
Abstract
Background
Prematurity and congenital heart disease (CHD) are risk factors for neonatal morbidity, including necrotising enterocolitis (NEC), and mortality. We describe the rates of NEC and survival in very preterm babies with severe CHD (sCHD), requiring cardiac intervention before discharge.
Methods
Retrospective cohort study utilizing the National Neonatal Research Database that included babies born <32weeks’ gestation admitted to neonatal units in England and Wales, 2012–2020. Exposure: Babies born <32weeks’ gestation with sCHD, that require intervention before discharge (excluding patent arterial ducts). Outcomes: rates of sCHD, severe NEC (requiring surgery or death) and mortality (death before 37 weeks’ CGA or neonatal discharge, whichever occurred first).
Results
438/68,423 babies had a sCHD diagnosis (6.4 per 1000 admissions <32weeks). Compared to non-CHD infants, sCHD infants had a higher rate of severe NEC (7.1% (95% CI 5.0–9.9%) vs.3.7% (95% CI 3.6–3.8%), (p < 0.001)) and higher mortality before 37weeks’ corrected gestational age (CGA) (31%, (95% CI 26.8–35.4%) vs. 10% (95% CI, 9.7, 10.2%) (p < 0.001)). Adjusted models showed that very preterm sCHD babies were two times more likely to develop NEC and six times more likely to die before 37weeks’ CGA.
Conclusion
Very preterm babies with sCHD have higher rates of NEC and mortality before cardiac intervention.
Impact
-
Prematurity and severe congenital heart disease increase the risk of necrotising enterocolitis (NEC) and death.
-
We found that in very preterm babies with severe CHD the odds of developing severe NEC were twice as high, and the odds of death were six times greater, compared to very preterm babies without sCHD.
-
Careful planning and counselling are needed in preterm deliveries of babies with severe CHD to reduce the odds of NEC and mortality.
Similar content being viewed by others
Introduction
Congenital heart disease (CHD) affects ~1 per 100 births each year, and accounts for nearly one-third of all congenital anomalies.1 Approximately a quarter of CHD lesions are considered severe and require intervention in the first year of life.2
Recent advancements in perinatal screening, diagnosis and management have increased the survival of babies with severe CHD (sCHD), particularly for term babies.3 However, preterm babies (born before 37 weeks’ gestation) with sCHD present significant challenges, and their outcomes are less well described. Prematurity and sCHD are independent risk factors for neonatal mortality and morbidity, including necrotising enterocolitis (NEC).4 Previous studies have found that preterm babies have a higher rate of CHD and this is associated with worse health outcomes compared to term babies.5,6,7,8,9,10,11 Additional research is needed to identify preterm sCHD infants at higher risk of NEC and mortality and explore clinical management strategies (e.g. feeding) that may ameliorate this risk.
In the United Kingdom, preterm babies with sCHD are typically admitted to, and remain in a neonatal unit until a corrected gestational age and weight considered adequate for cardiac intervention. This period in the neonatal unit allows for optimal growth and development in preparation for cardiac intervention. In addition, for certain cardiac conditions, intravenous prostaglandin may be administered to maintain patency of the ductus arteriosus. This practice differs for term babies who have earlier cardiac intervention or may be cared for in a paediatric intensive care unit or ward from birth. In England and Wales only three of 45 neonatal intensive care units have on-site cardiac surgery services, known as co-located cardiac centres. Therefore, most preterm babies born will require transfer postnatally to a cardiac centre for surgery.
Data from neonatal units in England and Wales are held in the National Neonatal Research Database (NNRD). The NNRD contains de-identified data from routine health records for all babies admitted to neonatal units in England and Wales.12 The NNRD provides an opportunity to explore outcomes of preterm babies admitted to a neonatal unit at a population-level prior to transfer to other healthcare settings for cardiac intervention. Data from paediatric intensive care or paediatric wards post cardiac intervention are not available on the NNRD.
We aimed to use routine data from the NNRD to determine the rates of sCHD in babies <32 weeks gestational age and compare rates of survival and severe NEC (sNEC), confirmed by laparotomy or cause of death, between babies with sCHD and without sCHD.
Patients and methods
Population
We included all babies born at <32 weeks gestational age born and admitted to a neonatal unit in England and Wales between 1 January 2012 to 31 December 2020. We defined sCHD as heart defects that require surgery or catheter intervention prior to discharge home (excluding patent arterial ducts). The diagnostic codes of sCHD were agreed by experts in neonatology and paediatric cardiology (Supplementary Tables S1, S2). We defined cases of severe NEC as confirmed by laparotomy or cause of death.13
Data extraction and defining our cohort
We aimed to identify a cohort of babies with severe congenital heart disease (sCHD) that require specialist intervention during the neonatal admissions. To do this, we defined babies with sCHD if they had one or more sCHD diagnoses at admission or discharge. To increase specificity for lesions requiring urgent specialist management. To focus on infants that had a specialist intervention in the neonatal period, we excluded babies born outside of a cardiac centre that were discharged home directly from the neonatal unit without any recorded transfers. Infants transferred to specialist care e.g. PICU and subsequently repatriated back to neonatal care prior to discharge remained included.
Analyses were conducted at the infant level using a unique baby identifier. Where infants had multiple neonatal episodes, they contributed once to the cohort.
Outcomes
We report the incidence of sCHD among preterm babies admitted to NNU, the most common severe cardiac anomalies as well as frequencies of co-occurring anomalies. The primary outcomes are (i) the rate of severe NEC (confirmed by laparotomy or cause of death) and (ii) survival to 37 weeks corrected age (CGA) or survival to discharge from the neonatal unit.13 Secondary outcomes include length of stay in NICU, postnatal age (days) at death, postnatal age at which enteral feeding was commenced and the first milk received and the age when exclusive enteral feeding was established (defined as three consecutive days with enteral feeding given without intravenous fluids or parenteral nutrition). We reported feeding exposures for babies who survived till at least 48 h following birth. We present rates of late onset sepsis, severe brain injury and bronchopulmonary dysplasia (Supplementary Table S3 for detailed definitions). To capture mortality prior to cardiac intervention, we chose to report survival to 37 weeks CGA or at discharge from neonatal care, whichever is sooner. 37 weeks CGA was advised by our expert panel (Supplementary Table S1), as this is the expected timepoint when preterm babies with sCHD will be transferred to a cardiac centre for surgical intervention. We do not report outcomes after surgical intervention as these are not available on the NNRD.
We present outcomes by two gestational age (GA) strata – very preterm (28+0–31+6 weeks gestation) and extremely preterm (22+0–27+6 weeks gestation).
Statistical analysis
We calculated the rate of sCHD per 1000 preterm neonatal admissions using data from the NNRD. We reported population proportions with 95% confidence interval (CI) calculated using the exact binomial test. Descriptive statistics were used to summarize baseline characteristics for babies in the sCHD and non-CHD cohorts across the <32 weeks’ gestation cohort, and gestational age groups - very preterm (28–31+6weeks) and extremely preterm (22–27+6 weeks).
We tested for differences in severe NEC and survival (primary outcomes) between the sCHD and the non-CHD groups using logistic regression to estimate odds ratios (OR) with 95% CI. Continuous outcomes were compared using linear regressions where appropriate and summarized using median (IQR). We used a multivariable model for the primary outcomes adjusted for a priori selected variables: sex, gestational age (weeks), birth weight, mode of delivery and antenatal steroids. We assessed the linearity assumption for birthweight z-score in logistic regression models. As there was evidence of non-linearity, birthweight z-score and gestational age at birth was modelled using natural cubic splines (3 degrees of freedom) in adjusted analyses. In gestational-stratified analyses, gestational age at birth was modelled as categorical variable given the linearity and restricted gestational age ranges. Model fit comparisons are presented in Supplementary Table S12. Mortality results were represented by a Kaplan-Meier Survival curve following each patient from birth till discharge or death and differences between groups were tested using log-rank test. Secondary outcome comparisons, subgroup analyses and post-hoc analyses (including feeding related exposures) were considered exploratory. To address multiplicity while retaining power, we controlled the false discovery rate (FDR) using the Benjamini–Hochberg procedure, reporting q-values alongside unadjusted p-values. FDR control is less conservative than family-wise error rate approaches (e.g., Bonferroni) and is commonly used when many related hypotheses are tested, particularly when outcomes are correlated.14,15 Findings from secondary analyses were interpreted as hypothesis-generating for future research. Data were analysed with statistical software packages (R version 4.3.1).16 Findings are reported in line with Reporting of studies Conducted using Observational Routinely collected Data (RECORD) guidelines.17
Research ethics and other approvals
We used de-identified data from the NNRD. No neonatal unit opted out of the study. This study received ethics committee approval from East Midlands – Leicester South Research Ethics Committee as part of the neoWONDER research program (Ref 21/EM/0130 IRAS Project ID 293603).18
Results
Characteristics of preterm babies with severe congenital heart disease admitted to neonatal units
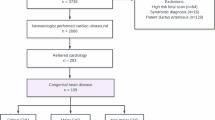
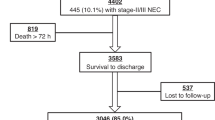
During the nine-year study period, 438 preterm babies born <32 weeks were admitted to neonatal units with a confirmed sCHD diagnosis (Table 1). These infants accounted for 0.64% of all 68,423 preterm admissions (438/68,423, 0.64%, 95% CI 0.58–0.70%), which represent an incidence of 6.4 sCHD per 1000 admissions <32 weeks’ gestation (Fig. 1). The most common cardiac anomalies across the study population were coarctation of the aorta (98/438, 23%), atrioventricular septal defect (90/438, 20%) and tetralogy of Fallot (79/438, 18%) (Supplementary Table S4). Anomalies are not mutually exclusive and 23% (101/438) had more than one sCHD diagnosis code recorded. Frequency of multiple sCHD diagnosis is summarised in Supplementary Table S5.

Flow diagram of babies born <32 weeks' gestation and admitted to neonatal units in England and Wales between 2012 and 2020, stratified by severe congenital heart disease status, severe NEC status and survival to 37 weeks' corrected gestational age.
Of the 438 babies born with sCHD, 338 were born very preterm (28–31+6weeks) and 100 extremely preterm (22–27 + 6 weeks). Among all preterm babies <32 weeks with sCHD, 52% (226/438) were iatrogenic births, where mothers were not in labour at the time of delivery and there was a maternal or fetal indication for delivery, compared to 43% (29,105/67,985) in the non-CHD group.
Compared to preterm babies without CHD, babies born <32 weeks with sCHD were more likely to be born with a birthweight under the 2nd centile, have non-cardiac congenital anomalies, lower Apgar score at 5 min and require intubation: 56% vs. 47% (Table 1). Less than 10% of all pregnancies had placenta previa, abruption or other types of antepartum haemorrhage. 15% of all preterm babies with sCHD were born in co-located cardiac centres (Table 1).
Mortality in babies born <32 weeks with severe CHD
Mortality rate before 37 weeks CGA across the whole study population <32 weeks was higher in babies with sCHD 31% vs 10%; adjusted Odds Ratio (aOR) 6.04 (95% CI, 4.83, 7.50). Mortality rates decreased with increasing gestational age in the non-CHD group, however this pattern was not observed in the sCHD group where mortality rate remained similar across all gestational ages (Fig. 1, Fig. 2, Supplementary Table S6). The median time of death was 15.2 days for the group that did not develop NEC compared to 39.5 days in the group that developed NEC (Supplementary Table S7). Lower gestational age, lower birthweight Z-score, and male sex were each independently associated with increased odds of mortality. Antenatal steroid exposure was strongly protective (aOR 0.46, 95% CI 0.43, 0.50) (Supplementary Table S8).

Crude mortality rate before 37 weeks' corrected gestational age shown for infants with severe congenital heart disease and infants without severe congenital heart disease, by completed gestational week at birth.
Corresponding mortality rates before 37 weeks CGA for the GA subgroups were similarly higher in the sCHD groups: odds of mortality were eight times higher in very preterm (28+0–31+6 weeks gestation) CHD 31% vs. non-CHD 4.6%, aOR 8.61 (95% CI 6.73, 10.93); two times higher in extremely preterm (22+0–27+6 weeks gestation) CHD 30% vs. non-CHD 20.5%, aOR 2.22 (95% CI 1.39, 3.47) (Tables 2 and 3, Supplementary Tables S7, S8).
The median postnatal age at death was 16.4 days (IQR 3.2, 37.3) in the sCHD group and 34.8 days (IQR 26.2, 44.7) in the non-CHD group. The log-rank tested indicated a significant difference in survival (p ≤ 0.0001) (Supplementary Fig. S1).
The severe cardiac anomalies associated with the highest mortality rate were congenital stenosis of the aortic valve (<10/<10, 100%), congenital subaortic stenosis (<10/<10, 100%), hypoplastic left heart syndrome (16/20, 80%), pulmonary valve atresia (<10/<10, 67%) and transposition of the great arteries (16/27, 59%) (Supplementary Table S4).
Severe NEC in babies with severe CHD
Across all preterm babies born <32 weeks with sCHD, severe NEC rates were at least two times higher 7.1% vs 3.7% (aOR 2.40 95% CI 1.61, 3.47). Birthweight-Z-score, gestation at births and sex were also independently associated with NEC (Supplementary Table S9). Corresponding severe NEC rates for GA subgroups were similarly higher in the sCHD group: very preterm 5.6% vs. 1.4% (aOR 3.35 95% CI 2.00, 5.28); extreme preterm 12% vs. 8.5%, aOR 1.54 (95% CI 0.79, 2.73). Among infants with severe NEC, case fatality was 45.2% (14/31) in the sCHD cohort and 37.4% (929/2486) in the non-CHD cohort. Death occurred a median of 25 days earlier in babies born <32 weeks with sCHD that did not develop severe NEC compared the group that did develop severe NEC and died.
Anomalies associated with the highest rate of severe NEC were common arterial trunk (<10/10, 14%), tetralogy of Fallot (10/79, 13%) and congenital pulmonary valve stenosis. (<10/<10, 13%) (Supplementary Table S4). Across all preterm babies with sCHD, those that developed severe NEC had a statistically significant lower birthweight (Supplementary Tables S7, S9).
Secondary outcomes
Given the number of secondary outcomes assess, we present q-values using Benjamini–Hochberg false discovery rate (BH-FDR) correction and interpret secondary and subgroup comparisons as exploratory. We found higher rates of BPD in preterm babies with sCHD compared to non-CHD (69% vs. 43% respectively), whilst rates of late onset sepsis and severe brain injury were similar in sCHD and non-CHD (4.3% vs. 4.5% and 14% vs 12%, respectively) (Table 2). Babies with a sCHD diagnosis had a longer length of stay in NICU (median 63days, IQR 27, 92 days) compared to those without sCHD (50 days, IQR 34, 72 days). Babies with sCHD needing transfer to a cardiac centre were most frequently transferred at a median weight of 2650 g (IQR 2249 g, 3025 g), median 71 days (IQR 47, 110 days) and median CGA 38 weeks (IQR 30, 41 weeks).
Feeding exposures
A lower proportion of preterm babies with sCHD received human milk as their first milk compared those without sCHD among all babies <32weeks 73% (95% CI 69–77%) vs. 77% (95% CI 76–77%) and extreme preterm (76% (95% CI 66–84%) vs. 85% (95% CI 85–86%)). The rates were more similar in the very preterm babies with sCHD 72% (95% CI 67–77%) vs 73% (95% CI 72–73%) non-CHD group. The majority received the first enteral feed at a median of 2 days, except very preterm babies without sCHD that received their first enteral feed by day 1 (Table 1). Babies born extreme preterm with sCHD took the longest time to reach full enteral feeds (19 days IQR (9–35)). In exploratory post-hoc analyses within infants with sCHD, first human milk feed was not significantly associated with severe NEC in adjusted models (aOR 2.08, 95% CI 0.77–7.25; p = 0.188), although unadjusted comparisons suggested differences in feeding timing (Supplementary Tables S10, S11). This analysis was underpowered (wide confidence intervals) and should be interpreted as hypothesis-generating. In our cohort, infants with severe NEC had a slightly longer time to first enteral feed (median 3 vs 2 days, p = 0.024) (Supplementary Table S10).
Discussion
Over a nine-year period, 0.6% (438/68,423) of preterm babies admitted to UK neonatal units were born with sCHD, requiring intervention in the neonatal period. This is an estimated incidence of 6.4 preterm babies per 1000 preterm admissions to the neonatal unit. This is similar to the incidence reported in international studies.6,7
1 in 14 preterm babies born <32 weeks with sCHD developed severe NEC and 1 in 3 died before 37 weeks CGA. This represents a two-fold increase in severe NEC and six-fold increase in odds of mortality compared to preterm babies without sCHD. As we report the severest cases of NEC, requiring surgery or leading to death, the overall incidence of NEC is likely to be higher if cases of medically managed NEC are included. Our rates of NEC in preterm babies with sCHD are similar to previously reported in the literature and higher to the incidence of NEC reported in term babies with sCHD.4,5,6,7,19
The heightened mortality rate of 30% in babies with sCHD before 37 weeks corrected gestational age across all gestational age groups is a key finding that will inform future counselling. The additional odds of mortality due to sCHD are more striking in the very preterm versus extremely preterm group (nine versus two times higher compared to non-CHD). This more pronounced impact on survival rates is due to the relatively higher survival among those born ≥28 weeks, with the majority expected to survive (44,438/46,585, 95.4% survival). These findings are consistent with research that shows the combination of sCHD, and prematurity exacerbates odds of mortality with previously reported mortality rates between 20–30%.5,7,20,21
We speculate that the higher rates of severe NEC and mortality among babies with sCHD may result from poorer gut perfusion, secondary to the cardiac anomaly and the need to maintain the patency of ductus arteriosus in duct dependent lesions. Additionally, the suboptimal fetal circulation in complex CHD increases the risk of prematurity. Half (52%, 226/438) of deliveries of babies with sCHD were iatrogenic and likely expedited for a maternal and/or fetal indication. Perinatal compromise that leads to emergency preterm delivery also increases the odds of NEC and mortality.
Babies born with sCHD outside of a cardiac centre were discharged at around 2650 g, which we infer is a target weight for surgical procedures and a corrected gestational age of 38 weeks (IQR 30, 40 weeks). It is important to study this group to determine the best ways of optimizing weight gain while minimizing the odds of NEC. Procedures which limit pulmonary blood flow, such as pulmonary artery banding, should be considered in cases where there is a high risk of systemic steal. However, these procedures carry their own risks, particular in babies weighing <2000 g.
Redirection or withdrawal of life-sustaining support are not reliably recorded in the NNRD, so we are unable to account for babies who had palliative care due to their cardiac condition. We found a higher incidence of non-cardiac anomalies in preterm babies is not surprising given the association of cardiac anomalies with genetic syndromes such as DiGeorge, Turner’s and chromosomal anomalies. Preterm babies with sCHD had a longer length of stay, received parenteral nutrition for longer and took longer to establish full enteral feeds. A lower proportion of preterm babies with sCHD received human milk as their first milk – a finding that calls for further study.
Our findings will inform counselling for parents based on antenatal diagnosis of cardiac anomaly, particularly regarding the high risk of NEC, mortality and prolonged length of stay in NICU. The consistent mortality rate of 30% among preterm infants irrespective of gestational week of birth is worth highlighting and has implications for counselling particularly for babies very preterm and it is important that these risks are understood and discussed when considering preterm delivery and timing of interventions.
This study has key strengths, including presenting population incidence rates of sCHD among preterm babies. Given the relatively low incidence of sCHD, utilizing routine population-based health records is a cost-effective and feasible method to study the epidemiology of sCHD among preterm babies. The NNRD is a high-quality validated database that includes information regarding maternal and labour history, routinely recorded feeding variables (including timing of initiation and establishment of full feeds and first milk type) and outcomes, transfer destinations, associated anomalies, and outcomes.12,22 To ensure a robust inclusion criteria, we involved paediatric cardiology and neonatal medicine experts in identifying a consensus list of diagnostic codes that represent sCHD.
However, there are also several limitations. Whilst we expect that the diagnosis on the NNRD is accurate, certain sCHD diagnosis can be difficult to diagnose antenatally and need to be confirmed postnatally. We cannot confirm cardiac intervention directly within NNRD; we used transfer/discharge destination as a proxy to improve specificity. For example, babies are admitted with a suspected diagnosis of “coarctation of the aorta” rather than confirmed diagnosis and this diagnosis remains on the electronic patient record despite it being excluded. This is particularly relevant for cardiac malformations that are difficult to diagnose until the ductus arteriosus has closed. We addressed this limitation by only assigning babies with a confirmed coarctation and sCHD if they were either born in a co-located cardiac centre or discharged to a cardiac centre.
Despite the NNRD representing population prevalence of sCHD among neonatal admissions, the low numbers resulted in wide confidence intervals, imprecise estimates of risk for adverse outcomes and limited sub-group analyses by specific diagnoses or perinatal characteristics. In this study we were able to examine selected feeding variables captured in the NNRD (time to first enteral feed, time to full enteral feeds, and whether the first milk was human milk [mother’s own or donor]) in exploratory analyses; however, we could not comprehensively characterise longitudinal feeding composition. The small sample size of subgroups with sCHD limited our ability to evaluate the impact of feeding strategies on neonatal outcomes. Furthermore, we were unable to evaluate feeding antecedents of NEC because the timing of NEC onset is not available in the dataset used. This prevents establishing temporality between exposures and NEC and limits more advanced approaches (e.g., time-to-event methods with competing risks). In addition, we did not have sufficiently reliable information on nil by mouth days or longitudinal feeding composition (e.g., proportion of feeds by mother’s own milk vs donor milk vs formula over time), which have been highlighted as important in prior work. The unknown timing of when NEC occurred prevented time-series analysis particularly to adjust for competing risk. Similarly, although late-onset sepsis was captured, we could not determine whether infection episodes preceded NEC onset, so we cannot infer causality or temporal sequence. Because NEC timing is unavailable, and because death may occur early, severe NEC incidence may be underestimated in the sickest infants. This is consistent with earlier deaths among infants with severe CHD who did not have recorded severe NEC, compared with those who did. These data do not include information on NEC or mortality following transfer to the cardiac unit, which also limits our study. We define BPD at 36 weeks corrected as babies receiving respiratory support, however we recognize that within the population some babies may need respiratory support for cardiac rather than respiratory disease leading to an inflated incidence of BPD. The nature of retrospective routine data means that unmeasured confounders cannot be controlled for.
Future research to reduce the risk of severe NEC among babies with sCHD should focus on prevention measures, particularly around feeding. Due to low numbers of sCHD, international collaboration and linkage to population registries such as the UK NICOR will be necessary.23 Future studies should report on health and educational outcomes following cardiac surgery for preterm babies with sCHD as these are important for counselling. Ongoing work in the neoWONDER data-linkage study will report outcomes longitudinally.18
Conclusions
In this population study, 438 (0.6%, 438/68,423) preterm babies <32 weeks admitted to neonatal units were born with sCHD. Mortality rates are high and ~1 in 3 babies with sCHD are not expected to survive to cardiac intervention, regardless of their gestation. Preterm babies with sCHD had twice the adjusted odds of developing severe NEC and six times the adjusted odds of death compared to non-CHD babies. The findings of this study are useful for antenatal counselling in sCHD, which should include consideration of the added odds of severe NEC and death when delivery occurs prematurely.
Data availability
The data are not publicly available due to privacy or ethical restrictions. Data are available upon reasonable request. Applications to use the data used within this project should be made to the Neonatal Data Analysis Unit, Imperial College London.
References
Liu, Y. et al. Global birth prevalence of congenital heart defects 1970–2017: updated systematic review and meta-analysis of 260 studies. Int. J. Epidemiol. 48, 455–463 (2019).
Pavlicek, J. et al. Major heart defects: the diagnostic evaluations of first-year-olds. BMC Pediatr. 21, 528 (2021).
Su, Z. et al. Global, regional, and national time trends in mortality for congenital heart disease, 1990–2019: an age-period-cohort analysis for the Global Burden of Disease 2019 study. eClinicalMedicine 43, 101249 (2022).
McElhinney, D. B. et al. Necrotising enterocolitis in neonates with congenital heart disease: risk factors and outcomes. Pediatrics 106, 1080–1087 (2000).
Dumitrascu Biris, I. et al. Mortality and morbidity in preterm infants with congenital heart disease. Acta Paediatr. 111, 151–156 (2022).
Archer, J. M. et al. Distribution of and mortality from serious congenital heart disease in very low birth weight infants. Pediatrics 127, 293–299 (2011).
Norman, M. et al. Neonatal outcomes in very preterm infants with severe congenital heart defects: an international cohort study. J. Am. Heart Assoc. 9, e015369 (2020).
Ib, A. et al. Cardiogenic necrotising enterocolitis in infants with congenital heart disease: a systematic review and meta-analysis. Pediatric Cardiol. 46, 2429–2442 (2025).
Cy, L. et al. Risk factors for necrotising enterocolitis in preterm infants: a meta analysis. Chin. J. Contemp. Pediatr. 24, 908–916 (2022).
Motta, C. et al. The association of congenital heart disease with necrotising enterocolitis in preterm infants: a birth cohort study. J. Perinatol. 35, 949–953 (2015).
Aly, S., Qattea, I., Kattea, M. O., Aly, H. Z. Neonatal outcomes in preterm infants with severe congenital heart disease: a national cohort analysis. Front. Pediatr. 12, 1326804 (2024).
Modi, N. Information technology infrastructure, quality improvement and research: the UK National Neonatal Research Database. Transl. Pediatr. 8, 193–198 (2019).
Battersby, C. et al. Incidence and enteral feed antecedents of severe neonatal necrotising enterocolitis across neonatal networks in England, 2012–13: a whole-population surveillance study. Lancet Gastroenterol. Hepatol. 2, 43–51 (2017).
Aickin, M. Other method for adjustment of multiple testing exists. BMJ 318, 127 (1999).
Perneger, T. V. What’s wrong with Bonferroni adjustments. BMJ 316, 1236–1238 (1998).
R. Core Team. R: A language and environment for statistical computing. R Foundation for Statistical Computing. https://www.r-project.org/ (2017).
Benchimol, E. I. et al. The REporting of studies Conducted using Observational Routinely-collected health Data (RECORD) statement. PLoS Med. 12, e1001885 (2015).
Blankenstein, E. V., Aveline, A. & Battersby, C. A protocol for neoWONDER: neonatal whole population data linkage to improve long-term health and wellbeing of preterm and sick babies. PLOS ONE 19, e0305113 (2024).
Ostlie, D. J. et al. Necrotising enterocolitis in full-term infants. J. Pediatr. Surg. 38, 1039–1042 (2003).
Chen, X. et al. Impact of congenital heart disease on the outcomes of very low birth weight infants. Am. J. Perinatol. 41, 1815–1821 (2024).
Chu, P. Y. et al. Congenital heart disease in premature infants 25-32 weeks’ gestational age. J. Pediatrics 181, 37–41.e1 (2017).
Battersby, C. et al. The United Kingdom National Neonatal Research Database: a validation study. PLoS One 13, e0201815 (2018).
National Congenital Heart Disease Audit (NCHDA) - NICOR, https://www.nicor.org.uk/national-cardiac-audit-programme/congenital-audit-nchda (2024).
Acknowledgements
We thank the UK Neonatal Collaborative comprising neonatal units contributing data to the National Neonatal Research Database: Dr Matthew Babirecki (Airedale General Hospital), Dr Anand Kamalanathan (Arrowe Park Hospital), Dr Clare Cane (Barnet Hospital), Dr Kavi Aucharaz (Barnsley District General Hospital), Dr Aashish Gupta (Basildon Hospital), Dr Alistair Ewing (Basingstoke & North Hampshire Hospital), Dr L M Wong (Bassetlaw District General Hospital), Dr Anita Mittal (Bedford Hospital), Dr Lindsay Halpern (Birmingham City Hospital), Dr Pinki Surana (Birmingham Heartlands Hospital), Dr Matt Nash (Birmingham Women’s Hospital), Dr Sam Wallis (Bradford Royal Infirmary), Dr Ahmed Hassan (Broomfield Hospital, Chelmsford), Dr Karin Schwarz (Calderdale Royal Hospital), Dr Shu-Ling Chuang (Chelsea & Westminster Hospital), Dr Penelope Young (Chesterfield & North Derbyshire Royal Hospital), Dr Ramona Onita (Colchester General Hospital), Dr Graham Whincup (Conquest Hospital), Dr Joanne Dangerfield (Countess of Chester Hospital), Dr Jocelyn Morris (Croydon University Hospital), Dr Yee Aung (Cumberland Infirmary), Dr Abdul Hasib (Darent Valley Hospital), Dr Mehdi Garbash (Darlington Memorial Hospital), Dr Alex Allwood (Derriford Hospital), Dr Pauline Adiotomre (Diana Princess of Wales Hospital), Dr Nigel Brooke (Doncaster Royal Infirmary), Dr Abby Deketelaere (Dorset County Hospital), Dr Toria Klutse (East Surrey Hospital), Dr Sonia Spathis (Epsom General Hospital), Sathish Krishnan (Frimley Park Hospital), Dr Samar Sen (Furness General Hospital), Dr Jez Jones (George Eliot Hospital), Dr Geedi Farah (Glan Clwyd Hospital), Dr Prem Pitchaikani (Glangwili General Hospital), Dr Jennifer Holman (Gloucester Royal Hospital), Dr Pinki Surana (Good Hope Hospital), Dr Stanley Zengeya (Great Western Hospital), Dr Geraint Lee (Guy’s & St Thomas’ Hospital), Dr Sobia Balal (Harrogate District Hospital), Dr Cath Seagrave (Hereford County Hospital), Dr Tristan Bate (Hillingdon Hospital), Dr Hilary Dixon (Hinchingbrooke Hospital), Dr Narendra Aladangady (Homerton Hospital), Dr Hassan Gaili (Hull Royal Infirmary), Dr Matthew James (Ipswich Hospital), Dr M Lal (James Cook University Hospital), Dr Oluseun Tayo (James Paget Hospital), Dr Poornima Pandey (Kettering General Hospital), Dr Ravindra Bhat (Kings College Hospital), Dr Simon Rhodes (King’s Mill Hospital), Dr Jonathan Filkin (Kingston Hospital), Dr Savi Sivashankar (Lancashire Women and Newborn Centre), Dr Lawrence Miall (Leeds Neonatal Service), Dr Jonathan Cusack (Leicester General Hospital), Dr Venkatesh Kairamkonda (Leicester Royal Infirmary), Dr Michael Grosdenier (Leighton Hospital), Dr Ajay Reddy (Lincoln County Hospital), Dr J Kefas (Lister Hospital), Dr Alison Bedford Russell (Liverpool Women’s Hospital), Dr Jennifer Birch (Luton & Dunstable Hospital), Dr Gail Whitehead (Macclesfield District General Hospital), Dr Ashok Karupaiah (Manor Hospital), Dr Ghada Ramadan (Medway Maritime Hospital), Dr I Misra (Milton Keynes General Hospital), Dr Nicola Johnson (Musgrove Park Hospital), Dr Richard Heaver (New Cross Hospital), Dr Mohammad Alam (Newham General Hospital), Dr Prakash Thiagarajan (Nobles Hospital), Dr Muthukumar (Norfolk & Norwich University Hospital), Dr Tiziana Fragapane (North Devon District Hospital), Dr Ngozi Edi-Osagie (North Manchester General Hospital), Dr Cheentan Singh (North Middlesex University Hospital), Dr Subodh Gupta (Northampton General Hospital), Jess Reynolds (Northumbria Specialist Emergency Care Hospital), Dr Khadija Ben-Sasi (Northwick Park Hospital), Dr Steven Wardle (Nottingham City Hospital), Dr Steven Wardle (Nottingham University Hospital, QMC), Dr Victoria Nesbitt (Ormskirk District General Hospital), Dr Eleri Adams (Oxford University Hospitals, John Radcliffe Hospital), Dr Katharine McDevitt (Peterborough City Hospital), Dr Ruchika Gupta (Pilgrim Hospital), Dr David Gibson (Pinderfields General Hospital, Pontefract), Prof Minesh Khashu (Poole General Hospital), Dr Iyad Al-Muzaffar (Prince Charles Hospital), Dr Kate Creese (Princess of Wales Hospital), Dr Chinnappa Reddy (Princess Alexandra Hospital), Dr Mark Johnson (Princess Anne Hospital), Dr Prashanth Bhat (Princess Royal Hospital), Dr Patricia Cowley (Princess Royal Hospital, previously Royal Shrewsbury Hospital), Dr Rashmi Gandhi (Princess Royal University Hospital), Dr Charlotte Groves (Queen Alexandra Hospital), Dr Lidia Tyszcuzk (Queen Charlotte’s Hospital), Dr Shilpa Ramesh (Queen Elizabeth Hospital, Gateshead), Dr Glynis Rewitzky (Queen Elizabeth Hospital, King’s Lynn), Mrs Julia Croft (Queen Elizabeth Hospital, Woolwich), Dr Bushra Abdul-Malik (Queen Elizabeth the Queen Mother Hospital), Dr Dominic Muogbo (Queen’s Hospital, Burton on Trent), Dr Ambalika Das (Queen’s Hospital, Romford), Dr Angela D’Amore (Rosie Maternity Hospital, Addenbrookes), Dr Soma Sengupta (Rotherham District General Hospital), Dr Christos Zipitis (Royal Albert Edward Infirmary), Dr Peter De Halpert (Royal Berkshire Hospital), Dr Archana Mishra (Royal Bolton Hospital), Dr Chris Warren (Royal Cornwall Hospital), Dr John McIntyre (Royal Derby Hospital), Dr Nagendra Venkata (Royal Devon & Exeter Hospital), Dr Lucinda Winckworth (Royal Hampshire County Hospital), Dr Joanne Fedee (Royal Lancaster Infirmary), Dr Anitha Vayalakkad (Royal Oldham Hospital), Dr Raju Narasimhan (Royal Preston Hospital), Dr Lee Abbott (Royal Stoke University Hospital), Dr Ben Obi (Royal Surrey County Hospital), Dr Prashanth Bhat (Royal Sussex County Hospital), Dr Stephen Jones (Royal United Hospital), Dr Richard Hearn (Royal Victoria Infirmary), Dr Anjali Petkar (Russells Hall Hospital), Dr Jim Baird (Salisbury District Hospital), Dr Kirsten Mack (Scarborough General Hospital), Dr Pauline Adiotomre (Scunthorpe General Hospital), Dr Arun Ramachandran (Singleton Hospital), Dr Vineet Gupta (Southend Hospital), Dr Faith Emery (Southmead Hospital), Dr Charlotte Huddy (St George’s Hospital), Dr Salim Yasin (St Helier Hospital), Dr Akinsola Ogundiya (St Mary’s Hospital, IOW), Dr Lidia Tyszcuzk (St Mary’s Hospital, London), Dr Ngozi Edi-Osagie (St Mary’s Hospital, Manchester), Dr Pamela Cairns (St Michael’s Hospital), Dr Vennila Ponnusamy (St Peter’s Hospital), Dr Victoria Sharp (St Richard’s Hospital), Dr Carrie Heal (Stepping Hill Hospital), Dr Sanjay Salgia (Stoke Mandeville Hospital), Dr Imran Ahmed (Sunderland Royal Hospital), Dr Jacqeline Birch (Tameside General Hospital), Dr Sunil Reddy (The Grange University Hospital), Dr Porus Bastani (The Jessop Wing, Sheffield), Dr Marice Theron (The Royal Free Hospital), Dr Divyen Shah (The Royal London Hospital – Constance Green), Dr Siba Paul (Torbay Hospital), Dr Se-Yeon Park (Tunbridge Wells Hospital), Dr Giles Kendall (University College Hospital), Dr Puneet Nath (University Hospital Coventry), Mrs Julia Croft (University Hospital Lewisham), Dr Mehdi Garbash (University Hospital of North Durham), Dr Hari Kumar (University Hospital of North Tees), Dr Nitin Goel (University Hospital of Wales), Dr Chris Rawlingson (Victoria Hospital, Blackpool), Dr Delyth Webb (Warrington Hospital), Dr Bird (Warwick Hospital), Dr Sankara Narayanan (Watford General Hospital), Dr Yee Aung (West Cumberland Hospital), Dr Elizabeth Eyre (West Middlesex University Hospital), Dr Jageer Mohammed (West Suffolk Hospital), Dr Sanjay Jaisal (Wexham Park Hospital), Dr Caroline Sullivan (Whipps Cross University Hospital), Dr Ros Garr (Whiston Hospital), Dr Wynne Leith (Whittington Hospital), Dr Vimal Vasu (William Harvey Hospital), Dr Anna Gregory (Worcestershire Royal Hospital), Dr Katia Vamvakiti (Worthing Hospital), Dr Brendan Harrington (Wrexham Maelor Hospital), Dr Ngozi Edi-Osagie (Wythenshawe Hospital), Dr Megan Eaton (Yeovil District Hospital), Dr Sundeep Sandhu (York District Hospital), and Dr Michael Cronin (Ysbyty Gwynedd).
Funding
This research was supported by the National Institute for Health Research (NIHR) grant ACF-2020-21-011 awarded to B.N.M. C.B. is supported through a UK NIHR Advanced Fellowship personal award (NIHR300617). Infrastructure support for this research was provided by the NIHR Imperial Biomedical Research Centre (BRC) to the NNRD. This article is independent research funded by the NIHR, and the views expressed in this publication are those of the authors and not necessarily those of the NHS, NIHR, or the Department of Health. None of the funders have had any influence over study design, collection, analysis and interpretation of the data, in writing the report and in the decisions to submit this article for publication. Imperial College London Open Access Fund supported the publication and dissemination of this work.
Author information
Authors and Affiliations
Consortia
Contributions
B.N.M. conceived and designed the study, carried out data-analysis and interpretation and drafted the first version of the manuscript. E.v.B. conceived and designed the study, edited the manuscript and approved the final manuscript as submitted. J.L. performed data extraction and data cleaning. A.M. conceived and designed the study, edited the manuscript and approved the final manuscript as submitted. H.B.-R. conceived and designed the study, edited the manuscript and approved the final manuscript as submitted. C.B. conceived and designed the study, contributed to interpretation, edited the manuscript and approved the final manuscript as submitted. C.B. acted as guarantor.
Corresponding author
Ethics declarations
Competing interests
C.B. reports personal support from NIHR Advanced Fellowship; grants from National Institute for Health Research; personal fees to support attendance at educational events from Chiesi Pharmaceuticals; she is deputy chair of the NIHR HTA Prioritisation committee for hospital-based care.
Ethics approval and consent to participate
Individual patient consent was not required for this study, as it used anonymised data from the National Neonatal Research Database (NNRD). The study was conducted under ethical approval granted from East Midlands – Leicester South Research Ethics Committee as part of the neoWONDER research program (Ref 21/EM/0130 IRAS Project ID 293603), which allows the use of routinely collected neonatal data for research purposes. All data were handled in accordance with relevant data protection and confidentiality regulations.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Nezafat Maldonado, B., van Blankenstein, E., Lanoue, J. et al. Necrotising enterocolitis and mortality in very preterm babies with severe congenital heart disease. Pediatr Res (2026). https://doi.org/10.1038/s41390-026-05033-0
Received:
Revised:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41390-026-05033-0
