
Abstract
Currently, there is still debate over the effectiveness of transcranial direct current stimulation (tDCS) in treating obsessive-compulsive disorder (OCD), posttraumatic stress disorder (PTSD) and anxiety disorders (ADs). To investigate the immediate and long-term effectiveness of tDCS in these diseases, we conducted a systematic review and quantitative analysis of existing literature on the treatment of OCD, PTSD, and ADs with tDCS. Following the PRISMA guidelines, we searched seven electronic databases and systematically retrieved articles published from May 2012 to June 2024 that compared the effects of active tDCS with sham stimulation in the treatment of these disorders. We included primary outcome measures such as the change scores in disorder-specific and general anxiety symptoms before and after treatment, as well as secondary outcomes such as changes in disorder-specific and general anxiety symptoms at follow-up. We also assessed the impact of tDCS on depressive symptoms. Fifteen papers met the eligibility criteria. Overall, the results of meta-analysis indicated that tDCS had a high effect in improving specific symptoms (SMD = −0.73, 95% CI: −1.09 to −0.37) and general anxiety symptoms (SMD = −0.75; 95% CI: −1.23 to −0.26) in OCD, PTSD and ADs, with effects lasting up to 1 month and showing a moderate effect size. Furthermore, tDCS demonstrated immediate and significant alleviation of depressive symptoms in these diseases. This study concludes that tDCS can serve as a non-invasive brain stimulation technology for treating these disorders, and the therapeutic effects can be maintained for a period of time.
Similar content being viewed by others


Introduction
The lifetime prevalence of obsessive-compulsive disorder (OCD), posttraumatic stress disorder (PTSD) and anxiety disorders (ADs) is approximately 21%, with an annual incidence of 14% [1]. These disorders share some basic clinical features, including excessive and persistent anxiety, attention bias towards threatening stimuli, hyperarousal and avoidance [2]. Therefore, the similar approaches would be applied composing drug treatment with selective serotonin reuptake inhibitors (SSRIs) and psychological intervention with cognitive behavioral therapy (CBT) [3,4,5]. However, the side effects of drug and issues such as the cost and commitment limitations of psychotherapy hinder adherence and affect treatment. About 30% of patients still cannot receive effective treatment [6,7,8]. New researches suggested non-invasive brain stimulation (NIBS), including repetitive transcranial magnetic stimulation (rTMS), transcranial direct current stimulation (tDCS), deep brain stimulation (DBS), and electroconvulsive therapy (ECT) may be a new treatment for OCD, PTSD and Ads [9]. Among these NIBS techniques, tDCS is characterized by its relatively safe, well-tolerable, low cost and convenient combination with pharmacotherapy, making it more suitable for clinical promotion and application [10]. Therefore, it is crucial and practical to determine the effect of tDCS on OCD, PTSD and ADs.
tDCS is a tool to modulate synaptic connections and induce cortical functioning by supplying a mild direct current (usually 0.5MA–2MA) over the scalp [10]. The effect of tDCS is polarity-dependent: anodal stimulation increases cortical excitability by depolarizing neurons, and cathodal stimulation inhibits cerebral excitability by hyperpolarizing neurons [11]. Additionally, parameters of tDCS such as current intensity, duration and stimulation sessions also have a significant influence on the level of excitability [12, 13]. However, the optimal protocol of tDCS is still being explored. Researches have shown that tDCS not only modulated cortical excitability by altering the resting membrane potential during stimulation but also modified synaptic activity to produce aftereffects [14]. Therefore, it is necessary to focus on both the immediate and long-term efficacy of tDCS.
NIBS, as a treatment technology, is based on physiology and pathological mechanism of the diseases. Increasing evidence to demonstrates that OCD is associate with hyperactivation of cortical-striatum-thalamus-cortical (CSTC) circuitry [15, 16], and several components of the circuitry such as orbitofrontal cortex (OFC), dorsolateral prefrontal cortex (DLPFC), and medial prefrontal cortex (mPFC) have been tested as targets for OCD treatment using NIBS [17, 18]. The brain regions involved in PTSD include the amygdal, dorsal anterior cingulate cortex (dACC) and mPFC, which are responsible for fear responses in humans [19, 20]. Moreover, DLPFC, as a core component of central executive network (CEN), is correlated with cognitive control in PTSD [21]. Although ADs involve different subtypes, they are closely related to fear responses [22]. Thus, the most consistent physiological characteristic of ADs is the overactivation of the amygdala, similar to PTSD [23, 24]. Neuroimaging studies have also highlighted the hypoactivity of the prefrontal cortex in anxiety patients, and emphasized that the hyperactivity amygdala might be caused by inadequate inhibitory control of the prefrontal cortex [25, 26]. As a result, the anodal target for NIBS in anxiety disorders is primarily focused on the left dorsolateral prefrontal cortex (L-DLPFC). Moreover, hypo- and hyperactivity in the left and right DLPFC is associated with emotional dysregulation and attention bias towards negative information in MDD [27]. tDCS may also be effective in alleviating symptoms of depression in these diseases. In summary, OCD, PTSD and ADs not only share fundamental clinical features but also involve similar neuropathological mechanisms, such as the amygdal and prefrontal cortex. Therefore, it is more valuable and meaningful to synthesize them in order to quantitatively analyze the effect of tDCS.
Previous meta-analysis studies amied to explore the efficacy of NIBS on specific symptoms of OCD [28], PTSD [29] and ADs [30] individually. Shu and colleagus inverstigated the efficacy of NIBS on OCD that included four tDCS studies. The authors concluded that tDCS was not superior to the sham stimulation in alleviating OCD symptoms [28]. Rebecca and colleagus did not quantitatively explore the effects of tDCS on posttraumatic core symptoms due to limitations in the number of studies. Their paper included two tDCS studies both of which suggested a significant reduction in PTSD symptoms compared to the sham tDCS [29]. Alessandra and colleagus conducted a quantitative analysis of the effectiveness of NIBS in the treatment of anxiety disorders. Their study showed that NIBS can alleviate clinical symptoms in patients with anxiety disorders, but they didn’t analyse the potency of tDCS separately [30]. Overall, on the one hand, we discover the effect of tDCS has not received enough attention, and its long-term effects are seldom noticed. On the other hand, previous meta-analysis explored the effect of tDCS on OCD, PTSD, and ADs separately instead of integrating them.
In conclusion, our study aims to conduct a quantitative analysis of existing studies on tDCS for OCD, PTSD, and ADs. We will investigate the immediate and long-term efficacy of tDCS for specific symptoms and general anxiety symptoms in these diseases. Considering that the comorbidity of anxiety and depression is up to 30–67% [31], and existing meta-analyses have already indicated that tDCS can treat major depressive episodes [32]. We will also examine the effectiveness of tDCS for depression symptoms in OCD, PTSD, and ADs. Finally, we will test the association between tDCS stimulation parameters and effect sizes using meta-analysis regression.
Methods
The present review followed the Preferred Reporting Items for Systematic Review and Meta-Analysis (PRISMA) [33]. This meta-analysis was registered with the PROSPERO, with the registration number CRD42023418957 (https://www.crd.york.ac.uk/PROSPERO).
Search strategy
Four English databases including PubMed, Web of Science, Embase and the Cochrane Library, and three Chinese databases involving Chinese National Knowledge Infrastructure (CNKI), WanFang and the Chinese Biomedical Literature Database (CBM), were systematically searched articles related to the treatment of OCD, PTSD, and ADs with tDCS from May 2012 to June 5th 2024. In our search, we discovered that the first study on tDCS therapy for related disorders was published in May 2012 [34], prompting us to commence within this period. We adopted Medical Subject Headings (MeSH) or Entry Terms for “tDCS” along with relevant disorders (such as “obsessive compulsive disorder,” “posttraumatic stress disorder,” “generalized anxiety disorder,” “panic disorder,” “agoraphobia,” “specific phobia,” “social anxiety disorder”) (See Supplementary materials STable 1). Additionally, we manually searched the related meta-analyses of our study to identify other eligible studies.
Inclusion and exclusion criteria
Studies were included if they fulfilled the following criteria: (1) 18–70 years old; (2) clinical diagnosis of OCD, PTSD or ADs according to DSM, ICD or CCMD, and clarify the diagnostic types of anxiety disorders; (3) Unrestricted use of medication and psychological therapy; (4) randomized, sham-controlled trials using tDCS, with consistent target areas for active and sham tDCS; if the study is the randomized controlled crossover trial, the data from the first stage will be used; (5) At least one validated clinical scale as an outcome measure.
Studies were excluded if: (1) no clear criteria of clinical diagnosis; (2) Comorbid neurological diseases, current addiction, bipolar, psychotic, and neurocognitive disorders; (3) no sham tDCS as control or the target areas for active and sham tDCS were inconsistent; (4) duplicated data sets; (5) review, case-report, meta-analysis, and meeting abstracts. Furthermore, comorbid depression and anxiety disorders were not considered as criteria for exclusion.
Records screening and data extraction
Firstly, two researchers (XL, HP) independently conducted preliminary screening according to inclusion and exclusion criteria based on the research title and abstract. The records were categorized as “include,” “exclude” or “maybe”. Then, studies that could not be determined for inclusion underwent full-text reading and screening. Any conflicts during the title-abstract and full-text screening stages were resolved through discussion and reach consensus. If consensus could not be reached, the researchers would discuss with a third senior researcher. Finally, two researchers independently extracted and verified data form included literature. The following data were extracted: article indexing information, subject demographic information, tDCS treatment parameters, outcome measures, and pre- and post- treatment data, including follow-up data. If the data was unavailable in original publications, the corresponding author was contacted.
Study quality assessment
Two researchers (XL, HP) conducted independent assessments of the quality of the included studies using the Cochrane Collaboration’s Risk of Bias Tool (RoB2) [35]. This tool is structured into five bias domains, which include “the randomization process,” “intended interventions,” “missing outcome data,” “measurement of the outcome” and “selection of the reported result.” The overall risk of bias for a study depends on assessment of each individual domain. If all domains are judged to have a low risk of bias, the overall risk of bias is considered low and the study is considered to have high quality. Conversely, if at least one domain is judged to raise some concerns and not to be at high risk of bias for any domain, the overall risk of bias is considered to have some cencerns and the study is considered to have moderate quality. Furthermore, other merging estimation is considered to have a high risk. To determine the bias in the domain of “selection of the reported result,” researchers examined the registered protocol provided in the paper. Conflicts were resolved through consultation, and a third researcher was consulted if necessary.
Quantitative analysis
The data extracted from each study were quantitatively analyzed. The primary outcome measures were the change scores of pre-post treatment mean difference in disorder-specific symptoms scale and general anxiety symptoms scale. The secondary outcome measures included the change scores of before treatment to follow-up mean difference in disorder-specific symptoms scale and general anxiety symptoms scale, as well as the change scores of pre-post treatment mean difference in general depression symptoms scale. When there were two validated clinical questionnaires assessing the same outcome (e.g., anxiety symptoms: HAMA, BAI), the scale that was used more frequently in other studies was selected. The standard deviation of the change score was calculated as suggested by the Cochrane Handbook for systematic Reviews of Interventions [35], as follows:
where corr is the correlation between pre- and post-measurements variances, set at 0.5 as suggested by Follman and colleagues [36].
The analysis was performed using Stata 16.0. Using the “metan” package to calculate Hedges’g as the measure of effect size. This calculation helps correct bias due to small samples sizes [36]. Heterogeneity was assessed using Q-test and I2 metric. Subgroup analysis by diseases was conducted to explore whether disease was the source of heterogeneity. Sensitivity analysis was performed using the “metaninf” package to test for heterogeneity caused by outliers in a study. Additionally, Egger’s regression and the funnel plot were used to analyze publication bias. Finally, meta-regression was employed to investigate the association between tDCS stimulation parameters (the number of sessions, current intensity, session duration, anode targets) and effect sizes. Among them, convert anode targets into dummy variables for regression analysis. According to the Cochrane Handbook’s recommendations, a funnel plot and meta-regression is conducted when there are at least 10 studies [35]. Due to the different features included in the studies (such as patient characteristics, stimulation parameters, scales, etc.) and the presence of varying effect sizes, the random effects model was chosen for all analyses. This model helps to account for the errors caused by sampling errors and real differences in effect sizes [37, 38].
Results
Study selection and characteristics
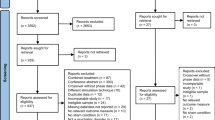
The literature search is presented in Fig. 1. A total of 2094 records were retrieved from 7 databases, and 683 duplicate records were removed. Based on the inclusion criteria, full-text of 28 papers was retrieved, and 15 papers were ultimately included in the analysis. Among these, the study by Jafari et al. [39] and Jaber et al. [40] included subjects divided into three groups: both active tDCS groups with different current intensities (1MA, 2MA), and a sham tDCS group. For the analysis, these reports were considered as two independent studies. In addition, the report by Smits et al. [41] included two types of diseases (PTSD and ADs), Due to the lack of definitive diagnosis of ADs, we only extracted data on PTSD symptoms for analysis. The characteristics of the participants are described in Table 1.

Flow chart of literature search.
Study quality assessment
The detailed results of the quality assessment are documented in Table 2. Among these studies, 70.6% (12/17) of the studies were deemed to have a low risk of bias and high quality, while 23.5% (4/17) of the studies were considered to have a moderate quality. Only one study has a high risk of bias. To improve the quality of meta-analysis, the study with high-risk bias was excluded in the main text. The supplementary materials will provide the results of all studies (the result has not changed).
The main sources of bias in the studies were identified as “selection of the reported result” and “intended interventions.” In terms of selective reporting, certain studies [42,43,44] did not mention the registered protocol, making it impossible to determine if selective reporting occurred. Regarding intervention bias, studies categorized as having “some concerns” did not explicitly state whether the experimenter who applied the tDCS was aware of the purposes of the study. Moreover, the randomization design, as a secondary factor, had an impact on bias. Despite the random allocation of participants, studies conducted by Gowda [45] and Smits [41] et al. had a significant statistical difference in the sex radio between sham and tDCS group, which could potentially impact the study results.
tDCS stimulation parameters
The stimulation parameters are detailed in Table 3. Firstly, regarding the placement of the target area, the anode was positioned on the L- DLPFC in 11 studies, while the cathode areas varied. Secondly, in terms of current intensity, it ranged from 1MA to 2MA, with 13 studies applying a current of 2MA. Moving on to stimulation sessions, 2 studies administered 5 sessions, while 10 studies included 10 sessions. Finally, with regards to session duration, 12 studies had a duration of 20 min, while the remaining studies had a duration of 30 min.
Analysis of the primary outcome
disorder-specific symptoms
A total of 15 studies fulfilled the eligibility criteria for the primary outcome with disorder-specific symptoms, including 643 participants (See supplementary materials STable 2–4). The results of meta-ananlysis showed that tDCS reduced the specific symptoms in OCD, PTSD, and ADs, with a high effect size (SMD = −0.73, 95% CI: −1.09 to −0.37; Z = −3.960, p < 0.001) and a high heterogeneity (I2 = 77.8%, p < 0.001) (Fig. 2A).

A Immediate effect size of tDCS on disorder-specific symptoms. B Immediate effect size of tDCS on general anxiety symptoms. C Long-term effect size of tDCS on disorder-specific symptoms. D Long-term effect size of tDCS on general anxiety symptoms. CI confidence interval.
Subgroup analysis indicated that tDCS effectively improved the specific symptoms in SAD, GAD, and OCD (SMDSAD = −2.27, 95% CI: −2.97 to −1.57, I2 = 0%, p > 0.05; SMDGAD = −0.61, 95% CI: −1.03 to −0.19, I2 = 0%, p > 0.05; SMDOCD = −0.55, 95% CI: −1.00 to −0.09, I2 = 77.1%, p < 0.001). Conversely, tDCS couldn’t alleviate specific symptoms of PD and PTSD (SMDPD = 0.27, 95% CI: −0.45 to 0.99, I2 = 0%, p < 0.001; SMDPTSD = −0.90, 95% CI: −1.82 to 0.03, I2 = 73.0%, p > 0.05).
Sensitivity test results showed that no outliers from any study influenced the overall results. Nevertheless, in terms of publication bias, the funnel plot indicated symmetry (Fig. 3A) and Egger’s regression test suggested no significant statistical difference (t = −1.03, p = 0.323).

A Immediate efficacy for disorder-specific symptoms. B Immediate efficacy for general anxiety symptoms. C Long-term efficacy for disorder-specific symptoms.
General anxiety symptoms
There were 10 studies involving 422 subjects that reported the general anxiety symptoms. The results of meta-analysis suggested that tDCS reduced the severity of general anxiety symptoms in OCD, PTSD and ADs, with a high effect size (SMD = −0.75; 95% CI: −1.23 to −0.26; Z = −2.999, p < 0.01). Q-statistics and I2 indicated that the included studies had a high heterogeneity (I2 = 80.7%, p < 0.001) (Fig. 2B).
The results of subgroup analysis indicated that tDCS alleviated general anxiety symptoms in SAD, PTSD and OCD (SMDSAD = −2.29, 95% CI: −3.59 to −0.98, I2 = 69.5%, p > 0.05; SMD PTSD = −0.80, 95% CI: −1.51 to −0.10, I2 = 0%, p < 0.001; SMDOCD = −0.50, 95% CI: −0.98 to −0.01; I2 = 73.4%, p < 0.01). However, tDCS had no significant impact on general anxiety symptoms in PD (SMD = 0.24, 95% CI: −0.48 to 0.96, I2 = 0%, p < 0.001).
The results of the sensitivity analysis indicated that omitting any study, the results of the remaining studies were consistent with the original results. The funnel plot may indicate the presence of publication bias (Fig. 3B), although Egger’s regression test did not show statistical significance (t = −0.67, p = 0.522).
Analysis of the secondary outcome
Follow-up of disorder-specific symptoms
A total of 13 studies reported the follow-up results. Among these, only one study recorded data for one-week follow-up [46], while the follow-up periods in other studies were longer or close to one month, our study focuses on the long-term effects of tDCS, so the study with a one-week follow-up was excluded. The meta-analysis of the remaining 12 studies, which involving 460 subjects, showed that tDCS had a long-term effect on disorder-specific symptoms in OCD, PTSD, and ADs, with a moderate effect size (SMD = −0.60; 95% CI: −1.04 to −0.16; Z = −2.650, p < 0.01) and a high heterogeneity (I2 = 79.7%, p < 0.001) (Fig. 2C).
Subgroup analysis showed that tDCS provide a long-term effect in alleviating the specific symptoms in SAD and OCD (SMDSAD = −2.20, 95% CI: −2.95 to −1.46, I2 = 0.0%, p > 0.05; SMDOCD = −0.39, 95% CI: −0.68 to −0.09, I2 = 22.3%, p > 0.05). However, tDCS did not provide a long-term effect in alleviating the specific symptoms in PTSD (SMD = −0.45, 95% CI: −1.49 to 0.60, I2 = 87.9%, p < 0.001).
The results of the sensitivity analysis indicated that omitting any study, the results of the remaining studies were consistent with the original results. Meanwhile, the funnel plot (Fig. 3C) and Egger’s regression test (t = −3.19, p < 0.05) indicated significant publication bias.
Follow-up of general anxiety symptoms
Follow-up results of general anxiety symptoms were recorded in 7 studies. The meta-analysis of the results suggested that tDCS does not provide a long-term effect in reducing the severity of general anxiety symptoms in OCD, PTSD, and ADs (SMD = −0.30; 95% CI: −0.68 to 0.09; Z = −1.523, p > 0.05), with a high heterogeneity (I2 = 53.3%, p < 0.05).
The results of sensitivity analysis showed the study of Aksu et al. [47] had a strong heterogeneity. After excluding this study, the results suggested that tDCS has a long-term effectiveness in reducing the severity of general anxiety symptoms in OCD, PTSD, and ADs (SMD = −0.41; 95% CI: −0.78 to −0.03; Z = −2.140, p < 0.05), with a moderate heterogeneity (I2 = 43.4%, p = 0.116) (Fig. 2D). Subgroup analysis showed that tDCS provided a long-term effect in alleviating the general anxiety symptoms in PTSD (SMD = −0.98, 95% CI: −1.70 to −0.26, I2 = 0%, p < 0.001) and has no long-term effect in alleviating the general anxiety symptoms in OCD (SMD = −0.28, 95% CI: −0.63 to 0.07, I2 = 26.5%, p > 0.05). Due to the limited number of studies, only Egger’s regression test was conducted, and the results indicated no significant publication bias (t = −1.10, p > 0.05).
General depression symptoms
A total of 9 studies involving 310 subjects have reported the results of general depression scales. The meta-analysis of results revealed that tDCS effectively improved the general depression symptoms in OCD, PTSD, and ADs (SMD = −0.70, 95% CI: −1.09 to −0.31; Z = −3.487, p < 0.001), with a high heterogeneity (I2 = 62.1%, p < 0.01). Subgroup analysis showed that tDCS could improve the general depression symptoms in SAD, PTSD, OCD (SMDSAD = −1.07, 95% CI: −2.06 to −0.09; I2 = 65.2%, p > 0.05; SMDPTSD = −1.14, 95% CI: −1.88 to −0.41, I2 = 0%, p < 0.001; SMDOCD = −0.62, 95% CI: −1.13 to −0.12, I2 = 60.6%, p > 0.05), while it did not significantly reduce the severity of general depression symptoms in PD (SMD = 0.05, 95% CI: −0.66 to 0.77, I2 = 0%, p < 0.001).
Sensitivity test results showed that no outliers from any study influenced the overall results. The Egger’s regression test (t = −2.85, p < 0.05) indicated the presence of some publication bias.
Meta-regression analysis
Meta-regression analysis was conducted on outcome measures that included at least 10 studies. The results showed that tDCS stimulation parameters such as the number of sessions, current intensity, session duration, and target location of the anode did not explain the heterogeneity. Statistical characteristics for each covariate are recorded in Table 4.
Discussion
The meta-analysis aimed to investigate the impact of tDCS in reducing disorder-specific symptoms, general anxiety, and depression symptoms for patients with OCD, PTSD and ADs. This study also explored the effects of different tDCS parameters on effectiveness. The results indicated that tDCS could immediately improve the clinical symptoms of OCD, PTSD, and ADs, with a high effect size. It is worth noting that the effect of tDCS on disease-specific and general anxiety symptoms can be maintained for up to one month, with a moderate effect size. Moreover, the tDCS parameters, including the number of sesssions, current intensity, session duration and target location of the anode did not have a significant influence on efficacy.
Immediate effects of tDCS on clinical symptoms of diseases
Based on the immediate therapeutic effects of tDCS on specific symptoms, general anxiety symptoms, and general depression symptoms of PTSD, OCD and ADs, we found that the effects of tDCS on different diseases varies.
First, only one randomized sham-controlled study about PD [47], Contrary to the researchers’ hypotheses, the results indicates that tDCS does not improve clinical outcomes. The researchers believe this may be due to the high placebo response in randomized controlled trials of anxiety disorders. Additionally, the clinical severity of PD included in the study is relatively low, which can lead to a higher placebo response and influence the results [47].
Secondly, our results suggest that tDCS has the potential to improve clinical symptoms of GAD and SAD with moderate and high effect sizes, respectively, which is consistent with the latest review of treatments for anxiety disorders [48]. Our study includes 2 studies on tDCS for GAD and 2 studies on tDCS for SAD, all with the anode placed at the L-DLPFC, further supporting that the L-DLPFC is an effective target for tDCS treatment of ADs. On the one hand, the excitatory stimulation of the L-DLPFC may upregulate the positive response to positive emotional stimuli and downregulate the negative response to emotional stimuli, enhancing emotional regulation ability [49]; On the other hand, tDCS may increase the functional connectivity between the DLPFC and limbic network, including the amygdala, thereby improving attention control and reducing hypersensitivity of the amygdala to threat stimuli [25, 50]. These processes are related to the core symptoms of anxiety disorders (fear, avoidance). In fact, neuroimaging studies have shown a negative correlation between DLPFC activity and anxiety [51].
Thirdly, our meta-analysis included three studies on tDCS treatment for PTSD, and the results suggested that tDCS did not improve specific symptoms of PTSD [41, 52, 53]. We cannot conclude the efficacy of tDCS on general anxiety and depressive symptoms in PTSD due to limited studies. The three studies showed variations in the severity of the PTSD, tDCS treatment protocols, and treatment outcomes. Therefore, we believe that the efficacy of tDCS may differ across various severities of PTSD. In addition, the target area, number of sessions, and interval between tDCS treatments may also influence effectiveness. Future research should continue to expand on existing studies to clarify the efficacy of tDCS for PTSD.
Long-term effects of tDCS on clinical symptoms of diseases
It is worth noting that as a novel result of this meta-analysis, we discovered that tDCS can improve specific symptoms and general anxiety symptoms of PTSD, OCD, and ADs for up to one month.
We believe that periodic tDCS may induce the late LTP-like plasticity. Long term potentiation (LTP), involves to the enduring functional enhancement of synaptic connections, or structural modification of neuronal connections [54]. It is divided into Early LTP (E-LTP) and Late LTP (L-LTP) depending on whether excitability alterations last for more than 3 h [55]. when the periodic tDCS protocols induce neuroplastic changes lasting for several days or weeks, this is referred to as L-LTP. L-LTP may be a candidate mechanism for long-term memory formation [56]. E-LTP relies on the activation of calcium-dependent kinases [57]. L-LTP requires gene expression and protein synthesis to achieve changes in synaptic strength, and also involves modifications to the activity of AMPA and NMDA receptors [58, 59].
Late LTP-Like plasticity might be the mechanism through which tDCS produces long-term effects. Additionally, studies have shown that the interval between tDCS sessions plays a crucial role in L-LTP [59], and future studies should consider controlling this variable to investigate the optimal treatment regimen with tDCS.
Limitation
When interpreting the research findings, it is important to consider the limitations of this study comprehensively. Firstly, due to differences in demographic data, assessment tools, and tDCS treatment parameters, most of the results showed quite heterogeneity. While we attempted to use a random effect model and performed meta-regression, it is crucial to acknowledge this as a significant limitation of our findings. However, it should also be noted that I2 may be overestimated in a small meta-analyses [60]. Secondly, the well-known high placebo response in tDCS must be taken into account [61], highlighting the importance of a blind procedure in study design. Unfortunately, due to the limitation of the number of studies, we were unable to strictly control this variable in our study. Thirdly, the number of randomized controlled studies on tDCS for OCD, PTSD, and ADs is limited, so we are unable to control for comorbidities or other interventions. In the future, further research should be conducted to investigate the immediate and long-term efficacy of tDCS in these disorders, in order to provide additional evidence to clarify of the efficacy of tDCS and elucidate the underlying pathological mechanisms of these diseases.
Conclusion
tDCS improves the clinical symptoms of OCD, PTSD and ADs immediately, and the efficacy can last for 1 month. tDCS can serve as a non-invasive brain stimulation technology for treating these disorders, and the therapeutic effects can be maintained for a period of time.
References
Baldwin DS, Anderson IM, Nutt DJ, Allgulander C, Bandelow B, den Boer JA, et al. Evidence-based pharmacological treatment of anxiety disorders, post-traumatic stress disorder and obsessive-compulsive disorder: a revision of the 2005 guidelines from the British Association for Psychopharmacology[J]. J Psychopharmacol. 2014;28:403–39.
Van’t Wout M, Longo SM, Reddy MK, Philip NS, Bowker MT, Greenberg BD. Transcranial direct current stimulation may modulate extinction memory in posttraumatic stress disorder[J]. Brain Behav. 2017;7:e00681.
Bandelow B. Current and novel psychopharmacological drugs for anxiety disorders[J]. Adv Exp Med Biol. 2020;1191:347–65.
Apolinário-Hagen J, Drüge M, Fritsche L. Cognitive behavioral therapy, mindfulness-based cognitive therapy and acceptance commitment therapy for anxiety disorders: integrating traditional with digital treatment approaches[J]. Adv Exp Med Biol. 2020;1191:291–329.
Thomsen PH. Obsessive-compulsive disorder: pharmacological treatment[J]. Eur Child Adolescent Psychiatry. 2000;9:S76–S84.
Montavon F, Vandenberghe F, Eap CB. Use of pharmacological treatment for posttraumatic stress disorder: analysis of a psychiatric population in Switzerland and comparison with international guidelines[J]. Encephale. 2022;49:446–52.
Atmaca Murad. Treatment-refractory obsessive compulsive disorder[J]. Progress in Neuro-Psychopharmacology and Biological Psychiatry. 2016;70:127–33.
Bystritsky A. Treatment-resistant anxiety disorders[J]. Molecular Psychiatry. 2006;11:805–14.
Freire RC, Cabrera-Abreu C, Milev R. Neurostimulation in anxiety disorders, post-traumatic stress disorder, and obsessive-compulsive disorder[J]. Adv Exp Med Biol. 2020;1191:331–46.
Zhao H, Qiao L, Fan D, Zhang S, Turel O, Li Y, et al. Modulation of brain activity with noninvasive transcranial direct current stimulation (tDCS): clinical applications and safety concerns[J]. Front Psychol. 2017;8:685.
Nitsche MA, Paulus W. Excitability changes induced in the human motor cortex by weak transcranial direct current stimulation[J]. J Physiol. 2000;527:633–9.
Dedoncker J, Brunoni AR, Baeken C, Vanderhasselt MA. A systematic review and meta-analysis of the effects of transcranial direct current stimulation (tDCS) over the dorsolateral prefrontal cortex in healthy and neuropsychiatric samples: influence of stimulation parameters[J]. Brain Stimul. 2016;9:501–17.
Salehinejad MA, Ghanavati E. Complexity of cathodal tDCS: relevance of stimulation repetition, interval, and intensity[J]. J Physiol. 2020;598:1127–9.
Stagg CJ, Nitsche MA. Physiological basis of transcranial direct current stimulation[J]. Neuroscientist. 2011;17:37–53.
Milad MR, Rauch SL. Obsessive-compulsive disorder: beyond segregated cortico-striatal pathways[J]. Trends Cogn Sci. 2012;16:43–51.
Van den Heuvel OA, Guido VW, Carles SM, Pino A, Samuel RC, Takashi N, et al. Brain circuitry of compulsivity[J]. Eur Neuropsychopharm. 2016;26:810–27.
Brunelin J, Mondino M, Bation R, Palm U, Saoud M, Poulet E. Transcranial direct current stimulation for obsessive-compulsive disorder: a systematic review[J]. Brain Sci. 2018;8:37.
Trevizol AP, Shiozawa P, Cook IA, Sato IA, Kaku CB, Guimarães FB, et al. Transcranial magnetic stimulation for obsessive-compulsive disorder: an updated systematic review and meta-analysis[J]. J ECT. 2016;32:262–6.
Philip NS, Barredo J, van ‘t Wout-Frank M, Tyrka AR, Price LH, Carpenter LL. Network mechanisms of clinical response to transcranial magnetic stimulation in posttraumatic stress disorder and major depressive disorder[J]. Biol Psychiatry. 2018;83:263–72.
Quirk GJ, Garcia R, González-Lima F. Prefrontal mechanisms in extinction of conditioned fear[J]. Biol Psychiatry. 2006;60:337–43.
Aupperle RL, Allard CB, Grimes EM, Simmons AN, Flagan T, Behrooznia M, et al. Dorsolateral prefrontal cortex activation during emotional anticipation and neuropsychological performance in posttraumatic stress disorder[J]. Arch Gen Psychiatry. 2012;69:360–71.
Lai CH. Task MRI-based functional brain network of anxiety[J]. Adv Exp Med Biol. 2020;1191:3–20.
Taylor JM, Whalen PJ. Neuroimaging and anxiety: the neural substrates of pathological and non-pathological anxiety[J]. Curr Psychiatry Rep. 2015;17:49.
Dresler T, Guhn A, Tupak SV, Ehlis AC, Herrmann MJ, Fallgatter AJ, et al. Revise the revised? New dimensions of the neuroanatomical hypothesis of panic disorder[J]. J Neural Transm. 2013;120:3–29.
Ironside M, Browning M, Ansari TL, Harvey CJ, Sekyi-Djan MN, Bishop SJ, et al. Effect of prefrontal cortex stimulation on regulation of amygdala response to threat in individuals with trait anxiety: a randomized clinical trial[J]. JAMA Psychiatry. 2019;76:71–78.
Cha J, DeDora D, Nedic S, Ide J, Greenberg T, Hajcak G, et al. Clinically anxious individuals show disrupted feedback between inferior frontal gyrus and prefrontal-limbic control circuit[J]. J Neurosci. 2016;36:4708–18.
Grimm S, Beck J, Schuepbach D, Hell D, Boesiger P, Bermpohl F, et al. Imbalance between left and right dorsolateral prefrontal cortex in major depression is linked to negative emotional judgment: an fMRI study in severe major depressive disorder[J]. Biol Psychiatry. 2008;63:369–76.
Zhou S, Fang Y. Efficacy of non-invasive brain stimulation for refractory obsessive-compulsive disorder: a meta-analysis of randomized controlled trials[J]. Brain Sci. 2022;12:943.
Kan RLD, Zhang BBB, Zhang JJQ, Kranz GS. Non-invasive brain stimulation for posttraumatic stress disorder: a systematic review and meta-analysis[J]. Transl Psychiatry. 2020;10:168.
Vergallito A, Gallucci A, Pisoni A, Punzi M, Caselli G, Ruggiero GM, et al. Effectiveness of noninvasive brain stimulation in the treatment of anxiety disorders: a meta-analysis of sham or behaviour-controlled studies[J]. J Psychiatry Neurosci. 2021;46:E592–E614.
Choi KW, Kim YK, Jeon HJ. Comorbid anxiety and depression: clinical and conceptual consideration and transdiagnostic treatment[J]. Adv Exp Med Biol. 2020;1191:219–35.
Zhang R, Lam CLM, Peng X, Zhang D, Zhang C, Huang R, et al. Efficacy and acceptability of transcranial direct current stimulation for treating depression: a meta-analysis of randomized controlled trials[J]. Neurosci Biobehav Rev. 2021;126:481–90.
Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews[J]. BMJ. 2021;372:n71.
Volpato C, Piccione F, Cavinato M, Duzzi D, Schiff S, Foscolo L, et al. Modulation of affective symptoms and resting state activity by brain stimulation in a treatment-resistant case of obsessive-compulsive disorder[J]. Neurocase. 2013;19:360–70.
Cochrane Handbook for Systematic Reviews of Interventions version 6.3 (updated February 2022). [Z]//TJ Higgins Jpt, Chandler J, Cumpston M, Li T, Page Mj, Welch Va Available from www.training.cochrane.org/handbook. 2022.
Hedges LV. Distribution theory for glass’s estimator of effect size and related estimators[J]. J Educ Stat. 1981;6:107–28.
Bender R, Friede T, Koch A, Kuss O, Schlattmann P, Schwarzer G, et al. Methods for evidence synthesis in the case of very few studies[J]. Res Synth Methods. 2018;9:382–92.
Nikolakopoulou A, Mavridis D, Salanti G. Demystifying fixed and random effects meta-analysis[J]. Evid Based Ment Health. 2014;17:53–57.
Jafari E, Alizadehgoradel J, Pourmohseni Koluri F, Nikoozadehkordmirza E, Refahi M, Taherifard M, et al. Intensified electrical stimulation targeting lateral and medial prefrontal cortices for the treatment of social anxiety disorder: a randomized, double-blind, parallel-group, dose-comparison study[J]. Brain Stimul. 2021;14:974–86.
Alizadehgoradel J, Molaei B, Barzegar Jalali K, Pouresmali A, Sharifi K, Hallajian AH, et al. Targeting the prefrontal-supplementary motor network in obsessive-compulsive disorder with intensified electrical stimulation in two dosages: a randomized, controlled trial[J]. Transl Psychiatry. 2024;14:78.
Smits FM, Geuze E, Schutter D, Honk JV, Gladwin TE. Effects of tDCS during inhibitory control training on performance and PTSD, aggression and anxiety symptoms: a randomized-controlled trial in a military sample[J]. Psychol Med. 2021;52:1–11.
Liu J, Xiang F, Huang Q, Zhu C. The efficacy of transcranial direct current stimulation in the treatment of generalized anxiety disorder (in chinese)[J]. Zhejiang Clinical. Medical J. 2022;24:690–2.
Zhou P, Cai M, Yuan P, Yang S, Xi M. Effects of fluvoxamine combined with transcranial direct current stimulation on cognitive function, anxiety symptoms, serum BDNF and 5-HT levels in patients with first-episode obessive-complusive disorder (in chinese)[J]. Shaanxi Med J. 2022;51:990–4.
Movahed FS, Goradel JA, Pouresmali A, Mowlaie M. Effectiveness of transcranial direct current stimulation on worry, anxiety, and depression in generalized anxiety disorder: a randomized, single-blind pharmacotherapy and sham-controlled clinical trial[J]. IJ Psychiatry Behav Sci. 2018;12:e11071.
Gowda SM, Narayanaswamy JC, Hazari N, Bose A, Chhabra H, Balachander S, et al. Efficacy of pre-supplementary motor area transcranial direct current stimulation for treatment resistant obsessive compulsive disorder: a randomized, double blinded, sham controlled trial[J]. Brain Stimul. 2019;12:922–9.
de Lima AL, Braga FMA, da Costa RMM, Gomes EP, Brunoni AR, Pegado R. Transcranial direct current stimulation for the treatment of generalized anxiety disorder: a randomized clinical trial[J]. J Affect Disord. 2019;259:31–37.
Aksu S, Soyata AZ, Mursalova Z, Eskicioğlu G, Tükel R. Transcranial direct current stimulation does not improve clinical and neurophysiological outcomes in panic disorder: a randomized sham-controlled trial[J]. Psychiatry Clin Neurosci. 2022;76:384–92.
Lee HJ, Stein MB. Update on treatments for anxiety-related disorders[J]. Curr Opin Psychiatry. 2023;36:140–5.
Vicario CM, Salehinejad MA, Felmingham K, Martino G, Nitsche MA. A systematic review on the therapeutic effectiveness of non-invasive brain stimulation for the treatment of anxiety disorders[J]. Neurosci Biobehav Rev. 2019;96:219–31.
Todder D, Gershi A, Perry Z, Kaplan Z, Levine J, Avirame K. Immediate effects of transcranial direct current stimulation on obsession-induced anxiety in refractory obsessive-compulsive disorder: a pilot study[J]. J ECT. 2018;34:e51–7.
Bishop S, Duncan J, Brett M, Lawrence AD. Prefrontal cortical function and anxiety: controlling attention to threat-related stimuli[J]. Nat Neurosci. 2004;7:184–8.
Ahmadizadeh MJ, Rezaei M, Fitzgerald PB. Transcranial direct current stimulation (tDCS) for post-traumatic stress disorder (PTSD): a randomized, double-blinded, controlled trial[J]. Brain Res Bull. 2019;153:273–8.
Eyraud N, Poupin P, Legrand M, Caille A, Sauvaget A, Bulteau S, et al. Combining trauma script exposure with tDCS to alleviate symptoms of posttraumatic stress disorder: a two-arm randomized sham-controlled multicenter trial[J]. Brain Stimul. 2024;17:591–3.
Feldman DE. Synaptic mechanisms for plasticity in neocortex[J]. Annu Rev Neurosci. 2009;32:33–55.
Reymann KG, Frey JU. The late maintenance of hippocampal LTP: requirements, phases, ‘synaptic tagging’, ‘late-associativity’ and implications[J]. Neuropharmacology. 2007;52:24–40.
Costa-Mattioli M, Sossin WS, Klann E, Sonenberg N. Translational control of long-lasting synaptic plasticity and memory[J]. Neuron. 2009;61:10–26.
Malenka RC, Bear MF. LTP and LTD: an embarrassment of riches[J]. Neuron. 2004;44:5–21.
Dozmorov M, Li R, Abbas AK, Hellberg F, Farre C, Huang FS, et al. Contribution of AMPA and NMDA receptors to early and late phases of LTP in hippocampal slices[J]. Neurosci Res. 2006;55:182–8.
Monte-Silva K, Kuo MF, Hessenthaler S, Fresnoza S, Liebetanz D, Paulus W, et al. Induction of late LTP-like plasticity in the human motor cortex by repeated non-invasive brain stimulation[J]. Brain Stimul. 2013;6:424–32.
von Hippel PT. The heterogeneity statistic I(2) can be biased in small meta-analyses[J]. BMC Med Res Methodol. 2015;15:35.
De Smet S, Nikolin S, Moffa A, Suen P, Vanderhasselt MA, Brunoni AR, et al. Determinants of sham response in tDCS depression trials: a systematic review and meta-analysis[J]. Prog Neuropsychopharmacol Biol Psychiatry. 2021;109:110261.
Silva R, Brunoni AR, Goerigk S, Batistuzzo MC, Costa DLDC, Diniz JB, et al. Efficacy and safety of transcranial direct current stimulation as an add-on treatment for obsessive-compulsive disorder: a randomized, sham-controlled trial[J]. Neuropsychopharmacology. 2021;46:1028–34.
Bation R, Mondino M, Le Camus F, Saoud M, Brunelin J. Transcranial direct current stimulation in patients with obsessive compulsive disorder: a randomized controlled trial[J]. Eur Psychiatry. 2019;62:38–44.
Yoosefee S, Amanat M, Salehi M, Mousavi SV, Behzadmanesh J, Safary V, et al. The safety and efficacy of transcranial direct current stimulation as add-on therapy to fluoxetine in obsessive-compulsive disorder: a randomized, double-blind, sham-controlled, clinical trial[J]. BMC Psychiatry. 2020;20:570.
Harika-Germaneau G, Heit D, Drapier D, Sauvaget A, Bation R, Chatard A, et al. Treating refractory obsessive compulsive disorder with cathodal transcranial direct current stimulation over the supplementary motor area: a large multisite randomized sham-controlled double-blind study[J]. Front Psychiatry. 2024;15:1338594.
Funding
This work was supported by the National Natural Science Foundation of China (82271546, 82101625); National Key Research and Development Program of China (2023YFC2506201); Fund Program for the Scientific Activities of Selected Returned Overseas Professionals in Shanxi Province (20240041); Special fund for Science and Technology Innovation Teams of Shanxi Province (202304051001049).
Author information
Authors and Affiliations
Contributions
LXX: conceptualization, methodology, software, writing—original draft. PNH: methodology, software, writing—original draft. ZLG: methodology, supervision. MC: methodology, software, validation. XW: methodology, software. XZD: software, supervision, validation. YL: methodology, visualization. BC: visualization, review & editing. JHZ: visualization, review & editing. WTZ: conceptualization, writing—review & editing. SL: conceptualization, writing—review & editing.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Xie, L., Hu, P., Guo, Z. et al. Immediate and long-term efficacy of transcranial direct current stimulation (tCDS) in obsessive-compulsive disorder, posttraumatic stress disorder and anxiety disorders: a systematic review and meta-analysis. Transl Psychiatry 14, 343 (2024). https://doi.org/10.1038/s41398-024-03053-0
Received:
Revised:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41398-024-03053-0
This article is cited by
-
Efficacy of CBT, intensified tDCS and their combination for reducing clinical symptoms and improving quality of life in social anxiety disorder with comorbid depression: a randomized controlled trial
BMC Psychiatry (2025)
-
Artificial Intelligence in Obsessive-Compulsive Disorder: A Systematic Review
Current Treatment Options in Psychiatry (2025)
