelerates granulation tissue formation by promoting the migration of fibroblasts, keratinocytes, and endothelial cells, thereby addressing impaired cell motility. During the final remodeling phase, ES improves collagen alignment and scar maturation, reducing scar thickness and enhancing tensile strength14,61,62. Complementary to these effects, PM using red light (650 nm) targets mitochondrial cytochrome-c oxidase, improving the efficiency of the electron transport chain. This results in elevated mitochondrial membrane potential, increased ATP production, and the suppression of excessive pathological reactive oxygen species18. By restoring redox homeostasis, PM alleviates oxidative stress, facilitates the resolution of chronic inflammation, and promotes the transition to active tissue proliferation. Importantly, the convergence of ES and PM activates key intracellular signaling pathways, including the PI3K/Akt axis and the MAPK/ERK cascade, both of which are crucial regulators of cell survival, proliferation, and metabolic reprogramming (Fig. 6g)63,64. Through this dual modulation of bioelectrical and bioenergetic pathways, EPST therapy creates a highly pro-regenerative microenvironment, ultimately accelerating wound closure by 15-20% compared to monotherapies.
Conclusion
This study introduces a fully PEDOT:PSS-based FDTD that integrates real-time biosensing capabilities and synergistic dual-modality therapy into an all-in-one platform. A novel two-step doping strategy was developed to tailor electrical conductivity (1 S/cm to 6.4 kS/cm) while maintaining exceptional biocompatibility. The modifiable PEDOT:PSS material not only exhibits markedly improved conductivity but also enables the scalable fabrication of multifunctional FDTD dressings that can dynamically monitor key wound biomarkers, including temperature, pH, and impedance. This real-time biosensing capability, coupled with the delivery of synergistic ES-PM intervention, offers a powerful tool for personalized wound management. In vivo studies conducted using SD rats with full-thickness wounds confirmed the FDTD system’s therapeutic efficacy. After 8-day treatment, the EPST group achieved remarkable wound closure rates of 98.8% for square wounds and 99.37% for circular wounds, a significant improvement that outperformed the ES, PM, and control groups. In-depth histological analyses further validated the efficacy of EPST in promoting accelerated wound healing, revealing that the combined treatment significantly enhanced the secretion of key proteins and growth factors, including CD31, EGF, TGF-β, and VEGF. These molecular-level changes observed in the EPST-treated wounds underscore the synergistic effects of ES and PM in promoting angiogenesis, stimulating cell proliferation, and accelerating ECM remodeling. Overall, the modifiable PEDOT:PSS-based FDTD platform uniquely unifies non-invasive, real-time biosensing with targeted, dual-modality therapeutic intervention, paving the way for personalized wound management strategies tailored to individual needs.
Experimental section
Ethics approval
All animal and human participant experiments were conducted in accordance with a standard protocol (1061420210617007) approved by the Ethics Committee of the Animal Experiment Center at the University of Electronic Science and Technology of China.
Fabrication of primary-doped PEDOT:PSS film
PEDOT:PSS (PH1000) was mixed with 6 wt% PTA and stirred until a homogeneous solution was obtained. The mixture was then blade-coated onto UV-treated glass substrates and dried on a hotplate or in an oven at 100 °C until a uniform and smooth film was formed. The free-standing primary-doped PEDOT:PSS film was then peeled off from the glass substrate in a moist environment and transferred onto a PET substrate, which served as the interlayer of the patch. The transferred film was dried at room temperature for 24 h.
Mechanical characterization
The stress-strain curve of the free-standing, humidified primary-doped PEDOT:PSS film was obtained using a tensile testing machine. The Young’s modulus of the film was calculated from the linear region of the stress-strain curve along with the initial length and its cross-sectional area.
Cell counting kit-8 (CCK-8) assay for cell proliferation
The cytotoxicity of FDTD extracts was evaluated using the Cell Counting Kit-8 (CCK-8, US Everbright) based on the proliferation of L929 mouse fibroblast cells. Cells were seeded into 96-well plates and custom-designed devices at an initial density of 2 × 103 cells/well in culture media containing the FDTD extracts. Cell viability was assessed on days 1, 3, and 5. At each time point, the CCK-8 working solution was added and incubated for 2 h. Subsequently, the reaction solution was transferred to a new 96-well plate to eliminate any background interference from the materials. Absorbance was measured at 450 nm using a BioTek microplate reader, and all measurements were performed in triplicate. The results were expressed as the percentage of CCK-8 absorbance relative to the control group, which was normalized to 100%.
Fabrication of modifiable PEDOT:PSS-based patch
The structure of the patch was designed using CAD software, and the primary-doped PEDOT:PSS film was patterned using a laser cutting machine according to the CAD design. A mask was then applied to expose specific electrode regions for secondary doping, and the exposed regions were immersed in a solution of reduced PTA (prepared using PTA, isopropanol, and water, with 250 W UV irradiation). Subsequently, HAuCl4 was applied to the exposed regions, followed by another round of UV irradiation. This process enabled non-invasive, surface-body level, patterned secondary doping, allowing for modifiable conductivity.
In vitro simulation of wound moisture conditions
To simulate the varying moisture levels commonly observed in wound exudate conditions, an in vitro humidity model was established using a sterile polyurethane sponge (5 cm × 5 cm × 0.4 cm, ~10 cm3) as a moisture-retentive substrate. A pair of secondary-doped PEDOT:PSS electrodes (diameter: 5 mm, spacing: 2 cm) was embedded horizontally within the sponge to enable direct-contact measurement. VWC was modulated by injecting sterile 0.9% NaCl solution into the sponge in controlled volumes ranging from 5 mL to 10 mL, corresponding to 50%–100% VWC in 10% increments.
pH sensor fabrication
The pH sensor was prepared using a three-electrode system. Polyaniline (PANI) was polymerized in a 0.1 M aniline/1 M hydrochloric acid solution, with a saturated calomel electrode (SCE) as the reference electrode and platinum (Pt) as the counter electrode. Cyclic voltammetry (CV) was performed at a scan rate of 100 mV/s, cycling the potential between 0 and 0.95 V for 25 cycles.
Animal studies
Six-week-old male Sprague-Dawley (SD) rats (180 ± 20 g) were purchased from Chengdu ENSIWEIER Biotechnology Co., Ltd. (Chengdu, China) for use in this study. All rats were housed under controlled temperature conditions (25 °C) and provided with standard food and water. All animal experiments were conducted in accordance with the approved protocols of the University of Electronic Science and Technology of China (UESTC) (1061420210617007).
Wound healing model preparation
Anesthesia was induced with 2–5% isoflurane and maintained with 2% isoflurane. Under anesthesia, rats were placed in a prone position. The dorsal area of each rat was then shaved using electric clippers, and a depilatory cream was applied uniformly to remove hair. After 5 min, the area was rinsed with PBS solution. Before surgery, the shaved dorsal skin was disinfected with iodine solution and alcohol. Full-thickness wounds of either square (1 cm edge length) or circular (1 cm diameter) shape were created along the dorsal midline of each rat.
H&E staining of skin
Skin tissues from the EPST, ES, and PM treatment groups, along with control group samples, were collected on day 8 for histological analysis. The samples were fixed in 4% paraformaldehyde and sectioned into 3 μm slices for subsequent H&E staining. The staining process involved sequentially exposing the sections to xylene, absolute ethanol, and a gradient of alcohol solutions to ensure complete dehydration, followed by rinsing in distilled water. Hematoxylin staining was performed to visualize nuclei, followed by differentiation using hydrochloric acid-ethanol. After additional rinsing to remove excess stains, the sections underwent dehydration with graded ethanol and xylene. The slides were then neutralized, mounted with a resin sealant, and dried. An inverted optical microscope was used to observe the stained sections and evaluate structural differences among the groups.
Masson’s trichrome staining of skin
To evaluate collagen deposition and tissue remodeling, the sections were processed using Masson’s trichrome staining. Similar to the H&E staining protocol, the sections were deparaffinized and rehydrated through xylene and graded ethanol. The slides were first stained with Weigert’s iron hematoxylin to highlight cell nuclei, followed by differentiation in hydrochloric acid-ethanol to enhance contrast. After thorough washing, the blue coloration was restored. The samples were subsequently stained with acidic fuchsin to identify cytoplasm and muscle fibers, treated with phosphomolybdic acid to prepare for selective collagen staining, and counterstained with aniline blue. After a final treatment with glacial acetic acid to stabilize the colors, the sections were dehydrated, sealed with resin, and examined microscopically to assess the extent of collagen fiber distribution and tissue repair across the experimental groups.
IHC staining
Paraffin-embedded tissue sections were first deparaffinized and rehydrated by sequential immersion in xylene, followed by graded ethanol solutions, and finally rinsed in distilled water. Antigen retrieval was performed by incubating the sections in 3% hydrogen peroxide to quench endogenous peroxidase activity, followed by heating in a microwave using a citric acid buffer until boiling. After allowing the slides to cool naturally, they were washed with PBS. Nonspecific binding was blocked by applying BSA evenly over the tissue sections at room temperature. The sections were then incubated with the primary antibody, followed by the appropriate secondary antibody, and the antigen-antibody complexes were visualized using DAB chromogen. Subsequently, the sections were counterstained with Harris hematoxylin for approximately 3 min. The protocol was finalized with differentiation in acid alcohol, dehydration, clearing, mounting, and microscopic examination.
IFC staining
For IFC staining, tissue sections underwent deparaffinization, antigen retrieval, and blocking following the same procedure as described for IHC. After these preparatory steps, the sections were incubated with the primary antibody, followed by incubation with the corresponding fluorescently labeled secondary antibody. Nuclear counterstaining was achieved using DAPI, and the slides were mounted using an appropriate mounting medium. The stained sections were imaged using a Nikon A1 confocal microscope, and subsequent quantitative analysis was performed using ImageJ software.
Data availability
The authors declare that all data supporting the findings of this study are available within the Article and its Supporting Information.
References
Falanga, V. et al. Chronic wounds. Nat. Rev. Dis. Prim. 8, 50 (2022).
Sen, C. K. Human wounds and its burden: an updated compendium of estimates. Adv. Wound Care 8, 39–48 (2019).
Olsson, M. et al. The humanistic and economic burden of chronic wounds: a systematic review. Wound Repair Regen. 27, 114–125 (2019).
Frykberg, R. G. & Banks, J. Challenges in the treatment of chronic wounds. Adv. Wound Care 4, 560–582 (2015).
Fierheller, M. & Sibbald, R. G. A clinical investigation into the relationship between increased periwound skin temperature and local wound infection in patients with chronic leg ulcers. Adv. Ski. Wound Care 23, 369–379 (2010).
Chanmugam, A. et al. Relative temperature maximum in wound infection and inflammation as compared with a control subject using long-wave infrared thermography. Adv. Ski. Wound Care 30, 406–414 (2017).
Pei, X. et al. Flexible wireless skin impedance sensing system for wound healing assessment. Vacuum 168, 108808 (2019).
Antoszewska, M., Spychalski, P., Kekonen, A., Viik, J. & Baranska-Rybak, W. Bioimpedance sensor array for monitoring chronic wounds: validation of method feasibility. Int. Wound J. 21, e14899 (2024).
Swisher, S. L. et al. Impedance sensing device enables early detection of pressure ulcers in vivo. Nat. Commun. 6, 6575 (2015).
Mariani, F. et al. Advanced wound dressing for real-time PH monitoring. ACS Sens. 6, 2366–2377 (2021).
Sim, P., Strudwick, X. L., Song, Y., Cowin, A. J. & Garg, S. Influence of acidic PH on wound healing in vivo: a novel perspective for wound treatment. Int. J. Mol. Sci. 23, 13655 (2022).
de Freitas, L. F. & Hamblin, M. R. Proposed mechanisms of photobiomodulation or low-level light therapy. IEEE J. Sel. Top. Quantum Electron. 22, 348–364 (2016).
Shimada, S. et al. Complex structure of cytochrome c-cytochrome c oxidase reveals a novel protein-protein interaction mode. EMBO J. 36, 291–300 (2017).
Luo, R., Dai, J., Zhang, J. & Li, Z. Accelerated skin wound healing by electrical stimulation. Adv. Healthc. Mater. 10, 2100557 (2021).
Shirzaei Sani, E. et al. A stretchable wireless wearable bioelectronic system for multiplexed monitoring and combination treatment of infected chronic wounds. Sci. Adv. 9, eadf7388 (2023).
Pang, Q. et al. Smart flexible electronics-integrated wound dressing for real-time monitoring and on-demand treatment of infected wounds. Adv. Sci. 7, 1902673 (2020).
Farahani, M. & Shafiee, A. Wound healing: from passive to smart dressings. Adv. Healthc. Mater. 10, 2100477 (2021).
Zhao, W., Wang, Y., Li, R., Liu, X. & Huang, W. Stretchable wireless optoelectronic synergistic patches for effective wound healing. npj Flex. Electron. 8, 77 (2024).
Yao, G. et al. A programmable and skin temperature-activated electromechanical synergistic dressing for effective wound healing. Sci. Adv. 8, eabl8379 (2022).
Thyssen, J. P. & Menné, T. Metal allergy-a review on exposures, penetration, genetics, prevalence, and clinical implications. Chem. Res. Toxicol. 23, 309–318 (2010).
Büdinger, L., Hertl, M. & Büdinger, L. Immunologic mechanisms in hypersensitivity reactions to metal ions: an overview. Allergy 55, 108–115 (2000).
Bhattacharya, S. et al. A chest-conformable, wireless electro-mechanical e-tattoo for measuring multiple cardiac time intervals. Adv. Electron. Mater. 9, 202201284 (2023).
Fan, J. A. et al. Fractal design concepts for stretchable electronics. Nat. Commun. 5, 3266 (2014).
Huang, Y., Tang, L. & Jiang, Y. Chemical strategies of tailoring PEDOT:PSS for bioelectronic applications: synthesis, processing and device fabrication. CCS Chem. 6, 1844–1867 (2024).
Jeong, J.-W. et al. Soft materials in neuroengineering for hard problems in neuroscience. Neuron 86, 175–186 (2015).
Banik, O., Salve, A. L., Kumar, P., Kumar, S. & Banoth, E. Electrically conductive nanomaterials: transformative applications in biomedical engineering—a review. Nanotechnology 36, 022001 (2024).
Cho, K. W. et al. Soft bioelectronics based on nanomaterials. Chem. Rev. 122, 5068–5143 (2021).
Kim, T., Cho, M. & Yu, K. J. Flexible and stretchable bio-integrated electronics based on carbon nanotube and graphene. Materials 11, 1163 (2018).
Jain, N. & Tiwari, S. Biomedical application of carbon nanotubes (CNTs) in vulnerable parts of the body and its toxicity study: a state-of-the-art-review. Mater. Today Proc. 46, 7608–7617 (2021).
Ali, A. et al. Recent advancements in MXene-based biosensors for health and environmental applications-a review. Biosensors 14, 497 (2024).
Yao, G., Li, P., Liu, M., Liao, F. & Lin, Y. Smart contact lenses: catalysts for science fiction becoming reality. Innovation 5, 100710 (2024).
Gan, X. et al. Closed-eye intraocular pressure and eye movement monitoring via a stretchable bimodal contact lens. Microsyst. Nanoengineering 11, 83 (2025).
Zhou, C. et al. Modulus-adjustable and mechanically adaptive dry microneedle electrodes for personalized electrophysiological recording. npj Flex. Electron. 9, 77 (2025).
Li, P. et al. Implantable magnetoelectric bioelectronics for wireless diagnosis and therapy. eScience 100483 (2025).
Dong, Q. et al. A stretchable and transparent electrode for visual electrophysiological acquisition. Biosensors 15, 701–701 (2025).
Lang, U., Naujoks, N. & Dual, J. Mechanical characterization of PEDOT:PSS thin films. Synth. Met. 159, 473–479 (2009).
Tahk, D., Lee, H. H. & Khang, D.-Y. Elastic moduli of organic electronic materials by the buckling method. Macromolecules 42, 7079–7083 (2009).
Chen, H. et al. Highly conductive, ultrastrong, and flexible wet-spun PEDOT:PSS/ionic liquid fibers for wearable electronics. ACS Appl. Mater. Interfaces 15, 20346–20357 (2023).
Yang, Y., Deng, H. & Fu, Q. Recent progress on PEDOT:PSS based polymer blends and composites for flexible electronics and thermoelectric devices. Mater. Chem. Front. 4, 3130–3152 (2020).
Xu, R. et al. Controlled water vapor transmission rate promotes wound-healing via wound re-epithelialization and contraction enhancement. Sci. Rep. 6, 24596 (2016).
Yousefian, H. et al. Solvent-doped PEDOT:PSS: structural transformations towards enhanced electrical conductivity and transferable electromagnetic shields. Surf. Interfaces 51, 104481 (2024).
Keshmiri, N., Sambyal, P., Najmi, P., Milani, A. S. & Arjmand, M. Stretchable water - repellent PEDOT:PSS - impregnated polyurethane nanofiber mats for electromagnetic interference shielding. Small 21, 2500723 (2025).
Chen, J.-S. et al. Phosphotungstic acid as a novel acidic catalyst for carbohydrate protection and glycosylation. RSC Adv. 9, 33853–33862 (2019).
Li, M. et al. Highly stable phosphotungstic acid/Au dual doped carbon nanotube transparent conductive films for transparent flexible heaters. Carbon 2023, 207, 219–229 (2023).
Li, Z. et al. Continuous PEDOT:PSS nanomesh film: towards aqueous AC line filtering capacitor with ultrahigh energy density. Chem. Eng. J. 430, 133012 (2022).
Shahrim, N. A., Ahmad, Z., Wong Azman, A., Fachmi Buys, Y. & Sarifuddin, N. Mechanisms for doped PEDOT:PSS electrical conductivity improvement. Mater. Adv. 2, 7118–7138 (2021).
Che, X. et al. Highly conductive broadband transparent DMSO-Doped PEDOT: PSS electrodes. Opt. Lett. 49, 7000 (2024).
Wei, T.-C., Chen, S.-H. & Chen, C.-Y. Highly conductive PEDOT:PSS film made with ethylene-glycol addition and heated-stir treatment for enhanced photovoltaic performances. Mater. Chem. Front. 4, 3302–3309 (2020).
Wang, X. et al. Photolithographic high-conductivity transparent conformal RGO/PEDOT:PSS electrodes for flexible skin-like all solution-processed organic transistors. Adv. Mater. Technol. 7, 202200660 (2022).
Huang, J., Liu, X. & Du, Y. Fabrication of free-standing flexible and highly efficient carbon nanotube film/PEDOT: PSS thermoelectric composites. J. Materiomics 8, 1213–1217 (2022).
Song, J. W. et al. Bioresorbable, wireless, and battery-free system for electrotherapy and impedance sensing at wound sites. Sci. Adv. 9, ade4687 (2023).
Lu, S.-H. et al. Multimodal sensing and therapeutic systems for wound healing and management: a review. Sens. Actuators Rep. 2022, 4, 100075 (2022).
Bandodkar, A. J. et al. Tattoo-based potentiometric ion-selective sensors for epidermal PH monitoring. Analyst 138, 123–128 (2013).
Shin, Y. et al. Functional-hydrogel-based electronic-skin patch for accelerated healing and monitoring of skin wounds. Biomaterials 314, 122802 (2025).
Jiang, Y. et al. Wireless, closed-loop, smart bandage with integrated sensors and stimulators for advanced wound care and accelerated healing. Nat. Biotechnol. 41, 652–662 (2023).
Lee, S. Y. et al. Combinatorial wound healing therapy using adhesive nanofibrous membrane equippedwith wearable LED patches for photobiomodulation. Sci. Adv. 8, abn1646 (2022).
Fushimi, T. et al. Green light emitting diodes accelerate wound healing: characterization of the effect and its molecular basis in vitro and in vivo. Wound Repair Regen. 20, 226–235 (2012).
Liang, Y. et al. Application of stable continuous external electric field promotes wound healing in pig wound model. Bioelectrochemistry 135, 107578 (2020).
Zhang, C. et al. Biodegradable hydrogels with photodynamic antibacterial activity promote wound healing and mitigate scar formation. Biomater. Sci. 11, 288–297 (2022).
Jeong, S.-H. et al. Accelerated wound healing with an ionic patch assisted by a triboelectric nanogenerator. Nano Energy 2021, 79, 105463 (2021).
Lin, F. et al. Lymphocyte electrotaxis in vitro and in vivo. J. Immunol. 181, 2465–2471 (2008).
Zhao, M. et al. Electrical signals control wound healing through phosphatidylinositol-3-OH kinase-gamma and PTEN. Nature 442, 457–460 (2006).
Katoh, K. Effects of electrical stimulation of the cell: wound healing, cell proliferation, apoptosis, and signal transduction. Med. Sci. 11, 11 (2023).
Leyane, T. S., Jere, S. W. & Houreld, N. N. Cellular signalling and photobiomodulation in chronic wound repair. Int. J. Mol. Sci. 22, 11223 (2021).
Acknowledgements
This work was supported by the National Natural Science Foundation of China under grant numbers U21A20460 (Y.L.), 62422104 (G.Y.), 62427806(Y.L.), 62371115 (G.Y.), 52021001 (Y.L.); Science and Technology Major Project of Tibetan Autonomous Region of China under grant no. XZ202201ZD0001G (G.Y.); Science and Technology Department of Sichuan Province under grant no. 2024NSFSC0234 (G.Y.); and the Medico-Engineering Cooperation Funds, Fundamental Research Funds for the Central Universities, UESTC under grant nos. ZYGX2025YGLH006 (G.Y.), ZYGX2020ZB041 (G.Y.), ZYGX2021YGLH002 (G.Y.).
Author information
Authors and Affiliations
Contributions
G.Y. and L.W. conceived the concept. G.Y. and L.W. discussed and finalized the project plan. Y.L. supervised the research and provided lab assistance. L.W., S.C., and X.G. performed the experiments and generated data in all figures. L.W., S.C., X.G., Y.G., X.R., C.Z., T.P., M.G., and Y.L. analyzed the data. L.W. and G.Y. wrote the manuscript. B.J., Z.Y., J.Z., and Z.H. contributed to scientific discussion and provided critical feedback during manuscript preparation. All authors reviewed and provided constructive feedback on the manuscript.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Wang, L., Yao, G., Cai, S. et al. Modifiable PEDOT:PSS-based flexible diagnostic and therapeutic dressings for personalized wound management. Microsyst Nanoeng 12, 148 (2026). https://doi.org/10.1038/s41378-026-01200-9
Received:
Revised:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41378-026-01200-9
