
Abstract
Study design
Prospective, descriptive, analytical, observational study involving 12 multicenter, international centers from Spain and Italy.
Objectives
Determine the method for bladder voiding in spinal cord injury (SCI) patients concerning different intrinsic and environmental variables.
Introduction
Neurogenic bladder is common in spinal cord injury (SCI) patients, profoundly impacting their quality of life. While clean intermittent catheterization (CIC) is the preferred method due to fewer complications and infections and improved quality of life, alternative methods like indwelling catheterization or condom catheters are viable options for bladder management.
Methods
Data was gathered along the acute (at hospital admission), subacute (expectations at discharge) and hospital discharge phases.
Results
Data from 266 SCI patients was gathered. Main procedure for bladder voiding at the time of admission was indwelling catheterization (n = 242, 91.0%) and CIC was the most used procedure at discharge (n = 122, 45.9%). CIC is the preferred procedure when the evaluation of expectations at discharge is done (n = 181, 68.6%). The probability of achieving reflex voiding at discharge was higher as the American Spinal Injury Association (ASIA) Impairment Scale score improved (p < 0.001). A relationship was established with the level of injury (p < 0.001) and body mass index (p = 0.017), in addition to marital status, age and history of depression. Initial information about CIC was mostly provided by the urologist (n = 137, 73.3%) while training was predominantly done by the nurse (n = 159, 87.8%).
Conclusions
Differences in neurogenic bladder management were identified regarding level and injury severity, SCIM, BMI, marital status, age and depression history.
Sponsorship
B Braun Medical S.A.U.
Similar content being viewed by others
Introduction
Spinal cord injury (SCI) is associated with numerous multi-system complications such as cardiovascular, pulmonary, gastrointestinal, neurologic or genitourinary problems, especially during the acute phase of care [1]. In the case of the bladder, coordination between both the central and peripheral nervous systems is essential for the correct function of this organ. In SCI patients, either of these can be altered, with urinary incontinence secondary to neurogenic detrusor overactivity being the classic symptom. Therefore, its pathophysiology is described as an alteration in the micturition reflex that interrupts this reciprocal innervation leading to a dysfunctional voiding pattern with resulting complications [2]. It has been estimated that almost 80% of SCI patients experience some degree of neurogenic bladder (NGB) within the first year after the injury, with 42% of them being hospitalized due to these problems [3]. In fact, both renal failure and urinary sepsis have been historically considered major causes of death in SCI patients [4].
The introduction of clean intermittent catheterization (CIC) in the 1970s was an essential step in the urologic care of SCI patients, becoming the “gold standard” for the management of NGB [5, 6]. Compared to indwelling catheterization or the use of condom catheters, CIC produces significantly fewer complications such as stones, urinary tract infections, urinary tract fistulae, strictures or cancer [7,8,9]. Although CIC is the optimal method of bladder management in these patients, its performing or maintenance might not be feasible in all patients due to age, gender, comorbidities, level and severity of injury, upper extremity function, spasticity and, in developing countries, access to running water, sanitation, and catheter supplies [10]. In addition, inconveniences like the potential dependence on others and the often-continued leakage lead to patient non-compliance and discontinuation of CIC [11,12,13]. Therefore, alternative treatments such as pharmacologic therapy [9], injection of botulinum toxin [14] and surgical augmentation [15] or urinary diversion [16] have been developed to address NGB physiology at the bladder level instead of targeting the neurologic injury that leads to this condition.
However, little is known about the number of patients undergoing CIC when they are discharged from SCI units, as well as the main reasons for not opting for CIC to void the bladder. Although there is some research about this topic [17], to our knowledge, no study has been conducted neither in Spain or Italy regarding the treatment of bladder dysfunction in SCI patients, either during the acute and expectations at discharge phase or at the time of discharge from the rehabilitation center.
Methods
Study design
It was a prospective, descriptive, analytical, observational study involving 12 multicenter, international centers, five from Spain and seven from Italy. The main objective was to determine the method for bladder voiding during both the acute and expectations at discharge phases, and at hospital discharge in SCI patients. The secondary objectives were determining the preferences for bladder voiding in patients with SCI concerning sex, level of injury, cause of injury and body mass index; establishing the factors and environment of the patient that might have influenced the final method; knowing whether the timing of initiating CIC after the acute phase influenced the final choice; determining the major source of information about neurogenic bladder management at the time of hospital discharge; establishing a link between training time and adherence to CIC treatment; and determining the degree of satisfaction and knowledge about CIC of both the patient and their caregivers.
Inclusion criteria included any patient in the acute phase with SCI of traumatic or non-traumatic origin either admitted to the SCI unit for the first time or referred from another unit or hospitalization center unless they meet any exclusion criteria and have signed the informed consent. Exclusion criteria included patients referred from other SCI units who had already started a rehabilitation process; patients coming from countries other than Spain and Italy whose follow-up was difficult to establish once they were discharged; patients with mental or consciousness alterations that were expected to impede the correct training and learning of bladder management procedures; and any other medical factors that in the judgment of the investigator are exclusionary.
The study was approved by the Clinical Research Ethics Committee of the “Complejo Hospitalario de Toledo” (approval number 123, dated October 16, 2017). All the procedures were in accordance with the ethical principles of the Declaration of Helsinki, following good clinical practice (GCP) and ICH guidelines. Written informed content was obtained from all subjects before study-related procedures.
Data collection
Data was gathered in five questionnaires. The first one was completed at the time of patient admission within a maximum period of two weeks, also known as acute phase. Data included sociodemographic information about the patient, duration of hospital admission, etiology of the injury, complications, bladder management, scores in Spinal Cord Independence Measure (SCIM), Hospital Anxiety and Depression Scale (HADS) and the American Spinal Injury Association (ASIA) Impairment Scale, and expectations about the evolution of the patient. The second one was completed at the time the patient was discharged from the SCI unit and was considered to have completed his or her rehabilitation period. Gathered data included general information about the patient and complications during the hospital admission, SCIM and HADS scores, and bladder management. The other three questionnaires were completed only in those cases in which patients underwent CIC. The first one was completed between two and seven days after CIC proposal. The second one was filled between two and seven days after CIC initiation and the last questionnaire was completed at the time of hospital discharge. All these questionnaires included information about CIC management and the perception of both the hospital staff and the patient and/or caregiver.
The SCIM III is a scale composed of 19 items covering three different dimensions related to patient independence. These groups include questions about self-care (score range, 0–20), breathing and sphincter control (score range, 0–40) and both indoor and outdoor mobility (score range, 0–40) [18]. On the other hand, HADS is a scale consisting of 14 items, grouped into two subscales. The first one is composed of seven items and include information about depression, while the second one, composed of another seven items, encompassed data about anxiety [19]. Finally, the ASIA Impairment scale classifies SCIs as either complete or incomplete. Grades include A, which indicates an absence of all motor and sensory functions; B for patients who have some sensory function but no motor function; C for patients who have more than half of the key muscles below the neurogenic level with a grade less than 3; and D for injuries that have at least half of key muscles below the neurological level with a grade of 3 or more [20].
Statistical analysis
While qualitative variables were represented as absolute and relative frequencies, quantitative variables were depicted as mean and standard deviation (SD). To compare between procedures for bladder voiding, we utilized an analysis of variance (ANOVA) test for continuous variables (or Kruskal Wallis in case of lack of normality) and Pearson’s χ2 tests for categorical variables. All analyses were performed through the SPSS v26.0. Statistical significance was established at p = 0.05.
To analyze the association between categories of variables with bladder management using CIC, a Multiple Correspondence Analysis (MCA) was performed, which is used to detect and represent underlying structures (relationships, associations) in a nominal categorical data set, allowing the visualization of associations between categories of variables. The two dimensions that provide the most relevant information and best explain the variability of the results (dimension 1 and 2) were represented. The analysis was performed with the Jamovi program (running under the R language).
Results
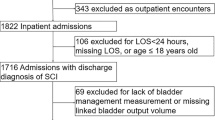
A total of 266 patients, 143 and 123 from Spanish and Italian centers respectively, were recruited.
Method for bladder voiding
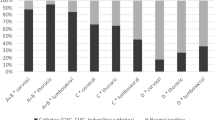
In the acute phase (at the time of admission to the SCI units), the main method for bladder voiding was indwelling catheterization (n = 242, 91.0%), while in the expectations at discharge was to use CIC (n = 181, 68.6%) as the primary method, followed by reflex voiding (n = 35, 13.3%) and transurethral indwelling catheterization (n = 22, 8.3%). At hospital discharge, intermittent catheterization (n = 122, 45.9%), reflex voiding (n = 78, 29.3%) and indwelling catheterization (n = 54, 20.3%) were mostly used (Fig. 1).

Data not available from n = 2 patients for the subacute phase. More than one method reported from some patients for the hospital discharge data.
Final bladder voiding method concerning sex, level of injury, cause of injury, body mass index and severity of injury
No statistically significant association was observed between bladder voiding method and patient sex (p = 0.260, Table 1). Comparisons involving condom catheters were inherently limited to male patients due to the nature of this modality. Patients with lumbosacral injuries had the lowest percentage requiring indwelling catheterization (5.9%), while intermittent catheterization was most common in dorsal (56.9%) and lumbosacral (55.9%) injuries. Reflex voiding was more frequent in patients with cervical or lumbosacral injuries compared to those with dorsal injuries (38.8%, 38.2% vs. 17.9% respectively). A significant association was observed between bladder management and injury level (p < 0.001). Among SCI patients, 158 (59.4%) had traumatic causes, and 108 (40.6%) had medical etiologies, with similar bladder voiding methods between groups (p = 0.575, Table 1). Finally, patients with higher body mass index (BMI) were more likely to use condom catheter or indwelling catheters than intermittent catheterization. Obesity significantly influenced bladder management (p = 0.017; Table 1).
Regarding severity of the injury, a statistically significant relationship was observed between the ASIA Impairment Scale and bladder management at discharge, with reflex voiding being more frequent in patients with better ASIA scale scores (p < 0.001). When ASIA grades were grouped, it was also observed that the probability of achieving reflex voiding at discharge was higher as ASIA improves (A/B vs C/D) (p < 0.001; Table 2). With regards to the SCIM scores, a statistically significant relationship was observed between partial and SCIM scores regarding bladder management. In fact, SCIM score was higher in patients with reflex voiding at discharge (p < 0.001; Table 3).
Patient and environmental factors that might influence the final method for bladder voiding
No relationship was observed between educational level and final voiding management (p = 0.263). Regarding marital status, indwelling catheterization was most common among widowed patients (n = 10, 52.6%), while intermittent catheterization was mainly used in single (n = 40, 53.3%) and married patients (n = 65, 46.1%). In divorced individuals, reflex voiding was mostly achieved (n = 11, 45.8%). Statistically significant differences were observed among the different groups (p < 0.001). Age was also significantly associated voiding method since patients undergoing indwelling catheter were older than those managed with intermittent catheterization, reflex voiding or condom catheters (70.0 ± 11.4 years vs. 47.4 ± 16.8 years, 48.6 ± 17.5 years and 58.1 ± 16.0 years, respectively; p < 0.001).
Only 8.3% (n = 22) presented a depression history. Of them, 40.9% (n = 9) underwent indwelling catheter, 27.3% (n = 6) intermittent catheterization, compared to 18.4% (n = 45) and 47.5% (n = 116) of patients without a history of depression. Reflex voiding was similar in both groups (31.8% [n = 7] vs 29.1% [n = 71]). The analysis revealed a statistically significant relationship with depression history (p = 0.044), while no association was observed between voiding method and anxiety history (p = 0.220; Table 4).
Influence of the timing of initiating CIC after the acute phase on the final bladder voiding method
A statistically significant association was observed between final bladder management and the days between injury (first hospital admission) and CIC proposal (p = 0.007), with fewer days for reflex voiding than indwelling catheterization (p = 0.014). A trend suggested fewer days with intermittent catheterization than indwelling catheterization (p = 0.083). Additionally, final management was linked to days from injury to CIC initiation (p = 0.002), with reflex showing fewer days than permanent catheterization (p = 0.014), condom catheter (p = 0.018) or intermittent catheterization (p = 0.045).
Degree of knowledge about CIC by patients and their caregivers
Initial information about CIC involved in 73.3% of the cases the urologist, in 54.0% the nurse and in 45.5% the rehabilitator specialist. The training was mostly provided by the nurse (87.8%). According to the investigators’ opinion, 88.0, 88.3 and 99.2% of patients understood the need for CIC during treatment proposal, treatment initiation and hospital discharge, respectively. On the other hand, 79.8% of patients undergoing CIC were prepared for the procedure during treatment initiation, while this percentage increased to 97.7% during hospital discharge.
Multivariate analysis
The multivariate analysis showed an association between bladder management with CIC with the variables of no obesity, no depression, <55 years, and dorsal and lumbosacral lesions (Fig. 2A). On the other hand, bladder management through indwelling catheterization or other methods other than CIC or micturition was associated with obesity, depression, cervical injury and age (≥55 years; Fig. 2B).

A Associations of CIC with nominal categorical variables. B Associations of indwelling catheterization or other non-CIC methods with nominal categorical variables.
Discussion
Neurogenic bladder is a widely common complication among SCI patients [3], significantly impacting quality of life for 40–60% of them. It interferes with daily activities, creating a barrier to social interaction and often requires extensive caregiver support making it a costly condition [21]. Therefore, it is crucial to understand the decisions underlying the choice of treatment for its management.
Our study found that indwelling catheterization was the main method for bladder voiding during hospital admission, shifting to CIC use during the subacute phase and hospital discharge. At discharge, 45.9% of patients used CIC, followed by reflex voiding (29.3%) and indwelling catheterization (20.3%). These findings align with previous studies, although prevalence rates underscore differences in clinical practices across region. In Switzerland, intermittent catheterization was most common (39%) in SCI patients [22], followed by indwelling catheterization (22%), while in Taiwan, self-voiding was predominant (47.6%), followed by indwelling catheterization (32.4%), whereas CIC usage remained at 18.4% [23]. Moreover, 55.0% of participants changed their voiding method, especially among singles (44.9%) and those with cervical (44%) and thoracic injuries (40.6%), a trend also observed in our results. Other studies reported that 59.2% of the patients underwent CIC at discharge from rehabilitation (61.5% male and 49.5% female), while indwelling catheterization stayed at 31.9% (29.3% for males and 42.9% for females) [17].
Our study further highlights the role of injury level on bladder management. Indwelling catheterization was less commonly used in patients with lumbosacral injuries (5.9%), due to better motor control, while intermittent catheterization was preferred in dorsal (56.9%) and lumbosacral injuries (55.9%), reflecting its suitability for neurogenic bladder management. Remarkably, although one patient used suprapubic catheter at admission, none were discharged with this method. This reflects clinical decision-making in the participating centers, where other methods, such as intermittent or indwelling catheterization, were preferred. These findings suggest the need to tailor bladder management strategies based on injury severity, functional capacity, and clinical context. Additionally, the public healthcare systems in Spain and Italy, which offer subsidized or free access to catheters and other essential supplies [24, 25], likely reduce financial barriers that could influence management decisions. However, indirect costs (caregiver support, transportation) may still affect adherence. In contrast, healthcare systems in other regions, where out-of-pocket expenses are more prevalent, may impose significant financial burdens that heavily impact patient choices.
Our study revealed that gender and injury etiology are not associated with bladder management, unlike the injury level and the BMI. This contrasts with previous research, where significant gender differences in bladder management were reported. For instance, a Norwegian study on SCI patients reported that males were more likely to perform CIC (72.8% vs. 48.5%) and use condom catheters, while females showed a higher reliance on Mitrofanoff uroplasty (1.7% vs. 7.4%, p < 0.01) and incontinence pads (8.3% vs. 35.3%, p < 0.01) [26]. These differences were particularly notable based on injury levels, particularly in thoracic injuries. Suprapubic catheter use at discharge was higher among females (22%) than males (17%), with females having thoracic grade A, B, C injuries showing higher odds of this method (p = 0.013) [27]. Similarly, a 40- to a 50-year follow-up study among 43 SCI patients in China reported that 75% of males with SCI initially used condom catheter, decreasing to 42% by the eighth 5-year interval, while 33% of females consistently used CIC over the same period [27]. Condom catheterization was more common in cervical injuries (63%) than in lower-level injuries (42%), with a similar decline observed over time. Additionally, another study observed that females were more likely to use bladder storage medications (p < 0.001) and Mitrofanoff uroplasty (7.4% vs. 1.7%), while males relied on CIC (72.8% vs. 48.5%) and condom catheters, particularly in individuals with AIS grade C or higher sub-cervical injuries [28]. In contrast, our study found no significant gender differences in bladder management methods available to both male and female patients. Comparisons involving condom catheters were inherently limited to male patients, and intermittent catheterization being the most frequent method at discharge (45.9%), particularly in patients with dorsal and lumbosacral injuries (56.9 and 55.9%, respectively). These differences may reflect variations in clinical practices, patient populations, and injury characteristics. While previous studies highlight the influence of gender and injury level on bladder management, our results suggest that management strategies should be tailored to functional recovery and the availability of optimal management options, such as CIC, which is associated with fewer complications and better outcomes.
Regarding the time to treatment initiation, it ranged from 40 days of reflex voiding to over 100 days for condom catheterization, with intermittent and indwelling catheterization between these values. This aligns with previous studies that reported a median of 58 days for long-term bladder management in SCI patients [29], while a Western Australian retrospective study found a median of 21.5 days for initial indwelling catheterization until progressing to CIC, extending to 40.4 days for patients with complete tetraplegia [30].
The duration of indwelling catheterization is particularly relevant. A retrospective study of inpatients with a new-onset SCI recommended limiting indwelling catheterization to 30 days to reduce urinary tract infection risk, which may may increase by four beyond this period [7]. In our cohort, the relatively short duration of indwelling catheter use before transitioning to other modalities reflects efforts to minimize such risks while promoting safer long-term strategies like CIC.
Additionally, the role of education in successful blader management was evident in our results, with urologist providing initial information (73.3%) and nurses leading patient training (87.8%). This aligns with findings from a Norwegian survey [24], where specialist at the spinal cord units were the main source of advice (45.9% female vs. 42.1% male), followed by general practitioners (29.7% female vs. 32.2% male) and urologists (24.3% female vs. 19.8% male) particularly for patients with tetraplegia compared to patients with paraplegia (52.6% vs 42.9%). Our study showed high preparedness rates for CIC at discharge (97.7%) highlighting the effectiveness of education in ensuring safe, long-term bladder management.
Regarding the time of CIC training sessions, previous studies have highlighted differences based on patients characteristics. One study found similar catheterization times for men (8.8 min) and women (8.5 min) (p = 0.864), but longer times for patients with cervical injuries (mean 12.4 min), women requiring caregiver assistance (mean 20 min), and in obese/overweight women (14.5 min vs. 7 min for normal weight, p = 0.036). These variations may impact treatment adherence and long-term decision-making in bladder management [31]. In our study, 97.7% of patients were adequately prepared for CIC at discharge underscoring the role of healthcare professionals in effective training. However, a survey among 1479 SCI patients identified challenges associated with CIC use, including inconvenience (36%), leakage (20%) and infections (19%) [32]. Similarly, another study reported that 42% of the patients transitioned from CIC to urethral indwelling catheterization (21.4%), citing recurrent urinary tract infections, incontinence, nephrolithiasis, dependence on caregivers and urethral structures [33]. Our findings align with these observations, emphasizing the importance of individualized support and education to ensure successful CIC use and reduce barriers.
This study has several strengths that enhance its relevance and applicability. Its prospective, multicenter design, involving 12 SCI units across Spain and Italy, ensures a broad representation of real-world clinical practices and captures variations across diverse healthcare settings. The use of validated tools (SCIM and ASIA Impairment Scale) strengthens the reliability of the findings, while the analysis of patient-specific and environmental factors (BMI, injury level, marital status, and depression history) provides valuable insights for personalized care. The emphasis on real-world data bridges the gap between controlled research environments and routine clinical practice, highlighting the practical challenges and successes of transitioning patients into long-term management. Additionally, high preparedness rates for CIC at discharge underscore the effectiveness of education and support provided by healthcare professionals. However, its focus on two Southern European countries may limit generalizability. The absence of systematic urodynamic evaluations, such as post-void residual volume or detrusor-sphincter dyssynergia, also restricts the ability to assess the functional adequacy of reflex voiding. Furthermore, the study focuses on the hospitalization period without evaluating post-discharge adherence. Despite these limitations, the findings provide actionable insights into neurogenic bladder management and highlight areas for improvement. Future studies should incorporate longer follow-up periods, urodynamic assessments, and adherence data to optimize SCI patient care.
CIC is the “gold standard” for the management of neurogenic bladder, due to fewer complications and a higher quality of life. However, it may not be the final method, as patient conditions and environmental factors influence bladder management. In this study, CIC is the most used procedure at discharge. Factors affecting bladder management included injury level, BMI, SCIM, marital status, age and depression. Reflex voiding at discharge was higher as the ASIA Impairment Scale score improved. CIC was more common in patients without obesity or depression, age below 55 years and either dorsal and lumbosacral injuries. The timing of CIC initiation also had an influence (reflex voiding occurred sooner than indwelling catheterization), and there was a trend towards an earlier CIC use.
Data availability
Data is available from the corresponding author upon reasonable request.
References
Eckert MJ, Martin MJ. Trauma: spinal cord injury. Surg Clin North Am. 2017;97:1031–45.
Hamid R, Averbeck MA, Chiang H, Garcia A, Al Mousa RT, Oh SJ, et al. Epidemiology and pathophysiology of neurogenic bladder after spinal cord injury. World J Urol. 2018;36:1517–27.
Redshaw JD, Lenherr SM, Elliott SP, Stoffel JT, Rosenbluth JP, Presson AP, et al. Protocol for a randomized clinical trial investigating early sacral nerve stimulation as an adjunct to standard neurogenic bladder management following acute spinal cord injury. BMC Urol. 2018;18:72.
Strauss DJ, Devivo MJ, Paculdo DR, Shavelle RM. Trends in life expectancy after spinal cord injury. Arch Phys Med Rehabil. 2006;87:1079–85.
Bloom DA, McGuire EJ, Lapides J. A brief history of urethral catheterization. J Urol. 1994;151:317–25.
Larsen LD, Chamberlin DA, Khonsari F, Ahlering TE. Retrospective analysis of urologic complications in male patients with spinal cord injury managed with and without indwelling urinary catheters. Urology. 1997;50:418–22.
Esclarín De Ruz A, García Leoni E, Herruzo Cabrera R. Epidemiology and risk factors for urinary tract infection in patients with spinal cord injury. J Urol. 2000;164:1285–9.
Abrams P, Agarwal M, Drake M, El-Masri W, Fulford S, Reid S, et al. A proposed guideline for the urological management of patients with spinal cord injury. BJU Int. 2008;101:989–94.
Stöhrer M, Blok B, Castro-Diaz D, Chartier-Kastler E, Del Popolo G, Kramer G, et al. EAU guidelines on neurogenic lower urinary tract dysfunction. Eur Urol. 2009;56:81–8.
Romo PGB, Smith CP, Cox A, Averbeck MA, Dowling C, Beckford C, et al. Non-surgical urologic management of neurogenic bladder after spinal cord injury. World J Urol. 2018;36:1555–68.
Wyndaele JJ. Complications of intermittent catheterization: their prevention and treatment. Spinal Cord. 2002;40:536–41. https://doi.org/10.1038/sj.sc.3101348
Cameron AP, Clemens JQ, Latini JM, McGuire EJ. Combination drug therapy improves compliance of the neurogenic bladder. J Urol. 2009;182:1062–7.
Manack A, Motsko SP, Haag-Molkenteller C, Dmochowski RR, Goehring EL Jr, Nguyen-Khoa BA, et al. Epidemiology and healthcare utilization of neurogenic bladder patients in a US claims database. Neurourol Urodyn. 2011;30:395–401.
Chen SF, Kuo HC. Will repeated botulinum toxin A improve detrusor overactivity and bladder compliance in patients with chronic spinal cord injury? Tzu Chi Med J. 2020;33:101–7.
Balanca A, Even A, Malot C, Chartier-Kastler E, Denys P, Joussain C. Long-term clinical and urodynamic effectiveness of augmentation ileocystoplasty with supra-trigonal cystectomy in individuals with spinal cord injury. World J Urol. 2022;40:2121–7.
Peterson AC, Curtis LH, Shea AM, Borawski KM, Schulman KA, Scales CD Jr. Urinary diversion in patients with spinal cord injury in the United States. Urology. 2012;80:1247–51.
Zlatev DV, Shem K, Elliott CS. How many spinal cord injury patients can catheterize their own bladder? The epidemiology of upper extremity function as it affects bladder management. Spinal Cord. 2016;54:287–91. https://doi.org/10.1038/sc.2015.169
Catz A, Itzkovich M, Agranov E, Ring H, Tamir A. SCIM-spinal cord independence measure: a new disability scale for patients with spinal cord lesions. Spinal Cord. 1997;35:850–6.
Zigmond AS, Snaith RP. The hospital anxiety and depression scale. Acta Psychiatr Scand. 1983;67:361–70. https://doi.org/10.1111/j.1600-0447.1983.tb09716.x
Roberts TT, Leonard GR, Cepela DJ. Classifications in brief: American Spinal Injury Association (ASIA) impairment scale. Clin Orthop Relat Res. 2017;475:1499–504.
Tate DG, Wheeler T, Lane GI, Forchheimer M, Anderson KD, Biering-Sorensen F, et al. Recommendations for evaluation of neurogenic bladder and bowel dysfunction after spinal cord injury and/or disease. J Spinal Cord Med. 2020;43:141–64.
Anderson CE, Birkhäuser V, Jordan X, Liechti MD, Luca E, Möhr S, et al. Urological management at discharge from acute spinal cord injury rehabilitation: a descriptive analysis from a population-based prospective cohort. Eur Urol Open Sci. 2022;38:1–9.
Yeh HL, Kuo HC, Tsai CH, Lee RP. Reasons for altering bladder management and satisfaction with current bladder management in chronic spinal cord injury patients. Int J Environ Res Public Health. 2022;19:17032.
Spain. Royal Decree 1030/2006, of September 15, establishing the common portfolio of services of the National Health System and the procedure for its update. Official State Gazette (BOE). 2006. https://www.sanidad.gob.es/profesionales/prestacionesSanitarias/CarteraDeServicios/docs/BOE-A-1030-2006-consolidado.pdf. Accessed 14 Jan 2025.
Italy. Law No. 833 of December 23, 1978: Establishment of the National Health Service. Official Gazette of the Italian Republic. 1978. https://faolex.fao.org/docs/pdf/ita194788.pdf. Accessed 14 Jan 2025.
Hagen EM, Rekand T. Management of bladder dysfunction and satisfaction of life after spinal cord injury in Norway. J Spinal Cord Med. 2014;37:310–6.
Gao Y, Danforth T, Ginsberg DA. Urologic management and complications in spinal cord injury patients: a 40- to 50-year follow-up study. Urology. 2017;104:52–58.
Anderson CE, Birkhäuser V, Liechti MD, Jordan X, Luca E, Möhr S, et al. Sex differences in urological management during spinal cord injury rehabilitation: results from a prospective multicenter longitudinal cohort study. Spinal Cord. 2023;61:43–50.
Hennessey DB, Kinnear N, MacLellan L, Byrne CE, Gani J, Nunn AK. The effect of appropriate bladder management on urinary tract infection rate in patients with a new spinal cord injury: a prospective observational study. World J Urol. 2019;37:2183–8.
Goodes LM, King GK, Rea A, Murray K, Boan P, Watts A, et al. Early urinary tract infection after spinal cord injury: a retrospective inpatient cohort study. Spinal Cord. 2020;58:25–34.
Velaer KN, Welk B, Ginsberg D, Myers J, Shem K, Elliott C. Time burden of bladder management in individuals with spinal cord injury. Top Spinal Cord Inj Rehabil. 2021;27:83–91.
Patel DP, Herrick JS, Stoffel JT, Elliott SP, Lenherr SM, Presson AP, et al. Reasons for cessation of clean intermittent catheterization after spinal cord injury: results from the Neurogenic Bladder Research Group spinal cord injury registry. Neurourol Urodyn. 2020;39:211–9.
Afsar SI, Yemisci OU, Cosar SN, Cetin N. Compliance with clean intermittent catheterization in spinal cord injury patients: a long-term follow-up study. Spinal Cord. 2013;51:645–9.
Funding
Financial support from B Braun Medical S.A.U. was received for this study.
Author information
Authors and Affiliations
Contributions
Conception and/or design: AGA, FGH, SB, ARS, MEFV, BMF, JBP, JVS, ABD, GDP, SP, EL, MGO, MS; Data acquisition: AGA, FGH, SB, ARS, MEFV, BMF, JBP, JVS, ABD, GDP, SP, EL, MGO, MS; Results interpretation: AGA, FGH, SB, ARS, MEFV, BMF, JBP, JVS, ABD, GDP, SP, EL, MGO, MS; Manuscript drafting and/or critical revision: AGA, FGH, SB, ARS, MEFV, BMF, JBP, JVS, ABD, GDP, SP, EL, MGO, MS; Final approval of the version to be published: AGA, FGH, SB, ARS, MEFV, BMF, JBP, JVS, ABD, GDP, SP, EL, MGO, MS.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethical approval
The study was approved by the Ethics Committee. All the procedures were in accordance with the ethical principles of the Declaration of Helsinki, following good clinical practice (GCP) and ICH guidelines.
Informed content
Written informed content was obtained from all subjects before study-related procedures.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Gil-Agudo, Á., Gutiérrez Henares, F., Biscotto, S. et al. Monitoring of neurogenic bladder management from hospital admission until discharge in spinal cord injury units: the SIRCA study. Spinal Cord 63, 530–537 (2025). https://doi.org/10.1038/s41393-025-01108-7
Received:
Revised:
Accepted:
Published:
Version of record:
Issue date:
DOI: https://doi.org/10.1038/s41393-025-01108-7
