
Abstract
Postoperative depression adversely influences breast cancer patients’ clinical outcomes. Our prior study demonstrated that intraoperative esketamine ameliorated postoperative depression in breast cancer patients, yet the underlying neural mechanism remains incompletely understood. We performed a double-blind randomized controlled trial in 35 breast cancer patients with preoperative depressive symptoms, who were randomly given intraoperative esketamine 0.25 mg·kg⁻¹ (n = 18) or saline placebo (n = 17) over the initial 40 min of anesthesia. Resting-state functional magnetic resonance imaging data were collected at preoperative baseline and postoperative day 1 follow-up to calculate brain functional network measures. In contrast to no significant change in the placebo group, the esketamine group showed increased degree centrality of the left inferior frontal gyrus, opercular part from baseline to follow-up, which was related to improvement in depressive symptoms. Additionally, we found significant associations of baseline network measures at the global, nodal, and edge levels with short-term and long-term improvements in depressive symptoms following esketamine administration. These findings may not only provide novel insights into the neural mechanism by which esketamine exerts its antidepressant efficacy during the perioperative period, but also highlight the prospect of functional network measures as useful predictors of antidepressant response to esketamine in patients with breast cancer.
Similar content being viewed by others

Introduction
Depressive symptoms have emerged as the primary mental health concern in patients with breast cancer [1]. Surgery, an effective therapeutic intervention for breast cancer, could potentially exacerbate depressive symptoms as a potent stressor [2]. It is now evident that postoperative depression adversely influences individuals’ clinical outcomes, such as increasing the risk of breast cancer recurrence, all-cause mortality and breast cancer-specific death [3]. Accordingly, there is an urgent clinical need to ameliorate postoperative depressive symptoms among patients with breast cancer.
Traditional oral antidepressants are limited in treating perioperative depression due to a delayed onset of action requiring weeks to achieve significant therapeutic effects, as well as their influences on anaesthesia and surgical outcomes [4]. Ketamine, a glutamate N-methyl-D-aspartic acid receptor (NMDAR) antagonist, has been proven to exert rapid (within hours) and sustained (lasting for up to 7 days) antidepressant effects after a single, low-dose administration in patients with treatment-resistant depression [5,6,7]. However, despite some promising clinical findings [8, 9], there remains ongoing debate about the efficacy and safety of perioperative intravenous ketamine [10]. Esketamine is the S-enantiomer of ketamine and similarly functions as an NMDAR antagonist [11, 12]. In addition to maintaining a rapid antidepressant response, esketamine shows higher potency, enhanced receptor affinity, and a reduced prevalence of adverse reactions in the nervous system relative to ketamine [13], rendering it a preferable option for preventing and treating depressive symptoms during the perioperative period. Recently, we designed a randomized controlled trial (RCT), termed EASE, to examine the influence of low-dose esketamine on postoperative depressive symptoms in patients with breast cancer [14], and found that esketamine significantly reduced short-term postoperative depression scores without provoking complications [15].
Investigation into brain correlates and predictors of antidepressant response to ketamine/esketamine has been an important topic in psychiatry and neuroscience, offering empirical insights into the neural therapeutic mechanisms of ketamine/esketamine. Animal experimental studies have demonstrated that ketamine exerts its antidepressant effect through blocking NMDAR-dependent bursting activity in the lateral habenula to disinhibit downstream monoaminergic reward centers [16,17,18]. Parallel human neuroimaging research has also attempted to identify brain biomarkers of the antidepressant effect of ketamine/esketamine in depressed or healthy individuals, but results from prior studies are neuroanatomically highly heterogeneous [19,20,21,22,23,24,25]. Despite these findings, there is still a paucity of literature examining the brain effects of intraoperative esketamine administration as well as their associations with postoperative depression in patients with breast cancer.
The human brain operates essentially as an interconnected complex network in support of cognition, emotion, and behavior [26]. Graph theory has long been recognized as a useful tool for studying the complexity of the brain network, with nodes representing anatomically defined brain areas and edges representing functional or structural connections between pairs of nodes [27,28,29]. The application of graph theoretical approaches has allowed for a detailed characterization of the brain network topological organization at the global, nodal, and edge levels. In this framework, the human brain has been evidenced to possess important topological properties, such as a small-world topology with high clustering and short path length that ensures within-network maximal communication rate with minimal wiring cost, and highly connected hubs [30,31,32,33,34,35,36]. Taking advantage of graph theoretical approaches, researchers have explored brain network topological alterations associated with diseases and treatments [37,38,39,40,41,42,43,44,45,46,47,48,49,50,51,52,53,54,55,56], advancing our understanding of the underlying neural mechanisms. Notably, although functional, diffusion, and structural magnetic resonance imaging (MRI) can be respectively used to construct functional connectivity, white matter anatomical connectivity, and structural covariance networks [37, 39, 43, 57,58,59], functional MRI (fMRI) may be advantageous in better capturing the rapid functional network reconfiguration or plasticity elicited by intraoperative esketamine over a short follow-up period.
In the present study, we conducted a double-blind RCT to examine the effects of intraoperative esketamine administration on brain functional networks in breast cancer patients with preoperative depressive symptoms, by combining resting-state fMRI data with graph theoretical analysis. Then, we investigated whether the esketamine-induced brain functional network alterations were related to improvement in postoperative depressive symptoms. Finally, we examined the associations of baseline functional network measures with depressive symptom improvement following esketamine administration to determine their outcome predictive value. We hypothesized that 1) intraoperative esketamine would induce alterations in brain functional networks that correlate with improvement in postoperative depressive symptoms, and 2) baseline functional network measures could predict depressive symptom improvement.
Methods
This was a secondary analysis study of the EASE trial [14], which focused on neuroimaging data analysis with the aim of elucidating the potential neural underpinnings of the effect of intraoperative esketamine on postoperative depression in patients with breast cancer observed in our primary analysis study [15]. The EASE trial was approved by the Clinical Medical Research Ethics Committee of The First Affiliated Hospital of Anhui Medical University (PJ2023-05-25) and registered in the Chinese Clinical Trial Registry (ChiCTR2300071062) at http://www.chictr.org.cn/ before study. This RCT followed Consolidated Standards of Reporting Trials (CONSORT) guidelines [60].
Participants
We screened potential participants using the Patient Health Questionnaire-9 (PHQ-9) [61] and the Montgomery-Åsberg Depression Rating Scale (MADRS) [62]. The PHQ-9 is a 9-item self-reported assessment tool designed to examine the presence and frequency of depressive symptoms [61]. The MADRS is a 10-item clinician-rated scale used to evaluate the severity of depressive symptoms, showing sensitivity to symptom changes following ketamine treatment [62, 63]. Our participants were female patients aged 18–65 years with an American Society of Anesthesiologists (ASA) physical status I-III, who were scheduled for elective breast cancer resection and exhibited mild-to-severe depressive symptoms (PHQ-9 ≥ 5 and MADRS ≥ 12) [61, 64]. The detailed inclusion and exclusion criteria are described in our prior publications [14, 15]. All participants provided written informed consent before participation.
Study design
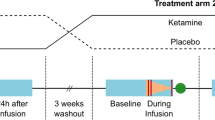
The RCT enrolled 108 eligible patients in total, of whom 83 consented to participate in the RCT with MRI scans. The patients were randomly allocated into either esketamine (n = 42) or saline placebo (n = 41) groups. Randomization was computer-generated with a block size of 4 and allocations were sealed in sequentially numbered opaque envelopes. An independent researcher who was not involved in the RCT opened the envelopes shortly before surgery and prepared the designated trial drug, which was 0.25 mg·kg⁻¹ esketamine diluted in 20 mL of normal saline for the esketamine group or 20 mL of normal saline for the placebo group. Both patients and researchers were fully blinded to treatment allocation. All patients received a standardized general anesthetic protocol as previously described in the EASE trial protocol [14]. Briefly, anesthesia was induced with propofol (2 mg·kg⁻¹), sufentanil (0.05 μg·kg⁻¹), and cisatracurium (0.1–0.15 mg·kg⁻¹) and maintained with propofol-based total intravenous anesthesia (continuous infusion of propofol 3–7 mg·kg⁻¹·h⁻¹ and remifentanil 0.1 μg·kg⁻¹·min⁻¹). The trial drugs were given intravenously over the initial 40 min of anesthesia. For both groups of patients, the severity of depressive symptoms was evaluated at 8 study visits: baseline (the day before surgery) and follow-up (postoperative days 1–5 and weeks 4 and 12), and MRI examination was performed twice at baseline and follow-up (postoperative day 1). In addition, 35 female healthy controls (HC) without any neurological illnesses, psychiatric disorders, or severe physical diseases underwent MRI examination at baseline.
MRI data acquisition
MRI data were collected on a 3.0-Tesla MR system (Discovery MR750w, General Electric) with a 24-channel head coil. All participants were instructed to relax, keep their eyes closed but not fall asleep, think of nothing in particular, and move as little as possible. Structural images were obtained using a high-resolution 3-dimensional T1-weighted brain volume (BRAVO) sequence with the following parameters: repetition time (TR) = 8.5 ms; echo time (TE) = 3.2 ms; inversion time (TI) = 450 ms; flip angle = 12 °; field of view (FOV) = 256 mm × 256 mm; matrix size = 256 × 256; slice thickness = 1 mm, no gap; 188 sagittal slices; and acquisition time = 296 s. Resting-state blood-oxygen level-dependent (BOLD) fMRI data were acquired using a gradient-echo single-shot echo planar imaging (GRE-SS-EPI) sequence with the following parameters: TR = 2000 ms; TE = 30 ms; FA = 90 °; FOV = 220 mm × 220 mm; matrix size = 64 × 64; slice thickness = 3 mm, slice gap = 1 mm; 35 interleaved axial slices; 185 volumes; and acquisition time = 370 s. Routine T2-weighted images were obtained to exclude any organic brain abnormality. All images were visually inspected to ensure that only images without visible artifacts were included in subsequent analyses.
fMRI data preprocessing
Resting-state fMRI data were preprocessed using Statistical Parametric Mapping (SPM12, http://www.fil.ion.ucl.ac.uk/spm) and Data Processing & Analysis for Brain Imaging (DPABI, http://rfmri.org/dpabi) [65] according to a validated pipeline [66,67,68,69]. The first 10 volumes for each participant were removed to allow the signal to reach equilibrium and the participants to adapt to the scanning noise. The remaining volumes were corrected for the acquisition time delay between slices. Then, realignment was performed to correct the motion between time points. Head motion parameters were computed by estimating the translation in each direction and the angular rotation on each axis for each volume. All BOLD data were within the defined motion thresholds (i.e., maximum translational or rotational motion parameters less than 2.0 mm or 2.0 °). We also calculated frame-wise displacement (FD), which indexes the volume-to-volume changes in head position. Several nuisance covariates (the linear drift, the estimated motion parameters based on the Friston-24 model, the spike volumes with FD > 0.5 mm, the white matter signal, and the cerebrospinal fluid signal) were regressed out from the data. Notably, we did not perform global signal regression since it is still a controversial topic in resting-state fMRI analysis [70]. The datasets were then band-pass filtered on a frequency range of 0.01 - 0.1 Hz. For spatial normalization, individual structural images were firstly co-registered with the mean functional images; then the transformed structural images were segmented and normalized to the Montreal Neurological Institute (MNI) space using the diffeomorphic anatomical registration through exponentiated Lie algebra (DARTEL) technique [71]. Finally, each filtered functional volume was spatially normalized to the MNI space using the deformation parameters estimated during the above step and resampled into a 3-mm cubic voxel.
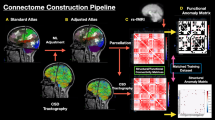
Brain functional network construction and analysis
Nodes (brain regions) and edges (functional connectivity between regions) are two basic elements of a brain functional network. To define nodes, an automated anatomical labeling (AAL) template was adopted to parcellate the cerebrum into 90 cortical and subcortical regions, which were considered a set of nodes in our network analysis. For each participant, the representative BOLD time course of each region was obtained by averaging the BOLD time courses over all voxels within that region. To define edges, we computed the Pearson’s correlation coefficients between the representative BOLD time courses of all possible pairs of nodes, yielding a 90 × 90 functional connectivity matrix per participant.
Graph theory analysis was performed on the resultant functional connectivity matrices using GRETNA software (http://www.nitrc.org/projects/gretna) [72]. To ensure a small-world topology with a sparse property, each functional connectivity matrix was thresholded using a sparsity threshold range of 0.10 to 0.34 with an interval of 0.01 [31, 73,74,75,76], and converted into a binary matrix. Based on the thresholded and binarized functional connectivity matrices, both global and nodal network properties were measured. For global property, we calculated small-world attributes including clustering coefficient (Cp), characteristic path length (Lp), normalized clustering coefficient (Gamma), normalized characteristic path length (Lambda), and small-worldness (Sigma) [31]. Cp and Gamma assess the extent of the local density or cliquishness of the network, which characterizes network segregation. Lp and Lambda assess the extent of average connectivity or overall routing efficiency of the network, which characterizes network integration. Sigma is an integrated measure defined as Gamma/Lambda. For nodal property, we calculated degree centrality, i.e., the number of edges connected to a node, to describe the importance of individual nodes within a network [77]. Brain regions with higher degree centrality are considered hubs interacting with many other regions in the network. The calculation procedure of these network measures is detailed in the previous literature [78]. Notably, we calculated the global and nodal network measures at each sparsity threshold, and then used the area under the curve across all the sparsity thresholds as a summarized scalar for each network measure.
Statistical analysis
Statistical analyses were performed using the SPSS 23.0 software package (SPSS, Chicago, IL, USA). For cross-sectional analyses of baseline data, we compared age and baseline FD across the esketamine, placebo, and control groups using a one-way analysis of variance (ANOVA). Differences in other demographic variables (height, weight, body mass index, and follow-up FD) and a range of clinical characteristics (e.g., PHQ-9, MADRS, and preoperative comorbidities, among others) between the esketamine and placebo groups were examined using a two-sample t test, a chi-square test, or a Mann-Whitney U test as appropriate. For longitudinal analyses of brain functional network measures at the global, nodal, and edge levels, we adopted a two-way repeated-measures ANOVA that included the between-subject factor group (esketamine vs. placebo) and the within-subject factor time (baseline vs. follow-up). We focused our analysis primarily on group × time interactions, followed by post-hoc paired t tests for comparing time points within each group separately. In addition, we calculated longitudinal changes (follow-up - baseline) in network measures and MADRS scores, followed by Pearson’s correlation analyses to assess their associations within each group. To determine the outcome predictive value of neuroimaging, we also examined the correlations between baseline network measures and changes in MADRS scores. For global network measures, the significance threshold was set at p < 0.05. For nodal and edge measures, correction for multiple testing was performed using a false-positive correction according to the numbers of nodes (i.e., p < [1/90] = 0.011) and edges (i.e., p < [1/4005] = 0.00024). The false-positive correction is not as conservative as a Bonferroni or a false discovery rate correction and thus does not yield strong type I error control for exploratory analysis. Given the large number of node-wise and edge-wise tests, all node-level and edge-level analyses were considered exploratory and hypothesis-generating, and thus any node-level and edge-level findings should be interpreted cautiously.
Results
Demographic and clinical characteristics
Eligibility, examinations, randomization, and follow-up of the patients are illustrated in Fig. 1. 45 participants declined follow-up MRI scans and 3 were excluded due to excessive fMRI head movement. This brought the final sample used in our study to 18 patients in the esketamine group, 17 patients in the placebo group, and 35 HC. Demographic and clinical characteristics of the participants are presented in Table 1. The three groups did not differ in age or baseline FD. In addition, there were no significant differences in other demographic variables (height, weight, body mass index, and follow-up FD) or clinical characteristics (e.g., PHQ-9, MADRS, and preoperative comorbidities, among others) between the esketamine and placebo groups.

ASA American Society of Anesthesiologists, BMI body mass index, fMRI functional magnetic resonance imaging.
Brain functional network change and its association with improvement in depressive symptoms following esketamine administration
For nodal network measures, two-way repeated-measures ANOVA demonstrated a significant group × time interaction effect on degree centrality of the left inferior frontal gyrus, opercular part (L-IFGoperc) (F = 8.097, p = 0.008) that survived the false-positive correction (Fig. 2A). Post-hoc paired t tests revealed significantly increased degree centrality of L-IFGoperc from baseline to follow-up in the esketamine group (t = −2.810, p = 0.012), but no significant change in the placebo group (t = 1.164, p = 0.261) (Fig. 2B). Compared to HC, the esketamine group at follow-up showed significantly higher degree centrality of L-IFGoperc (t = 2.808, p = 0.007), but no significant differences were observed between HC and other patient groups (p > 0.05) (Fig. 2C). Moreover, we found a significant negative correlation between degree centrality change of L-IFGoperc (postoperative day 1 - baseline) and MADRS score change (postoperative day 1 - baseline) in the esketamine group (r = −0.515, p = 0.029) but not the placebo group, indicating an association between increased degree centrality of L-IFGoperc and improvement in depressive symptoms following esketamine administration (Fig. 2D). However, there were no significant group × time interactions or correlations for global or edge network measures.

(A) Group × time interaction effect on degree centrality of L-IFGoperc (blue node). (B) Longitudinal change in degree centrality of L-IFGoperc in the esketamine and placebo groups. (C) Difference in degree centrality of L-IFGoperc between HC and patient groups. (D) Correlation between degree centrality change of L-IFGoperc and MADRS score change in the esketamine group. Change = follow-up (postoperative day 1) - baseline. HC healthy controls, L-IFGoperc left inferior frontal gyrus, opercular part, MADRS Montgomery-Åsberg Depression Rating Scale.
Associations between baseline functional network measures and improvement in depressive symptoms
To determine the outcome predictive value of baseline functional network measures, we examined their correlations with longitudinal changes in MADRS scores. Results showed significant associations of baseline network measures at the global, nodal, and edge levels with short-term and long-term changes in MADRS scores in the esketamine group (Fig. 3). With respect to global measures, Lp was negatively correlated with long-term MADRS change (postoperative week 12 - baseline, r = −0.557, p = 0.03) (Fig. 3A). In terms of nodal measures, degree centrality of L-IFGoperc was positively correlated with short-term MADRS changes (postoperative day 1 - baseline, r = 0.671, p = 0.002; postoperative day 2 - baseline, r = 0.668, p = 0.002; postoperative day 3 - baseline, r = 0.611, p = 0.007); long-term MADRS change (postoperative week 12 - baseline) was negatively correlated with degree centrality of the right middle cingulate gyrus (R-MCG) (r = −0.698, p = 0.004) and left inferior occipital gyrus (L-IOG) (r = −0.713, p = 0.003), and was positively correlated with degree centrality of the left putamen (L-PUT) (r = 0.711, p = 0.003) (Fig. 3B). As to edge measures, short-term MADRS change (postoperative day 2 - baseline) was negatively correlated with functional connectivity between the right supramarginal gyrus (R-SMG) and the left pallidum (L-PAL) (r = −0.785, p = 0.0001); long-term MADRS change (postoperative week 12 - baseline) was negatively correlated with functional connectivity between the left superior frontal gyrus, dorsolateral part (L-SFGdor) and the left superior temporal gyrus (L-STG) (r = −0.825, p = 0.0002), between the right postcentral gyrus (R-PoCG) and the right superior parietal gyrus (R-SPG) (r = −0.820, p = 0.0002), and between the left precuneus (L-PCUN) and the left inferior temporal gyrus (L-ITG) (r = −0.845, p = 0.0001) (Fig. 3C). However, no significant associations between baseline network measures and MADRS changes were observed in the placebo group.

Scatter plots show significant correlations of baseline network measures at the global (A), nodal (B), and edge (C) levels with short-term (postoperative days 1–3) and long-term (postoperative week 12) changes in MADRS scores in the esketamine group. FC functional connectivity, L-IFGoperc left inferior frontal gyrus, opercular part, L-IOG left inferior occipital gyrus, L-ITG left inferior temporal gyrus, Lp characteristic path length, L-PAL left pallidum, L-PCUN left precuneus, L-PUT left putamen, L-SFGdor left superior frontal gyrus, dorsolateral part, L-STG left superior temporal gyrus, MADRS, Montgomery-Åsberg Depression Rating Scale, R-MCG right middle cingulate gyrus, R-PoCG right postcentral gyrus, R-SMG right supramarginal gyrus, R-SPG right superior parietal gyrus.
Discussion
By applying graph theoretical analysis to resting-state fMRI data, this is the first neuroimaging RCT to investigate the effects of intraoperative esketamine on brain functional networks as well as their correlations with and predictions of improvement in postoperative depressive symptoms in patients with breast cancer. The key finding was that breast cancer patients, following esketamine administration, showed increased degree centrality of L-IFGoperc, which was related to improvement in depressive symptoms. In addition, we found significant associations of baseline network measures at the global, nodal, and edge levels with short-term and long-term improvements in depressive symptoms following esketamine administration, highlighting the prospect of functional network measures as useful predictors of antidepressant response to esketamine in patients with breast cancer.
In our prior study based on the EASE trial, we examined the clinical effect of intraoperative esketamine on postoperative depression in a relatively larger sample (52 patients in the esketamine group and 52 in the placebo group) [15]. Results showed that esketamine non-significantly doubled the proportion of patients with ≥ 50% reduction in depression scores, and esketamine significantly lowered MADRS scores on postoperative days 1 - 5 by nearly half. These previous findings suggest that esketamine could be a promising treatment for postoperative depression in patients with breast cancer. The current work complements and extends our prior study by demonstrating that intraoperative esketamine induced an increase in degree centrality of L-IFGoperc that was related to postoperative depressive symptom improvement, shedding light on the possible neural mechanism of esketamine action as an antidepressant in the context of breast cancer surgery. Indeed, the IFGoperc is typically thought to be an important brain region involved in emotional processes [79,80,81,82,83,84,85,86]. Structural and functional abnormalities of the IFGoperc have been well documented in patients with depression [83, 84, 87,88,89,90,91], emphasizing its pivotal role in depression neuropathology. Increased degree centrality of L-IFGoperc may reflect its strengthened role in coordinating whole-brain functional networks in response to esketamine treatment. Moreover, we found that the esketamine group at follow-up exhibited significantly higher degree centrality of L-IFGoperc than HC, but no significant differences were seen between HC and other patient groups, suggesting that the observed degree centrality increase may reflect a compensatory neuroadaptive change. Combined, our results invited the speculation that intraoperative esketamine may cause compensatory neuroplasticity in the L-IFGoperc characterized by its elevated functional importance in global information integration, which may in turn lead to depressive symptom improvement in breast cancer patients.
Our further analyses demonstrated significant associations of baseline network measures at the global, nodal, and edge levels with short-term and long-term improvements in depressive symptoms in the esketamine group. With respect to global measures, there was a negative correlation between baseline Lp and long-term MADRS change, indicating that breast cancer patents who have brain functional networks with worse global integration may show greater long-term improvement in depressive symptoms following esketamine administration. In terms of nodal measures, baseline degree centrality of L-IFGoperc was positively correlated with short-term MADRS changes, further confirming its outcome predictive value aside from unraveling the neural therapeutic mechanism described above. In addition, long-term MADRS change was negatively correlated with degree centrality of R-MCG and L-IOG, and was positively correlated with degree centrality of L-PUT. The opposite correlation patterns imply that the esketamine treatment outcome is by no means determined by a single brain region, but rather depends on the complex functional interactions across multiple different brain regions. The cingulate gyrus is a key node involved in emotion and acute pain [92], and abnormal functional connectivity of the cingulate gyrus has been reported in depression [93, 94]. The inverse association between baseline degree centrality of R-MCG and 12-week symptom change indicates that patients with relatively more baseline functional connectivity of R-MCG may show greater long-term improvement in depressive symptoms following esketamine, in support of the possibility that esketamine would induce more pronounced long-term neuroplasticity in a subset of patients characterized by a better baseline network state. As to edge measures, short-term MADRS change was negatively correlated with R-SMG to L-PAL functional connectivity, and long-term MADRS change was negatively correlated with L-SFGdor to L-STG, R-PoCG to R-SPG, and L-PCUN to L-ITG functional connectivity, suggesting that cortico-striatal and cortico-cortical connectivity are predictive of short-term and long-term improvements in depressive symptoms, respectively. It is largely known that SMG dysfunction has been associated with cognitive impairment [95], and the PAL is a striatal output nucleus that helps regulate movement and emotion [96]. One may suspect that efficient functional communication between the SMG and the PAL could facilitate rapid improvement in depressive symptoms after esketamine administration.
The novel contribution of our study lies in the confirmation of the practical dual use of intraoperative esketamine: as an adjunct anesthetic while simultaneously initiating antidepressant effects. This ‘two-for-one’ perioperative profile may be attractive for emerging surgical psychiatry, because symptom relief could be embedded into routine anesthetic care without adding a separate psychiatric procedure. The esketamine-induced increase in L-IFGoperc connections may represent a candidate network mechanism for this dual benefit, although this interpretation remains exploratory. From the perspective of clinical translation, the associations between baseline brain functional network measures and depressive symptom improvement suggest their prognostic value and potential utility to stratify patients, identifying those who will maximally benefit from perioperative esketamine administration. If validated in larger cohorts, such biomarkers could support earlier, biomarker-guided selection and personalized follow-up planning for perioperative depression management, echoing the recent concept of closed-loop precision psychiatry emphasizing the integration of MRI biomarkers for diagnostic classification, treatment response prediction, and individualized interventions [97].
Our study faces a few limitations. First, although our small sample size is commonplace for longitudinal study designs investigating within-person changes, it limits the statistical power and the generalization of the findings. Future studies in a larger sample are warranted to verify these preliminary results. Second, breast cancer patients enrolled in our study had mild-to-severe depressive symptoms, yet few met formal diagnostic criteria for major depressive disorder, which may influence our interpretation. Third, we used a single dose of 0.25 mg·kg⁻1 esketamine that appears insufficient to achieve satisfactory antidepressant efficacy due to the fact that the typical ketamine dose for antidepressant treatment is 0.5 mg·kg⁻¹ infused over 40 min [98]. Our dosing regimen accords with empirical evidence for comparable antidepressant efficacy between 0.25 mg·kg⁻¹ esketamine and 0.5 mg·kg⁻¹ racemic ketamine [99], as it is known that esketamine has approximately twice the affinity for NMDAR as ketamine. Fourth, all the included patients were Chinese women diagnosed with breast cancer, which might restrict generalizability to other populations. Fifth, given the rather small sample size and the exploratory nature of our study, a less rigorous false-positive correction for multiple testing was employed to balance the type Ⅰ and type Ⅱ errors. Sixth, our study only focused on brain functional network changes derived from resting-state fMRI. Future work should incorporate multimodal imaging techniques (e.g., diffusion MRI and PET) to futher elucidate other aspects of the neural effect of intraoperative esketamine. Finally, the follow-up resting-state fMRI scans were limited to postoperative day 1. We did not collect resting-state fMRI data at week 12 follow-up, hampering the possibility to further investigate the long-term effects of esketamine on brain functional networks.
In conclusion, using a combination of resting-state fMRI and graph theoretical analysis, the current RCT study demonstrated that intraoperative esketamine induced increased degree centrality of L-IFGoperc that was related to improvement in postoperative depressive symptoms in breast cancer patients. In addition, baseline network measures at the global, nodal, and edge levels were found to associate with short-term and long-term improvements in depressive symptoms following esketamine administration. These findings may not only provide novel insights into the neural mechanism by which esketamine exerts its antidepressant efficacy during the perioperative period, but also highlight the prospect of functional network measures as useful predictors of antidepressant response to esketamine in patients with breast cancer.
Data availability
The data that support the findings of this study are available from the corresponding author upon reasonable request.
References
Pilevarzadeh M, Amirshahi M, Afsargharehbagh R, Rafiemanesh H, Hashemi SM, Balouchi A. Global prevalence of depression among breast cancer patients: a systematic review and meta-analysis. Breast Cancer Res Treat. 2019;176:519–33.
Ghoneim MM, O’Hara MW. Depression and postoperative complications: an overview. BMC Surg. 2016;16:5. https://doi.org/10.1186/s12893-016-0120-y.
Wang X, Wang N, Zhong L, Wang S, Zheng Y, Yang B, et al. Prognostic value of depression and anxiety on breast cancer recurrence and mortality: a systematic review and meta-analysis of 282,203 patients. Mol Psychiatry. 2020;25:3186–97.
Vita G, Compri B, Matcham F, Barbui C, Ostuzzi G. Antidepressants for the treatment of depression in people with cancer. Cochrane Database Syst Rev. 2023;3:Cd011006, https://doi.org/10.1002/14651858.CD011006.pub4.
McIntyre RS, Rosenblat JD, Nemeroff CB, Sanacora G, Murrough JW, Berk M, et al. Synthesizing the evidence for ketamine and esketamine in treatment-resistant depression: An international expert opinion on the available evidence and implementation. Am J Psychiatry. 2021;178:383–99.
Kryst J, Kawalec P, Mitoraj AM, Pilc A, Lasoń W, Brzostek T. Efficacy of single and repeated administration of ketamine in unipolar and bipolar depression: a meta-analysis of randomized clinical trials. Pharmacol Rep. 2020;72:543–62.
Salloum NC, Fava M, Hock RS, Freeman MP, Flynn M, Hoeppner B, et al. Time to relapse after a single administration of intravenous ketamine augmentation in unipolar treatment-resistant depression. J Affect Disord. 2020;260:131–9.
Zhou Y, Sun W, Zhang G, Wang A, Lin S, Chan MTV, et al. Ketamine alleviates depressive symptoms in patients undergoing intracranial tumor resection: A randomized controlled trial. Anesth Analg. 2021;133:1588–97.
Yao J, Song T, Zhang Y, Guo N, Zhao P. Intraoperative ketamine for reduction in postpartum depressive symptoms after cesarean delivery: A double-blind, randomized clinical trial. Brain Behav. 2020;10:e01715, https://doi.org/10.1002/brb3.1715.
Guo J, Qiu D, Gu HW, Wang XM, Hashimoto K, Zhang GF, et al. Efficacy and safety of perioperative application of ketamine on postoperative depression: A meta-analysis of randomized controlled studies. Mol Psychiatry. 2023;28:2266–76.
Krystal JH, Charney DS, Duman RS. A New Rapid-Acting Antidepressant. Cell. 2020;181:7, https://doi.org/10.1016/j.cell.2020.02.033.
Mahase E. Esketamine is approved in Europe for treating resistant major depressive disorder. Bmj. 2019;367:l7069, https://doi.org/10.1136/bmj.l7069.
Molero P, Ramos-Quiroga JA, Martin-Santos R, Calvo-Sánchez E, Gutiérrez-Rojas L, Meana JJ. Antidepressant efficacy and tolerability of ketamine and esketamine: A critical review. CNS Drugs. 2018;32:411–20.
Wei Q, Chen C, Zhu J, Mei B, Liu X. Influence of low-dose esketamine on postoperative depressive symptoms in patients with breast cancer (EASE): Study protocol for a randomised controlled trial. BMJ Open. 2023;13:e075767, https://doi.org/10.1136/bmjopen-2023-075767.
Wei Q, Li M, Du Q, Zhang H, Liang Y, Cheng C, et al. Effect of esketamine on postoperative depression in women with breast cancer and preoperative depressive symptoms: The EASE randomized trial. J Clin Anesth. 2025;103:111821, https://doi.org/10.1016/j.jclinane.2025.111821.
Yang Y, Cui Y, Sang K, Dong Y, Ni Z, Ma S, et al. Ketamine blocks bursting in the lateral habenula to rapidly relieve depression. Nature. 2018;554:317–22.
Cui Y, Hu S, Hu H. Lateral habenular burst firing as a target of the rapid antidepressant effects of ketamine. Trends Neurosci. 2019;42:179–91.
Ma S, Chen M, Jiang Y, Xiang X, Wang S, Wu Z, et al. Sustained antidepressant effect of ketamine through NMDAR trapping in the LHb. Nature. 2023;622:802–9.
Evans JW, Szczepanik J, Brutsché N, Park LT, Nugent AC, Zarate CA Jr. Default mode connectivity in major depressive disorder measured up to 10 days after ketamine administration. Biol Psychiatry. 2018;84:582–90.
Alario AA, Niciu MJ. Biomarkers of ketamine’s antidepressant effect: a clinical review of genetics, functional connectivity, and neurophysiology. Chronic Stress (Thousand Oaks). 2021;5:24705470211014210, https://doi.org/10.1177/24705470211014210.
Medeiros GC, Matheson M, Demo I, Reid MJ, Matheson S, Twose C, et al. Brain-based correlates of antidepressant response to ketamine: a comprehensive systematic review of neuroimaging studies. Lancet Psychiatry. 2023;10:790–800.
Zavaliangos-Petropulu A, Al-Sharif NB, Taraku B, Leaver AM, Sahib AK, Espinoza RT, et al. Neuroimaging-derived biomarkers of the antidepressant effects of ketamine. Biol Psychiatry Cogn Neurosci Neuroimaging. 2023;8:361–86.
Ionescu DF, Felicione JM, Gosai A, Cusin C, Shin P, Shapero BG, et al. Ketamine-Associated brain changes: A review of the neuroimaging literature. Harv Rev Psychiatry. 2018;26:320–39.
Kotoula V, Webster T, Stone J, Mehta MA. Resting-state connectivity studies as a marker of the acute and delayed effects of subanaesthetic ketamine administration in healthy and depressed individuals: A systematic review. Brain Neurosci Adv. 2021;5:23982128211055426, https://doi.org/10.1177/23982128211055426.
Abdallah CG, Salas R, Jackowski A, Baldwin P, Sato JR, Mathew SJ. Hippocampal volume and the rapid antidepressant effect of ketamine. J Psychopharmacol. 2015;29:591–5.
Sporns O. The human connectome: a complex network. Ann N Y Acad Sci. 2011;1224:109–25.
Bullmore ET, Bassett DS. Brain graphs: Graphical models of the human brain connectome. Annu Rev Clin Psychol. 2011;7:113–40.
He Y, Evans A. Graph theoretical modeling of brain connectivity. Curr Opin Neurol. 2010;23:341–50.
Bullmore E, Sporns O. Complex brain networks: Graph theoretical analysis of structural and functional systems. Nat Rev Neurosci. 2009;10:186–98.
Bassett DS, Bullmore E. Small-world brain networks. Neuroscientist. 2006;12:512–23.
Watts DJ, Strogatz SH. Collective dynamics of ‘small-world’ networks. Nature. 1998;393:440–2.
Achard S, Salvador R, Whitcher B, Suckling J, Bullmore E. A resilient, low-frequency, small-world human brain functional network with highly connected association cortical hubs. J Neurosci. 2006;26:63–72.
Bassett DS, Meyer-Lindenberg A, Achard S, Duke T, Bullmore E. Adaptive reconfiguration of fractal small-world human brain functional networks. Proc Natl Acad Sci USA. 2006;103:19518–23.
Hagmann P, Kurant M, Gigandet X, Thiran P, Wedeen VJ, Meuli R, et al. Mapping human whole-brain structural networks with diffusion MRI. PLoS One. 2007;2:e597, https://doi.org/10.1371/journal.pone.0000597.
He Y, Chen ZJ, Evans AC. Small-world anatomical networks in the human brain revealed by cortical thickness from MRI. Cereb Cortex. 2007;17:2407–19.
Salvador R, Suckling J, Coleman MR, Pickard JD, Menon D, Bullmore E. Neurophysiological architecture of functional magnetic resonance images of human brain. Cereb Cortex. 2005;15:1332–42.
Zhu J, Zhuo C, Liu F, Qin W, Xu L, Yu C. Distinct disruptions of resting-state functional brain networks in familial and sporadic schizophrenia. Sci Rep. 2016;6:23577, https://doi.org/10.1038/srep23577.
Zhu J, Zhao W, Zhang C, Wang H, Cheng W, Li Z, et al. Disrupted topological organization of the motor execution network in alcohol dependence. Psychiatry Res Neuroimaging. 2018;280:1–8.
Liu S, Zhong H, Qian Y, Cai H, Jia YB, Zhu J. Neural mechanism underlying the beneficial effect of Theory of Mind psychotherapy on early-onset schizophrenia: a randomized controlled trial. J Psychiatry Neurosci. 2023;48:E421–E430.
Chen C, Liu Z, Xi C, Tan W, Fan Z, Cheng Y, et al. Multimetric structural covariance in first-episode major depressive disorder: A graph theoretical analysis. J Psychiatry Neurosci. 2022;47:E176–E185.
Sankar A, Scheinost D, Goldman DA, Drachman R, Colic L, Villa LM, et al. Graph theory analysis of whole brain functional connectivity to assess disturbances associated with suicide attempts in bipolar disorder. Transl Psychiatry. 2022;12:7, https://doi.org/10.1038/s41398-021-01767-z.
Manelis A, Almeida JR, Stiffler R, Lockovich JC, Aslam HA, Phillips ML. Anticipation-related brain connectivity in bipolar and unipolar depression: a graph theory approach. Brain. 2016;139:2554–66.
Song Y, Zhou X, Zhao H, Zhao W, Sun Z, Zhu J, et al. Characterizing the role of the microbiota-gut-brain axis in cerebral small vessel disease: An integrative multi‑omics study. Neuroimage. 2024;303:120918, https://doi.org/10.1016/j.neuroimage.2024.120918.
Zhang Y, Mu N, Qi S, Sun C, Rao Y, Yang X, et al. Improved brain functional network in major depressive disorder with suicidal ideation after individual target-transcranial magnetic stimulation treatment: a graph-theory analysis. Front Psychiatry. 2025;16:1486835, https://doi.org/10.3389/fpsyt.2025.1486835.
Xie Y, He Y, Guan M, Wang Z, Zhou G, Ma Z, et al. Low-frequency rTMS treatment alters the topographical organization of functional brain networks in schizophrenia patients with auditory verbal hallucination. Psychiatry Res. 2022;309:114393, https://doi.org/10.1016/j.psychres.2022.114393.
Geng Y, Zhang H, Dong Z, Zhang H. Effects of electroconvulsive therapy on functional brain networks in patients with schizophrenia. BMC Psychiatry. 2024;24:29, https://doi.org/10.1186/s12888-023-05408-1.
Li Y, Li Y, Wei Q, Bai T, Wang K, Wang J, et al. Mapping intrinsic functional network topological architecture in major depression disorder after electroconvulsive therapy. J Affect Disord. 2022;311:103–9.
Wang LX, Guo F, Zhu YQ, Wang HN, Liu WM, Li C, et al. Effect of second-generation antipsychotics on brain network topology in first-episode schizophrenia: A longitudinal rs-fMRI study. Schizophr Res. 2019;208:160–6.
Odkhuu S, Kim WS, Tsogt U, Shen J, Cheraghi S, Li L, et al. Network biomarkers in recovered psychosis patients who discontinued antipsychotics. Mol Psychiatry. 2023;28:3717–26.
Dai YR, Wu YK, Chen X, Zeng YW, Li K, Li JT, et al. Eight-week antidepressant treatment changes intrinsic functional brain topology in first-episode drug-naïve patients with major depressive disorder. J Affect Disord. 2023;329:225–34.
Lin WC, Cheng LK, Su TP, Chen LF, Tu PC, Li CT, et al. Triple-network model-based graph theory analysis of the effectiveness of low-dose ketamine in patients with treatment-resistant depression: two resting-state functional MRI clinical trials. Br J Psychiatry. 2025;227:1–9.
Luo WY, Liu H, Feng Y, Hao JX, Zhang YJ, Peng WF, et al. Efficacy of cathodal transcranial direct current stimulation on electroencephalographic functional networks in patients with focal epilepsy: Preliminary findings. Epilepsy Res. 2021;178:106791, https://doi.org/10.1016/j.eplepsyres.2021.106791.
Yang H, Chen X, Chen ZB, Li L, Li XY, Castellanos FX, et al. Disrupted intrinsic functional brain topology in patients with major depressive disorder. Mol Psychiatry. 2021;26:7363–71.
Guo ZP, Liao D, Chen L, Wang C, Qu M, Lv XY, et al. Transcutaneous auricular vagus nerve stimulation modulating the brain topological architecture of functional network in major depressive disorder: An fMRI study. Brain Sci. 2024;14:945, https://doi.org/10.3390/brainsci14090945.
Xu K, Long D, Zhang M, Wang Y. The efficacy of topological properties of functional brain networks in identifying major depressive disorder. Sci Rep. 2024;14:29453, https://doi.org/10.1038/s41598-024-80294-5.
Vecchio D, Piras F, Ciullo V, Piras F, Natalizi F, Ducci G, et al. Brain network topology in deficit and non-deficit schizophrenia: Application of graph theory to local and global indices. J Pers Med. 2023;13:799, https://doi.org/10.3390/jpm13050799.
Zhang L, Hu X, Hu Y, Tang M, Qiu H, Zhu Z, et al. Structural covariance network of the hippocampus-amygdala complex in medication-naïve patients with first-episode major depressive disorder. Psychoradiology. 2022;2:190–8.
Zhang W, Lei D, Keedy SK, Ivleva EI, Eum S, Yao L, et al. Brain gray matter network organization in psychotic disorders. Neuropsychopharmacology. 2020;45:666–74.
Zhu J, Qian Y, Zhang B, Li X, Bai Y, Li X, et al. Abnormal synchronization of functional and structural networks in schizophrenia. Brain Imaging Behav. 2020;14:2232–41.
Moher D, Schulz KF, Altman DG. The CONSORT statement: revised recommendations for improving the quality of reports of parallel-group randomised trials. Clin Oral Investig. 2003;7:2–7.
Kroenke K, Spitzer RL, Williams JB. The PHQ-9: validity of a brief depression severity measure. J Gen Intern Med. 2001;16:606–13.
Williams JB, Kobak KA. Development and reliability of a structured interview guide for the Montgomery Asberg Depression Rating Scale (SIGMA). Br J Psychiatry. 2008;192:52–8.
Floden L, Hudgens S, Jamieson C, Popova V, Drevets WC, Cooper K, et al. Evaluation of Individual Items of the Patient Health Questionnaire (PHQ-9) and Montgomery-Asberg Depression Rating Scale (MADRS) in Adults with treatment-resistant depression treated with esketamine nasal spray combined with a new oral antidepressant. CNS Drugs. 2022;36:649–58.
Montgomery SA, Asberg M. A new depression scale designed to be sensitive to change. Br J Psychiatry. 1979;134:382–9.
Yan CG, Wang XD, Zuo XN, Zang YF. DPABI: Data processing & analysis for (Resting-State) brain imaging. Neuroinformatics. 2016;14:339–51.
Mo F, Zhao H, Li Y, Cai H, Song Y, Wang R, et al. Network localization of state and trait of auditory verbal hallucinations in schizophrenia. Schizophr Bull. 2024;50:1326–36.
Zhang X, Xu R, Ma H, Qian Y, Zhu J. Brain structural and functional damage network localization of suicide. Biol Psychiatry. 2024;95:1091–9.
Cheng Y, Cai H, Liu S, Yang Y, Pan S, Zhang Y, et al. Brain network localization of gray matter atrophy and neurocognitive and social cognitive dysfunction in schizophrenia. Biol Psychiatry. 2025;97:148–56.
Xu R, Zhang X, Zhou S, Guo L, Mo F, Ma H, et al. Brain structural damage networks at different stages of schizophrenia. Psychol Med. 2024;54:4809–19.
Murphy K, Fox MD. Towards a consensus regarding global signal regression for resting state functional connectivity MRI. Neuroimage. 2017;154:169–73.
Ashburner J. A fast diffeomorphic image registration algorithm. Neuroimage. 2007;38:95–113.
Wang J, Wang X, Xia M, Liao X, Evans A, He Y. GRETNA: a graph theoretical network analysis toolbox for imaging connectomics. Front Hum Neurosci. 2015;9:386, https://doi.org/10.3389/fnhum.2015.00458.
Suo X, Lei D, Li K, Chen F, Li F, Li L, et al. Disrupted brain network topology in pediatric posttraumatic stress disorder: A resting-state fMRI study. Hum Brain Mapp. 2015;36:3677–86.
He Y, Chen Z, Evans A. Structural insights into aberrant topological patterns of large-scale cortical networks in Alzheimer’s disease. J Neurosci. 2008;28:4756–66.
Achard S, Bullmore E. Efficiency and cost of economical brain functional networks. PLoS Comput Biol. 2007;3:e17, https://doi.org/10.1371/journal.pcbi.0030017.
Bassett DS, Bullmore E, Verchinski BA, Mattay VS, Weinberger DR, Meyer-Lindenberg A. Hierarchical organization of human cortical networks in health and schizophrenia. J Neurosci. 2008;28:9239–48.
Zuo XN, Ehmke R, Mennes M, Imperati D, Castellanos FX, Sporns O, et al. Network centrality in the human functional connectome. Cereb Cortex. 2012;22:1862–75.
Rubinov M, Sporns O. Complex network measures of brain connectivity: uses and interpretations. Neuroimage. 2010;52:1059–69.
Du J, Rolls ET, Cheng W, Li Y, Gong W, Qiu J, et al. Functional connectivity of the orbitofrontal cortex, anterior cingulate cortex, and inferior frontal gyrus in humans. Cortex. 2020;123:185–99.
Shi K, Li J, Zhang H, Wang K, Li C, Xia Y, et al. The functional and structural alterations in brain regions related to the fear network model in panic disorder: A resting-state fMRI and T1-weighted imaging study. J Psychiatr Res. 2024;177:59–65.
Imajo N, Matsuzaki Y, Kobayashi A, Sakaki K, Nouchi R, Kawashima R. Self-Choice emotion regulation enhances stress reduction: Neural basis of self-choice emotion regulation. Brain Sci. 2024;14:1077, https://doi.org/10.3390/brainsci14111077.
Liu S, Zhang X, Wang Q, Xu Y, Huang X, Liu T, et al. Increased attentional network activity in premature ejaculation patients with anxiety revealed by resting-state functional magnetic resonance imaging. Eur J Neurosci. 2021;54:5417–26.
Lin X, Zhou RB, Huang J, Su YS, Mao RZ, Niu ZA, et al. Altered resting-state fMRI signals and network topological properties of bipolar depression patients with anxiety symptoms. J Affect Disord. 2020;277:358–67.
Keller M, Mendoza-Quiñones R, Cabrera Muñoz A, Iglesias-Fuster J, Virués AV, Zvyagintsev M, et al. Transdiagnostic alterations in neural emotion regulation circuits - neural substrates of cognitive reappraisal in patients with depression and post-traumatic stress disorder. BMC Psychiatry. 2022;22:173, https://doi.org/10.1186/s12888-022-03780-y.
Fu S, Liang S, Lin C, Wu Y, Xie S, Li M, et al. Aberrant brain entropy in posttraumatic stress disorder comorbid with major depressive disorder during the coronavirus disease 2019 pandemic. Front Psychiatry. 2023;14:1143780, https://doi.org/10.3389/fpsyt.2023.1143780.
Schwarzmeier H, Kleint NI, Wittchen HU, Ströhle A, Hamm AO, Lueken U. Characterizing the nature of emotional-associative learning deficits in panic disorder: An fMRI study on fear conditioning, extinction training and recall. Eur Neuropsychopharmacol. 2019;29:306–18.
Zhou Y, Zhu Y, Ye H, Jiang W, Zhang Y, Kong Y, et al. Abnormal changes of dynamic topological characteristics in patients with major depressive disorder. J Affect Disord. 2024;345:349–57.
Guo W, Liu F, Zhang Z, Liu J, Yu M, Zhang J, et al. Unidirectionally affected causal connectivity of cortico-limbic-cerebellar circuit by structural deficits in drug-naive major depressive disorder. J Affect Disord. 2015;172:410–6.
Li X, Chen X, Zhou Y, Dai L, Cui LB, Yu R, et al. Altered regional homogeneity and amplitude of low-frequency fluctuations induced by electroconvulsive therapy for adolescents with depression and suicidal ideation. Brain Sci. 2022;12:1121, https://doi.org/10.3390/brainsci12091121.
Dai D, Lacadie CM, Holmes SE, Cool R, Anticevic A, Averill C, et al. Ketamine normalizes the structural alterations of inferior frontal gyrus in depression. Chronic Stress (Thousand Oaks). 2020;4:2470547020980681, https://doi.org/10.1177/2470547020980681.
Cao P, Dai K, Liu X, Hu J, Jin Z, Xu S, et al. Differences in resting-state brain activity in first-episode drug-naïve major depressive disorder patients with and without suicidal ideation. Eur J Neurosci. 2024;59:2766–77.
Vogt BA. Pain and emotion interactions in subregions of the cingulate gyrus. Nat Rev Neurosci. 2005;6:533–44.
Yang X, Su Y, Yang F, Song Y, Yan J, Luo Y, et al. Neurofunctional mapping of reward anticipation and outcome for major depressive disorder: A voxel-based meta-analysis. Psychol Med. 2022;52:3309–22.
Fu YJ, Liu X, Wang XY, Li X, Dai LQ, Ren WY, et al. Abnormal volumetric brain morphometry and cerebral blood flow in adolescents with depression. World J Psychiatry. 2023;13:386–96.
Hoshi H, Kobayashi M, Hirata Y, Fukasawa K, Ichikawa S, Shigihara Y. Decreased beta-band activity in left supramarginal gyrus reflects cognitive decline: Evidence from a large clinical dataset in patients with dementia. Hum Brain Mapp. 2023;44:6214–26.
Obeso JA, Rodríguez-Oroz MC, Benitez-Temino B, Blesa FJ, Guridi J, Marin C, et al. Functional organization of the basal ganglia: Therapeutic implications for Parkinson’s disease. Mov Disord. 2008;23:S548–59.
Gao QL, Chen X, Castellanos FX, Lu B, Yan CG. Towards closed-loop precision psychiatry: Integrating MRI biomarkers for individualized care of major depressive disorder. Psychoradiology. 2025;5:kkaf024, https://doi.org/10.1093/psyrad/kkaf024.
Sanacora G, Frye MA, McDonald W, Mathew SJ, Turner MS, Schatzberg AF, et al. A consensus statement on the use of ketamine in the treatment of mood disorders. JAMA Psychiatry. 2017;74:399–405.
Correia-Melo FS, Leal GC, Vieira F, Jesus-Nunes AP, Mello RP, Magnavita G, et al. Efficacy and safety of adjunctive therapy using esketamine or racemic ketamine for adult treatment-resistant depression: A randomized, double-blind, non-inferiority study. J Affect Disord. 2020;264:527–34.
Acknowledgements
We sincerely thank all participants for their time and commitment to this study. We also thank the clinical and research staff who contributed to participant recruitment, perioperative coordination, MRI data acquisition, and study implementation. Additionally, we acknowledge the support provided by The First Affiliated Hospital of Anhui Medical University.
Funding
The study was supported by the National Natural Science Foundation of China (grant numbers: 82471952 and 82371928), the Anhui Provincial Natural Science Foundation (grant number: 2308085MH277), the Scientific Research Key Project of Anhui Province Universities (grant number: 2022AH051135), and the Scientific Research Foundation of Anhui Medical University (grant number: 2022xkj143).
Author information
Authors and Affiliations
Contributions
HZ analyzed the data and wrote the first draft. HZ, QW, SX and YS collected the data. XL supervised the project. JZ and YY acquired funding, planned and supervised the study and reviewed the manuscript. HZ and JZ revised the manuscript. All authors read and approved the final manuscript.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Zhu, H., Wei, Q., Xu, S. et al. Brain functional network correlates and predictors of the perioperative antidepressant effect of esketamine in breast cancer patients: a double-blind randomized controlled trial using resting-state fMRI and graph theory. Transl Psychiatry 16, 135 (2026). https://doi.org/10.1038/s41398-026-03929-3
Received:
Revised:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41398-026-03929-3
