
Abstract
The transition from Child and Adolescent (CAMHS) to Adult Mental Health Services (AMHS) can be challenging. Drawing on the sample of the European MILESTONE project, we explored changes in clinical profiles and treatment outcomes in adolescents transitioning to AMHS over two years, focusing on different pharmacological treatment patterns. The sample (N = 690; mean age: 17.7 years; SD = 0.29) was categorised into three groups based on medication patterns: continuous (Group 1), intermittent (Group 2), and never medicated (Group 3). Participants underwent four evaluations over two years using tools measuring psychopathology and functioning, including the Health of the Nation Outcome Scale for Child and Adolescents (HoNOSCA) and ASEBA Battery. We employed repeated-measures models to analyse clinical rating changes and a two-way mixed ANOVA to assess interaction between time and groups. Group 3 had significantly lower mean HoNOSCA ratings than Groups 1 and 2 (p < 0.001), indicating better mental health. By the last time point (T4), the factors associated with a reduced risk of severe illness included an improvement in the risk of suicide attempts (p = 0.038), enhanced everyday functional skills (p = 0.008), higher quality of life (p = 0.001), and being male (p = 0.020). The ASEBA Battery showed Group 1 had more internalising symptoms, while Group 2 had more externalising symptoms than Group 3. During the transition from CAMHS to AMHS, continuous medication was associated with higher symptom severity than intermittent or no pharmacological treatment. This may reflect either a more severe initial symptomatology requiring sustained pharmacotherapy or a medication-related paradox, whereby symptoms persist or intensify owing to treatment resistance or side effects.
Trial registration
“MILESTONE study” registration: ISRCTN ISRCTN83240263 Registered 23 July 2015; ClinicalTrials.gov NCT03013595 Registered 6 January 2017.
Similar content being viewed by others
Background
Adolescence is a period of increased susceptibility to mental health challenges owing to significant physical, emotional, and social changes [1]. Hormonal fluctuations, ongoing brain maturation [2], and external stressors such as academic demands and the search for social identity influence this vulnerability [3, 4]. In addition, individual traits, family dynamics, and social interactions can affect the mental well-being of young people. Factors such as low self-esteem, challenging family circumstances, and peer victimisation may lead to depression, anxiety, and behavioural problems [5]. A meta-analysis showed a rising prevalence of mental disorders among young people in Europe; almost one in five young people in Europe was found to suffer from mental disorders, with a pooled prevalence rate of 15.5% in 14 European countries [6]. Other epidemiological investigations have indicated that approximately 14% of individuals aged 10-19 experience such conditions during this phase of life [7,8,9,10], which can significantly affect functioning in later life [11]. Although the median age of onset for many disorders in males and females is similar, there are significant sex differences in the lifetime prevalence of mental disorders [12]. Anxiety and major depressive disorders are more commonly experienced in female population, while impulse control and substance use disorders are more prevalent in male population. [13].
In recent decades there has been a corresponding global increase in the prescription of psychotropic medications for children and adolescents [14], but changes in physical development during childhood and adolescence may contribute to suboptimal treatment effectiveness and tolerability in young individuals. This may lead to unexpected outcomes in the young population [15]. For young people facing transition from Child and Adolescent Mental Health Services (CAMHS) to Adult Mental Health Services (AMHS), ensuring seamless continuity of care and pharmacological treatment for those in need is important but can be challenging. This phase occurs during a vulnerable period and is compounded by existing mental health challenges [16, 17]. Adolescents taking psychotropic medications may require treatment adjustments during this transition, whereas those not taking such medications tend to have higher dropout rates [18]. Close collaboration between CAMHS and AMHS professionals is essential to ensure continuity of care and address changing medication needs and/or potential side effects. Ineffective transition management can lead to care disruptions, treatment gaps, and an increased risk of relapse or mental health deterioration.
To explore and address the treatment gaps that occur during transition, we conducted a cluster randomised controlled trial (cRCT) of Managed Transition with a parallel longitudinal cohort study (together called the “MILESTONE study”) as part of the wider the MILESTONE project (2014–2019) [19]. The aim of the project was to improve the understanding and strengthen transitional care processes from CAMHS to AMHS across European healthcare systems. This study was a secondary analysis of the longitudinal MILESTONE study data which aimed to explore clinical profile changes in adolescents transitioning from CAMHS to AMHS over a two-year follow-up. The aim of this study was to examine mental health trajectories and treatment outcomes in young people with different medication regimes. We achieved this by examining how sociodemographic factors interact with psychopathological severity beyond single diagnostic categories and using a comprehensive evaluation method integrating patient self-reports and clinician-rated reports.
Method
Study design and participants
The MILESTONE study was designed to investigate service utilisation, mental health, and additional outcomes during a 2-year monitoring period among a group of 1004 young individuals aged 17-19 who have reached the upper age limit of their CAMHS across eight European countries.
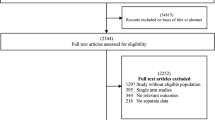
Previous studies have described their study design and recruitment procedures in detail [19]. In the present study, we focused on analysing data from all participants (N = 1004). Participants who did not report any information regarding psychopharmacological treatment were excluded from this study (Fig. 1S): finally, data from 690 individuals, including both males and females, were analysed. Participants were eligible if they met the following criteria: (i) they were CAMHS users and were within one year of the upper age limit (almost 18 years old), or were up to three months older (mean = 17.68; SD = 0.29) if they were still under CAMHS care during the study period; (ii) they had a documented psychiatric diagnosis or regularly attended CAMHS; (iii) they had an IQ of more than 70 or showed no evidence of intellectual impairment, as determined by clinician assessment or previous diagnosis, and (iv) were able to complete all required assessments. The sample size was estimated for three groups assessed at four time points over a 24-month period. This estimation focused on the change from baseline to 24 months across three clinical scales: HoNOSCA, ASEBA Internalizing, and ASEBA Externalizing, which were identified as the primary outcomes.
Assuming a within-subject correlation of approximately 0.6, with baseline standard deviations ranging from 8–10 points and a small to moderate group effect (Cohen’s f ≈ 0.12), the required sample size was calculated using an ANOVA framework based on change scores. The goal was to achieve 80% power with a significance level of α = 0.05.
After applying Bonferroni correction for the three endpoints and accounting for an anticipated 20% attrition rate, the final required sample size was approximately 153 participants per group.
Measures, procedures, and variables
Participants took part in four assessments over a 24-month follow-up period: 3 months before transitioning from CAMHS to AHMS (T1), 9 months after T1 (T2), 15 months after T1 (T3), and 24 months after T1 (T4). At T1, all patients received CAMHS treatment. Following obteined informed consent, participants and parents took part in a baseline assessment (T1) in CAMHS approximately six months before reaching the upper age limit. Trained researchers gathered sociodemographic data and assessed care needs via interviews conducted at CAMHS, at home, or by telephone, accommodating the participants’ preferences. Sociodemographic information was sourced from clinicians, parents, medical files, and online questionnaires were accessed via HealthTracker™ (https://www.healthtracker.co.uk).
The assessment battery administered included (see Table 2S): (1) HoNOSCA (Range 0-52) [20, 21], used to assess the need for care based on a wide range of problems (behaviour, impairment, symptoms, and social functioning); it was filled through semi-structured interviews with the young person, and (where possible) with parent/caregiver and the relevant clinician (or review of medical records if the relevant clinician was unavailable); (2) ASEBA battery [22, 23], including Youth Self Report (YSR) or Adult Self Report (ASR), and the parent/caregiver-reported Child Behaviour Checklist (CBCL) or Adult Behaviour Checklist (ABCL) to assess dimensions of emotional and behavioural problems; (3) Specific Levels of Functioning Scale (SLOF) (Range 43–125) [24, 25], a parent-reported measure used to assess levels of functioning of the young person from the parent/caregiver’s perspective (4) Life events questionnaire (Range 0-13), an ad hoc tool specifically developed within the MILESTONE project, administered to patients and used to assess significant life events, such as accidents, deaths in the family, separation and job loss of the parent/caregiver; (5) World Health Organization Quality of Life Brief (WHOQOL-Bref) (Range 0–100) [26], administered to patients to assess quality of life and covering physical and psychological health, social relationships, and the current environment of the young patients; (6) Bullying, adapted from Retrospective Bullying and Friendship Interview Schedule, a patient-completed questionnaire used to assess the experiences with bullying in different settings (e.g., at school, home, and college) [27]; (7) Clinical Global Impression - Severity scale (CGI-S) (Range 1-7) rated by the clinician and used to assess the severity of the patient’s illness at the time of assessment [28]. Information regarding psychopharmacological treatment were collected using from the clinician, from clinical documentation and directly from patients using a form created ad hoc: whenever there was a disagreement between these three sources of information, we retained the information provided by the clinician.
To assess the link between psychotropic prescriptions and patients’ clinical course, we categorised our sample into three groups: (i) ‘continuous medication,’ comprising patients prescribed at least one psychotropic medication across all four time points; (ii) ‘intermittent medication,’ including patients prescribed at least one psychotropic medication at any time points; and (iii) ‘never medicated,’ consisting of patients never prescribed psychotropic medications throughout the four time points.
Statistical analysis
Continuous variables were compared between the three psychotropic medication groups using t-tests, while categorical variables were assessed using the χ2 test. As mentioned previously, we selected patients from the entire sample (N = 1004) with available psychotropic medication data (including those who declared that they weren’t receiving medications) at all four time points (N = 690). See Table 1S for the characteristics of the excluded sample. To address missing clinical scores (HoNOSCA and ASEBA), we used multiple imputations [29] across all four time points to identify temporal patterns before fitting the mixed models. We used logistic regression analysis with a binomial family at the final time point to assess the association between sociodemographic variables and the clinical course/outcomes across the three psychotropic medication groups. The CGI-S, which assesses the severity of symptoms, dichotomised patients into no/mild severity (0-1-2-3) and moderate/severe severity (4-5-6-7) groups. Patients who had experienced bullying at least once were classified as victims; if they have experienced both, bullying and being a victim, they were labelled as bullies. General health and social functioning over the four time points were evaluated using HoNOSCA total ratings, while emotional and behavioural problems were assessed using ASEBA battery ratings from patients and parents. First, we employed repeated-measures models with to assess the interaction effect between time and psychotropic medication groups, accounting for the random effects of each subject and of each country. Finally, we conducted a two-way ANOVA to explore the interaction between time point and the type of assessment. Analyses were conducted using R software version 4.3.2 with a significance threshold of 0.05. The code used for the analyses is available from the corresponding author upon reasonable request.
Results
Sociodemographic and clinical characteristics of participants
Table 1 shows the sociodemographic characteristics of the 690 adolescent patients from the 9 centres in eight European countries. The sample had a mean age of 17.7 years (SD = 0.29), with over 80.0% Caucasians and 64.1% women. In terms of household composition, 55.9% of adolescents lived with their biological parents, 7.5% lived with a single parent, and only 33.3% had other living arrangements (including foster care or residential facilities). Almost 70% of the participants did not attend school or university at the time of recruitment, whereas 5.8% were currently enrolled in school.
Sociodemographic and clinical associations among the three psychotropic medication groups
Table 2 shows the clinical characteristics of the patients. Across all three groups, most participants were rated as “borderline/mildly/moderately ill” on the CGI-S (58.1% in Group 1, 58.9% in Group 2, and 62.5% in Group 3), with a smaller proportion rated as “not at all ill” (8.1% in Group 1, 5.9% in Group 2, and 14.5% in Group 3). There was significant difference between the groups (p = 0.018). Group 3 had a significantly lower mean HoNOSCA score (9.3) than Groups 1 (13.9) and 2 (12.8) (p < 0.001), indicating better mental health. Group 3 also had a lower percentage (17.0%) of participants with a lifetime history of suicide attempts than Groups 1 (30.1%) and 2 (29.6%). Significant differences (p < 0.001) were observed between these groups in the proportion of participants with one or more suicide attempts. Concerning non-accidental self-injury (HoNOSCA domain), most participants across all three groups had “no problem of this kind” (67.2% in Group 1, 66.8% in Group 2, and 81.5% in Group 3). The groups differed significantly in the proportion of participants with varying degrees of self-injury and suicidal intent (p < 0.001).
There were significant differences in the overall quality of life scores rated with the WHOQOL-BREF (p < 0.001) among the three groups (79.2 for Group1, 77.9 for Group2, and 80.2 for Group3). Significant differences were found among the three groups in any functional skill domain or total SLOF score (p < 0.001), and the same applies to the mean number of life events among the three groups (183.5 for Group1, 188.8 for Group2, and 192.5 for Group3). The proportion of participants involved in bullying incidents differed significantly between the three medication groups (p < 0.001). In summary, Group 3 generally showed better mental health outcomes, with lower psychopathology severity, fewer suicide attempts, and better social quality of life than Groups 1 and 2.
Table 3 presents the distribution of psychotropic prescriptions at baseline and T4, distinguishing between continuously medicated patients and intermittently medicated patients. Most continuously medicated patients received only one medication. Antidepressants were the most common, prescribed to 63.9% of patients at T1 and 58.1% at T4. Second-generation antipsychotics were used by 31.7% at T1 and 32.3% at T4, while benzodiazepine use dropped from 9.1% at baseline to 4.3% at T4. Among intermittently medicated patients, the proportion using each drug class was significantly lower than in continuously medicated individuals. For instance, antidepressant prescriptions fell from 35.9% at T1 to 11.8% at T4, and second-generation antipsychotics dropped from 15.5%–3.6%. The average number of psychotropic medications per patient in this group also decreased from 0.9 at T1 to 0.4 at T4. In the intermittent group, 133 patients (43.7%) received medication at one time point, with 75 patients (24.7%) treated only at T1. Additionally, 89 patients (29.3%) were treated at two timepoints, while 82 patients (27.0%) received treatment at three time points during the observation period.
Figures S5 and S6 illustrate the number of medications administered at each time point for the continuously and intermittently medicated groups, respectively. The distribution of the number of medications prescribed at each time point, including counts and percentages for both groups, is detailed in Table 5S. Table 6S shows the patterns of medication prescriptions for each class considered at each time point.
The logistic regression model shows that several factors were associated with the risk of severe disorder assessed at the last time point (T4). An improvement in the risk of suicide attempts (p = 0.038), higher everyday functional skills (p = 0.008), higher quality of life (p = 0.001) and being male (p = 0.020) were associated to a reduced risk of severe illness. In addition, continuous medication status (0.051) was marginally associated with a higher risk of severe illness, suggesting that those on continuous medication may face a higher risk. The effects of being a victim of bullying were not found to be statistically significant.
Course and outcomes of adolescents rated with HoNOSCA
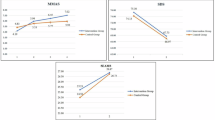
Figure 1 displays the patient- and clinician-rated HoNOSCA ratings across the three medication profiles (e.g., continuous medication, intermittent medication, and never medicated). This analysis revealed associations between patient and clinician assessments across various medication regimens over time. However, there were notable differences in rating magnitudes. In both self-administered and clinician-reported assessments, never-medicated patients showed significantly different ratings compared to patients in the continuous medication group. For the self-administered reports, differences were particularly evident at T3 (p = 0.001) and T4 (p < 0.001). Similarly, for the clinician reports, significant differences were observed at T3 (p = 0.001) and T4 (p < 0.001). Additionally, investigators rate symptom severity were higher than patients’ self-assessments. However, the difference between the self- and clinician-assessed ratings varied significantly across the three psychotropic medication profiles (p < 0.001; for further information, see Fig. S2 in the Supplementary Material).

Honosca total ratings: patients’ vs. clinicians’ ratings by medication status.
Course and outcomes of adolescents rated with ASEBA Battery
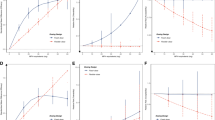
Figure 2 shows the analysis of the internalising and externalising domains based on medication status, comparing self-reported (ASR and YSR scores) with parental reports (CBCL and ABCL scores). Regarding internalising factors, there was a distinct trend: patients who never had never been medicated exhibited the lowest ratings, suggesting fewer internalising symptoms, followed by those with an intermittent medication status. Patients taking continuous medication had the highest ratings, indicating more internalising symptoms. This pattern revealed a significant association between medication status and internalising domains, with statistically significant changes across the three medication profiles and over the four time points (p < 0.001) for both patient and parent ratings. In both self- and parent-reported assessments, never-medicated patients showed significantly different ratings compared to patients in the continuous medication group. For self-reports, significant differences were observed at T1 (p = 0.002), T2 (p = 0.001), T3 (p = 0.016), and T4 (p < 0.001). For parent reports, significant differences were found at T1 (p < 0.001), T2 (p < 0.001), T3 (p < 0.001), and T4 (p < 0.001). However, the difference between self- and parent-assessed ratings did vary significantly across the three psychotropic medication profiles (p = 0.007; for further information, see Fig. S3 in Supplementary Material).

Internalising and externalising domains: self-report (asr + ysr) vs. parent-report (cbcl + abcl) ratings by medication status.
For the externalising domain based on medication status, the data show a clear trend: patients who had never been medicated displayed the lowest scores, indicating fewer externalising symptoms. Those with intermittent medication status had moderately higher scores, and those on continuous medication exhibited the highest scores, suggesting more reported externalising symptoms. This trend underscores that medication status is significantly associated with externalising factors, as measured by both self-report (ASR and YSR) and parent-report (CBCL and ABCL) assessments. Notably, while statistically significant changes across the three medication profiles and the four time points were observed in both self-report (p = 0.027) and parent-report assessments (p < 0.001), the pattern and magnitude of these changes differed, highlighting a discrepancy in the perception of externalising behaviours between adolescents and their caregivers. According to the parents’ ratings, never-medicated patients showed significantly different ratings compared to patients in the continuous medication group, especially at T1 and T4 (p = 0.034 vs p = 0.019, and p = 0.002 vs p = 0.135, respectively). Additionally, the difference between the self-assessed and parent-assessed ratings varied significantly across the medication regimens (p = 0.038; for further information, see Fig. S4 in the Supplementary Material).
Correlation between self-reported and observer-reported assessments
Table 3S presents the correlation coefficients between the self- and observer-reported assessments across various time points. When patients and clinicians were compared using the HoNOSCA Total Rating, the overall correlation coefficient was 0.589, indicating a moderate level of association. The correlations at each time point were consistent, ranging from 0.508 at T1 to 0.626 at T4. Regarding internalising factors, the correlation between self-reports (ASR + YSR) and parental reports (CBCL + ABCL) was moderate, with an overall correlation coefficient of 0.605. However, there was an increasing trend in the association over time, starting at 0.576 at T1 to 0.635 at T4. For externalising factors, the correlation between self-reports and parental reports was moderate overall (0.545); however, the association decreased over time, with correlations ranging from 0.563 at T1 to 0.511 at T4. All correlation coefficients were statistically significant (p < 0.001), indicating robust relationships between self- and observer-reported assessments across all measures and time points [30].
Discussion
As part of the broader MILESTONE project, this study offers a nuanced exploration of clinical trajectories and outcomes among adolescents, aged 17-19, with mental disorders undergoing various medication regimens over two years. Using the wealth of MILESTONE study data and by categorising adolescents into continuous, intermittent, and never medicated groups, we created a comprehensive framework for analysing the association between medication patterns and clinical outcomes. Our results suggest a complex relationship between medication regimens and changes in mental health symptoms, as measured by assessment tools such as the HoNOSCA, YSR, ASR, CBCL, and ABCL. Continuous medication was associated with higher symptom severity scores than intermittent or no medication, possibly reflecting either a more severe initial symptomatology requiring sustained pharmacological treatment or a medication-related paradox, where symptoms persist or intensify despite ongoing treatment due to issues such as treatment resistance or side effects [31].
While the existing literature provides valuable insights into the prevalence and correlates of psychotropic medication use among adolescents with mental disorders, several notable gaps remain. The studies conducted by Olfson et al. [32], Altuwairqi et al. [33], Goodwin et al. [34], and Brown et al. [35] have contributed to our understanding of medication prescribing patterns, prevalence trends, sociodemographic characteristics, and their associations with adverse outcomes. However, these studies primarily offer cross-sectional snapshots or systematic reviews and often lack longitudinal perspectives and detailed assessments of clinical profiles. In Italy, Clavenna et al. [36] conducted an epidemiological study to estimate the treatment coverage for mental disorders in paediatric patients. In this survey involving 59,987 young people in the Lombardy Region, 37.1% had attended CAMHS at least once, 2.2% had been hospitalised, and 1.7% had received at least one prescription for psychotropic drugs. Among all users, 23.1% had disorders requiring a high level of care, such as recurrent drug prescriptions and inpatient treatments.
Discrepancies between patient and clinician assessments, particularly instances in which patients reported greater symptom decreases than clinicians, highlight the subjective nature of symptom changes and may indicate clinicians’ cautious perspectives or possible underestimation of patient-reported improvements. Recognising these differences in clinical practice is essential to enhance communication and treatment planning [37,38,39]. Our findings emphasise the importance of considering psychosocial dimensions in mental health trajectories. Adolescents with mental health conditions navigate through complex social environments that can exacerbate or alleviate their symptoms. Factors such as family dynamics, bullying experiences, and major life events play critical roles and were considered in this study. For example, the prevalence of bullying and its correlation with worse mental health outcomes underscores the need for robust support systems in educational and community settings to mitigate these impacts [40, 41].
Service transitions and treatment continuity
The transition from CAMHS to AMHS emerged as a critical period, laden with potential disruptions in care continuity. Adolescents undergoing this transition are particularly vulnerable and often experience significant shifts in their support systems and care protocols. Our data reflect this transitional turbulence, with some participants showing unexpected spikes in symptom severity scores at the final assessment points. This phenomenon may be attributed to the challenges of adjusting to new care settings, differences in treatment approaches between paediatric and adult services, or gaps in service provision [42,43,44].
Limitations
The MILESTONE cohort study had several limitations. The most important limitation was the potential selection bias, as CAMHS were affiliated with the MILESTONE consortium and were not randomly selected. The missing data analysis showed a potential bias, with more missing parental information in young people with severe diagnosis. A common limitation of studies on medication prescriptions is the lack of adherence data: we gathered details on prescribed medications, recipients, and timing but could not confirm if patients took the medications as prescribed. This does not affect the never medicated group; however, for the intermittently and continuously medicated groups, adherence cannot be verified. Despite this, the distinct clinical profiles and changes observed over time suggest that most patients were likely to adhere to their treatment plans.
Conclusions
This study examined the association of different medication regimens with the clinical trajectories of adolescents with mental disorders. Through a better understanding of treatment adherence, symptomatology, and critical transition periods, we can develop more effective approaches to support young people facing psychological problems. Longitudinal studies of adolescents undergoing pharmacological treatment face challenges, including ethical considerations and distinguishing treatment effects from natural development. An accurate diagnosis is crucial because the symptoms overlap with typical adolescent behaviours. Further research is needed to understand developmental trajectories, symptom progression, and treatment variations, while we also comply with necessary ethical standards. Our study aimed to fill the gaps in the literature using a unique dataset from a European sample to inform clinical practice and policy decisions regarding adolescent mental health management.
Data availability
The data that support the findings of this study are available from the corresponding author upon reasonable request.
References
Blakemore SJ. Adolescence and mental health. Lancet. 2019;393:2030–1.
Galván A. Adolescence, brain maturation and mental health. Nat Neurosci. 2017;20:503–4.
MacLeod KB, Brownlie EB. Mental health and transitions from adolescence to emerging adulthood: developmental and diversity considerations. Can J Community Ment Health. 2014;33:77–86.
Blakemore SJ, Mills KL. Is adolescence a sensitive period for sociocultural processing? Annu Rev Psychol. 2014;65:187–207.
Lin J, Guo W. The research on risk factors for adolescents’ mental health. Behav Sci. 2024;14:263.
Sacco R, Camilleri N, Eberhardt J, Umla-Runge K, Newbury-Birch D A systematic review and meta-analysis on the prevalence of mental disorders among children and adolescents in Europe. Eur Child Adolesc Psychiatry. 2022;1–18.
Polanczyk GV, Salum GA, Sugaya LS, Caye A, Rohde LA. Annual research review: a meta‐analysis of the worldwide prevalence of mental disorders in children and adolescents. J Child Psychol Psychiatry. 2015;56:345–65.
Kovess-Masfety V, Husky MM, Keyes K, Hamilton A, Pez O, Bitfoi A, et al. Comparing the prevalence of mental health problems in children 6-11 across Europe. Soc Psychiatry Psychiatr Epidemiol. 2016;51:1093–103.
Hossain MM, Nesa F, Das J, Aggad R, Tasnim S, Bairwa M, et al. Global burden of mental health problems among children and adolescents during COVID-19 pandemic: An umbrella review. Psychiatry Res. 2022;317:114814.
Scheiner C, Grashoff J, Kleindienst N, Buerger A. Mental disorders at the beginning of adolescence: prevalence estimates in a sample aged 11-14 years. Public Health Pract. 2022;4:100348.
Seker S, Boonmann C, d’Huart D, Bürgin D, Schmeck K, Jenkel N, et al. Mental disorders into adulthood among adolescents placed in residential care: A prospective 10-year follow-up study. Eur Psychiatry. 2022;65:e40.
Solmi M, Radua J, Olivola M, Croce E, Soardo L, Salazar de Pablo G, et al. Age at onset of mental disorders worldwide: large-scale meta-analysis of 192 epidemiological studies. Mol Psychiatry. 2022;27:281–95.
McGrath JJ, Al-Hamzawi A, Alonso J, Altwaijri Y, Andrade LH, Bromet EJ, et al. Age of onset and cumulative risk of mental disorders: a cross-national analysis of population surveys from 29 countries. Lancet Psychiatry. 2023;10:668–81.
Smogur M, Onesanu A, Plessen KJ, Eap CB, Ansermot N. Psychotropic drug prescription in children and adolescents: approved medications in European countries and the United States. J Child Adolesc Psychopharmacol. 2022;32:80–8.
Kearns GL, Abdel-Rahman SM, Alander SW, Blowey DL, Leeder JS, Kauffman RE. Developmental pharmacology-drug disposition, action, and therapy in infants and children. N Engl J Med. 2003;349:1157–67.
Hendrickx G, De Roeck V, Maras A, Dieleman G, Gerritsen S, Purper-Ouakil D, et al. Challenges during the transition from child and adolescent mental health services to adult mental health services. BJPsych Bull. 2020;44:163–8.
Singh SP, Paul M, Ford T, Kramer T, Weaver T. Transitions of care from child and adolescent mental health services to adult mental health services (TRACK Study): a study of protocols in greater London. BMC Health Serv Res. 2008;8:135.
Reneses B, Escudero A, Tur N, Agüera-Ortiz L, Moreno DM, Saiz-Ruiz J, et al. The black hole of the transition process: dropout of care before transition age in adolescents. Eur Child Adolesc Psychiatry. 2023;32:1285–95.
Singh SP, Tuomainen H, Girolamo Gde, Maras A, Santosh P, McNicholas F, et al. Protocol for a cohort study of adolescent mental health service users with a nested cluster randomised controlled trial to assess the clinical and cost-effectiveness of managed transition in improving transitions from child to adult mental health services (the MILESTONE study). BMJ Open. 2017;7:e016055.
D’Avanzo B, Lovaglio P, Parabiaghi A, Conti P, Frigerio A, Molteni M, et al. Health of the nation outcome scales for children and adolescents (HoNOSCA): psychometric properties of the Italian version. Child Youth Serv Rev. 2018;94:340–6.
Gowers SG, Harrington RC, Whitton A, Beevor A, Lelliott P, Jezzard R, et al. Health of the nation outcome scales for children and adolescents (HoNOSCA). glossary for HoNOSCA score sheet. Br J Psychiatry. 1999;174:428–31.
Achenbach TM, Rescorla LA Manual for the ASEBA School-Age Forms & Profiles. Burlington, VT: University of Vermont, Research Center for Children, Youth, & Families.; 2001.
Achenbach TM, Rescorla L Manual for the ASEBA Preschool Forms & Profiles. Burlington: University of Vermont, Research Center for Children, Youth, and Families. 2000.
Schneider LC, Struening EL, Elmer Struening TL SLOF: a behavioral rating scale for assessing the mentally ill. 1983. http://swra.oxfordjournals.org/.
Mucci A, Rucci P, Rocca P, Bucci P, Gibertoni D, Merlotti E, et al. The specific level of functioning scale: construct validity, internal consistency and factor structure in a large Italian sample of people with schizophrenia living in the community. Schizophr Res. 2014;159:144–50.
de Girolamo G, Rucci P, Scocco P, Becchi A, Coppa F, D’Addario A, et al. Quality of life assessment: validation of the italian version of the WHOQOL-Brief. Epidemiol Psichiatr Soc. 2000;9:45–55.
Wolke D, Sapouna M. Big men feeling small: childhood bullying experience, muscle dysmorphia and other mental health problems in bodybuilders. Psychol Sport Exerc. 2008;9:595–604.
Busner J, Targum SD. The clinical global impressions scale: applying a research tool in clinical practice. Psychiatry. 2007;4:28–37.
Van Buuren S, Groothuis-Oudshoorn K. mice: Multivariate imputation by chained equations in R. Journal of statistical software. 2011;45:1–67.
Singh SP, Tuomainen H, Bouliotis G, Canaway A, De Girolamo G, Dieleman GC, et al. Effect of managed transition on mental health outcomes for young people at the child-adult mental health service boundary: a randomised clinical trial. Psychol Med. 2023;53:2193–204.
Smith SW, Hauben M, Aronson JK. Paradoxical and bidirectional drug effects. Drug Saf. 2012;35:173–89.
Olfson M, He JP, Merikangas KR. Psychotropic medication treatment of adolescents: results from the national comorbidity survey-adolescent supplement. J Am Acad Child Adolesc Psychiatry. 2013;52:378–88.
Altuwairqi Y. Trends and prevalence of psychotropic medication use in children and adolescents in the period between 2013 and 2023: a systematic review. Cureus. 2024;16:e55452.
Goodwin R, Gould MS, Blanco C, Olfson M. Prescription of psychotropic medications to youths in office-based practice. Psychiatr Serv. 2001;52:1081–7.
Brown TL, Gutierrez PM, Grunwald GK, DiGuiseppi C, Valuck RJ, Anderson HD. Access to psychotropic medication via prescription is associated with choice of psychotropic medication as suicide method: a retrospective study of 27,876 suicide attempts. J Clin Psychiatry. 2018;79:16348.
Clavenna A, Cartabia M, Sequi M, Costantino MA, Bortolotti A, Fortino I, et al. Burden of psychiatric disorders in the pediatric population. Eur Neuropsychopharmacol. 2013;23:98–106.
Beharie N, Scheidell JD, Quinn K, McGorray S, Vaddiparti K, Kumar PC, et al. Associations of adolescent exposure to severe violence with substance use from adolescence into adulthood: direct versus indirect exposures. Subst Use Misuse. 2019;54:191–202.
Nilsen W, Karevold EB, Kaasbøll J, Kjeldsen A. Nuancing the role of social skills- a longitudinal study of early maternal psychological distress and adolescent depressive symptoms. BMC Pediatr. 2018;18:133.
Laurenssen EMP, Hutsebaut J, Feenstra DJ, Van Busschbach JJ, Luyten P. Diagnosis of personality disorders in adolescents: a study among psychologists. Child Adolesc Psychiatry Ment Health. 2013;7:3.
Herrenkohl TI, Kosterman R, Hawkins JD, Mason WA. Effects of growth in family conflict in adolescence on adult depressive symptoms: mediating and moderating effects of stress and school bonding. J Adolesc Health. 2009;44:146–52.
Kehusmaa J, Ruotsalainen H, Männikkö N, Alakokkare AE, Niemelä M, Jääskeläinen E, et al. The association between the social environment of childhood and adolescence and depression in young adulthood - a prospective cohort study. J Affect Disord. 2022;305:37–46.
Singh SP, Paul M, Ford T, Kramer T, Weaver T, McLaren S, et al. Process, outcome and experience of transition from child to adult mental healthcare: multiperspective study. Br J Psychiatry. 2010;197:305–12.
Ragnhildstveit A, Tuteja N, Seli P, Smart L, Uzun N, Bass LC, et al. Transitions from child and adolescent to adult mental health services for eating disorders: an in-depth systematic review and development of a transition framework. J Eat Disord. 2024;12:36.
Hill A, Wilde S, Tickle A. Review: transition from child and adolescent mental health services (CAMHS) to adult mental health services (AMHS): a meta-synthesis of parental and professional perspectives. Child Adolesc Ment Health. 2019;24:295–306.
Funding
The MILESTONE project was funded by the European Union’s Seventh Framework Programme for research, technological development, and demonstration under grant agreement no 602442.
Author information
Authors and Affiliations
Consortia
Contributions
M.M.: Conceptualization, Methodology, Investigation, Data Curation, Formal Analysis, Writing – Original Draft; D.Ma.: Conceptualization, Methodology, Investigation, Data Curation, Formal Analysis, Writing – Original Draft; S.L.: Conceptualization, Methodology, Investigation, Data Curation, Formal Analysis, Writing – Original Draft; G.dG.: Conceptualization, Methodology, Investigation, Data Curation, Formal Analysis, Writing – Original Draft; G.A.: Writing – Review & Editing; A.B.: Writing – Review & Editing; E.C.: Writing – Review & Editing; P.C.: Writing – Review & Editing; S.C.: Writing – Review & Editing; G.D.: Writing – Review & Editing; T.F.: Writing – Review & Editing; S.G.: Writing – Review & Editing; D.Mf.: Writing – Review & Editing; F.Ma.: Writing – Review & Editing; O.M.: Writing – Review & Editing; F.McN.: Writing – Review & Editing; R.Mi.: Writing – Review & Editing; R.Na.: Writing – Review & Editing; D.P.O.: Writing – Review & Editing; A.Pa.: Writing – Review & Editing; F.Ri.: Writing – Review & Editing; P.Sa.: Writing – Review & Editing; P.Sc.: Writing – Review & Editing; U.S.: Writing – Review & Editing; A.Sq.: Writing – Review & Editing; P.St.: Writing – Review & Editing; C.S.: Writing – Review & Editing; E.T.: Writing – Review & Editing; H.T.: Writing – Review & Editing; L.S.vB.: Writing – Review & Editing; S.V.: Writing – Review & Editing; S.S.: Funding Acquisition.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethics Approval
The study protocol (study registration numbers: ISRCTN83240263 and NCT03013595) was approved by the UK National Research Ethics Service Committee West Midlands, South Birmingham (15/WM/0052) and the ethical committee of the Italian coordinating site IRCCS Fatebenefratelli on 4.12.2014 (permission 70/2014). All procedures contributing to this study comply with the Helsinki Declaration of 1975, as revised in 2008.The project was approved by the local Ethics Committee on 4th December 2014 (opinion 70/2014). The authors affirm that all procedures involved in this work adhere to the ethical standards set by the appropriate national and institutional committees on human experimentation.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Magno, M., Martella, D., Leone, S. et al. Mental health trajectories of adolescents treated with psychotropic medications: insights from the european milestone study. Mol Psychiatry 31, 94–103 (2026). https://doi.org/10.1038/s41380-025-03307-3
Received:
Revised:
Accepted:
Published:
Version of record:
Issue date:
DOI: https://doi.org/10.1038/s41380-025-03307-3
