
Abstract
Purpose
To assess long-term survival in a “STAMPEDE-like” cohort of high-risk locally advanced prostate cancer, staged with PSMA PET-CT, treated with hypofractionated radiotherapy (RT) and long-term androgen deprivation therapy (LT-ADT) without abiraterone.
Materials & methods
Patients with non-metastatic prostate cancer fulfilling “STAMPEDE high-risk” criteria, staged with PSMA PET-CT, treated with external beam RT from 2016 to 2021 were included. RT dose was >74 Gy equivalent to prostate with LT-ADT ≥ 2 years. We analysed metastatic-free survival (MFS), prostate cancer specific survival (PCSS) and overall survival (OS) using Kaplan-Meier method.
Results
170 patients were eligible, treated with hypofractionated RT with median prostate 2Gy-equivalent dose of 82 Gy. About one-third were node-positive and treated with whole pelvic RT. Over median follow up of 65 months, 6-years MFS, PCSS and OS were 80.7%, 95.8% and 94.4% respectively. On multivariate analysis, Gleason score and nodal stage showed significant association with MFS.
Conclusion
For PSMA-PETCT staged high risk prostate cancer, appropriately intensified local treatment could be complementary or an alternative to systemic intensification in selected patients.
Similar content being viewed by others


Introduction
Curative radiotherapy with long-term androgen deprivation therapy (LT-ADT) for 2-3 years is the standard treatment for non-metastatic, high-risk and node-positive prostate cancer [1]. Systemic intensification is increasingly preferred for these patients after the STAMPEDE trial, which demonstrated improved metastasis free survival (MFS) and overall survival (OS) with addition of abiraterone to LT-ADT and radiotherapy in high-risk prostate cancer [2]. Recently, at Advanced Prostate Cancer Consensus Conference 2024 at Lugano, in response to the question “In the majority of patients with high-risk localised/locally advanced prostate cancer (STAMPEDE definition) N0 M0 on next-generation imaging, what is your recommended treatment?”, 68% of the expert panellists recommended adding abiraterone for two years with radiotherapy and LT-ADT [3].
The STAMPEDE trial used conventional imaging (CI) with technetium-99 bone scan and abdominopelvic CT scan for staging at diagnosis and recurrence, prostate radiotherapy 74 Gy (or equivalent), and discretionary pelvic nodal radiotherapy, reflecting the clinical standards at trial design and execution. Since then, molecular imaging using prostate-specific membrane antigen-based positron emission tomography (PSMA-PETCT) based staging, dose escalation to the prostate (focal or entire gland), and whole pelvic radiotherapy (WPRT) have influenced global practice considerably [4,5,6,7].
We report long-term survival outcomes in a “STAMPEDE-like” cohort of locally advanced prostate cancer, staged with PSMA-PETCT at diagnosis and recurrence, treated with dose escalated, hypofractionated radiotherapy and LT-ADT without intensification with novel androgen receptor targeted agents (ARTA).
Methods
After institutional ethics committee approval (IEC no. 900936), patients with non-metastatic prostate adenocarcinoma, treated with curative external beam radiotherapy from 2016 to 2021 were identified from our prospective institutional database. Patients fulfilling the STAMPEDE high-risk criteria – either node positive, or at least two factors - stage T3-4, Gleason score 8–10, PSA ≥ 40 ng/mL - were included. Additional inclusion criteria were PSMA-PETCT staging at diagnosis, prostate radiotherapy >74 Gy equivalent (a/b = 1.5), ADT ≥ 24 months, and at least two years follow up. Patients with conventional imaging for staging, metastasis beyond pelvic nodes, radiotherapy for recurrent prostate cancer or after prostatectomy, or prior ARTA, were excluded.
Patients experiencing Phoenix defined biochemical failure (defined as a rise of 2 ng/ml or more above the PSA nadir after EBRT with hormonal therapy) were restaged with PSMA-PETCT. Survival outcomes including metastasis-free-survival (MFS, from diagnosis to first distant metastasis visible in PSMA-PETCT or any-cause death), prostate cancer-specific survival (PCSS, from diagnosis to death due to prostate cancer), and overall survival (OS, from diagnosis to any-cause death) were analysed using Kaplan–Meier method. Univariate analysis for known prognostic and predictive factors was done using log-rank test. For multivariate analysis, cox regression model was used, and variables were selected stepwise with univariate p-value < 0.2. P-value < 0.05 was considered statistical significance. SPSS version 23 was used for statistical analysis.
Results
Of total 451 patients screened, 170 were eligible (Supplementary Fig. 1). Median age was 68.5 years (IQR: 62–74). Median PSA value was 44 ng/ml (IQR: 21–84 ng/ml). About one-third of the study cohort (36%) had node-positive cancer. All patients received hypofractionated prostate radiotherapy with a median dose equivalent (EQD2) of 82 Gy. In those treated with ultra-hypofractionation, 65% received WPRT with 25 Gy in 5 fractions. For node-positive cancer, all patients (97%) received dose-escalated prostate radiotherapy and WPRT without boost to gross nodes. Median duration of ADT was 24 months (IQR: 22–27 months). About 20% had surgical castration. Study cohort characteristics were comparable to STAMPEDE trial arms (Table 1).
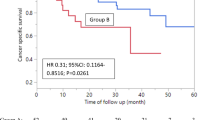
Over a median follow-up of 65 months, 45 patients experienced biochemical failure. Restaging PSMA-PETCT showed that local (n = 12) and regional (n = 16) failure was less than distant (n = 26) failure suggesting efficacy of more comprehensive locoregional EBRT. Six-year MFS, PCSS, and OS for the entire cohort were 80.7%, 95.8%, and 94.4% respectively (Supplementary Fig. 2). Patients with node-positive disease had a 6-year MFS of 77% vs 83% for node-negative subgroup (p = 0.23) (Supplementary Fig. 3). Univariable and multivariable analysis identified age at diagnosis (HR: 0.41) and Gleason score (HR: 3.36) as prognostic for MFS (Supplementary Table 1).
Discussion
Survival outcomes in this ‘STAMPEDE-like’ cohort provide some insights into the management of high-risk prostate cancer in the PSMA-PET era. Higher sensitivity and specificity of PSMA-PETCT for index staging in high-risk prostate cancer, coupled with dose-escalated, hypofractionated radiotherapy to prostate and nodes, can achieve high disease control with LT-ADT alone. The MFS and PCSS in our cohort are similar to the test arm of STAMPEDE, without systemic intensification.
Across the spectrum of high-risk prostate cancer, various strategies for local and systemic treatment intensification have been used (Fig. 1). ‘Augmented radiotherapy’ by escalating dose to the whole prostate or the dominant lesion, and nodal irradiation may be adequate for early high-risk disease. Dose escalation to 80 Gy in the RTOG 0126 randomised trial improved DMFS with only modest increase in late toxicity [7]. Similarly, pelvic radiotherapy showed 6.7% higher 5-year MFS with no significant increase in late morbidity [6, 8]. While a 6-year MFS of about 80% in our cohort using local intensification is encouraging, it may be further improved by systemic intensification. Patients with worse prognosis due to multiple high-risk factors or nodal involvement may be preferentially selected for addition of ARTA to radical radiotherapy and LT-ADT [9].

ADT androgen deprivation therapy, ST short term, LT long term, RT radiotherapy, WPRT whole pelvic radiotherapy, ARTA androgen receptor targeted agents.
The benefit of abiraterone must be put in context of its adverse effects profile and cost. In the STAMPEDE trial, 37% of men reported severe adverse events with abiraterone and 13% needed to discontinue the drug. Additionally, regulatory and financial barriers limit access to abiraterone globally, including many high-income countries [10]. An elaborate quality-adjusted life years based analysis by the STAMPEDE investigators suggests that addition of abiraterone to ADT would be cost-effective for non-metastatic prostate cancer if it costs less than 28 GBP/day [11]. Ongoing randomised trials are exploring alternative ARTAs including enzalutamide (ENZARAD, NCT02446444), apalutamide (ATLAS, NCT02531516; NRG GU-009 PREDICT-RT), and darolutamide (THUNDER, NCT06282588; DASL-HiCAP-ANZUP1801, NCT04136353), or using novel imaging (PRIME, NCT03561961; THUNDER) and genetic biomarkers (THUNDER, NRG GU-009 PREDICT-RT), refining systemic therapy for high-risk prostate cancer.
Although we have made all attempts to check the veracity of the data, we acknowledge the inherent limitations of survival outcomes from a retrospective study in a limited single-institution cohort. Additionally, the PSMA-based MFS as used in this cohort is different from the CI-based MFS used in the STAMPEDE trial. The events for PSMA-MFS occur earlier but may not correlate with OS, though using CI at recurrence in our cohort would have resulted in a higher MFS than reported.
Treatment intensification, be it local or systemic, comes at a cost and should be done judiciously. Addition of ARTA to augmented radiotherapy and LT-ADT may benefit patients with node-positive disease, multiple high-risk factors, or in the absence of PSMA-PET imaging. PSMA-PET imaging exemplifies the potential of advanced diagnostic tools to refine treatment. However, it also needs a nuanced understanding of phenomena like the Will Rogers effect to interpret clinical outcomes accurately and ensure optimal patient care. The ongoing trials will provide more answers for personalising treatment for high-risk prostate cancer.
References
National Comprehensive Cancer Network. NCCN clinical practice guidelines in oncology: prostate cancer. 2023. https://www.nccn.org/professionals/physician_gls/pdf/prostate.pdf (accessed March 18, 2023).
Attard G, Murphy L, Clarke NW, Cross W, Jones RJ, Parker CC, et al. Abiraterone acetate and prednisolone with or without enzalutamide for high-risk non-metastatic prostate cancer: a meta-analysis of primary results from two randomised controlled phase 3 trials of the STAMPEDE platform protocol. Lancet. 2022;399:447–60. https://doi.org/10.1016/S0140-6736(21)02437-5.
Gillessen S, Turco F, Davis ID, Efstathiou JA, Fizazi K, James ND et al. Management of patients with advanced prostate cancer. Report from the 2024 Advanced Prostate Cancer Consensus Conference (APCCC). Eur Urol. 2025;87:157–216.
Hofman MS, Lawrentschuk N, Francis RJ, Tang C, Vela I, Thomas P, et al. Prostate-specific membrane antigen PET-CT in patients with high-risk prostate cancer before curative-intent surgery or radiotherapy (proPSMA): a prospective, randomised, multicentre study. Lancet. 2020;395:1208–16. https://doi.org/10.1016/S0140-6736(20)30314-7.
Kerkmeijer LGW, Groen VH, Pos FJ, Haustermans K, Monninkhof EM, Smeenk RJ, et al. Focal boost to the intraprostatic tumor in external beam radiotherapy for patients with localized prostate cancer: results from the FLAME randomized phase III trial. J Clin Oncol. 2021;39:787–96. https://doi.org/10.1200/JCO.20.02873.
Murthy V, Maitre P, Kannan S, Panigrahi G, Krishnatry R, Bakshi G, et al. Prostate-only versus whole-pelvic radiation therapy in high-risk and very high-risk prostate cancer (POP-RT): outcomes from phase III randomized controlled trial. J Clin Oncol. 2021;39:1234–42. https://doi.org/10.1200/JCO.20.03282.
Michalski JM, Moughan J, Purdy J, Bosch W, Bruner DW, et al. Effect of standard vs dose-escalated radiation therapy for patients with intermediate-risk prostate cancer: the NRG oncology RTOG 0126 randomized clinical trial. JAMA Oncol. 2018;4:e180039.
Maitre P, Maheshwari G, Sarkar J, Singh P, Kannan S, Dutta S, et al. Late urinary toxicity and QOL with pelvic radiotherapy for high-risk prostate cancer: Dose-effect relations in the POP-RT randomized phase III trial. Int J Radiat Oncol. 2024. https://doi.org/10.1016/j.ijrobp.2024.03.023.
Ravi P, Xie W, Buyse M, Halabi S, Kantoff PW, Sartor O, et al. Refining risk stratification of high-risk and locoregional prostate cancer: a pooled analysis of randomized trials. Eur Urol. 2024. https://doi.org/10.1016/j.eururo.2024.04.038.
James ND, Tannock I, N’Dow J, Feng F, Gillessen S, Ali SA, et al. The Lancet Commission on prostate cancer: planning for the surge in cases. Lancet. 2024;403:1683–722. https://doi.org/10.1016/S0140-6736(24)00651-2.
Clarke CS, Hunter RM, Gabrio A, Brawley CD, Ingleby FC, Dearnaley DP, et al. Cost-utility analysis of adding abiraterone acetate plus prednisone/prednisolone to long-term hormone therapy in newly diagnosed advanced prostate cancer in England: lifetime decision model based on STAMPEDE trial data. PLOS ONE. 2022;17:e0269192. https://doi.org/10.1371/journal.pone.0269192.
Funding
Open access funding provided by Department of Atomic Energy.
Author information
Authors and Affiliations
Contributions
VM and PM conceptualized the study. VM, AS, PM, PN and PS were involved in patient accrual and study procedures. The manuscript was drafted by VM, AS, PM, AA, AJ and GP. All authors approved the final manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethical approval and consent to participate
We confirm that all methods were performed in accordance with the relevant guidelines and regulations. Ethical approval was taken from the Institutional Ethical Committee of Tata Memorial Hospital, Mumbai (IEC no. 900936). No informed consent as Ethics Committee granted wavier.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Murthy, V., Samanta, A., Maitre, P. et al. Abiraterone for “STAMPEDE-Like” cohort of high-risk prostate cancer in the PSMA-PET era: too much, too early?. Prostate Cancer Prostatic Dis 28, 985–988 (2025). https://doi.org/10.1038/s41391-025-00983-8
Received:
Revised:
Accepted:
Published:
Version of record:
Issue date:
DOI: https://doi.org/10.1038/s41391-025-00983-8
