
Abstract
Maternal mental health is associated with fetal neurodevelopment. Identifying effective treatments for maternal psychiatric conditions is a public health priority. SRIs (SSRIs and SNRIs) are commonly prescribed for prenatal mental health conditions; however, their impact on fetal brain development remains understudied. In this observational cohort study, we compared fetal brain and placental structures between SRI-exposed and unexposed pregnancies divided by categories of maternal depressive symptom severity from the Edinburgh Postnatal Depression Scale (EPDS). Pregnant women treated with SRIs and controls without mental illness or antidepressant exposure underwent fetal MRI studies between 20-40 weeks’ gestation. Fetal brain motion correction and 3D reconstructions were performed using slice-to-volume registration. Fetal brain volumes (cortical gray matter, white matter, deep gray matter, cerebellum, brainstem, and hippocampi) were quantified using deep learning-based segmentation with manual correction. Cerebral cortical folding measures included local gyrification index, sulcal depth, curvedness, and surface area. Placental volume and microstructure were assessed with T2-weighted and diffusion-weighted MRI, respectively. EPDS scores were categorized as low ( ≤ 4), moderate (5–9), and high ( ≥ 10). A total of 182 pregnant women were included [62 SRI-exposed (59 SSRIs, 3 SNRIs); 120 controls]. Notably, 29% of SRI-exposed women continued to report elevated depression. SRI-exposed fetuses had smaller hippocampal volumes and reduced cortical gyrification, curvedness, and surface area. Subgroup analysis of stratification by EPDS scores revealed that SRI-exposed fetuses had reduced hippocampal volumes compared to unexposed fetuses with low and moderate, but not high, EPDS scores, and reduced cortical curvedness compared to unexposed subgroups. Among unexposed subgroups, fetuses exposed to high maternal EPDS scores had smaller hippocampal volumes compared to those with low scores. Placenta volume and microstructural diffusion were increased in the SRI-exposed compared to the unexposed group. Larger placental volume was associated with larger total fetal brain volume, and higher placental diffusion was associated with larger fetal white matter and cerebellar volumes in the SRI-exposed group. These findings suggest that prenatal SRI exposure may be associated with altered fetal hippocampal volumes, cerebral cortical maturation, and placental volume and microstructural diffusion. The clinical significance and long-term neurodevelopmental consequences of these structural alterations remain unknown and are currently under study.
Similar content being viewed by others


Introduction
Maternal depression and anxiety are prevalent and impact up to 15% of women in the peripartum period [1,2,3]. Increasing evidence highlighting potential risks of untreated maternal depression includes complications such as miscarriage [4], preeclampsia [5], preterm delivery [6], and low birth weight [7]. Untreated depression during pregnancy is increasingly recognized as a risk factor adversely affecting offspring brain development, such as reduced cerebral and cerebellar gray matter volumes, increased cerebral cortical gyrification, and altered amygdala and hippocampal volumes as well as altered brain microstructure and functional connectivity [8,9,10,11,12,13,14]. Additionally, adverse child neurodevelopmental outcomes such as cognitive, language, learning, memory, social-emotional problems, and neuropsychiatric dysfunction [15,16,17] are reported after prenatal exposure to maternal mental health conditions, underscoring the importance of effective treatment strategies for both mother and child.
Selective serotonin reuptake inhibitors (SSRIs) and serotonin-norepinephrine reuptake inhibitors (SNRIs) are among the most commonly prescribed medications for managing mental illness during pregnancy [18]. Although both classes are generally considered low-risk choices for use during pregnancy [19, 20], they have potential risks. Women treated with SSRIs during pregnancy are at elevated risk for preterm birth and growth restriction [21, 22]. Brain MRI studies suggest that prenatal SSRI exposure is associated with alterations in brain structure and connectivity in the offspring, including increased gray matter volume in the right amygdala and right insula, as well as increased structural connectivity between the right amygdala and right insula in infants [23]. Higher connectivity in putative auditory resting-state networks [24] and lower fractional anisotropy, increased mean and radial diffusivity for multiple white matter fiber bundles have been reported in newborns [25]. Prenatal SSRI exposure has also been associated with reduced cerebral gray matter volume and steeper increases in amygdala and fusiform gyrus volumes in children aged 7–15 years [26]. Additionally, prenatal SSRI exposure may be associated with altered neurodevelopment and behavior in offspring, such as attenuated pain response in infants, and increased likelihood of anxiety or depression in adolescence [27,28,29,30,31,32]. Moreover, while placental dysfunction is implicated in preterm birth and growth restriction [33, 34], its relationship to maternal depression and SSRI exposure remains poorly understood. Understanding the impact of prenatal SSRI exposure on fetal brain and placental development is imperative.
We investigated the effects of prenatal exposure to SSRIs and SNRIs, collectively referred to as SRIs, on fetal brain volumes, cortical folding, and placental development. Given that the effects of SRI exposure are likely to be confounded by the severity of maternal psychiatric illness [35], maternal Edinburgh Postnatal Depression Scale (EPDS) scores were included as a continuous covariate in the main analyses to account for variance attributable to depressive symptoms. Additionally, we conducted subgroup analyses using a categorical approach (low, moderate, high EPDS) to examine whether fetal brain and placental differences between SRI-exposed and unexposed pregnancies varied across levels of maternal depressive symptoms which allowed assessment of whether observed differences were related to SRI exposure, maternal depressive symptoms, or both.
Participants and methods
Study design
This study included pregnant individuals undergoing treatment with SRIs, confirmed via medical records. A comparison group consisted of pregnant women without a current or lifetime episode of mental illness and without antidepressant treatment. Women were eligible if record reviews confirmed normal fetal ultrasounds and biometry studies. We excluded: (1) fetuses with known or suspected congenital infection, dysmorphic features, or dysgenetic lesions, or documented genetic or chromosomal abnormalities; and (2) pregnant women with multiple pregnancies or contraindications to MRI. Fetal brain and placenta MRI studies were performed between 20 and 40 weeks of gestation. This study was approved by the institutional review board at Children’s National Hospital and written informed consent was obtained by all participants prior to enrollment.
Prenatal maternal depression
The Edinburgh Postnatal Depression Scale (EPDS) [36] was used to quantify depressive symptoms and was completed on the day of the MRI visit. The EPDS is the most commonly used screening tool during the perinatal period [37]. It is a 10-item questionnaire (range: 0–30) designed to measure the severity of symptoms over the prior 7 days. An EPDS score ≥10 is a positive screen for depression during pregnancy [38, 39]. We assigned EPDS scores into categories of ≤4, 5–9, and ≥10 as low, moderate, and high symptom levels, respectively. These clinically relevant cutoffs are well established and commonly used in obstetric and psychiatric studies [38,39,40].
Fetal brain MRI acquisition
Fetal brain T2-weighted MRI was performed using a 1.5 T GE DISCOVERY MR450 scanner with an 8-channel receiver coil or a 3.0 T Siemens MAGNETOM Vida scanner with up to 48-channel surface receive coil system. Scanning protocols were harmonized between 1.5 T and 3.0 T scanners. At 1.5 T, the protocol included multiplanar single shot fast spin echo (SSFSE) acquisitions [echo time (TE): 160 ms; repetition time (TR): 1100 ms; flip angle (FA): 90°; field of view (FOV): 32×32 cm]. At 3.0 T, multi-plane multi-phase Half-Fourier acquisition single-shot turbo spin-echo (HASTE) T2-weighted images were performed (TE: 107 ms; TR: 1500 ms, FOV: 33 × 33 cm). For both 1.5 T and 3.0 T, imaging parameters included a matrix of 256 × 192, 2-mm slice thickness, and 0-mm slice gap. Interleaved acquisition, including odd and even slices, was performed to avoid slice crosstalk. For each subject, three T2w images were collected from each of axial, sagittal, and coronal planes. Participants were scanned during free breathing without the use of sedation or contrast agents.
Fetal brain reconstruction
After acquisition, motion-corrupted stacks of 2-dimensional slices from coronal, sagittal, and axial planes were reconstructed into a 3-dimensional image (Supplementary Fig. 1). In this step, the fetal brain in MRI slices were automatically detected using You Only Look Once (YOLO) [41], a deep convolutional neural network designed for object detection. After brain detection, a parallel slice-to-volume reconstruction method with evaluated point-spread functions was applied to remove motion and reconstructed brain slices into a 3D image [42]. The reconstructed brain was rigidly registered to an in-house developed fetal brain atlas from 18 to 37 gestational weeks for reorientation using FSL FLIRT [43]. After brain reorientation, the image with 0.86 × 0.86 × 0.86 mm3 resolution was used in the following measures.
MRI volumetric analysis
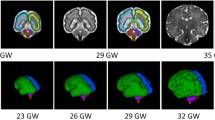
Volumes of cortical gray matter, white matter, deep gray matter, cerebellum, brainstem, and left and right hippocampi were automatically segmented using a 3D U-Net based model (Fig. 1) [44]. 3D U-Net has demonstrated strong performance in medical image segmentation and has been validated for use in fetal brain image segmentation [44, 45]. Automatic segmentations were manually corrected using ITK-SNAP. A neuroradiologist with over 20 years’ experience in reading fetal MRI studies assisted with anatomical localization of these brain structures on MRI images. All structures were manually corrected by the same experienced rater, and 20% scans were randomly chosen and corrected by a second experienced rater. Inter-rater reliabilities using intraclass correlation coefficient for all measured regions were higher than 0.95. Raters were blinded to cohort status.

Segmentation of cortical gray matter (green), white matter (blue), deep gray matter (yellow), cerebellum (violet), brainstem (brown), left hippocampus (orange), and right hippocampus (red) of a reconstructed fetal brain image at 29.7 gestational weeks.
Cerebral cortical folding
The inner surface of cortical gray matter was used to measure the cortical folding [46]. We analyzed: (1) Local gyrification index, the ratio between the cortical surface area and the corresponding area on cerebral hull surface within a sphere centered at each surface vertex [47]. (2) Sulcal depth, the distance from each vertex on the cortical surface to the nearest point on the cerebral hull surface [48]. (3) Curvedness, a measurement of the intensity of surface curvature [49]. (4) Surface area, the total cortical surface area calculated by summing the areas of all triangular surface meshes [47].
Placenta MRI acquisition
Placenta imaging was acquired on the same scanner along with fetal brain MRI. At 1.5 T, T2-weighted sequence was acquired using multiplanar SSFSE (TR: 1100 ms; TE: 160 ms). At 3.0 T, HASTE T2-weighted images were acquired (TR: 1500 ms; TE: 107 ms). For both 1.5 T and 3.0 T, imaging parameters included a field of view 42 × 42 cm, 4-mm slice thickness, and 0-mm slice gap. Diffusion-weighted imaging (DWI) was performed using pulsed gradient spin echo (TR: 8000 ms, TE: 53.8 ms, matrix size 96×96, FOV: 42 × 42 cm, 4-mm slice thickness) with b-values: 0, 25, 50, 114, 243, 500, 543, 800, 900 sec/mm2, diffusion time of 25 ms. Scanning protocols were harmonized between 1.5 T and 3.0 T scanners.
Placenta MRI processing
The placenta was manually segmented on T2-weighted MR image for volumetric measurement. For microstructure diffusion, the placenta was manually segmented on the diffusion weighted image with b value of 0 s/mm2 using ITK-SNAP (Fig. 2). The corresponding T2-weighted image was used as anatomical reference during the manual segmentation. The placental mask was propagated to each b-value image and non-rigid registration was applied between b0 and subsequent b-value images for motion correction [50]. After that, the apparent diffusion coefficient (ADC) map was calculated by fitting of voxel-by-voxel using: S(b) = S0 (-b×ADC), where S(b) is the signal intensity at a certain b-value, S0 is the signal intensity at b = 0 [51]. ADC provides information about the magnitude of water molecule diffusion in tissues.

Placenta T2-weighted MRI scan (1st row) and diffusion weighted imaging scans with different b values (2nd and 3rd rows) of a subject at 30.29 gestational weeks.
Statistical analysis
Analysis was performed using SAS 9.3 and MATLAB R2024a. Subject characteristics in the SRI-exposed and unexposed groups were compared using t test for continuous variables and Fisher’s exact test for categorical variables. General linear model (GLM) was used to measure changes of fetal brain volumes, cortical folding, placenta measures, and maternal depression scales by gestational age (GA) and sex. Fetal brain measures between SRI-exposed group and unexposed controls were compared using analysis of covariance (ANCOVA), adjusting for GA at MRI, fetal sex, maternal depression score at MRI visit, and maternal weight at MRI. Fetal brain measures were further analyzed using ANCOVA, stratified by varying levels of maternal depression (EPDS ≤ 4, 5–9, ≥10) and adjusted for GA at MRI, fetal sex, and maternal weight at MRI. Placenta measures between SRI-exposed group and unexposed controls were compared using ANCOVA, adjusting for GA at MRI, maternal depression score at MRI visit, and maternal weight at MRI. Placental measures in the three categories of maternal depressive symptoms (EPDS ≤ 4, 5–9, ≥10) were analyzed using ANCOVA, adjusting for GA at MRI and maternal weight at MRI. p values in each table were adjusted for multiple testing based on the false discovery rate according to the Benjamini-Hochberg method [52], and adjusted p values ≤ 0.05 were considered significant.
Results
Demographics
Our cohort consisted of 182 participants: 62 with SRI (59 SSRIs, 3 SNRIs) exposure and 120 unexposed controls (Table 1). None of our enrolled participants reported receiving or undergoing psychotherapy. The mean (SD) [range] GA at MRI was 31.72 (4.05) [20.0-38.57] weeks for the SRI-exposed group and 32.04 (4.32) [23.57-39.71] weeks for controls, respectively. There were 27 (44%) and 67 (56%) of women carrying male fetuses for the SRI-exposed group and controls, respectively. Maternal weight at MRI was higher in the SRI group versus controls (86.21 vs 76.58 kg, p = 0.0001). Maternal alcohol use during pregnancy was higher in the SRI versus the unexposed group (16% vs 5%, p = 0.02). In both groups, more than half of women were non-Hispanic White. More than 90% and 84% of women were college graduates, and 82% and 84% reported professional employment in the SRI and control groups, respectively.
Maternal depressive symptoms
Maternal depression scores were significantly higher in the SRI-exposed group compared to unexposed controls (mean: 6.55 vs 4.75, p = 0.01). The proportion of EPDS score ≥10 was significantly higher in women treated with SRIs (29%) versus unexposed controls (13%). EPDS scores did not significantly change with increasing GA in controls (β = 0.03, p = 0.70). However, maternal scores decreased with advancing GA in the SRI-exposed group (β = –0.34, p = 0.02).
Fetal brain volume and cortical folding
All measured fetal brain volume and cortical folding measures significantly increased with advancing GA in both the SRI and control groups (all p < 0.0001). In unexposed controls, males had significantly larger volumes in white matter (104.13 vs 99.94 cm3, p = 0.04), deep gray matter (16.03 vs 15.41 cm3, p = 0.03), and total brain (203.98 vs 197.71 cm3, p = 0.04), compared to females. In the SRI-exposed group, males had larger total brain volume compared to female fetuses (203.40 vs 187.59 cm3, p = 0.01). Left hippocampal volumes were smaller than the right hippocampus in both SRI-exposed (0.46 vs 0.50 cm3, p = 0.002) and control (0.52 vs 0.56 cm3, p < 0.0001) groups. Fetal cerebral cortical folding measures did not significantly differ in males and females.
Placenta volume and microstructure measures
The placental volume significantly increased as GA increased in both groups (SRI: β = 39.91 cm3/week, p < 0.0001, controls: β = 30.07 cm3/week, p < 0.0001). In controls, placental ADC_D decreased with advancing GA (β = –0.00004, p = 0.03); however, no significant association was observed between placental ADC_D and GA in the SRI-exposed group. Placental measures did not significantly differ in pregnancies with male versus female fetuses.
Fetal brain measures in SRI-exposed group vs controls
SRI-exposed fetuses showed significantly smaller left (0.45 vs 0.53 cm3, adjusted p = 0.0004) and right (0.48 vs 0.56 cm3, adjusted p = 0.0004) hippocampal volumes compared with controls (Table 2). Additionally, the SRI-exposed group showed reduced cerebral cortical local gyrification index (1.24 vs 1.28, adjusted p = 0.03), curvedness (0.21 vs 0.24 mm–1, adjusted p = 0.0004), and surface area (143.35 vs 151.36 cm2, adjusted p = 0.02) compared with controls (Table 2).
Because maternal alcohol use during pregnancy was higher in the SRI compared to the unexposed group (Table 1), sensitivity analyses were performed by excluding participants with alcohol use during pregnancy from the comparison of fetal brain and placental measures between the SRI-exposed and unexposed groups, adjusting for the same covariates as in the main analyses. In this sensitivity analysis (Table S1), in addition to the main findings (in Table 2), fetal cerebellar volume also differed between the SRI-exposed and unexposed groups (mean: 9.15 vs. 9.67 cm³; 95% CI: −1.03 to −0.004) before adjustment for multiple comparisons. However, this difference was no longer statistically significant after correction for multiple comparisons (adjusted p = 0.10), consistent with the main findings in Table 2.
Fetal brain measures in SRI-exposed group and controls relative to maternal depressive symptoms
For measures with significant differences between the SRI-exposed and unexposed groups (Table 2), additional subgroup analyses were conducted by stratifying based on maternal depression severity (Table S2). Both left and right hippocampal volumes in unexposed low- and moderate-EPDS groups were significantly larger than those in all three EPDS subgroups of SRI-exposed participants. Of note, fetuses in the unexposed high-EPDS group had smaller left and right hippocampal volumes compared to the unexposed low-EPDS group. Additionally, SRI-exposed fetuses in both the low and moderate EPDS subgroups showed reduced cortical curvedness compared to unexposed subgroups (Table S2). Fetal hippocampal volumes and cortical folding measures did not differ significantly across the low, moderate, and high EPDS subgroups within the SRI-exposed group (Table S2).
In the sensitivity analyses of the subgroup comparison after excluding participants with alcohol use during pregnancy (Table S3), the difference in fetal cortical curvedness between SRI-exposed fetuses with low and moderate EPDS scores and the unexposed group with high EPDS (in Table S2) remained significant before, but not after, adjustment for multiple comparisons (Table S3), suggesting that the observed subgroup differences in fetal cortical curvedness between SRI-exposed fetuses with low and moderate EPDS and the unexposed group with high EPDS may be less significant by the exclusion of participants with alcohol use during pregnancy.
Placenta measures in SRI-exposed group vs controls
Placenta volumes (753.11 cm3 vs 656.00 cm3, adjusted p = 0.004) and ADC_D (0.004 vs 0.003, adjusted p = 0.048) were higher in SRI-exposed group vs unexposed controls (Table 3). Additional subgroup analyses stratified by maternal depression severity are presented in Table S4; however, the differences between subgroups were no longer significant after adjusting for multiple testing.
The placenta results in the sensitivity analyses (Tables S5 and S6) by excluding participants with alcohol use during pregnancy were consistent with the main findings in Table 3 and S4.
Associations between placenta measures and fetal brain measures in SRI-exposed group
Larger placenta volume was associated with larger volumes in fetal deep gray matter (β = 0.002, p = 0.02) and total brain (β = 0.05, p = 0.005) (Table S7) as well as larger cortical surface area (β = 0.03, p = 0.03) (Table S8). Increased placenta ADC_D was associated with larger volumes in fetal cortical gray matter (β = 2493.92, p = 0.04), white matter (β = 6153.24, p = 0.01), cerebellum (β = 525.99, p = 0.01), and total brain (β = 6886.81, p = 0.03) as well as increased cortical gyrification index (β = 18.53, p = 0.03) and surface area (β = 6595.05, p = 0.008) (Table S8). The associations between placental volume and fetal total brain volume, as well as between placental ADC_D and fetal white matter and cerebellar volumes, remained significant after adjusting for multiple testing (Table S7).
Discussion
We report that altered fetal brain development may be associated with both SRI exposure and elevated depression symptoms. SRI-exposed fetuses had smaller left and right hippocampal volumes, decreased cortical gyrification index, curvedness, and surface area. Notably, hippocampal volumes were reduced in SRI-exposed fetuses compared to unexposed fetuses in the low and moderate EPDS groups, and cortical curvedness was decreased in SRI-exposed fetuses in low and moderate EPDS groups compared to unexposed controls. Among unexposed fetuses, reduced hippocampal volumes were observed in those with high versus low maternal EPDS scores. Additionally, SRI-exposed pregnancies had increased placental volume and microstructural diffusion compared with unexposed pregnancies. Finally, within the SRI-exposed group, larger placental volume was associated with larger fetal total brain volume, and higher placental diffusion was associated with larger fetal white matter and cerebellar volumes.
We observed an unsettling 29% of women in the SRI-treated group continued to report EPDS scores ≥10. This rate is comparable to 32% reported in a similar sample of SRI-treated pregnant women [40] and significantly higher than the 13% observed in the unexposed group, which highlights the frequency of persistent depressive symptoms during pregnancy. The remaining SRI-exposed participants had low or moderate EPDS scores, suggesting remission or partial response. These findings may suggest inadequate SRI dosing or reductions in plasma concentrations due to increased drug clearance in pregnancy [53,54,55]. Importantly, this variation in symptom severity among SRI-treated participants provided an opportunity to explore potential differences in fetal and placental development associated with symptom control in SRI-treated mothers.
Importantly, we observed decreased left and right hippocampal volumes, as well as reduced cortical gyrification index, curvedness, and surface area in fetuses exposed to SRIs compared to unexposed controls after adjusting for maternal depression scales. Stratified analyses by maternal depression severity also suggested reduced hippocampal volumes and cerebral cortical curvedness in SRI-exposed subgroups (low, moderate, and high depression) compared to unexposed fetuses, indicating that these brain alterations may not be solely attributable to maternal depression, but also associated with SRI exposure across varying levels of maternal depression symptoms. Additionally, we found no significant differences in fetal hippocampal volumes when comparing SRI-exposed subgroups to unexposed fetuses with high maternal depression. This finding raises the possibility that high maternal depressive symptoms alone may adversely affect fetal hippocampal development to a similar extent as SRI exposure. The observed differences in fetal brain development may also reflect underlying genetic or familial vulnerability factors rather than SRI exposure per se. Notably, among unexposed subgroups, fetuses of women with high symptoms had smaller left and right hippocampal volumes compared to those with low depression, consistent with prior findings [10, 12], suggesting that elevated depressive symptoms can impact fetal hippocampal development independent of SRI exposure. In contrast, hippocampal volumes did not significantly differ across SRI-exposed subgroups with low, moderate, and high EPDS scores, which suggest that prenatal SRI treatment may mitigate the associations between elevated maternal depression and reduced fetal hippocampal volumes observed in the unexposed group. Therefore, in the presence of high depressive symptoms, the observed brain structural differences likely reflect a combination of medication exposure and underlying high-level maternal depressive symptoms, making it challenging to identify the independent effect of SRI exposure alone. These findings underscore the difficulty of disambiguating the effects of SRI treatment from those of maternal psychiatric illness. While these structural differences may reflect alterations in fetal brain maturation, the clinical significance and long-term neurodevelopmental consequences remain uncertain. The hippocampus is critical for memory and emotional regulation, while cortical curvature, a marker of cortical folding, reflects brain maturation [56,57,58]. Longitudinal follow-up studies incorporating genetic and familial factors are needed to determine the relationship between early brain structural alterations and subsequent developmental outcomes.
The potential mechanisms underlying the effects of SRI exposure on fetal hippocampal and cortical folding development are complex and multifaceted. In addition to the confounding effects of maternal psychiatric illness, comorbid conditions, and shared genetic and environmental factors [35, 59, 60], SRIs cross the placenta and potentially influence fetal brain development by altering levels of critical neurotransmitters [61,62,63]. Indeed, changes in serotonin levels during critical periods of brain development could alter the formation of neural circuits and potentially lead to brain structural alterations and subsequent neuropsychiatric outcomes [64].
To better understand feto-placental-maternal relationships, we investigated in vivo placental development and observed that SRI-exposed pregnancies showed larger placental volume and higher microstructural diffusion than controls. The DWI ADC model quantifies tissue microstructure by measuring water diffusion, enabling detection of subtle changes undetectable by conventional imaging [65, 66]. Diffusion variations may reflect altered vascularization and intervillous space, indicating disrupted villous maturation and placental dysfunction [67, 68]. Such dysfunction has been implicated in adverse outcomes including preterm birth and growth restriction, conditions previously associated with prenatal SRI exposure [21, 22]. Prior MRI-based studies have demonstrated that larger placental volume is associated with increased fetal cerebral and cerebellar volumes in fetal growth restriction and healthy pregnancies [69], as well as with increased subcortical gray matter, total brain, and intracranial volumes in fetuses with congenital heart disease (CHD) [70]. In addition, placental hypoplasia, vascular malperfusion, and the presence of placental pathology have been associated with reduced fetal total intracranial volume, particularly in CHD [71]. To our knowledge, the current study is the first to show that prenatal SRI exposure is associated with increased placental volume and microstructural diffusion, and that these placental alterations are associated with fetal total brain, white matter, and cerebellar volumes in SRI-exposed pregnancies. Our findings may reflect a compensatory adaptation to enhance the transfer of nutrients and growth factors, potentially supporting fetal brain development. The observed associations between placental volume and diffusion with fetal brain volumes highlight the complex relationship between placental function and fetal brain development in the context of SRI exposure. This study focused on fetal life, a specific stage in development, and interpretations of functional effects of these alterations are premature. Reassuringly, a large, fully adjusted pharmacoepidemiologic study found that prenatally antidepressant-exposed and unexposed siblings had similar risks of neurodevelopmental disorders through age 14 years [72].
Limitations of this study deserve mention. First, we were unable to evaluate the impact of the amount, timing, and duration of SRI exposure on fetal brain and placenta measures, due to the lack of detailed data. Second, although GA at MRI was included as a covariate in all analyses, the span of imaging between 20 and 40 weeks’ gestation encompasses a wide range of dynamic neurodevelopmental changes. GA represents a relatively broad developmental marker and may not fully serve as a proxy for other age-related biological processes (e.g., cerebral blood flow or metabolic demand) not directly measured in the current study. Similarly, maternal depression itself, independent of SRI exposure, may be associated with reduced physical activity and altered fetal movement patterns, which were not assessed in the current study. Such unmeasured developmental, behavioral, or physiological factors may have influenced fetal brain and placental development. Third, none of the enrolled participants reported receiving or undergoing psychotherapy during pregnancy, which may have led to underrepresentation of individuals with milder depressive symptoms and who may have been managed with psychotherapy alone, indicating our SRI-exposed group may reflect women with more clinically severe or treatment-resistant symptoms, which may affect the generalizability of our findings and should be considered when interpreting the results. Fourth, our cohort predominantly consisted of high-income, well-educated women which limits the generalizability of our findings to pregnant women across diverse socio-demographic backgrounds. In addition, with only three SNRI-exposed participants, we were unable to compare SSRI- and SNRI-specific effects. Larger samples of SNRI-exposed pregnancies are needed to evaluate potential class-specific differences. Although we examined differences across maternal depression severity, subgroups with high depression scores had relatively small sample sizes, which may have limited the statistical power of these analyses. Larger samples will be needed to more definitively evaluate fetal brain and placental development in relation to treatment response (remission versus persistent symptoms) during prenatal SRI exposure. The significance of maternal depressive symptoms can also vary based on assigned cut-off scores; in this study, we selected cut-off scores which have been previously used for pregnant women [38,39,40]. Furthermore, one-timepoint EPDS score does not capture the cumulative burden or temporal variability of depressive symptoms across pregnancy. While the EPDS is a well-validated measure for perinatal depression, it does not incorporate other dimensions of maternal psychological distress, such as perceived stress or anxiety, which may independently or jointly influence fetal brain and placenta development. In this study, we focused on depressive symptoms, given that prenatal depression is the most common perinatal mental health condition [73, 74] and is typically treated with SRIs when pharmacotherapy is needed during pregnancy [75, 76]. A detailed lifetime and prenatal course of maternal mental illness would clarify the impact of maternal psychiatric symptoms, beyond depression alone, and SRI treatment on fetal brain and placental development. Due to the challenges in fetal MRI, 9% of scans were unusable following 3D reconstruction because of excessive fetal motion; however, this proportion is consistent with or superior to other fetal MRI studies [77]. While we adjusted for age at MRI, sex, maternal weight, and maternal depression scores in the model, our sample size limited our ability to adjust for additional potential confounding factors, such as maternal physical health and lifestyle factors. Lastly, alcohol use during pregnancy was assessed as a binary self-reported variable with limited information on timing or frequency, and its impact on the main findings needs further investigation in prospective studies. Future studies with larger cohorts (including both SSRI- and SNRI-exposed pregnancies), detailed longitudinal exposure data (including timing, duration, and dosage of medication use), and more specific physiological, behavioral, and maternal mental health measures (including stress, anxiety, and ability to function) across gestation are needed to further characterize the effects of prenatal SRI exposure and maternal psychological distress on fetal brain and placenta development. Longitudinal investigations are underway to explore the impact of fetal brain and placenta developmental changes associated with depression and SRI exposure on birth and long-term neurobehavioral outcomes.
Conclusions
In summary, this study provides novel insights into the association between prenatal SRI exposure, depressive symptom severity, and fetal brain and placenta development. These findings underscore the use of novel research tools to understand the contributions of both exposure to depressive symptoms and SRI treatment during pregnancy, which advances clinical decision-making aimed at improving both maternal health and offspring neurodevelopmental outcomes. Considering the well-established risks of untreated maternal depression, decisions regarding prenatal antidepressant use should be guided by clinical indications and individualized risk-benefit assessments, rather than structural imaging findings alone. These results highlight the need for longitudinal studies to examine the potential effects of prenatal SRI exposure and maternal depression on offspring neurodevelopment.
Data availability
The datasets generated and analyzed during the current study are available from the corresponding author on reasonable request.
References
Jha S, Salve HR, Goswami K, Sagar R, Kant S. Prevalence of common mental disorders among pregnant women—Evidence from population-based study in rural Haryana, India. J Fam Med Prim Care. 2021;10:2319.
Vesga-Lopez O, Blanco C, Keyes K, Olfson M, Grant BF, Hasin DS. Psychiatric disorders in pregnant and postpartum women in the United States. Arch Gen Psychiatry. 2008;65:805–15.
Wisner KL, Sit DKY, McShea MC, Rizzo DM, Zoretich RA, Hughes CL, et al. Onset timing, thoughts of self-harm, and diagnoses in postpartum women with screen-positive depression findings. JAMA Psychiatry. 2013;70:490.
Fenster L, Schaefer C, Mathur A, Hiatt RA, Pieper C, Hubbard AE, et al. Psychologic stress in the workplace and spontaneous abortion. Am J Epidemiol. 1995;142:1176–83.
Kurki T, Hiilesmaa V, Raitasalo R, Mattila H, Ylikorkala O. Depression and anxiety in early pregnancy and risk for preeclampsia. Obstet Gynecol. 2000;95:487–90.
Paarlberg, Vingerhoets KM, Passchier ADJJM, Dekker J, Van GA, Geijn HP. Psychosocial factors and pregnancy outcome: a review with emphasis on methodological issues. J Psychosom Res. 1995;39:563–95.
Lou HC, Hansen D, Nordentoft M, Pryds O, Jensen F, Nim J, et al. Prenatal stressors of human life affect fetal brain development. Dev Med Child Neurol. 1994;36:826–32.
Buss C, Davis EP, Muftuler LT, Head K, Sandman CA. High pregnancy anxiety during mid-gestation is associated with decreased gray matter density in 6–9-year-old children. Psychoneuroendocrinology. 2010;35:141–53.
Rifkin-Graboi A, Meaney MJ, Chen H, Bai J, Hameed WB, Tint MT, et al. Antenatal maternal anxiety predicts variations in neural structures implicated in anxiety disorders in newborns. J Am Acad Child Adolesc Psychiatry. 2015;54:313–21.
Wu Y, Lu Y-C, Jacobs M, Pradhan S, Kapse K, Zhao L, et al. Association of prenatal maternal psychological distress with fetal brain growth, metabolism, and cortical maturation. JAMA Netw Open. 2020;3:e1919940–e1919940.
Sandman CA, Buss C, Head K, Davis EP. Fetal exposure to maternal depressive symptoms is associated with cortical thickness in late childhood. Biol Psychiatry. 2015;77:324–34.
Wu Y, Kapse K, Jacobs M, Niforatos-Andescavage N, Donofrio MT, Krishnan A, et al. Association of maternal psychological distress with in utero brain development in fetuses with congenital heart disease. JAMA Pediatr. 2020;174:e195316.
Qiu A, Anh TT, Li Y, Chen H, Rifkin-Graboi A, Broekman BFP, et al. Prenatal maternal depression alters amygdala functional connectivity in 6-month-old infants. Transl Psychiatry. 2015;5:e508.
Wu Y, De Asis-Cruz J, Limperopoulos C. Brain structural and functional outcomes in the offspring of women experiencing psychological distress during pregnancy. Mol Psychiatry. 2024;29:2223–40.
Wu Y, Espinosa KM, Barnett SD, Kapse A, Quistorff JL, Lopez C, et al. Association of elevated maternal psychological distress, altered fetal brain, and offspring cognitive and social-emotional outcomes at 18 months. JAMA Netw Open. 2022;5:e229244–e229244.
Goodman SH, Rouse MH, Connell AM, Broth MR, Hall CM, Heyward D. Maternal depression and child psychopathology: a meta-analytic review. Clin Child Fam Psychol Rev. 2011;14:1–27.
Weissman MM, Wickramaratne P, Gameroff MJ, Warner V, Pilowsky D, Kohad RG, et al. Offspring of depressed parents: 30 years later. Am J Psychiatry. 2016;173:1024–32.
McDonald M, Alhusen J. A review of treatments and clinical guidelines for perinatal depression. J Perinat Neonatal Nurs. 2022;36:233–42.
Heinonen E, Blennow M, Blomdahl-Wetterholm M, Hovstadius M, Nasiell J, Pohanka A, et al. Sertraline concentrations in pregnant women are steady and the drug transfer to their infants is low. Eur J Clin Pharm. 2021;77:1323–31.
Bellantuono C, Vargas M, Mandarelli G, Nardi B, Martini MG. The safety of serotonin–noradrenaline reuptake inhibitors (SNRIs) in pregnancy and breastfeeding: a comprehensive review. Hum Psychopharmacol: Clin Exp. 2015;30:143–51.
Eke AC, Saccone G, Berghella V. Selective serotonin reuptake inhibitor (SSRI) use during pregnancy and risk of preterm birth: a systematic review and meta-analysis. BJOG. 2016;123:1900–7.
Dubovicky M, Belovicova K, Csatlosova K, Bogi E. Risks of using SSRI/SNRI antidepressants during pregnancy and lactation. Interdiscip Toxicol. 2017;10:30–34.
Lugo-Candelas C, Cha J, Hong S, Bastidas V, Weissman M, Fifer WP, et al. Associations between brain structure and connectivity in infants and exposure to selective serotonin reuptake inhibitors during pregnancy. JAMA Pediatr. 2018;172:525–33.
Rotem-Kohavi N, Williams LJ, Virji-Babul N, Bjornson BH, Brain U, Werker JF, et al. Alterations in resting-state networks following in utero selective serotonin reuptake inhibitor exposure in the neonatal brain. Biol Psychiatry Cogn Neurosci Neuroimag. 2019;4:39–49.
Jha SC, Meltzer-Brody S, Steiner RJ, Cornea E, Woolson S, Ahn M, et al. Antenatal depression, treatment with selective serotonin reuptake inhibitors, and neonatal brain structure: A propensity-matched cohort study. Psychiatry Res Neuroimag. 2016;253:43–53.
Koc D, Tiemeier H, Stricker BH, Muetzel RL, Hillegers M, El Marroun H. Prenatal antidepressant exposure and offspring brain morphologic trajectory. JAMA Psychiatry. 2023;80:1208.
Casper RC, Fleisher BE, Lee-Ancajas JC, Gilles A, Gaylor E, DeBattista A, et al. Follow-up of children of depressed mothers exposed or not exposed to antidepressant drugs during pregnancy. J Pediatr. 2003;142:402–8.
Oberlander TF, Gingrich JA, Ansorge MS. Sustained neurobehavioral effects of exposure to SSRI antidepressants during development: molecular to clinical evidence. Clin Pharm Ther. 2009;86:672–7.
Singal D, Chateau D, Dahl M, Derksen S, Ruth C, Katz L, et al. In-utero SSRI and SNRI exposure and the risk of neurodevelopmental disorders in children: a population-based retrospective cohort study utilizing linked administrative data. Int J Popul Data Sci. 2018;3:375.
Vlenterie R, van Gelder MMHJ, HR Anderson, Andersson L, Broekman BFP, Dubnov-Raz G, et al. Associations between maternal depression, antidepressant use during pregnancy, and adverse pregnancy outcomes. Obstet Gynecol. 2021;138:633–46.
Lattimore KA, Donn SM, Kaciroti N, Kemper AR, Neal CR, Vazquez DM. Selective serotonin reuptake inhibitor (SSRI) use during pregnancy and effects on the fetus and newborn: a meta-analysis. J Perinatol. 2005;25:595–604.
Morag I, Batash D, Keidar R, Bulkowstein M, Heyman E. Paroxetine use throughout pregnancy: does it pose any risk to the neonate? J Toxicol Clin Toxicol. 2004;42:97–100.
Morgan T. Role of the Placenta in Preterm Birth: A Review. Am J Perinatol. 2016;33:258–66.
Haizler-Cohen L, Limperopoulos C, Kapse K, Sharker Y, Lopez C, Andescavage NN. Quantitative MRI in placentas of pregnancies complicated by hypertensive disorders and fetal growth restriction. Am J Obstet Gynecol. 2023;228:S528–S529.
Talati A. Maternal Depression, Prenatal SSRI Exposure, and Brain Trajectories in Childhood. JAMA Psychiatry. 2023;80:1191.
Cox JL, Holden JM, Sagovsky R. Detection of postnatal depression: development of the 10-item Edinburgh Postnatal Depression Scale. Br J Psychiatry. 1987;150:782–6.
Evans J, Heron J, Francomb H, Oke S, Golding J. Cohort study of depressed mood during pregnancy and after childbirth. Bmj. 2001;323:257–60.
Levis B, Negeri Z, Sun Y, Benedetti A, Thombs BD Accuracy of the Edinburgh Postnatal Depression Scale (EPDS) for screening to detect major depression among pregnant and postpartum women: systematic review and meta-analysis of individual participant data. BMJ. 2020;371:m4022.
Areias ME, Kumar R, Barros H, Figueiredo E. Comparative incidence of depression in women and men, during pregnancy and after childbirth. Validation of the Edinburgh Postnatal Depression Scale in Portuguese mothers. Br J Psychiatry. 1996;169:30–35.
Mesches GA, Ciolino JD, Stika CS, Sit DK, Zumpf K, Fisher S, et al. Trajectories of depressive and anxiety symptoms across pregnancy and postpartum in selective serotonin reuptake inhibitor-treated women. Psychiatr Res Clin Pr. 2022;4:32–41.
Shafiee MJ, Chywl B, Li F, Wong A. Fast YOLO: A Fast You Only Look Once System for Real-time Embedded Object Detection in Video. 2017. 18 September 2017.
Kainz B, Steinberger M, Wein W, Kuklisova-Murgasova M, Malamateniou C, Keraudren K, et al. Fast volume reconstruction from motion corrupted stacks of 2D slices. IEEE Trans Med Imaging. 2015;34:1901–13.
Jenkinson M, Bannister P, Brady M, Smith S. Improved optimization for the robust and accurate linear registration and motion correction of brain images. Neuroimage. 2002;17:825–41.
Zhao L, Asis-Cruz JD, Feng X, Wu Y, Kapse K, Largent A, et al. Automated 3D fetal brain segmentation using an optimized deep learning approach. Am J Neuroradiol. 2022;43:448–54.
Çiçek Ö, Abdulkadir A, Lienkamp SS, Brox T, Ronneberger O. 3D U-Net: learning dense volumetric segmentation from sparse annotation. International conference on medical image computing and computer-assisted intervention, 2016. p. 424-32.
Dubois J, Benders M, Cachia A, Lazeyras F, Ha-Vinh Leuchter R, Sizonenko SV, et al. Mapping the early cortical folding process in the preterm newborn brain. Cereb Cortex. 2007;18:1444–54.
Tadayon E, Pascual-Leone A, Santarnecchi E. Differential contribution of cortical thickness, surface area, and gyrification to fluid and crystallized intelligence. Cereb Cortex. 2020;30:215–25.
Yun HJ, Im K, Yang J-J, Yoon U, Lee J-M. Automated sulcal depth measurement on cortical surface reflecting geometrical properties of sulci. PLoS One. 2013;8:e55977.
Koenderink JJ, van Doorn AJ. Surface shape and curvature scales. Image Vis Comput. 1992;10:557–64.
You W, Andescavage N, Zun Z, Limperopoulos C. Semi-automatic segmentation of the placenta into fetal and maternal compartments using intravoxel incoherent motion MRI. Medical Imaging 2017. Biomed Appl Mol, Struct, Funct Imaging. 2017;10137:1013726.
De Cobelli F, Ravelli S, Esposito A, Giganti F, Gallina A, Montorsi F, et al. Apparent diffusion coefficient value and ratio as noninvasive potential biomarkers to predict prostate cancer grading: comparison with prostate biopsy and radical prostatectomy specimen. Am J Roentgenol. 2015;204:550–7.
Benjamini Y, Hochberg Y. Controlling the false discovery rate: a practical and powerful approach to multiple testing. J R Stat Soc: Ser B (Methodol. 1995;57:289–300.
Wisner KL, Avram MJ, George AL, Abramova TV, Yang A, Caritis SN, et al. Concentrations of fluoxetine enantiomers decline during pregnancy and increase after birth. J Clin Psychopharmacol. 2024;44:100–6.
Stika CS, Avram MJ, George AL, Yang A, Ciolino JD, Jeong H, et al. Changes in s -citalopram plasma concentrations across pregnancy and postpartum. Clin Pharm Ther. 2025;118:106–17.
Stika CS, Wisner KL, George AL, Avram MJ, Zumpf K, Rasmussen-Torvik LJ, et al. Changes in sertraline plasma concentrations across pregnancy and postpartum. Clin Pharm Ther. 2022;112:1280–90.
Eichenbaum H. Hippocampus: cognitive processes and neural representations that underlie declarative memory. Neuron. 2004;44:109–20.
White T, Su S, Schmidt M, Kao C-Y, Sapiro G. The development of gyrification in childhood and adolescence. Brain Cogn. 2010;72:36–45.
Li G, Nie J, Wang L, Shi F, Lin W, Gilmore JH, et al. Mapping region-specific longitudinal cortical surface expansion from birth to 2 years of age. Cereb Cortex. 2013;23:2724–33.
Rommel A-S, Bergink V, Liu X, Munk-Olsen T, Molenaar NM. Long-term effects of intrauterine exposure to antidepressants on physical, neurodevelopmental, and psychiatric outcomes: a systematic review. J Clin Psychiatry. 2020;81:19r12965.
Hutchison SM, Mâsse LC, Pawluski JL, Oberlander TF. Perinatal selective serotonin reuptake inhibitor (SSRI) and other antidepressant exposure effects on anxiety and depressive behaviors in offspring: A review of findings in humans and rodent models. Reprod Toxicol. 2021;99:80–95.
Wisner KL. Pharmacologic Treatment of Depression During Pregnancy. JAMA. 1999;282:1264.
McDonagh M, Matthews A, Phillipi C, Romm J, Peterson K, Thakurta S, et al. Antidepressant treatment of depression during pregnancy and the postpartum period. Evid Rep Technol Assess. 2014;1:1–308.
Sarkar D, Mandal S, Bandyopadhyay S, Bose S, Parkash J, Singh SK. Use of serotonin reuptake inhibitors (SSRIs) and serotonin and norepinephrine reuptake inhibitors (SNRIs) during pregnancy: Effect on fetal growth and long-term reproductive outcomes. Reprod Toxicol. 2025;136:108960.
Sodhi MSK, Sanders-Bush E Serotonin and brain development 2004. 111–74.
Manganaro L, Fierro F, Tomei A, La Barbera L, Savelli S, Sollazzo P, et al. MRI and DWI: feasibility of DWI and ADC maps in the evaluation of placental changes during gestation. Prenat Diagn. 2010;30:1178–84.
Abdel Razek AAK, Thabet M, Salam EA. Apparent diffusion coefficient of the placenta and fetal organs in intrauterine growth restriction. J Comput Assist Tomogr. 2019;43:507–12.
Derwig I, Lythgoe DJ, Barker GJ, Poon L, Gowland P, Yeung R, et al. Association of placental perfusion, as assessed by magnetic resonance imaging and uterine artery Doppler ultrasound, and its relationship to pregnancy outcome. Placenta. 2013;34:885–91.
Andescavage N, You W, Jacobs M, Kapse K, Quistorff J, Bulas D, et al. Exploring in vivo placental microstructure in healthy and growth-restricted pregnancies through diffusion-weighted magnetic resonance imaging. Placenta. 2020;93:113–8.
Andescavage N, DuPlessis A, Metzler M, Bulas D, Vezina G, Jacobs M, et al. In vivo assessment of placental and brain volumes in growth-restricted fetuses with and without fetal Doppler changes using quantitative 3D MRI. J Perinatol. 2017;37:1278–84.
Ajwani S, Jamro EL, Taylor K, Wang Y, Mangin-Heimos K, Odibo AO, et al. Placental and fetal brain volumes in congenital heart disease are smallest among fetuses with genetic abnormalities. Prenat Diagn. 2025;45:1621–31.
Baldauf C, Rosas V, Zamiara P, Reynolds WT, Wang S, Tran N, et al. Placental hypoplasia and vascular malperfusion are associated with reduced brain volumes in fetal congenital heart disease. Pediatr Res. 2026. 7 January 2026. https://doi.org/10.1038/s41390-025-04698-3.
Suarez EA, Bateman BT, Hernández-Díaz S, Straub L, Wisner KL, Gray KJ, et al. Association of antidepressant use during pregnancy with risk of neurodevelopmental disorders in children. JAMA Intern Med. 2022;182:1149.
Roddy Mitchell A, Gordon H, Lindquist A, Walker SP, Homer CSE, Middleton A, et al. Prevalence of perinatal depression in low- and middle-income countries. JAMA Psychiatry. 2023;80:425.
Woody CA, Ferrari AJ, Siskind DJ, Whiteford HA, Harris MG. A systematic review and meta-regression of the prevalence and incidence of perinatal depression. J Affect Disord. 2017;219:86–92.
Latendresse G, Elmore C, Deneris A. Selective serotonin reuptake inhibitors as first-line antidepressant therapy for perinatal depression. J Midwifery Women’s Health. 2017;62:317–28.
Fleschler R, Peskin MF. Selective serotonin reuptake inhibitors (SSRIs) in pregnancy. MCN: Am J Matern/Child Nurs. 2008;33:355–61.
Scott JA, Habas PA, Kim K, Rajagopalan V, Hamzelou KS, Corbett-Detig JM, et al. Growth trajectories of the human fetal brain tissues estimated from 3D reconstructed in utero MRI. Int J Dev Neurosci. 2011;29:529–36.
Acknowledgements
We thank the participants in our study. We also thank our laboratory members for their contributions. This study was funded by A. James & Alice B. Clark Foundation.
Author information
Authors and Affiliations
Contributions
All authors made substantial contributions to this study. YW: Study design; data analysis and interpretation; drafting and revising the manuscript. NA: Study design; data acquisition and interpretation; revising the manuscript. KLW: Study design; data interpretation; revising the manuscript. KK: Data acquisition and preprocessing; revising the manuscript. JM: Data interpretation; revising the manuscript. JS.N: Statistical analysis support; revising the manuscript. CL: Study design; data acquisition and interpretation; revising the manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Wu, Y., Andescavage, N., Wisner, K.L. et al. Prenatal serotonin reuptake inhibitor exposure and maternal depression symptoms are associated with altered fetal brain and placental development. Neuropsychopharmacol. (2026). https://doi.org/10.1038/s41386-026-02436-9
Received:
Revised:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41386-026-02436-9
