
Abstract
Background and objective
High fasting plasma glucose (HFPG) is a major risk factor for diseases, posing a serious public health challenge. This study examines the global burden of 13 non-communicable diseases (NCDs) attributed to HFPG.
Methods
We used the 2021 GBD Study to analyze deaths and DALYs linked to HFPG( > 4.90–5.30 mmol/L). Socio-Demographic Index (SDI) was used to assess development levels, with subgroup analyses by geography, year, gender, and SDI.
Results
In 2021, HFPG contributed to 5.15 million deaths and 151.95 million DALYs globally. From 1990 to 2021, the estimated annual percentage change (EAPC) in deaths and DALYs were 0.11 and 0.55, respectively. Diabetes, ischemic heart disease (IHD), and stroke accounted for the most deaths (1.66, 1.35, and 0.84 million). Liver cancer, chronic kidney disease (CKD), and pancreatic cancer showed the fastest mortality increases, with EAPCs of 1.90, 1.69, and 1.34, respectively. IHD and stroke had declining mortality burdens, with EAPCs of -0.13 and -0.98.
Conclusion
Over 30 years, HFPG-related NCDs have increased globally. Diabetes, IHD, and stroke remain the top burdens, while liver cancer, CKD, and pancreatic cancer are rising fastest. The disease burden in men is higher than in women, except for people with Alzheimer’s disease and other dementias and people with blindness and vision loss (BVL).
Similar content being viewed by others
Introduction
Glucose is the primary source of energy for human life activities, involved in human biosynthesis and metabolism [1]. The stability of glucose metabolism is crucial for maintaining health [2]. High fasting plasma glucose (HFPG) is an independent risk factor not only for communicable diseases, such as tuberculosis [3] but also for various non-communicable diseases (NCDs), including cardiovascular diseases (CVD), cancer, chronic kidney disease (CKD), and disorders of the central nervous system [4,5,6]. Since 1980, global fasting blood glucose levels have shown a decade-on-decade increase of approximately 0.09 millimoles per liter in women and 0.07 millimoles per liter in men [7]. Furthermore, driven by population growth and an aging demographic, the global number of adults living with diabetes reached an estimated 828 million in 2022, an increase of 630 million since 1990 [8]. In 2019, the number of deaths caused by CVD, CKD, and cancer due to HFPG were 3.76 million, 0.48 million, and 0.41 million, respectively. The DALYs lost were 72.59, 13.09, and 8.60 million, respectively [9,10,11].
In recent years, the increased public awareness of diabetes prevention and control, the popularization of basic hypoglycemic drugs, and the emergence of new hypoglycemic drugs have provided more means for blood glucose control at normal physiological levels [12, 13]. Hence, investigating the disease burden attributed to various types of NCDs caused by HFPG is essential. Such studies can contribute valuable data to guide the optimal assignment of health-care resources and help global health authorities to develop effective prevention and control strategies.
The GBD 2021 study, which analyzes trends in the burden of disease over the past three decades, provides a comprehensive framework for assessing the impact of NCDs resulting from HFPG in different regions of the globe [14]. We utilized the comprehensive statistical models from the 2021 GBD to assess mortality and DALYs caused by HFPG-related NCDs. Additionally, we analyzed the trends in disease burden over these 30 years across different genders, ages, and regions.
Methods
Data sources
371 health risk burdens associated with diseases and injuries, and 88 risk factors were assessed in the 2021 GBD data [15]. The research involved over 11,500 contributors from 164 countries, who comprehensively assessed the global health situation and the burden of disease by providing data, conducting analyses, and performing reviews. GBD 2021 employed the disease model-bayesian meta-regression (DisMod-MR) 2.1 model for non-fatal disease burden estimation, the cause of death ensemble modeling (CODEm) model for cause-of-death estimation, the spatiotemporal Gaussian process regression (ST-GPR) model to impute estimates for locations with missing data, and the comparative risk assessment (CRA) framework to quantify risk-factor effects. The accompanying papers for GBD 2021 provide a detailed introduction to the data inputs, processing, synthesis, and final modeling used for predicting the burden of disease [15, 16].
Definition
HFPG is defined as fasting plasma glucose (FPG) levels above the theoretical minimum-risk exposure threshold (TMREL) of 4.90–5.30 mmol/L, measured as a continuous variable. This study encompassed 13 NCDs across six major categories: neoplasms (including colon and rectum cancer, liver cancer, pancreatic cancer, tracheal, bronchial, and lung cancer, breast cancer, and bladder cancer), cardiovascular diseases (CVDs), such as ischemic heart disease (IHD), stroke, and lower extremity peripheral arterial disease (LEPAD), neurological diseases like Alzheimer’s disease and other dementias, diabetes mellitus (DM), chronic kidney diseases (CKD), and sense organ diseases including blindness and vision loss (BVL). Detailed disease definitions are provided in Supplementary Material. Drawing on similarities in geography, epidemiology, and cause-of-death profiles, the GBD study divides 204 countries and territories into 21 regions to enable comparative analyses of regional health patterns and trends. To investigate how socioeconomic development influences disease burden, these regions and countries are further stratified into five Socio-demographic Index (SDI) regions. The SDI, a composite index based on income, education, and fertility rates [14], quantifies regional economic development levels. Higher SDI values indicate greater development. This study categorizes SDI into five tiers: low, low-middle, middle, high-middle, and high.
Estimation of disease burden
Death data is estimated based on data from verbal autopsies, censuses, surveys, vital registration, surveillance systems, and cancer registries. For locations where mortality data is lacking, mortality-to-incidence ratio models are utilized to extrapolate death estimates from incidence data. To estimate disability-adjusted life years (DALYs) for GBD 2021, we first estimate the mortality rates and non-fatal health losses for each cause. DALYs are computed by aggregating the years of life lost (YLL) and the years lived with disability (YLD) for each specific age, sex, and location group. The 95% uncertainty intervals (UIs) for YLLs and YLDs are derived from 500 simulation draws using the percentile method (2.5th–97.5th percentiles). GBD 2021 generates these by iteratively sampling input data distributions, transformation parameters, and model specifications. Uncertainty quantification is embedded throughout the analytic pipeline. DALYs are the sum of YLL and YLD for each cause, age group, location, year and sex [14, 15].
Statistical analysis
The following formula is to compute the age-standardized rate (ASR) per 100,000 people [17]:
αi denotes the rate unique to the i-th age group, while Wᵢ signifies the count of individuals in that age group based on the GBD 2021 standard population. The standard population was constructed using the unweighted average of the age-specific proportional distributions from countries and territories with populations exceeding 5 million in 2021 [18]. To assess temporal trends, we calculated the estimated annual percentage change (EAPC) in ASR using linear regression on the natural log-transformed ASR. The formula is [19]:
x represents the calendar year, α is the intercept, and ϵ is the random error term. The β in the (2) and (3) formulas represent the annual rate of change and the regression coefficient obtained from the log-linear model, respectively. The 95% confidence interval (CI) of EAPC was calculated as:
where \({t}_{0.975}^{{df}}\) is the t-distribution critical value, and df=n − 2(n=years). If the 95% CI does not include 0, it indicates that the trend is statistically significant.
Spearman’s correlation analysis was used to calculate the coefficient of correlation (r) and p-value among the burden of disease indicators and the SDI. To visualize global disparities in disease burden, we mapped the data according to GBD-defined regions. We utilized the R software package (version 4.2.3) in combination with JD_GBDR (developed by Jingding Medical Technology Co., Ltd.) to generate the charts.
Results
Global, regional, and national burden of NCDs
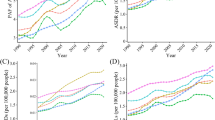
Globally, in 2021, HFPG-related NCDs accounted for an estimated 5.15 million deaths globally (95% UI: 4.37–5.94 million). Equivalent ASDR is 62.01 per 100,000 people. Additionally, these conditions resulted in approximately 151.95 million DALYs (95% UI: 129.02–175.49 million), with an DALYs rate(age-standardized) of 1,775.66 years per 100,000 population. (Table 1). From 1990 to 2021, global ASDR and DALY rates increased by EAPCs of 0.11 and 0.55, respectively. The low-middle SDI region had the highest rates (85.25 and 2337.33) with EAPCs of 1.13 and 1.23, while the high SDI region had the lowest ASDR (41.67) with a -0.87 EAPC. (Table 1 and Fig. S1). Among 21 GBD regions, Southern Sub-Saharan Africa has the highest EAPC for ASDR (2.12) and age-standardized DALY rate (2.05), while High-income Asia Pacific has the lowest EAPC for ASDR (-2.12) and Australasia for DALY rate(age-standardized) (-0.65) (Table 1 and Fig. 1). Moreover, SDI exhibits a significant negative correlation with ASDR(R = -0.57, P < 0.01) and DALYs rates(age-standardized)(R = -0.54, P < 0.01) across the 21GBD regions (Figure S2). In 2021, among 204 countries and regions, The highest ASDR of 409.34 (95%UI: 330.11, 504.27) and age-standardized DALYs rate of 10,504.66 (95%UI: 8515.21, 12,988.41) were observed in Fiji (Fig. S3 and Table S1-2). Over the past 30 years, Lesotho has had the highest EAPC for both ASDR(3.71) and age-standardized DALYs rates(3.74). (Figure S4 and Table S1-2). Similarly, there is a negative association between SDI and both ASDR(R = -0.43, P < 0.01) and DALYs rates(age-standardized) (R = -0.39, P < 0.01)in 204 different countries and regions (Fig. S5). Over the past 30 years, globally and across the five SDI regions, males have consistently had higher ASDR and DALYs rates compared to females. Around 2005, there was a notable decrease in ASDR in two SDI regions(high and high-middle) (Fig. S6). In contrast, age-standardized DALYs rates have risen notably in middle- and low-middle SDI regions. (Figure S7). From Fig. S8, It can be visualized that both mortality and DALYs rates increase with age and are higher for males than females in practically every age category (Table S3).

The estimated annual percentage change in age-standardized death rate and DALY rate for non-communicable diseases in global, 5SDI and 21 regions from 1990 to 2021.
Global, regional, and national burden of neoplasms
Globally in 2021, HFPG-attributable neoplasms caused 0.33 million deaths (ASDR: 3.88; EAPC: 0.87) and 7.05 million DALYs (age-standardized rate: 81.35; EAPC: 0.77) (Table S4). Pancreatic cancer showed the highest mortality burden among six neoplasms (0.13 million deaths; ASDR 1.57), while liver cancer had the fastest-growing burden (EAPC 1.90) (Table S12). Neoplasm ASDR/DALY rates rose with SDI (peaking at 5.72/118.39 in high-SDI regions), with fastest 30-year growth in low-middle SDI areas (EAPCs: 2.32/2.30) (Table S4). Among the 21 GBD regions, Central Europe had the highest ASDR (7.33) and DALYs rate (157.66). North Africa and the Middle East showed the fastest ASDR growth (EAPC: 2.75), while Southern Sub-Saharan Africa had the highest DALYs growth (EAPC: 2.73). In contrast, High-income Asia Pacific exhibited a decline -0.16 EAPC DALYs rate (Table S4). Among 204 countries and regions, the highest EAPC for ASDR was in Egypt at 5.70 (Fig. S9 and Table S10). For the DALYs rate, the highest EAPC was in Lesotho at 5.75 (Fig. S10 and Table S10).
Global, regional, and national burden of CVD
Globally, in 2021, HFPG-related CVD caused 2.21 million deaths (ASDR: 26.85, EAPC: -0.47) and 42.95 million DALYs (rate: 504.57, EAPC: -0.34). (Table S5). Among three CVDs, IHD showed the highest mortality burden (1.35million deaths; ASDR 16.27). While IHD and stroke burdens declined, LEPAD increased (EAPC: 0.44) (Table S12).The high SDI region has the lowest disease burden and the sharpest decline, with 2021 ASDR and DALY rates of 15.66 and 295.18, and EAPCs of -2.12 and -1.87. (Table S5). Among the 21 GBD regions, North Africa and the Middle East had the highest ASDR (57.06) and DALYs rate (1037.04), while High-income Asia Pacific had the lowest (ASDR: 8.30; DALYs: 155.76). High-income Asia Pacific showed the sharpest decline (EAPC: -3.69 for ASDR; -3.29 for DALYs), whereas Southern Sub-Saharan Africa experienced the largest increase (EAPC: 1.65 for ASDR; 1.67 for DALYs). (Table S5). Lesotho showed the highest EAPCs for both ASDR (4.09) and age-standardized DALY rates (4.36) among 204 countries/regions (Figs. S9-S10, Table S10).
Global, regional, and national burden of Alzheimer’s disease and other dementias
Globally, in 2021, HFPG-related Alzheimer’s disease and other dementias caused 0.29 million deaths (ASDR: 3.73, EAPC: 1.20) and 5.35 million DALYs (rate: 66.42, EAPC: 1.18). (Table S6). Across SDI regions, disease burden trended upward. ASDR (4.27) and DALYs rates (75.11) are highest in high SDI area. The Low-middle SDI region showed the greatest increases in ASDR(EAPC:1.72) and DALYs rate(EAPC:1.55) (Table S6). Among the 21 GBD regions, High-income North America had the highest ASDR (5.66) and DALYs rate(age-standardized) (99.65) in 2021, while Central Asia had the fastest growth (EAPC: 2.44 for ASDR; 2.50 for DALYs). (Table S6). Among the 204 countries and regions, Georgia has the highest EAPC for both ASDR and DALYs rate(age-standardized), with 3.50 and 3.39, respectively (Fig. S9-10 and Table S10).
Global, regional, and national burden of DM
In 2021, HFPG-induced DM caused 1.66 million global deaths (ASDR: 19.61, EAPC: 0.16) and 78.93 million DALYs (rate: 916.14, EAPC: 0.94) (Table S7). High SDI regions had the lowest ASDR at 9.35, with the most significant decline (EAPC: -1.54). Conversely, low-middle SDI regions had the highest DALYs rate(age-standardized) at 1259.54, showing the greatest increase (EAPC: 1.33) (Table S7). In the 21 GBD regions, the highest and lowest ASDR in 2021 were in Oceania (109.64) and High-income Asia Pacific (3.96), respectively. The region with the most significant decline in disease burden trend was High-income Asia Pacific, with an EAPC of -2.97. The highest and lowest DALYs rates(age-standardized) were in Oceania (3585.13) and Australasia (471.73), respectively. The region with the most significant increase in DALYs burden trend was Southern Sub-Saharan Africa, with an EAPC of 2.13 (Table S7). Mauritius had the highest EAPC in ASDR (3.80), while Lesotho led in age-standardized DALYs EAPC (3.54) among 204 countries/regions (Figs. S9-S10, Table S10)
Global, regional, and national burden of CKD
Globally, in 2021, HFPG-related CKD led to 0.66 million deaths (ASDR: 7.95, EAPC: 1.69) and 15.99 million DALYs (rate: 187.46, EAPC: 1.37) (Table S8). In 2021, the highest ASDR and DALY rates were in low (9.98) and low-middle SDI regions (234.50). The fastest increases occurred in high SDI regions, with EAPCs of 2.89 and 2.35, respectively. (Table S8). In the 21 GBD regions, the highest and lowest ASDR in 2021 were in Andean Latin America (20.43) and Eastern Europe (1.66), respectively. The region with the highest DALYs rate(age-standardized) was Central Latin America (481.14), while the lowest was in Eastern Europe (56.35). The region with the most significant increase in disease burden was High-income North America, with an EAPC of 5.14 for ASDR and 4.14 for DALYs rates(age-standardized). (Table S8). Among 204 countries/regions, Ukraine ranked highest in ASDR EAPC (14.25) and Lesotho in age-standardized DALYs EAPC (4.81) (Figs. S9,S10, Table S10).
Global, regional, and national burden of BVL
In 2021, the global DALYs, DALYs rate(age-standardized), and EAPC due to HFPG-induced BVL were: 1.67 million, 19.72, and 0.61, respectively (Table S9). Among the five SDI regions, the highest DALY rate is in low-middle SDI (44.80), while high-middle SDI shows the largest increase (EAPC: 0.97). (Table S9). Among the 21 GBD regions, the highest and lowest DALYs rates(age-standardized) were found in South Asia (53.98) and High-income Asia Pacific (4.29), respectively. The most notable increase was in High-income North America (EAPC:1.89) (Table S9). Among the 204 countries and regions, the EPAC for DALYs rate(age-standardized) is highest in Luxembourg (2.89) (Figs. S10 and Table S10).
Temporal trends, regional disparities, and gender differences in various NCDs
Globally, from 1990 to 2021, CVD triggered by HFPG has been the disease with the persistently highest ASDR, and DM triggered by HFPG has been the disease with the persistently highest age-standardized DALYs rate. Moreover, the burden of DALYs caused by DM is on an upward trend (Fig. 2). From the perspective of different SDI regions, the mortality rates of five different types of NCDs have shown varying degrees of increase over these 30 years, with the exception of CVD and DM, which have seen a decline in regions with High-middle SDI and High SDI (Fig. S11). The DALYs rates have generally shown an increasing trend as well, except for CVD, which has also experienced a decline in High-middle SDI and High SDI regions (Fig. S12). Among different genders, both mortality rates and DALYs rates gradually increase with age (Figs. S13-14 and Table S11).

Trends in age-standardized death rate and DALY rate for six types of non-communicable diseases from 1990 to 2021 globally.
In 2021, the top three NCDs by ASDR were DM (19.61), IHD (16.27), and stroke (10.26). Except for Alzheimer’s disease and other dementias, ASDR was higher in males. Over three decades, liver cancer, CKD, and pancreatic cancer showed the highest ASDR increases (EAPCs: 1.90, 1.69, 1.34), while IHD and stroke declined (EAPCs: -0.13, -0.98). (Table S12). Among the 13 NCDs, DM, IHD, and stroke lead in age-standardized DALYs (916.14, 303.49, and 194.35, respectively). Except for dementia and BVL, which are higher in females, all other diseases have higher rates in males. Liver cancer, CKD, and pancreatic cancer show the highest DALY increases (EAPCs: 1.65, 1.37, 1.22). (Table S13).
In the 5 SDI regions, DM is the leading cause of death burden in middle, low-middle, and low SDI regions, while IHD is the top cause in high and high-middle SDI regions. (Fig. 3 and Table S14). In the 21 GBD regions, DM or IHD predominantly account for the highest death burden, with the exception of East Asia, where stroke is the leading cause, and the High-income Asia Pacific region, where Alzheimer’s disease and other dementias take the lead (Fig. 3 and Table S14). The disease with the highest disability burden is DM across all five SDI and 21 GBD regions (Fig. S15 and Table S14).

“NO” refers to the number of deaths, and different colors represent different ranges of death rates.
Discussion
The results of this systematic analysis indicate that the overall burden of NCDs attributable to HFPG has been on an upward trend globally. However, the burden of mortality has been declining in regions with higher SDI quintiles. The disease burden is greater in males than in females. Among various types of NCDs, CVD and DM have the highest burdens in mortality and DALYs, respectively. CKD shows the greatest increase, while CVD is the only condition declining. Pancreatic cancer has the highest disease burden among neoplasms, while liver cancer shows the fastest increase.
In line with the earlier studies [20], the global burden of NCDs due to HFPG is rising, with CVD, DM, and CKD leading in deaths and DALYs. Only CVD (IHD and stroke) shows a declining trend, especially in economically developed regions. The overall burden is expected to keep increasing. In the future, it is expected that the global disease burden of NCDs will continue to rise. Due to socio-economic progress and the reduction in the burden of infectious diseases, leading to a sharp decline in related mortality rates, this trend is ongoing in developing regions [21]. These improvements bring new challenges—namely, an aging population. According to estimates, the proportion of the global population aged 65 and older will rise from 10% in 2024 to over 16% by 2050 [22]. The rapid increase in the elderly population has led to a higher incidence of NCDs, such as CKD, hypertension, diabetes, and tumors [22, 23]. Regional disparities in diet, lifestyle, and healthcare levels also play varying roles in the increase of the burden of NCDs [24, 25]. Among the various NCDs, only CVD shows a declining trend in mortality and DALYs rates. This trend is mainly observed in IHD and stroke. The improvement in these conditions is attributed to a combination of lifestyle interventions, risk factor management, and efficient medical care [26]. For example, the decline in smoking rates and the widespread use of antihypertensive medications [27, 28]. People often pay less attention to neoplasms associated with HFPG. However, our research found that in 2021, six types of malignant tumors caused 328,308.88 deaths, with pancreatic cancer causing the most deaths at 132,753.26, and liver cancer had the fastest growth rate in mortality, reaching an annual increase of 1.9%. Hyperglycemia, as a controllable risk factor for malignant tumors [29, 30], to reduce the burden of tumor diseases it causes, individuals and health administrative departments should strengthen the control of diabetes-related risk factors (obesity, smoking, low physical activity, etc.) and increase the rate of early diagnosis and treatment of cancer in the future [31, 32]. Dementia is the leading cause of disability among older adults, imposing a significant burden on individuals, families, and healthcare systems [33]. Although the exact causes are not yet known, there is a close association with obesity, diabetes, smoking, and alcohol consumption [34]. Globally, in 2021, the number of deaths and DALYs attributed to Alzheimer’s disease and other dementias related to HFPG ranks just after DM, IHD, stroke, and CKD among the 13 leading NCDs. With the aging population surge, dementia-related disease burden is projected to rise persistently, necessitating targeted interventions including: enhanced insurance incentives, dementia-inclusive communities, and healthy aging initiatives [33, 35].
DM from HFPG dominates global disease burden but shows the lowest mortality rise among growing NCDs (EAPC: 0.16), likely due to controllable progression mechanisms like hypoglycemic drugs, risk factor management, and lifestyle/dietary interventions [36]. The prevalence of this controllable approach is higher in economically developed areas, resulting in a downward trend in mortality rates in high-middle and high SDI regions. HFPG-related CKD ranks second among the 13 NCDs in terms of the rate of increase in mortality and DALYs. As a common complication of diabetes, kidney disease related to diabetes affects two-fifths of people with diabetes and is a leading cause of end-stage kidney disease [37]. CVDs are the leading cause of death among people living with diabetes, and CKD further increases the overall risk of CVD [38]. The interplay between cardiovascular, renal, and metabolic factors ultimately leads to significant multi-organ dysfunction and a markedly elevated risk of adverse cardiovascular events [39]. Although BVL does not directly cause death, they restrict an individual’s ability to engage in social production activities, ultimately leading to a serious burden on healthcare and socio-economic development [40, 41]. Cataracts, refractive errors, glaucoma, age-related macular degeneration, and diabetes-related retinopathy are the main causes of global vision impairment [42]. Diabetes is a risk factor for all of these conditions except refractive errors [43, 44]. In the future, with the intensification of population aging and the increase in the number of DM, the burden of disease caused by BVL is forecast to remain on the rise.
With an aging population, HFPG-related NCDs are expected to rise. However, economic growth, medical advances, and public health policies may slow increases in mortality and disability rates. This decline is closely linked to economic development, with DM, IHD, and stroke showing slower increases in developed regions. These three diseases also rank highest in disease burden in most regions. However, in the High-income Asia Pacific, Alzheimer’s disease and other dementias rank first in terms of mortality. Therefore, when formulating public health policies, it is essential to take targeted measures based on the regional differences in the disease spectrum. Among 13 types of NCDs, the disease burden for males is generally higher than for females, with the exception of burden among people with Alzheimer’s disease and other dementias, and people with BVL. When developing disease prevention and control strategies and conducting mechanism research, the gender differences in disease burden across different types of diseases need to be taken into comprehensive consideration.
Using 2021 GBD data, this study comprehensively evaluates the global burden of 13 HFPG-related NCDs, offering critical evidence for epidemiological research and health policy development. However, it also has certain limitations. Firstly, the insufficiency of data sources, particularly in low SDI regions, can affect the accuracy of disease burden estimates. Secondly, HFPG often coexists with obesity, hyperlipidemia, hypertension, and other conditions, making it difficult to distinguish its independent effect on certain NCDs, such as IHD and stroke. Thirdly, there is a lack of estimation for the disease burden of other NCDs, such as atrial fibrillation, heart failure, and autonomic neuropathy.
Future policy and research directions
To reduce the disease burden caused by HFPG, future policy-making should adopt a multi-faceted approach encompassing prevention, screening, treatment, and rehabilitation. For example, implementing a national sugar-reduction plan could involve taxing sugary drinks and restricting the marketing of junk food. Encourage physical activity and expand free public sports facilities. Strengthen diabetes screening through regular blood-glucose checks for high-risk groups, improving primary-care capacity, and issuing community screening guidelines. On the therapeutic front: guarantee broad coverage of essential glucose-lowering drugs for people who need them, intensify research and development for novel antidiabetic agents, and implement multidisciplinary, integrated care. Because low- to middle-SDI regions bear the heaviest disease burden from HFPG, we should channel medical resources toward them to secure universal, affordable access to these medications for their populations. Concurrently, develop region-specific, composite intervention packages tailored to local realities. Investigate the pathogenesis of HFPG-related liver and pancreatic cancers and develop novel therapeutics to reduce incidence at its source. Given the sex-specific differences in disease burden, future work must dissect the underlying biological mechanisms that drive these disparities. Meanwhile, region-specific evaluations of intervention effectiveness should be conducted using real-world data, delivering low-cost, high-efficiency, and readily implementable solutions that provide robust, evidence-based guidance tailored to the economic realities of each area.
Conclusion
From 1990 to 2021, the global HFPG-related NCD burden increased, led by DM, IHD, and stroke. Liver cancer, CKD, and pancreatic cancer showed the fastest growth, while DM (in high and high-middle SDI), IHD, and stroke declined. The disease burden in men is higher than in women, except for people with Alzheimer’s disease and other dementias, and people with BVL.
Availability of data and materials
The data can be downloaded from “https://vizhub.healthdata.org/gbd-results/”.
References
Mulukutla BC, Yongky A, Le T, Mashek DG, Hu WS. Regulation of glucose metabolism - a perspective from cell bioprocessing. Trends Biotechnol. 2016;34:638–51.
Wat LW, Svensson KJ. Novel secreted regulators of glucose and lipid metabolism in the development of metabolic diseases. Diabetologia. 2024;67:2626–36.
Ngo MD, Bartlett S, Ronacher K. Diabetes-associated susceptibility to tuberculosis: contribution of hyperglycemia vs. dyslipidemia. Microorganisms. 2021;9:2282.
Wong ND, Sattar N. Cardiovascular risk in diabetes mellitus: epidemiology, assessment and prevention. Nat Rev Cardiol. 2023;20:685–95.
Ilic I, Jakovljevic V, Zivanovic Macuzic I, Ravic-Nikolic A, Ilic M, Sorak M, et al. Trends in global burden of Alzheimer’s disease and other dementias attributable to high fasting plasma glucose, 1990-2021. Medicina. 2024;60:1783.
Chen J, Li C, Bu C, Wang Y, Qi M, Fu P, et al. Global burden of non-communicable diseases attributable to kidney dysfunction with projection into 2040. Chin Med J (Engl). 2025;138:1334–44.
Danaei G, Finucane MM, Lu Y, Singh GM, Cowan MJ, Paciorek CJ, et al. National, regional, and global trends in fasting plasma glucose and diabetes prevalence since 1980: systematic analysis of health examination surveys and epidemiological studies with 370 country-years and 2·7 million participants. Lancet. 2011;378:31–40.
(NCD-RisC) NRFC. Worldwide trends in diabetes prevalence and treatment from 1990 to 2022: a pooled analysis of 1108 population-representative studies with 141 million participants. Lancet. 2024;404:2077–93.
Dong XJ, Zhang XQ, Wang BB, Hou FF, Jiao Y. The burden of cardiovascular disease attributable to high fasting plasma glucose: findings from the global burden of disease study 2019. Diabetes Metab Syndr. 2024;18:103025.
Wei H, Ren J, Li R, Qi X, Yang F, Li Q. Global, regional, and national burden of chronic kidney disease attributable to high fasting plasma glucose from 1990 to 2019: a systematic analysis from the global burden of disease study 2019. Front Endocrinol. 2024;15:1379634.
Safiri S, Nejadghaderi SA, Karamzad N, Kaufman JS, Carson-Chahhoud K, Bragazzi NL, et al. Global, regional and national burden of cancers attributable to high fasting plasma glucose in 204 countries and territories, 1990-2019. Front Endocrinol. 2022;13:879890.
Zhang J, Xu S, Liu X, Zhang J, Hu S, Liu X, et al. Time trends and regional variation in utilization of antidiabetic medicines in China, 2015-2022. Diabetes Obes Metab. 2024;26:2752–60.
Park J, Kim G, Kim BS, Han KD, Kwon SY, Park SH, et al. Insulin fact sheet in type 1 and 2 diabetes mellitus and trends of antidiabetic medication use in insulin users with type 2 diabetes mellitus: 2002 to 2019. Diabetes Metab J. 2023;47:211–9.
Collaborators G2DaI. Global incidence, prevalence, years lived with disability (YLDs), disability-adjusted life-years (DALYs), and healthy life expectancy (HALE) for 371 diseases and injuries in 204 countries and territories and 811 subnational locations, 1990-2021: a systematic analysis for the Global Burden of Disease Study 2021. Lancet. 2024;403:2133–61.
GBD 2021 Causes of Death Collaborators. Global burden of 288 causes of death and life expectancy decomposition in 204 countries and territories and 811 subnational locations, 1990-2021: a systematic analysis for the Global Burden of Disease Study 2021. Lancet. 2024;403:2100–32.
GBD 2021 Risk Factors Collaborators. Global burden and strength of evidence for 88 risk factors in 204 countries and 811 subnational locations, 1990-2021: a systematic analysis for the Global Burden of Disease Study 2021. Lancet. 2024;403:2162–203.
Sun P, Yu C, Yin L, Chen Y, Sun Z, Zhang T, et al. Global, regional, and national burden of female cancers in women of child-bearing age, 1990-2021: analysis of data from the global burden of disease study 2021. EClinicalMedicine. 2024;74:102713.
GBD 2021 Demographics Collaborators. Global age-sex-specific mortality, life expectancy, and population estimates in 204 countries and territories and 811 subnational locations, 1950-2021, and the impact of the COVID-19 pandemic: a comprehensive demographic analysis for the Global Burden of Disease Study 2021. Lancet. 2024;403:1989–2056.
Yang X, Chen H, Zhang T, Yin X, Man J, He Q, et al. Global, regional, and national burden of blindness and vision loss due to common eye diseases along with its attributable risk factors from 1990 to 2019: a systematic analysis from the global burden of disease study 2019. Aging. 2021;13:19614–42.
Ye L, Xu J, Zhang T, Lin X, Pan X, Zeng W, et al. Global burden of noncommunicable diseases attributable to high fasting plasma glucose. J Diabetes. 2020;12:807–18.
Hambleton IR, Caixeta R, Jeyaseelan SM, Luciani S, Hennis A. The rising burden of non-communicable diseases in the Americas and the impact of population aging: a secondary analysis of available data. Lancet Reg Health Am. 2023;21:100483.
Chesnaye NC, Ortiz A, Zoccali C, Stel VS, Jager KJ. The impact of population ageing on the burden of chronic kidney disease. Nat Rev Nephrol. 2024;20:569–85.
Xi JY, Lin X, Hao YT. Measurement and projection of the burden of disease attributable to population aging in 188 countries, 1990-2050: a population-based study. J Glob Health. 2022;12:04093.
Aslam MZ, Trail M, Cassell AK, Khan AB, Payne S. Establishing a sustainable healthcare environment in low- and middle-income countries. BJU Int. 2022;129:134–42.
Allen L, Williams J, Townsend N, Mikkelsen B, Roberts N, Foster C, et al. Socioeconomic status and non-communicable disease behavioural risk factors in low-income and lower-middle-income countries: a systematic review. Lancet Glob Health. 2017;5:e277–e289.
Campbell N, Ordunez P, Giraldo G, Rodriguez Morales YA, Lombardi C, Khan T, et al. WHO HEARTS: a global program to reduce cardiovascular disease burden: experience implementing in the Americas and opportunities in Canada. Can J Cardiol. 2021;37:744–55.
GBD 2019 Tobacco Collaborators. Spatial, temporal, and demographic patterns in prevalence of smoking tobacco use and attributable disease burden in 204 countries and territories, 1990-2019: a systematic analysis from the Global Burden of Disease Study 2019. Lancet. 2021;397:2337–60.
Mills KT, Stefanescu A, He J. The global epidemiology of hypertension. Nat Rev Nephrol. 2020;16:223–37.
Klein AP. Pancreatic cancer epidemiology: understanding the role of lifestyle and inherited risk factors. Nat Rev Gastroenterol Hepatol. 2021;18:493–502.
Ghareghomi S, Arghavani P, Mahdavi M, Khatibi A, García-Jiménez C, Moosavi-Movahedi AA. Hyperglycemia-driven signaling bridges between diabetes and cancer. Biochem Pharm. 2024;229:116450.
Ismail L, Materwala H, Al Kaabi J. Association of risk factors with type 2 diabetes: A systematic review. Comput Struct Biotechnol J. 2021;19:1759–85.
Yang J, Xu R, Wang C, Qiu J, Ren B, You L. Early screening and diagnosis strategies of pancreatic cancer: a comprehensive review. Cancer Commun. 2021;41:1257–74.
Gaugler JE, Borson S, Epps F, Shih RA, Parker LJ, McGuire LC. The intersection of social determinants of health and family care of people living with Alzheimer’s disease and related dementias: a public health opportunity. Alzheimers Dement. 2023;19:5837–46.
Cao X, Wang M, Zhou M, Mi Y, Fazekas-Pongor V, Major D, et al. Trends in prevalence, mortality, and risk factors of dementia among the oldest-old adults in the United States: the role of the obesity epidemic. Geroscience. 2024;46:4761–78.
Fleming R, Bennett K, Preece T, Phillipson L. The development and testing of the dementia friendly communities environment assessment tool (DFC EAT). Int Psychogeriatr. 2017;29:303–11.
Gregg EW, Buckley J, Ali MK, Davies J, Flood D, Mehta R, et al. Improving health outcomes of people with diabetes: target setting for the WHO global diabetes compact. Lancet. 2023;401:1302–12.
Pereira PR, Carrageta DF, Oliveira PF, Rodrigues A, Alves MG, Monteiro MP. Metabolomics as a tool for the early diagnosis and prognosis of diabetic kidney disease. Med Res Rev. 2022;42:1518–44.
Hahr AJ, Molitch ME. Management of diabetes mellitus in patients with CKD: core curriculum 2022. Am J Kidney Dis. 2022;79:728–36.
Ndumele CE, Rangaswami J, Chow SL, Neeland IJ, Tuttle KR, Khan SS, et al. Cardiovascular-kidney-metabolic health: a presidential advisory from the American Heart Association. Circulation. 2023;148:1606–35.
Mannava S, Borah RR, Shamanna BR. Current estimates of the economic burden of blindness and visual impairment in India: a cost of illness study. Indian J Ophthalmol. 2022;70:2141–5.
Zhao C, Ding Q, Yang Z. Burdens and trends of blindness and vision loss among those aged 55 years and older: a systematic analysis for the Global Burden of Disease Study 2019. Eur J Ophthalmol. 2024;34:1852–64.
GBD 2019 Blindness and Vision Impairment Collaborators, Vision Loss Expert Group of the Global Burden of Disease Study. Causes of blindness and vision impairment in 2020 and trends over 30 years, and prevalence of avoidable blindness in relation to VISION 2020: the Right to Sight: an analysis for the Global Burden of Disease Study. Lancet Glob Health. 2021;9:e144–e160.
Drinkwater JJ, Davis WA, Davis T. A systematic review of risk factors for cataract in type 2 diabetes. Diabetes Metab Res Rev. 2019;35:e3073.
Lin C, Jivraj S. Are diabetes and blood sugar control associated with the diagnosis of eye diseases? An English prospective observational study of glaucoma, diabetic eye disease, macular degeneration and cataract diagnosis trajectories in older age. BMJ Open. 2025;15:e091816.
Acknowledgements
None.
Funding
This research was supported by Hunan Provincial Natural Science Foundation of China(2024JJ9260), Changsha Natural Science Foundation of China(kq2403125), High-Level Talent Support Program of Hunan Cancer Hospital (20250731-1003), Health Research Project of Hunan Provincial Health Commission (grant number:20254719), Scientific Research Project of Changsha Health Commission (KJ-202516,KJ-202529).
Author information
Authors and Affiliations
Contributions
Conception and design: Junfeng Zhou, Ning Ding, Zhengbin Yao; Administrative support and writing: Jiao Qin, Yingjie Su, Yong Long; Provision of study materials or patients:Ning Ding, Zhao Zeng, Shugen Xu; Collection and assembly of data: Yingjie Su, Junfeng Zhou, Jiao Qin; Data analysis and interpretation: Yingjie Su, Zhao Zeng, Yong Long; Final approval of manuscript: All authors.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Consent for publication
All participants in this study consented to publication.
Ethics approval and consent to participate
Ethical approval and informed consent were not required for this study, as the analysis was based on the publicly available Global Burden of Disease (GBD) database, which contains no identifiable personal information.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Zhou, J., Yao, Z., Xu, S. et al. Global burden of 13 non-communicable diseases attributable to high fasting plasma glucose from the GBD 2021 study. Nutr. Diabetes 15, 50 (2025). https://doi.org/10.1038/s41387-025-00405-7
Received:
Revised:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41387-025-00405-7
