
Abstract
Background
Finland’s national vitamin D fortification policy has significantly improved the population’s vitamin D sufficiency. This study investigates the association between serum vitamin D concentration and muscle health, considering the impact of menopause and aging in Finnish cohorts.
Methods
The study comprised two cohorts: 237 middle-aged women (aged 47–55 years) from the Estrogenic Regulation of Muscle Apoptosis (ERMA) study and its follow-up, and 908 older adults (aged 75, 80, and 85 years) from the Active Aging (AGNES) study. Vitamin D concentration was assessed through serum 25-hydroxyvitamin D (25(OH)D) concentrations, alongside measurements of muscle mass and function.
Results
High concentrations of 25(OH)D were observed across both cohorts, aligning with Finland’s fortification efforts. Furthermore, no significant correlations were found between 25(OH)D concentrations and indicators of muscle mass or function in either age group. Notably, middle-aged women in menopausal transition exhibited a slight increase in 25(OH)D concentrations, yet this did not translate into improved muscle outcomes. Similarly, older adults demonstrated sufficient 25(OH)D concentrations without a corresponding enhancement in muscle health.
Conclusions
The findings indicate that, within the context of Finland’s vitamin D fortification program, serum 25(OH)D sufficiency does not directly correlate with better muscle mass or function among middle-aged and older Finnish populations. These results suggest a need for a broader approach to sarcopenia prevention, incorporating factors beyond vitamin D sufficiency. Further research is warranted to explore the multifactorial nature of muscle health during aging and the menopausal transition, to develop targeted interventions for sarcopenia prevention.
Similar content being viewed by others
Introduction
Aging diminishes muscle mass and function, elevating the risk of falls, fractures, and metabolic disorders [1]. Studies even in middle-aged individuals indicate that reduced muscle mass contributes to worsened cholesterol profiles and insulin resistance [2]. Notably, a decade-long study on over 2000 adults found that higher skeletal muscle mass (SMM) significantly lowers cardiovascular disease (CVD) risk [3], highlighting its predictive value for CVD outcomes.
Research has shown a decline in lean mass between peri- and early postmenopause, with Juppi et al. reporting reductions of 0.5–1.5% during this transition, as measured by Dual-energy X-ray Absorptiometry (DXA) and Computed Tomography (CT) imaging [4]. The findings underscore the significance of hormonal shifts during menopause in reducing lean and muscle mass, distinct from aging’s impact. Specifically, cellular apoptosis pathways like heat-shock proteins, cell death receptor ligands, and microRNAs targeting apoptosis are primary suspects in muscle decline due to estrogen deficiency [5, 6]. Yet, whether the decrease in protein synthesis or heightened proteolysis due to hormonal changes drives this loss remains debated [6].
Vitamin D plays a critical role in muscle growth, development [7], and contraction [8]. Insufficient vitamin D concentration can impair muscle cell function [9], leading to reduced muscle mass and power, particularly in the lower limbs [10, 11]. This deficiency is also associated with diminished physical capabilities and a higher risk of falls, especially in the elderly [12]. Aging further impacts the synthesis of active vitamin D, exacerbating these effects [13]. Research links low 25-hydroxyvitamin D (25(OH)D) concentration in menopausal women to muscle mass reduction, independent of factors like age and lifestyle [14]. Studies confirm that vitamin D deficiency, particularly in menopausal women, is associated with muscle strength decline and increased sarcopenia risk [15]. Furthermore, vitamin D supplementation in postmenopausal women has been shown to enhance muscle strength and prevent lean mass loss [16], although no previous study has investigated the anabolic effect of vitamin D supplementation during menopausal transition. These results underscore the importance of adequate vitamin D for muscle preservation among middle-aged and older women.
Launched in 2003, Finland’s fortification policy, aimed at combating vitamin D deficiency due to limited sunlight, has markedly enhanced the population’s vitamin D status by fortifying milk products and fat spreads with vitamin D3 and promoting oral supplementation in darker months [17, 18]. This initiative has significantly raised vitamin D intake from an average of 5 µg/day to 17 µg/day in men and 3 µg/day to 12 µg/day in women, resulting in an average serum 25(OH)D concentration increase of 17 nmol/L [19]. While no direct comparison exists regarding sarcopenia rates before and after Finland’s fortification policy, the notable improvement in vitamin D status implies a strong potential to reduce muscle mass and function decline in menopausal and post-menopausal women.
The purpose of this study is to assess the association between serum 25(OH)D concentrations and SMM and function in middle-aged and older populations in Finland, considering the impact of menopausal status and lifestyle factors. The study aims to provide insights into the potential role of vitamin D in preserving muscle health against age-related decline and the impact of lifestyle factors such as diet, supplement use, physical activity, and obesity on vitamin D status within the Finnish context.
Subjects and methods
Study design
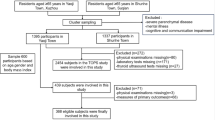
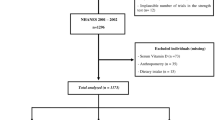
This study uses the data and blood samples from two observational datasets comprising middle-aged women and older women and men age cohorts. The middle-aged women cohort is part of the Estrogenic Regulation of Muscle Apoptosis (ERMA) study and its four-year follow-up Estrogen, MicroRNAs and the Risk of Metabolic Dysfunction (EsmiRs) study (dataset: doi.10.17011/jyx/dataset/83491) representing 47–55-years old white Finnish women. The older cohort is part of the Active aging – resilience and external support as modifiers of the disablement outcome (AGNES) study [20] including three age cohorts (75, 80, and 85 years) of white Finnish women and men living independently in the city of Jyväskylä in Central Finland (dataset: doi.10.17011/jyx/dataset/83811). The ERMA study was approved by the Ethics Committee of the Central Finland Health Care District in 2014 (K-S shp Dnro U/2014). Participants provided two separate signed consents: initial consent for the use of prequestionnaire data in research and publications (phase one) and additional informed consent before laboratory examinations, detailing potential risks and benefits and authorizing data use for research and publications (phase two) [21]. The AGNES study was approved by the Ethics Committee of the Central Finland Health Care District on August 23, 2017. Participants provided written informed consent before the home interview, with separate approvals for research center assessments, patient record use, and future contact. The study adhered to the Declaration of Helsinki [20].
The ERMA study began in December 2014 [21] with subsequent phases including EsmiRs starting November 2018 [22]. The ERMA study initially included 1393 women, with 1158 participating in later phases. The sample and contact information were sourced as a random sample of the target population from the Population Information System managed by the Population Register Center (http://vrk.fi/en). To minimize self-exclusion and ensure a representative sample for the study’s initial phase, the invitation letter did not mention exclusion criteria. Exclusion criteria included significant health conditions or medication use affecting hormonal or inflammatory statuses. For EsmiRs, 811 were invited, with 494 completing questionnaires and 304 undergoing lab tests. The AGNES study was collected between September 2017 to December 2018 [23]. It targeted 2791 individuals, with 1021 completing surveys or interviews and 910 participating in physiological tests. All studies adhered to the Declaration of Helsinki, with participant consent and ethical approval (ERMA 8U/2014, EsmiRs 9U/2018, AGNES August 23, 2017). The current analysis focused on participants with available 25(OH)D blood samples and at least one physiological test, including 237 middle-aged women and 908 older individuals (56.8% women).
Measurement of vitamin D concentration, vitamin D sufficiency groups and use of vitamin D supplements
Fasting (middle-aged women cohort) and non-fasting (older women and men cohort) blood samples were taken from the antecubital vein. Serum was collected by standard procedures, aliquoted and stored at −80 °C or immediately used for biomarker assessments. For the current study, 25(OH)D concentration was measured by two clinical laboratories: Vita Laboratoriot Oy (Helsinki, Finland) using Elecsys Vitamin D total II electrochemiluminescence binding assay (Roche Diagnostics, Finland) and Synlab Suomi (Espoo, Finland) using ARCHITECT chemiluminescent microparticle immunoassay (Abbot architect, USA). Serum 25(OH)D cut-offs are defined by the Institute of Medicine (IOM) as follows: deficiency (<30 nmol/L), inadequacy (30 to <50 nmol/L), sufficiency (≥50 nmol/L), and excessive (>125 nmol/L), based on the 2011 guidelines [24].
In the middle-aged women cohort, participants self-reported the use of any supplements, number of supplements and type or brand names of the used supplements. This data was used to construct the following variables: use of any supplement (yes/no), number of supplements used (none, 1–2, 3–5, ≥6), and use of vitamin D supplements (yes/no). In the older women and men cohort, participants self-reported the use of medication prescribed by a medical doctor, but the use of self-prescribed supplements was not asked. Of the reported medications, a variable use of vitamin D medication was constructed (yes/no).
Physiological tests
Detailed procedures for physiological tests are described in the Supplemental Information. Briefly, body composition was assessed using DXA (LUNAR Prodigy; GE Healthcare, Chicago, IL) for middle-aged women and BIA (InBody 720, Biospace, Seoul, Korea) for older women and men, analyzing total (LBM) and appendicular lean body mass (summed lean mass of arms and legs, ALM) as SMM proxies. Similarly, BIA provided skeletal (SM) and soft lean mass estimates (LBM).
Both cohorts underwent knee extension (KE) and handgrip force (HG) evaluations using a custom dynamometer chair (Good Strength; Metitur Oy, Palokka, Finland), with measurements taken at specified limb angles and positions [20, 23, 25, 26]. The middle-aged women’s cohort also had vertical jump height assessed via a contact mat, calculating elevation from flight time [25]. For all performance tests, the best of three to five maximal efforts was recorded.
Descriptive and other variables
In both cohorts, socioeconomic status data was obtained via questionnaires, with education categorized as ≤secondary or ≥tertiary, and smoking status as never or ever (including current/past smokers). For the middle-aged women cohort, menopausal status was assessed using menstrual diaries and follicle-stimulating hormone (FSH) measurements at the ERMA baseline [21], and by questionnaires and FSH at the EsmiRs [22]. This informed a menopausal transition variable comprising three groups: transition (from pre-/perimenopausal to postmenopausal), PRE/PERI (consistent pre-/perimenopausal), and POST (consistent postmenopausal). The Executive Summary of the Stages of Reproductive Aging criteria for defining menopausal status is based on increasing variability (in perimenopause) and finally the absence of menstrual bleeding for 12 months (in postmenopause), as well as elevated FSH levels in two consecutive measurements [27]. The ERMA study used self-reported menstrual cycles and two FSH measurements to confirm postmenopause. When tracking menstrual bleeding was not possible, i.e., for women using progesterone-releasing intrauterine devices or those who had undergone hysterectomy, FSH levels were the primary criterion.
In the middle-aged women cohort, physical activity was measured using the SR-PA L7 scale, categorizing activities into low, medium, and high levels based on daily activities to competitive sports [28]. Longitudinal activity groups were established based on changes in these levels over time. Leisure-time activity was evaluated through a questionnaire assessing frequency, intensity, duration, and commuting time, from which MET hours per day for leisure activity were calculated [29]. Physical activity of older women and men was categorized into three levels using the activity scale with six options was used, omitting the lowest activity level due to its rare selection in past studies [30]. In the ERMA and EsmiRs studies, participants completed the main questionnaires at home before visiting the research center, where staff checked for missing responses. In the AGNES study, questionnaires were completed during face-to-face interviews at participants’ homes or the research center. Trained research staff conducted these interviews to ensure consistency and minimize missing data. In both cohorts, body mass and height were measured, and body mass index (BMI; kg/m2) was calculated. Participants were categorized into normal (BMI ≤ 24.9), overweight (BMI 25–29.9), and obesity (BMI ≥ 30). Longitudinally, BMI categories were defined based on changes toward normal weight, obesity, or severe obesity.
Seasonality was recorded at blood sampling and categorized into winter (December, January, and February), spring (March, April, and May), summer (June, July, and August), and autumn (September, October and November), with winter and autumn as dark seasons due to limited sunlight. In the cohort of middle-aged women, sampled twice, seasons were classified into light season (spring or summer at both timepoints), towards lightness (baseline sampling at winter or autumn and follow-up sampling at spring or summer), towards darkness (baseline sampling at spring or summer and follow-up sampling at winter or autumn), or dark season (winter or autumn at both timepoints) based on the sampling timeline.
Statistics
Descriptive statistics including frequencies, means, and standard deviations were used to describe the study cohorts. Univariate group comparisons were performed using t-tests or general linear models (GLM). Repeated measurement data structure of the middle-aged women cohort was taken into account in the analysis. Potential confounders identified by the literature were age, sex, season, education, smoking, physical activity, and BMI, influencing 25(OH)D concentrations. Univariate models linked sex, menopausal status, physical activity, and BMI to 25(OH)D concentrations. Adjustments for body dimensions used body mass and height instead of BMI. Linear mixed-effect models for middle-aged women included time (0 = baseline, 1 = follow-up), vitamin D, menopausal status, body mass, height, and physical activity, excluding sex and age due to uniformity. Linear regression for older cohorts used 25(OH)D concentration as a predictor with confounders like sex, body mass, height, physical activity, and mean-centered age; menopausal status was omitted as participants were postmenopausal. Sex-stratified analyses, showing no significant differences, led to a combined analysis with sex as a covariate. The normality of residuals and other model assumptions were evaluated by graphical methods before accepting the results. All statistical analyses were performed with IBM SPSS Statistics software version 28 (Chicago, IL, US), and p < 0.05 was considered statistically significant.
Results
Based on the measured 25(OH)D concentrations, 79–90% of participants were classified as having “sufficient” 25(OH)D levels (Table 1). Older men showed the highest deficiency (2%) and insufficiency (8%), with excessive 25(OH)D concentrations most common among them (10%) and least common in middle-aged women at baseline (6%).
The self-reported use of any type of supplements including those containing vitamin D, appeared to be frequent among middle-aged women. At baseline nearly 80% and at follow-up 73% reported using vitamin D-containing supplements. The corresponding numbers for the use of any supplements were 87% and 85%, respectively. Of the older women and men cohort, only the use of medication prescribed by physicians was assessed, thus numbers cannot be compared between cohorts. Of the older women, 16%, and of the older men, 7% reported using vitamin D-containing drugs.
In the middle-aged women cohort, 25(OH)D concentrations were generally high and significantly higher at follow-up timepoint than at baseline (82.8 ± 23.8 vs. 87.3 ± 29.4 nmol/l, p < 0.001, Table 2). Group variables were constructed from the potential effectors of the 25(OH)D concentrations and presented in Table 2.
Women transitioning from pre- or perimenopause to postmenopause showed a smaller increase in 25(OH)D concentrations compared to those who were postmenopausal at both timepoints (4.5 vs. 5.9 units, p = 0.001). Physical activity level was also associated significantly with 25(OH)D concentration (p = 0.033). Women belonging to the normal body mass group had higher 25(OH)D concentrations than women belonging to the group with obesity (p = 0.024). In older women and men cohort, 25(OH)D concentrations were higher among women than men (86.8 ± 30.0 vs. 81.3 ± 30.9, p = 0.007, Table 3). Potential effectors that may influence 25(OH)D concentrations are presented as group variables in Table 3. Only BMI had a significant group difference (p = 0.004) while all others reproduced the sex difference in 25(OH)D concentrations.
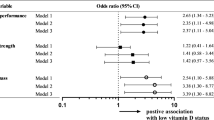
Associations of 25(OH)D concentration with proxies of SMM and KE, HG, and VJH were analyzed using linear mixed-effect models for the middle-aged women cohort (Table 4) and linear regression models for older women and men cohort (Table 5). The 25(OH)D concentration had a negligible effect with a non-significant regression coefficient of −0.034 to 0.082 in models constructed with data from middle-aged women and <0.001 to 0.106 in models constructed with data from older women and men when models were controlled for potential confounding factors.
Discussion
This study explored the link between serum 25-hydroxycholecalciferol (25(OH)D) and muscle mass and function in Finnish middle-aged women and older adults. Findings revealed that none of the middle-aged women were vitamin D deficient, with the majority displaying sufficient 25(OH)D concentrations. A small fraction of the older cohort had vitamin D deficiency, though most had adequate levels. Notably, after adjusting for confounders, no significant correlation was found between 25(OH)D concentrations and muscle mass or function in any group, indicating that serum 25(OH)D is not related to the loss of muscle mass or function due to menopause or aging in these cohorts.
Aging leads to a 50% decrease in vitamin D biosynthesis, attributed to lower 7-dehydrocholesterol levels and reduced UV light response [13]. Studies have shown serum 25(OH)D concentrations are lower in postmenopausal than in premenopausal women [31]. Premenopausal women have higher serum 25(OH)D and vitamin D-binding protein (DBP) levels compared to postmenopausal women, with estradiol independently associated with DBP concentrations [31]. However, the precise connection between DBP and estrogen remains uncertain. In our study, no middle-aged subjects were “deficient” in vitamin D, with only 4–6% “insufficient”. Among the older cohort, 0.4% of women and 2.3% of men had insufficient 25(OH)D concentrations. These findings indicate that Finnish middle-aged and older individuals mostly maintained healthy serum 25(OH)D concentrations, and contrary to previous research [32], postmenopausal women had significantly higher 25(OH)D concentrations than pre- or perimenopausal women.
In this study we observed relatively high group mean concentrations of 25(OH)D ranging from 81 to 87 nmol/l and at group mean level being above 50 nmol/l threshold level even among those who reported not to use supplements, indicating that policy has been successful. An 11-year follow-up study (from 2000 to 2011) in Finland, showed serum 25(OH)D concentrations rose from 48 nmol/l to 65 nmol/l in men and from 48 nmol/l to 66 nmol/l in women, with the prevalence of levels below 50 nmol/l dropping from 55% to 9% in men and from 57% to 9% in women [33]. However, our research did not find a significant correlation between fortified milk intake and 25(OH)D concentrations in middle-aged women, suggesting the possible role of other fortified items. Furthermore, 70–80% of middle-aged women in the present study took supplements containing vitamin D, which may also have contributed to the increase in serum 25(OH)D and prevented the age-associated reduction in serum 25(OH)D. In the older cohort, we did not have information regarding the supplement use but only 16% of women and 7% of men reported use of vitamin D containing medication prescribed by a physician. Nevertheless, the serum 25(OH)D concentrations were quite high, indicating that participants may be using additional non-prescribed supplements.
Research indicates that physical activity, particularly vigorous exercise, is linked to higher 25(OH)D concentrations in middle-aged and older individuals [34,35,36], often due to increased sun exposure [37] but also through intrinsic effects on vitamin D metabolism [34, 36]. Exercise not only boosts serum 25(OH)D concentrations [38, 39] but may also enhance vitamin D receptor and CYP27B1 expression in skeletal muscle [40], suggesting a direct impact on vitamin D metabolism. In our study, middle-aged participants with higher activity levels had superior serum 25(OH)D compared to less active peers, although this association was not observed in older participants. This underscores the potential of physical activity to prevent vitamin D decline, especially in populations like Finnish middle-aged women who generally maintain adequate vitamin D status.
Research consistently shows obesity’s negative impact on 25(OH)D concentrations in middle-aged and older adults [36, 41]. A systematic review of 34 studies identified a slight but significant inverse correlation between BMI and serum 25(OH)D concentrations [42]. Various theories have been proposed, including reduced sunlight exposure among obese individuals [43] and lower vitamin D supplement usage compared to those of normal body mass [41]. Additionally, the hypothesis suggests that vitamin D is more rapidly depleted in obesity due to higher absorption by adipose tissue [44]. Our findings confirm that obese individuals in both middle-aged and older groups have significantly lower serum 25(OH)D concentrations, underscoring obesity as a key factor in diminished vitamin D levels.
Our study utilized a linear mixed model to explore the impact of vitamin D on muscle function and mass, controlling for confounders. Nonetheless, no significant association was found between 25(OH)D concentrations and muscle outcomes in middle-aged women, as well as older men and women. Previous research has documented the association between vitamin D status and muscle outcomes in older adults [15, 45, 46]. Therefore, the lack of a relationship between 25(OH)D concentrations and muscle mass and muscle function may be due in part to the generally high vitamin D levels of the subjects included in this study. Interestingly, in the current cohort, most of the subjects were, in addition to a fortified diet, either taking vitamin D as a supplement or as prescribed drugs. In a meta-analysis, vitamin D supplementation has been shown to protect against lean mass loss and improve lower extremity muscle strength in postmenopausal women [47]. However, other clinical studies have found no significant effect of vitamin D monotherapy on indices of sarcopenia such as muscle mass or strength in community-dwelling older adults [48]. Alternatively, there may be an optimum 25(OH)D concentration required to regulate protein metabolism in skeletal muscle, and exceeding it may not be effective. Further studies are warranted to investigate the optimal 25(OH)D concentration for the prevention of sarcopenia.
This study leverages the robustness of large population-based data, enhancing the generalizability of our findings. However, it is crucial to acknowledge limitations. First, the sampled participants likely represent a healthier segment of the population. This selection bias suggests we might not have fully captured those with the poorest health statuses and the lowest vitamin D status. Second, muscle quality and function were not assessed uniformly between cohorts, as DXA was used in the middle-aged cohort and BIA in the older cohort, which may limit comparability. Third, we did not account for self-prescribed vitamin D supplements in the older cohort, potentially affecting 25(OH)D concentrations. Lastly, physical activity was measured via self-reported questionnaires, which could introduce bias; objective measures like accelerometry would have provided more accurate data.
In conclusion, cohort data from middle-aged and older women and men were used to investigate the relationship between serum 25(OH)D concentrations and SMM and function during the menopausal transition and aging. Sufficient 25(OH)D concentrations were found in the majority of both Finnish middle-aged women and older men and women. However, while menopause leads to a decrease in muscle mass and function, maintaining adequate 25(OH)D concentrations alone does not prevent this decline in middle-aged women. Future studies should investigate the optimal serum 25(OH)D levels needed to affect muscle quality, function, and strength across different age groups, given the lack of significant association found in this study. Examining the influence of vitamin D-related factors, such as vitamin D receptor (VDR) polymorphisms, on muscle function could also reveal insights into individual variability in response to vitamin D fortification or supplementation.
Data availability
Data analyzed during this study are included in this published article. The complete individual-level data is not publicly available due to privacy or ethical restrictions; however, data can be made available upon reasonable requests and subject to ethical approval. The metadata of the ERMA study (doi:10.17011/jyx/dataset/83491) and the AGNES study (doi.10.17011/jyx/dataset/83811) are publicly available at the JYX Digital Repository of the University of Jyväskylä.
References
Xu Y, Hu T, Shen Y, Wang Y, Bao Y, Ma X. Association of skeletal muscle mass and its change with diabetes occurrence: a population-based cohort study. Diabetol Metab Syndr. 2023;15:53 https://doi.org/10.1186/s13098-023-01027-8
Kim JA, Hwang SY, Yu JH, Roh E, Hong SH, Lee YB, et al. Association of the triglyceride and glucose index with low muscle mass: KNHANES 2008-2011. Sci Rep. 2021;11:450 https://doi.org/10.1038/s41598-020-80305-1
Tyrovolas S, Panagiotakos D, Georgousopoulou E, Chrysohoou C, Tousoulis D, Haro JM, et al. Skeletal muscle mass in relation to 10 year cardiovascular disease incidence among middle aged and older adults: the ATTICA study. J Epidemiol Community Health. 2020;74:26–31. https://doi.org/10.1136/jech-2019-212268
Juppi HK, Sipilä S, Cronin NJ, Karvinen S, Karppinen JE, Tammelin TH, et al. Role of Menopausal Transition and Physical Activity in Loss of Lean and Muscle Mass: A Follow-Up Study in Middle-Aged Finnish Women. J Clin Med. 2020;9:1588 https://doi.org/10.3390/jcm9051588
Karvinen S, Juppi HK, Le G, Cabelka CA, Mader TL, Lowe DA, et al. Estradiol deficiency and skeletal muscle apoptosis: Possible contribution of microRNAs. Exp Gerontol. 2021;147:111267 https://doi.org/10.1016/j.exger.2021.111267
Collins BC, Laakkonen EK, Lowe DA. Aging of the musculoskeletal system: How the loss of estrogen impacts muscle strength. Bone. 2019;123:137–44. https://doi.org/10.1016/j.bone.2019.03.033
Endo I, Inoue D, Mitsui T, Umaki Y, Akaike M, Yoshizawa T, et al. Deletion of vitamin D receptor gene in mice results in abnormal skeletal muscle development with deregulated expression of myoregulatory transcription factors. Endocrinology. 2003;144:5138–44. https://doi.org/10.1210/en.2003-0502
Vazquez G, de Boland AR, Boland R. Stimulation of Ca2+ release-activated Ca2+ channels as a potential mechanism involved in non-genomic 1,25(OH)2-vitamin D3-induced Ca2+ entry in skeletal muscle cells. Biochem Biophys Res Commun. 1997;239:562–5. https://doi.org/10.1006/bbrc.1997.7501
Romeu Montenegro K, Amarante Pufal M, Newsholme P. Vitamin D Supplementation and Impact on Skeletal Muscle Function in Cell and Animal Models and an Aging Population: What Do We Know So Far? Nutrients. 2021;13. https://doi.org/10.3390/nu13041110.
Tieland M, Brouwer-Brolsma EM, Nienaber-Rousseau C, van Loon LJ, De Groot LC. Low vitamin D status is associated with reduced muscle mass and impaired physical performance in frail elderly people. Eur J Clin Nutr. 2013;67:1050–5. https://doi.org/10.1038/ejcn.2013.144
Glerup H, Mikkelsen K, Poulsen L, Hass E, Overbeck S, Andersen H, et al. Hypovitaminosis D myopathy without biochemical signs of osteomalacic bone involvement. Calcif Tissue Int. 2000;66:419–24. https://doi.org/10.1007/s002230010085
Kotlarczyk MP, Perera S, Ferchak MA, Nace DA, Resnick NM, Greenspan SL. Vitamin D deficiency is associated with functional decline and falls in frail elderly women despite supplementation. Osteoporos Int. 2017;28:1347–53. https://doi.org/10.1007/s00198-016-3877-z
Gallagher JC. Vitamin D and aging. Endocrinol Metab Clin North Am. 2013;42:319–32. https://doi.org/10.1016/j.ecl.2013.02.004
Zhang J, Cheng Y, Chen C, Wang Q, Yang C, Qiu J, et al. Interaction of estradiol and vitamin D with low skeletal muscle mass among middle-aged and elderly women. BMC Women’s Health. 2023;23:491 https://doi.org/10.1186/s12905-023-02646-z
Park S, Ham JO, Lee BK. A positive association of vitamin D deficiency and sarcopenia in 50 year old women, but not men. Clin Nutr. 2014;33:900–5. https://doi.org/10.1016/j.clnu.2013.09.016
Cangussu LM, Nahas-Neto J, Orsatti CL, Bueloni-Dias FN, Nahas EA. Effect of vitamin D supplementation alone on muscle function in postmenopausal women: a randomized, double-blind, placebo-controlled clinical trial. Osteoporos Int. 2015;26:2413–21. https://doi.org/10.1007/s00198-015-3151-9
Itkonen ST, Andersen R, Björk AK, Brugård Konde Å, Eneroth H, Erkkola M, et al. Vitamin D status and current policies to achieve adequate vitamin D intake in the Nordic countries. Scand J Public Health. 2021;49:616–27. https://doi.org/10.1177/1403494819896878
Blomhoff R, Andersen, R., Arnesen, E.K., Christensen, J.J., Eneroth, H., Erkkola, M., et al. Nordic Nutrition Recommendations 2023. Nordic Council of Ministers, Copenhagen, 2023. pp 374.
Raulio S, Erlund I, Männistö S, Sarlio-Lähteenkorva S, Sundvall J, Tapanainen H, et al. Successful nutrition policy: improvement of vitamin D intake and status in Finnish adults over the last decade. Eur J Public Health. 2017;27:268–73. https://doi.org/10.1093/eurpub/ckw154
Rantanen T, Saajanaho M, Karavirta L, Siltanen S, Rantakokko M, Viljanen A, et al. Active aging - resilience and external support as modifiers of the disablement outcome: AGNES cohort study protocol. BMC Public Health. 2018;18:565 https://doi.org/10.1186/s12889-018-5487-5
Kovanen V, Aukee P, Kokko K, Finni T, Tarkka IM, Tammelin T, et al. Design and protocol of Estrogenic Regulation of Muscle Apoptosis (ERMA) study with 47 to 55-year-old women’s cohort: novel results show menopause-related differences in blood count. Menopause. 2018;25:1020–32. https://doi.org/10.1097/gme.0000000000001117
Hyvärinen M, Juppi HK, Taskinen S, Karppinen JE, Karvinen S, Tammelin TH, et al. Metabolic health, menopause, and physical activity-a 4-year follow-up study. Int J Obes (Lond). 2022;46:544–54. https://doi.org/10.1038/s41366-021-01022-x
Portegijs E, Karavirta L, Saajanaho M, Rantalainen T, Rantanen T. Assessing physical performance and physical activity in large population-based aging studies: home-based assessments or visits to the research center? BMC Public Health. 2019;19:1570 https://doi.org/10.1186/s12889-019-7869-8
Institute of Medicine (US) Committee to Review Dietary Reference Intakes for Vitamin D and Calcium. Dietary Reference Intakes for Calcium and Vitamin D. Dietary Reference Intakes for Calcium and Vitamin D. Washington (DC): National Academies Press (US); 2011.
Bondarev D, Laakkonen EK, Finni T, Kokko K, Kujala UM, Aukee P, et al. Physical performance in relation to menopause status and physical activity. Menopause. 2018;25:1432–41. https://doi.org/10.1097/gme.0000000000001137
Bondarev D, Finni T, Kokko K, Kujala UM, Aukee P, Kovanen V, et al. Physical Performance During the Menopausal Transition and the Role of Physical Activity. J Gerontol A Biol Sci Med Sci. 2021;76:1587–90. https://doi.org/10.1093/gerona/glaa292
Harlow SD, Gass M, Hall JE, Lobo R, Maki P, Rebar RW, et al. Executive summary of the Stages of Reproductive Aging Workshop + 10: addressing the unfinished agenda of staging reproductive aging. J Clin Endocrinol Metab. 2012;97:1159–68. https://doi.org/10.1210/jc.2011-3362
Hyvärinen M, Sipilä S, Kulmala J, Hakonen H, Tammelin TH, Kujala UM, et al. Validity and Reliability of a Single Question for Leisure-Time Physical Activity Assessment in Middle-Aged Women. J Aging Phys Act. 2020;28:231–41. https://doi.org/10.1123/japa.2019-0093
Kujala UM, Kaprio J, Sarna S, Koskenvuo M. Relationship of leisure-time physical activity and mortality: the Finnish twin cohort. Jama. 1998;279:440–4. https://doi.org/10.1001/jama.279.6.440
Portegijs E, Sipilä S, Viljanen A, Rantakokko M, Rantanen T. Validity of a single question to assess habitual physical activity of community-dwelling older people. Scand J Med Sci Sports. 2017;27:1423–30. https://doi.org/10.1111/sms.12782
Pop LC, Shapses SA, Chang B, Sun W, Wang X. Vitamin D-Binding Protein In Healthy Pre- And Postmenopausal Women: Relationship With Estradiol Concentrations. Endocr Pr. 2015;21:936–42. https://doi.org/10.4158/ep15623.Or
Arunabh S, Pollack S, Yeh J, Aloia JF. Body fat content and 25-hydroxyvitamin D levels in healthy women. J Clin Endocrinol Metab. 2003;88:157–61. https://doi.org/10.1210/jc.2002-020978
Jääskeläinen T, Itkonen ST, Lundqvist A, Erkkola M, Koskela T, Lakkala K, et al. The positive impact of general vitamin D food fortification policy on vitamin D status in a representative adult Finnish population: evidence from an 11-y follow-up based on standardized 25-hydroxyvitamin D data. Am J Clin Nutr. 2017;105:1512–20. https://doi.org/10.3945/ajcn.116.151415
Li H, Han D, Wang H, Shu D, Xu L, Hou L, et al. The Relationship Between Vitamin D and Activity of Daily Living in the Elderly. Int J Gen Med. 2022;15:6357–64. https://doi.org/10.2147/ijgm.S366203
Scott D, Ebeling PR, Sanders KM, Aitken D, Winzenberg T, Jones G. Vitamin d and physical activity status: associations with five-year changes in body composition and muscle function in community-dwelling older adults. J Clin Endocrinol Metab. 2015;100:670–8. https://doi.org/10.1210/jc.2014-3519
Brock K, Huang WY, Fraser DR, Ke L, Tseng M, Stolzenberg-Solomon R, et al. Low vitamin D status is associated with physical inactivity, obesity and low vitamin D intake in a large US sample of healthy middle-aged men and women. J Steroid Biochem Mol Biol. 2010;121:462–6. https://doi.org/10.1016/j.jsbmb.2010.03.091
Lee YM, Kim SA, Lee DH. Can Current Recommendations on Sun Exposure Sufficiently Increase Serum Vitamin D Level?: One-Month Randomized Clinical Trial. J Korean Med Sci. 2020;35:e50 https://doi.org/10.3346/jkms.2020.35.e50
Dzik KP, Grzywacz T, Łuszczyk M, Kujach S, Flis DJ, Kaczor JJ. Single bout of exercise triggers the increase of vitamin D blood concentration in adolescent trained boys: a pilot study. Sci Rep. 2022;12:1825 https://doi.org/10.1038/s41598-022-05783-x
Zhang J, Cao ZB. Exercise: A Possibly Effective Way to Improve Vitamin D Nutritional Status. Nutrients. 2022;14:2652 https://doi.org/10.3390/nu14132652
Makanae Y, Ogasawara R, Sato K, Takamura Y, Matsutani K, Kido K, et al. Acute bout of resistance exercise increases vitamin D receptor protein expression in rat skeletal muscle. Exp Physiol. 2015;100:1168–76. https://doi.org/10.1113/ep085207
Orces C. The Association between Body Mass Index and Vitamin D Supplement Use among Adults in the United States. Cureus. 2019;11:e5721 https://doi.org/10.7759/cureus.5721
Saneei P, Salehi-Abargouei A, Esmaillzadeh A. Serum 25-hydroxy vitamin D levels in relation to body mass index: a systematic review and meta-analysis. Obes Rev. 2013;14:393–404. https://doi.org/10.1111/obr.12016
Kull M, Kallikorm R, Lember M. Body mass index determines sunbathing habits: implications on vitamin D levels. Intern Med J. 2009;39:256–8. https://doi.org/10.1111/j.1445-5994.2009.01900.x
Vanlint S. Vitamin D and obesity. Nutrients. 2013;5:949–56. https://doi.org/10.3390/nu5030949
Halfon M, Phan O, Teta D. Vitamin D: a review on its effects on muscle strength, the risk of fall, and frailty. Biomed Res Int. 2015;2015:953241 https://doi.org/10.1155/2015/953241
Kim Y, Chang Y, Ryu S, Cho IY, Kwon MJ, Wild SH, et al. Serum 25-hydroxy vitamin D and the risk of low muscle mass in young and middle-aged Korean adults. Eur J Endocrinol. 2022;186:477–87. https://doi.org/10.1530/eje-21-1229
Tabrizi R, Hallajzadeh J, Mirhosseini N, Lankarani KB, Maharlouei N, Akbari M, et al. The effects of vitamin D supplementation on muscle function among postmenopausal women: a systematic review and meta-analysis of randomized controlled trials. EXCLI J. 2019;18:591–603. https://doi.org/10.17179/excli2019-1386
Prokopidis K, Giannos P, Katsikas Triantafyllidis K, Kechagias KS, Mesinovic J, Witard OC, et al. Effect of vitamin D monotherapy on indices of sarcopenia in community-dwelling older adults: a systematic review and meta-analysis. J Cachexia Sarcopenia Muscle. 2022;13:1642–52. https://doi.org/10.1002/jcsm.12976
Acknowledgements
We would like to thank all participants who contributed their time to take part in ERMA and AGNES studies and the staff of the Gerontology Research Center and the Sport and Health Laboratory of the University of Jyväskylä for their continued involvement.
Funding
This study has been supported by the following grants: Research Council of Finland grants 309504, 314181, 335249 to EKL; JSPS KAKENHI Grant Number JP21KK0177, JYU Visiting Fellow Programme Grant 2022 to SF. This work was supported by an Advanced Grant from the European Research Council (grant no. 693045 to TR) and the Academy of Finland (grant 310526 to TR). The content of this article does not reflect the official opinion of the European Union. Responsibility for the information and views expressed in the article lies entirely with the authors. Open Access funding provided by Ritsumeikan University.
Author information
Authors and Affiliations
Contributions
EKL was principal investigator of the ERMA study and TR was principal investigator of the AGNES study. EKL, SS, and HL contributed to the data collection and validation of the ERMA study and TR, KK, and EP contributed to the data collection and validation of the AGNES study. SF, EKL, and MH contributed to the analysis of the results and the writing of the first draft of the manuscript. SF, HL, KK, MH, SS, EP, TR, and EKL approved the final version.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Fujita, S., Lankila, H., Koivunen, K. et al. Vitamin D sufficiency and its relationship with muscle health across the menopausal transition and aging: Finnish cohorts of middle-aged women and older women and men. Eur J Clin Nutr 79, 731–739 (2025). https://doi.org/10.1038/s41430-025-01610-4
Received:
Revised:
Accepted:
Published:
Version of record:
Issue date:
DOI: https://doi.org/10.1038/s41430-025-01610-4
This article is cited by
-
Prevalence and risk factors of CKD-associated osteoporosis in maintenance hemodialysis patients aged over 50 years: a cross-sectional study
Scientific Reports (2026)
-
Plasma vitamin profiles and their associations with metabolic health and mental wellbeing in midlife Asian women
Scientific Reports (2026)
