
Abstract
Introduction
Benign prostatic hyperplasia (BPH) and associated lower urinary tract symptoms (LUTS) can significantly impair a man’s quality of life. While traditional surgical treatments are effective, they often pose risks to sexual function, particularly in the form of ejaculatory and/or erectile dysfunction. Minimally invasive surgical treatments (MISTs) have emerged as alternative procedures that aim to alleviate LUTS while preserving sexual function.
Objective
Investigate the impact of MISTs for BPH on sexual function including erectile and ejaculatory function.
Methods
In May 2025, a systematic review and meta-analysis of sexual function outcomes in MISTs was performed using the Ovid, Embase, and Medline/PubMed databases. Articles were included if they were in English, assessed a MIST, and incorporated sexual function outcomes. Articles were excluded if they included pooled analyses, were abstracts without full text, and/or were ongoing incomplete clinical trials. We included studies on water vapor thermal therapy (Rezum), prostatic urethral lift (Urolift), prostatic artery embolization (PAE), temporary implantable nitinol device (iTIND), Optilume BPH catheter system, and transperineal laser ablation (TPLA). Outcomes included erectile function using International Index of Erectile Function (IIEF) scores and ejaculatory function using the Male Sexual Health Questionnaire (MSHQ).
Results
The initial search yielded 2646 studies. After screening and full text review, 77 studies met inclusion criteria encompassing a total of 11,477 patients. Based on the pooled analyses, IIEF scores significantly improved after Rezum and Urolift. Urolift significantly improved MSHQ-function and bother scores, while Rezum only improved MSHQ-bother scores. PAE, iTind, Optilume, and TPLA did not significantly impact erectile or ejaculatory function.
Conclusions
MISTs are a promising option for management of BPH in patients interested in maintaining sexual function, preserving or even improving erectile and ejaculatory function.
Similar content being viewed by others
Introduction
Benign prostatic hyperplasia (BPH) is a histologic diagnosis referring to the proliferation of smooth muscle, epithelial, and connective tissue in the transition zone of the prostate [1]. BPH is a highly prevalent disease in aging men, and is often associated with bothersome lower urinary tract symptoms (LUTS) due to prostatic enlargement and obstruction. Treatment of LUTS may involve medications (i.e., alpha blockers and/or 5-alpha-reductase inhibitors) and/or surgery. Historically, transurethral resection of the prostate (TURP) has been considered the gold standard surgical treatment for BPH with LUTS. Additional surgical options have included simple prostatectomy, holmium laser enucleation of the prostate (HoLEP), and photoselective vaporization of the prostate (PVP). While these treatments have been shown to be efficacious in terms of urinary symptoms, they can cause sexual side effects including ejaculatory dysfunction (EjD) and potential worsening of erectile dysfunction (ED) [2]. Unlike medication-related sexual side effects, those associated with BPH surgeries are often permanent. The 2023 American Urological Association (AUA) BPH guidelines therefore highlight the importance of counseling patients regarding potential sexual side effects preoperatively [3].
Several procedures defined as minimally invasive surgical treatments (MISTs) have emerged, aiming to achieve similar functional outcomes while preserving sexual function. MISTs include water vapor thermal therapy (wVTT, Rezum), prostatic urethral lift (PUL, Urolift), prostatic artery embolization (PAE), the Optilume BPH catheter system, the temporary implantable nitinol device (iTIND), and transperineal laser ablation (TPLA). Often performed in outpatient settings under local anesthesia, these procedures typically offer shorter recovery times and less postoperative bleeding than traditional BPH surgeries [4]. Concerns regarding erectile function and preservation of antegrade ejaculation also make MISTs an appealing option for many patients. The aim of this systematic review was to evaluate and compare sexual function outcomes among contemporary MISTs.
Methods
Search strategy and study selection
In May 2025, a systematic electronic search of the published English literature was performed to identify relevant articles discussing sexual function related to MISTs in patients with BPH. MISTs were defined based on the prior literature as BPH treatments which incorporate the ability to be performed in the outpatient setting, lack the need for general anesthesia, have minimal bleeding risk, allow for early postoperative recovery of daily activities, and have reduced impact on urinary and sexual function [4]. Accordingly, MISTs that were included in our review were: Urolift, iTIND, Optilume BPH, Rezum, PAE, and TPLA. While aquablation therapy has been shown to have favorable sexual outcomes compared to traditional surgeries, it was not incorporated into our review as it did not meet the criteria above to be defined as a MIST, which is consistent with prior literature [4, 5]. A comprehensive search strategy was developed alongside a medical librarian (N.N.). Indexing terms and keywords with truncation were combined using Boolean operators. The following databases were searched from inception until May 19th, 2025: Medline (Ovid), Embase (Ovid), Scopus, and Cochrane Library. Search terms included: “BPH” AND “prostatic urethral lift” or “urolift” or “iTIND” or “temporary implantable nitinol device” or “optilume” or “drug coated balloon” or “rezum” or “water vapor” or “prostate artery embolization” or “MIST” or “TPLA” or “transperineal laser ablation” AND “sexual dysfunction” or “sex” or “erect” or “ejaculat” or “anejaculat” or “orgasm” or “anorgasm.”
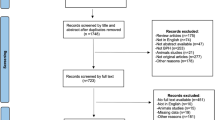
After removal of duplicates, search results were independently screened and the titles and abstracts were assessed by two authors (EC and BL) based on inclusion criteria. A third author (RB) resolved conflicts. Full text of all titles that met screening criteria by a majority vote were obtained. Full text was then reviewed. Studies were included if they assessed patients with BPH who underwent Urolift, Rezum, iTIND, TPLA, PAE, or Optilume treatment and evaluated sexual outcomes including erectile and/or ejaculatory function. Randomized controlled trials (RCTs), prospective, and retrospective cohort studies were included. Reference lists from included papers were checked for other relevant studies. Reviews, case reports, and abstracts without full text were excluded. The complete PRISMA flow chart is available in Fig. 1.

MIST therapies included Urolift, iTIND, Optilume BPH, Rezum, PAE, and TPLA. 1354 abstracts were screened leaving 167 full texts for review. 77 articles met inclusion criteria for the review.
This systematic review adhered to PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines and utilized the PICO (Population, Intervention, Outcomes) criteria [6, 7]. Studies were included if they assessed men with BPH and LUTS (P) undergoing MIST (I) with or without comparison (C) evaluating the impact on erectile and/or ejaculatory function (O). This systematic review was registered with PROSPERO (CRD420251074473). Covidence systematic review software was used to manage, screen, deduplicate, and document this systematic review (Veritas Health Innovation, Melbourne, Australia).
Data extraction and analysis
For each of the included studies, the relevant data of interest was collected in a dedicated data extraction form, including: title, first author’s name, publication year, number of patients, MIST(s) studied, sexual function outcome measures, and sexual function results. For erectile function, outcomes included various iterations of the International Index of Erectile Function (IIEF) including the IIEF-15, IIEF-5 (also known as the Sexual Health Inventory for men (SHIM)), and IIEF-Erectile Function (EF). For ejaculatory function, outcomes included rate of retrograde ejaculation (RE) and Male Sexual Health Questionnaire (MSHQ-EjD) function and bother scores.
Meta-analyses of the included studies were performed using Review Manager 5.4 (RevMan v.5.4; Cochrane Collaboration, Oxford, UK). The pooled analyses were conducted on studies including postoperative measurement of IIEF-EF, MSHQ-EjD, or RE rate at 12 months for each MIST. Results were reported as mean and standard deviation (SD) or the percentage of patients with a particular outcome. For continuous variables reported as the median (range), results were converted to mean ± SD [8]. In order to pool the effects within the same MIST, the weighted mean difference (WMD) and 95% confidence intervals (CIs) were estimated and pooled for each surgical technique. Pooled mean differences were determined using a random-effects model. The results were displayed as forest plots showing mean effect sizes and I2 was used to assess heterogeneity between studies. Statistical significance was set at p = 0.05. Data not suitable for meta-analysis were presented narratively.
Risk of bias
The risk of bias and quality of studies included in the meta-analyses were independently assessed using the standard Cochrane Collaboration risk-of-bias tools including the Risk of Bias in Non-Randomized Studies of Interventions (ROBINS-I) tool for comparative studies and the revised Cochrane risk-of-bias tool of randomized trials (ROB 2) for RCTs (Supplementary 1) [9, 10].
Results
Literature search
Our initial electronic search yielded 2646 articles. After removal 1292 duplicates, 1354 studies remained. Title and abstract screening excluded 1187 articles not relevant to the query. This left 167 articles for full-text review, of which 90 articles were excluded. Ultimately, 77 articles, with a total of 11,477 patients, met the inclusion criteria and were included in the review as shown in the PRISMA diagram (Fig. 1).
Selected studies
A summary of the 77 selected studies including study characteristics and sexual function outcomes can be found in Table 1 [11,12,13,14,15,16,17,18,19,20,21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51,52,53,54,55,56,57,58,59,60,61,62,63,64,65,66,67,68,69,70,71,72,73,74,75,76,77,78,79,80,81,82,83,84,85,86,87]. Of the 77 studies selected, 27 (35.1%) evaluated Rezum, 3 (3.9%) evaluated iTIND, 22 (28.6%) evaluated PAE, 2 (2.6%) evaluated Optilume, 19 (24.7%) evaluated Urolift, and 9 (9.1%) evaluated TPLA. 17 (22.1%) studies were randomized controlled trials, while 34 (44.2%) were prospective non-randomized trials, and 24 (31.2%) were retrospective. 11 (14.3%) studies compared a MIST to a traditional BPH surgery and 3 (3.9%) compared two MISTs to each other.
Assessment of sexual outcomes
The most commonly utilized validated questionnaire for erectile function was the IIEF in its various forms (i.e., IIEF-5, IIEF-15, or IIEF-EF), reported in 68 (88.3%) studies. For ejaculatory dysfunction, 35 (45.5%) studies reported on rate of retrograde ejaculation and 33 (42.9%) studies utilized the MSHQ function and/or bother scores.
Outcomes by MIST
Rezum
Rezum therapy has been shown to preserve or improve erectile function across multiple studies [40, 41, 43, 66]. Babar 2023 reported no differences in erectile function outcomes based on the number of injections administered (1–4) [21]. Hawks Ladds 2024 found that patients with baseline ED demonstrated significant improvement in IIEF-EF scores at 48 months, despite no early differences compared with those without baseline dysfunction [46]. Long term data from McVary and colleagues confirmed preservation of sexual function up to five years post-procedure [59,60,61]. In contrast, McVary 2018 observed worsening erectile outcomes among patients managed with medical therapy, while those undergoing Rezum maintained erectile and overall sexual function [62]. Similarly, Cindolo 2023 reported no significant differences in EF between patients who met versus did not meet 5-year RCT criteria (i.e., no history of urinary retention or previous prostate surgery, postvoid residual (PVR) < 250 mL, prostate volume >30 mL and <80 mL, no use of antiplatelet or anticoagulant medication, and few comorbidities) [32]. Alegorides 2020 and Dixon 2016 both noted stable EF with significant improvement in MSHQ bother scores at 1 and 2 years, respectively [14, 37]. Manfredi 2025 found comparable EF outcomes between Rezum and thulium laser enucleation of the prostate (ThuLEP) [57].
Ejaculatory function was also preserved or improved following Rezum in several studies. Campobasso 2023 and Minore 2025 reported increased rates of antegrade ejaculation post-treatment, likely related to medication discontinuation [27, 64]. McVary 2018 demonstrated maintenance of ejaculatory function compared with deterioration in patients on medical therapy, while Cindolo 2023 observed no differences in ejaculatory outcomes between those who met the 5-year RCT criteria versus those who did not [32, 62]. In comparative analyses, Manfredi 2025 found Rezum significantly preserved ejaculation relative to THULEP, and Ozkaptan 2025 reported RE in over 94% of HoLEP patients versus 5% following Rezum [57, 67]. Additionally, Aguero 2025, Balsamo 2024 and Hawks Ladds 2024 found no significant differences in sexual outcomes between patients with large ( > 80 g)and small ( < 80 g) prostates [11, 23, 47].
Rezum IIEF pooled analysis
A meta-analysis was conducted on 14 studies [11, 14, 21,22,23, 27, 32, 37, 43, 46, 57, 64, 67, 76] (n = 1505 at baseline) to assess the change in IIEF scores following Rezum wVTT for BPH. The pooled estimate showed a statistically significant mean improvement in IIEF score of 1.26 (95% CI: –2.30 to –0.18; p = 0.02) at 12 months. The total change is displayed in the forest plot (Fig. 2). Significant statistical heterogeneity was observed across the included studies, with an I2 value of 86% and a Chi [2] value of 93.19 (df = 13, p < 0.00001). The substantial heterogeneity suggests that the true effect size varies significantly among the studies, likely due to differences in patient characteristics, follow-up duration, or measurement protocols. The Tau [2] was 2.89, which is also indicative of high true variance between studies. While the overall pooled effect showed a small increase, the effect sizes varied substantially among individual studies, ranging from a mean difference of 3.90 (Manfredi 2025) [57] to –3.10 (Hawks-Ladds 2024) [46]. Four studies (Manfredi 2025 [57], Ghahhari 2022 [43], Balsamo 2024 [23], and Samir 2024 [76]) reported a statistically significant improvement. The remaining studies reported changes that were not statistically significant [11, 14, 21, 22, 27, 32, 37, 46, 64].

BPH Benign prostatic hyperplasia, CI confidence interval, df degree of freedom, IIEF international index of erectile function, IV inverse variance.
Rezum MSHQ-EjD pooled analysis
For MSHQ—Ejd scores, a meta-analysis of five studies [14, 22, 37, 41, 57], encompassing 211 patients in the intervention arm, was conducted to assess the change in MSHQ-Ejd function score at 12 months after the procedure. The pooled mean difference was calculated at 1.68 points (95% CI: –0.18 to 3.54), which did not achieve statistical significance (Z = 1.77, p = 0.08), suggesting no robust evidence for a definitive overall change in this outcome following the Rezum procedure. (Fig. 3) Significant statistical heterogeneity was observed across the included studies I2 = 82%, Chi2 = 22.68, p = 0.0001, indicating substantial variability in effect size among the trials. While one study (Manfredi 2025 [57]) reported a large, statistically significant improvement (4.20 points, 95% CI: 3.19–5.21), the non-significant pooled result highlights that this positive effect was not consistently demonstrated across the meta-analysis.

BPH Benign prostatic hyperplasia, CI confidence interval, df degree of freedom, IV inverse variance, MSHQ-EjD male sexual health questionnaire—ejaculatory dysfunction.
Rezum MSHQ-bother pooled analysis
For MSHQ –bother sub-score, a meta-analysis was conducted on four studies [14, 37, 41, 57] (n = 188 patients) to assess the change in MSHQ-EjD Bother. The pooled mean difference of –1.07 points (95% CI: –1.58 to –0.56) indicates a statistically significant overall improvement in this specific sub-score following the Rezum procedure (Z = 4.10, p < 0.0001) (Fig. 4). Moderate statistical heterogeneity was observed (I2 = 70%, p = 0.02). Furthermore, all four individual studies reported a decrease in score, and three of the four (Alegorides 2020 [14], Dixon 2016 [37], and Manfredi 2025 [57]) reported a statistically significant improvement, supporting the conclusion of a significant aggregate improvement in this sexual function outcome.

BPH Benign prostatic hyperplasia, CI confidence interval, df degree of freedom, IV inverse variance, MSHQ-Bother male sexual health questionnaire- bother score.
Urolift
Several studies showed no difference in erectile or ejaculatory function post-urolift [16, 19, 20, 29, 51, 55]. Ahn 2022 found that Urolift did not impact erectile or ejaculatory function in patients who were healthy or in those with high comorbidities [12]. Annese 2024 also found no difference in semen parameters including volume, sperm counts, and motility post-Urolift in young men [19]. When comparing patients who opted for Urolift versus continued medical management, Gonzalez Enguita 2025 found that those undergoing Urolift were more often able to preserve ejaculation [44]. Roehrborn 2022 found improvements in ejaculatory function scores at 12 months post-Urolift compared to sham control [73]. In a RCT compared to TURP, patients undergoing Urolift were more likely to preserve ejaculation [45].
Urolift IIEF pooled analysis
A meta-analysis of nine studies [12, 19, 20, 22, 29, 51, 73, 81, 86] encompassing 322 patients in the intervention arm, was conducted to assess the change in IIEF score at 12 months (Fig. 5). The pooled estimate demonstrated a statistically significant overall improvement in this score, with a mean increase of 1.86 points (95% CI: 0.54–3.18, Z = 2.76, p = 0.006). Moderate statistical heterogeneity was observed (I2 = 69, p = 0.001), indicating some variability in the effect size among the studies. Notably, eight of the nine studies reported a mean improvement (positive mean difference), with the largest effect reported by Woo 2012 [86] (4.70 points, 95% CI: 4.72–10.68). Only one study (Kim 2020 [51]) reported a negative mean difference (worsening), which was not statistically significant.

BPH Benign prostatic hyperplasia, CI confidence interval, df degree of freedom, IIEF international index of erectile function, IV inverse variance.
Urolift MSHQ-EjD pooled analysis
For MSHQ-EjD, a meta-analysis of eight studies [12, 19, 20, 22, 29, 73, 81, 86] including 279 patients who underwent the Urolift procedure, was conducted to assess the change in this sexual function score. The pooled mean difference demonstrated a statistically significant overall improvement of 1.06 points (95% CI: 0.44 to 1.69, Z = 3.32, p = 0.0009) (Fig. 6). Moderate statistical heterogeneity was observed across the studies (I2 = 48%, p = 0.06 for Chi [2]), indicating that the magnitude of the effect was somewhat varied but not highly inconsistent. The majority of studies showed a mean improvement, with four studies reporting statistically significant improvements [20, 22, 73, 86]. Only two studies (Annese 2024 [19] and Ahn 2022 [12]) reported a non-significant decline in MSHQ-EjD.

BPH Benign prostatic hyperplasia, CI confidence interval, df degree of freedom, MSHQ-EjD male sexual health questionnaire-ejaculatory dysfunction.
Urolift MSHQ-Bother pooled analysis
A meta-analysis of four studies [12, 73, 81, 86], including 172 patients, was conducted to assess the change in MSHQ Bother scores following the Urolift procedure (Fig. 7). The mean difference was calculated as Post-Intervention Score minus Baseline Score, where a negative value (lower score) indicates improvement (less bother). The pooled mean difference demonstrated a statistically significant overall reduction in ejaculatory bother of –0.53 points (95% CI: –0.95 to –0.11, p = 0.01). Moderate statistical heterogeneity was observed across the studies (I2 = 61%, p = 0.05). Two of the four individual studies reported a statistically significant improvement (Roehrborn 2017 [73] and Woo 2012 [86]), supporting the overall conclusion of a net decrease in ejaculatory bother.

BPH Benign prostatic hyperplasia, CI confidence interval, df degree of freedom, MSHQ-bother male sexual health questionnaire-bother score.
PAE
Studies have shown overall preservation of erectile function post PAE, with improved ejaculatory function compared to traditional BPH surgery [26, 34, 38, 54, 70]. Alrawashdash 2020 found improvements in IIEF-5 at 18 months, with 88.5% of patients preserving antegrade ejaculation [15]. Compared to TURP, Carnevale 2016 showed lower rates of ejaculatory dysfunction following PAE [30]. In a comparison with HoLEP, PAE was found to better preserve both ejaculatory and erectile function [52]. Richardson 2025 found no difference in erectile or ejaculatory function when comparing traditional versus coil embolization [72].
PAE IIEF pooled analysis
A meta-analysis of nine studies [26, 30, 34, 38, 68, 70, 71, 82, 83], encompassing 815 patients in the intervention arm, was conducted to assess the change in IIEF scores following PAE (Mean Difference = Post-Intervention Score minus Baseline Score, where a positive value indicates improvement). The pooled mean difference suggested an overall mean increase of 0.97 points (95% CI: –0.33 to 2.26). However, this overall effect did not reach statistical significance (Z = 1.46, p = 0.15), suggesting no definitive overall change in IIEF score following PAE (Fig. 8). Extremely high statistical heterogeneity was observed (I2 = 91%, Chi2 = 84.27, p < 0.00001), indicating substantial variability in the reported effects across the trials. While three studies (Bhatia 2022 [26], Delazar 2025 [34] and Pisco 2016 [70]) reported statistically significant improvements, another study (Theurich 2022 [82]) reported a statistically significant worsening, further emphasizing the lack of a robust, consistent overall effect.

BPH Benign prostatic hyperplasia, CI confidence interval, df degree of freedom, IV inverse variance, IIEF international index of erectile function, IV inverse variance, PAE prostatic artery embolization.
Due to a general paucity of studies utilizing MSHQ-EjD or the MSHQ Bother score following PAE, a formal quantitative synthesis (meta-analysis) of these ejaculatory outcomes could not be performed. While some studies have reported on these measures, their inclusion criteria, follow-up times, and reporting formats were too heterogeneous or sparse to allow for pooled data analysis.
iTind
Three studies evaluated sexual outcomes after iTind. When compared to a sham control, Elterman 2023 found no differences in IIEF-5 3 months after iTind [39]. DeNunzio 2021 found significant improvements in both IIEF-5 and MSHQ-EjD 6 months after iTind [35]. Amparore 2021 reported a 4% RE rate post-iTind [17].
A formal quantitative synthesis (meta-analysis) of erectile and ejaculatory outcomes using the IIEF, MSHQ-EjD function or bother scores following the iTind procedure could not be performed due to a limited number of published studies that report these outcomes with extractable mean and standard deviation data. While individual trials and reviews consistently suggest that iTind preserves or has a negligible effect on ejaculatory function, the current evidence base lacks the necessary homogeneity and volume to calculate a statistically robust, aggregate pooled effect size for MSHQ-EjD scores. This necessitates reliance on single-study data for drawing conclusions on ejaculatory bother and function preservation.
TPLA
Overall, studies have shown preservation of erectile and ejaculatory function post-TPLA [36, 42, 85]. Minafra 2023 found TPLA to improve ejaculatory function and preserve erectile function at three-years post-procedure [63]. TPLA was shown to preserve ejaculatory function significantly more often compared to TURP across two studies [25, 28].
TPLA IIEf pooled analysis
In the case of TPLA there was only data available suitable for a meta-analysis for a follow-up time of 6 months in 3 studies [36, 42, 63]. The pooled mean difference in IIEF scores suggested an overall mean increase of 1.01 points (95% CI: –1.11 to 3.14) (Fig. 9). However, this overall effect did not achieve statistical significance (Z = 0.93, p = 0.35), showing no definitive overall change in this outcome following the intervention. Notably, no heterogeneity was detected across the studies I2 = 0%, p = 0.57. While two studies (DeRienzo 2021 [36] and Frego 2021 [42]) reported non-significant improvements, one study (Minatra 2023 [63]) reported a non-significant worsening, ultimately contributing to the inconclusive pooled result.

BPH Benign prostatic hyperplasia, CI confidence interval, df degree of freedom, IIEF international index of erectile function, IV inverse variance, TPLA transperineal laser ablation.
In the case of MSHQ-Ejd and MSHQ bother scores, a formal meta-analyses could not be done due to the limited number of available studies. The two studies that report MSHQ -EjD data, (de Rienzo 2021 [36] and Minafra 2023 [63]), both report a discreet improvement after 6 months, with no available follow up data at 12 months.
Optilume BPH
Only two studies were identified for Optilume BPH. Both Copelan 2025 and Kaplan 2024 found preservation of erectile and ejaculatory function 12-24 months post-Optilume BPH compared to a sham control [33, 49].
Risk of publication bias
There was no clear publication bias evidenced in the funnel plots of the respective meta-analyses (Supplementary 2). Funnel plots did not show a clear asymmetry in any comparisons.
However, these results must be judged with caution because only one of the eight comparison groups exceed the recommended ten-record threshold to adequately assess the presence of a publication bias.
Discussion
Since their introduction, MISTs have become increasingly utilized for patients with BPH seeking definitive treatment [88]. While enucleation techniques may offer superior durability for LUTS, the benefits of MISTs include same-day discharge, minimal anesthesia, and preservation of sexual function [4, 45]. In this systematic review and meta-analysis, we found that both erectile and ejaculatory function were either preserved or improved across multiple MISTs. Specifically, patients who underwent Urolift and Rezum had significant improvements in erectile and ejaculatory function, while those undergoing TPLA, iTind, PAE, and Optilume preserved sexual function as compared to traditional BPH surgery.
When counseling patients interested in surgical management for BPH, it is critical to assess their priorities for sexual function [89]. A survey of 300 BPH patients found that over 90% considered erectile and ejaculatory function to be important considerations when considering treatment [90]. While men aged 50–59 were most concerned with permanent impacts on sexual function, over 60% of men over age 70 indicated that maintaining erectile and ejaculatory function was important to them. Therefore, it is essential to engage in shared decision-making with patient across all ages. While validated questionnaires such as the IIEF and MSHQ should certainly be utilized, clinicians must recognize their limitations. As noted in a recent review of ejaculatory dysfunction after various BPH treatments, the current questionnaires lack specific questions regarding the force, consistency, sensation, volume, and pain associated with ejaculation [91]. Additionally, clinicians must recognize that small changes in these questionnaires may not be clinically meaningful. A study by Rosen et al., for example. found that the minimal clinically important difference in IIEF scores was a change in four points or more [92]. Therefore, in addition to validated questionnaires, clinicians should seek to gain a detailed understanding of patient symptoms and bother in order to best address sexual health.
MISTs offer superior outcomes to medical therapy for both urinary and sexual function. Prior research has shown MISTs offer an average IPSS reduction of 50% and a Qmax improvement of 40–90%, while pharmacological combination therapy yields an IPSS reduction of 20% and Qmax improvement of 10% [93,94,95]. Furthermore, both alpha-blockers and 5-alpha-reductase inhibitors are associated with sexual side effects including retrograde ejaculation, decreased libido, and erectile dysfunction. Thus, minimally invasive treatments should be considered in patients dissatisfied with the sexual side effects of medical therapy. Across several studies comparing MISTs to medical therapy, we found improved sexual function outcomes with MISTs [44, 62, 74, 77]. It is important to note that the included studies in the present systematic review inconsistently reported pre- and post-operative data for whether patients were on alpha-blockers, 5-alha-reductease inhibitors, and/or phosphodiesterase-type 5 inhibitors such as daily tadalafil for urinary symptoms. The use of and potential discontinuation of these medications pos-operatively has the ability to impact the results of each study and our pooled outcomes pm sexual function, especially for retrospective studies.
While MISTs may offer superior outcomes for erectile and ejaculatory function compared to traditional surgeries, head to head comparisons have shown that they may not be as efficacious in terms of reducing urinary symptoms [45]. Studies have shown there may be a higher need for surgical re-treatment and/or need for medical therapies for BPH after undergoing treatment with a MIST [96]. One study found that 31% of patients who underwent Rezum resumed medical treatment for BPH with alpha-blockers, daily tadalafil, and/or 5-alpha-reductase inhibitors at a mean of 9 months post-procedure [97]. It is therefore important for clinicians to understand a patient’s priorities and counsel patients effectively regarding potential symptomatic improvement and side effects relative to other BPH treatment options.
Our findings show overall favorable outcomes for erectile and ejaculatory function after MISTs. This is similar to a recent pooled analysis, which showed ejaculatory dysfunction rates of 5% for TPLA, 3% for Rezum, 1% for iTIND, and 0% for Urolift, respectively [95]. Manfredi et al. (2022) compared sexual function outcomes across traditional surgeries to MIST, finding a statistically significantly higher rate of retrograde ejaculation after TURP (RR 13.31, 95% CI 8.37, 21.17), enucleation (RR 34.77, 95% CI 10.58, 127.82), and laser surgery (RR 17.37, 95% CI 5.93, 50.81) compared to the MISTs [98]. Data comparing MISTs to each other is currently limited. In three studies comparing Rezum and Urolift, there were no differences in erectile or ejaculatory outcomes [22, 31, 56]. Accordingly, patient characteristics, surgeon expertise, and institutional resources will likely continue to drive MIST selection in real-world settings until further comparative research is done.
Our study is not without limitations. Notably, the included studies were heterogeneous in terms of baseline erectile/ejaculatory function, sexual function questionnaires utilized (e.g. IIEF-5 vs. IIEF-EF vs. IIEF-15), and follow up duration. Additionally, many of the included studies were retrospective in nature. Differing numbers of patients in the included studies were on medical therapy for BPH and/or ED pre-operatively, and it is unclear how many of these patients discontinued therapy post-operatively, which may confound sexual function outcomes. This heterogeneity limits our ability to compare outcomes across MISTs. Despite these limitations, to the best of our knowledge this is the most up-to-date and comprehensive analysis of sexual function after MISTs. Future directions include long term follow up of both sexual function and urinary symptoms after MISTs, comparison of sexual outcomes amongst different MISTs, and evaluation of MISTs in patients with baseline erectile/ejaculatory dysfunction. Additionally, consideration should be given to the creation of more comprehensive questionnaires for ejaculatory function after various BPH treatments.
Conclusion
MISTs represent a promising option for patients with LUTS secondary to BPH who wish to preserve sexual function. This systematic review and meta-analysis demonstrated overall preservation or improvement in erectile and ejaculatory outcomes across MISTs compared with traditional BPH surgery. For patients considering surgical management for BPH, urologists must assess sexual function priorities and incorporate discussion of minimally invasive approaches as part of shared decision-making.
References
Patel ND, Parsons JK. Epidemiology and etiology of Benign prostatic hyperplasia and bladder outlet obstruction. Indian J Urol. 2014;30:170–6. https://doi.org/10.4103/0970-1591.126900.
Becher EF, McVary KT. Surgical procedures for BPH/LUTS: impact on male sexual health. Sex Med Rev. 2014;2:47–55. https://doi.org/10.1002/smrj.20.
Sandhu JS, Bixler BR, Dahm P, Goueli R, Kirkby E, Stoffel JT, et al. Management of lower urinary tract symptoms attributed to Benign prostatic hyperplasia (BPH): AUA guideline amendment 2023. J Urol. 2024;211:11–19. https://doi.org/10.1097/ju.0000000000003698.
Passarelli F, Castellani D, Secco S, Gacci M, Sibona M, Goumas IK, et al. Minimally invasive surgical techniques (MISTs) for Benign prostatic hyperplasia: results from a Delphi consensus project to shed light on controversial topics. World J Urol. 2025;43:363 https://doi.org/10.1007/s00345-025-05727-w.
Reale G, Cimino S, Bruno G, Palmieri F, Giardina R, Russo GI, et al. “Aquabeam® System” for Benign prostatic hyperplasia and LUTS: birth of a new era. A systematic review of functional and sexual outcome and adverse events of the technique. Int J Impot Res. 2019;31:392–9. https://doi.org/10.1038/s41443-019-0158-3.
Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372:n71 https://doi.org/10.1136/bmj.n71.
Schardt C, Adams MB, Owens T, Keitz S, Fontelo P. Utilization of the PICO framework to improve searching PubMed for clinical questions. BMC Med Inf Decis Mak. 2007;7:16. https://doi.org/10.1186/1472-6947-7-16.
Wan X, Wang W, Liu J, Tong T. Estimating the sample mean and standard deviation from the sample size, median, range and/or interquartile range. BMC Med Res Methodol. 2014;14:135. https://doi.org/10.1186/1471-2288-14-135.
Sterne JA, Hernán MA, Reeves BC, Savović J, Berkman ND, Viswanathan M, et al. ROBINS-I: a tool for assessing risk of bias in non-randomised studies of interventions. Bmj. 2016;355:i4919 https://doi.org/10.1136/bmj.i4919.
Sterne JAC, Savović J, Page MJ, Elbers RG, Blencowe NS, Boutron I, et al. RoB 2: a revised tool for assessing risk of bias in randomised trials. Bmj. 2019;366:l4898 https://doi.org/10.1136/bmj.l4898.
Agüero C, Depaquit TL, Uleri A, Berchiche W, Corral R, Peyrottes A, et al. Water vapor thermal therapy for treatment of lower urinary tract symptoms due to large Benign prostatic hyperplasia (≥ 80 g). World J Urol. 2025;43:69 https://doi.org/10.1007/s00345-024-05433-z.
Ahn ST, Lee DH, Cho SB, Lee HS, Han DE, Park TY, et al. Is prostate urethral lift effective in patients with multiple comorbidities? J Clin Med. 2022;11 https://doi.org/10.3390/jcm11071928
Aladesuru O, Amankwah K, Elterman D, Zorn KC, Bhojani N, Te A, et al. Pilot study of “Less is More” rezum for treatment of BPH. Urology. 2022;165:256–60. https://doi.org/10.1016/j.urology.2022.01.039.
Alegorides C, Fourmarier M, Eghazarian C, Lebdai S, Chevrot A, Droupy S. Treatment of Benign prostate hyperplasia using the Rezum® water vapor therapy system: results at one year. Prog Urol. 2020;30:624–31. https://doi.org/10.1016/j.purol.2020.05.004.
Al Rawashdah SF, Pastore AL, Velotti G, Fuschi A, Capone L, Suraci PP, et al. Sexual and functional outcomes of prostate artery embolisation: a prospective long-term follow-up, large cohort study. Int J Clin Pr. 2020;74:e13454. https://doi.org/10.1111/ijcp.13454.
Al-Singary W, Patel R, Obi-Njoku O, Patel HRH. The UroLift(®) System for lower urinary tract obstruction: patient selection for optimum clinical outcome. Minim Invasive Ther Allied Technol. 2022;31:456–61. https://doi.org/10.1080/13645706.2020.1816554.
Amparore D, Fiori C, Valerio M, Schulman C, Giannakis I, De Cillis S, et al. 3-Year results following treatment with the second generation of the temporary implantable nitinol device in men with LUTS secondary to Benign prostatic obstruction. Prostate Cancer Prostatic Dis. 2021;24:349–57. https://doi.org/10.1038/s41391-020-00281-5.
Anan G, Minami H, Fujishima Y, Kaga K. Efficacy and safety of prostatic urethral lift according to preoperative urinary retention and prostate volume: A Japanese real-world multicenter data. Int J Urol. 2025;32:190–7. https://doi.org/10.1111/iju.15621.
Annese P, d’Altilia N, Falagario UG, Tocci E, Mirone V, Simone G, et al. UroLift to preserve seminal parameters in young male with LUTS from BPH. World J Urol. 2024;42:486 https://doi.org/10.1007/s00345-024-05127-6.
Annese P, d’Altilia N, Mancini V, Falagario UG, Del Giudice F, Ferro M, et al. Preserving ejaculatory function in young patients with lower urinary tract symptoms: medium- to long-term follow-up of prostatic urethral lift at a single center. Ther Adv Urol. 2021;13:17562872211037109. https://doi.org/10.1177/17562872211037109.
Babar M, Loloi J, Azhar U, Tang K, Ines M, Singh S, et al. Rezum outcomes in relationship to number of injections: is less more? J Endourol. 2023;37:157–64. https://doi.org/10.1089/end.2022.0390.
Baboudjian M, Fourmarier M, Gondran-Tellier B, Pradere B, Userovici M, Alegorides C, et al. Head-to-head comparison of prostatic urethral lift and water vapor thermal therapy for the treatment of symptomatic Benign prostatic hyperplasia: a real-life study. Int Urol Nephrol. 2021;53:1757–63. https://doi.org/10.1007/s11255-021-02899-3.
Balsamo R, Tammaro S, Trivellato M, Crocetto F, Barone B, Fusco F, et al. Water vapor thermal therapy (Rezūm System) in patients with large prostates: results from a prospective comparative study. Minerva Urol Nephrol. 2024;76:759–67. https://doi.org/10.23736/s2724-6051.24.05883-x.
Bertolo R, Cipriani C, Giuliani MS, Maiorino F, Vittori M, Carilli M, et al. Prostatic arterial embolization as a micro-invasive treatment option for Benign prostatic obstruction: a subtle balance between short-term follow-up patient-reported outcomes and de-obstructive effectiveness. Community Case Study Front Urol. 2022;ume 2:2022 https://doi.org/10.3389/fruro.2022.960875.
Bertolo R, Iacovelli V, Cipriani C, Carilli M, Vittori M, Antonucci M, et al. Ejaculatory function following transperineal laser ablation vs TURP for Benign prostatic obstruction: a randomized trial. BJU Int. 2023;132:100–8. https://doi.org/10.1111/bju.16008.
Bhatia S, Acharya V, Jalaeian H, Kumar J, Bryant E, Richardson A, et al. Effect of prostate artery embolization on erectile function - a single center experience of 167 patients. J Sex Med. 2022;19:594–602. https://doi.org/10.1016/j.jsxm.2022.01.006.
Campobasso D, Siena G, Chiodini P, Conti E, Franzoso F, Maruzzi D, et al. Composite urinary and sexual outcomes after Rezum: an analysis of predictive factors from an Italian multi-centric study. Prostate Cancer Prostatic Dis. 2023;26:410–4. https://doi.org/10.1038/s41391-022-00587-6.
Canat HL, Gurbuz C, Bozkurt M. Transurethral resection of the prostate (TURP) versus transperineal laser ablation (TPLA) due to Benign prostatic hyperplasia (BPH): prospective and comparative study. Int Urol Nephrol. 2023;55:2747–52. https://doi.org/10.1007/s11255-023-03717-8.
Cantwell AL, Bogache WK, Richardson SF, Tutrone RF, Barkin J, Fagelson JE, et al. Multicentre prospective crossover study of the ‘prostatic urethral lift’ for the treatment of lower urinary tract symptoms secondary to Benign prostatic hyperplasia. BJU Int. 2014;113:615–22. https://doi.org/10.1111/bju.12540.
Carnevale FC, Iscaife A, Yoshinaga EM, Moreira AM, Antunes AA, Srougi M. Transurethral resection of the prostate (TURP) versus original and PErFecTED prostate artery embolization (PAE) due to Benign prostatic hyperplasia (BPH): preliminary results of a single center, prospective, urodynamic-controlled analysis. Cardiovasc Inter Radio. 2016;39:44–52. https://doi.org/10.1007/s00270-015-1202-4.
Chin CP, Garden EB, Ravivarapu KT, Shukla D, Omidele O, Levy M, et al. Medium-term real-world outcomes of minimally invasive surgical therapies for Benign prostatic hyperplasia: water vapor thermal therapy (rezum) vs prostatic urethral lift (UroLift) in a high-volume urban academic center. J Endourol. 2022;36:1559–66. https://doi.org/10.1089/end.2022.0385.
Cindolo L, Campobasso D, Conti E, Uricchio F, Franzoso F, Maruzzi D, et al. Do patients treated with water vapor therapy and meeting randomized clinical trial criteria have better urinary and sexual outcomes than an unselected cohort?. J Endourol. 2023;37:323–9. https://doi.org/10.1089/end.2022.0637.
Copelan O, Moss J, Freedman S, Coutinho K, Elterman D, Marotte J, et al. Preservation of sexual function with Optilume-a novel treatment for lower urinary tract symptoms secondary to Benign prostatic hyperplasia. J Sex Med. 2025;22:446–53. https://doi.org/10.1093/jsxmed/qdae206.
Delazar S, Azadnajafabad S, Firouznia K, Nowroozi MR, Amini E, Fotouhi M, et al. Outcomes of prostatic artery embolization for treating Benign prostatic hyperplasia symptoms: a prospective single-center study. Health Sci Rep. 2025;8:e70565. https://doi.org/10.1002/hsr2.70565.
De Nunzio C, Cantiello F, Fiori C, Crocerossa F, Tognoni P, Amparore D, et al. Urinary and sexual function after treatment with temporary implantable nitinol device (iTind) in men with LUTS: 6-month interim results of the MT-06-study. World J Urol. 2021;39:2037–42. https://doi.org/10.1007/s00345-020-03418-2.
de Rienzo G, Lorusso A, Minafra P, Zingarelli M, Papapicco G, Lucarelli G, et al. Transperineal interstitial laser ablation of the prostate, a novel option for minimally invasive treatment of Benign prostatic obstruction. Eur Urol. 2021;80:95–103. https://doi.org/10.1016/j.eururo.2020.08.018.
Dixon CM, Cedano ER, Pacik D, Vit V, Varga G, Wagrell L, et al. Two-year results after convective radiofrequency water vapor thermal therapy of symptomatic Benign prostatic hyperplasia. Res Rep Urol. 2016;8:207–16. https://doi.org/10.2147/rru.S119596.
Dogan K, Erbagci A, Sen H, Kervancioglu S, Erturhan MS, Seckiner İ, et al. Clinical outcomes of prostatic artery embolization in patients with Benign prostatic hyperplasia: a prospective clinical study. Turk J Urol. 2022;48:215–21. https://doi.org/10.5152/tud.2022.22004.
Elterman D, Alshak MN, Martinez Diaz S, Shore N, Gittleman M, Motola J, et al. An evaluation of sexual function in the treatment of lower urinary tract symptoms secondary to Benign prostatic hyperplasia in men treated with the temporarily implanted nitinol device. J Endourol. 2023;37:74–79. https://doi.org/10.1089/end.2022.0226.
Elterman D, Bhojani N, Vannabouathong C, Chughtai B, Zorn KC. Rezūm therapy for ≥80-mL Benign prostatic enlargement: a large, multicentre cohort study. BJU Int. 2022;130:522–7. https://doi.org/10.1111/bju.15753.
Elterman D, Bhojani N, Vannabouathong C, Chughtai B, Zorn KC. Large, multi-center, prospective registry of rezūm water vapor therapy for Benign prostatic hyperplasia. Urology. 2022;165:261–7. https://doi.org/10.1016/j.urology.2022.02.001.
Frego N, Saita A, Casale P, Diana P, Contieri R, Avolio PP, et al. Feasibility, safety, and efficacy of ultrasound-guided transperineal laser ablation for the treatment of Benign prostatic hyperplasia: a single institutional experience. World J Urol. 2021;39:3867–73. https://doi.org/10.1007/s00345-021-03685-7.
Ghahhari J, Sountoulides P, Campobasso D, Faieta A, Sessa F, Viola L, et al. Mid-term results of water vapor thermal therapy in patients with lower urinary tract symptoms related to Benign prostatic hyperplasia. Brief Res Rep Front Urol. 2022;ume 2:2022 https://doi.org/10.3389/fruro.2022.990560.
González Enguita C, López Martín L, Herranz Fernández LM, Sinues Ojas B, Barrera Rodríguez C, Extramiana Cameno J, et al. Multicenter study of the impact of Urolift® implantation in patients undergoing medical treatment for lower urinary tract symptoms secondary to Benign prostatic hyperplasia. Actas Urol Esp (Engl Ed). 2025;49:501708. https://doi.org/10.1016/j.acuroe.2025.501708.
Gratzke C, Barber N, Speakman MJ, Berges R, Wetterauer U, Greene D, et al. Prostatic urethral lift vs transurethral resection of the prostate: 2-year results of the BPH6 prospective, multicentre, randomized study. BJU Int. 2017;119:767–75. https://doi.org/10.1111/bju.13714.
Hawks-Ladds N, Cook R, Babar M, Zhu M, Schulz A, Loloi J, et al. Four years of real-world sexual function outcomes after Rezum therapy in men with and without baseline erectile dysfunction. J Sex Med. 2024;21:777–86. https://doi.org/10.1093/jsxmed/qdae087.
Hawks-Ladds N, Tawfik MM, Babar M, Zhu M, Loloi J, Labagnara K, et al. Long-term water vapor thermal therapy outcomes across a broad range of prostate volumes. Urol Pr. 2024;11:727–34. https://doi.org/10.1097/upj.0000000000000596.
Jankauskas T, Buržinskis E, Kaupas RS, Basevičius A, Jievaltas M. Prostatic artery embolization as a treatment option for symptomatic Benign prostatic hyperplasia: results from the prospective follow-up study in Lithuania. Medicina (Kaunas). 2023;59 https://doi.org/10.3390/medicina59101871
Kaplan SA, Moss JL, Freedman SJ. Two-year long-term follow-up of treatment with the Optilume BPH catheter system in a randomized controlled trial for Benign prostatic hyperplasia (The PINNACLE Study). Prostate Cancer Prostatic Dis. 2024;27:531–6. https://doi.org/10.1038/s41391-024-00833-z.
Kato Y, Kamatani A, Shigehara K, Mizokami A. Real-world short-term outcomes of prostate urethral lift in Japan: a prospective cohort study. Int J Urol. 2024;31:852–8. https://doi.org/10.1111/iju.15468.
Kim JH, Lee KS, Kim TH. Evaluation of clinical outcomes of prostatic urethral lift for Benign prostatic hyperplasia: an Asian population study. World J Mens Health. 2020;38:338–44. https://doi.org/10.5534/wjmh.190015.
Lim EC, Gu HM, Yu SH, Lim DG, Chung HS, Jung SI, et al. Comparison of the efficacy and safety of holmium laser enucleation of the prostate and prostate artery embolization: short-term follow-up results. Prostate Int. 2025;13:155–60. https://doi.org/10.1016/j.prnil.2025.03.001.
Lin YT, Amouyal G, Thiounn N, Pellerin O, Pereira H, Del Giudice C, et al. Intra-vesical prostatic protrusion (IPP) can be reduced by prostatic artery embolization. Cardiovasc Inter Radio. 2016;39:690–5. https://doi.org/10.1007/s00270-015-1235-8.
Loffroy R, Quirantes A, Guillen K, Mazit A, Comby PO, Aho-Glélé LS, et al. Prostate artery embolization using n-butyl cyanoacrylate glue for symptomatic Benign prostatic hyperplasia: a six-month outcome analysis in 103 patients. Diagn Inter Imaging. 2024;105:129–36. https://doi.org/10.1016/j.diii.2023.12.006.
Lombardo R, Santarelli V, Turchi B, Santoro G, Guercio A, Franco A, et al. Evaluation of peri-operative outcomes after prostatic urethral lift with emphasis on urodynamic changes, symptom improvement and sexual function. Diagnostics (Basel). 2024;14 https://doi.org/10.3390/diagnostics14192110
Long Depaquit T, Reus R, Uleri A, Bastide C, Berchiche W, Peyrottes A, et al. Comparative analysis of functional and economic outcomes of prostatic urethral lift and water vapor thermal therapy for male LUTS: a French perspective. Fr J Urol. 2025;35:102872. https://doi.org/10.1016/j.fjurol.2025.102872.
Manfredi C, Spirito L, Quattrone C, Bottone F, Romano L, Balsamo R, et al. Rezūm water vapor therapy vs. thulium laser enucleation for the treatment of Benign prostatic hyperplasia in patients with large prostates: a multicenter prospective comparative study. Prostate Cancer Prostatic Dis. 2025;https://doi.org/10.1038/s41391-025-00971-y
Marzano L, Thiounn N, Pereira H, Pellerin O, Dariane C, Del Giudice C, et al. Prostatic artery embolization allows to maintain full sexual activity in patients suffering from bothersome lower urinary tracts symptoms related to Benign prostatic hyperplasia. Cardiovasc Inter Radio. 2020;43:1202–7. https://doi.org/10.1007/s00270-020-02520-7.
McVary KT, El-Arabi A, Roehrborn C. Preservation of sexual function 5 years after water vapor thermal therapy for Benign prostatic hyperplasia. Sex Med. 2021;9:100454 https://doi.org/10.1016/j.esxm.2021.100454.
McVary KT, Gange SN, Gittelman MC, Goldberg KA, Patel K, Shore ND, et al. Erectile and ejaculatory function preserved with convective water vapor energy treatment of lower urinary tract symptoms secondary to Benign prostatic hyperplasia: randomized controlled study. J Sex Med. 2016;13:924–33. https://doi.org/10.1016/j.jsxm.2016.03.372.
McVary KT, Gittelman MC, Goldberg KA, Patel K, Shore ND, Levin RM, et al. Final 5-year outcomes of the multicenter randomized sham-controlled trial of a water vapor thermal therapy for treatment of moderate to severe lower urinary tract symptoms secondary to Benign prostatic hyperplasia. J Urol. 2021;206:715–24. https://doi.org/10.1097/ju.0000000000001778.
McVary KT, Rogers T, Mahon J, Gupta NK. Is sexual function better preserved after water vapor thermal therapy or medical therapy for lower urinary tract symptoms due to Benign prostatic hyperplasia?. J Sex Med. 2018;15:1728–38. https://doi.org/10.1016/j.jsxm.2018.10.006.
Minafra P, G DER, Gerbasi S, Cindolo L, Battaglia M, Ditonno P. Three years outcomes of transperineal laser ablation of the prostate. Minerva Urol Nephrol. 2023;75:471–8. https://doi.org/10.23736/s2724-6051.23.05270-9.
Minore A, Cacciatore L, Ferrari G, Siena G, Balsamo R, Morselli S, et al. Safety and efficacy of WVTT (Rezum) in young men: preliminary data. Int Urol Nephrol. 2025;57:2853–9. https://doi.org/10.1007/s11255-025-04463-9.
Müllhaupt G, Hechelhammer L, Graf N, Mordasini L, Schmid HP, Engeler DS, et al. Prostatic artery embolisation versus transurethral resection of the prostate for Benign prostatic obstruction: 5-year outcomes of a randomised, open-label, noninferiority trial. Eur Urol Focus. 2024;10:788–95. https://doi.org/10.1016/j.euf.2024.03.001.
Nguyen V, Winograd J, Codelia-Anjum AJ, Zorn KC, Elterman D, Bhojani N, et al. Feasibility assessment of catheter-free water vapor thermal therapy for treatment of Benign prostatic hyperplasia. World J Urol. 2024;42:383 https://doi.org/10.1007/s00345-024-05002-4.
Özkaptan O, Sevinç C, Çanakcı C, Aydoğan TB, Türkyılmaz O, Mert MS, et al. Comparison of outcome for holmium laser enucleation prostate and Rezum system in Benign prostate hyperplasia: a matched pair analysis. World J Urol. 2025;43:242 https://doi.org/10.1007/s00345-025-05644-y.
Patel NR, Elterman DS, Thulasidasan N, Altman R, Tai E, Zener R, et al. Initial canadian experience of prostate artery embolization for symptomatic Benign prostatic hyperplasia: midterm outcomes. Can Assoc Radio J. 2021;72:876–82. https://doi.org/10.1177/0846537120939930.
Pisco JM, Rio Tinto H, Campos Pinheiro L, Bilhim T, Duarte M, Fernandes L, et al. Embolisation of prostatic arteries as treatment of moderate to severe lower urinary symptoms (LUTS) secondary to Benign hyperplasia: results of short- and mid-term follow-up. Eur Radio. 2013;23:2561–72. https://doi.org/10.1007/s00330-012-2714-9.
Pisco JM, Bilhim T, Pinheiro LC, Fernandes L, Pereira J, Costa NV, et al. Medium- and long-term outcome of prostate artery embolization for patients with Benign prostatic hyperplasia: results in 630 patients. J Vasc Inter Radio. 2016;27:1115–22. https://doi.org/10.1016/j.jvir.2016.04.001.
Pisco J, Campos Pinheiro L, Bilhim T, Duarte M, Rio Tinto H, Fernandes L, et al. Prostatic arterial embolization for Benign prostatic hyperplasia: short- and intermediate-term results. Radiology. 2013;266:668–77. https://doi.org/10.1148/radiol.12111601.
Richardson A, Bhatia A, Maini A, Richardson K, Issa C, Strauber Z, et al. Impact on Sexual Function of Protective Coil Embolization of Penile Collaterals During Prostatic Artery Embolization. CardioVascular Interventional Radio. 2025;48:512–21. https://doi.org/10.1007/s00270-025-03966-3.
Roehrborn CG, Barkin J, Gange SN, Shore ND, Giddens JL, Bolton DM, et al. Five year results of the prospective randomized controlled prostatic urethral L.I.F.T. study. Can J Urol. 2017;24:8802–13.
Roehrborn CG, Rukstalis DB. Prostatic urethral lift versus medical therapy: examining the impact on sexual function in men with Benign prostatic hyperplasia. Eur Urol Focus. 2022;8:217–27. https://doi.org/10.1016/j.euf.2020.12.013.
Salem R, Hairston J, Hohlastos E, Riaz A, Kallini J, Gabr A, et al. Prostate artery embolization for lower urinary tract symptoms secondary to Benign prostatic hyperplasia: results from a prospective FDA-approved investigational device exemption study. Urology. 2018;120:205–10. https://doi.org/10.1016/j.urology.2018.07.012.
Samir M, Elaal AAA, Gad KAS, Basyony MW. Two-year follow-up comparing Rezūm therapy versus bipolar transurethral resection of the prostate for treating Benign prostatic hyperplasia. A prospective randomized study. Int J Urol. 2024;31:545–50. https://doi.org/10.1111/iju.15410.
Sapoval M, Thiounn N, Descazeaud A, Déan C, Ruffion A, Pagnoux G, et al. Prostatic artery embolisation versus medical treatment in patients with Benign prostatic hyperplasia (PARTEM): a randomised, multicentre, open-label, phase 3, superiority trial. Lancet Reg Health Eur. 2023;31:100672. https://doi.org/10.1016/j.lanepe.2023.100672.
Sessa F, Polverino P, Bisegna C, Siena G, Lo Re M, Spatafora P, et al. Transperineal laser ablation of the prostate with EchoLaser™ system: perioperative and short-term functional and sexual outcomes. Brief Res Rep Front Urol. 2022;ume 2:2022 https://doi.org/10.3389/fruro.2022.969208.
Sheba M, El Gamal F, Abd El Wahed M, Kotb S, Meshref A, Aly Hussein H, et al. Randomised controlled trial comparing safety and efficacy of Urolift to monopolar TURP. Urologia. 2025;92:59–64. https://doi.org/10.1177/03915603241277905.
Siena G, Cindolo L, Ferrari G, Maruzzi D, Fasolis G, Condorelli SV, et al. Water vapor therapy (Rezūm) for lower urinary tract symptoms related to Benign prostatic hyperplasia: early results from the first Italian multicentric study. World J Urol. 2021;39:3875–80. https://doi.org/10.1007/s00345-021-03642-4.
Sønksen J, Barber NJ, Speakman MJ, Berges R, Wetterauer U, Greene D, et al. Prospective, randomized, multinational study of prostatic urethral lift versus transurethral resection of the prostate: 12-month results from the BPH6 study. Eur Urol. 2015;68:643–52. https://doi.org/10.1016/j.eururo.2015.04.024.
Theurich AT, Leistritz L, Leucht K, Franiel T, Teichgräber U, Foller S, et al. Influence of prostate artery embolization on different qualities of lower urinary tract symptoms due to Benign prostatic obstruction. Eur Urol Focus. 2022;8:1323–30. https://doi.org/10.1016/j.euf.2022.01.011.
Thulasidasan N, Kok HK, Elhage O, Clovis S, Popert R, Sabharwal T. Prostate artery embolisation: an all-comers, single-operator experience in 159 patients with lower urinary tract symptoms, urinary retention, or haematuria with medium-term follow-up. Clin Radio. 2019;74:569.e1–569.e8. https://doi.org/10.1016/j.crad.2019.03.006.
Totaro A, Gavi F, Fettucciari D, Bizzarri FP, Sanesi D, Cosenza L, et al. Efficacy of the Rezūm system for lower urinary tract symptoms in patients with Benign prostatic hyperplasia: long term results from a single centre prospective study. Urologia. 2025;92:141–7. https://doi.org/10.1177/03915603241297137.
van Kollenburg R, van Riel L, Bloemen P, de Reijke T, Beerlage H, de Bruin D, et al. Transperineal laser ablation as treatment for Benign prostatic obstruction: Safety, feasibility and functional outcomes-A pilot study. BJUI Compass. 2024;5:52–59. https://doi.org/10.1002/bco2.278.
Woo HH, Bolton DM, Laborde E, Jack G, Chin PT, Rashid P, et al. Preservation of sexual function with the prostatic urethral lift: a novel treatment for lower urinary tract symptoms secondary to Benign prostatic hyperplasia. J Sex Med. 2012;9:568–75. https://doi.org/10.1111/j.1743-6109.2011.02568.x.
Young S, Moran P, Golzarian J. Ejaculatory dysfunction following prostate artery embolization: a retrospective study utilizing the male sexual health questionnaire-ejaculation dysfunction questionnaire. Diagn Inter Imaging. 2022;103:310–5. https://doi.org/10.1016/j.diii.2022.01.003.
Ditonno F, Manfredi C, Licari LC, Bologna E, Franco A, Pandolfo SD, et al. Benign prostatic hyperplasia surgery: a snapshot of trends, costs, and surgical retreatment rates in the USA. Eur Urol Focus. 2024;10:826–32. https://doi.org/10.1016/j.euf.2024.04.006.
Malde S, Umbach R, Wheeler JR, Lytvyn L, Cornu JN, Gacci M, et al. A systematic review of patients’ values, preferences, and expectations for the diagnosis and treatment of male lower urinary tract symptoms. Eur Urol. 2021;79:796–809. https://doi.org/10.1016/j.eururo.2020.12.019.
Bouhadana D, Nguyen DD, Zorn KC, Elterman DS, Bhojani N. Patient perspectives on Benign prostatic hyperplasia surgery: a focus on sexual health. J Sex Med. 2020;17:2108–12. https://doi.org/10.1016/j.jsxm.2020.07.006.
Khooblall P, Bole R, Leelani N, Lundy S, Bajic P. A scoping review of ejaculatory dysfunction due to surgical treatments for Benign prostatic hyperplasia: limitations of available tools for assessment and reporting. Sex Med Rev. 2023;11:375–83. https://doi.org/10.1093/sxmrev/qead002.
Rosen RC, Allen KR, Ni X, Araujo AB. Minimal clinically important differences in the erectile function domain of the International Index of Erectile Function scale. Eur Urol. 2011;60:1010–6. https://doi.org/10.1016/j.eururo.2011.07.053.
Cindolo L, Pirozzi L, Fanizza C, Romero M, Tubaro A, Autorino R, et al. Drug adherence and clinical outcomes for patients under pharmacological therapy for lower urinary tract symptoms related to Benign prostatic hyperplasia: population-based cohort study. Eur Urol. 2015;68:418–25. https://doi.org/10.1016/j.eururo.2014.11.006.
Cornu JN, Ahyai S, Bachmann A, de la Rosette J, Gilling P, Gratzke C, et al. A systematic review and meta-analysis of functional outcomes and complications following transurethral procedures for lower urinary tract symptoms resulting from Benign prostatic obstruction: an update. Eur Urol. 2015;67:1066–96. https://doi.org/10.1016/j.eururo.2014.06.017.
Franco A, Ditonno F, Manfredi C, Bologna E, Licari LC, Orecchia L, et al. Systematic review and pooled analysis of functional and sexual outcomes of minimally invasive surgical treatments for Benign prostatic obstruction. Eur Urol. 2025;https://doi.org/10.1016/j.eururo.2025.09.004
Dean NS, Assmus MA, Lee MS, Guo JN, Krambeck AE. Benign prostatic hyperplasia surgical re-treatment after prostatic urethral lift A narrative review. Can Urol Assoc J. 2023;17:353–9. https://doi.org/10.5489/cuaj.8334.
Nguyen V, Tran E, Cerrato C, Finegan JL, Leach MC, Bechis SK. Do patients Rezum medications?-a real-world analysis of medical retreatment after water vapor thermal therapy. Transl Androl Urol. 2025;14:3546–53. https://doi.org/10.21037/tau-2025-568.
Manfredi C, García-Gómez B, Arcaniolo D, García-Rojo E, Crocerossa F, Autorino R, et al. Impact of surgery for Benign prostatic hyperplasia on sexual function: a systematic review and meta-analysis of erectile function and ejaculatory function. Eur Urol Focus. 2022;8:1711–32. https://doi.org/10.1016/j.euf.2022.06.007.
Author information
Authors and Affiliations
Contributions
Conceptualization: RB, EC, MM. Methodology: MM, EC, NN, BL, RB. Investigation: EC, MM, AE, BL, VA, RB. Formal analysis: MM, EC. Project administration: RB, MM. Supervision: RB, RB, SD. Validation: NN, MM. Software: MM, EC. Visualization: MM, EC. Writing – original draft: EC, MM, NN, AE, VA. Writing–review and editing: RB, PB, SD, EC, MM.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Cahill, E.M., Lindenbaum, M.M., Estright, A. et al. The impact of minimally invasive surgical therapy for Benign prostatic hyperplasia on sexual function: a systematic review and meta-analysis. Prostate Cancer Prostatic Dis (2026). https://doi.org/10.1038/s41391-026-01091-x
Received:
Revised:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41391-026-01091-x
