
Abstract
Poor inhibitory control and decision-making are often considered as risks for substance use and other adverse psychiatric outcomes. The Stop-Signal Task (SST) is a widely used protocol, from which inhibitory control is indexed by stop signal reaction time (SSRT). However, heretofore models of SSRT may be too simplistic to capture complex processes underlying task performance. In contrast, the Racing Diffusion Ex-Gaussian ABCD (RDEX-ABCD) model provides a more mechanistic framework, capturing both inhibitory control and task-general decision-making processes during the SST. Here, we applied the RDEX-ABCD model to SST data from the IMAGEN cohort (n > 1000) at ages 19 and 23, and examined model parameters in relation to substance use via Elastic Net regression. Connectome-based predictive modeling was then performed to identify brain networks predicting parameters, and the association between these networks and substance use was examined. We found that parameters indexing inhibitory control had no associations with substance use and were only weakly associated with brain connectivity. In contrast, parameters reflecting general decision-making processes – such as efficiency of evidence accumulation, decision threshold (response caution), probability of go failure – and their associated brain activity were significant predictors of cannabis and cigarette use. These findings suggested that efficiency of evidence accumulation, a neurocognitive mechanism that facilitates adaptive decision making across many contexts, emerged as a robust predictor of substance use vulnerability. Overall, general decision-making mechanisms may act as more reliable indicators of vulnerability to substance use than the conventional inhibitory control measures.
Similar content being viewed by others
Introduction
Inhibitory control is a core cognitive process implicated in several psychiatric disorders [1, 2], such as substance use disorders or attention deficit hyperactivity disorder (ADHD). As a latent construct, inhibitory control is often inferred from task performance. The Stop-Signal task (SST) requires individuals to complete a choice response time task; on a subset of trials, infrequent and unpredictable stop signals that the prepotent response should be withheld. The stop signal reaction time (SSRT) is a latent measure of individual differences calculated from SST performance. The measurement of SSRT is often based on the assumptions of the independent race model [3], which posits that a latent “stop” process races the “go” response process, with the winner determining whether the response is successfully inhibited. This model remains the most prevalent theoretical framework for SSRT estimation [4]. However, this model is too simplistic to capture the full array of complex cognitive processes involved in performance of the SST [5].
Recent advances in computational modeling enable the use of cognitive process models with precise assumptions about the mechanistic processes contributing to behavior, offering a comprehensive description of SST performance. The ex-Gaussian race model [6, 7] describes Go reaction time (RT) and SSRT distributions using parametric assumptions about mechanisms underlying the latency and variability of the go and stop processes [4, 5]. Racing diffusion models go further by positing that the go and stop processes both involve accumulation of noisy evidence from the environment until that evidence crosses a critical threshold for either initiating a go choice response or stopping the response [8]. As racing diffusion models provide a more detailed description of processes involved in the SST than ex-Gaussian race models but can have problematic parameter recovery properties [9], a hybrid racing diffusion ex-Gaussian model (RDEX) has been proposed [10].
Critically, cognitive process models have begun to provide novel insights about inhibitory performance in clinical groups. Application of these models to case-control samples in ADHD [11] and schizophrenia [12] indicate that poorer inhibitory performance in both disorders is likely related to broader problems with inattentive and inefficient processing rather than specific inhibition deficits. Although case-control studies demonstrate the clinical relevance of cognitive process models, such models have yet to be applied in broader population samples to better characterize the neural and clinical correlates of individual differences in mechanisms of SST performance. Further, no prior studies have used these SST models to characterize neurocognitive risk factors for substance use, a behavior that is widely thought to be linked to poorer inhibitory control [2, 13].
The IMAGEN study is a large longitudinal neuroimaging study of community-recruited European youth [14], spanning mid-adolescence to young adulthood, with extensive characterization of substance use. Hence, application of cognitive process models to IMAGEN provides a key opportunity to characterize the neural correlates of the array of mechanistic processes contributing to SST performance and link these processes to substance use. IMAGEN includes an SST with a design identical to the SST used in the ABCD study [14, 15]. This allows the RDEX-ABCD model [16], which was recently developed to address context independence violations in the ABCD task [17, 18], to be applied to IMAGEN (See Methods and Fig. 1 for details). Application of RDEX-ABCD within IMAGEN provides a portable framework for deriving mechanistically interpretable latent decision-process parameters, linking them to neural circuitry, and using them to make predictions about future substance use in the ABCD cohort once youth in ABCD mature. Critically, the relevance of this work also extends well beyond IMAGEN and ABCD; these large, well-powered cohorts yield stable effect estimates that can serve as a benchmark for replication in independent samples.

A The “hybrid” racing-diffusion ex-Gaussian (RDEX) model framework combining an evidence-accumulation model for the go process with an ex-Gaussian model for the stop process. In this framework, Go reaction times (RT) results from a competition between accumulators that collect noisy evidence for both the choice matching the stimulus and the choice mismatching it (e.g., a right-facing arrow). These accumulators operate at average rates of vt and vf, respectively, and the process concludes when one of the accumulators reaches a predefined response threshold. The stop process is the Gaussian distribution characterized by a mean (μ) and standard deviation (σ), convolved with an exponential distribution with a mean of τ. B The RDEX-ABCD model accounts for the impact of context independence violations on Stop trials by introducing a perceptual growth function. In this function, evidence signals for both the matching and mismatching accumulators on Stop trials with a given stop signal delay (SSD) are composed of two components: a processing speed component that influences evidence accumulation equally for both choices and a discrimination component that favors the choice aligned with the presented stimulus. The processing speed is determined by parameter v0 and remains constant across all SSDs. At an SSD of 0 s, the discrimination component is absent (equal to 0) since the choice stimulus has not been presented yet. However, this component increases linearly at the same rate g for both the matching and mismatching accumulators as SSD lengthens until it reaches the levels of vt and vf, as observed in Go trials. Consequently, at an SSD of 0 s, the rates for matching and mismatching choices are identical, but as SSD increases, these rates diverge gradually until they match their respective Go trial levels. Panel B illustrates the linear growth form. C Empirical growth patterns of matching (blue lines increasing from SSD = 0) and mismatching (red lines decreasing from SSD = 0) go process accumulator rates by SSD for the sample average parameter estimates (thick lines) and for parameter estimates from several randomly drawn participants (thin lines) to illustrate individual variability. In panel C, the top subpanel shows the linear perceptual growth function, and the bottom subpanel shows the non-linear (power) growth function (determined via model comparison). This figure is adapted and modified from [16] (Figure is licensed under CC BY-NC-ND 4.0).
Two processes measured by RDEX-ABCD are of particular relevance to understanding individual differences in substance use. First, efficiency of evidence accumulation (EEA) for decision making processes is a neurocognitive risk factor for externalizing behavior and substance use [19,20,21]. Second, lower values of the decision threshold for choice processes, reflecting individuals’ response caution, have been linked with substance use behaviors [14, 22, 23]. However, these previous studies were limited by small samples, low power, and minimal consideration of the neuroimaging correlates. Characterizing the neural correlates of these processes allows us to link computational measures to brain function, improving understanding of the biological mechanisms contributing to substance use risk.
Emerging neuroimaging work indicated that evidence accumulation was supported by frontoparietal network [24,25,26] and decision threshold is associated with fronto-basal ganglia network [26, 27]. However, prior studies have largely relied on region-based activation analyses, limiting inferences about how distributed, whole-brain functional networks support individual differences in these cognitive processes. Therefore, we adopted connectome-based predictive modeling (CPM) [28, 29], a well-validated data-driven machine learning approach, to identify brain networks that predict behavioral performance on the SST based on whole-brain functional connectivity.
In this study, we used the IMAGEN sample (n > 1000) to assess how mechanistic processes captured by the RDEX-ABCD model relate to whole-brain functional connectivity (derived from a previous study [30]) and substance use. A prior report using the same dataset focused on only Go-trial RT variability as a putative sustained-attention index and examined longitudinal associations with substance use [30]. Here, we extend this work by applying RDEX-ABCD to both Go and Stop trials at ages 19 and 23 to dissociate latent decision processes, and by machine learning methods (Elastic Net regularized regression and CPM) to identify robust links between these processes (and their neural correlates) and substance use. We hypothesized that computational parameters would show stronger and more specific associations with neural connectivity and substance use than SSRT from the standard integration method. Based on previous findings [24, 26], we expected EEA-related network activity to primarily involve the frontoparietal network, whereas networks associated with decision threshold would involve fronto-basal ganglia circuitry; additionally, higher EEA and lower decision threshold were expected to be associated with greater substance use.
Methods and materials
Participants
This study used data from IMAGEN at ages 19 and 23. Written and informed consent was obtained from all participants by the IMAGEN consortium, and the study was approved by the institutional ethics committees of all participating sites in accordance with the Declaration of Helsinki (see the Supplementary Materials for site-specific approvals). Data from age 14 were excluded because the stimulus delivery program at this age did not record response and RTs for trials with an SSD of 0, rendering modeling impossible. Participants were excluded based on criteria outlined by Weigard et al. [16]; if their behavioral data did not align with race model assumptions (See Supplementary Materials for details). The final sample for model estimation included 1256 and 1089 participants at ages 19 and 23, respectively. For fMRI prediction analysis, participants with excessive head motion (mean framewise displacement>0.5 mm) were additionally excluded (n = 1202/1045 at age 19/23). Details on fMRI acquisition, and preprocessing details are available in a previous study [30].
Stop-signal task
The SST required participants to respond to a Go signal —an arrow pointing left or right— the corresponding left or right button on Go trials, while withholding their response if the Go signal was unpredictably followed by a Stop signal (an upward-pointing arrow) on Stop trials (see [30]). To adjust task difficulty dynamically, a tracking algorithm on the delay was used between the Go signal and Stop signal (stop-signal delay, 250–900 ms in 50 ms increments) [4], to produce ~50% successful inhibition trials. This task included 300 Go trials and 60 Stop trials with variable delays.
Timeline followback
The Timeline Followback, a calendar-based interview with established strong reliability and validity [31], was used to evaluate prior alcohol, drugs, and smoking consumption over the past 30 days. Distributions of the frequency measures (including a subset of high-frequency users) are shown in Fig. S1, and the corresponding items are provided in Table S1.
RDEX-ABCD model
The RDEX-ABCD model combines an evidence-accumulation model of the go process with an ex-Gaussian model of the stop process (Fig. 1A). This model assumes that Go RTs and choice accuracy arise from a race between accumulators gathering noisy evidence for the matching and mismatching choices, with match rate (vt) and mismatch rate (vf), until a response threshold (B) is reached. Here, ‘matching choice’ refers to selecting the response corresponding to the direction of the Go stimulus, whereas ‘mismatching choice’ refers to selecting the opposite (incorrect) response. Stop process finishing times are assumed to follow an ex-Gaussian distribution, defined by Gaussian mean (μ) and standard deviation (σ) parameters, convolved with an exponential tail (τ), which effectively captures both the central tendency and skew of RT data [32]. The model includes the probability of go failure (Pgf) which captures omissions or failures to respond to the Go signal on Go trials, and the probability of trigger failure (Ptf), which reflects failures to initiate the inhibitory process following a Stop signal on Stop trials due to attentional lapses [11, 33, 34]. The RDEX-ABCD model addresses violations of context independence by introducing a perceptual growth function [16]. This function characterizes the relationship between stop-signal delay (SSD) and Go-stimulus processing, modeled as either a linear or non-linear function (see Supplementary Materials and Fig. 1B).
RDEX-ABCD model evaluation and estimation
We tested four variants of the original RDEX-ABCD model to evaluate cognitive processes in IMAGEN. Two features were assessed: (1) whether including Ptf improved model fit, and (2) whether a generalized power function better captured growth in choice evidence quality than the linear form (Fig. 1C). Model complexity and number of parameters are detailed in Table S2. Model performance was compared using the Deviance Information Criterion [35] and Bayesian Predictive Information Criterion [36], which reward goodness-of-fit while penalizing unnecessary complexity; lower values indicate better fit.
Models were estimated using the RDEX-ABCD code (available at https://osf.io/2h8a7/) within the Dynamic Models of Choice (DMC) framework (a free set of R functions for Bayesian estimation and simulation of evidence accumulation and stop-signal task models [37]). Individual-level Bayesian estimation employed a differential-evolution Markov chain Monte Carlo algorithm [38] to sample from the posterior distribution, which is particularly suitable for evidence-accumulation models because it allows for more efficient sampling when model parameters are correlated. For Bayesian estimation, an initial exploratory analysis used the informative priors derived from the ABCD dataset [16], whereas broad, uninformative priors were adopted for the main analysis (Table S3). To ensure robustness of the parameter estimates, we also performed parameter recovery, with full details of model estimation and recovery provided in the Supplementary Materials.
EEA and SSRT calculation
Two higher-order parameters – EEA and SSRTRDEX – were derived from the model. EEA was computed by subtracting mismatching rates from matching rates. SSRTRDEX was computed by simulating finishing time from ex-Gaussian posterior distributions [16], and SSRTINT was estimated using the integration method [4, 39]. Further details on SSRTs estimation are provided in Supplementary Materials.
Relationship between substance use and RDEX-ABCD model parameters
Exploratory factor analysis on timeline followback
Exploratory factor analysis was performed on ten selected items from Timeline Followback, yielding three common factors scores related to alcohol, cigarette and cannabis (Cig+CB), and drug use. According to the rotated factor loadings, the factors were labeled as (i) alcohol, (ii) Cig + CB, and (iii) drug (including cocaine, ecstasy, and ketamine) use. Detailed information is provided in Supplementary Materials and in a previous study [30]. These factor scores were subsequently used to measure substance use in the analysis.
Elastic net regression
To assess the relationship between RDEX-ABCD parameters and substance use, we applied Elastic Net regularized regression, which is a multivariable approach that combines the L1 (LASSO) and L2 (ridge) penalties. Here, 11 RDEX-ABCD parameters compromising the optimal model (See Results) and covariates (age, sex, and sites) served as predictor variables, and the substance use score (e.g., Cig+CB) derived from Timeline Followback as targets. We applied a ten-fold nested repeated cross-validation using the glmnet [40] and nestedcv packages [41] in Rstudio and R (v4.3.1). In the nested cross-validation procedure, the inner loop optimized the hyperparameters α and λ via a grid search [42], selecting the set with the lowest mean RMSE. These optimal hyperparameters were then applied in the corresponding outer loop to evaluate performance. Performance was averaged across outer folds to yield final RMSE and R². A final model was fitted on the whole data using the median hyperparameters from outer folds to estimate feature-wise beta values. To assess the stability of model performance and feature weights, the Elastic Net regression was repeated 100 times. From these repetitions, we calculated the mean model performance (RMSE and R²), the mean regression coefficient (β) and selection frequency for each predictor. To evaluate the model’s statistical significance, a permutation test (1000) iterations generated a null distribution of model performance. The mean model performance from the 100 repetitions was then compared against this null distribution using a significance threshold of P < 0.05. The Elastic Net regression was performed to assess the relationship between RDEX-ABCD parameters and substance use, including Cig+CB, alcohol use, and drug use. A schematic (Fig. S2) and further methodological details are provided in the Supplementary Materials.
CPM prediction
CPM was performed to explore individual differences in brain connectivity related to behavioral variables [28, 29]. Two whole-brain generalized psychophysiological interaction matrices [43] — for Successful Stop or Go trials — were generated using the Shen atlas (See Supplementary Materials and our previous study [30] for details).
The CPM was implemented using ten-fold cross-validation. First, functional connection (i.e., edges) in matrices associated with behavioral variables (i.e., model parameters) were selected using a threshold of P < 0.01, controlling for age, sex, site, and head motion in the training set. Edges positively/negatively correlated with parameters were regarded as positive/negative predictive networks. Network strength was calculated by summing the edge weights, with the combined network defined as positive minus negative strength. Linear predictive models were constructed between network strength and model parameters in the training set, with age, sex, site and mean framewise displacement (head motion) included as covariates. In the test set, network strengths were input into the predictive model, along with covariates, to predict behavioral variables. To avoid over-fitting to a random ten-fold split [44], CPMs were repeated 100 times, yielding averaged model performance. Model significance was assessed using a permutation test (1000 iterations), in which behavioral variables were randomly shuffled across participants while keeping connectivity and covariates data fixed. The full CPM procedure was rerun for each permutation to generate a null distribution of predictive performance for significance testing [45].
The Elastic Net regression identified match rate (vt), probability of go failure (Pgf), and response threshold (B) as the strongest predictors of cigarette and cannabis use (Cig+CB; see Results). Therefore, we assessed the predictive networks associated with these three cognitive processes and their relationship with Cig+CB. Additionally, the higher-order parameter EEA (the difference between match and mismatch rates), captures overall efficiency of evidence accumulation across both types of choices and has been linked to substance use [19, 20]. Accordingly, CPM analysis focused on EEA rather than vt to identify brain networks associated with the efficiency of evidence accumulation, as well as on Pgf and B. Additional CPM analyses were performed to predict SSRTRDEX and SSRTINT. Because EEA, B, and Pgf reflect the go process, connectivity matrices from Go trials were used to predict these parameters. Conversely, since SSRT reflects the stop process, connectivity matrices from Successful Stop trials were used to predict SSRTREDX and SSRTINT. We focused on the predictive performance of the combined network.
Correlation between network strength and substance use
Correlations between network strength of parameters and Cig+CB were assessed. Spearman correlations were calculated between residual network strength of parameters (controlling for age, sex, site, and head motion) and residual Cig+CB score (controlling for age, sex, and site).
Statistical analysis
To evaluate consistency over time, correlations of model parameters, and predictive network strength between two timepoints were calculated.
Results
Model fit
Demographic information for participants included in RDEX-ABCD analyses is shown in Table 1. The model estimation included 1256 participants aged 19 and 1089 participants aged 23.
The model comparison results, as indicated by the Deviance Information Criterion and Bayesian Predictive Information Criterion values, demonstrated that the power function model without Ptf was the winning model for ages 19 and 23 (Table S2). The lack of evidence for the Ptf parameter suggests that occasional failures to initiate the inhibitory process (i.e., due to attentional lapses) have a reduced impact in this age group than in younger adolescents from ABCD study. Evidence favoring power function over linear growth further indicates that the relationship between SSD duration and Go-signal processing (e.g., the perceptual growth function) follows a non-linear trajectory in these older participants. The final model included 11 core parameters (see Table S4 for mean values).
The posterior predictive checks (Fig. S3) confirmed that the RDEX-ABCD model provided an adequate description of the real data for the IMAGEN study. Parameter recovery analysis (Figs. S4, S5) indicated that the model parameters could be reliably estimated. Together, these results indicate that the RDEX-ABCD model reliably estimates parameters and adequately captures the observed data.
Parameter correlation over time
Figure 2 displays correlations of model parameters between ages 19 and 23. Correlations for SSRT derived from the RDEX-ABCD model (SSRTRDEX) and integration method (SSRTINT) did not differ significantly (r’s=0.39 vs. 0.36, P = 0.465).

The first three rows are original parameters yielded from the RDEX-ABCD model. The last row represents the parameter estimated from the model parameters. *, P < 0.05; **, P < 0.01; †, P < 0.001.
RDEX-ABCD model parameters and substance use
Elastic Net regression was conducted at each timepoint to assess whether RDEX-ABCD parameters predicted factor score derived from Timeline Followback. Model metrics (RMSE and R2) for Cig+CB were significantly better than null models generated via random-label permutation (P’s < 0.001) at ages 19 and 23. Figure 3 displays the mean coefficients and selection frequencies of RDEX-ABCD parameters across 100 iterations of Elastic Net regression. At age 19, all parameters correlated with Cig+CB, with the top three feature weights being Pgf, vt, and B (β’s = 0.105, -0.071, -0.055, respectively); remaining parameter values had smaller effect (| β’s | < 0.04). At age 23, five parameters correlated with Cig+CB, with vt, Pgf and B as the top three (β’s = -0.119, 0.061, -0.023, respectively); These three were selected for all 100 Elastic Net iterations at both ages.

A Mean beta value for each parameter predicting Cig+CB score in Elastic Net regression model at ages 19 and 23. B Frequency of each parameter predicting Cig+CB in 100 iterations of Elastic Net regression model. C Predictive performances of connectome-based predictive modeling (CPM). Cig+CB, Cigarette and cannabis use. EEA, efficiency of evidence accumulation; B decision threshold; Pgf, probability of go failure. SSRTRDXE, stop signal reaction time derived from RDEX-ABCD; SSRTINT, stop signal reaction time derived from integration method; *, P < 0.05; **, P < 0.01; †, P < 0.001.
There were no significant correlations between any model parameters and alcohol/other drug use at ages 19 and 23 (all P > 0.05, Fig. S2).
CPM results
Figure 3C shows the CPM results. Combined networks significantly predicted EEA, B, and Pgf at age 19 (r’s=0.37, 0.10, 0.28, respectively, P’s < 0.01) and at age 23 (r’s=0.33, 0.14, 0.28, respectively, P’s < 0.01). The combined network predicted SSRTRDEX (r = 0.21, P < 0.001) and SSRTINT (r = 0.16, P’s < 0.001): these r values were not significantly different from each other (P = 0.30) at age 19. At age 23, the network predicted SSRTRDEX (r = 0.17, P < 0.001) but not SSRTINT (r = 0.07, P = 0.077): these r values were significantly different (P = 0.019). The above results were validated using a ten-fold cross-validation; similar results were obtained using five-fold cross-validation and leave-site-out cross-validation (Table S5).
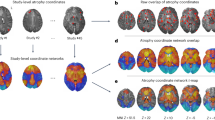
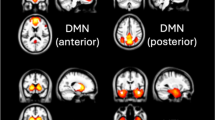
The brain networks predicting EEA, B and Pgf at ages 19 and 23 are shown in Fig. 4A, B, with the top contributing connections and node degree maps provided in Figs. S6–8. The brain networks predicting SSRTRDEX and SSRTINT at ages 19 and 23 are shown in Fig. S9, with the top contributing connections and node degree maps presented in Figs. S10–S11.

A Connectome pattern of predictive networks at age 19. B Connectome pattern of predictive networks at age 23. Pink and blue color represent positive and negative networks separately. C Correlation between cigarette and cannabis use (Cig+CB) and combined network strength derived from Go trials. MF Medial frontal, FP Frontoparietal, DMN Default mode, MOT Motor, VI Visual I, VII Visual II, Vas Visual association, SAL Salience, SC Subcortical, CBL Cerebellar. R/L, right/left hemisphere. *, P < 0.05; **, P < 0.01; ***, P < 0.001.
Correlation between network strength at ages 19 and 23
The network strength of EEA (R = 0.60, P = 3.02E-79), B (R = 0.30, P = 6.58E-18), Pgf (R = 0.25, P = 2.64E-12), SSRTRDEX (R = 0.42, P = 3.50E-34) and SSRTINT (R = 0.25, P = 1.71E-11) were correlated between ages 19 and 23 (Table S6).
Correlation between network strength and Cig+CB
At age 19, only the Pgf network strength correlated with Cig+CB (Rho=0.07, P = 0.016), whereas EEA and B network strengths showed no significant correlations (Rho = -0.04, P = 0.226; and Rho = -0.06, P = 0.060; Fig. 4C). At age 23, the EEA and B network strength – but not Pgf – correlated with Cig+CB (Rho = -0.12, P = 2.57E-04; Rho = -0.11, P = 4.99E-04; and Rho=0.06, P = 0.058 respectively). No significant correlations were observed for the SSRTRDEX or SSRTINT network strength and Cig+CB (P’s > 0.05). P values were corrected using false discovery rate correction (q < 0.05). Detailed results are shown in Table S7.
Discussion
The RDEX-ABCD model was applied to IMAGEN data and model parameters were subsequently associated with substance use and neural connectivity. Key RDEX-ABCD parameters— including those indexing evidence accumulation for correct responses, decision threshold, and probability of go failure (i.e., attentional lapses)—were robust predictors of cigarette and cannabis use at both ages. However, parameters that described the inhibitory control process had no apparent associations with substance use. Although brain networks predicted multiple model parameters describing the go and stop process, the neural signatures of EEA, decision threshold, probability of go failure, were all associated with substance use, whereas neural signatures for the inhibitory control process (SSRTRDEX, SSRTINT) were not. Among these parameters, EEA stood out as having the most robust and consistent associations with both neural features and with substance use.
Efficiency of evidence accumulation and substance use
EEA reflects the ability to selectively accumulate goal-relevant evidence to make adaptive decisions under conditions of background noise. Our identified associations of EEA, and its neural signature, with substance use are consistent with prior studies [19, 46, 47]. For instance, lower EEA and reductions in its neural-level correlates at ages 18–21 previously predicted greater substance use during ages 22–26 [19]. This association may reflect EEA as a domain-general decision-making mechanism, with lower levels leading to noisier and less reliable decisions [20]. It is plausible that neural systems supporting Go-trials decision making underpin real-world decisions requiring self-control, such as resisting substance use. In real-world contexts with greater uncertainty and noise, decision making is further challenged, making the accumulation of goal-relevant evidence even more difficult. Individuals with lower EEA may therefore be more prone to impulsive or maladaptive decisions that conflict with their long-term goals, ultimately increasing vulnerability to substance use.
EEA is also major driver of performance across executive tasks, including those measuring inhibition [48], and may act as a promising computationally characterized transdiagnostic vulnerability factor in psychopathology [20, 49]. Lower EEA has been proposed as a risk factor for various disorders, especially those involving impairments in cognitive control [24, 50,51,52]. These findings are consistent with ours in indicating that lower EEA is linked with impaired cognitive control and may reflect a common pathological process underlying diverse externalizing psychopathologies.
Brain networks predicting EEA, particularly involving the frontoparietal network, align with previous studies [24, 25]. Weigard et al. [24] demonstrated that EEA flexibly modulates attention in response to environmental demands, supported by task-positive networks like frontoparietal and dorsal attention networks, crucial for attention control and goal-directed cognition. Key regions in the frontoparietal network, such as the frontal eye field [53], and lateral intraparietal area [54] have also been shown to affect EEA. Beyond this, our CPM analysis suggests neural mechanisms of EEA supported by extensive brain regions, spanning cortex to subcortical networks.
Decision threshold and substance use
Lower decision thresholds, reflecting reduced response caution, predicted increased cigarette and cannabis use, consistent with previous studies [22, 23, 47]. For example, Gao et al. [47] reported higher decision thresholds in nonsmokers than cigarette smokers. Drift-diffusion model analysis further linked lower response caution to increased risk choice and active gambling [55], behaviors commonly correlated with substance use [56]. This study suggests that individuals with lower response caution are more likely to engage in cigarette and cannabis use. Although the effect sizes are small by conventional standards, this is expected in adequately powered neuroimaging [57,58,59] and individual differences [60] studies, where effect sizes are typically modest but more reproducible than inflated estimates from underpowered work [57,58,59]. These reproducible associations may offer clinically meaningful insights into decision-making processes linked to substance-use risk and may have a substantial impact at the population level [61]. Moreover, our sample includes a meaningful subset of high-frequency users, and frequent use in late adolescence/early adulthood is a key risk marker for later substance use disorders [62, 63]; for example, higher age-18 substance use disorder symptoms severity predicted greater adult prescription drug use (odds ratio [OR] = 1.56), supporting relevance to emerging problematic-use trajectories and motivating replication in clinically diagnosed substance use disorder samples.
Interpretation of SSRT results
SSRT was not as sensitive and robust as markers derived from Go trials (e.g., EEA) in neuroimaging predictions or substance use associations. A meta-analysis [64] highlighted replicability limitations of response inhibition task (e.g., Go/No-Go, SST) as markers for substance use disorder. SSRT demonstrates lower reliability over time than manifest behavior variables [65,66,67,68], whereas measures of manifest behavior, which are directly observable task performance measures (e.g., Go RT and SSD), and non-inhibitory processing tend to be more stable over time [66]. Aligned with this, EEA was the most test-retest reliable parameter across IMAGEN waves, potentially explaining its superior performance.
The relatively poor performance of SSRT likely partly stems from limited Stop trials (e.g., 60 vs. 300 Go trials), which reduces reliability for individual-differences analyses [4]. Go-trial measures like EEA are derived from more observations and thus are more stable. Although RDEX-ABCD improved SSRT prediction, limited Stop-trial data may still constrain the detection of brain–behavior associations relevant to inhibitory control deficits in psychiatric populations. Another explanation may relate to modeling differences. SSRT is typically estimated with non-parametric (integration) or parametric (ex-Gaussian) approaches. In contrast, EEA is derived from fine-grained computational components, potentially enhancing predictive validity. Future research could utilize models that describe both the go and stop processes as evidence accumulation processes, allowing for a more direct comparison. However, such models currently display problematic parameter recovery [9], limiting their research applications. Although SSRTINT remains the gold standard measure of inhibitory control [4] and SSRTRDEX represents a methodological advance, the lack of association with substance use in this well-powered sample casts doubt on its utility as a risk marker.
Exploring go process insights for understanding latent stop process
The go process could provide valuable insights into the latent stop process, as evidence suggests a potential link between the two [69]. Stop and go processes share a common neural basis [70, 71]. White et al. [70] found drift rate on Go trials positively correlated with activation of inhibitory-control regions (i.e., right inferior frontal gyrus and basal ganglia) during Stop trials. Individuals with stronger go processing, reflected by drift rates, Go RT, and frontal pole activation, also demonstrated stronger inhibitory processing, as shown by SSRTs and the stopping-network activation. These findings indicated a robust relationship between stimulus-processing speed and inhibitory processing at the neural level.
Conclusion
The RDEX-ABCD model was applied to IMAGEN to estimate mechanistic processes underlying SST performance. This model, in contrast to previous work (including work in this sample [30]) that relied on summary statistics, affords richer insight into the potential underlying cognitive processes engaged during the SST. We found that three go process parameters—EEA, decision threshold, and probability of go failure—as well as their neural signatures could predict cigarette and cannabis use. In comparison, stop process parameters exhibited poorer reliability, weaker relations with neural data, and no apparent predictive utility for substance use, highlighting the need for further refinement in modeling stop-related mechanisms. Notably, our findings underscore the substantial potential of EEA, other general mechanisms of decision making, and their neural correlates, as robust predictors of vulnerability to substance use.
Data availability
IMAGEN data are available from a dedicated database: https://imagen2.cea.fr. Due to participant consent restrictions, IMAGEN data cannot be made fully open access. Code for CPM analysis is available at https://osf.io/6ejpd/.
References
Cardinale EM, Bezek J, Siegal O, Freitag GF, Subar A, Khosravi P, et al. Multivariate Assessment of Inhibitory Control in Youth: Links With Psychopathology and Brain Function. Psychol Sci. 2024;35:376–89.
Ceceli AO, King SG, McClain N, Alia-Klein N, Goldstein RZ. The Neural Signature of Impaired Inhibitory Control in Individuals with Heroin Use Disorder. J Neurosci. 2023;43:173–82.
Logan GD, Cowan WB. On the Ability to Inhibit Thought and Action - a Theory of an Act of Control. Psychol Rev. 1984;91:295–327.
Verbruggen F, Aron AR, Band GPH, Beste C, Bissett PG, Brockett AT, et al. A consensus guide to capturing the ability to inhibit actions and impulsive behaviors in the stop-signal task. Elife. 2019;8:e46323.
Matzke D, Verbruggen F, Logan GD. The Stop-Signal Paradigm. Stevens’ Handbook of Experimental Psychology and Cognitive Neuroscience. 2018;1–45.
Matzke D, Love J, Wiecki TV, Brown SD, Logan GD, Wagenmakers EJ. Release the BEESTS: Bayesian Estimation of Ex-Gaussian STop-Signal reaction time distributions. Front Psychol. 2013;4:918.
Matzke D, Curley S, Gong CQ, Heathcote A. Inhibiting responses to difficult choices. J Exp Psychol Gen. 2019;148:124–42.
Logan GD, Van Zandt T, Verbruggen F, Wagenmakers EJ. On the Ability to Inhibit Thought and Action: General and Special Theories of an Act of Control. Psychol Rev. 2014;121:66–95.
Matzke D, Logan GD, Heathcote A. A Cautionary Note on Evidence-Accumulation Models of Response Inhibition in the Stop-Signal Paradigm. Computat Brain Behav. 2020;3:269–88.
Tanis CC, Heathcote A, Zrubka M, Matzke D. A hybrid approach to dynamic cognitive psychometrics : Dynamic cognitive psychometrics. Behav Res Methods. 2024;56:5647–66.
Weigard A, Heathcote A, Matzke D, Huang-Pollock C. Cognitive Modeling Suggests That Attentional Failures Drive Longer Stop-Signal Reaction Time Estimates in Attention Deficit/Hyperactivity Disorder. Clin Psychol Sci. 2019;7:856–72.
Heathcote A, Suraev A, Curley S, Gong Q, Love J, Michie PT. Decision processes and the slowing of simple choices in schizophrenia. J Abnorm Psychol. 2015;124:961–74.
Whelan R, Watts R, Orr CA, Althoff RR, Artiges E, Banaschewski T, et al. Neuropsychosocial profiles of current and future adolescent alcohol misusers. Nature. 2014;512:185–9.
Mascarell Maricic L, Walter H, Rosenthal A, Ripke S, Quinlan EB, Banaschewski T, et al. The IMAGEN study: a decade of imaging genetics in adolescents. Mol Psychiatry. 2020;25:2648–71.
Karcher NR, Barch DM. The ABCD study: understanding the development of risk for mental and physical health outcomes. Neuropsychopharmacol. 2021;46:131–42.
Weigard A, Matzke D, Tanis C, Heathcote A. A cognitive process modeling framework for the ABCD study stop-signal task. Dev Cogn Neurosci. 2023;59:101191.
Bissett PG, Hagen MP, Jones HM, Poldrack RA. Design issues and solutions for stop-signal data from the Adolescent Brain Cognitive Development (ABCD) study. Elife. 2021;10:e60185.
Bissett PG, Jones HM, Poldrack RA, Logan GD. Severe violations of independence in response inhibition tasks. Sci Adv. 2021;7:abf4355.
Weigard AS, Brislin SJ, Cope LM, Hardee JE, Martz ME, Ly A, et al. Evidence accumulation and associated error-related brain activity as computationally-informed prospective predictors of substance use in emerging adulthood. Psychopharmacology. 2021;238:2629–44.
Weigard A, Sripada C. Task-general efficiency of evidence accumulation as a computationally-defined neurocognitive trait: Implications for clinical neuroscience. Biol Psychiatry Glob Open Sci. 2021;1:5–15.
Ziegler S, Pedersen ML, Mowinckel AM, Biele G. Modelling ADHD: A review of ADHD theories through their predictions for computational models of decision-making and reinforcement learning. Neurosci Biobehav Rev. 2016;71:633–56.
Zhao X, Liu X, Zan X, Jin G, Maes JH. Male Smokers’ and Non-Smokers’ Response Inhibition in Go/No-Go Tasks: Effect of Three Task Parameters. PLoS ONE. 2016;11:e0160595.
Copeland A, Stafford T, Field M. Recovery From Nicotine Addiction: A Diffusion Model Decomposition of Value-Based Decision-Making in Current Smokers and Ex-smokers. Nicotine Tob Res. 2023;25:1269–76.
Weigard A, Angstadt M, Taxali A, Heathcote A, Heitzeg MM, Sripada C. Flexible adaptation of task-positive brain networks predicts efficiency of evidence accumulation. Commun Biol. 2024;7:801.
Wittkuhn L, Eppinger B, Bartsch LM, Thurm F, Korb FM, Li SC. Repetitive transcranial magnetic stimulation over dorsolateral prefrontal cortex modulates value-based learning during sequential decision-making. Neuroimage. 2018;167:384–95.
Mulder MJ, van Maanen L, Forstmann BU. Perceptual Decision Neurosciences - a Model-Based Review. Neuroscience. 2014;277:872–84.
Domenech P, Dreher JC. Decision threshold modulation in the human brain. J Neurosci. 2010;30:14305–17.
Finn ES, Shen X, Scheinost D, Rosenberg MD, Huang J, Chun MM, et al. Functional connectome fingerprinting: identifying individuals using patterns of brain connectivity. Nat Neurosci. 2015;18:1664–71.
Shen X, Finn ES, Scheinost D, Rosenberg MD, Chun MM, Papademetris X, et al. Using connectome-based predictive modeling to predict individual behavior from brain connectivity. Nat Protoc. 2017;12:506–18.
Weng Y, Kruschwitz J, Rueda-Delgado LM, Ruddy K, Boyle R, Franzen L, et al. A robust brain network for sustained attention from adolescence to adulthood that predicts later substance use. Elife. 2024;13:RP97150.
Sobell LC, Brown J, Leo GI, Sobell MB. The reliability of the Alcohol Timeline Followback when administered by telephone and by computer. Drug Alcohol Depend. 1996;42:49–54.
Heathcote A, Popiel SJ, Mewhort DJ. Analysis of response time distributions: An example using the Stroop task. Psychol Bull. 1991;109:340–47.
Matzke D, Love J, Heathcote A. A Bayesian approach for estimating the probability of trigger failures in the stop-signal paradigm. Behav Res Methods. 2017;49:267–81.
Matzke D, Hughes M, Badcock JC, Michie P, Heathcote A. Failures of cognitive control or attention? The case of stop-signal deficits in schizophrenia. Atten Percept Psychophys. 2017;79:1078–86.
Spiegelhalter DJ, Best NG, Carlin BP, Van Der Linde A. Bayesian measures of model complexity and fit. J R Stat Soc Ser B. 2002;64:583–639.
Ando T. Predictive Bayesian Model Selection. Am J Math Manag Sci. 2011;31:13–38.
Heathcote A, Lin YS, Reynolds A, Strickland L, Gretton M, Matzke D. Dynamic models of choice. Behav Res Methods. 2019;51:961–85.
Turner BM, Sederberg PB, Brown SD, Steyvers M. A method for efficiently sampling from distributions with correlated dimensions. Psychol Methods. 2013;18:368–84.
Verbruggen F, Chambers CD, Logan GD. Fictitious inhibitory differences: how skewness and slowing distort the estimation of stopping latencies. Psychol Sci. 2013;24:352–62.
Friedman J, Hastie T, Tibshirani R, Narasimhan B, Tay K, Simon N, et al. glmnet: Lasso and elastic-net regularized generalized linear models. Astrophys Source Code Library. 2023;ascl-2308.
Lewis MJ, Spiliopoulou A, Goldmann K, Pitzalis C, McKeigue P, Barnes MR. nestedcv: an R package for fast implementation of nested cross-validation with embedded feature selection designed for transcriptomics and high-dimensional data. Bioinform Adv. 2023;3:vbad048.
Chekroud AM, Hawrilenko M, Loho H, Bondar J, Gueorguieva R, Hasan A, et al. Illusory generalizability of clinical prediction models. Science. 2024;383:164–67.
Di X, Biswal BB. Toward Task Connectomics: Examining Whole-Brain Task Modulated Connectivity in Different Task Domains. Cereb Cortex. 2019;29:1572–83.
Scheinost D, Noble S, Horien C, Greene AS, Lake EM, Salehi M, et al. Ten simple rules for predictive modeling of individual differences in neuroimaging. Neuroimage. 2019;193:35–45.
Yip SW, Lichenstein SD, Liang Q, Chaarani B, Dager A, Pearlson G, et al. Brain Networks and Adolescent Alcohol Use. JAMA Psychiatry. 2023;80:1131–41.
Biernacki K, Molokotos E, Han C, Dillon DG, Leventhal AM, Janes AC. Enhanced decision-making in nicotine dependent individuals who abstain: A computational analysis using Hierarchical Drift Diffusion Modeling. Drug Alcohol Depend. 2023;250:110890.
Gao X, Sawamura D, Saito R, Murakami Y, Yano R, Sakuraba S, et al. Explicit and implicit attitudes toward smoking: Dissociation of attitudes and different characteristics for an implicit attitude in smokers and nonsmokers. PLoS ONE. 2022;17:e0275914.
Loffler C, Frischkorn GT, Hagemann D, Sadus K, Schubert AL. The common factor of executive functions measures nothing but speed of information uptake. Psychol Res. 2024;88:1092–114.
Sripada C, Weigard A. Impaired Evidence Accumulation as a Transdiagnostic Vulnerability Factor in Psychopathology. Front Psychiatry. 2021;12:627179.
Shen C, Calvin OL, Rawls E, Redish AD, Sponheim SR. Clarifying Cognitive Control Deficits in Psychosis via Drift Diffusion Modeling and Attractor Dynamics. Schizophr Bull. 2024;50:1357–70.
Banca P, Vestergaard MD, Rankov V, Baek K, Mitchell S, Lapa T, et al. Evidence accumulation in obsessive-compulsive disorder: the role of uncertainty and monetary reward on perceptual decision-making thresholds. Neuropsychopharmacol. 2015;40:1192–202.
Fosco WD, White CN, Hawk LW Jr. Acute Stimulant Treatment and Reinforcement Increase the Speed of Information Accumulation in Children with ADHD. J Abnorm Child Psychol. 2017;45:911–20.
Krajbich I, Mitsumasu A, Polania R, Ruff CC, Fehr E. A causal role for the right frontal eye fields in value comparison. Elife. 2021;10:e67477.
O’Connell RG, Shadlen MN, Wong-Lin K, Kelly SP. Bridging Neural and Computational Viewpoints on Perceptual Decision-Making. Trends Neurosci. 2018;41:838–52.
Wilkinson CS, Lujan MA, Hales C, Costa KM, Fiore VG, Knackstedt LA, et al. Listening to the Data: Computational Approaches to Addiction and Learning. J Neurosci. 2023;43:7547–53.
Welte JW, Barnes GM, Wieczorek WF, Tidwell MC, Parker JC. Risk factors for pathological gambling. Addict Behav. 2004;29:323–35.
Marek S, Tervo-Clemmens B, Calabro FJ, Montez DF, Kay BP, Hatoum AS, et al. Reproducible brain-wide association studies require thousands of individuals. Nature. 2022;603:654–60.
Ekhtiari H, Sangchooli A, Carmichael O, Moeller FG, O’Donnell P, Oquendo MA, et al. Neuroimaging biomarkers of addiction. Nature Mental Health. 2024;2:1498–517.
Button KS, Ioannidis JPA, Mokrysz C, Nosek BA, Flint J, Robinson ESJ, et al. Power failure: why small sample size undermines the reliability of neuroscience. Nat Rev Neurosci. 2013;14:365–76.
Owens MM, Potter A, Hyatt CS, Albaugh M, Thompson WK, Jernigan T, et al. Recalibrating expectations about effect size: A multi-method survey of effect sizes in the ABCD study. PLoS ONE. 2021;16:e0257535.
Funder DC, Ozer DJ. Evaluating Effect Size in Psychological Research: Sense and Nonsense. Adv Meth Pr Psych. 2019;2:156–68.
McCabe SE, Schulenberg JE, Schepis TS, McCabe VV, Veliz PT. Longitudinal Analysis of Substance Use Disorder Symptom Severity at Age 18 Years and Substance Use Disorder in Adulthood. Jama Netw Open. 2022;5:e225324.
Silins E, Horwood LJ, Patton GC, Fergusson DM, Olsson CA, Hutchinson DM, et al. Young adult sequelae of adolescent cannabis use: an integrative analysis. Lancet Psychiatry. 2014;1:286–93.
Fascher M, Nowaczynski S, Spindler C, Strobach T, Muehlhan M. Neural underpinnings of response inhibition in substance use disorders: weak meta-analytic evidence for a widely used construct. Psychopharmacology. 2024;241:1–17.
Fassbender K, Meyhofer I, Ettinger U. Latent state-trait and latent growth curve modeling of inhibitory control. J Exp Psychol Gen. 2023;152:1396–419.
Thunberg C, Wiker T, Bundt C, Huster RJ. On the (un)reliability of common behavioral and electrophysiological measures from the stop signal task: Measures of inhibition lack stability over time. Cortex. 2024;175:81–105.
Sebastian A, Forstmann BU, Matzke D. Reliability of triggering the stop process is related to prefrontal-subthalamic hyperdirect pathway recruitment. Imaging Neurosci. 2025;3:imag_a_00454.
Huang YQ, Luan SH, Wu BZ, Li YG, Wu JH, Chen WF, et al. Impulsivity is a stable, measurable, and predictive psychological trait. Proc Natl Acad Sci USA. 2024;121:e2321758121.
Sebastian A, Forstmann BU, Matzke D. Towards a model-based cognitive neuroscience of stopping - a neuroimaging perspective. Neurosci Biobehav Rev. 2018;90:130–36.
White CN, Congdon E, Mumford JA, Karlsgodt KH, Sabb FW, Freimer NB, et al. Decomposing decision components in the stop-signal task: a model-based approach to individual differences in inhibitory control. J Cogn Neurosci. 2014;26:1601–14.
Jahfari S, Waldorp L, Ridderinkhof KR, Scholte HS. Visual information shapes the dynamics of corticobasal ganglia pathways during response selection and inhibition. J Cogn Neurosci. 2015;27:1344–59.
Acknowledgements
IMAGEN consortium: Tobias Banaschewski, Arun L.W. Bokde, Sylvane Desrivières, Herta Flor, Antoine Grigis, Hugh Garavan, Penny Gowland, Andreas Heinz, Rüdiger Brühl, Jean-Luc Martinot, Marie-Laure Paillère Martinot, Eric Artiges, Frauke Nees, Dimitri Papadopoulos Orfanos, Luise Poustka, Nathalie Holz, Sarah Hohmann, Michael N. Smolka, Nilakshi Vaidya, Gunter Schumann, Henrik Walter, Robert Whelan.
Funding
This work received support from the following sources: the European Union-funded FP6 Integrated Project IMAGEN (Reinforcement-related behavior in normal brain function and psychopathology) (LSHM-CT- 2007-037286), the Horizon 2020 funded ERC Advanced Grant ‘STRATIFY’ (Brain network based stratification of reinforcement-related disorders) (695313), Human Brain Project (HBP SGA 2, 785907, and HBP SGA 3, 945539), the Medical Research Council Grant ‘c-VEDA’ (Consortium on Vulnerability to Externalizing Disorders and Addictions) (MR/N000390/1), the National Institute of Health (NIH) (R01DA049238, A decentralized macro and micro gene-by-environment interaction analysis of substance use behavior and its brain biomarkers), the National Institute for Health Research (NIHR) Biomedical Research Centre at South London and Maudsley NHS Foundation Trust and King’s College London, the Bundesministeriumfür Bildung und Forschung (BMBF grants 01GS08152; 01EV0711; Forschungsnetz AERIAL 01EE1406A, 01EE1406B; Forschungsnetz IMAC-Mind 01GL1745B), the Deutsche Forschungsgemeinschaft (DFG grants SM 80/7-2, SFB 940, TRR 265, NE 1383/14-1), the Medical Research Foundation and Medical Research Council (grants MR/R00465X/1 and MR/S020306/1), the National Institutes of Health (NIH) funded ENIGMA (grants 5U54EB020403-05 and 1R56AG058854-01), NSFC grant 82150710554 and European Union funded project ‘environMENTAL’, grant no: 101057429. Further support was provided by grants from: - the ANR (ANR-12-SAMA-0004, AAPG2019 – GeBra), the Eranet Neuron (AF12-NEUR0008-01 – WM2NA; and ANR-18-NEUR00002-01 – ADORe), the Fondation de France (00081242), the Fondation pour la Recherche Médicale (DPA20140629802), the Mission Interministérielle de Lutte-contre-les-Drogues-et-les-Conduites-Addictives (MILDECA), the Assistance-Publique-Hôpitaux-de-Paris and INSERM (interface grant), Paris Sud University IDEX 2012, the Fondation de l’Avenir (grant AP-RM-17-013), the Fédération pour la Recherche sur le Cerveau; the National Institutes of Health, Science Foundation Ireland (16/ERCD/3797), U.S.A. (Axon, Testosterone and Mental Health during Adolescence; RO1 MH085772-01A1) and by NIH Consortium grant U54 EB020403, supported by a cross-NIH alliance that funds Big Data to Knowledge Centres of Excellence. ImagenPathways “Understanding the Interplay between Cultural, Biological and Subjective Factors in Drug Use Pathways” is a collaborative project supported by the European Research Area Network on Illicit Drugs (ERANID). This paper is based on independent research commissioned and funded in England by the National Institute for Health Research (NIHR) Policy Research Programme (project ref. PR-ST-0416-10001), China Scholarship Council—Trinity College Dublin Joint Scholarship Programme (202006750028). The views expressed in this article are those of the authors and not necessarily those of the national funding agencies or ERANID. Alexander Weigard was supported by NIDA K23 DA051561. Open Access funding provided by the IReL Consortium.
Author information
Authors and Affiliations
Consortia
Contributions
Robert Whelan, Alexander Weigard, and Yihe Weng conceptualized this study. Tobias Banaschewski, Arun L.W. Bokde, Sylvane Desrivières, Herta Flor, Antoine Grigis, Hugh Garavan, Penny Gowland, Andreas Heinz, Rüdiger Brühl, Jean-Luc Martinot, Marie-Laure Paillère Martinot, Eric Artiges, Frauke Nees, Dimitri Papadopoulos Orfanos, Luise Poustka, Nathalie Holz, Sarah Hohmann, Michael N. Smolka, Nilakshi Vaidya, Gunter Schumann, Henrik Walter acquired the data. Yihe Weng processed and analyzed the data. Alexander Weigard, Rory Boyle, and Chi Tak Lee contributed to data analyses. Yihe Weng, Robert Whelan, and Alexander Weigard wrote the manuscript. All authors edited the paper and gave final approval before submission.
Corresponding author
Ethics declarations
Competing interests
Dr Banaschewski served in an advisory or consultancy role for eye level, Infectopharm, Medice, Neurim Pharmaceuticals, Oberberg GmbH and Takeda. He received conference support or speaker’s fee by Janssen-Cilag, Medice and Takeda. He received royalities from Hogrefe, Kohlhammer, CIP Medien, Oxford University Press; the present work is unrelated to these relationships. Dr Poustka served in an advisory or consultancy role for Roche and Viforpharm and received speaker’s fee by Shire. She received royalties from Hogrefe, Kohlhammer and Schattauer. The present work is unrelated to the above grants and relationships. The other authors report no biomedical financial interests or potential conflicts of interest.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Weng, Y., Boyle, R., Lee, C.T. et al. Model-based analysis of stop-signal data reveals robust neural and clinical correlates of evidence accumulation but not inhibition. Neuropsychopharmacol. (2026). https://doi.org/10.1038/s41386-026-02401-6
Received:
Revised:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41386-026-02401-6
