
Abstract
Background
This study aims to evaluate the efficacy and advantages of MR navigation system in robot-assisted radical prostatectomy (RARP) for high-risk prostate cancer (PCa).
Methods
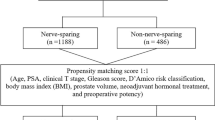
We retrospectively studied 147 patients with high-risk PCa based on D’Amico risk criteria from July 2021 to November 2023. All patients chose MR-assisted RARP (MR-RARP) or standard RARP (S-RARP) after receiving comprehensive counseling on the benefits and risks of both procedures. After propensity score-matching, 57 patients were included in each group. Perioperative, functional and oncological outcomes were compared. Logistic and Cox regression models were used to identify predictors of positive surgical margin (PSM), biochemical recurrence (BCR), continence and potency recovery.
Results
The MR-RARP group had higher nerve-sparing (NS) rates (78.9% vs 54.4%, P = 0.021) and lower PSM rates (10.5% vs 26.3%, P = 0.030). Continence recovery rates were higher in the MR-RARP group at catheter removal (40.4% vs 22.8%, P = 0.044), 1 month (61.4% vs 38.6%, P = 0.015) and 3 months (73.7% vs 47.4%, P = 0.004), with no significant differences at 6 months (82.5% vs 73.7%, P = 0.258) and 12 months (93.0% vs 87.7%, P = 0.341). Furthermore, the MR-RARP group demonstrated higher potency rates at 1 month (42.1% vs 21.1%, P = 0.016) and 3 months (57.9% vs 36.8%, P = 0.024), whereas outcomes were comparable at 6 months (66.7% vs 56.1%, P = 0.248) and 12 months (77.2% vs 66.7%, P = 0.211). With a median follow-up of 28 months, BCR-free survival showed no significant differences (P = 0.295). Multivariate analyses confirmed MR navigation as an independent predictor of PSM, continence, and potency recovery (all P < 0.05). Statistical power analysis indicated a power of 0.847.
Conclusions
Real-time intraoperative MR navigation enhances surgical precision, facilitates NS techniques, and optimizes early continence and potency recovery without compromising oncological safety.
This is a preview of subscription content, access via your institution
Access options
Subscribe to this journal
Receive 6 print issues and online access
$259.00 per year
only $43.17 per issue
Buy this article
- Purchase on SpringerLink
- Instant access to the full article PDF.
USD 39.95
Prices may be subject to local taxes which are calculated during checkout



Similar content being viewed by others
Data availability
The data used and analyzed during the current study are available from the corresponding author upon reasonable request.
References
Bray F, Laversanne M, Sung H, Ferlay J, Siegel RL, Soerjomataram I, et al. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2024;74:229–63.
Ou YC, Yang CK, Wang J, Hung SW, Cheng CL, Tewari AK, et al. The trifecta outcome in 300 consecutive cases of robotic-assisted laparoscopic radical prostatectomy according to D’Amico risk criteria. Eur J Surg Oncol. 2013;39:107–13.
Yossepowitch O, Eggener SE, Serio AM, Carver BS, Bianco FJ Jr, et al. Secondary therapy, metastatic progression, and cancer-specific mortality in men with clinically high-risk prostate cancer treated with radical prostatectomy. Eur Urol. 2008;53:950–9.
Williams S, Chiong E, Lojanapiwat B, Umbas R, Akaza H. Management of prostate cancer in Asia: resource-stratified guidelines from the Asian Oncology Summit 2013. Lancet Oncol. 2013;14:e524–534.
Mottet N, van den Bergh RCN, Briers E, Van den Broeck T, Cumberbatch MG, De Santis M, et al. EAU-EANM-ESTRO-ESUR-SIOG guidelines on prostate cancer-2020 update. Part 1: screening, diagnosis, and local treatment with curative intent. Eur Urol. 2021;79:243–62.
Patel VR, Sivaraman A, Coelho RF, Chauhan S, Palmer KJ, Orvieto MA, et al. Pentafecta: a new concept for reporting outcomes of robot-assisted laparoscopic radical prostatectomy. Eur Urol. 2011;59:702–7.
Checcucci E, Amparore D, De Luca S, Autorino R, Fiori C, Porpiglia F. Precision prostate cancer surgery: an overview of new technologies and techniques. Minerva Urol Nefrol. 2019;71:487–501.
Liu W, Zhang E, Zhang M. Current application of navigation systems in robotic-assisted and laparoscopic partial nephrectomy: focus on the improvement of surgical performance and outcomes. Ann Surg Oncol. 2024;31:2163–72.
Checcucci E, Piana A, Volpi G, Quarà A, De Cillis S, Piramide F, et al. Visual extended reality tools in image-guided surgery in urology: a systematic review. Eur J Nucl Med Mol Imaging. 2024;51:3109–34.
Hu HZ, Feng XB, Shao ZW, Xie M, Xu S, Wu XH, et al. Application and prospect of mixed reality technology in medical field. Curr Med Sci. 2019;39:1–6.
Li G, Dong J, Wang J, Cao D, Zhang X, Cao Z, et al. The clinical application value of mixed-reality-assisted surgical navigation for laparoscopic nephrectomy. Cancer Med. 2020;9:5480–9.
Zeng S, Zhou Y, Wang M, Bao H, Na Y, Pan T. Holographic reconstruction technology used for intraoperative real-time navigation in robot-assisted partial nephrectomy in patients with renal tumors: a single center study. Transl Androl Urol. 2021;10:3386–94.
Porpiglia F, Checcucci E, Amparore D, Peretti D, Piramide F, De Cillis S, et al. Percutaneous kidney puncture with three-dimensional mixed-reality hologram guidance: from preoperative planning to intraoperative navigation. Eur Urol. 2022;81:588–97.
Cornford P, van den Bergh RCN, Briers E, Van den Broeck T, Brunckhorst O, Darraugh J, et al. EAU-EANM-ESTRO-ESUR-ISUP-SIOG guidelines on prostate cancer-2024 update. Part I: screening, diagnosis, and local treatment with curative intent. Eur Urol. 2024;86:148–63.
Rashid R, Sohrabi C, Kerwan A, Franchi T, Mathew G, Nicola M, et al. The STROCSS 2024 guideline: strengthening the reporting of cohort, cross-sectional, and case-control studies in surgery. Int J Surg. 2024;110:3151–65.
Liu W, Wang Y, Wang Z, Cao Z, Yu Y, Wang J, et al. The application of mixed reality navigation system in laparoscopic partial nephrectomy for highly complex renal tumors (RENAL score ≥10): a retrospective cohort study. Int J Surg. 2025;111:1513–6.
Weinreb JC, Barentsz JO, Choyke PL, Cornud F, Haider MA, Macura KJ, et al. PI-RADS prostate imaging - reporting and data system: 2015, version 2. Eur Urol. 2016;69:16–40.
Thüroff JW, Abrams P, Andersson KE, Artibani W, Chapple CR, Drake MJ, et al. EAU guidelines on urinary incontinence. Eur Urol. 2011;59:387–400.
Vroege JA. The sexual health inventory for men (IIEF-5). Int J Impot Res. 1999;11:177.
Li JK, Tang T, Zong H, Wu EM, Zhao J, Wu RR, et al. Intelligent medicine in focus: the 5 stages of evolution in robot-assisted surgery for prostate cancer in the past 20 years and future implications. Mil Med Res. 2024;11:58.
Park BH, Jeon HG, Jeong BC, Seo SI, Lee HM, Choi HY, et al. Influence of magnetic resonance imaging in the decision to preserve or resect neurovascular bundles at robotic assisted laparoscopic radical prostatectomy. J Urol. 2014;192:82–88.
Ficarra V, Novara G, Secco S, D’Elia C, Boscolo-Berto R, Gardiman M, et al. Predictors of positive surgical margins after laparoscopic robot assisted radical prostatectomy. J Urol. 2009;182:2682–8.
Soeterik TFW, van Melick HHE, Dijksman LM, Stomps S, Witjes JA, van Basten JPA. Nerve sparing during robot-assisted radical prostatectomy increases the risk of ipsilateral positive surgical margins. J Urol. 2020;204:91–95.
Schiavina R, Bianchi L, Lodi S, Cercenelli L, Chessa F, Bortolani B, et al. Real-time augmented reality three-dimensional guided robotic radical prostatectomy: preliminary experience and evaluation of the impact on surgical planning. Eur Urol focus. 2021;7:1260–7.
Checcucci E, Pecoraro A, Amparore D, De Cillis S, Granato S, Volpi G, et al. The impact of 3D models on positive surgical margins after robot-assisted radical prostatectomy. World J Urol. 2022;40:2221–9.
Porpiglia F, Checcucci E, Amparore D, Manfredi M, Massa F, Piazzolla P, et al. Three-dimensional elastic augmented-reality robot-assisted radical prostatectomy using hyperaccuracy three-dimensional reconstruction technology: a step further in the identification of capsular involvement. Eur Urol. 2019;76:505–14.
Carbin DD, Shah A, Kusuma VRM. Artificial intelligence in robot-assisted radical prostatectomy: where do we stand today?. J Robot Surg. 2024;18:404.
Rajpurkar P, Chen E, Banerjee O, Topol EJ. AI in health and medicine. Nat Med. 2022;28:31–38.
Khanna A, Antolin A, Bar O, Ben-Ayoun D, Zohar M, Boorjian SA, et al. Automated identification of key steps in robotic-assisted radical prostatectomy using artificial intelligence. J Urol. 2024;211:575–84.
Bianchi L, Chessa F, Angiolini A, Cercenelli L, Lodi S, Bortolani B, et al. The use of augmented reality to guide the intraoperative frozen section during robot-assisted radical prostatectomy. Eur Urol. 2021;80:480–8.
Yossepowitch O, Briganti A, Eastham JA, Epstein J, Graefen M, Montironi R, et al. Positive surgical margins after radical prostatectomy: a systematic review and contemporary update. Eur Urol. 2014;65:303–13.
Chadebecq F, Lovat LB, Stoyanov D. Artificial intelligence and automation in endoscopy and surgery. Nat Rev Gastroenterol Hepatol. 2023;20:171–82.
Funding
This research was supported by the National Natural Science Foundation of China (No. 82173372 and No. 81802540), the Education Department Grant of Liaoning Province (No. LJKMZ20221138), Central Funds Guiding the Local Science and Technology Development (2024JH6/100800011), the Science and Technology Program of Liaoning Province (2021JH1/10400045), and the Bethune Urologic Oncology Special Project Research Fund (No. mnzl202023).
Author information
Authors and Affiliations
Contributions
WL, SZ, XY, and YY drafted the manuscript; WL, XY, and YY collected the data; SZ and MG did the data analysis; HS, QM, ZC, and JB completed the figures and tables; LC, JW, and MZ managed the article design; WL, LC, JW, and MZ reviewed the manuscript; JB and MZ provided funding support. All authors have read and approved the final manuscript.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethics approval and consent to participate
This study was approved by the Ethics Review Committee of The First Hospital of China Medical University (ethical approval No. 2024-770-2) and written informed consent was obtained from all participants. In addition, written informed consent for publication of his images was obtained from the patient in Fig. 3. All methods were conducted in accordance with the ethical guidelines of the Declaration of Helsinki and the STROCSS guidelines.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Liu, W., Zhou, S., Yu, X. et al. The application of mixed reality navigation system in robot-assisted radical prostatectomy for high-risk prostate cancer: a propensity score‑matched cohort study. Prostate Cancer Prostatic Dis 29, 144–151 (2026). https://doi.org/10.1038/s41391-025-01003-5
Received:
Revised:
Accepted:
Published:
Version of record:
Issue date:
DOI: https://doi.org/10.1038/s41391-025-01003-5
